
Abstract
This chapter summarizes Chaps. 1, 2, 3, 4 and 5 and introduces the principles of injury prevention. It is concluded that important aspects of human vulnerability appear largely overlooked in traditional fire safety practices and need to be addressed much more seriously if deaths and injuries are to be significantly reduced. When residential fires exceptionally lead to serious harm, it is often due to certain medical, functional, and/or social vulnerabilities of the victim. Since the same vulnerabilities tend to put residents at risk of many other health and safety hazards as well, the fire safety community should join efforts with health and social resources to develop broader programs for safer housing among vulnerable groups, including fire safety. As part of this, new and innovative fire-related solutions are urgently needed to better compensate for human shortcomings in the event of a fire at home.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction – Empirical Summary
The preceding chapters all contribute to a richer understanding of the global fire safety problem. Chapter 1 identifies major data availability and validity problems in many countries, but from what is published on international fire mortality, patterns emerge which seem to reflect well-known global socioeconomic and gender inequalities as well as lifestyle and other cultural patterns such as smoking and alcohol habits, and clothing and cooking traditions. As countries develop, fewer people tend to die from fire, and a transition seems to occur from younger to older victims. Possibly, this also implies a shift over time from female to male victims, as females remain overrepresented mostly in low-income countries while men are at greater risk in high-income countries. Risk factors for residential fire death are explored more in-depth in Chap. 2, identifying both living alone and being under weaker socioeconomic conditions as significant determinants together with demographic and lifestyle factors such as alcohol consumption and smoking. Chapter 3 widens the scope to all residential fires, regardless of consequences, and concludes that most fires seem to be successfully handled by the residents themselves without injuries and without assistance from fire and rescue services. Only exceptionally, residential fires lead to serious harm, and when that happens, it is usually due to certain vulnerabilities related to the victim.
One critical aspect of vulnerability is evacuation ability, as described in Chap. 4. For residents with functional impairments, whether perceptual, cognitive, or motor, normal housing conditions may raise significant barriers for safe evacuation in due time. Chapter 5 identifies intoxication and burn as the leading injury mechanisms from domestic fire. In many cases, intoxication comes first and tends to gradually incapacitate the victim before the heat becomes critical. Both mechanisms covariate with the exposed individual’s age, health, and functional status. Being under the influence of alcohol, medicines, or other substances (including CO from smoking) will accelerate the incapacitation process. The time frame for evacuation is short. Prompt and adequate care (prehospital and clinical) impacts survival and injury severity as well, which makes health care a complementary parameter in reducing death and severe injuries from fires. Finally, as pointed out in Chap. 6, proper surveillance of fire-related injuries and deaths is a fundamental prerequisite for the systematic prevention thereof.
2 General Accident and Injury Prevention Principles
This book concentrates on the prevention of deaths and injuries from fires. Experts in fire safety are usually well trained in fire engineering, but less trained in injury prevention. This gap is what we here wish to bridge with complementary perspectives and theoretical frameworks. When analysing accident and injury causation, a web of intertwined factors emerges behind both the events and their consequences. The consequences are always associated with more contributing factors since these also include vulnerability-related factors in addition to those leading up to the event. Deaths and injuries from fires are therefore not explained solely by the occurrence of the fire, but also by a number of additional factors determining the severity of its outcome.
Injury prevention is a discipline rooted in the medical sphere, taking human vulnerability to sudden external impacts as its point of departure. The nature of impacts varies by type of events; mechanical in case of traffic crashes or falls, thermal and toxic in case of fire, and so on. Humans, just as other species, entail intrinsic tolerances against external impacts to certain degrees, but if the thresholds are exceeded, injuries and death may follow. Moreover, tolerance varies from individual to individual depending on age, sex, health status, etc.
As we now recognize that most people manage fires without being injured and that those killed and severely injured increasingly appear among socially, functionally, and medically disadvantaged groups, the focus of interest will inevitably shift from an exclusive focus on the exposure (the fire) to the specific circumstances that exceptionally contribute to severe outcomes, that is toward the vulnerability side of the problem. The fire occurrence is clearly a necessary cause, but far from sufficient to explain why people die or sustain severe injuries from a fire. It is therefore the complementary causes determining the severe outcomes we need to identify, understand, and address to become able to seriously deal with the number of deaths and injuries from fires.
One of the most influential researchers on injury prevention, representing a human-centered and vulnerability-oriented approach, is undoubtedly Dr. William Haddon Jr. [1, 2]. He had a combined background in epidemiology, medicine, and engineering and published extensively on the principles of prevention, while, at the same time, serving as the first appointed director of the then newly established American federal traffic safety agency in the 1960s [3]. Haddon built his conceptualization of injury causation and prevention on existing frameworks in public health and epidemiology, especially the so-called epidemiologic triad; the host (the exposed individual), the agent (the hazard), and the environment [4]. Accordingly, illness, including injuries, is generally seen as emanating from an interaction between these three components. What distinguishes injuries from diseases is the agent factor, which in the case of injuries consists of a sudden release of energy (or the sudden absence thereof), in contrast to biological or other health hazards. Fractures result from mechanical energy, burns from thermal etc. if exposures occur at amounts and intensity exceeding thresholds for human tolerance. Understanding human tolerance (the vulnerability side) is, therefore, just as important as understanding the sudden hazard exposure conditions (the accident) from a preventative point of view. The basic principle for injury prevention is to control potential exposures and preferably keep them under the human threshold limits. Haddon also built on the, in health sciences well-established, view that preventative measures can be taken in three phases; before, during, and even after an injury occur. Primary preventative measures (before) aim to prevent the exposure as such (the accident), while secondary (during) and tertiary (after) preventions aim to reduce the injury severity, either during the accident sequence (secondary) or afterwards (tertiary) through medical treatment and rehabilitation [5]. One of Haddon’s most famous theoretical contributions is the so-called Haddon Matrix, resulting from a cross-tabulation of the epidemiological triad and the three temporal phases of prevention [1, 4].
Haddon’s theoretical contributions have influenced safety philosophy in many areas, perhaps most clearly in road traffic where the energy perspective, that injuries ultimately are caused by energies allowed to reach individuals at levels exceeding human thresholds of tolerance and therefore need to be kept under these thresholds, has become a dimensioning principle of vehicle and road environment design [6]. The Haddon Matrix is frequently applied as an analytic tool to a wide spectrum of topics in safety research, as well as in public health research in general [1].
Haddon also contributed with a well-known list of ten preventative alternatives, spanning from primary to tertiary prevention [4].
-
1.
To prevent the creation of the hazard in the first place
-
2.
To reduce the amount of hazard brought into being
-
3.
To prevent the release of the hazard that already exists
-
4.
To modify the rate or spatial distribution of release of the hazard from its source
-
5.
To separate, in time or space, the hazard and that which is to be protected
-
6.
To separate the hazard and that which is to be protected by the interposition of a material barrier
-
7.
To modify relevant basic qualities of the hazard
-
8.
To make what is to be protected more resistant to damage from the hazard
-
9.
To begin to counter the damage already done by the environmental hazard
-
10.
To stabilize, repair, and rehabilitate the object of the damage
Reason [7] contributed with a similar view when arguing for, what he called, the principle of “defense-in-depth”, meaning that there is usually a need for several barriers complementing each other. His so-called “Swiss Cheese Model” illustrates how multiple barriers (imaged as cheese slices), each of them with their weaknesses (the holes in the slices), when combined, may complement each other in reducing the likelihood of serious consequences if a harmful event should occur. Thus, one gets access to not just a plan A, but also a plan B, C, D, and so on, in order to reduce the targeted outcome.
The medically anchored approach in injury prevention, as exemplified by Haddon’s theoretical contributions, is a fundamental point of departure in all safety management aiming at preventing human consequences such as deaths and injuries. In addition, safety research has contributed with more engineering-oriented frameworks focused on the events as such (as opposed to the consequences) and their causes, plus managerial issues in administration and organizations to advance performance in safety work. It is, of course, not enough to know what should be done; it takes systematics and leadership as well to make things done and ensure intended results in a societal or organizational context. Part II of this book provides examples of effective measures to save lives and prevent injuries from fire, and the final section will highlight issues on how to implement such measures and make things happen at a broader scale.
3 Implications for the Prevention of Fire-Related Deaths and Injuries
The above summarized can be concluded as follows:
-
It is always the consequences that burden individuals and the community, and therefore, the consequences that need to be prevented and reduced, in this case, deaths and injuries from a fire. A radical way of doing this is to prevent the fires as such. However, since fires remain relatively common, while serious injuries from these are rare, it might be more effective to direct preventative efforts to the contributing factors that mostly determine the negative consequences.
-
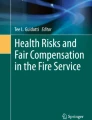
Preventing serious injuries from fire, ultimately deaths, can be accomplished by interventions across the entire process from before to after the fire, see Fig. 7.1. The measures taken can be either individually, technically, and/or organizationally oriented. The principle of “defense-in-depth” is clearly applicable [7].

A tentative illustration of the fire-injury process and how deaths and injuries from fires may be counteracted by interventions along the entire process from pre-fire to post-fire conditions
With reference to Fig. 7.1, the fire-injury process can be described as follows:
-
1.
Ignition may occur through spark, open flame, or hot object.
-
2.
For the fire to grow, it takes dry combustible material in the presence of oxygen.
-
3.
The emissions that harm living organisms in case of fire include toxic gases and heat, primarily. The gases typically attack first by incapacitating the victim. The toxicity depends on the material that is burning, ventilation conditions, and if smouldering or open flame.
-
4.
The degree of exposure, in combination with the lethality of the emissions, determines the speed of the injury process.
-
5.
If the fire continues and escalates, evacuation remains the only option. This can be performed either without assistance or with assistance from cohabitants, neighbours, or professional resources.
-
6.
For those evacuated injured, but still alive, there remains the possibility of avoiding worsening complications and restoring health through adequate treatment and rehabilitation. The result determines the final outcome in terms of deaths and injury severity.
Preventative measures are all those intervening in the implied process and affecting the final outcome. As pointed out, the measures can be individually, technically, or organizationally oriented, separately or in combination. Weaknesses in one respect can be compensated by strengthened measures in other respects. Humans are often considered the least reliable component of so-called sociotechnical systems, and the less one can expect from the individual, the more efforts need to be placed on technology and organization to compensate for human shortcomings. In the context of residential fires and vulnerable groups, the organization can be seen to include actors with the role of supporting the individual, such as social services and medical resources.
Accumulated evidence now demonstrates that serious injury outcomes from fire, including deaths, increasingly are to be seen as a vulnerability problem, at least in richer countries with ageing populations. Vulnerability aspects play roles in several phases of the fire-injury process, such as increasing the risk of ignition and escalation, reducing the capacity to evacuate, and impairing the medical resilience and capacity to respond to care and rehabilitation. Thus, the strategical alternatives to reduce the impact of human vulnerability remain:
-
1.
To try to reduce vulnerabilities, that is, strengthening capacities and resilience among groups at risk
-
2.
To try to compensate for the vulnerabilities by means of technical and organizational arrangements in
-
(a)
Existing homes, as complementary arrangements
-
(b)
Alternative homes, meeting higher intrinsic safety standards (e.g. nursing homes)
-
(a)
The first alternative encompasses three perspectives; first, the medical vulnerability following increasing age and illness and resulting in reduced resilience to a fire’s physiological injury mechanisms; second, impaired perceptual and cognitive capacities resulting in increased difficulties to perceive and understand what might happen; and third, a reduced physical capacity to act adequately. To address these impairments and reach significant improvements entail considerable challenges, but general efforts to promote health at the population level can be expected to result in long-term positive effects.
Alternative 2a offers certain possibilities in terms of warning systems that are easier to perceive and understand, and extinguishing systems activated automatically. Redirecting warning signals to neighbours or professional first responders ready to assist swiftly is another possibility.
Alternative 2b offers the most radical possibilities to improve the protection for those unable to care for themselves for their safety. The enhanced safety standard may include organizational arrangements as well, such as the continuous presence of staff with sufficient capacities to intervene in case of danger.
4 Technical and Organizational Measures for Prevention
As described above, decreasing the vulnerability of the individual is one of the main goals of public health and medical services, but this might be difficult to address from a fire-specific perspective. Therefore, the majority of this anthology is focused on technical and organizational aspects aiming to compensate for this vulnerability.
Inspired by Gielen et al. [8], a modified Haddon-matrix has been developed and is presented in Table 7.1. In the matrix, the temporal dimension is divided into several subsections adopted from Runefors et al. [9] where it was found to be a generic sequence of events in fatal fires.
For each phase, the opportunities for prevention are divided into four different categories: Host, Equipment, Physical environment, and Socio/Cultural environment. The Host relates to aspects in relation to the victim themselves or other individuals and could be, for example, attitudes, knowledge, and behaviour. The Equipment includes aspects of the specific objects involved in the fire, while the Physical environment includes other objects in the environment. Finally, Socio/Cultural factors are external factors such as legislation, campaigns, and institutions such as the rescue service and hospitals.
The matrix, including a range of different identified measures, is presented in Table 7.1.
As can be seen in the table above, there is a wide range of different measures that can all be a part of a fire safety strategy. The measures are not presented here, but the reader is referred to the chapter in this anthology which is cited in the table.
Due to the variation in both exposure and vulnerability, the effectiveness of different technical measures also varies significantly between different socio-demographic groups in society, and this is also true for who currently have the different measures implemented. This is further discussed in Chap. 14.
5 Conclusions
Section one of this anthology clearly shows that fatalities due to residential fires are strongly related to the vulnerability of the individual. It is of paramount importance for fire safety professionals to acknowledge this fact and let it influence the strategies developed.
Despite this, it is argued that directly influencing the vulnerability of the individual is typically out of reach for fire safety professionals. Instead, fire prevention should focus on compensatory measures from a technical and organizational perspective. A range of such measures that each can play a role in fire safety promotion is presented in the following section of this anthology.
However, even if fire safety professionals typically are not able to affect the vulnerability aspect per se, it is very important to apply the knowledge of risk factors presented in Chap. 1 to target safety promotion activities to individuals with high risk. Since the same risk factors tend to put residents at risk of many other health and safety hazards as well, the fire safety community should join efforts with health and social resources to develop broader programs for safer housing among vulnerable groups, including fire safety.
References
Runyan C (2003) Introduction: back to the future – revisiting Haddon’s conceptualization of injury epidemiology and prevention. Epidemiol Rev 25:60–64
Williams AF (1999) The Haddon matrix: its contribution to injury prevention and control. In: Third national conference on injury prevention and control, pp 1999-05-09–1999-05-12
Independent Council for Road Safety International, ICORSI. Dr. William Haddon, Jr. (1926–1985). https://www.icorsi.org/dr-william-haddon-jr-1926-1985. Accessed Sept 2021
Haddon W (1980) Advances in the epidemiology of injuries as a basis for public policy. Publ Health Rep 95(5):411–421
Gjestland T (1955) The Oslo study of untreated syphilis. Acta Derm Venereol Suppl, p 34
Johansson R (2009) Vision Zero – implementing a policy for traffic safety. Saf Sci 47:826–831
Reason J (1997) Managing the risks of organizational accidents. Ashgate, Aldershot
Gielen AC, Frattaroli S, Pollack KM, Peek-Asa C, Yang JG (2018) How the science of injury prevention contributes to advancing home fire safety in the USA: successes and opportunities. Inj Prev 24:i7–i13. https://doi.org/10.1136/injuryprev-2017-042356
Runefors M, Johansson N, van Hees P (2016) How could the fire fatalities have been prevented? An analysis of 144 cases during 2011–2014 in Sweden. J Fire Sci 34(6):515–527. https://doi.org/10.1177/0734904116667962
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2023 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Andersson, R., Runefors, M. (2023). Implications for Prevention. In: Runefors, M., Andersson, R., Delin, M., Gell, T. (eds) Residential Fire Safety. The Society of Fire Protection Engineers Series. Springer, Cham. https://doi.org/10.1007/978-3-031-06325-1_7
Download citation
DOI: https://doi.org/10.1007/978-3-031-06325-1_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-06324-4
Online ISBN: 978-3-031-06325-1
eBook Packages: EngineeringEngineering (R0)