
Abstract
Intrauterine adhesions (IUAs) are primarily an iatrogenic condition, where surgical scarring of the uterus can cause menstrual and reproductive dysfunction. When associated with hematometra through outflow obstruction, IUA can result in pain colloquially known as Asherman’s syndrome. Hysteroscopy seems more accurate in identification of IUA than other modalities. Hysteroscopic adhesiolysis is the primary treatment, though there are multiple emerging approaches for reducing reformation of IUAs, including hormonal therapy, stents, hyaluronic acid, carboxymethylcellulose, and more. Postoperative outcomes largely relate to the extent of preoperative disease, where many women can successfully conceive, particularly for those with mild to moderate IUAs preoperatively. Though IUAs continue to pose a meaningful burden on affected women more than a century after they were first described, research demonstrates prognosis in IUA detection, treatment, and long-term outcomes.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Intrauterine adhesions
- Intrauterine synechiae
- Asherman’s syndrome
- Curettage
- Endometritis
- Infertility
- Amenorrhea
Background
Intrauterine adhesions (IUA) have been recognized as a source for reproductive dysfunction for over a century. The condition was first described in 1894 by Henrich Fritsch for a woman who underwent curettage 24 days postpartum for bleeding, and then she subsequently became amenorrheic [1]. A more comprehensive description of the condition was published by Israeli gynecologist Joseph Asherman 54 years later in his landmark paper “Amenorrhoea traumatica (atretica)” [2]. Of note, this initial article by Dr. Asherman emphasized cervical adhesive disease. His article “Traumatic intrauterine adhesions,” 2 years later gave greater emphasis to the more common finding of intrauterine disease [3].
The condition is often still referred to through terms relating to Joseph Asherman and his article titles, including Asherman’s syndrome, traumatic uterine atrophy, and uterine atresia, as well as endometrial sclerosis. When initially published and described as Asherman’s syndrome, there was emphasis on hematometra with associated pain. Intrauterine adhesions has come to be the preferred term, as it includes circumstances without pain and covering the full spectrum of disease.
Etiology
Setting aside deliberate creation of IUA through endometrial ablation, 90% of IUA or more can relate to curettage [4,5,6], consistent with how it was first described by Fritsch [1]. A study with hysteroscopy 8–10 weeks after dilation and curettage (D&C) saw a 31% incidence of post-D&C intrauterine adhesion formation [7]. Non-curettage surgeries can also contribute to IUA, including myomectomies (hysteroscopic, laparoscopic, and abdominal) (Fig. 5.1), metroplasty, and compressive uterine suturing post-partum, as well as inflammatory environments such as with an embedded IUD (Fig. 5.2) [8]. As a more general principle, the greater the number of procedures that can traumatize the endometrium, the greater the risk for intrauterine adhesions [9].

Complete obliteration of the left portion of the endometrial cavity after open myomectomy

Thick and filmy adhesions after removal of an embedded IUD
The reason surgery is often a driving force for IUA is that it can cause trauma to the stratum basalis, when damage to the stratum functionale can frequently be sloughed with menses. For this reason, it is uncommon to see IUA associated with ascending infections such as PID, unless there is concurrent surgery, such as with curettage for septic abortion. Similarly, when chronic endometritis is found at hysteroscopic adhesiolysis, there is a higher rate of IUA recurrence (44.8% vs 20.8%) [10]. Uterine tuberculosis (and arguably schistosomiasis) seems to be among the rare non-iatrogenic causes and can result in meaningful IUA [6, 11]. Also of note, etiology can influence distribution of IUA. Curettage-associated adhesions are often midline with lower rates of loss of the ostial landmarks. However, IUA deriving from infection may be less likely to follow this pattern and appear more random in their distribution. IUAs after septal incision tend to be in the location of the transected septum and myomectomy-associated IUAs tend to be in the site of the previous myoma(s). Also notably, as a general surgical principle, juxtaposed traumatized surfaces are more likely to result in adhesions than when distant from each other, which is part of why laparoscopy results in fewer adhesions than laparotomy. For IUA, curettage often traumatizes both the anterior and posterior stratum basale. Similarly, hysteroscopic myomectomy for a single fibroid is less likely to result in adhesions than resection of anterior and posterior “kissing” fibroids [12].
Estimates of the extent attributable to obstetrical curettage (elective termination, miscarriage, and postpartum indications) vary widely. One summary suggested that misoprostol-induced expulsion of pregnancy led to negligible rates of IUA, while it was 15–20% after D&C and 20–40% after curettage for postpartum hemorrhage [13]. Variation in estimates can relate to indications, instrumentation (sharp vs. suction curettage), and visualization (blind vs. ultrasound guided). Postpartum curettage may have IUA exacerbated by lactational amenorrhea hindering endometrial proliferation. It has been proposed that hysteroscopic management of retained products of conception may decrease IUA risk [14].
Pathophysiology
Intrauterine adhesions at the microscopic level can be characterized by loss of ribosomes and mitochondria, as well as cellular hypoxia [15]. Correction of hypoxia relates to successful correction of IUA, where patients with higher VEGF levels and microvessel density appear more likely to redevelop the endometrium after surgical management [15]. Histology can be myometrial, endometrial, or connective tissue and may relate to etiology. Fibromuscular bands are the most common finding and these sometimes contain endometrial tissue [16].
Clinical Presentation
IUA are considered rare, with Orphanet estimating the prevalence at 1–5/10,000 people. (Orpha:137686, [17]) Paradoxically, Orphanet also estimates the prevalence in subfertile populations from 2.8% to 46%, when subfertility affects one in eight couples. Regardless, the true incidence of IUA is likely underreported. If only 10% of the uterine cavity is annealed and 90% is normal, some women may not notice a 10% reduction in menstrual volume. Also, when IUA are more extensive, many women do not seek gynecologic care to assess lighter menstrual flow. A recent study saw a trend toward lighter menses with increasing severity of IUA, where for mild disease 57.4% of women had light or absent menses, for moderate 69.6%, and severe 90% (9/10), but this trend was not statistically significant [18].
Additionally, though IUA may be recognizable to experienced sonographers, some are more attuned to finding masses than they are to endometrial thinning or loss of the border delineating anterior from posterior endometrium. Because it is difficult to find what one is not looking for, IUA-associated absences on sonography can require insight similar to that in Sherlock Holmes’s recognition of a “dog that didn’t bark.” Wider use of office hysteroscopy will likely lead to increased estimates in the prevalence of IUA.
Acknowledging that the most common presentation for IUA may be an absence of symptoms, menstrual disturbance is likely the most common complaint resulting from IUA. A large study from four decades ago noted in women with IUA a 37% rate of amenorrhea and 31% reporting hypomenorrhea [4]. A more recent study in a subfertility population observed 14.6% and 46.3% rates respectively [19]. Symptoms do not clearly correlate with the extent of adhesions [20].
If amenorrhea and hypomenorrhea relate to the extent of endometrial loss, then dysmenorrhea and pelvic pain are proportionate to menstrual entrapment. In this setting, it is easier for pain-associated symptoms to derive from cervical adhesive disease than uterine. The reason is that it takes an extended area of adhesions within the uterus to fully obstruct outflow from a small area (and with proportionate reduction in menstrual flow for that adherent region). However, adhesions only a few millimeters wide in the cervix may be sufficient to completely block outflow. Tubal occlusion can further exacerbate dysmenorrhea and pelvic pain from intrauterine and intracervical adhesions when menses are obstructed, similar to that seen with iatrogenically induced adhesions found in post-ablation tubal sterilization syndrome (PATSS).
IUA can also contribute to subfertility and recurrent pregnancy loss. IUA don’t have overlying endometrium favorable to implantation and typically lack vascularity that would help sustain a developing pregnancy. Though up to half of women with IUA can have difficulties conceiving and sustaining a pregnancy, this may be an overestimate influenced by detection bias [21, 22].
Diagnosis of Intrauterine Adhesions
Multiple approaches are used to identify IUA, including hysterosalpingography (HSG), sonography, saline infusion sonography (SIS), 3D sonohysterography (including 3D power Doppler), and MRI. HSG seems to have a particularly high rate of false positives and negatives for IUA relative to SIS, with relative accuracies of 26.9% and 63.2% respectively [23]. Hysteroscopy remains the gold standard and can identify up to a third more IUA than 3D sonohysterography [24], but not all studies find a clear advantage [25]. Not only can saline infusion sonography be used for preoperative visualization of IUA, but catheter placement and balloon inflation can even offer some development of the cavity. However, beyond detection of adhesions, there are multiple advantages to office hysteroscopy relative to other approaches prior to surgical intervention. First, office hysteroscopy is the best proxy for intraoperative conditions. Knowing whether there are visible intraoperative landmarks has important implications when addressing the balance of risk and benefit for informed consent, including expectations for the number of procedures required for more extensive disease. Second, office hysteroscopy facilitates better preparation, such as whether intraoperative sonography would be advantageous. Third, office hysteroscopy allows for a degree of see and treat, where with gentle sweeping of filmy adhesions, one can better develop the cavity, better delineating surgical planes.
For detecting IUA, all estimates of accuracy through sonography should be interpreted in the light of the year of the study, the timing within the menstrual cycle, the nature of image analysis, and the type of IUA being identified. The earlier the study, the greater the risk for lower resolution which negatively affects sensitivity and specificity. Within the menstrual cycle, the luteal phase allows for easier delineation of intracavitary structures that contrast with the robust endometrium. The greater the use of iatrogenic contrast or 3D, the greater the amount of information, which enhances accuracy. Finally, the more prevalent hematometra are in studies, the easier it is to identify IUA due to contrasting intracavitary blood.
Intracervical adhesions often present sonographically as an echogenic line that can be traced from the cervix to a point where the line dissipates. Depending on where the patient is in the menstrual cycle, a cervical mucocele or hematocele should prompt suspicion for adhesions or stricture in the lower cervix. These may fill the upper cervix due to difficult egression, with difficulty identifying the lower path to the outer cervical os on sonography. When MRI is used due to cervical adhesions hindering SIS, T2-weighted images will visualize IUA as having low signal intensity within the uterine cavity.
When using sonography for intracavitary evaluation, intrauterine adhesions may present more as heterogeneous opacity, where there is homogeneous echogenicity across measurements of endometrial thickness, excepting portions where an interface between the anterior and posterior can be segmentally identified. The less the interface can be visualized, the greater the potential for thicker adhesions. Saline and other contrast, such as fluids, foams, and gels, can further help delineate points of fusion between the anterior and posterior endometrium. Hematometra may present as low-level homogeneous echoes, though this will be dependent on where the patient is in the menstrual cycle and the duration the hematometra has been present.
Classification of Intrauterine Adhesions
In 1978, March proposed a hysteroscopic classification system for intrauterine adhesions that remains in wide use due to its simplicity [26]. It is broken into three categories: minimal (Fig. 5.3), moderate (Fig. 5.4), and severe (Fig. 5.5). This approximately correlates with the American Fertility Society classifications of I, II, and III respectively [27]. Though these classification systems are easy to understand and communicate, their ability to predict subsequent menstrual function and fecundity are limited. However, more advanced classification systems, such as those proposed by the European Society for Hysteroscopy [28], Nasr [29], and others have had less widespread use (Table 5.1). Moreover, heterogeneity in IUA etiology, presentation, severity, and management (both technique and surgical skill) will hinder the predictive value for any model.

Minimal adhesions after dilation and curettage for endometrial hyperplasia, followed by Megace treatment

Moderate adhesions after dilation and curettage for first-trimester miscarriage

Severe adhesions, with almost complete intracavitary obliteration after dilation and curettage to remove a polyp (rather than directed visualization and resection). Central and fundal location of the hysteroscope was confirmed with concurrent sonography
Surgical Considerations
In 1950, Joseph Asherman described the management of IUA through hysterotomy and sweeping his finger to lyse adhesions [3]. With advancements in intraoperative imaging and hysteroscopy, such an approach should be rarely utilized for modern surgical management. Surgical planning to correct IUA focuses on patients wishing to preserve fertility, as hysterectomy and uterine artery embolization are less depending on the extent of intracavitary disease.
Under March’s classification system, mild and moderate diseases have lateral landmarks, which would typically allow them to be managed as a single hysteroscopic surgery, whether in the office or in the operating room. Severe disease often should be managed in the operating room owing to the degree of risk for uterine perforation. Two preoperative steps have high value in facilitating surgery prior to the actual event. First, preoperative estrogen (2 mg estradiol BID or TID for 4–8 weeks) driving endometrial proliferation may help visualize the endometrium when intraoperative sonography is used (particularly if adhesions prevent saline-associated delineation of the uterine cavity), as well as contribute to postoperative healing. Second, preoperative mapping within the office may enhance planes and efficiency within the operating room. Care is needed to avoid false tracts and patient analgesia must be considered if using sonographically guided dilators or small caliber office hysteroscopy. However, sweeping filmy adhesions to define landmarks and more dense adhesions, coupled with a degree of healing preoperatively, can facilitate efficient use of time within the operating room, as well as guide expectations for outcomes. This preoperative approach parallels McComb and Wagner’s operative technique with laparoscopic observation of transcervical exploration with 13 French Pratt dilators, followed by hysteroscopic resection of residual bands [33].
For surgical technique, there is significant debate among gynecologists regarding the use of scissors relative to energy (or laser), such as with a resectoscope or needle point cautery. Proponents of a cold scissors approach note that the use of cautery can hinder endometrial regrowth and perforation when energy has been used poses greater risk of meaningful bowel injury than when this occurs through mechanical means [34]. However, when adhesions have strictured the cervix and a cruciate incision for expansion is planned or when myometrial scoring is used to expand the uterine cavity, cautery can reduce bleeding that might otherwise lead to early cessation of the procedure [35, 36].
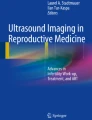
Intraoperatively, concurrent sonographic imaging can enhance confidence for location when surgical boundaries are obscured. Particularly in obese patients, transrectal sonography may offer greater clarity through improved proximity to the anatomy. If transabdominal visualization of the remaining distance to the fundal serosa is suboptimal, a few air bubbles can be added and may be more readily visible due to their echogenicity (Fig. 5.6a, b).

(a, b). Transabdominal ultrasound-guided resection of intrauterine adhesions, where the distance from the endometrial apex to fundal serosa is less clear in a, but more clear after addition of air bubbles in b
Postoperative Management
The need for postoperative adhesion prevention is proportionate to the extent of disease. One study did not observe adhesion reformation for mild disease, but it occurred in a sixth with moderate disease and in 42% of those with severe disease [37]. There are three core approaches to preventing adhesion recurrence postoperatively: hormonal therapy, barrier placement, and office hysteroscopy with lysis of newly forming adhesions. All approaches appear beneficial in preventing reformation of adhesions and there isn’t clear or convincing evidence that use in combination improves outcomes. However, this may also be a function of limited statistical power to assess such differences. Though estrogen is known to improve endometrial proliferation, it may not be able to cause regeneration over scarred and devascularized tissue. Of note, sildenafil has been used for endometrial proliferation after IUA, but this was a case report with only two patients [38].
IUDs have been used as barriers, but copper IUDs can be inflammatory. Though one trial showed improved menses with copper IUD use [39], another study showed worse outcomes than not using any postoperative treatment [40]. Similarly, progesterone containing IUDs can thin endometrium, when the goal is for endometrial proliferation. Inflating the balloon for a pediatric foley catheter is particularly good for midline disease and one study showed superior outcomes relative to the use of an IUD (33.9% vs 27.5% subsequent conception) [41]. However, when using this approach, one should avoid overinflation, as this can lead to significant discomfort. There are balloon stents designed for placement after hysteroscopic adhesiolysis, but these can be difficult to place and remove.
Though not shown to be superior for outcomes, arguably second look office hysteroscopy should be the gold standard. The reason is that it is not only effective in treating recurring adhesions, but will also validate the efficacy of the initial surgery [12, 42]. Cost in some settings can be an obstacle, and as such may be more appropriate for patients with moderate to severe IUA, where recurrence is more probable. Alternatively, pressure lavage under ultrasound guidance (PLUG) can be performed, where overdistention of the uterus can lead to lysis of filmy adhesions through separation of the anterior and posterior walls [43]. However, without direct visualization there may be a greater risk for missing lateral adhesion reformation. Additionally, though in the initial publication only 43% (three out of seven) patients reported moderate discomfort, procedures that overdistend the uterus are inherently more likely to be uncomfortable than those that do not.
Regarding emerging approaches to prevent postoperative IUA recurrence, antibiotics do not appear to improve outcomes before or after surgical management of IUA [9]. The use of barriers derived from hyaluronic acid and freeze-dried amnion applied to a Foley balloon seem to have potential according to a meta-analysis of randomized controlled trials [44]. However, the challenge in interpreting results relating to dissolvable barrier therapy is that few centers have published data relating to their use, leading to debate for external validity. The most supportive data seem to relate to alginate hyaluronate–carboxymethylcellulose use and to polyethylene oxide with sodium carboxymethyl cellulose. However comparative effectiveness, as well as cost-effectiveness, relative to approaches such as postoperative estrogen and second-look hysteroscopy need to be better addressed before there is wider uptake. There has been a case report of successful stem cell use after bone marrow biopsy (coupled with estrogen therapy and subsequent IVF with donor eggs), but without additional data, this is likely best left to research settings at this time [45]. Similarly, aspirin, nitroglycerin, and sildenafil have been used for enhancing myometrial and endometrial perfusion, but additional studies are needed to have confidence in recommendations.
Postoperative Outcomes
The more severe the presence of adhesions, the greater the likelihood for needing additional surgery. Patients with limited endometrium preoperatively are less likely to have a satisfactory postoperative outcome [46]. (Fig. 5.7) Minimal disease is almost always manageable with a single procedure. For moderate IUA, 78% of women require a single surgery for completion, and 50% with severe IUA [31, 47]. Moreover, for severe disease, 26% may require three to four surgeries [47]. Additionally, Adhesion recurrence is highly dependent on the extent of initial disease. One large series with hysteroscopic reassessment 8–10 weeks postoperatively in 683 women saw a 28.7% rate of IUA recurrence [6]. Favorable outcomes seem linked not only to preexisting pathology, but also the age of the patient and adhesions being more in the uterus than the cervix [48].

Partially reconstructed uterine cavity after endometrial ablation
Postoperative success is not simply surgical completion, or restoration of the uterine cavity—for women with procreative goals, success is defined through conception leading to a live birth. Approximately half of women having adhesiolysis for IUA will subsequently conceive [49]. For good prognosis women, pregnancy rates can be as high as 79% with a 63.7% chance of live birth [5]. Of note, for these good prognosis women, two-thirds of them conceived spontaneously. Practically all of these conceptions were within the first year when followed as far as 5 years postoperatively. However, for women with severe IUA, only 27–32% may successfully have a live birth [20, 47, 50]. A recent large retrospective study via phone survey saw 54.3% (38/70) of women with mild adhesions able to have a term or pre-term delivery or ongoing pregnancy and 70.9% (51/72) of those with moderate adhesions [18]. However, for those with severe disease, only 28.8% (2/7) had a term, pre-term, or ongoing pregnancy. Similarly, a large retrospective study from China’s largest women’s hospital showed subsequent conception rates of 60.7% for mild disease, 53.4% for moderate disease, and 25% for severe disease [51].
Patients with severe disease should know that a quarter to a third of pregnancies may result in first- or second-trimester loss and 10.1% of live births may be associated with placenta accreta [5, 49]. The recent large retrospective study previously cited saw 45.7% of those with mild disease having spontaneous loss, termination, or ectopic pregnancy [18]. This was only 29.2% of those with moderate disease but 71.4% (5/7) of those with severe disease. Another large study detailing obstetrical outcomes saw 17.6% with abnormal placentation, 4.7% with postpartum hysterectomy, and 29.4% with prematurity [5].
Conclusions
Intrauterine adhesions are a meaningful source of reproductive dysfunction. Causing hypomenorrhea, dysmenorrhea, pelvic pain, and subfertility, correction can improve reproductive outcomes. Imaging or hysteroscopic visualization coupled with an appropriate index of suspicion are central to diagnosis. Multiple treatment options exist, but limitations of sample size for many established approaches and single or a few centers having expertise for emerging approaches need to be considered when considering overall validity. However, many women after treatment, particularly with minimal or moderate disease, will successfully conceive without need for a gestational carrier. Core research opportunities include not only better understanding of the molecular mechanisms behind IUA, but also surgical technique and postoperative treatments to minimize recurrence.
References
Fritsch H. Ein fall von volligem schwaund der gebormutterhohle nach auskratzung. Zentralbl Gynaekol. 1894;18:1337–42.
Asherman JG. Amenorrhoea traumatica (atretica). J Obstet Gynaecol Br Emp. 1948;55:23–30.
Asherman JG. Traumatic intrauterine adhesions. J Obstet Gynaecol Br Emp. 1950;57:892–6.
Schenker JG, Margalioth EJ. Intrauterine adhesions: an updated appraisal. Fertil Steril. 1982;37(5):593–610.
Deans R, Vancaillie T, Ledger W, Liu J, Abbott JA. Live birth rate and obstetric complications following the hysteroscopic management of intrauterine adhesions including Asherman syndrome. Hum Reprod. 2018;33(10):1847–53.
Hanstede MM, Van Der Meij E, Goedemans L, Emanuel MH. Results of centralized Asherman surgery, 2003–2013. Fertil Steril. 2015;104(6):1561–8.
Hooker AB, de Leeuw RA, Twisk JW, Brölmann HA, Huirne JA. Reproductive performance of women with and without intrauterine adhesions following recurrent dilatation and curettage for miscarriage: long-term follow-up of a randomized controlled trial. Hum Reprod. 2021;36:70–81.
Ibrahim MI, Raafat TA, Ellaithy MI, Aly RT. Risk of postpartum uterine synechiae following uterine compression suturing during postpartum haemorrhage. Aust N Z J Obstet Gynaecol. 2013;53(1):37–45.
Deans R, Abbott J. Review of intrauterine adhesions. J Minim Invasive Gynecol. 2010;17:555–69.
Chen Y, Liu L, Luo Y, Chen M, Huan Y, Fang R. Prevalence and impact of chronic endometritis in patients with intrauterine adhesions: a prospective cohort study. J Minim Invasive Gynecol. 2017;24:74–9.
Krolikowski A, Janowski K, Larsen JV. Asherman syndrome caused by schistosomiasis. Obstet Gynecol. 1995;85:898–9.
Taskin O, Sadik S, Onoglu A, Gokdeniz R, Erturan E, Burak K, Wheeler JM. Role of endometrial suppression on the frequency of intrauterine adhesions after resectoscopic surgery. J Am Assoc Gynecol Laparosc. 2000;7(3):351–4.
Hooker AB, Lemmers M, Thurkow AL, Heymans MW, Opmeer BC, Brolmann HA, Mol BW, Huirne JA. Systematic review and meta-analysis of intrauterine adhesions after miscarriage: prevalence, risk factors and long-term reproductive outcome. Hum Reprod Update. 2013;20:262–78.
Vitale SG, Parry JP, Carugno J, Chokeri-Singh A, Della Corte L, Cianci S, Schiattarella A, Riemma G, De Franciscis P. Surgical and reproductive outcomes after hysteroscopic removal of retained products of conception: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2021;28(2):204–17.
Chen Y, Chang Y, Yao S. Role of angiogenesis in endometrial repair of patients with severe intrauterine adhesion. Int J Clin Exp Pathol. 2013;15:1343–50.
Dmowski WP, Greenblatt RB. Asherman’s syndrome and risk of placenta accreta. Obstet Gynecol. 1969;34:288–99.
Morales B, Movilla P, Wang J, Wang J, Williams A, Chen T, Reddy H, Tavcar J, Loring M, Morris S, Isaacson K. Patient reported menstrual and obstetrical outcomes following hysteroscopic adhesiolysis for Asherman syndrome. F S Rep. 2021;2:118–25.
Baradwan S, Baradwan A, Al-Jaroudi D. The association between menstrual cycle pattern and hysteroscopic March classification with endometrial thickness among infertile women with Asherman syndrome. Medicine. 2018;97(27):1–4.
March CM. Intrauterine adhesions. Obstet Gynecol Clin N Am. 1995;22:491–505.
Schenker JG. Etiology of a therapeutic approach to synechia uteri. Eur J Obstet Gynecol Reprod Biol. 1996;65:109–13.
Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98(5):1103–11.
Acholonu UC Jr, Silberzweig J, Stein DE, Keltz M. Hysterosalpingography versus sonohysterography for intrauterine abnormalities. JSLS. 2011;15(4):471–4.
Makris N, Kalmantis K, Skartados N, et al. Three-dimensional hysterosonography versus hysteroscopy for the detection of intracavitary uterine abnormalities. Int J Gynecol Obstet. 2007;97:6–9.
Abou-Salem N, Elmazny A, El-Sherbiny W. Value of 3-dimensional sonohysterography for detection of intrauterine lesions in women with abnormal uterine bleeding. J Minim Invasive Gynecol. 2010;17:200–4.
March C, Israel R, March A. Hysteroscopic managment of intrauterine adhesions. Am J Obstet Gynecol. 1978;130:653–7.
American Fertility Society classifications of adnexal adhesions, distal tubal occlusion, tubal occlusion secondary to tubal ligation, tubal pregnancies, Mullerian anomalies and intrauterine adhesions. Fertil Steril. 1988;49:944–55.
Wamsteker K, DeBlok SJ. Diagnostic hysteroscopy: technique and documentation. In: Sutton C, Diamond M, editors. Endoscopic surgery for gynecologists. New York: Lippincott Williams & Wilkins Publishers; 1995. p. 263–76.
Nasr AL, Al-Inany HG, Thabet SM, Aboulghar MA. A clinicohysteroscopic scoring system of intrauterine adhesions. Gynecol Obstet Investig. 2000;50:178–81.
Hamou J, Salat-Baroux J, Siegler A. Diagnosis and treatment of intrauterine adhesions by microhysteroscopy. Fertil Steril. 1983;39:321–6.
Valle RF, Sciarra JJ. Intrauterine adhesions: hysteroscopic diagnosis classification, treatment, and reproductive outcome. Am J Obstet Gynecol. 1988;158:1459–70.
Donnez J, Nisolle M. Hysteroscopic adheisolysis of intrauterine adhesions (Asherman syndrome). In: Donnez J, editor. An atlas of laser operative laparoscopy and hysteroscopy. London: Parthenon Publishing Group; 1994.
McComb PF, Wagner BL. Simplified therapy for Asherman’s syndrome. Fertil Steril. 1997;68:1047–50.
March CM, Miller C. Hysteroscopic lysis of intrauterine adhesions. Obs Gynecol News. 2006;41:36–7.
Wood MA, Kerrigan KL, Burns MK, Glenn TL, Ludwin A, Christianson MS, Bhagavath B, Lindheim SR. Overcoming the challenging cervix: identification and techniques to access the uterine cavity. Obstet Gynecol Surv. 2018;73(11):641–9.
Protopapas A, Shushan A, Magos A. Myometrial scoring: a new technique for the management of severe Asherman’s syndrome. Fertil Steril. 1998;69:860–4.
Yu D, Tin-Chiu L, Xia E, et al. Factors affecting reproductive outcome of hysteroscopic adhesiolysis for Asherman’s syndrome. Fertil Steril. 2008;89(3):715–22.
Zinger M, Liu JH, Thomas MA. Successful use of vaginal sildenafil citrate in two infertility patients with Asherman’s syndrome. J Women’s Health. 2006;15:442–4.
Vesce F, Jorizzo G, Bianciotto A, Gotti G. Use of the copper intrauterine device in the management of secondary amenorrhea. Fertil Steril. 2000;73:162–5.
Acunzo G, Guida M, Pellicano M, et al. Effectiveness of auto-crosslinked hyaluronic acid gel in the prevention of intrauterine adhesions after hysteroscopic adhesiolysis: a prospective, randomized, controlled study. Hum Reprod. 2003;18:1918–21.
Orhue AA, Aziken ME, Igbefoh JO. A comparison of two adjunctive treatments for intrauterine adhesions following lysis. Int J Gynaecol Obstet. 2003;82:49–56.
Robinson JK, Colimon LM, Isaacson KB. Postoperative adhesiolysis therapy for intrauterine adhesions (Asherman’s syndrome). Fertil Steril. 2008;90(2):409–14.
Coccia ME, Becattini C, Bracco GL, Pampaloni F, Bargelli G, Scarselli G. Pressure lavage under ultrasound guidance: a new approach for outpatient treatment of intrauterine adhesions. Fertil Steril. 2001;75(3):601–6.
Yan Y, Xu D. The effect of adjuvant treatment to prevent and treat intrauterine adhesions: a network meta-analysis of randomized controlled trials. J Minim Invasive Gynecol. 2018;25(4):589–99.
Nagori CB, Panchal SY, Patel H. Endometrial regeneration using autologous adult stem cells followed by conception by in vitro fertilization in a patient of severe Asherman’s syndrome. J Hum Reprod Sci. 2011;4:43–8.
Schlaff WD, Hurst BS. Preoperative sonographic measurement of endometrial pattern predicts outcome of surgical repair in patients with severe Asherman’s syndrome. Fertil Steril. 1995;63:410–3.
Capella-Allouc S, Morsad F, Rongieres-Bertrand C, et al. Hysteroscopic treatment of severe Asherman’s syndrome and subsequent fertility. Hum Reprod. 1999;14(5):1230–3.
Chen L, Xiao S, He S, Tian Q, Xue M. Factors that impact fertility after hysteroscopic adhesiolysis for intrauterine adhesions and amenorrhea: a retrospective cohort study. J Minim Invasive Gynecol. 2020;27:54–9.
Guo EJ, Chung JP, Poon LC, Li TC. Reproductive outcomes after surgical treatment of Asherman syndrome: a systematic review. Best Pract Res Clin Obstet Gynaecol. 2019;59:98–114.
Fernandez H, Peyrelevade S, Legendre G, et al. Total adhesions treated by hysteroscopy: must we stop at two procedures? Fertil Steril. 2012;98(4):980–5.
Chen L, Zhang H, Wang Q, Xie F, Gao S, Song Y, Dong J, Feng H, Xie K, Sui L. Reproductive outcomes in patients with intrauterine adhesions following hysteroscopic adhesiolysis: experience from the largest women’s hospital in China. J Minim Invasive Gynecol. 2017;24:299–304.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Parry, J.P., Ott, J. (2022). Intrauterine Adhesions. In: Lindheim, S.R., Petrozza, J.C. (eds) Reproductive Surgery. Springer, Cham. https://doi.org/10.1007/978-3-031-05240-8_5
Download citation
DOI: https://doi.org/10.1007/978-3-031-05240-8_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-05239-2
Online ISBN: 978-3-031-05240-8
eBook Packages: MedicineMedicine (R0)