
Abstract
A wide range of bacterial, viral, fungal and parasitic infections can cause myelopathy. Some infections are endemic in certain geographical regions e.g. HTLV-1, West Nile virus and Lyme disease, and some infections are more frequent in certain populations e.g. spinal epidural abscess in patients with diabetes mellitus. Pathological mechanisms resulting in myelopathy include direct spinal cord infection, para-infectious immune-mediated myelitis, and spinal cord compression due to infection of surrounding structures. Clinical presentations of infectious myelopathies are diverse and range from acute flaccid paralysis, acute transverse myelitis, radiculomyelitis, to chronic progressive paraparesis. A careful history and examination in patients with a possible infectious myelopathy should include factors such as geographical region, travel history, prodromal symptoms, the temporal profile and nature of neurological deficits. Useful investigations include MRI, lumbar puncture, microbiological, serological and other laboratory studies tailored to suspected micro-organisms. Many infectious myelopathies are amenable to treatment with specific anti-microbials. Early diagnosis and treatment may improve outcome and reduce long-term disability in many cases. The clinical, diagnostic and management considerations for the most common and most important causes of infectious myelopathies are presented in this chapter.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Myelopathy
- Infectious myelopathy
- Transverse myelitis
- Radiculomyelitis
- Acute flaccid paralysis
- Viral myelopathy
- Spinal epidural abscess
- Bacterial myelopathy
- Fungal myelopathy
- Parasitic myelopathy
Introduction
Infections are an important cause of myelopathy globally. Causative organisms vary by population and region (Tables 8.1 and 8.2). Clinical presentations of infections affecting the spinal cord vary according to the micro-organism involved and the pathological process and can include acute flaccid myelitis, acute myelitis, radiculomyelitis and chronic progressive paraparesis. Certain populations are at increased risk of infectious myelopathies, such as immunocompromised patients. Establishing the correct diagnosis is essential in infectious myelopathies, as many of these diseases are amenable to treatment with specific anti-microbials. The clinical, diagnostic and management considerations for the most common and most important causes of micro-organism associated myelopathy will be presented in this chapter.
Viral Myelopathies
Retroviruses
HIV
Myelopathy in HIV can result from a number of underlying pathologic processes. The most common form is HIV-associated vacuolar myelopathy, named after the distinct histopathological features described below [1]. HIV-associated vacuolar myelopathy typically occurs in longstanding HIV infection with low CD4 cell counts or in the context of AIDS. However, it has been reported as an early or presenting feature of HIV on rare occasions [2]. Autopsy series in the pre-antiretroviral era demonstrated pathological changes of HIV-associated vacuolar myelopathy in 22% of spinal cords of AIDS-patients, some of whom did not have spinal cord symptoms, suggesting that the clinical syndrome is subtle or asymptomatic in some patients [1].
Early symptoms can include paresthesias, leg discomfort and erectile dysfunction [3, 4]. These are followed by progressive spastic paraparesis which is typically symmetric and may involve gait ataxia [3]. Bowel and bladder dysfunction with incontinence occurs in over half of patients [1]. Sensory deficits predominantly reflect dorsal column involvement with impaired vibration and proprioception [3]. The clinical syndrome may plateau after many years. A caveat in interpreting sensory findings and reflexes in HIV patients is the possibility of a co-existing HIV-associated peripheral neuropathy which has been reported in approximately 40% of patients with HIV [5].
HIV-associated vacuolar myelopathy is considered a clinical diagnosis and one of exclusion in HIV patients, as there are no specific diagnostic investigations other than pathological examination. MRI of the spinal cord is usually unremarkable, although high T2 signal in the posterior and lateral cord may be seen in some cases [6]. CSF analysis is often undertaken to rule out opportunistic infection which can occur in HIV and serological studies for HTLV should be sent, since co-infection with human T-cell lymphotropic virus-1 (HTLV-1) and HIV is associated with increased risk of myelopathy [7].
Anti-retroviral therapy is not thought to alter the natural history of HIV-associated vacuolar myelopathy in individuals [4], although the incidence of this syndrome in the HIV population has reduced since the introduction of highly active anti-retroviral therapy [8].
Characteristic pathological findings at autopsy are vacuolation of the white matter with infiltrate of lipid-laden macrophages, most prominent in the lateral and posterior regions of the mid to lower thoracic spinal cord [1]. As the pathological changes are very similar to those seen in subacute combined degeneration of the cord due to B12 deficiency, it has been suggested that metabolic pathways may be involved in the pathogenesis of this disorder [9]. However, the clinical syndrome does not respond to B12 supplementation [8].
Other causes of myelopathy related to HIV are also possible. Acute transverse myelitis has been reported as a complication of seroconversion and has been successfully treated with corticosteroids and anti-retroviral therapy [10]. Co-infection or opportunistic infection with mycobacterium tuberculosis, HTLV-1, cytomegalovirus, herpes simplex virus, varicella zoster virus, syphilis or cryptococcus neoformans should also be considered as causes of myelopathy, while epidural abscess from a variety of bacteria resulting in compressive myelopathy is also more frequent in HIV patients [4].
Human T-cell Lymphotropic Virus (HTLV)
HTLV is transmitted through exchange of bodily fluids, typically in the setting of sexual intercourse, blood product transfusions, or shared needles. HTLV-1 is endemic in South America, the Caribbean, Japan and western, central and southern Africa [11], while HTLV-2 is found in certain populations in the Americas, such as American Indians [4, 12]. HTLV-1 seropositivity in the United States is very rare, with the exception being intravenous drug users and commercial sex workers in whom sero-prevalence may be as high as 18% [13]. Of the two subtypes, HTLV-1 causes myelopathy much more frequently than HTLV-2, although cases have been reported in association with HTLV-2 [14].
Most individuals with HTLV-1 seropositivity are asymptomatic carriers, with less than 4% of infected persons developing ‘HTLV-associated myelopathy’ (HAM) or ‘tropical spastic paraparesis’ (TSP) [15, 16]. Risk of progression from carrier to symptomatic state is thought to be modified by proviral load, host HLA genotype and immune response [11]. Pathological findings seen in the spinal cord at autopsy are perivascular inflammatory infiltrates in the grey and white matter and hyaloid thickening of the media and adventitia of blood vessels, with demyelination and axonal degeneration of the anterior and lateral columns of the spinal cord, most marked in the thoracic region [17].
Clinical presentation is similar to that of HIV-associated myelopathy. Patients develop a slowly progressive myelopathy with prominent spasticity and early bladder dysfunction. Pain and sensory symptoms are less prominent but can occur [18]. Symptoms and signs are typically limited to the lower extremities which results in progressive gait disturbance, without remission or plateau. Patients may become wheelchair-bound around 20 years after symptom onset [11].
Laboratory testing for HTLV-1 antigen and antibody can be performed on both serum and CSF, with newer assays providing high sensitivity and specificity [19]. Proviral load can be tested in peripheral blood [11]. Routine CSF analysis may be normal [20] or may demonstrate mild non-specific abnormalities suggestive of inflammation i.e. mild lymphocytosis, elevated protein or positive oligoclonal bands [8]. MRI of the spinal cord may be normal or show atrophy, with a minority of patients demonstrating focal or diffuse spinal cord lesions [20,21,22]. It has been suggested that patients with HTLV-1 (both symptomatic and asymptomatic patients) may frequently have non-specific white matter lesions seen on MRI brain [20, 21].
Treatment with corticosteroids may be beneficial in the early inflammatory stage of the disease [11]. Various antivirals and immunomodulatory treatments such as interferon-alpha, cyclosporine A and diazole have also been reported to be of benefit in small numbers of patients [11, 23].
Herpesviruses
Herpesviruses are a family of DNA viruses with high prevalence worldwide. Herpes simplex virus (HSV), varicella zoster virus (VZV), Epstein-Barr virus (EBV) and cytomegalovirus (CMV) can cause a myelitis during primary infection or after remaining latent in sensory ganglia or the immune system for years.
Herpes Simplex Virus (HSV)
HSV-1 is a common infection transmitted via oral contact, while HSV-2 is typically transmitted during sexual contact with active genital lesions. HSV-2 can cause a myeloradiculitis of the lower spinal cord during primary infection or reactivation (Elsberg Syndrome), with symptoms of lower extremity weakness, bladder dysfunction, radicular pain, numbness or paresthesia in a lumbosacral distribution [24]. Attacks are usually self-limiting but can be recurrent. MRI may be normal, or show edema/hyperintensity/enhancement of the lower cord and nerve roots [24].
A more severe presentation of HSV-2 is acute necrotizing myelitis beginning in the lumbo-sacral region and ascending to the thoracic and cervical regions [25]. This presentation is most frequent in the immunocompromised (particularly with HIV), though cases have also been reported in immunocompetent patients [24, 26, 27]. Paraplegia can be severe and in early stages is often flaccid with absent reflexes [8]. CSF usually shows elevated protein and a mild-to-moderate pleocytosis (lymphocyte-predominant, although polymorphs can be seen with necrotizing lesions) [8].
For both presentations of HSV-2 myelitis, viral DNA can usually be detected from CSF using PCR [25, 28]. Patients can be treated with aciclovir, although the benefit of this medication is unproven in this setting. Outcome varies from complete recovery with Elsberg syndrome to severe residual spastic paraparesis with acute necrotizing lesions.
While encephalitis is the recognized manifestation of HSV-1 in the CNS, rare cases of myelitis have been reported with this viral subtype [29].
Varicella Zoster Virus (VZV)
After primary infection, VZV remains latent in the dorsal root ganglion. Reactivation is more common in the immunocompromised and results in a characteristic vesicular painful dermatomal rash commonly known as shingles, with associated neuropathic pain. Rarely, during an episode of zoster, the virus may spread retrogradely to the spinal cord and cause a myelitis, days to weeks after the dermatomal rash [30]. In immunocompetent patients, myelitis symptoms are often mild and self-limiting [31]. By contrast, in immunocompromised individuals, the presentation is more insidious, severe or potentially fatal, and can even occur without preceding zoster rash (zoster sine herpete) [30, 32].
MRI in VZV myelitis demonstrates T2 hyperintensity at the spinal level corresponding to the involved dermatome, with lesions appearing asymmetric in axial sequences [8]. CSF findings are similar to those seen in HSV myelitis. CSF VZV PCR , VZV IgM and IgG should be tested, with antibody tests reported to demonstrate higher sensitivity than PCR tests in diagnosing CNS complications of VZV [33]. However, physicians should remember that a clinical diagnosis of VZV myelitis can often be made in the appropriate context, allowing early treatment with intravenous acyclovir. The addition of corticosteroids has also been reported to be helpful in some patients [34].
VZV vasculopathy is another well-recognized CNS complication of VZV infection, and it is important to remember that this vasculopathy can cause ischemic myelopathy as well as cerebral stroke [30].
Cytomegalovirus (CMV) & Epstein-Barr Virus (EBV)
CMV is a global infection. Population seroprevalence is between 50% and 60% in highly developed countries [35, 36] while developing countries demonstrate higher seroprevalence, even approaching 100% in some populations [37, 38]. CMV can cause a subacute polyradiculomyelitis in immunocompromised patients, particularly in individuals with advanced HIV (CD4 count <50 cells/mm3) or organ transplant recipients. Clinical presentation is usually ascending weakness and sensory impairment, loss of reflexes and sphincter dysfunction [39]. MRI shows inflammation of the spinal cord and/or nerve roots. Pleocytosis is expected in CSF, and hypoglycorrhachia can also be observed in some cases [39]. CMV DNA can be identified in the CSF with PCR, and serum antibody studies can confirm the presence of CMV IgG antibody. Patients should be treated with intravenous ganciclovir and/or intravenous foscarnet, however, the outcome is often poor [40].
Transverse myelitis occurring in association with primary CMV infection in immunocompetent hosts is likely an immune-mediated phenomenon rather than direct viral infection of the spinal cord, supported by the absence of CMV DNA in CSF of these patients [41], although rare case reports have suggested that direct infection may be possible even in immunocompetent hosts [42]. A similar clinical picture of immune-mediated para-infectious transverse myelitis can occur in association with primary EBV infection, another global infection with high population prevalence [43]. The clinical features of para-infectious transverse myelitis will be discussed later in this chapter.
Rabies Virus
Clinical presentations of rabies virus have become exceedingly rare in developed countries such as the United States, due to effective disease control at an animal level and the availability of rabies vaccine and immunoglobulin for exposed individuals [44]. However, the disease still causes morbidity and mortality in Africa and Asia, with annual human deaths worldwide estimated at almost 60,000 [45]. Rabies virus is transmitted through animal bites (typically dog or bat bites) and spreads to the CNS via peripheral nerves during an incubation period of 20–90 days [44]. Clinical manifestation can be with encephalitic ‘furious’ rabies or less commonly with a radiculomyelitic ‘paralytic’ form. These clinical presentations seem to be determined by whether the initial burden of disease occurs in the brain or the spinal cord. Both forms are usually fatal within days, although time to death in patients with the paralytic form is approximately twice that of encephalitic form [46].
Rabies virus enters the nervous system through the neuro-muscular junction and travels by retrograde tran-synaptic transmission via motor neurons to the CNS [47, 48]. The virus is also thought to spread to peripheral sensory ganglia and peripheral sensory nerves via centrifugal propagation and anterograde axonal transport [47, 49]. The predilection of rabies virus for neurons and its rapid spread through the nervous system may be related to the expression of specific neuronal membrane molecules which bind the virus, and the ability of virally-infected neurons to evade apoptosis [48, 50]. Electrophysiologic and pathophysiologic studies suggest significant peripheral nerve and nerve root dysfunction in paralytic rabies, compared to prominent anterior horn cell dysfunction in furious rabies [44, 51]. The pathogenetic reasons for these differences in clinical presentation are not completely understood, but may relate to host immunological factors [51].
Clinical presentation of paralytic rabies is with flaccid areflexic paralysis which can begin in one limb before evolving to quadriparesis, respiratory failure and dysautonomia. Neuropathic pain can occur and presentation can be mistaken for Guillain-Barre Syndrome. Radiculomyelitis also occurs in the encephalitic form of rabies, but is a later and less clinically important feature in this form as the patient is typically already comatose and severely ill [46].
MRI spinal cord typically shows T2 hyperintensity of the nerve roots and grey matter [46, 52, 53]. MRI brain shows similar non-enhancing increased T2 signal in the brainstem, thalamus, limbic system and white matter of the cerebral hemispheres [46]. Lymphocytic pleocytosis is seen in CSF. Rabies virus RNA can be isolated in CSF, saliva or skin biopsy and anti-rabies virus antibodies can be detected in serum [44]. Rabies virus antigen can also be isolated in skin biopsy taken from a region with hair follicles (viral antigen can be identified in adjacent small sensory nerves) [54].
There is no proven treatment for human rabies, although multiple strategies including rabies vaccination, immunoglobulin, ribavirin, sedatives and interferon-alpha have been attempted. Survival is extremely rare but has occurred with bat-variant rabies. Survival in these rare cases has not been consistently associated with given treatments, and may instead be determined by host immune response [46].
Flaviviruses
West Nile Virus
West Nile virus is an RNA virus transmitted to humans by the Culex mosquito [55]. The virus was first isolated from a female patient in the West Nile region of Uganda in 1937 and was named accordingly [56]. However, this nomenclature is misleading as outbreaks were quickly recognized in other regions such as the Mediterranean, Israel, North Africa, Russia and India [57]. Over the past 20 years, the epidemiology and clinical characteristics of West Nile virus have evolved [57]. Outbreaks of symptomatic disease have become more frequent in diverse locations, and CNS manifestations have become more widely recognized [57]. The first cases in the US were seen in 1999 in New York, and since then the virus has spread across the country [55]. In 2016, 2149 US cases from 46 states were reported to the Centers for Disease Control and Prevention, of which 1309 were reported to be neuro-invasive [58]. Highest incidence occurred in central states including North and South Dakota, Wyoming and Montana [58]. While North America currently has the highest global incidence of West Nile virus, presentations also remain frequent in areas of North Africa, Eastern Europe and France [59].
Symptomatic West Nile virus can be either neuroinvasive or non-neuroinvasive. As many infections are asymptomatic, neuroinvasive disease with direct infection of the nervous system only occurs in approximately 1% of overall infection [60]. Clinical presentation of neuroinvasive disease is with meningitis, encephalitis, myelitis, and radiculitis, either alone or in combination. Infectious symptoms (fever with or without maculopapular rash) usually occur 1–2 days prior to onset of West Nile myelitis, and neurological presentation is with acute flaccid paralysis due to involvement of the anterior horn cells of the spinal cord [60]. Rapid evolution of asymmetric weakness is seen, often with monoplegia, however severe presentations with quadriplegia and respiratory failure can occur [61]. Weakness usually reaches a nadir within 72 h of onset [61]. Cranial nerve manifestations such as facial weakness, extraocular muscle weakness, dysarthria and dysphagia are seen in the majority of patients [61]. Pain in affected limbs is frequent, but sensory loss or paresthesia are uncommon [60]. In rare cases, where polyradiculopathy is more prominent than myelitis, presentation with a Guillain-Barre-like syndrome of ascending weakness and sensory symptoms can occur, and a demyelinating sensorimotor neuropathy can be seen on nerve conduction studies in these patients [60, 61]. Encephalitis is frequently concurrent with other neurological involvement, which can make clinical assessment challenging.
CSF in neuroinvasive West Nile virus demonstrates a pleocytosis (typically a mixed population of lymphocytes and neutrophils with median white cell count of 100 or 200), while protein is usually elevated to the range of 100 mg/dL [61, 62]. The yield of serological and PCR tests varies depending on the stage of infection. West Nile virus replicates at the site of inoculation then spreads to lymph nodes to cause primary viremia, so in early infection viral RNA may be detectable in the serum [63, 64]. By the time symptoms of neuroinvasive infection occur, West Nile virus has typically been cleared from the serum and peripheral organs, and West Nile virus IgM antibody is typically detectable in both serum and CSF [62, 63]. In some cases, viral RNA may also be isolated in CSF with PCR, however sensitivity of this test is low [55]. MRI spinal cord in patients with myelitis shows T2 hyperintensity most prominent in the ventral horn grey matter, with or without enhancement of the conus medullaris and cauda equina) [65,66,67].
Prevention of outbreaks relies on protection from mosquito bites. There is no definitively proven effective treatment for West Nile virus, although case series suggest that IVIG may be beneficial [68]. IVIG is hypothesized to be therapeutic due to the presence of anti-West Nile virus antibodies, which can be detected at high titers in products pooled from endemic regions [69]. Moreover, a preparation of IVIG developed in Israel using only plasma from donors with anti-West Nile virus antibodies has shown promise in animal models [70].
Outcome is variable, though most patients with polio-like presentations will have persistent weakness [60, 61]. Respiratory failure and quadriparesis are associated with the poorest outcomes and possibility of death [60].
Other Flaviviruses
Zika is an emerging mosquito-borne virus. Rare cases of human zika infection were described prior to 2007, when the first significant outbreak occurred in the Federated States of Micronesia [71]. Over subsequent years the virus has spread across pacific regions, South America, Central America and the Caribbean [72]. Multiple neurological complications have been recognized including congenital microcephaly, Guillain-Barre syndrome, myelitis and encephalitis. A handful of cases of myelitis have been reported in association with zika infection [73, 74]. Zika infection can be diagnosed with serum and/or CSF rRT-PCR or with anti-zika IgM (if cross-reactivity with dengue virus IgM can be excluded) [74]. Further research is required to determine whether myelitis associated with zika infection is a result of direct infection, or an immune-mediated para-infectious process.
Dengue virus is another mosquito-borne virus with a significant global disease burden. Neurological manifestations are uncommon, but include encephalopathy, encephalitis, myelitis and post-infectious peripheral nervous system complications [75]. While myelitis is thought to be immune-mediated in most cases, occurrence of myelitis in the acute infectious phase with detectable dengue virus in the CSF suggests the possibility of direct infection in rare cases [75, 76].
Japanese encephalitis predominantly affects children and young adults in southern and eastern Asia, while tick-borne encephalitis is seen in Europe, Russia and East Asia [77, 78]. Both viruses typically present with encephalitis, but the spinal cord may be involved in a minority of cases. Myelitis manifests with acute flaccid paralysis and motor recovery is typically poor. Vaccination is available for both viruses.
Polio Virus
Poliomyelitis caused by the polio virus has essentially become a historical diagnosis, and for this reason we will not provide a detailed description of this disease. Due to concerted global efforts towards eradication, there were only 20 reported cases worldwide in 2017, occurring in Pakistan and Afghanistan [79]. It is hoped that poliomyelitis will become completely eradicated in the coming years. The virus is usually acquired via the fecal-oral route, and poliomyelitis almost exclusively occurs in children [80]. Clinical presentation is characterized by a flu-like illness followed by fever, meningismus, nausea and vomiting. The next symptoms are myalgia and muscle spasms, followed by asymmetric flaccid areflexic paralysis predominantly affecting the lower limbs which evolves over 48 hours [80]. Bulbar involvement, respiratory failure and autonomic involvement result in higher morbidity and mortality, and encephalitis may rarely occur [81].
CSF is typically inflammatory. The virus can frequently be isolated from nasopharyngeal or stool samples. Serological studies and PCR studies on CSF or blood may also be useful in establishing the diagnosis [81]. MRI spine shows hyperintensity of the anterior horn cells, the neuronal cell type most prominently affected [82]. Treatment is supportive and therapy should be undertaken to reduce contractures and deformity. Survivors usually experience significant residual weakness, loss of muscle bulk and skeletal deformity. Some patients will experience functional decline decades later, named post-polio syndrome, the etiology of which is uncertain [80].
Pediatric Acute Flaccid Myelitis
Since 2014, clusters of cases of ‘polio-like’ illness in children have been reported in North America, Australia, South America and Europe [83,84,85,86]. Cases have typically occurred in seasonal and/or regional clusters and affected children ranging in age from 3 months to 15 years [85, 86]. Clinical presentation is associated with prodromal symptoms of infection such as fever, upper respiratory tract symptoms or gastroenteritis. Neurological manifestations occur 1–14 days after prodromal illness [83, 86]. Pain in affected limbs often precedes acute weakness, which reaches a nadir between 4 and 72 h [86]. Asymmetric flaccid paralysis is the hallmark of this clinical syndrome, with depressed or absent reflexes in affected limbs. Cranial nerves or respiratory muscles may be involved, with some patients requiring mechanical ventilation [83, 86]. Sensory deficits, bowel/bladder dysfunction and altered mental status occur in a minority of cases [87].
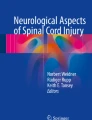
CSF shows a lymphocytic-predominant mild-to-moderate pleocytosis and mildly elevated protein [87]. MRI demonstrates T2 hyperintensity in the gray matter of the spinal cord which is often patchy/poorly defined in the early stage but becomes confluent as the disease progress, extending over multiple vertebral levels and in some cases involving the whole length of the spinal cord and brainstem (Fig. 8.1) [87]. MRI abnormalities are typically non-enhancing at onset, although nerve-root enhancement may evolve later in the disease process [87]. Edema of the spinal cord may also be seen. Neurophysiology may demonstrate a motor neuropathy or neuronopathy in affected limbs, with electromyography changes persisting for a year or more [87].

Acute flaccid myelitis in a 3 year old male
Patchy asymmetric grey matter predominant hyperintensity can be seen throughout the spinal cord on sagittal (a) and (b–d) axial T2 sequences
The pathophysiology of AFM is not completely understood, but is thought to be primarily caused by non-polio enterovirus infection. Prodromal infectious symptoms are ubiquitous, and infectious organisms have been isolated in respiratory secretions or stool in many cases. The most frequently identified micro-organism in patients to date is enterovirus D68, with epidemiological evidence supporting an association between enterovirus D68 outbreaks and AFM clusters [87]. However, CSF PCR and next-generation sequencing studies have typically failed to identify viral organisms in the CNS of affected patients [87, 88].
There is no evidence-based treatment for AFM. Therapy with immunomodulatory or antiviral agents has been instituted in many cases, however it is unclear if any treatment affects the disease course [87]. Complete recovery following AFM is rare. Most patients have persistent motor deficits with muscle atrophy in affected limbs, and some patients may even remain ventilator dependent [87].
Bacterial Myelopathies
Abscesses in the Spinal Canal
Pyogenic Spinal Epidural Abscess
Abscess formation in the epidural space can result from hematogenous, lymphatic or contiguous sources of bacteria or from iatrogenic inoculation during medical procedures in the spinal region. The most common causative organism is Staphylococcus aureus, followed by gram-negative bacilli such as Enterobacter, Klebsiella and Pseudomonas [89, 90]. However, many other bacteria have been implicated in this infection (Table 8.3). Many risk factors for spinal epidural abscess have been identified (Table 8.3), the most important of which is diabetes mellitus [89, 91, 92]. However, in approximately 20% of cases there are no discernable risk factors [93].
The classic clinical triad described with spinal epidural abscess is back pain, fever and neurological deficits [92]. However, the full triad is only present in 10–15% of patients at first presentation [94]. Back pain is present in the vast majority of patients and is reported as acute, focal and severe. The pain may radiate in a radicular manner and the clinician may be able to elicit tenderness to palpation. A septic patient complaining of back pain should alert the physician to the possibility of a spinal epidural abscess. Meningism may occur as the disease progresses. The evolution of clinical symptoms ranges from days to weeks and neurological deficits usually follow other symptoms [94]. Findings on neurological examination will vary depending on the location of the abscess; from tetraparesis with cervical abscesses to cauda equina syndrome with lower lumbar abscesses.
Laboratory tests show raised inflammatory markers (C-reactive protein, erythrocyte sedimentation rate) and peripheral leukocytosis. MRI of the whole spine is the investigation of choice to diagnose spinal epidural abscess, as there may be multiple abscesses at different levels [90, 91]. Sensitivity of MRI is greater than 90%. Abscesses are most commonly seen in the thoracic and lumbar spine, specifically at the thoraco-lumbar junction [95]. The abscess is visualized as a T2 hyperintense, T1 hypointense mass in the epidural space, with associated thickening of overlying displaced dura. Post-contrast imaging is important as this demonstrates a rim-enhancing mass [90]. The spinal cord may show edema at the affected level, or there may be evidence of vascular compromise due to compressed or thrombosed vessels (arterial-pattern ischaemia or venous congestion can be seen). There may also be associated diskitis or facet joint infection, and fat-saturated images can be helpful in delineating areas of soft tissue and bone involvement [90, 94]. CSF is not particularly informative in spinal epidural abscess, and should be avoided in most scenarios due to the risk of creating further nidus of infection and the risk of downward spinal coning in cases with complete spinal subarachnoid block above the level of CSF sampling [96]. Instead, the causative organism should be isolated using other means. Positive blood cultures or sampling from another source of infection (e.g. cellulitis) may identify the culprit organism. However, blood cultures are negative in approximately 40% of cases, so direct sampling using CT-guided aspiration should not be delayed in cases where the organism cannot be quickly identified by other means [97]. In patients requiring urgent surgical decompression, microbiological samples can be obtained during the procedure. The decision on whether to withhold antibiotics until after a microbiological sample has been obtained depends on the patient’s condition and the urgency of treatment.
In recent years, treatment of spinal epidural abscess has evolved, with approximately 40% of patients now treated by a primary medical approach rather than surgery [95]. Surgery (decompressive laminectomy and drainage) should be considered immediately in patients presenting with neurological deficits, and outcome is best with early intervention [98]. Medical therapy alone has a significant failure rate, with 10%–50% of these patients eventually requiring surgery [98]. Antibiotics are required in all cases, starting with broad-spectrum empiric treatment covering staphylococcus, streptococcus and gram-negative species, which can later be tailored according to culture and sensitivity findings.
Neurological deficits at presentation, older age (over 70 years) and co-morbid diabetes mellitus are predictors of poorer outcome in this patient group [98]. Recovery is particularly poor in patients with spinal cord injury secondary to vascular compromise [89].
Other Sites of Abscess Formation
Spinal intramedullary abscesses are extremely rare but can be a devastating neurological infection. They most frequently occur in association with an unrecognized congenital dermal sinus tract, often presenting in childhood [99, 100]. Intramedullary abscesses can also occur with penetrating trauma/procedure to the spinal canal [101], as a complication of bacterial or fungal meningitis [102, 103], or in association with infective endocarditis [104, 105]. Patients present with localized or radicular back pain and neurological deficits. MRI typically shows a rim-enhancing lesion with associated spinal cord edema [106].
Finally, bacterial infections in structures outside the spinal canal can also lead to compressive myelopathy e.g. diskitis and vertebral osteomyelitis.
Tuberculosis
Neurological complications of mycobacterium tuberculosis (TB) infection remain common in the developing world. In the developed world, TB cases predominantly occur in immigrants from regions of endemicity and in higher-risk subpopulations including prisoners, illicit drug users, homeless individuals, patients with HIV and patients treated with anti-TNF therapies [107, 108]. Almost 10,000 cases of TB are reported annually in the US [107].
Pott’s Disease
Myelopathy in patients with TB most commonly results from skeletal vertebrae involvement, in the form of Pott’s disease (tuberculous spondylitis). The spine is the most frequent location of skeletal TB, with Pott’s disease occurring in 1–2% of TB cases [109]. Infection of the vertebrae arises after spread of mycobacteria from an active source (via blood, lymphatics or adjacent lung tissue), or occurs in situ as a result of latent reactivation [110]. Any region of the vertebrae may be involved, but the anterior or central portion of lower thoracic or upper lumbar vertebrae is characteristic [110, 111]. Myelopathy results from direct compression of the spinal cord or vascular compromise (inflammatory arterial thrombosis or venous obstruction). Clinical presentation is insidious, with patients often exhibiting advanced changes on imaging by the time of diagnosis. Back pain, fever and neurological deficits (gait disturbance, leg weakness or sensory changes) are the most frequent presenting symptoms [112,113,114]. Advanced cases may present with Gibbus deformity, an angulated thoracolumbar kyphosis due to wedge-shaped destruction of vertebral bodies. Involvement of cervical paravertebral regions may result in dysphagia or stridor. Systemic symptoms including fever, weight loss, night sweats and cough are present in approximately half of cases, and pulmonary TB is identified in less than half of patients presenting with Pott’s disease [109, 112].
Plain x-ray films remain important for diagnosis in the developing world and may demonstrate loss of vertebral body height, bony erosion, wedge-shaped destruction, kyphosis or associated soft-tissue changes [110]. Computed tomography can identify bony changes with more accuracy and may also identify pulmonary involvement. However, MRI of the entire spine should be the imaging modality of choice in patients with Pott’s disease. This allows evaluation of the extent of bone and soft tissue involvement, and assessment of the spinal canal and spinal cord. Multiple non-contiguous vertebrae may be involved or a well-defined paravertebral abscess may be identified. Involvement of the intervertebral disc occurs late in Pott’s disease, and sparing of the disc may be helpful in differentiating TB from other pyogenic infections which typically arise from the disc [110]. Increased signal in the spinal cord can be a result of direct compression, or the pattern may suggest arterial compromise (prominent gray matter changes) or venous congestion (edematous lower spinal cord) [110]. Differential diagnosis includes other pyogenic infections, fungal infection, histiocytosis, lymphoma and bony metastases. Ancillary investigations for TB such as Mantoux test, serum interferon-gamma release assays, Ziehl-Neelsen staining or Lowenstein-Jensen culture of respiratory samples should be considered. However, diagnosis may be challenging and bone biopsy is frequently performed to identify caseating granulomas [109]. In addition to systemic anti-TB therapy, surgical decompression is usually required in individuals exhibiting neurological deficits.
Spinal Tuberculous Arachnoiditis
Tuberculous radiculomyelopathy results from inflammation of the arachnoid membrane and exiting nerve roots (spinal arachnoiditis). Spinal arachnoiditis can occur in association with TB meningitis, tuberculous spondylitis, or as the primary CNS TB manifestation [115]. Clinical presentation is characterized by subacute areflexic paralysis, often associated with radicular pain and sphincter disturbance [116]. Most patients present with a syndrome of polyradiculopathy, with less than 15% manifesting with myelitis [116]. Clinical findings may suggest cauda equina syndrome or conus medullaris syndrome. MRI spine demonstrates varying degrees of enhancing arachnoiditis, with possible loculated CSF spaces, cystic changes, clumping of nerve roots or spinal cord inflammation and edema [117, 118]. MRI brain should also be performed to assess for pachymeningitis, hydrocephalus or intracranial tuberculomas. Grossly elevated CSF protein (up to 8 g/L) is characteristic of TB meningitis and arachnoiditis [117]. CSF also demonstrates lymphocytic pleocytosis and low CSF glucose [117].
Other Causes of Myelopathy in TB
Cases of acute transverse myelitis (including longitudinally extensive transverse myelitis) have been reported with TB [119]. Intradural-extramedullary or intramedullary tuberculoma can also cause myelopathy and occur most frequently in the thoracic region; presentation is chronic and patients are usually not systemically unwell [116]. Epidural tuberculous abscess can result in compressive spinal cord injury [120]. Syringomyelia can occur as an early or late complication of TB meningitis or spinal arachnoiditis [121, 122]. TB can also trigger CNS vasculitis which can result in spinal cord infarction [116]. MRI and CSF studies are the cornerstone of diagnosis of CNS complications of TB. It is important to remember that patients with HIV are more likely to have disseminated TB with CNS involvement. Patients with CNS manifestations of TB may require longer courses of anti-TB therapy than patients with other manifestations. The addition of corticosteroids has been demonstrated to improve mortality in patients with TB meningitis [123].
Lyme Disease
Borrelia burgdorferi is transmitted by the Ixodes tick species and infection with the spirochete causes Lyme disease. Lyme disease is endemic in North America (particularly north-east and mid-Atlantic states), Europe (highest incidence in Central and North-Eastern Europe) and Asia (Russia, China, Mongolia and Japan) [124]. An estimated 30,000 people are diagnosed with Lyme disease annually in the US [125], with acute cases occurring in a seasonal manner (highest incidence in spring and summer) [126]. While a tick bite is necessary to acquire the infection, many patients do not report or recall this occurring.
Erythema Migrans is the initial presentation of Lyme infection, and is reported in the majority of patients [127]. EM usually occurs 1–2 weeks after the tick bite and is clinically characterized by single or multiple flat erythematous skin lesions which may be painful, itchy or associated with mild systemic symptoms such as malaise, fever and lymphadenopathy [126]. The rash may have a ‘bull’s eye’ appearance or a clear central punctum , but these features are not always present. If early infection is untreated, Lyme disease may disseminate and result in cardiac, rheumatologic or neurologic involvement.
Neuroborreliosis occurs in around 10% of patients with Lyme disease, and can be divided into early and late manifestations [128]. Spinal cord involvement is uncommon in both phases. The most common early complications are cranial neuritis, lymphocytic meningitis and painful polyradiculitis [126, 129]. Very rarely, involvement of the spinal cord can occur during this phase in the form of acute transverse myelitis, which can be longitudinally extensive or can occur as a focal lesion in association with radiculitis [126, 130, 131]. This extension of radicular inflammation into the spinal cord to cause segmental myelitis has been reported with European subspecies of Borrelia. Late complications of Lyme disease (disease duration greater than 6 months) are an area of ongoing debate and some uncertainty, particularly in the case of neurological complications [132,133,134]. Rare cases of chronic progressive Lyme encephalomyelitis have been suggested with longstanding untreated infection, however there is a relative paucity of recent studies in this field [135,136,137]. Patients with late CNS complications arising from longstanding untreated Lyme disease demonstrate inflammatory CSF abnormalities and intrathecal production of Borrelia specific antibodies [128].
Diagnosis of Lyme disease (with or without neuroborreliosis) is also an area of some contention. Two-tier serologic testing is recommended (screening with enzyme immunoassay or indirect immunofluorescence assay followed by confirmation with reflexive immunoblotting for Borrelia IgM and IgG to increase specificity), however these tests may be negative in the earliest stages of infection [138]. Consideration of clinical context is crucial, as even Borrelia IgM may persist for years after infection [138]. CSF culture and PCR for Borrelia are both low yield, and therefore indirect serological studies remain the mainstay of diagnosis for neurological complications [129]. In Europe, the European Academy of Neurology requires fulfillment of 3 of the following criteria for definite neuroborreliosis, and 2 of 3 for possible neuroborreliosis; [1] neurological symptoms suggestive of neuroborreliosis, [2] CSF pleocytosis, and [3] intrathecal production of borrelia burgdorferi-specific antibodies [139]. In the US, which has less heterogeneity of Borrelia subspecies, some groups suggest that positive two-tier serology in the context of a characteristic neurological syndrome may be sufficient for diagnosis [138]. Regardless, CSF study should be performed. The vast majority of patients with neuroborreliosis demonstrate lymphocytic pleocytosis, while elevated CSF protein, and positive oligoclonal bands are also common. Intrathecal Borrelia-specific antibody production is the most specific test for neuroborreliosis. CSF levels should be compared to serum antibody levels, with ratio >1.0 supportive of intrathecal synthesis rather than passive transfer from serum [138]. MRI may demonstrate a segmental or longitudinally extensive enhancing lesion in cases of acute transverse myelitis (Fig. 8.2).

Lyme myelitis in an 18 year old male
Longitudinally extensive central cord hyperintensity is demonstrated on sagittal (a, d) and axial (b, c) T2 sequences. Extensive contrast enhancement can be seen in the thoracic spinal cord on sagittal T1 post-gadolinium sequence (e)
Treatment of neuroborreliosis should be in accordance with regional guidelines; intravenous ceftriaxone for 2 weeks is a typical recommended treatment , while other options include intravenous penicillin or oral doxycycline [138].
Syphilis
Syphilitic infection is caused by the bacterium Treponema pallidum. Almost 30,000 cases of syphilis were reported in the US in 2016 and disease rates have been increasing over the past 15 years, particularly amongst men who have sex with men [140].
T. pallidum is thought to invade the CNS at an early stage of infection, with asymptomatic CSF abnormalities detectable in up to 48% of early syphilis cases [141]. Early or late neurosyphilis can occur in patients who do not clear the organism from the CNS in this early phase (either by immune response or antibiotic treatment) [142]. Neurosyphilis occurs more frequently in patients with syphilis who are HIV-positive than in those who are HIV-negative [141]. Myelopathy as a result of syphilis infection has become rare in the antibiotic era, however it can still occur at any stage in the illness due to a variety of underlying pathologies.
Symptomatic syphilitic meningitis is the most common early CNS manifestation and typically occurs within a year of infection [142]. Spinal cord involvement can occur at this stage in the form of syphilitic meningomyelitis [143,144,145]. Clinical presentation is with an acute or subacute myelopathic syndrome, with or without concurrent symptoms of meningitis. MRI spine shows a T2 hyperintense lesion in the cord which is often central and longitudinally extensive, associated with cord expansion, and demonstrates areas of focal enhancement [144].
Tabes dorsalis is a late complication of untreated syphilis infection which has become very rare. It usually manifests insidiously 15 to 30 years following initial infection [141]. The first symptom is usually severe ‘lightning-like’ pains in the limbs or trunk with associated allodynia. Associated Argyll-Robertson pupils demonstrating light-near dissociation are characteristic. Proprioceptive deficits follow and cause sensory ataxia which can result in Charcot joints [141]. Interestingly, Romberg’s sign was first described based on findings in patients with tabes dorsalis [146]. Loss of deep pain sensation can be demonstrated with a number of eponymous signs such as Abadie sign (absence of pain on squeezing the Achilles tendon) [141]. Loss of muscle stretch reflexes results in absent lower extremity reflexes. Autonomic impairment manifests with erectile dysfunction, bladder and bowel symptoms [141]. End-stage tabes dorsalis is characterized by painful spastic paraplegia with incontinence. MRI spine in untreated tabes dorsalis may show spinal cord atrophy and high signal in the posterior cord [147].
Myelopathy can also occur due to syphilitic gumma in the spinal canal (intramedullary or extramedullary) [148, 149]. Meningovascular syphilis can cause cerebral stroke, and rarely may cause spinal cord infarction [150].
Diagnosis of neurosyphilis is supported by serological tests and CSF findings in the appropriate clinical context, and there are no broadly accepted diagnostic criteria. Non-treponemal serology tests such as the rapid plasma reagin (RPR) test or the venereal disease research laboratory (VDRL) test detect IgM and IgG antibodies to a cardiolipin-lecithin-cholesterol antigen [142]. However, levels may be undetectable in late neurosyphilis, and by contrast, false positives can occur due to a range of other conditions including pregnancy, autoimmune disease and other infections such as malaria [142, 151]. Treponemal tests such as the T. pallidum particle agglutination assay (TPPA) measure IgM and IgG antibodies to the treponemal bacteria [142]. Treponemal test reactivity usually persists after treatment, while non-treponemal titers fall with treatment. Non-treponemal tests are usually used as a screening tool followed by treponemal tests if positive.
CSF findings can be very helpful in diagnosing neurosyphilis. Lymphocytic pleocytosis is seen in most cases, but white cell counts drop as the disease progresses and may even normalize in late disease [142]. There may also be elevated CSF protein, elevated IgG index or positive oligoclonal bands [141]. A positive CSF-VDRL test is very specific for diagnosing neurosyphilis, but less than 70% sensitive [142]. Treponemal tests can be performed on CSF but may be positive in patients with latent or asymptomatic syphilis, and therefore lack specificity in diagnosing neurosyphilis [141]. Overall, physicians should remember that there are multiple treponemal and non-treponemal tests that can be performed on serum and CSF, with varying sensitivity and specificity, so results should be considered in the context of the type of laboratory test used and the clinical scenario.
T. pallidum is highly sensitive to penicillin, and treatment should be instituted upon diagnosis. Guidelines for treatment of neurosyphilis typically suggest intravenous or intramuscular penicillin preparations for 10–21 days [141]. Early neurosyphilis (e.g. syphilitic meningomyelitis) may respond well to treatment, but late complications such as tabes dorsalis may not improve. Non-treponemal serum and CSF (e.g. VDRL) titers can be monitored and should fall after treatment, but it can take from 3 months to 5 years to convert to ‘seronegativity’ [141, 142].
Fungal Myelopathies
Fungal infections of the CNS are uncommon, and most frequently occur in immunocompromised patients.
Cryptococcus neoformans myelitis or myeloradiculitis has been reported in patients with HIV/AIDS, particularly in areas of endemicity, and rarely in immunocompetent hosts [152,153,154]. Formation of intramedullary or extramedullary cryptococcal granulomas is also possible [155,156,157,158], and may occur in association with cryptococcal meningitis or osteomyelitis. CSF should be stained with India ink and can be cultured with Sabouraud dextrose agar to isolate C. neoformans. Rapid screening for cryptococcal antigen in the CSF can also be performed, with sensitivity of over 90% in cases of cryptococcal meningitis [159].
CNS aspergillosis (most commonly due to aspergillus fumigatus) occurs almost exclusively in patients who are markedly immunocompromised e.g. patients with hematological malignancy, bone marrow or solid organ transplant recipients. CNS infection tends to occur in association with systemic sites of infection such as the lung. Rarely, the spinal cord may be involved in CNS aspergillosis, in the form of necrotizing transverse myelitis with or without associated spinal cord infarction [160]. CSF galactomannan testing has high sensitivity and specificity for CNS aspergillosis [161]. PCR can also be performed for aspergillus species in the CSF. CSF fungal cultures are frequently negative [162], and some patients with CNS aspergillosis undergo biopsy for histopathological examination [159].
Fungal infection may also result in spinal cord compromise due to the formation of epidural abscess, vertebral osteomyelitis and spondylodiskitis. These complications have been reported with aspergillus, cryptococcus, candida, blastomycoses and histoplasma species, among others [163,164,165,166,167,168,169,170,171], though it should be emphasized that these manifestations are exceedingly rare.
Parasitic Myelopathies
Schistosomiasis
Schistosomiasis is a parasitic infection acquired through contact with fresh water containing larval forms of Schistosoma parasites (cerceriae) which penetrate human skin. The disease occurs in Sub-Saharan Africa, Asia (China, Japan and South-East Asia) and South America (particularly Brazil and Venezuela), and different sub-species of the parasite have regional preponderances [172]. However, outbreaks in Europe have also been recognized in recent years and traced to Southern European fresh-water locations such as Corsica [173]. It is estimated that over 200 million people are infected worldwide [174].
Clinical manifestations of acute schistosoma infection are most frequently seen in individuals visiting endemic areas with no prior exposure to schistosoma species i.e. travelers [175]. A pruritic maculopapular rash at the site of larval penetration, ‘cercarial dermatitis’, may occur within 24 h of exposure. Acute schistosomiasis occurs several weeks later and manifests with cough, fever, cough, gastrointestinal symptoms and urticarial or angioedema [175]. This phase of disease is thought to be an allergic/toxic reaction to circulating parasites. However, many patients also proceed to chronic infection without any acute symptoms [175]. Chronic infection typically causes inflammation and fibrosis of gastrointestinal, hepatic or urinary tract structures.
Neurological manifestations are rare, but can occur at any stage of schistosomiasis and usually occur without other systemic symptoms. Cerebral involvement is seen with S. japonicum, while spinal cord involvement is seen most commonly with S. mansoni and less frequently with S. haematobium [172]. Myeloradiculopathy is the most frequent presentation, with a minority of patients presenting with either isolated myelitis or cauda equina involvement [172]. Neurological symptoms evolve over less than 2 weeks [176]. Back pain or radicular pain is the most frequent initial symptom, followed by sphincter dysfunction, leg weakness and sensory symptoms. Weakness is usually severe, with most patients unable to walk at clinical nadir. The full complement of motor, sensory and autonomic involvement are seen in the vast majority of patients [176].
CSF examination shows elevated protein and lymphocytic pleocytosis, however eosinophils are also seen in up to 50% of cases and may be a clue to the diagnosis [172, 176]. Oligoclonal bands may be present [177]. MRI typically shows a T2 hyperintense lesion with spinal cord enlargement and nerve root thickening, with associated contrast enhancement in affected regions [172]. Nearly all lesions occur in the lower thoracic or lumbar region, which may be related to venous anastomoses linking the portal venous system (a reservoir for schistosomal parasites) in this spinal region [172].
Establishing a definitive diagnosis can be challenging. S. mansoni ova can be identified with stool examination in less than half of cases, or with rectal biopsy which has higher sensitivity [172]. Serological studies are only useful in patients from non-endemic regions i.e. travellers. CSF ELISA for antibodies to S. mansoni and CSF PCR for S. Mansoni DNA have both been suggested as tests with high specificity [177, 178].
Treatment is with anti-schistosomal therapy such as Praziquantel, and the addition of steroids is probably beneficial (high-dose initially, followed by a taper over at least 2 months) [179]. Most patients have a good functional recovery after treatment. Outcome is worst with delayed diagnosis and with isolated myelitis [172, 180].
Neurocysticercosis
Neurocysticercosis is caused by the larval form of the tapeworm Taenia solium, and is the most common parasitic CNS infection [181]. The tapeworm develops in humans after ingestion of viable larval cysts in contaminated pork, resulting in taeniasis [181]. When the tapeworm matures to adulthood, eggs are released in the host’s feces. Cysticercosis develops after humans become infected with T. solium eggs via the fecal-oral route (typically due to contaminated food or water due to poor hygiene). Eggs penetrate the intestinal wall and travel hematogenously to distant sites – typically the brain, eye, subcutaneous tissues and muscle [181]. This infection is endemic in countries lacking sanitation and clean water supplies, such as South and Central America, Sub-Saharan Africa, China, India and Southeast Asia [181, 182]. Cases in North America and Europe occur predominantly in people who have previously lived in endemic regions [181], although outbreaks have also been reported in those who have never travelled and have been traced to tapeworm carriage in infected food handlers or domestic workers [183].
Neurocysticercosis is an important cause of seizures in endemic countries [184], but other intracranial manifestations include hydrocephalus, meningitis, arachnoiditis, psychiatric disturbance, cranial neuropathies and vasculitis [181]. Spinal cord involvement is rare (occurring in less than 3% of cases of neurocysticercosis) [185] and accompanies basal subarachnoid intracranial disease more frequently than intraparenchymal cerebral disease [186]. Spinal cord involvement without intracranial disease is exceptionally rare [187]. Spinal involvement is most frequently intradural-extramedullary [186, 188], but can also be intramedullary [187, 189].
Clinical presentation is typically with a subacute or chronic myelopathic syndrome or cauda equina syndrome, depending on lesion location [187, 189, 190]. Symptoms may include radicular pain in addition to motor, sensory or sphincter dysfunction [181]. Spinal involvement may also be asymptomatic but detectable on MRI imaging of patients presenting with intracranial manifestations [186].
Diagnosis is difficult, with diagnostic criteria including findings from histology, neuroimaging and clinical/exposure history [191]. Characteristic CNS lesions may be seen on MRI such as demonstration of a high-density scolex (the tapeworm’s head) within a cystic lesion, or a ‘starry sky’ pattern caused by multiple intraparenchymal cysts [181]. CT may demonstrate calcifications in up to half of patients [181]. Spinal MRI findings are usually less specific. Multiple spinal segments are often involved [186], and extramedullary cystic lesions may mimic an arachnoid cyst [190] or Tarlov cyst [192]. Intramedullary involvement is characterized by well-demarcated enhancing cystic lesions with surrounding edema [187]. Subretinal cysticerci can be visualized on ophthalmologic examination in some cases, confirming CNS involvement [191]. Biopsy can be considered for brain lesions, but is not usually undertaken with spinal cord lesions.
CSF shows elevated protein and pleocytosis, with eosinophils frequently present [193]. Antibodies to T. solium antigens can be detected in serum or CSF using enzyme-linked immunoelectrotransfer blot (EITB), however seroprevalence may be up to 20% in endemic regions, and EITB testing may give false-negative results in patients with a single CNS lesion or calcified lesions [191]. ELISA testing for cysticercal antigen in serum or CSF is a recently described method which may also be useful [191]. The diagnosis may also be supported by identification of extra-CNS cysticercosis, for example in subcutaneous nodules [191].
Treatment is with cysticidal drugs such as albendazole and praziquantel. However, rapid death of tapeworms can trigger extensive inflammatory response in the CNS, potentially precipitating neurological deterioration, or hydrocephalus in patients with arachnoiditis or intraparenchymal lesions [181]. Furthermore, anti-cysticercal therapy does not affect calcified cysts containing dead parasites. Therefore, the full burden of CNS disease should be assessed carefully prior to consideration of treatment, and steroids should be initiated prior to anti-cysticercal therapy (and continued throughout treatment) [181]. Lastly, parenchymal neurocysticercosis lesions may self-resolve with time, and so there is some debate about whether all patients actually require treatment [194]. Surgery may be required on some spinal cases, to reduce compression of the spinal cord [190, 192].
Case reports of spinal disease suggest good clinical outcomes with both medical and surgical treatment [187, 189, 190, 192].
Other Parasites
Other parasitic causes of myelopathy are extremely rare. Intramedullary Toxoplasma gondi lesions have been reported in patients with HIV/AIDS [195,196,197]. Hydatid cysts resulting from Echinococcus granulosus infection can occur in vertebral bodies, paraspinal, extradural or intradural-extramedullary locations resulting in progressive compressive myelopathy or cauda equina syndrome [198,199,200,201,202]. Myelitis or myeloradiculitis can occur with visceral larva migrans due to ascaris suum or toxocara canis infection [203,204,205].
Para-infectious Myelitis
Para-infectious myelitis , one of the causes of the syndrome ‘acute transverse myelitis’, may be provoked by systemic infection with a range of micro-organisms, most of which are not known to cause direct infection of the spinal cord. Para-infectious myelitis is felt to be an immune-mediated process, with hypotheses such as molecular mimicry or superantigen effect proposed as pathophysiologic mechanisms [206]. Numerous micro-organisms have been implicated in triggering this process, including (but not limited to) mycoplasma pneumonia, enteroviruses, influenza, adenoviruses, measles virus, mumps virus, haemophilus influenza, streptococcus pneumonia, hepatitis A, rubeola, rubella, legionella and bartonella [206,207,208,209]. In many cases the organism is never identified, despite the presence of infectious symptoms prior to myelitis [210].
Patients present with an acute or subacute myelopathy with first neurological symptoms occurring 3–21 days after onset of infectious symptoms such as fever, upper respiratory symptoms, gastroenteritis or flu-like illness [211]. Sensory symptoms are most frequent, followed by motor symptoms and autonomic symptoms. A sensory level is often elicited on examination [210]. Around half of patients experience severe paraplegia at clinical nadir [212]. Reflexes are often depressed in the initial days of neurological illness, but become brisk as the disease process is established.
Non-specific inflammatory markers such as serum C-reactive protein (CRP) or white blood cell counts may be elevated, supporting recent or ongoing systemic infection. MRI typically shows a T2 hyperintense lesion which may be longitudinally extensive and enhances post-contrast. In some cases there may be multiple lesions [210]. CSF typically shows evidence of inflammation with pleocytosis, elevated protein, positive oligoclonal bands or elevated CSF IgG index [210, 211], though these studies may be normal particularly if obtained early on. Cultures, PCR or antibody studies of blood, stool, or nasopharyngeal swabs should be considered in an attempt to identify the infectious agent.
It is important to consider direct causes of infection such as those discussed in this chapter, prior to proceeding with diagnosis and treatment of immune-mediated para-infectious myelitis. Other disorders that cause myelitis (such as neuromyelitis optica, multiple sclerosis or neurosarcoidosis) should be excluded as far as practicable.
Patients are treated with short course high-dose intravenous steroids (e.g. intravenous methylprednisolone 1 g daily for 3–5 days) and/or intravenous immunoglobulin. Plasma exchange can be considered for severe cases or if there is a poor response to initial steroid treatment [212].
Prognosis is varied and difficult to describe, as case series of transverse myelitis often include a wide variety of underlying etiologies [212]. By natural history, para-infectious myelitis should be a monophasic illness. Recurrent or relapsing myelitis should prompt consideration of other etiologies.
Conclusions
A wide range of infections can cause myelopathy through a number of pathological processes including direct infection, spinal cord compression, or para-infectious etiology. Some infections are endemic in certain regions or are seen more frequently in certain populations e.g. the immunocompromised. These factors should be considered when evaluating a patient with a potential infectious cause of myelopathy. Physicians should also pay careful attention to elements of the clinical presentation such as the temporal profile, prodromal symptoms, and type of neurological deficits. MRI and CSF study are the cornerstone of investigation in most cases, while further laboratory tests such as serological or PCR studies should be tailored to the specific micro-organism(s) suspected. In many cases, clinical outcome may improve with prompt diagnosis and treatment, often with specific anti-microbials.
References
Petito CK, Navia BA, Cho ES, Jordan BD, George DC, Price RW. Vacuolar myelopathy pathologically resembling subacute combined degeneration in patients with the acquired immunodeficiency syndrome. N Engl J Med. 1985 Apr 04;312(14):874–9.
Eyer-Silva WA, Auto I, Pinto JF, Morais-de-Sá CA. Myelopathy in a previously asymptomatic HIV-1-infected patient. Infection. 2001 Mar-Apr;29(2):99–102.
Berger J, Sabet A. Infectious myelopathies. Semin Neurol. 2002;22(2):133–42.
Berger JR. Infectious myelopathies. Continuum (Minneap Minn). 2011 Aug;17(4):761–75.
Oshinaike O, Akinbami A, Ojo O, Ogbera A, Okubadejo N, Ojini F, et al. Influence of age and neurotoxic HAART use on frequency of HIV sensory neuropathy. AIDS Research and Treatment. 2012;2012:1–5.
Sartoretti-Schefer S, Blättler T, Wichmann W. Spinal MRI in vacuolar myelopathy, and correlation with histopathological findings. Neuroradiology. 1997 Dec;39(12):865–9.
Dhasmana D, Taylor GP. Human T-lymphotropic virus/HIV co-infection: a clinical review. Curr Opin Infect Dis. 2014 Feb;27(1):16–28.
Cho TA, Vaitkevicius H. Infectious myelopathies. Continuum (Minneap Minn). 2012 Dec;18(6 Infectious Disease):1351–73.
Di Rocco A, Bottiglieri T, Werner P, Geraci A, Simpson D, Godbold J, et al. Abnormal cobalamin-dependent transmethylation in AIDS-associated myelopathy. Neurology. 2002 Mar 12;58(5):730–5.
Hamada Y, Watanabe K, Aoki T, Arai N, Honda M, Kikuchi Y, et al. Primary HIV infection with acute transverse myelitis. Intern Med. 2011;50(15):1615–7.
Bangham CRM, Araujo A, Yamano Y, Taylor GP. HTLV-1-associated myelopathy/tropical spastic paraparesis. Nat Rev Dis Primers. 2015 June 18;1:15012.
Lyons JL. Myelopathy associated with microorganisms. Continuum (Minneap Minn). 2015 Feb;21(1 Spinal Cord Disorders):100–20.
Khabbaz RF, Darrow WW, Hartley TM, Witte J, Cohen JB, French J, et al. Seroprevalence and risk factors for HTLV-I/II infection among female prostitutes in the United States. JAMA, 1990 Jan 05. 263(1):60–4.
Lehky TJ, Flerlage N, Katz D, Houff S, Hall WH, Ishii K, et al. Human T-cell lymphotropic virus type II-associated myelopathy: clinical and immunologic profiles. Ann Neurol. 1996 Nov;40(5):714–23.
Orland JR, Engstrom J, Fridey J, Sacher RA, Smith JW, Nass C, et al. Prevalence and clinical features of HTLV neurologic disease in the HTLV outcomes study. Neurology. 2003 Dec 09;61(11):1588–94.
Maloney EM, Cleghorn FR, Morgan OS, Rodgers-Johnson P, Cranston B, Jack N, et al. Incidence of HTLV-I-associated myelopathy/tropical spastic paraparesis (HAM/TSP) in Jamaica and Trinidad. J Acquir Immune Defic Syndr Hum Retrovirol. 1998 Feb 01;17(2):167–70.
Akizuki S, Nakazato O, Higuchi Y, Tanabe K, Setoguchi M, Yoshida S, et al. Necropsy findings in HTLV-I associated myelopathy. Lancet. 1987 Jan 17;1(8525):156–7.
San-Martin DL, Santos DND, Baptista AF. Pain prevalence, characteristics and associated factors in human T-cell lymphotropic virus type 1 infected patients: a systematic review of the literature. Braz J Infect Dis. 2016 Nov – Dec;20(6):592–8.
Malm K, Kjerstadius T, Andersson S. Evaluation of a new screening assay for HTLV-1 and -2 antibodies for large-scale use. J Med Virol. 2010 Sep;82(9):1606–11.
Takatani M, Crispim ME, Fraiji N, Stefani MMA, Kiesslich D. Clinical and laboratory features of HTLV-I asymptomatic carriers and patients with HTLV-I-associated myelopathy/tropical spastic paraparesis from the Brazilian Amazon. Rev Inst Med Trop Sao Paulo. 2017 Apr 03;59:e5.
Bagnato F, Butman JA, Mora CA, Gupta S, Yamano Y, Tasciyan TA, et al. Conventional magnetic resonance imaging features in patients with tropical spastic paraparesis. J Neurovirol. 2005 Dec;11(6):525–34.
Liu W, Nair G, Vuolo L, Bakshi A, Massoud R, Reich DS, et al. In vivo imaging of spinal cord atrophy in neuroinflammatory diseases. Ann Neurol. 2014 Sep;76(3):370–8.
Nakagawa M, Nakahara K, Maruyama Y, Kawabata M, Higuchi I, Kubota H, et al. Therapeutic trials in 200 patients with HTLV-I-associated myelopathy/ tropical spastic paraparesis. J Neurovirol. 1996 Oct;2(5):345–55.
Berger JR, Houff S. Neurological complications of herpes simplex virus type 2 infection. Arch Neurol. 2008 May 1;65(5):596–600.
Nakajima H, Furutama D, Kimura F, Shinoda K, Ohsawa N, Nakagawa T, et al. Herpes simplex virus myelitis: clinical manifestations and diagnosis by the polymerase chain reaction method. Eur Neurol. 1998;39(3):163–7.
Wiley CA, VanPatten PD, Carpenter PM, Powell HC, Thal LJ. Acute ascending necrotizing myelopathy caused by herpes simplex virus type 2. Neurology. 1987 Jan 11;37(11):1791.
Nardone R, Versace V, Brigo F, Tezzon F, Zuccoli G, Pikija S, et al. Herpes simplex virus type 2 myelitis: case report and review of the literature. Front Neurol. 2017;8:199.
Savoldi F, Kaufmann T, Flanagan E, Toledano M, Weinshenker B. Elsberg syndrome: a rarely recognized cause of cauda equina syndrome and lower thoracic myelitis. Neurology: Neuroimmunology & Neuroinflammation. 2017 Jul:4(4).
Figueroa D, Isache C, Sands M, Guzman N. An unusual case of acute transverse myelitis caused by HSV-1 infection. IDCases. 2016;5:29–31.
Nagel MA, Gilden D. Neurological complications of VZV reactivation. Curr Opin Neurol. 2014 June;27(3):356–60.
Steiner I, Kennedy PG, Pachner AR. The neurotropic herpes viruses: herpes simplex and varicella-zoster. Lancet Neurol. 2007 November 1;6(11):1015–28.
Manian FA, Kindred M, Fulling KH. Chronic varicella-zoster virus myelitis without cutaneous eruption in a patient with AIDS: report of a fatal case. Clin Infect Dis. 1995;21(4):986–8.
Nagel MA, Forghani B, Mahalingam R, Wellish MC, Cohrs RJ, Russman AN, et al. The value of detecting anti-VZV IgG antibody in CSF to diagnose VZV vasculopathy. Neurology. 2007 Mar 27;68(13):1069–73.
Takahashi T, Tamura M, Miki K, Yamaguchi M, Kanno A, Nunomura S, et al. Varicella zoster virus myelitis in two elderly patients: diagnostic value of nested polymerase chain reaction assay and antibody index for cerebrospinal fluid specimens. Case Rep Neurol. 2013 Jan;5(1):81–90.
Staras SAS, Dollard SC, Radford KW, Flanders WD, Pass RF, Cannon MJ. Seroprevalence of Cytomegalovirus Infection in the United States, 1988–1994. Clin Infect Dis. 2006 Jan 11;43(9):1143–51.
Seale H, Raina MacIntyre C, Gidding HF, Backhouse JL, Dwyer DE, Gilbert L. National serosurvey of cytomegalovirus in Australia. Clin Vacc Immunol. 2006 Nov 1;13(11):1181–4.
Saraswathy TS, Az-Ulhusna A, Asshikin RN, Suriani S, Zainah S. Seroprevalence of cytomegalovirus infection in pregnant women and associated role in obstetric complications: a preliminary study. Southeast Asian J Trop Med Public Health. 2011 Mar;42(2):320–2.
Krech U, Tobin J. A collaborative study of cytomegalovirus antibodies in mothers and young children in 19 countries. Bull World Health Organ. 1981;59(4):605.
Cohen BA, McArthur JC, Grohman S, Patterson B, Glass JD. Neurologic prognosis of cytomegalovirus polyradiculomyelopathy in AIDS. Neurology. 1993 Mar;43(3 Pt 1):493–9.
Maschke M, Kastrup O, Diener H. CNS manifestations of cytomegalovirus infections: diagnosis and treatment. CNS Drugs. 2002;16(5):303–15.
Fux CA, Pfister S, Nohl F, Zimmerli S. Cytomegalovirus-associated acute transverse myelitis in immunocompetent adults. Clin Microbiol Infect. 2003 Dec;9(12):1187–90.
Karunarathne S, Govindapala D, Udayakumara Y, Fernando H. Cytomegalovirus associated transverse myelitis in an immunocompetent host with DNA detection in cerebrospinal fluid; a case report. BMC Research Notes. 2012 Jan 1;5(1):364.
Scheld WM, Whitley RJ, Marra CM. Infections of the central nervous system. Lippincott Williams & Wilkins; 2014.
Jackson A. Human rabies: a 2016 update. Curr Infect Dis Rep. 2016 Nov;18(11):1–6.
Hampson K, Coudeville L, Lembo T, Sambo M, Kieffer A, Attlan M, et al. Estimating the global burden of endemic canine rabies. PLoS Negl Trop Dis. 2015 Apr;9(4):e0003709.
Hemachudha T, Ugolini G, Wacharapluesadee S, Sungkarat W, Shuangshoti S, Laothamatas J. Human rabies: neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013 May 1;12(5):498–513.
Ugolini G. Chapter 10: Rabies virus as a transneuronal tracer of neuronal connections. In: Jackson AC, editor. Advances in virus research. Academic Press; 2011. p. 165–202.
Lafon M. Rabies virus receptors. J Neurovirol. 2005 Feb;11(1):82–7.
Bauer A, Nolden T, Schröter J, Römer-Oberdörfer A, Gluska S, Perlson E, et al. Anterograde glycoprotein-dependent transport of newly generated rabies virus in dorsal root ganglion neurons. J Virol. 2014 Dec 15;88(24):14172–83.
Reiss CS. Neurotropic viral infections. Cambridge University Press; 2008.
Mitrabhakdi E, Shuangshoti S, Wannakrairot P, Lewis RA, Susuki K, Laothamatas J, et al. Difference in neuropathogenetic mechanisms in human furious and paralytic rabies. J Neurol Sci. 2005 Nov 15;238, 3(1–2):–10.
Desai RV, Jain V, Singh P, Singhi S, Radotra BD. Radiculomyelitic rabies: can MR imaging help? AJNR Am J Neuroradiol. 2002 Apr;23(4):632–4.
Kalita J, Bhoi SK, Bastia JK, Lashkar S, Mahadevan A, Misra UK. Paralytic rabies: MRI findings and review of literature. Neurol India. 2014 Nov–Dec;62(6):662–4.
Bryceson ADM, Greenwood BM, Warrell DA, Davidson NM, Pope HM, Lawrie JH, et al. Demonstration during life of rabies antigen in humans. J Infect Dis. 1975 Jan 01;131(1):71–4.
Lyons J, McArthur J. Emerging infections of the central nervous system. Curr Infect Dis Rep. 2013 Dec;15(6):576–82.
Smithburn KC, Hughes TP, Burke AW, Paul JH. A neurotropic virus isolated from the blood of a native of Uganda. American Journal of Tropical Medicine. 1940;20:471–2.
Sejvar JJ. West Nile virus: an historical overview. Ochsner J. 2003;5(3):6–10.
Centers for Disease Control and Prevention. West Nile virus, cumulative data 1999–2016; 2017. Available at https://www.cdc.gov/westnile/statsmaps/cumMapsData.html. Accessed 24 Oct 2017
WHO GIDEON (Global Infectious Diseases and Epidemiology Online). West Nile fever; 2017. Available at https://www.gideononline.com/cases/westnilefever/. Accessed 24 Oct 2017
Sejvar JJ. Clinical manifestations and outcomes of West Nile virus infection. Viruses. 2014 Feb;6(2):606–23.
Sejvar JJ, Bode AV, Marfin AA, Campbell GL, Ewing D, Mazowiecki M, et al. West Nile virus-associated flaccid paralysis. Emerging Infect Dis. 2005 Jul;11(7):1021–7.
Tyler KL, Pape J, Goody RJ, Corkill M, Kleinschmidt-DeMasters BK. CSF findings in 250 patients with serologically confirmed West Nile virus meningitis and encephalitis. Neurology. 2006 Feb 14;66(3):361–5.
Sambri V, Capobianchi MR, Cavrini F, Charrel R, Donoso-Mantke O, Escadafal C, et al. Diagnosis of West Nile virus human infections: overview and proposal of diagnostic protocols considering the results of external quality assessment studies. Viruses. 2013 Sept 25;5(10):2329–48.
Samuel MA, Diamond MS. Pathogenesis of West Nile virus infection: a balance between virulence, innate and adaptive immunity, and viral evasion. J Virol. 2006 Oct;80(19):9349–60.
Petropoulou KA, Gordon SM, Prayson RA, Ruggierri PM. West Nile virus meningoencephalitis: MR imaging findings. AJNR Am J Neuroradiol. 2005 Sep;26(8):1986–95.
Maramattom BV, Philips G, Sudheesh N, Arunkumar G. Acute flaccid paralysis due to West nile virus infection in adults: a paradigm shift entity. Ann Indian Acad Neurol. 2014 Jan;17(1):85–8.
Ali M, Safriel Y, Sohi J, Llave A, Weathers S. West Nile virus infection: MR imaging findings in the nervous system. AJNR Am J Neuroradiol. 2005 Feb;26(2):289–97.
Shimoni Z, Bin H, Bulvik S, Niven M, Hazzan R, Mendelson E, et al. The clinical response of West Nile virus neuroinvasive disease to intravenous immunoglobulin therapy. Clin Pract. 2012 Jan 27;2(1)
Haley M, Retter AS, Fowler D, Gea-Banacloche J, O’Grady NP. The role for intravenous immunoglobulin in the treatment of West Nile virus encephalitis. Clin Infect Dis. 2003 Sep 15;37(6):88.
Ben-Nathan D, Gershoni-Yahalom O, Samina I, Khinich Y, Nur I, Laub O, et al. Using high titer West Nile intravenous immunoglobulin from selected Israeli donors for treatment of West Nile virus infection. BMC Infect Dis. 2009 Feb 17;9:18.
Duffy MR, Chen T, Hancock WT, Powers AM, Kool JL, Lanciotti RS, et al. Zika Virus outbreak on Yap Island, Federated States of Micronesia. New England Journal of Medicine. 2009 June 11;360(24):2536–43.
Muñoz L, Barreras P, Pardo C. Zika Virus – associated neurological disease in the adult: Guillain–Barré syndrome, encephalitis, and myelitis. Semin Reprod Med. 2016 Sep 9;34(5):273–9.
Mécharles S, Herrmann C, Poullain P, Tran T, Deschamps N, Mathon G, et al. Acute myelitis due to Zika virus infection. The Lancet. 2016 April 02;387(10026):1481.
da Silva IRF, Frontera JA, de Filippis AMB, do Nascimento OJM. Neurologic complications associated with the Zika Virus in Brazilian adults. JAMA Neurol. 2017 Oct 01;74(10):1190–8.
Carod-Artal FJ, Wichmann O, Farrar J, Gascón J. Neurological complications of dengue virus infection. Lancet Neurol. 2013 Sept 01;12(9):906–19.
Kunishige M, Mitsui T, Tan BH, Leong HN, Takasaki T, Kurane I, et al. Preferential gray matter involvement in dengue myelitis. Neurology. 2004 Nov 23;63(10):1980–1.
Solomon T, Dung NM, Kneen R, Gainsborough M, Vaughn DW, Khanh VT. Japanese encephalitis. J Neurol Neurosurg Psych. 2000 April 01;68(4):405–15.
Taba P, Schmutzhard E, Forsberg P, Lutsar I, Ljøstad U, Mygland Å, et al. EAN consensus review on prevention, diagnosis and management of tick-borne encephalitis. Eur J Neurol. 2017 Oct;24(10):e61.
Polio Global Eradication Initiative. Polio now; 2017. Available at: http://polioeradication.org/polio-today/polio-now/this-week/. Accessed 5 Jan 2018
Howard RS. Poliomyelitis and the postpolio syndrome. BMJ. 2005 Jun 04;330(7503):1314–8.
Howard RS. Poliomyelitis. In: Hilton-Jones D, Turner MR, editors. Oxford textbook of neuromuscular disorders. Oxford University Press; 2014. p. 51–7.
Haq A, Wasay M. Magnetic resonance imaging in poliomyelitis. Arch Neurol. 2006 May 01;63(5):778.
Ruggieri V, Paz MI, Peretti MG, Rugilo C, Bologna R, Freire C, et al. Enterovirus D68 infection in a cluster of children with acute flaccid myelitis, Buenos Aires, Argentina, 2016. Eur J Paediatr Neurol. 2017 Nov;21(6):884–90.
Andersen EW, Kornberg AJ, Freeman JL, Leventer RJ, Ryan MM. Acute flaccid myelitis in childhood: a retrospective cohort study. Eur J Neurol. 2017 August 1;24(8):1077–83.
Hübner J, Kruse B, Christen HJ, Weidenmann J, Weiner V, Schöne-Bake JC, et al. Acute flaccid myelitis in German children in 2016-the return of polio? Dtsch Arztebl Int. 2017 August;114(33–34):557.
Messacar K, Schreiner TL, Maloney JA, Wallace A, Ludke J, Oberste MS, et al. A cluster of acute flaccid paralysis and cranial nerve dysfunction temporally associated with an outbreak of enterovirus D68 in children in Colorado, USA. Lancet. 2015 Apr 25;385(9978):1662–71.
Messacar K, Schreiner TL, Van Haren K, Yang M, Glaser CA, Tyler KL, et al. Acute flaccid myelitis: a clinical review of US cases 2012–2015. Ann Neurol. 2016 Sep;80(3):326–38.
Sejvar JJ, Lopez AS, Cortese MM, Leshem E, Pastula DM, Miller L, et al. Acute flaccid myelitis in the United States, August–December 2014: results of nationwide surveillance. Clin Infect Dis. 2016 Sept 15;63(6):737–45.
Roos KL. Bacterial infections of the central nervous system. Continuum: Lifelong Learning in Neurology. 2015 Dec 01;21(6, Neuroinfectious Disease):1679–91.
Tali ET, Oner AY, Koc AM. Pyogenic spinal infections. Neuroimaging Clinics of North America. 2015 May 1;25(2):193–208.
Bond A, Manian FA. Spinal epidural abscess: a review with special emphasis on earlier diagnosis. BioMed Research International. 2016 Jan 1;2016:1–6.
Alerhand S, Wood S, Long B, Koyfman A. The time-sensitive challenge of diagnosing spinal epidural abscess in the emergency department. Intern Emerg Med. 2017 Dec;12(8):1179–83.
Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospective review of 128 cases. The Spine Journal. 2014 February 1;14(2):326–30.
Sendi P, Bregenzer T, Zimmerli W. Spinal epidural abscess in clinical practice. QJM. 2008 Jan 01;101(1):1–12.
Arko L, Quach E, Nguyen V, Chang D, Sukul V, Kim B. Medical and surgical management of spinal epidural abscess: a systematic review. Neurosurg Focus. 2014 Aug;37(2):E4.
Hollis PH, Malis LI, Zappulla RA. Neurological deterioration after lumbar puncture below complete spinal subarachnoid block. J Neurosurg. 1986 Feb;64(2):253–6.
Curry WT, Hoh BL, Amin-Hanjani S, Eskandar EN. Spinal epidural abscess: clinical presentation, management, and outcome. Surg Neurol. 2005;63(4):371. discussion 371
Suppiah S, Meng Y, Fehlings MG, Massicotte EM, Yee A, Shamji MF. How best to manage the spinal epidural abscess? A current systematic review. World Neurosurg. 2016 Sep;93:20–8.
Kanaheswari Y, Lai C, Raja Lope RJ, Azizi AB, Zulfiqar MA. Intramedullary spinal cord abscess: the result of a missed congenital dermal sinus. J Paediatr Child Health. 2015 Feb;51(2):223–5.
Papaevangelou G, Tsitsopoulos PP, Flaris N, Iliadis C, Tsonidis C. Dermal sinus tract of the thoracic spine presenting with intramedullary abscess and cranial nerve deficits. Pediatr Neurosurg. 2015;50(6):339–43.
da Silva PSL, de Souza Loduca RD. Intramedullary spinal cord abscess as complication of lumbar puncture: a case-based update. Childs Nerv Syst. 2013 July;29(7):1061–8.
Vo DT, Cravens GF, Germann RE. Streptococcus pneumoniae meningitis complicated by an intramedullary abscess: a case report and review of the literature. J Med Case Rep. 2016 Dec;10(1)
Bajema KL, Dalesandro MF, Fredricks DN, Ramchandani M. Disseminated coccidioidomycosis presenting with intramedullary spinal cord abscesses: management challenges. Med Mycol Case Rep. 2017 Mar;15:1–4.
Fernández-Ruiz M, López-Medrano F, García-Montero M, Hornedo-Muguiro J, Aguado J. Intramedullary cervical spinal cord abscess by viridans group streptococcus secondary to infective endocarditis and facilitated by previous local radiotherapy. Intern Med. 2009;48(1):61–4.
Arnáiz-García ME, González-Santos JM, López-Rodriguez J, Dalmau-Sorli MJ, Bueno-Codoñer M, Arévalo-Abascal A. Intramedullary cervical abscess in the setting of aortic valve endocarditis. Asian Cardiovasc Thorac Ann. 2015 Jan;23(1):64–6.
Dörflinger-Hejlek E, Kirsch EC, Reiter H, Opravil M, Kaim AH. Diffusion-weighted MR imaging of intramedullary spinal cord abscess. AJNR Am J Neuroradiol. 2010 Oct;31(9):1651–2.
Centers for Disease Control and Prevention Trends in tuberculosis – United States; 2017. Available at https://www.cdc.gov/tb/publications/factsheets/statistics/tbtrends.htm. Accessed 20 Nov 2017
Xie X, Li F, Chen J, Wang J. Risk of tuberculosis infection in anti-TNF-α biological therapy: from bench to bedside. Journal of Microbiology, Immunology and Infection. 2014 August 1;47(4):268–74.
Schlesinger N, Lardizabal A, Rao J, Rao J, McDonald R. Tuberculosis of the spine: experience in an inner city hospital. J Clin Rheumatol. 2005 Feb;11(1):17–20.
Kilborn T, van Rensburg PJ, Candy S. Pediatric and adult spinal tuberculosis: imaging and pathophysiology. Neuroimaging Clinics of North America. 2015 May 1;25(2):209–31.
Hogan JI, Hurtado RM, Nelson SB. Mycobacterial musculoskeletal infections. Infectious Disease Clinics of North America. 2017 June 1;31(2):369–82.
Johansen IS, Nielsen SL, Hove M, Kehrer M, Shakar S, Wøyen AVT, et al. Characteristics and clinical outcome of bone and joint tuberculosis from 1994 to 2011: a retrospective register-based study in Denmark. Clin Infect Dis. 2015 Aug 15;61(4):554–62.
Turgut M. Spinal tuberculosis (Pott’s disease): its clinical presentation, surgical management, and outcome. A survey study on 694 patients. Neurosurg Rev. 2001 Apr;24(1):8–13.
Moghtaderi A, Alavi-Naini R, Rahimi-Movaghar V. Tuberculous myelopathy: current aspects of neurologic sequels in the southeast of Iran. Acta Neurol Scand. 2006 Apr;113(4):267–72.
Hernández-Albújar S, Arribas JR, Royo A, González-García JJ, Peña JM, Vázquez JJ. Tuberculous radiculomyelitis complicating tuberculous meningitis: case report and review. Clin Infect Dis. 2000 June 01;30(6):915–21.
Garg RK, Malhotra HS, Gupta R. Spinal cord involvement in tuberculous meningitis. Spinal Cord, 2015 Sep 1. 53(9):649.
Abdelmalek R, Kanoun F, Kilani B, Tiouiri H, Zouiten F, Ghoubantini A, et al. Tuberculous meningitis in adults: MRI contribution to the diagnosis in 29 patients. International Journal of Infectious Diseases. 2006 September 1;10(5):372–7.
Srivastava T, Kochar D. Asymptomatic spinal arachnoiditis in patients with tuberculous meningitis. Neuroradiology. 2003 Oct;45(10):727–9.
Sahu SK, Giri S, Gupta N. Longitudinal extensive transverse myelitis due to tuberculosis: a report of four cases. J Postgrad Med. 2014 Oct–Dec;60(4):409–12.
Metta H, Corti M, Redini L, Yampolsky C, Schtirbu R. Spinal epidural abscess due to Mycobacterium tuberculosis in a patient with AIDS: case report and review of the literature. Brazilian Journal of Infectious Diseases. 2006 Apr 1;10(2):146–8.
Kaynar MY, Koçer N, Gençosmanoğlu BE, Hancı M. Syringomyelia – as a late complication of tuberculous meningitis. Acta Neurochir. 2000 Aug;142(8):935–9.
Daif AK, al Rajeh S, Ogunniyi A, al Boukai A, al Tahan A. Syringomyelia developing as an acute complication of tuberculous meningitis. Can J Neurol Sci. 1997 Feb;24(1):73–6.
Prasad K, Singh MB, Ryan H. Corticosteroids for managing tuberculous meningitis. Cochrane Database Syst Rev. 2016;4:CD002244.
Mead PS. Epidemiology of Lyme disease. Infectious Disease Clinics of North America. 2015 June 1;29(2):187–210.
Nelson C, Saha S, Kugeler K, Delorey M, Shankar M, Hinckley A, et al. Incidence of clinician-diagnosed Lyme disease, United States, 2005–2010. Emerg Infect Dis. 2015;21(9):1625–31. https://doi.org/10.3201/eid2109.150417.
Marques AR. Lyme neuroborreliosis. Continuum: Lifelong Learning in Neurology. 2015 Dec 01;21(6, Neuroinfectious Disease):1729–44.
Allen HB, Vin H. Lyme disease: beyond erythema migrans. Journal of Clinical & Experimental Dermatology Research. 2016;7(2)
Koedel U, Pfister H. Lyme neuroborreliosis. Curr Opin Infect Dis. 2017 Feb;30(1):101–7.
Koedel U, Fingerle V, Pfister H. Lyme neuroborreliosis-epidemiology, diagnosis and management. Nat Rev Neurol. 2015 Aug;11(8):446.
Bigi S, Aebi C, Nauer C, Bigler S, Steinlin M. Acute transverse myelitis in Lyme neuroborreliosis. Infection. 2010 Oct 1;38(5):413–6.
Rousseau JJ, Lust C, Zangerle PF, Bigaignon G. Acute transverse myelitis as presenting neurological feature of Lyme disease. Lancet. 1986 Nov 22;2(8517):1222–3.
Halperin JJ. Chronic Lyme disease: misconceptions and challenges for patient management. Infection and Drug Resistance. 2015;8:119–28.
Ballantyne C. The chronic debate over Lyme disease. Nature Medicine. 2008 Nov 01;14(11):1135.
Rowe PM. Chronic Lyme disease: the debate goes on. The Lancet. 2000 April 22;355(9213):1436.
Halperin JJ. Nervous system Lyme disease. Curr Infect Dis Rep. 2015 Jan;17(1):445.
Oschmann P, Dorndorf W, Hornig C, Schäfer C, Wellensiek HJ, Pflughaupt KW. Stages and syndromes of neuroborreliosis. J Neurol. 1998 May;245(5):262–72.
Logigian EL, Kaplan RF, Steere AC. Chronic neurologic manifestations of Lyme disease. N Engl J Med. 1990;323(21):1438–44.
Moore A, Nelson C, Molins C, Mead P, Schriefer M. Current guidelines, common clinical pitfalls, and future directions for laboratory diagnosis of Lyme disease. United States Emerging Infect Dis. 2016;07:22(7).
Mygland A, Ljøstad U, Fingerle V, Rupprecht T, Schmutzhard E, Steiner I. EFNS guidelines on the diagnosis and management of European Lyme neuroborreliosis. Eur J Neurol. 2010 Jan;17(1):4.
Centers for Disease Control and Prevention Syphilis – 2016 STD surveillance report. 10-17T05:35:17Z; 2017
Berger JR, Dean D. Neurosyphilis. In: Biller J, Ferro JM, editors. Handbook of clinical neurology. Elsevier; 2014. p. 1461–72.
Marra CM. Neurosyphilis. Continuum: Lifelong Learning in Neurology. 2015 Dec 01;21(6, Neuroinfectious Disease):1714–28.
Tohge R, Shinoto Y, Takahashi M. Longitudinally extensive transverse myelitis and optic neuropathy associated with syphilitic meningomyelitis and human immunodeficiency virus infection: a case report and review of the literature. Intern Med. 2017;56(15):2067–72.
Chilver-Stainer L, Fischer U, Hauf M, Fux CA, Sturzenegger M. Syphilitic myelitis: rare, nonspecific, but treatable. Neurology. 2009 Feb 17;72(7):673–5.
Siu G. Syphilitic meningomyelitis. J Am Osteopath Assoc. 2017 Dec 01;117(10):671.
Pearce JMS. Romberg and his sign. Eur Neurol. 2005;53(4):210–3.
Pandey S. Magnetic resonance imaging of the spinal cord in a man with tabes dorsalis. J Spinal Cord Med. 2011 Nov;34(6):609–11.
Yang C, Li G, Fang J, Liu H, Yang B, Xu Y. Spinal intramedullary syphilitic gumma: an unusual presentation of neurosyphilis. World Neurosurgery. 2016 November 1;95(Supplement C):622.e23.
Zhou H, Zhan R, Chen M, Cao F, Zheng X. Solitary spinal dural syphilis granuloma mimicking a spinal meningioma. Turk Neurosurg. 2014;24(2):288–91.
Terry PM, Glancy GR, Graham A. Meningovascular syphilis of the spinal cord presenting with incomplete Brown-Séquard syndrome: case report. Genitourin Med. 1989 Jun;65(3):189–91.
Maves RC, Dean K, Gadea N, Halsey ES, Graf PCF, Lescano AG. False-positive rapid plasma reagin testing in patients with acute Plasmodium vivax malaria: a case control study. Travel Med Infect Dis. 2014 May–Jun;12(3):268–73.
Gumbo T, Hakim JG, Mielke J, Siwji S, Just-Nübling G, Ismail A. Cryptococcus myelitis: atypical presentation of a common infection. Clin Infect Dis. 2001 Apr 15;32(8):1235–6.
Dromer F, Moulignier A, Dupont B, Guého E, Baudrimont M, Improvisi L, et al. Myeloradiculitis due to cryptococcus curvatus in AIDS. AIDS. 1995 Apr;9(4):395–6.
Rai AK, Synmon B, Basumatary LJ, Das M, Goswami M, Kayal AK. Cryptococcal myelitis: a rare manifestation in immunocompetent patients. Neurol India. 2014 May–Jun;62(3):321–2.
Su MC, Ho WL, Chen JH. Intramedullary cryptococcal granuloma of spinal cord: a case report. Zhonghua Yi Xue Za Zhi (Taipei). 1994 Jan;53(1):58–61.
Ramamurthi B, Anguli VC. Intramedullary cryptococcic granuloma of the spinal cord. Journal of Neurosurgery. 1954 November 1;11(6):622–4.
Asanuma Y, Fujimoto H, Nakabayashi H, Akeda K, Asanuma K, Tanaka M, et al. Extradural cryptococcoma at the sacral spine without bone involvement in an immunocompetent patient. J Orthop Sci. 2014;19(6):1040.
Rao SB, Rao KS, Dinakar I. Spinal extradural cryptococcal granuloma. A case report. Neurol India. 1970 Sep;18(3):192–3.
Murthy JMK, Sundaram C. Fungal infections of the central nervous system. In: Biller J, Ferro JM, editors. Handbook of clinical neurology. Elsevier; 2014. p. 1383–401.
Kleinschmidt-DeMasters BK. Central nervous system aspergillosis: a 20-year retrospective series. Hum Pathol. 2002 Jan;33(1):116–24.
Chong GM, Maertens JA, Lagrou K, Driessen GJ, Cornelissen JJ, Rijnders BJA. Diagnostic performance of galactomannan antigen testing in cerebrospinal fluid. J Clin Microbiol. 2016 Feb;54(2):428–31.
Sonneville R, Magalhaes E, Meyfroidt G. Central nervous system infections in immunocompromised patients. Current Opinion in Critical Care. 2017 Apr 01;23(2):128–33.
N’dri Oka D, Varlet G, Kakou M, Zunon-Kipre Y, Broalet E, Ba ZV. Spondylodiscitis due to Histoplasma duboisii. Report of two cases and review of the literature. Neurochirurgie. 2001 Sep;47(4):431–4.
Ozdemir N, Celik L, Oğuzoğlu S, Yildirim L, Bezircioğlu H. Cervical vertebral osteomyelitis and epidural abscess caused by Candida albicans in a patient with chronic renal failure. Turk Neurosurg. 2008 Apr;18(2):207–10.
Chia SL, Tan BH, Tan CT, Tan SB. Candida spondylodiscitis and epidural abscess: management with shorter courses of anti-fungal therapy in combination with surgical debridement. J Infect. 2005 Jul;51(1):17–23.
Garbino J, Schnyder I, Lew D, Bouchuiguir-Wafa K, Rohner P. An unusual cause of vertebral osteomyelitis: Candida species. Scand J Infect Dis. 2003;35(4):288–91.
Dimar JR, Puno RM, Nowacki MR, Carreon LY. Surgery for blastomycosis of the spine. Am J Orthop. 2014 Nov;43(11):266.
Makary CA, Roberts TD, Wetmore SJ. Disseminated blastomycosis presenting as mastoiditis and epidural abscess. W V Med J. 2014 Jan-Feb;110(1):46–7.
Gupta SK, Chhabra R, Sharma BS, Das A, Khosla VK. Vertebral cryptococcosis simulating tuberculosis. Br J Neurosurg. 2003 Dec;17(6):556–9.
Raj KA, Srinivasamurthy BC, Nagarajan K, Sinduja MGI. A rare case of spontaneous aspergillus spondylodiscitis with epidural abscess in a 45-year-old immunocompetent female. J Craniovertebr Junction Spine. 2013 Jul;4(2):82–4.
Jiang Z, Wang Y, Jiang Y, Xu Y, Meng B. Vertebral osteomyelitis and epidural abscess due to Aspergillus nidulans resulting in spinal cord compression: case report and literature review. J Int Med Res. 2013 Apr;41(2):502–10.
Coyle CM. Chapter 22 - schistosomiasis of the nervous system. In: Garcia HH, Tanowitz HB, Del Brutto OH, editors. Handbook of clinical neurology. Elsevier; 2013. p. 271–81.
Boissier J, Moné H, Mitta G, Bargues MD, Molyneux D, Mas-Coma S. Schistosomiasis reaches Europe. The Lancet Infectious Diseases. 2015 July 1;15(7):757–8.
Centers for Disease Control and Prevention. Neglected tropical diseases: the burden of schistosomiasis; 2011. Available at https://www.cdc.gov/globalhealth/ntd/diseases/schisto_burden.html. Accessed 18 Dec 2017
Jauréguiberry S, Paris L, Caumes E. Acute schistosomiasis, a diagnostic and therapeutic challenge. Clinical Microbiology and Infection. 2010 March 1;16(3):225–31.
Ferrari TCA, Moreira PRR, Cunha AS. Spinal cord schistosomiasis: a prospective study of 63 cases emphasizing clinical and therapeutic aspects. Journal of Clinical Neuroscience. 2004 April 1;11(3):246–53.
Pammenter MD, Haribhai HC, Epstein SR, Rossouw EJ, Bhigjee AI, Bill PLA. The value of immunological approaches to the diagnosis of schistosomal myelopathy. The American Journal of Tropical Medicine and Hygiene. 1991 March 01;44(3):329–35.
Bruscky IS, de Melo FL, de Medeiros ZM, Albuquerque FF, Wanderley LB, da Cunha-Correia C. Nested polymerase chain reaction in cerebrospinal fluid for diagnosing spinal cord schistosomiasis: a promising method. J Neurol Sci. 2016 Jul 15;366:87–90.
Silva LCS, Maciel PE, Ribas JGR, Souza-Pereira SR, Antunes CM, Lambertucci JR. Treatment of schistosomal myeloradiculopathy with praziquantel and corticosteroids and evaluation by magnetic resonance imaging: a longitudinal study. Clin Infect Dis. 2004 Dec 01;39(11):1618–24.
Alsomaili M, Abulaban AA. Spinal cord schistosomiasis: two different outcomes. Case Reports in Neurology. 2016 Jan;8(1):47–52.
Gripper LB, Welburn SC. Neurocysticercosis infection and disease – a review. Acta Trop. 2017 Feb;166:218–24.
Webb CM, White AC. Update on the diagnosis and management of neurocysticercosis. Curr Infect Dis Rep. 2016 Dec;18(12):44.
Schantz PM, Moore AC, Muñoz JL, Hartman BJ, Schaefer JA, Aron AM, et al. Neurocysticercosis in an orthodox Jewish community in New York City. N Engl J Med. 1992 Sep 03;327(10):692–5.
Ndimubanzi PC, Carabin H, Budke CM, Nguyen H, Qian Y, Rainwater E, et al. A systematic review of the frequency of neurocyticercosis with a focus on people with epilepsy. PLoS Negl Trop Dis. 2010 Nov 02;4(11):e870.
Canelas HM, Ricciardi-Cruz O, Escalante AD. Cysticercosis of the nervous system: less frequent clinical forms III, spinal cord forms. Arq Neuropsiquiatr. 1963 Jun;21:77–86.
Callacondo D, Garcia HH, Gonzales I, Escalante D, Nash TE. High frequency of spinal involvement in patients with basal subarachnoid neurocysticercosis. Neurology. 2012 May 01;78(18):1394–400.
Datta SGS, Mehta R, Macha S, Tripathi S. Primary spinal intramedullary neurocysticercosis: a report of 3 cases. World Neurosurg. 2017 Sep;105:1037.e7.
Jongwutiwes U, Yanagida T, Ito A, Kline SE. Isolated intradural-extramedullary spinal cysticercosis: a case report. J Travel Med. 2011 July 01;18(4):284–7.
Salazar Noguera EM, Pineda Sic R, Escoto SF. Intramedullary spinal cord neurocysticercosis presenting as Brown-Séquard syndrome. BMC Neurol. 2015 Jan 16;15:1.
Pal A, Biswas C, Ghosh TR, Deb P. A rare case of recurrence of primary spinal neurocysticercosis mimicking an arachnoid cyst. Asian J Neurosurg. 2017 Apr–Jun;12(2):250–2.
Del Brutto OH, Nash TE, White AC, Rajshekhar V, Wilkins PP, Singh G, et al. Revised diagnostic criteria for neurocysticercosis. J Neurol Sci. 2017 Jan 15, 372:202–10.
Bansal S, Suri A, Sharma MC, Kakkar A. Isolated lumbar intradural extra medullary spinal cysticercosis simulating tarlov cyst. Asian J Neurosurg. 2017 Apr–Jun;12(2):279–82.
dos Reis JB, Bei A, Reis-Filho JB, Nasser J. Cerebrospinal fluid in cysticercosis of the brain. Arq Neuropsiquiatr. 1979 Jun;37(2):113–26.
García HH, Evans CAW, Nash TE, Takayanagui OM, White AC, Botero D, et al. Current Consensus Guidelines for Treatment of Neurocysticercosis. Clin Microbiol Rev. 2002 Oct 01;15(4):747–56.
Agrawal SR, Singh V, Ingale S, Jain AP. Toxoplasmosis of spinal cord in acquired immunodeficiency syndrome patient presenting as paraparesis: a rare entity. J Glob Infect Dis. 2014 Oct;6(4):178–81.
García-García C, Castillo-Álvarez F, Azcona-Gutiérrez JM, Herraiz MJ, Ibarra V, Oteo JA. Spinal cord toxoplasmosis in human immunodeficiency virus infection/acquired immunodeficiency syndrome. Infect Dis (Lond). 2015 May;47(5):277–82.
Pérez-Lazo G, Castillo-Córdova R, Maquera-Afaray J. Intramedullary toxoplasmosis in HIV-tuberculosis co-infected patient. Rev Chil Infectol. 2017 Feb;34(1):77–80.
Sridharan S, Jagan Narayana GS, Chidambaram K, Jayachandiran AP. Primary Paraspinal Hydatidosis causing acute paraplegia. J Neurosci Rural Pract. 2017 Jul–Sep;8(3):472–4.
Gennari A, Almairac F, Litrico S, Albert C, Marty P, Paquis P. Spinal cord compression due to a primary vertebral hydatid disease: a rare case report in metropolitan France and a literature review. Neurochirurgie. 2016 Aug;62(4):226–8.
Celik C, Sasmaz MF, Oktay F, Ucan H, Kaptanoglu E. Paraplegia associated with spinal hydatid cyst: a case report. Spine. 2010 Apr 20;35(9):356.
Kalkan E, Cengiz SL, Ciçek O, Erdi F, Baysefer A. Primary spinal intradural extramedullary hydatid cyst in a child. J Spinal Cord Med. 2007;30(3):297–300.
Prabhakar MM, Acharya AJ, Modi DR, Jadav B. Spinal hydatid disease: a case series. J Spinal Cord Med. 2005;28(5):426–31.
Osoegawa M, Matsumoto S, Ochi H, Yamasaki K, Horiuchi I, Kira YO, et al. Localised myelitis caused by visceral larva migrans due to Ascaris suum masquerading as an isolated spinal cord tumour. J Neurol Neurosurg Psychiatry. 2001 Feb;70(2):265–6.
Yoshida S, Matsui M, Wang H, Oeda T, Sasaki T, Komure O, et al. A case of myeloradiculitis as a complication of visceral larva migrans due to Ascaris suum. Rinsho Shinkeigaku. 2004 Mar;44(3):198–202.
Umehara F, Ookatsu H, Hayashi D, Uchida A, Douchi Y, Kawabata H, et al. MRI studies of spinal visceral larva migrans syndrome. J Neurol Sci. 2006 Nov 01;249(1):7–12.
Awad A, Stuve O. Idiopathic transverse myelitis and neuromyelitis optica: clinical profiles. Pathophysiology and Therapeutic Choices Current Neuropharmacology. 2011 Sep;9(3):417–28.
Yeshokumar AK, Waubant E. Pediatric demyelinating diseases of the central nervous system and their mimics. 1st ed. Springer; 2017.
Williams T, Thorpe J. Post-infective transverse myelitis following Streptococcus pneumoniae meningitis with radiological features of acute disseminated encephalomyelitis: a case report. J Med Case Rep. 2012 Sep 19;6:313.
Candler PM, Dale RC. Three cases of central nervous system complications associated with mycoplasma pneumoniae. Pediatr Neurol. 2004 Aug;31(2):133–8.
Harzheim M, Schlegel U, Urbach H, Klockgether T, Schmidt S. Discriminatory features of acute transverse myelitis: a retrospective analysis of 45 patients. J Neurol Sci. 2004 Feb 15;217(2):217–23.
Jeffery DR, Mandler RN, Davis LE. Transverse myelitis. Retrospective analysis of 33 cases, with differentiation of cases associated with multiple sclerosis and parainfectious events. Arch Neurol. 1993 May;50(5):532–5.
Krishnan C, Kaplin AI, Deshpande DM, Pardo CA, Kerr DA. Transverse Myelitis: pathogenesis, diagnosis and treatment. Front Biosci. 2004 May 01;9:1483–99.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Murphy, O.C., Venkatesan, A. (2022). Infectious Myelopathies. In: Greenberg, B. (eds) Myelopathy. Springer, Cham. https://doi.org/10.1007/978-3-030-99906-3_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-99906-3_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-99905-6
Online ISBN: 978-3-030-99906-3
eBook Packages: MedicineMedicine (R0)