
Abstract
Traditionally, patients with recurrent anterior instability have been treated with s soft-tissue technique, mostly Bankart. Higher recurrence rates in the presence of bone defects have increased the interest in techniques that may restore glenoid bone stock, and Latarjet has been the most favored technique. The effective results of this technique in patients with bone defects has extended its use for patients without them promoted by the high rate of recurrence after long-term follow-up of isolated Bankart repairs. Some techniques have been developed to augment Bankart repair with other procedures to decrease the rate of recurrence, remplissage being the most widely used in the presence of Hill-Sachs injuries. This chapter will focus mainly on the highest available evidence regarding the results of recurrent anterior instability comparing mostly the Bankart and Latarjet techniques although the reader should keep in mind that there are many other operations for this problem and that these techniques are subject to a myriad of combinations and additaments that can make comparisons between studies difficult and may be artificial.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
4.1 Introduction
Anterior shoulder dislocation is the most common major joint dislocation [1]. Anterior instability represents 90% of all shoulder dislocations [2]. Recurrence is frequent in the younger age groups in certain patterns of injury with bone loss and certain activities mostly overhead or contact sports. These populations represent a challenge to the treating surgeon.
In patients with recurrent shoulder dislocation, a surgical operation may be needed to improve shoulder function. The most reported shoulder surgeries for this problem are the arthroscopic Bankart repair and an open Latarjet procedure [1, 3].
The new technology of implants and techniques make Bankart repair of older studies (before 2000–2004) difficult to compare with more modern studies even though the surgical technique could be considered analogous [4].
It is undisputed that an arthroscopic Bankart repair has a few advantages with respect to the open Bankart technique, mostly less operative time, less morbidity, less postoperative pain, less hospitalization time, and less risk of complications [5].
Most surgeons will use arthroscopic techniques, in part influenced by the preferences of the patients, in part influenced by the exposure they have had during their training, in which they rarely see an open Bankart repair. However, recurrent instability is a frequent complication after an arthroscopic Bankart repair [6].
The Latarjet technique has been popular in France, where it was developed, not so much in the rest of the world. Its use has since expanded favored by the recognition of the importance of bone loss in the genesis of recurrences and its good outcomes in this setting when compared to other techniques [7].
Also, the development of arthroscopic techniques, new modes of fixation, and modifications of the Latarjet technique (including repair of glenohumeral ligaments) may modify the results of this technique and, perhaps, the rate of complications, so the debate is guaranteed to last a few more years [8]. The debate between the choices of techniques is based on the preference and skills of the surgeon more than in the published evidence [7].
It is almost unanimous that in the face of a critical glenoid bone defect (>25%) most surgeons will perform some kind of glenoid bone grafting, typically a Latarjet, but it is not clear what the attitude should be in defects under 25% in what has been termed ambiguously as subcritical or borderline bone defects or even in the absence of a glenoid bone defect [9].
Some surgeons will skew their decision based on the age and type of activity. It has been shown that, in the younger patients and those practicing throwing sports, anteroinferior shoulder instability is a frequent condition [10].
Patients older than 40 years were thought to have less recurrent instability after a Bankart repair, but recent long-term follow-up has shown increased recurrence rate when compared to Latarjet (9 vs 3; P = 0.037, in a cohort of 37 shoulders) and without the supposed benefit of decreasing the rate of arthropathy. The mechanism for arthropathy is unknown, but it has been correlated with the number of preoperative dislocations, the time of follow-up, and graft malposition or protruding implants [11].
The best procedure for recurrent anterior instability is yet controversial, and good results can be achieved with most techniques, but analysis of failures can help us guide our decision-making [12].
In this chapter, we will perform a review of available modern literature to try to determine which of the surgical techniques are recommended for treatment of anterior instability of the shoulder.
4.2 Bankart Procedure
4.2.1 Open Bankart Repair
According to Moroder et al. (2015), it was thought that neglected osseous glenoid defects was one of the causes for the high rates of recurrence published after long-term follow-up of open Bankart repair [13]. In a level IV study, the authors hypothesized that, in the absence of an important glenoid defect, an open Bankart repair would obtain a low rate of recurrence, so they examined 47 patients treated with an open Bankart repair. They obtained a double-contrast computed tomography scanning to exclude patients with a significant glenoid bone defect. Forty patients (85.1%) are available for evaluation after minimum follow-up of 20 years (maximum 25 years). Twenty-six (65%) were evaluated using a clinical exam and a bilateral radiograph of the shoulder, and the rest responded to a self-administered questionnaire and a telephone interview. Seven patients (17.5%) reported a recurrence, and in six of them it happened after being asymptomatic for more than 8 years. The mean Western Ontario Shoulder Instability Index (WOSI, See Appendix 1) score was 256.7 points, the mean Rowe score (Table 4.1) was 88.7 points, and the mean Subjective Shoulder Value (SSV) was 90.1%. When comparing it to the contralateral side, the mean range of motion of the operated shoulder was reduced in 4° of flexion, two levels of internal rotation, 5° of internal rotation, 5° of internal rotation in 90° of abduction, 7° of external rotation in neutral, and 7° of external rotation in 90° of abduction. The collective instability arthropathy index was 0.92 and 0.35 for the affected shoulder and the contralateral one, respectively. An open Bankart procedure obtained good results at 20 years of follow-up. However, the rate of recurrence was high, even after excluding patients with significant glenoid defects, and was associated with an increased shoulder-specific activity level [13].
According to Boshan et al., open Bankart repair shows a low rate of complications, and it still is an excellent surgical option for a selected group of patients with risk factors for failure after an arthroscopic Bankart repair, those being a previous history of recurrent instability or ligamentous laxity, concomitant glenoid or humeral bone defects, being a male, having a young age, and practicing contact sports. The authors highlight that controlling risk factors is especially important in patients that are not candidates for glenoid bone augmentation [2].
4.2.2 Arthroscopic Bankart Repair
Balg et al. described in 2007 the Instability Severity Index Score (Table 4.2). They found that a younger age, the use of the shoulder score for contact sports or overhead use, the use of the shoulder for sports competition activities, the association of hyperlaxity, and the presence of Hill-Sachs or glenoid erosion or avulsion were associated with increased failure rates after an arthroscopic Bankart repair [14].
Some controversy exists in the ability to predict failure by the ISIS score. Loppini et al. reported failure rates after an arthroscopic Bankart repair of 7% with ISIS scores <3, 14% with an ISIS of 4–6 (hazard ratio 2), and 45% when the ISIS>6 (hazard ratio 9) [15]. Accordingly, Thomazeau et al. published a recurrent rate after an isolated Bankart repair of 10% with an ISIS of <2 and of 35.6% when the ISIS was 3–4 [16]. On the other hand, other authors like Ruiz-Iban et al. found that an ISIS <7 was not predictive of failure, showing recurrence rates of 12.8% with an ISIS <3, 20% with an ISIS of 4–6, the difference not being significant [17, 18].
In 2014, Bouliane et al. evaluated if the ISIS and the WOSI scores could detect patients at risk of failure after an arthroscopic Bankart repair [19]. The authors registered the preoperative ISIS and WOSI scores of 110 patients (87 men, 79%) that underwent an arthroscopic Bankart repair for recurrent anterior glenohumeral instability. The mean age at the time of the intervention was 25.1 years (range 16–61). Patients were telephonically interviewed after 2 years of follow-up to determine if the patients had suffered a recurrent dislocation and to determine the rate of return to sport to preinjury levels. Six patients (5%) have an ISIS >6. One hundred patients (91% of the study population) were available for the interview. Six patients (6%) had a recurrent dislocation, and 28 (28%) did not go back to preinjury sports participation. No patient with dislocation had an ISIS >6. There were no differences in the mean WOSI scores of patients suffering a dislocation and those that did not. However, the ISIS was not associated to a return to preinjury activity [19].
In 2016, Aboalata et al. researched the long-term results of arthroscopic Bankart repair and the risk factors for failure in young patients [10]. They tested the hypotheses that the results of such intervention would be comparable to results of open repair published in the literature. They designed a level 4 evidence (case series) in 180 patients undergoing an arthroscopic Bankart procedure for recurrent instability that were followed-up for a minimum of 10 years (Fig. 4.1). Of those patients, 143 accepted the participation in this study. One hundred four patients where clinically evaluated using the ASES score, the Constant score, the AAOS score, the Rowe score, and the Dawson 12-pont questionnaire. The Samilson-Prieto classification was used to assess for arthropathy changes in the available radiographs of 100 patients. Additionally, 14 patients were assessed using a specific questionnaire and 24 patients after a telephone interview.

Arthroscopic view of Bankart repair. A view of a Bankart repair performed with suture anchors and a mattress configuration repair is observed. The view is from the posterior portal of a right shoulder in the lateral decubitus position
The global rate of redislocation was 18.18%. The rates of redislocation were different according for the different types of fixation: FASTak/Bio-FASTak, 15.1% (17/112); SureTac, 26.3% (5/19); and Panalok, 33.3% (4/12). Concomitant superior labral anterior to posterior (SLAP) repair did not influence the clinical results. The rate of redislocation was significantly altered by the age of the patient and the duration of postoperative rehabilitation. The rate of redislocation also tended toward an increase in cases of more than one dislocation event prior to the intervention. A severe dislocation arthropathy was present in 12% of the shoulders, and these degenerative changes were positively associated with the number of preoperative dislocations, the age of the patients, and the number of anchors. The rate of patient satisfaction with the procedure was 92.3%, and the return to sports was 49.5%. The authors concluded that the long-term results of arthroscopic Bankart repair were comparable to the published results of open Bankart repair with the added benefit of being able to treat concomitant lesions. The authors suggested that stabilization after a first dislocation event produced better clinical and radiological results than waiting for successive shoulder dislocations prior to the operation [10].
Other than recurrent dislocation, other forms of failure have been reported. A specific form of failure after Bankart repair using impacted glenoid anchors is the fracture of the anterior glenoid rim. In 2014, Park et al. reported the incidence of postoperative anterior glenoid rim fractures and the relationship of this fracture with the presence of osteolysis around the implants, the pattern of fracture, the number of anchors, and the amount of postoperative activity [20]. They reviewed the results of 570 patients undergoing an arthroscopic Bankart repair using anchors and found 9 patients, with at least 2-year follow-up, who required a revision for a glenoid rim fracture after a Bankart repair. The mean age of these patients was 28.8 years (range, 18–49) and a mean follow-up of 36.4 years. The mean time between the fracture and the index procedure was 27.3 months. The suture anchors used at the index operation were resorbable (poly-d-Lactic acid, PDLLA) without ceramic osteo-filler (seven cases) or metal (two cases). For revision surgery, PDLLA without ceramic osteo-filler suture anchors were used. Five patients including three and two with bioabsorbable and metal suture anchors, respectively, experienced glenoid rim fracture at more than 2 years postoperatively. Patients showing osteolysis around the initial suture anchor groups showed a higher incidence of glenoid rim fractures compared with the control group. The authors suggested that osteolysis around the anchors may predispose to a glenoid rim fracture, and the use of metal or bioabsorbable suture anchors without ceramic composite implants could be a stress riser at 2 years postoperatively [20].
The rate of recurrent instability may be unacceptable, more so in the event of associated lesions like humeral bone loss, glenoid bone loss, bad quality tissue, or very active young patients. To control some of these risk factors, associated techniques augmenting an arthroscopic Bankart repair have been developed. After elaboration of the ISIS score, Boileau has suggested the use of associated augmentation techniques after a Bankart repair and has suggested the use of an associated Trillat procedure in the presence of isolated hyperlaxity without significant bone loss, an associated remplissage in the presence of an isolated large Hill-Sachs, and an associated Bristow-Latarjet procedure in the presence of a glenoid or combined bone loss [21].
In 2016, Cho et al. compared in a case-control design study (level III evidence) the results of isolated arthroscopic Bankart repair with and without posterior capsulodesis for anterior shoulder instability with engaging Hill-Sachs lesions [22]. Thirty-five shoulders that underwent an isolated Bankart repair were prospectively evaluated and compared to another group of patients with a Bankart repair plus a remplissage (Fig. 4.2). The mean age at the time of surgery was 26.1 and 24.8 years for Bankart and Bankart + remplissage groups, respectively. Both Rowe and UCLA scores improved in both groups. The mean loss of external rotation was 3° and 8° for Bankart and Bankart + Remplissage groups, respectively. There was no loss of strength in any of the patients. The recurrence rate was 25.5% for the Bankart group and 5.4% in the Remplissage group. In conclusion, the addition of a posterior capsulodesis obtained good clinical results with a low recurrence rate at the expense of a minimal loss of external rotation without any loss of strength [22].

Arthroscopic view of a remplissage repair in a right shoulder positioned in the lateral decubitus. The view is from the anterosuperior portal. A Hill-Sachs injury is viewed from the anterosuperior portal, and a remplissage procedure is being performed via use of suture anchors (a). After securing the knots on top of the infraspinatus, the capsulodesis effect is observed (b). This type of repair will prevent engagement of the Hill-Sachs injury
According to Camus et al., an arthroscopic remplissage in the presence of a Hill-Sachs lesion is one of the surgical options for the treatment of chronic anterior shoulder instability [23]. These authors performed a literature review comparing the results of isolated Bankart and Bankart with remplissage for patients with shoulder instability and an engaging Hill-Sachs lesion. Their hypothesis was that Bankart + remplissage patients would obtain superior results when compared to an isolated Bankart repair. They performed a meta-analysis of the literature (level III evidence). They identified three comparative studies including 146 patients, 74 of whom underwent an isolated Bankart repair and 72 underwent a Bankart repair with remplissage procedure. The authors found a significant risk of recurrent instability and dislocation after an isolated Bankart repair without differences in the rate of reoperation or the time of return to sport. Both Rowe and UCLA scores were inferior in the isolated Bankart repair group, and the authors concluded that the addition of a remplissage procedure in the presence of an engaging Hill-Sachs lesion and glenoid bone loss of less than 25% was superior with regard to redislocation rate, recurrent instability, or functional scores [23].
In 2018, Lee et al. performed a retrospective case-control study (level III evidence) trying to identify risk factors for instability after an arthroscopic Bankart repair [24]. They performed a retrospective review of patients with anteroinferior shoulder instability that underwent a Bankart repair. Patients under 30 years with a minimum follow-up of 2 years were divided in two groups according to the presence of recurrent instability. An assessment of risk factors was performed using binary logistic regression analysis. Functional results were assessed by Row and Walch-Duplay scores. One hundred seventy shoulders (138 without recurrence, 32 with recurrent instability, 18.8% recurrent instability rate) were included. Both Rowe and Walch-Duplay scores were improved, although improvements were diminished in cases of recurrence. A high number of preoperative dislocations, an off-track Hill-Sachs lesion, and surgery after 6 months of the first episode showed a higher risk of recurrence [24].
In 2019, Brilakis et al. evaluated the long-term results of remplissage in addition to a an arthroscopic Bankart repair in cases of recurrent anterior shoulder instability with engaging Hill-Sachs without a critical glenoid bone defect in a level IV therapeutic case study [25]. Sixty-five patients with 30.1 years underwent the operation, and 51 (82%) were available for long-term evaluation (mean 8.1 years). Three patients suffered a new dislocation (5.6%). The rest of the patients were satisfied with the result of the operation, and 71% were able to practice sports without restriction. The mean ASES score improved from 72.5 points to 100 after surgery. Mean Rowe score improved from 40 to 100, and mean Oxford Shoulder Instability Score improved from 29 to 48 (48 being the best possible score). No significant ROM deficit was observed. The combination of arthroscopic remplissage with the classic Bankart repair was safe and effective for treating engaging Hill-Sachs lesions in patients without an inverted pear-shape glenoid (Fig. 4.3). The long-term results were good with a low rate if recurrence and no significant loss of eternal rotation [25].

Arthroscopic image of a glenoid with an inverted pear appearance. The scope is in the anterosuperior portal, and the Wissinger rod is being introduced from the posterior portal. Anteroinferior glenoid bone loss is observed. An inverted pear appearance usually represents a glenoid bone loss of approximately 25%
According to Iizawa et al., glenoid bone loss contributes to recurrent shoulder instability after an isolated arthroscopic Bankart repair. In the setting of significant glenoid bone loss, it seems that there is an increased failure rate. However, there is scarce data comparing augmentation using bone graft with non-augmentation for glenoid bone loss [26]. Iizawa et al. evaluated the clinical results of an arthroscopic Bankart repair with or without arthroscopic bone graft augmentation in a level 4 clinical evidence study. They tested the hypothesis that such bone graft augmentation techniques would restore shoulder stability and would produce excellent clinical results. Of the 552 patients treated for anterior glenohumeral instability with an arthroscopic Bankart repair, 68 patients met the inclusion criteria of presenting anterior glenoid bone loss greater than 20% and a minimum follow-up of 2 years. Patients were then divided into two groups depending on whether they had received bone graft augmentation or not (Fig. 4.4). There were 35 patients that received bone graft augmentation with a mean age of 21 years (group A) and 33 patients that did not receive bone augmentation with a mean age of 21 years (group B). For grafting, either autologous iliac bone or artificial bone made of hydroxyapatite was used (Fig. 4.4). Patients were evaluated with the rate of instability; the return to sport and the Rowe score were used. The mean Rowe score was 95 in group A and 69.7 on group B; the recurrence rate was 2.9% in group A and 48.5% in group B. Regarding collision athletes, 24 were in group A and 22 were in group B. Out of the patients with recurrence, 13 (59.1%) were contact athletes. Fifty percent of contact or collision athletes from both groups went back to practice their sport at the same preoperative level. Seven of the 11 patients in group B that went back to their preoperative sport suffered a recurrent dislocation. Nine athletes in group A and 3 in group B abandoned the sport for unrelated causes. In conclusion, in the presence of recurrent anterior instability of the shoulder with glenoid bone loss bone graft augmentation was beneficial when it was used in association with an arthroscopic Bankart repair, especially in athletes that practice collision sports [26].

Postoperative radiographs of a glenoid augmentation technique for instability using iliac crest bone graft fixed with a double suture-button technique. Anteroposterior (a) and lateral (b) views
4.3 Latarjet Procedure
Many authors have used anterior bone grafting technique, mostly Latarjet, to reconstruct anterior glenoid bone defects greater than 25% in what has been termed a critical defect with success. The presence of a combined Hill-Sachs injury has been shown to reduce the effective arc of motion of the shoulder free of instability and can influence the results of any technique, being a Bankart or a Latarjet procedure.
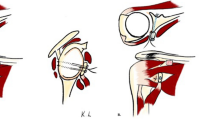
The initial concept of an engaging Hill-Sachs lesion was referred to as those lesions engaging with the arm at abduction and external rotation of 90° resembling a cocking phase of a throwing mechanism. It is obvious that all Hill-Sachs lesions were produced after a dislocation or subluxation event after engaging with the anterior glenoid rim, but after reduction the location of the Hill-Sachs lesion will influence the risk of dislocation. Medial Hill-Sachs injury will engage earlier than lateral Hill-Sachs lesions as they will reduce more the effective arc of motion of the shoulder. This evolution of concept was termed the glenoid track, resembling the track of motion the humeral head prints on the anterior glenoid as it is placed in a cocking position, and it is obviously affected by both the glenoid width and the location of the Hill-Sachs injury. As such, Hill-Sachs injuries are now classified as being on-track when they do not engage and off-track when they engage into the anterior glenoid rim. As such, some investigators will measure the glenoid track (the distance after calculating 83% of the native glenoid and subtracting the current glenoid defect), the Hill Sachs interval which is the distance from the insertion of the rotator cuff to the medial border of the Hill Sachs. If the HSI > GT, the lesion is considered as being off-track and has a greater risk of incurring into engagement during activities with external rotation of the shoulder. If the HSI < GT, the lesion is on-track (Fig. 4.5).

The glenoid track concept can be calculated using a CT scan or, alternatively, in an appropriately performed MR scan. Typically, the width of the glenoid would be calculated on an “en face” view of the shoulder (in this case an axial cut) (a), and the Hill-Sachs interval (HIS) is calculated on an axial view (b). The glenoid has a 24% defect and a 20 mm diameter that multiplied by 83% gives a glenoid track of 15.7 mm. The HIS is 19 mm. Since the HIS is greater than the GT, this is considered an off-track Hill-Sachs injury
Some authors have used this preoperative tool to assess the risk of recurrence and, even in the presence of anterior glenoid bone defects <25%, will use an anterior bone augmentation in cases with an off-track Hill-Sachs injury to alter the relation of the glenoid track and the Hill-Sachs interval to make this an on-track injury (Fig. 4.6).

An arthroscopic view from the anterosuperior portal of an arthroscopic Latarjet procedure using the classic arthroscopic techniques fixed with 2 screws
This concept has been clinically validated by Shaha et al. [27]. They studied 57 shoulders treated with an isolated, primary arthroscopic Bankart reconstruction with a mean patient age of 25.5 years, and a mean follow-up was of 48.3 months. Preoperative magnetic resonance imaging was used to determine glenoid bone loss and Hill-Sachs lesion size and location and to measure the glenoid track to classify the shoulders as on-track or off-track. They reported 10 recurrences (18%). Of the 49 on-track patients, 4 (8%) had treatment that failed compared with 6 (75%) of 8 off-track patients (p = 0.0001). Six (60%) of 10 patients with recurrence of instability were off-track compared with 2 (4%) of 47 patients in the stable group (p = 0.0001). The positive predictive value of an off-track measurement was 75% compared with 44% for the predictive value of glenoid bone loss of >20% highlighting the importance of the Hill-Sachs lesion, the interplay of the humeral and glenoid defect at some point of the arc of motion, and the ability to predict the risk of recurrence [27].
This concept highlights the importance of appropriately sizing of the anterior bone defect in the presence of critical glenoid bone defects in the presence of medial Hill-Sachs lesions (large HSI). Latarjet may only correct for certain combined defects and can be prone to failure in cases of smaller coracoids or very medial Hill-Sachs injuries. In these cases, the use of larger glenoid bone grafts or the association of a remplissage procedure must be pondered and points out that preoperative assessment of the coracoid dimensions will now have a role in the preoperative assessment and decision-making of the unstable shoulder with combined bone defects.
Calvo et al. in a level-IV evidence case-control study reported in the rates of recurrent instability according to the glenoid track concept using the arthroscopic classic Latarjet procedure [28]. A postoperative computed tomography scan and a clinical evaluation, including the Rowe and Western Ontario Shoulder Instability scores, were performed at a minimum 1- and 2-year follow-up, respectively. Postoperatively, 2 groups of patients were obtained: (1) patients with postoperative persistent off-track Hill-Sachs lesions and (2) patients with postoperative on-track Hill-Sachs lesions. Clinical and imaging data were compared between the 2 groups. A total of 51 patients (n = 51 shoulders), with a mean age of 29.8 ± 8.4 years (range, 15–50 years), met the inclusion criteria. Six shoulders (11.8%) still showed off-track Hill-Sachs lesions despite Latarjet surgery. There were no postoperative dislocations, but three patients reported subluxations. The subluxation rate was significantly higher in the postoperative persistent off-track Hill-Sachs lesions (2 [33%] vs 1 [2.2%]; P = 0.033). There was a wider preoperative HSI (29.8 ± 2.4 mm vs. 22.9 ± 3.5 mm; P < 0.001) and a larger preoperative ΔHSI-GT (12.2 ± 3.8 mm vs 4.82 ± 3.2 mm; P < 0.001) in the persistent off-track Hill-Sachs lesions. A receiver operating characteristic curve was performed based on preoperative ΔHSI-GT values. A preoperative ΔHSI-GT value ≥7.45 mm predicted a persistent off-track Hill-Sachs lesions after Latarjet surgery (sensitivity, 100%; specificity, 87%; positive predictive value, 50%; and negative predictive value, 100%). Six patients (11.8%) retained an OFF-HS and had a statistically significantly higher failure rate after Latarjet surgery compared with those with postoperative on-track Hill-Sachs lesions [28].
4.3.1 Modified Open Latarjet
According to Yang et al., recurrent anterior shoulder dislocation in the setting of an engaging Hill-Sachs lesion is frequent. The Latarjet procedure has been well described to restore shoulder stability in patients with glenoid bone loss >25%. However, the treatment of those patients with a combined humoral head and mild glenoid bone loss (<25%) is yet not clear [29]. A level-III cohort study assessed the results of the modified Latarjet procedure for patients with combined defects of the humeral head and anterior glenoid. They also compared the results of patients with <25% of glenoid bone loss with those having >25% glenoid bone loss (Fig. 4.5). The hypothesis was that both groups would have similar recurrence rates and subjective results. A modified Latarjet procedure was performed in 40 patients with recurrent anterior shoulder instability. An engaging Hill-Sachs by arthroscopic examination was confirmed, and glenoid bone loss <25% formed group A. A second group of 12 patients with glenoid bone loss >25% and an engaging Hill-Sachs lesion formed Group B. At a mean follow-up of 3.5 years, patients were evaluated with the Instability Severity Index Score (ISIS), the Beighton score, and the use of 3D imaging to assess bone loss (Fig. 4.7). To assess postoperative results, the authors used the Single Assessment Numeric Evaluation (SANE), Western Ontario Shoulder Instability Index (WOSI), recurrence rate, radiographs, ROM, and dynamometer strength. The main glenoid bone loss was 15% in Group A and 34% in Group B. Both groups had comparable WOSI scores (356 vs. 475). The SANE score was better in Group A (86 versus 77), and Group B suffered a greater loss of external rotation (9.2° versus 15.8°) and weaker thumbs-down abduction and external rotation strength. Strength in abduction and external rotation and subscapularis achieved at least 75% of the contralateral shoulder. Graft resorption was similar in both groups (32% versus 33%). The global rate of recurrent instability for the study defined as any subluxation or dislocation was 15%, the rates being similar for both groups (15% versus 17%). The rate of complications was 25% for both groups. The modified Latarjet procedure produced satisfactory results in patients with combined bone loss that usually suffered greater recurrence rates after traditional arthroscopic stabilization procedures. Previous surgical attempts and a higher Beighton score negatively influenced the results after a modified Latarjet. Additionally, it was observed that a higher number of surgical stabilization procedures and a higher Beighton score could predict the WOSI score [29].

Glenoid defects are best studied using 3d-CT reconstructions in the “en face” view. Two examples can be observed: a patient with a critical glenoid bone defect <25% (a) and a patient with a subcritical bone defect (b)
4.3.2 Arthroscopic Latarjet
In 2014, Dumont et al. described the results of the arthroscopic Latarjet technique combining the benefits of arthroscopic surgery with the low rate of recurrent instability associated with the procedure (Fig. 4.7). Additionally, up to that date, only short-term results of arthroscopic Latarjet had been published. They described the results of a series of cases (level-IV evidence) to evaluate the results after a minimum follow-up of 5 years after an arthroscopic Latarjet technique using two screws for fixation. Patients reported if they had suffered a dislocation or a subluxation or a new surgery, and they completed the WOSI score. A total of 62 of 87 patients were contacted for evaluation at a mean follow-up of 76.4 months. No patient suffered a new dislocation after surgery, and one patient reported subluxations after surgery for a total rate of 1.59% of recurrent instability with a mean WOSI score of 90.6% [30].
4.3.3 Open Latarjet Vs. Arthroscopic Latarjet
In 2017, Kordasiewicz et al. compared the short-term clinical results of open and arthroscopic Latarjet in patients with anterior shoulder instability. They tested the hypothesis that the arthroscopic technique would be comparable to the open technique. In a Level- III evidence study, they analyzed the clinical results of patients operated with the Latarjet technique [31]. Consecutive patients operated between 2006 and 2011 comprised the open group and patient operated after 2011 comprised the arthroscopic group. They were able to evaluate 48 out of 55 (87%) shoulders in the open group and 62 of 64 (97%) shoulders in the arthroscopic group. Patients’ results were evaluated using the Walch-Duplay score, the Rowe score, and a self-reported subjective score on satisfaction and function of the shoulder. CT scan evaluation was used to assess graft healing. The surgical time was 10 min less in the arthroscopic group (110 min versus 120 min). The number of intraoperative complications was six in the open group and five in the arthroscopic group, and results were comparable in both groups without significant differences with a satisfaction rate of 96.8% in open and 91.9% in the arthroscopic group. The subjective shoulder function score was 92.2% in open and 90% in arthroscopic group, the Rowe score was 87.8 in the open 78.9 in the arthroscopic group, the Walch-Duplay score was 83.9 and 91.9% in the arthroscopic group, and the presence of subjective apprehension was 28.7% in the open group and 50% in the arthroscopic group. The range of motion was similar in both groups with external rotation with the arm at the side being greater in the arthroscopic group (14° versus 7°). Three cases of recurrent instability were reported in the open group for a rate of 6.2% and 4.8% in the arthroscopic group. Revision surgery was performed in four patients in the open group and six in the arthroscope group. The radiographic evaluation showed significant less problems of bone healing after arthroscopic surgery (5%). However, partial osteolysis of the proximal part of the bone block was significantly more frequent using the arthroscopic technique. The authors concluded that arthroscopic stabilization showed satisfactory results and were comparable to the open procedure [31].
A recent meta-analysis by Hurley et al. reported the results of shoulder anterior instability with significant glenoid bone loss [32]. Even though open Latarjet is the standard treatment, the use of arthroscopic techniques is increasing, and the authors underwent this investigation to provide insight as to which technique gave better results.
They included six studies with 896 patients with a similar recurrent instability rate (2% vs 2.4%, open versus arthroscopic, respectively), revision procedures (2.4 vs. 5.4%), and total rate of complications (13.8 vs. 11.9%). However, the open procedure had a lower rate of persistent apprehension (10.2% vs. 35.7%). After achieving the learning curve, the operative time was similar for both procedures. Although technically difficult, the arthroscopic technique proved to be a valuable and safe alternative at the cost of a steep learning curve. The authors suggested that only centers with a greater caseload and expert arthroscopists should perform the arthroscopic technique (Fig. 4.8) [32].

One-year follow-up computer tomography (CT) scan after an arthroscopic Latarjet. Partial graft resorption following Wolff law is observed. As this case was fixed using a FiberTape cerclage fixation system, no problem with implant protrusion or hardware problems are observed
4.3.4 Latarjet vs. Anterior Glenoid Reconstruction Using Fresh Distal Tibia Allograft (DTA)
Early results of fresh distal tibial allograft (DTA) reported by Frank et al. suggested encouraging early results for the treatment of recurrent shoulder instability but lacked a comparison with the Latarjet procedure. The authors performed a cohort study (level III evidence) in which they compared the clinical results of patients undergoing DTA or Latarjet. They reviewed patients with a minimum glenoid bone loss greater than 15% that underwent either a DTA or Latarjet procedure after a minimal follow-up of 2 year [33]. Patients undergoing DTA were matched 1:1 with the Latarjet procedure with regard to age, BMI, contact sports, and previous number of operations. Patients were evaluated before and after the operation with a clinical exam and SST, VAS, ASES score, WOSI score, and SANE score. They analyzed the complications, the reoperations, and the number of episodes of recurrent instability. They reviewed 100 patients (50 Latarjet and 50 DTA) with a mean age of 25.6 years and a mean follow-up of 45 months. Thirty-two patients (64%) in each group had had a previous operation of the shoulder. Patients undergoing a DSA had a significantly greater bone loss than patients undergoing the Latarjet procedure (28.6% vs. 22.4%). Patients in both groups experienced significant improvements for all scores after surgery. No differences were found in VAS (0.67 vs. 1.83), ASES (91.06 vs. 89.74), Western Ontario Shoulder Instability Index (74.30 vs. 89.69), or Single Assessment Numeric Evaluation (80.68 vs. 90.08). However, Latarjet patients had a higher SSV score. Ten complications were reported, 5 for each group with 3 reinterventions in each group, for a total recurrent instability rate of 1%. Fresh DTA reconstruction was effective in restoring clinical stability in recurrent shoulder instability, but longer-term follow-up is required to test if these results are maintained over time [33].
4.3.5 Latarjet After Failed Arthroscopic Bankart Repair
Given that the complication profile is different between a Bankart repair and a Latarjet procedure, some surgeons make the decision of performing a primary Bankart repair and will leave Latarjet as a bailout surgery in case of recurrent instability after a failed Bankart repair. Werthel et al. tried to determine if the outcome of primary Latarjet and secondary Latarjet after a failed primary arthroscopic Bankart repair was equivalent [34]. They developed a level III cohort study in which the authors reviewed two cohorts of patients: primary Latarjet versus secondary Latarjet after a failed primary Bankart repair in a multicentric study. They analyzed the rate of recurrent instability, reoperation rate, the complications, the pain, the Walch-Duplay score, and the SST. Three hundred and eight patients participated in the study. Seventy-two patients (23.4%) did not answer and were considered lost to follow-up, so 236 patients were available for analysis. The mean follow-up was 3.4 years, and there were 20 patients in group 1 and 216 patients in group 2. Recurrent instability was similar for both groups (5% in group 1 versus 2.3% in group 2) and revision surgery (0% in group 1 and 2.3% in group 2). Group 1 patients had significant worse pain results (2.56 vs. 1.2) and patient-reported outcomes (Walch-Duplay 52 vs. 72.2 and SST 9.3 vs 10.7) than patients undergoing a primary Latarjet technique. The authors stated that the assumption that a failed Bankart repair could be revised to a Latarjet procedure with a similar result is incorrect and highlighted the importance of performing the right intervention at the right time [34].
4.4 Comparative Studies: Bankart Vs. Latarjet
4.4.1 Arthroscopic Bankart vs. Open Bristow-Latarjet
In 2014, Zarezade et al. compared an arthroscopic Bankart procedure and an open Latarjet procedure [1]. Patients were evaluated after surgery using Rowe, UCLA, and Constant scores. Six patients (16.22%) had a Rowe score of less than 75 points: one having undergone a Latarjet procedure and five undergoing a Bankart repair (5.26 vs. 27.78). Nine patients (24.32%) showed a moderate improvement, six Latarjet and three Bankart surgeries. Twenty-two patients showed a great improvement in the Rowe score, including 12 Latarjet and 10 Bankart (63.16 vs. 55.56). Both techniques were similar although some of the variables like the level of performance, the pain level, the use of analgesia, and the range of internal rotation were improved with the Latarjet technique. The authors concluded that the Latarjet was the preferable technique if there was no contraindication for its use [1].
An et al. performed a systematic review and meta-analysis to compare the results of a Bankart repair against the Latarjet technique [35]. They identified eight studies with 795 shoulders: 416 undergoing an open or arthroscopic Bankart repair and 379 undergoing an open Latarjet. They included primary and revision surgeries. The authors reported that the Latarjet procedure was associated with a significant decreased rate of recurrent instability and redislocation without significant differences in the rate of complications between both techniques. The Latarjet procedure showed a higher Rowe score and had decreased loss of external rotation and concluded it was viable alternative, and probably superior to a Bankart repair due to its increased restoration of stability without an increase in the rate of complications [35].
In 2018, Jeon et al. compared in a cohort study (level-III evidence) the clinical result and recurrence rate between a Bankart repair and a Latarjet procedure in patients with a subcritical glenoid bone defect (glenoid bone loss between 15 and 20%) [9]. They reviewed 149 patients (118 Bankart and 31 Latarjet) with a mean follow-up of 28.9 months and a mean age at the time of the index operation of 28.9 years. Rowe and UCLA scores improved from 42 and 22. 9 preoperatively to 90 and 32.5 postoperatively in the Bankart group and from 31 and 22.3 points to 91.1 and 32.3 in the Latarjet group, respectively. In the final evaluation, no differences were found between groups in Rowe or UCLA scores. The mean loss of motion in flexion, external rotation in abduction, and internal rotation was 3°, 11.6°, and 0.6 of vertebral bodies in the Bankart group and 3.7°, 10.3°, and 0.9 spinal segments in the Latarjet group, respectively. However, the loss of external rotation was greater in the Bankart group when compared with the Latarjet group (13.3° vs. 7.3°), and the recurrence rate was lower in the Bankart group when compared to the Latarjet group (22.9% vs. 6.5%). Both techniques showed improved clinical results and pain relief in patients with a borderline glenoid bone loss. However, the Latarjet procedure showed fewer recurrences (6.5% vs. 22.9%) and less decrease of external rotation (7.3° vs. 13.3°), and the authors stated that Latarjet could be a more reliable operation in patients with a borderline glenoid bone defect [9].
4.4.2 Arthroscopic Bankart vs. Open Bristow-Latarjet in Patients Older than 40
In 2020, Ernstbrunner et al. analyzed in a level-III evidence cohort study comparing the long-term results of an arthroscopic Bankart repair and the Latarjet technique in patients older than 40 [11]. They reported the results on 35 patients (36 shoulders) with a mean age at the time of the operation of 47 years and a mean follow-up of 13.2 years. The clinical and radiographic results were compared with those of a prior study including 39 patients (40 shoulders) of a similar age that had been treated using an open Latarjet technique. Six shoulders (17%) suffered a recurrent dislocation at a mean of 5.3 years after the index operation, and three additional shoulders suffered subluxation (8%), and three more experience persistent apprehension (8%). Revision surgery was performed in 8 patients (22%), consisting of 2 Bankart surgeries and 6 open Latarjet procedures. The relative Constant score and the SSV increased at final follow-up. Stabilization arthropathy was advanced in 16 shoulders (47%) and had progressed by at least 2 grades in 21 patients (62%). In the Bankart group, there were higher rates of redislocation and subluxation than in the open Latarjet (9 versus 3); also, the mean final SSV was significantly decreased in the Bankart group (86% versus 91%). There were no significant differences in between the two groups in the final rates of advanced arthropathy (16 versus 14) and revision (8 versus 7). This study shows that Latarjet is a more reliable operation regarding restoration of stability when compared to an arthroscopic Bankart repair. It is noteworthy to point out that the rates of arthropathy are not different in this age group as some surgeons have the initial thought that Latarjet may be more prone to arthropathy than the Bankart procedure [11].
4.4.3 Arthroscopic Bankart Repair with Remplissage vs. Open Latarjet
In 2018, Bah et al. compared short-term shoulder stability after an arthroscopic Bankart with remplissage and open Latarjet in patients with recurrent instability with a large Hill-Sachs lesion with the hypothesis that the recurrence rate would be higher after the Bankart-remplissage procedure [36]. They performed a retrospective comparative study in two hospitals recruiting patients with chronic anterior instability with a large Hill-Sachs defect in a Level-II evidence study comparing 43 patients treated with an arthroscopic Bankart repair and remplissage with 53 patients treated with an open Latarjet technique. Both groups were similar in age at the time of surgery and length of follow-up. All patients were evaluated by independent observers in which they assessed the number of recurrences, the range of motion, and functional scores including the subjective shoulder value (SSV), the Walch-Duplay score, and the Rowe score. The mean time to follow up was 47.3 months. The rate of recurrence at last follow-up was not significantly different between both groups (9.3% vs. 11.2%). The Bankart group showed higher loss of external rotation, and a higher proportion of patients had residual pain (21% vs. 9%). The SSV, the Walch-Duplay, and Rowe scores were similar for both groups. This study highlights that augmentation of a Bankart procedure will reduce the short-term radiolocation rate of an arthroscopic procedure and will perform similarly to a Latarjet procedure. It remains to be seen if the long-term results will reproduce this initial data. However, loss of external rotation and residual pain were significantly higher with the Bankart and remplissage technique, and patients should be counseled in this regard [36].
4.4.4 Arthroscopic Bankart Repair vs. Open Latarjet vs. Capsular Shift
In a level-III therapeutic study published by Xu et al. in 2019, the authors explored the hypothesis that the result of open traditional techniques and modern arthroscopic techniques would be similar [12]. They retrospectively analyzed 168 patients with recurrent anterior shoulder instability with a mean age of 30.8 years in which they compared three techniques: a Bankart arthroscopic repair in 33 men and 20 women, an open Latarjet in 34 men and 18 women, and a capsular shift in 31 men 14 women. They analyzed the ISIS, the Rowe score and the SSV at the mean follow-up of 67.6 months.
The preoperative ISIS score was higher than three, with a mean preoperative score of 6.4 points. All three techniques were effective in improving the function of the shoulder and reducing symptoms although the Latarjet was the best with regard to subjective perception of the shoulder. The Rowe scores were 92.3, 96.2, and 93.2 for arthroscopic Bankart, open Latarjet, and capsular shift, respectively. There were no differences with regard to functional scores; however, the Latarjet group was superior to the other groups in SSV and subjective shoulder value for sports (SSV sports) practice. There were two recurrences in both the Bankert group and capsular shift group and no recurrences in the open Latarjet group. The authors concluded that the latter was the most effective technique in reducing recurrences and achieved higher stability although all surgeries increased the preoperative function and improved pain [12].
4.5 Conclusions
A systematic review has shown that open Latarjet is better than open Bankart achieving less recurrences with a similar rate of complications. In another study, patients operated with the Latarjet technique showed less recurrences and higher Rowe scores when compared with an arthroscopic Bankart repair. One publication supported better results for return to sport and subjective perception of the shoulder in patients undergoing an arthroscopic Bankart repair.
In the presence of a critical bone defect, most authors support the use of some bony reconstruction, mostly Latarjet. In a study comparing borderline glenoid bone defects (15–20%) and glenoid bone loss, both techniques were effective in reducing pain and clinical symptoms, but the Latarjet showed less recurrences and less loss of external rotation than arthroscopic Bankart. It is yet to be cleared if that benefit is maintained in glenoid bone loss <15%.
In patients older than 40 years, both Bankart and Latarjet have been effective, but Latarjet achieves less recurrences, and the degree of shoulder arthropathy was not decreased using an arthroscopic Bankart repair.
In patients with recurrent anterior shoulder instability and a significant Hill-Sachs lesion, both an arthroscopic Bankart repair with remplissage and open Latarjet are safe and effective with similar recurrent rates, but loss of external rotation and residual pain were more frequent with the Bankart and remplissage group.
Another study compared an arthroscopic Bankart against open Latarjet and open capsular shift and highlighted the benefits of each procedure but showed that Latarjet was most effective in reducing recurrence.
Additional long-term data is needed to assess the effectiveness of these techniques, and more comparative studies are warranted to tailor the best treatment for each patient. As highlighted in the introduction, listening to the patient’s wants and needs, performing a meticulous clinical exam, and having a candid discussion about the results and complications of the available techniques will generally produce a satisfactory result. Preoperative tools for assessing the risk of recurrence are available and may be helpful in guiding the clinical decision-making. Different augmentation techniques can be used to reduce the rate of recurrent dislocation.
References
Zarezade A, Dehghani M, Rozati AR, Banadaki HS, Shekarchizade N. Comparison of Bristow procedure and Bankart arthroscopic method as the treatment of recurrent shoulder instability. Adv Biomed Res. 2014;3:256.
Bokshan SL, Marcaccio SE, Lemme NJ, Owens BD. Open Bankart repair for anterior shoulder instability. Oper Tech Orthop. 2020;30:100822.
Blonna D, Bellato E, Caranzano F, Assom M, Rossi R, Castoldi F. Arthroscopic Bankart repair versus open Bristow-Latarjet for shoulder instability: a matched-pair multicenter study focused on return to sport. Am J Sports Med. 2016;44:3198–205.
Gao B, DeFroda S, Bokshan S, Ready LV, Sullivan K, Etzel C, Owens BD. Arthroscopic versus open Bankart repairs in recurrent anterior shoulder instability: a systematic review of the association between publication date and postoperative recurrent instability in systematic reviews. Arthroscopy. 2020;36:862–71.
Uchiyama Y, Handa A, Shimpuku E, Omi H, Hashimoto H, Imai T, Watanabe M. Open Bankart repair plus inferior capsular shift versus arthroscopic Bankart repair without augmentations for traumatic anterior shoulder instability: a prospective study. J Orthop Surg. 2017;25:1–8.
Pogorzelski J, Fritz EM, Horan MP, Katthagen JC, Provencher MT, Millett PJ. Failure following arthroscopic Bankart repair for traumatic anteroinferior instability of the shoulder: is a glenoid labral articular disruption (GLAD) lesion a risk factor for recurrent instability? J Shoulder Elb Surg. 2018;27:e235–42.
Bessiere C, Trojani C, Carles M, Mehta SS, Boileau P. The open Latarjet procedure is more reliable in terms of shoulder stability than arthroscopic Bankart repair. Clin Orthop Relat Res. 2014;472:2345–51.
Hachem AI, Costa DOG, Rondanelli SR, Rius X, Barco R. Latarjet cerclage: the metal-free fixation. Arthrosc Tech. 2020;9:e1397–408.
Jeon YS, Jeong HY, Lee DK, Rhee YG. Borderline glenoid bone defect in anterior shoulder instability: Latarjet procedure versus Bankart repair. Am J Sports Med. 2018;46:2170–6.
Aboalata M, Plath JE, Seppel G, Juretzko J, Vogt S, Imhoff AB. Results of arthroscopic Bankart repair for anterior-inferior shoulder instability at 13-year hollow-up. Am J Sports Med. 2016;45:782–7.
Ernstbrunner L, De Nard B, Olthof M, Beeler S, Bouaicha S, Gerber C, Wieser K. Long-term results of the arthroscopic Bankart repair for recurrent anterior shoulder instability in patients older than 40 years: a comparison with the open Latarjet procedure. Am J Sports Med. 2020;48:2090–6.
Xu Y, Wu K, Ma Q, Zhang L, Zhang Y, Xu W, Guo JJ. Comparison of clinical and patient-reported outcomes of three procedures for recurrent anterior shoulder instability: arthroscopic Bankart repair, capsular shift, and open Latarjet. J Orthop Surg Res. 2019;14:326.
Moroder P, Odorizzi M, Pizzinini S, Demetz E, Resch H, Moroder P. Open Bankart repair for the treatment of anterior shoulder instability without substantial osseous glenoid defects: results after a minimum follow-up of twenty years. J Bone Joint Surg Am. 2015;97:1398–405.
Balg F, Boileau P. The instability severity index score. A simple pre-operative score to select patients for arthroscopic or open shoulder stabilisation. J Bone Joint Surg Br. 2007;89:1470–7.
Loppini M, Delle Rose G, Borroni M, et al. Is the instability severity index score a valid tool for predicting failure afterprimary arthroscopic stabilization for anterior glenohumeral instability? Arthroscopy. 2019;35:361–6.
Thomazeau H, Courage O, Barth J, Pélégri C, Charousset C, Lespagnol F, Nourissat G, Audebert S, Guillo S, Toussaint B, Lafosse L, Bradel J, Veillard D, Boileau P. French arthroscopy society. Can we improve the indication for Bankart arthroscopic repair? A preliminary clinical study using the ISIS score. Orthop Traumatol Surg Res. 2010;96(8 Suppl):S77–83.
Ruiz Ibán MA, Asenjo Gismero CV, Moros Marco S, Ruiz Díaz R, Del Olmo HT, Del Monte BG, García Navlet M, Ávila Lafuente JL, Díaz HJ. Instability severity index score values below 7 do not predict recurrence after arthroscopic Bankart repair. Knee Surg Sports Traumatol Arthrosc. 2019;27:3905–11.
Dekker TJ, Peebles LA, Bernhardson AS, et al. Limited predictive value of the instability severity index score: evaluation of 217 consecutive cases of recurrent anterior shoulder instability. Arthroscopy. 2021;37:1381–91.
Bouliane M, Saliken D, Beaupre LA, Silveira A, Saraswat MK, Sheps DM. Evaluation of the instability severity index score and the Western Ontario shoulder instability index as predictors of failure following arthroscopic Bankart repair. Bone Joint J. 2014;96-B:1688–92.
Park J-Y, Lee S-J, Oh S-K, Oh KS, Noh YM, Suh K-T. Glenoid rim fracture through anchor points after arthroscopic Bankart repair for shoulder instability. Int Orthop (SICOT). 2015;39:241–8.
Boeileau P, Lemmex DB. Editorial commentary: which patients are likely to undergo redislocation after an arthroscopic Bankart repair? Preoperative instability severity index scoring over 3 points-the game is vver! Arthroscopy. 2019;35:367–71.
Cho NS, Yoo JH, Juh HS, Rhee YG. Anterior shoulder instability with engaging Hill–Sachs defects: a comparison of arthroscopic Bankart repair with and without posterior capsulodesis. Knee Surg Sports Traumatol Arthrosc 2016;24:3801-3808.
Camus D, Domos P, Berard E, Toulemonde J, Mansat P, Bonnevialle N. Isolated arthroscopic Bankart repair vs. Bankart repair with “remplissage” for anterior shoulder instability with engaging hill-Sachs lesion: a meta-analysis. Orthop Traumatol Surg Res. 2018;104:803–9.
Lee SH, Lim KH, Kim JW. Risk factors for recurrence of anterior-inferior instability of the shoulder after arthroscopic Bankart repair in patients younger than 30 years. Arthroscopy. 2018;34:2530–6.
Brilakis E, Avramidis G, Malahias MA, Stathellis A, Deligeorgis A, Chiotis I, Mataragas E, Chronopoulos E, Antonogiannakis E. Long-term outcome of arthroscopic remplissage in addition to the classic Bankart repair for the management of recurrent anterior shoulder instability with engaging Hill–Sachs lesions. Knee Surg Sports Traumatol Arthrosc. 2019;27:305–13.
Iizawa N, Yoneda M, Yamada S, Mizuno N, Goto K, Iwashita S, Mae T, Hashiguchi H, Takai S. Benefits of bone graft augmentation to arthroscopic Bankart repair for recurrent anterior shoulder instability with glenoid bone loss. Knee Surg Sports Traumatol Arthrosc. 2020;28:2325–33.
Shaha JS, Cook JB, Rowles DJ, Bottoni CR, Shaha SH, Tokish JM. Clinical validation of the glenoid track concept in anterior glenohumeral instability. J Bone Joint Surg Am. 2016;98:1918–23.
Calvo E, Luengo G, Morcillo D, Foruria AM, Valencia M. Revision arthroscopic Bankart repair versus arthroscopic Latarjet for failed primary arthroscopic stabilization with subcritical bone loss. Orthop J Sports Med. 2021;9:23259671211001809.
Yang JS, Mazzocca AD, Cote MP, Edgar CM, Arciero RA. Recurrent anterior shoulder instability with combined bone loss: treatment and results with the modified Latarjet procedure. Am J Sports Med. 2016;44:922–32.
Dumont GD, Fogerty S, Rosso C, Lafosse L. The arthroscopic Latarjet procedure for anterior shoulder instability: 5-year minimum follow-up. Am J Sports Med. 2014;42:2560–6.
Kordasiewicz B, Małachowski K, Kicinski M, Chaberek S, Pomianowski S. Comparative study of open and arthroscopic coracoid transfer for shoulder anterior instability (Latarjet)—clinical results at short term follow-up. Int Orthop (SICOT). 2017;41:1023–33.
Hurley ET, Fat DL, Farrington SK, Mullet H. Open versus arthroscopic Latarjet procedure for anterior shoulder instability: a systematic review and meta-analysis. Am J Sports Med. 2019;47:1248–53.
Frank RM, Romeo AA, Richardson C, Sumner S, Verma NN, Cole BJ, Nicholson GP, Provencher MT. Outcomes of Latarjet versus distal tibia allograft for anterior shoulder instability repair: a matched cohort analysis. Am J Sports Med. 2018;46:1030–8.
Werthel J-D, Sabatier V, Schoch B, Amsallem L, Vigan M, Hardy A. Outcomes of the Latarjet procedure for the treatment of chronic anterior shoulder instability: patients with prior arthroscopic Bankart repair versus primary cases. Am J Sports Med. 2020;48:27–32.
An VVG, Sivakumar BS, Phan K, Trantalis J. A systematic review and meta-analysis of clinical and patient-reported outcomes following two procedures for recurrent traumatic anterior instability of the shoulder: Latarjet procedure vs. Bankart repair. J Shoulder Elbow Surg. 2016;25:853–63.
Bah A, Lateur GM, Kouevidjin BT, Bassinga JYS, Issa M, Jaafar A, Beaudouin E. Chronic anterior shoulder instability with significant Hill–Sachs lesion: Arthroscopic Bankart with remplissage versus open Latarjet procedure. Orthop Traumatol Surg Res. 2018;104:17–22.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Appendix 1: WOSI Score
Appendix 1: WOSI Score
The WOSI score is a patient-reported outcome score using 21 items pertaining to 4 domains (physical symptoms, emotion, lifestyle and sports recreation, and work) with 0 being the best possible score (no instability related symptoms or limitations and 2100 being the worst possible score). Some authors will express it as a percentage. The WOSI score can be accessed in its English version in the following publication:
The Development and Evaluation of a Disease-Specific Quality of Life Measurement Tool for Shoulder Instability The Western Ontario Shoulder Instability Index (WOSI)Am J Sports Med November 1998 vol. 26 no. 6 764-772 Alexandra Kirkley, MD, FRCSC*, Sharon Griffin, CSS, Heidi McLintock, BSc, PT, MSc and, Linda Ng, BSc, PT.
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Barco, R., Rodríguez-Merchán, E.C. (2022). Recurrent Anterior Shoulder Instability in Adults: Bankart or Latarjet?. In: Rodríguez-Merchán, E.C., Moreno-Garcìa, A. (eds) Controversies in Orthopedic Surgery of The Upper Limb . Springer, Cham. https://doi.org/10.1007/978-3-031-04907-1_4
Download citation
DOI: https://doi.org/10.1007/978-3-031-04907-1_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-031-04906-4
Online ISBN: 978-3-031-04907-1
eBook Packages: MedicineMedicine (R0)