
Abstract
Oral health is fundamental to people’s overall health and well-being, including adolescents. Though preventable, globally, oral diseases pose a major health burden with substantial social and economic implications. This chapter focuses on the distribution/prevalence of common oral problems such as dental caries, dental traumatic injuries, fluorosis, periodontal diseases, and soft tissue lesions among adolescents in the MENA countries.
The world’s Middle-Income Countries (MICs) are a diverse group by size, population, and income level. They are defined as lower middle-income economies (such as Egypt Arab Republic, Morocco & Tunisia those with a gross national income (GNI) per capita between $1036 and $4045; and upper middle-income economies (such as Jordan, Iraq, and Libya) – those with a GNI per capita between $4046 and $12,535 (World Bank Country and Lending Groups: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Introduction
Globally, around 1.2 billion people are aged 10–19 years, totaling 16% of the world population of which 75 million live in the Middle East and North Africa (MENA) (UNICEF 2019). According to the life course approach to health—which advocates for starting disease prevention at early-life stages through to adulthood (Jacob et al. 2017)—adolescence is considered a sensitive period of rapid development, experimentation, and choice-making during which adolescents establish certain behavioral patterns. Adopting unhealthy behaviors such as poor diet and high sugar intake, alcohol consumption, substance use, smoking, and the use of smokeless tobacco during this phase might contribute to lifetime detrimental health consequences in adulthood and even jeopardize the health of the next generations (WHO 2018). Most of those health-comprising behaviors are common risk factors between oral diseases and other chronic conditions such as obesity, diabetes, cardiac problems, and some cancers (Sheiham and Watt 2000). Though, in general, oral health is considered a reliable indicator of an individual’s overall health and well-being, minimal attention is paid to promoting adolescents’ oral health in both practice and policy (Percy 2008). As a consequence, globally, the prevalence of unmet dental needs is quite high in this age group, with highest rates in the Eastern Mediterranean region (84.2%) and Africa (78.0%) (Ghafari et al. 2019). At least three out of every ten adolescents between 13 and 18 years experience dental pain at some point in life.(Pentapati et al. 2020). Moreover, of all health services, oral care is usually the most commonly unmet health need among children and adolescents with special healthcare needs (SHCN) (Lewis 2009). Access to dental care usually poses a challenge for people with SHCN due to the inability to afford treatment costs or difficulty finding a dental practitioner who is willing and capable to treat this population (Norwood and Slayton 2013).
2 Methodology
A comprehensive literature review was conducted to explore the common oral health problems in adolescence and their prevalence in the MENA region. Two electronic databases—Web of Science and Embase —were searched, and only English articles were assessed. The review included research studies based in countries in the MENA region, particularly in the last 5 years (2015–2020). Editorials and commentaries were excluded.
The search strategy included the following combination of controlled vocabulary and keywords: [Adolescen* OR teen* OR preteen* OR “high school students” OR Underage] AND [“Oral health” OR “dental health” OR “dental disease” OR “oral disease” OR dental caries OR “DMFS” OR “DMFT” OR “defs” OR “deft” OR “Cast index” OR“ICDAS” OR “periodontitis” OR “periodontal index” OR “periodontal pockets” OR gingivitis OR “gingival index” OR “dental plaque” OR “oral hygiene” OR “dental hygiene” OR flossing OR toothbrushing OR “orthodontic needs” OR “oral lesions” OR “Oral cancer” OR “dental trauma” OR “oro-facial trauma” OR “oral habits” OR “dental fluorosis” OR “dental neglect” OR “dental needs” OR “dental pain” OR “oral pain”].
All the references were imported to EndNote, and duplicates were identified by EndNote and subsequently removed. Titles and abstracts of all entries were analyzed by two reviewers, and only full texts of relevant references were retrieved and reevaluated. Additionally, the Global Burden of Disease (GBD) 2017 dataset was used to generate epidemiologic data on oral conditions among adolescents and youth in the MENA region. In order to acquire data relevant to adolescence and teenage, only the 10–14 and 15–19 age groups were selected. Graphs depicting disease frequencies were developed using the GBD Results Tool.
3 Findings
3.1 Common Oral Health Risks in Adolescents
3.1.1 Dental Caries
Adolescence marks a period of increased activity of dental caries (tooth decay) due to the immaturity of the recently erupted permanent teeth, increased intake of sugary diet and beverages, and lack of attention to oral hygiene practices in this age group (“Adolescent Oral Health Care” 2017). When left untreated, carious lesions lead to pain and infection, which could impair the child/adolescent’s ability to eat and sleep, thus resulting in poor growth and development. Tooth decay has been strongly associated with school absenteeism and low academic performance in adolescents, and parents have reported experiencing distress and sense of guilt, work absenteeism, and financial hardships due to their children’s poor oral health conditions. In some instances, owing to the increased esthetic desire and awareness in this age group, when multiple front teeth are involved, adolescents might refrain from smiling or interacting with others due to compromised esthetics, which in turn reduce their self-esteem and impair their social relationships (“Adolescent Oral Health Care” 2017).
Though preventable, globally, the burden of dental caries is still high and varies considerably both between and within countries. Middle-income countries (MICs)* have the highest burden of dental caries among 12-year-old adolescents, two thirds of which are left untreated. Even in high-income countries, more than half of tooth decay, in this age group, is not managed (FDI World Dental Federation 2015), which unveils the high rates of unmet dental needs in adolescence worldwide.
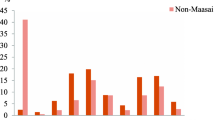
In the MENA region, however, data sources on trends in dental caries in adolescence per se are limited in most countries. One national study in Kuwait reported a 14% prevalence of caries among 12-year-olds (Alqaderi et al. 2016), while according to Egypt’s 2013–2014 national oral health survey, around 70% of both children and adolescents aged 4–18 years experienced some form of tooth decay (WHO.EMRO 2014). In Saudi Arabia, the prevalence rates of dental caries in adolescents were determined at the province level and varied from over 90% in Jazan to 64.98% in the Riyadh region. (Al-Rafee et al. 2019; Aljanakh 2017; Alshahrani et al. 2018; Alzahrani 2018; Quadri et al. 2015). Figure 8.1 presents the prevalence rates of dental caries among adolescents aged 10–14 and 15–19 years in the MENA region in comparison with global statistics based on findings from the GBD study of 2017.

(a) Global prevalence of dental caries among adolescents aged 10–14 and 15–19 years (Source: Institute for Health Metrics Evaluation. Used with permission. All rights reserved). (b) Prevalence of dental caries among adolescents aged 10–14 and 15–19 years from the MENA. (Source: Institute for Health Metrics Evaluation. Used with permission. All rights reserved)
Noticeably, in the MENA countries, there has been a decline in the prevalence of dental caries among 10–14- and 15–19-year-olds. As revealed in Fig. 8.1, gender differences seem to be consistent at both global and regional levels, where female adolescents tend to be at higher risk to develop tooth decay than males in both age groups. On the other hand, unlike global data estimates, in the MENA countries, younger adolescents (10–14 years) in both genders had higher caries prevalence rates than those aged 15–19 years (Fig. 8.1).
3.1.2 Periodontal Diseases
Periodontal diseases refer collectively to a myriad of conditions that affect the gums, the supporting dental tissues, and/or the alveolar bone. Gingivitis (which is a chronic reversible inflammation of the gums) is a very common condition in adolescents. The prevalence of gingivitis in adolescents is higher than in adults and younger children (“Adolescent Oral Health Care” 2017), mostly due to hormonal fluctuations during puberty. Sex hormones might cause gingivitis through altering the composition of oral microflora, affecting fluid accumulation in the gingival tissues, or modifying the inflammatory response of the gingival tissues (“Adolescent Oral Health Care” 2017; Armitage 1986). Gingivitis in adolescents could also be secondary to mouth breathing, orthodontic therapy, pregnancy, smoking, or intake of certain drugs (“Adolescent Oral Health Care” 2017; Al-Ghutaimel et al. 2014).
Another advanced form of gum disease is periodontitis, a serious condition that affects the tooth-supporting tissues and the alveolar bone (FDI World Dental Federation 2015). All forms of periodontitis can occur during adolescence; however, aggressive (juvenile) periodontitis is more common during the circumpubertal period, while chronic periodontitis is only seen occasionally (Al-Ghutaimel et al. 2014; Armitage 1986).
Estimates of the frequency of gingival and periodontal problems among adolescents are available from very few countries in the MENA region. A nationally representative study of Kuwait, in 2016, revealed that 42.5% of 12-year-old Kuwaiti adolescents had gingivitis (Alqaderi et al. 2016), while in Saudi Arabia, the prevalence was as high as 65% in a nationally representative sample of high school-attending adolescents (AlGhamdi et al. 2020b). On the other hand, according to (AlGhamdi et al. 2020a), the prevalence of periodontitis among 15–19-year-olds in Saudi Arabia was 8.6%, while in one study in Benslimane Province in Morocco, it was found that 3.7% and 2.6% of adolescents aged 12–15 and 4.9% and 7% of adolescents aged 16–18 had aggressive and chronic periodontitis, respectively (Kissa et al. 2016).
Findings from the GBD data (up to 2017) have shown that significant variations exist between global and regional frequencies of periodontal diseases among adolescents (Fig. 8.2). This could be attributed to the paucity of up-to-date reliable evidence on disease burden in adolescence at the population level in most of the MENA countries. Another conspicuous difference between the MENA countries and the global data is the distinct gap in gender prevalence at the regional level.

(a) Global prevalence of periodontal diseases among 15–19-year-olds (Source: Institute for Health Metrics Evaluation. Used with permission. All rights reserved). (b) Prevalence of periodontal diseases among 15–19-year-olds in the MENA countries. (Source: Institute for Health Metrics Evaluation. Used with permission. All rights reserved)
As noticed in Fig. 8.2 male adolescents in the MENA countries have significantly higher burden of periodontal diseases which might possibly indicate common unhealthy practices such as smoking, khat chewing, or substance abuse.
3.1.3 Malocclusion
Malocclusion refers to any abnormal position of the teeth or jaws, which leads to impaired orofacial functions and in severe cases facial asymmetry. The condition is usually associated with a combination of genetic and environmental factors and requires orthodontic and/or surgical intervention. Though not considered a pathological disease, malocclusion is a common problem in adolescent populations, which when overlooked could lead to serious consequences.
Among adolescents from different cultural backgrounds, malocclusion is known to adversely affect their psychological well-being and lower their self-esteem due to compromised facial esthetics (Dimberg et al. 2015).
Aside from the speech difficulties, malalignment of teeth could also increase the risk of sustaining dental trauma, particularly when upper anterior (front) teeth are protruded (“Adolescent Oral Health Care” 2017). Owing to pain, loss of function, and poor esthetics, traumatic injuries could be distressing at the physical, psychological, and emotional levels (Lee and Divaris 2009). An abnormal teeth arrangement or relation could also be associated with temporomandibular joint affection (“Adolescent Oral Health Care” 2017).
Furthermore, crowded teeth, being more difficult to cleanse, are more prone to food accumulation and plaque retention, which in turn increases the risk of dental caries and gingivitis (Kolawole and Folayan 2019). Based on one recent systematic review, it was found that the prevalence of unmet orthodontic treatment needs among adolescents in the MENA countries is as high as 40.8% (Ghafari et al. 2019), which highlights the necessity of directing more attention toward ensuring equitable access to orthodontic care in this age group.
3.1.4 Orofacial Traumatic Injuries
Trauma to oral tissues could result in fracture, loss, or dislocation of teeth, bruises or laceration of the soft tissues, or fractures of the facial bones. Craniofacial trauma causes more than four million deaths worldwide, which is half of all the trauma-related deaths (FDI World Dental Federation 2015). Several risk factors for traumatic dental injuries among adolescents were identified including protrusion of anterior teeth, peer relationships, exposure to violence or abuse, as well as the socioeconomic level (Glendor 2009). Another prominent cause of oral injuries among adolescents is sports activities, during which they get exposed to facial injuries due to falls or collisions with other players or surfaces (“Adolescent Oral Health Care” 2017). Such injuries could have serious physical, psychosocial, and economic impacts on adolescents and their families.
Though teen years are a high-risk time for traumatic orofacial injuries, in the MENA region, only data on exposure of adolescents to serious injuries in general without reference to dental injuries is available. One study, however, in Jordan revealed that the prevalence of traumatic dental injuries was 14.6% among 12-year-old schoolchildren of Amman, indicating that one out of every seven adolescents has suffered from some form of dental trauma by the age of 12 (Rajab and Abu Al Huda 2019).
3.1.5 Dental Fluorosis
Fluoride is considered among the most commonly studied protective factors of dental decay, despite that excess amounts of fluoride (above 1.5 mg/L) uptake can be destructive to permanent dentition. Dental fluorosis usually manifests as whitish or brownish discoloration or (in its severe form) pitting of teeth surface(s). Such defects start to be visible as soon as the permanent teeth erupt during childhood and early adolescence. It is also noteworthy that dental fluorosis is not only an esthetic problem, but it also increases teeth liability to decay.
Excessive fluoride content in drinking water is one of the major causes of dental fluorosis in some countries of the MENA region. Fluoride concentrations exceeding 10 mg/L were reported in countries such as Oman and Yemen (Aldeghaither 2018). One study in Yemen reported that 30.8% of 14-year-old Yemeni adolescents suffered from dental fluorosis (Kadir and Al-Maqtari 2010), and according to a national oral health survey in the UAE, up to 61% of 12-year-olds and 53% of 15-year-olds, in some areas in the country , had some form of clinical dental fluorosis (El-Nadeef et al. 2009).
4 Discussion and Future Implications
Adolescents should be regarded as a separate, unique population with special oral healthcare needs that differ substantially from those of adults or younger children, taking into consideration the following factors: (i) the potentially higher liability during this age group to various oral diseases like tooth decay, gingivitis, and oral trauma; (ii) the suboptimal dietary habits of adolescents that are affected by many social and environmental factors; (iii) the likelihood of adolescents to engage in risky behaviors like smoking, drug abuse, or alcohol consumption, which reflects on their oral and general health; (iv) some conditions like orthodontic problems or congenitally missing teeth start to be discernable in this age; (v) adolescents have special psychological needs that can affect dental health both directly and indirectly; (vi) the higher demand for esthetics particularly among adolescent girls; (vii) tendency to seek dental treatment might be hindered by dental anxiety in this age group; and (viii) some adolescents are also commonly affected by some other coexisting conditions that might further affect their oral health such as pregnancy, eating disorders, or systemic diseases (“Adolescent Oral Health Care” 2017).
Despite that, in most countries of the MENA region, the oral health of adolescents is a neglected area of research and reliable, up-to-date data on frequency and severity of different oral conditions, the psychosocial attributes of oral diseases, and the prevalence of unmet dental care needs in this age group are still lacking. Furthermore, oral health needs among adolescents and youth with special healthcare needs such as Down’s syndrome, cerebral palsy, autistic disorder, and other genetic and hereditary disorders are not adequately studied in any of the region’s countries. The absence of a comprehensive data collection system and the inadequacy of local research on oral health outcomes in adolescence and teenage hinder policy-making and limit the development of effective public health responses to promote adolescents’ oral health at the country level.
Given the complex nature of oral health issues arising during adolescence, all regional countries need to develop a research agenda for surveillance of oral health outcomes and common health determinants influencing oral health-related quality of life in both early and late phases of adolescence. Addressing knowledge gaps in the identification of causal factors and management of oral diseases among adolescents at the country level and establishing national quality standards for the provision of oral health services in this age group are warranted. There is also a pressing need to engage the youth of diverse ages and social backgrounds, especially those who are most vulnerable such as youth with SHCNs, in advocacy programs, community assessment activities, and decision-making to secure the success of the policy-making process. Furthermore, non-dental healthcare providers should encourage and assist in the referral of adolescents for routine dental checkups and risk assessment.
References
Adolescent Oral Health Care, 2017. Pediatr. Dent. 39, 213–220.
Al-Ghutaimel, H., Riba, H., Al-Kahtani, S., Al-Duhaimi, S., 2014. Common periodontal diseases of children and adolescents. Int. J. Dent.
Al-Rafee, M.A., Al Shammery, A.R., Al Rumikan, A.S., Pani, S.C., 2019. A comparison of dental caries in urban and rural children of the Riyadh region of Saudi Arabia. Front. Public Heal.
Aldeghaither, 2018. Fluoride in the Greater Middle East and Its Source: A Literature Review.
AlGhamdi, A., Almarghlani, A., Alyafi, R., Ibraheem, W., Assaggaf, M., Howait, M., Alsofi, L., Banjar, A., Al-Zahrani, M., Kayal, R., 2020a. Prevalence of periodontitis in high school children in Saudi Arabia: a national study. Ann. Saudi Med.
AlGhamdi, A., Almarghlani, A., Alyafi, R., Kayal, R., Al- Zahrani, M., 2020b. Gingival health and oral hygiene practices among high school children in Saudi Arabia. Ann. Saudi Med.
Aljanakh, M., 2017. Prevalence and severity of dental caries among public school students aged 16-l8 in Hai’l, Kingdom of Saudi Arabia. Int. J. Health Sci. (Qassim). 11, 50–53.
Alqaderi, H., Tavares, M., Hartman, M., Goodson, J.M., 2016. Effect of sleep and salivary glucose on gingivitis in children. J. Dent. Res.
Alshahrani, I., Tikare, S., Meer, Z., Mustafa, A., Abdulwahab, M., Sadatullah, S., 2018. Prevalence of dental caries among male students aged 15–17 years in southern Asir, Saudi Arabia. Saudi Dent. J.
Alzahrani, A.A., 2018. The Oral Health Status and Attitudes of Saudi Adolescent Male Students in Albaha Province: A Cross-Sectional Study. Adv. Dent. Oral Heal.
Armitage, G.C., 1986. Periodontal diseases of children and adolescents. CDA J. 14, 57–61.
Dimberg, L., Arnrup, K., Bondemark, L., 2015. The impact of malocclusion on the quality of life among children and adolescents: A systematic review of quantitative studies. Eur. J. Orthod.
El-Nadeef, M.A.I., Al Hussani, E., Hassab, H., Arab, I.A., 2009. National survey of the oral health of 12- and 15-year-old schoolchildren in the United Arab Emirates. East. Mediterr. Heal. J.
FDI World Dental Federation., 2015. The Challenge of Oral Disease–A Call for Global Action. The Oral Health Atlas, 2nd edition.
Ghafari, M., Bahadivand-Chegini, S., Nadi, T., Doosti-Irani, A., 2019. The global prevalence of dental healthcare needs and unmet dental needs among adolescents: a systematic review and meta-analysis. Epidemiol. Health.
Glendor, U., 2009. Aetiology and risk factors related to traumatic dental injuries - A review of the literature. Dent. Traumatol.
Jacob, C.M., Baird, J., Barker, M., Cooper, C., Hanson, M., 2017. The Importance of a Life Course Approach to Health: Chronic Disease Risk from Preconception through Adolescence and Adulthood, Who Report.
Kadir, R.A., Al-Maqtari, R.A.S., 2010. Endemic fluorosis among 14-Year-old Yemeni adolescents: An exploratory survey. Int. Dent. J.
Kissa, J., Chemlali, S., El Houari, B., Amine, K., Khlil, N., Mikou, S., Nadifi, S., Albandar, J.M., 2016. Aggressive and chronic periodontitis in a population of Moroccan school students. J. Clin. Periodontol.
Kolawole, K.A., Folayan, M.O., 2019. Association between malocclusion, caries and oral hygiene in children 6 to 12 years old resident in suburban Nigeria. BMC Oral Health.
Lee, J.Y., Divaris, K., 2009. Hidden consequences of dental trauma: The social and psychological effects. In: Pediatric Dentistry.
Lewis, C.W., 2009. Dental Care and Children with Special Health Care Needs: A Population-Based Perspective. Acad. Pediatr.
Norwood, K.W., Slayton, R.L., 2013. Oral health care for children with developmental disabilities. Pediatrics.
Pentapati, K.C., Yeturu, S.K., Siddiq, H., 2020. Global and regional estimates of dental pain among children and adolescents—systematic review and meta-analysis. Eur. Arch. Paediatr. Dent.
Percy, M.S., 2008. Oral health of adolescents--it’s more than dental caries. MCN. Am. J. Matern. Child Nurs.
Quadri, F.A., Hendriyani, H., Pramono, A., Jafer, M., 2015. Knowledge, attitudes and practices of sweet food and beverage consumption and its association with dental caries among schoolchildren in Jazan, Saudi Arabia. East. Mediterr. Heal. J.
Rajab, L.D., Abu Al Huda, D., 2019. Impact of treated and untreated traumatic dental injuries on oral health-related quality of life among 12-year-old schoolchildren in Amman. Dent. Traumatol.
Sheiham, A., Watt, R.G., 2000. The Common Risk Factor Approach: A rational basis for promoting oral health. Community Dent. Oral Epidemiol.
UNICEF, 2019. Adolescents overview [WWW Document]. URL https://data.unicef.org/topic/adolescents/overview/
WHO.EMRO, 2014. Egypt releases results of epidemiological study on oral health status [WWW Document]. URL http://www.emro.who.int/egy/egypt-events/results-of-epidemiological-study-on-oral-health-status-released.html
WHO, 2018. Adolescents: health risks and solutions Factsheet [WWW Document]. URL https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Reflection Questions
Reflection Questions
-
How do adolescents’ oral health needs differ from those of younger children?
-
Why are oro-dental problems such as dental caries, gingival problems, and malocclusion highly prevalent among adolescents in the MENA region?
-
How can oral diseases impact social and psychological development of adolescents?
-
What actions need to be undertaken, at both national and regional levels, to promote adolescents’ oral health in the MENA countries?
-
How can promotion of adolescents’ oral health be an effective tool in reducing global burden of oral diseases?
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Abou El Fadl, R.K., Mousa, H.R.F. (2022). Oral Health of Adolescents in the MENA Region. In: Barakat, C., Dghaim, R., Al Anouti, F. (eds) Adolescent Health in the Middle East and North Africa. Global Perspectives on Health Geography. Springer, Cham. https://doi.org/10.1007/978-3-030-92107-1_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-92107-1_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-92106-4
Online ISBN: 978-3-030-92107-1
eBook Packages: Earth and Environmental ScienceEarth and Environmental Science (R0)