
Abstract
The minimally invasive procedures used by interventional neuroradiologists accomplish a wide variety of treatments designed to provide correct life-threatening conditions, such as haemorrhagic or ischemic stroke.
Endovascular treatment strategies of haemorrhagic intracranial aneurysms include coiling, balloon-assisted coiling, intrasaccular flow-disruptors, stent-assisted coiling, and flow-diverter devices.
Interventional neuroradiology allows also minimally invasive treatments of haemorrhagic stroke, which are due to an underlying vascular lesion such as arteriovenous malformations or dural arterio-venous fistulas. Embolization with acrylic glues or with non-adhesive embolic materials may be used for “target” embolization in the setting of intracerebral haemorrhage.
Finally, endovascular treatment of acute ischemic stroke is now the younger field of interventional neuroradiology. It is important to recognize that modern endovascular stroke therapy focuses on direct clot removal with mechanical devices and it represents the standard of care in cases of proximal large vessel occlusion of the anterior circulation.
In this chapter, we review the current practice on neuroendovascular therapy in acute phase and we discuss the main techniques used by interventional neuroradiologists.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Intracranial aneurysms
- Endovascular management
- Intervention
- Coil
- Flow diverter devices
- Brain arteriovenous malformations
- Dural arteriovenous fistulas
- Acute ischemic stroke
- Thrombectomy
1 Endovascular Treatment of Haemorrhagic Intracranial Aneurysms
1.1 Introduction
Non-traumatic subarachnoid haemorrhage (SAH) is an uncommon and severe subtype of stroke with high mortality and morbidity. The rupture of an intracranial aneurysm is the underlining cause in about 85% of cases (Mayer et al. 2002). The estimated incidence of SAH is around 9/100,000 people/year globally. It is a devastating event with a case fatality rate of 51% and a 50% rate of significant disability among survivors (Mayer et al. 2002).
Treatment is typically carried out urgently rather than emergently, usually within 24–72 h after the arrival of the patient to the hospital.
Therapy is influenced by the patient’s general and neurological conditions, as well as by the morphology and location of the aneurysm. Theoretically, all patients should undergo surgical obliteration of the aneurysm sac, but mortality is unacceptably high if the patient is in a stupor or coma (grade IV or V on the Hunt-Hess scale [HHS] or with low Glasgow Coma Scale [GCS]). So, before any therapeutic approach, it is advisable to evaluate the patient on the basis of the Hunt & Hess scale (Tables 1 and 2) and the Computed Tomography (CT) grading scale according to Fisher classification (Table 3).
Endovascular treatment of cerebral aneurysm has been revolutionized by ISAT (International Subarachnoid Aneurysm Trial) (Molyneux et al. 2005).
This multi-center randomized trial has compared microsurgical and endovascular techniques in the treatment of ruptured intracranial aneurysms.
Evaluation of the results at 1 year revealed a reduction in mortality and disability from 31% in the microsurgical arm to 24% in the endovascular arm. This difference was mainly linked to the decrease in the rate of disability among survivors treated intravascularly (16%) compared to patients treated with microsurgery (22%) (Molyneux et al. 2005).
However, the study showed a slightly higher re-bleeding rate in the case of aneurysms treated endovascularly (2.9%) compared to the clip approach (0.9%).
Later studies underlined the significant incidence of aneurysm recanalization after a time, with risk of greater re-rupture after coil embolization compared with surgical clipping (3.4% versus 1.3%) (Johnston et al. 2008).
In the setting of SAH, neuro-endovascular techniques include coiling (Pierot et al. 2008) and balloon-assisted coiling (BAC).
Stent-assisted coiling (SAC) (Muto et al. 2017; Shapiro et al. 2012) and new generation stents, such as Flow-Diverter Devices (FDD) (Lozupone et al. 2018), have been proposed in the setting of SAH in limited series. They have been mainly used in patients with more complex aneurysm morphologies, fusiform, dissecting, or blister aneurysms. Despite these results, intracranial stenting in the setting of SAH is an off-label treatment because of an increased haemorrhagic risk, due to the need of dual antiplatelet therapy.
There are four objectives for the endovascular occlusion of aneurysms: Block bleeding in progress; avoid re-bleeding; determine the exclusion of the aneurysm sac from the circle; guarantee the duration of the result over time.
1.2 Factors Influencing Endovascular Approach
Several factors influence endovascular treatment of intracranial aneurysms. They include aneurysm shape, size, location, and thrombus inside the sac.
1.2.1 Aneurysm Shape
Dome-to-neck ratio: if the neck is small compared to the maximum diameter of the bag, with a ratio of 1:3 or greater, the aneurysm is susceptible to the treatment with coils. In the event that the ratio is in the order of 1:1 or 1:2, it is necessary to resort to self-expanding devices, stents or balloons, able to create an artificial neck.
1.2.2 Aneurysm Size
Absolute dimensions of the aneurysm: large aneurysms (ø 15–25 mm) or giant (ø>25 mm) usually present with a wide collar that incorporates a large part of the circumference of the vessel wall.
1.2.3 Location
Location: it is very often the determining factor in the choice of the type of treatment; excluding the posterior circulation aneurysms, which are preferentially treated with an endovascular approach, some sites, such as especially the bifurcation from the middle cerebral or the aneurysms located at the level of the terminal branches, make this type of approach difficult.
1.2.4 Thrombus Inside The Sac
Presence of unstable thrombus inside the sac is not a contraindication to treatment with coils, but increases the risk of inter and peri-procedural thromboembolic phenomena; moreover, the presence of the thrombus, especially if large, could hinder the correct positioning of the coils inside the sac.
1.3 Endovascular Treatments and Techniques
All procedures are usually performed under general anaesthesia in the angiography suite. All patients received heparin (70 IU/kg) intravenous bolus after femoral puncture and continuous intravenous infusion throughout the procedure for a target activated clotting time of 250–300 s.
After single femoral puncture, a 6 F or 7 F guiding catheter is placed in the internal carotid artery or vertebral artery. Then a designed microcatheter is carefully navigated into the aneurysmal sac. The size and type of the coils were chosen according to measurement of the aneurysm width and height on three-dimensional gradient volume rendering reconstructions of rotational angiography in two orthogonal projections. Occlusion rate is commonly evaluated at the end of the procedure according to the modified Raymond-Roy occlusion classification (mRROC) (Table 4).
1.3.1 Coiling
These flexible, soft, detachable coils could be delivered through a microcatheter that could be safely navigated into the targeted aneurysm (Pierot et al. 2008). Complex-shaped, three-dimensional coils were developed to facilitate the embolization of wide-necked aneurysms. Coils with faster detachment times were developed to speed the process of embolization and shorten procedure times (Fig. 1). As aneurysm embolization with the Guglielmi Detachable Coil (GDC, Boston Scientific Corporation, Natick, MA) became increasingly accepted and more widely performed, competitors emerged, and additional brands of embolization coils became available.

(a) Endovascular treatment with coiling of a small ruptured anterior communicating artery aneurysm. (b) Under fluoroscopic roadmap, the microcatheter is positioned into the aneurysm sac. (c) Deployment of the coils (d) Complete embolization at the end of the procedure
1.3.2 Balloon-Assisted Coiling
Wide neck intracranial aneurysms represent a challenge. Aneurysms with a neck >4 mm could be difficult to treat with a non-assisted endovascular coiling. In fact, migration of heterologous material or the same coils into the vessel could cause local thrombosis and thromboembolism in the intracranial circulation.
For these reasons, balloon-assisted coiling, also known as remodeling technique, was introduced by J. Moret and his collaborators. This technique consists in inflating a thin balloon into the parent vase along the aneurysm neck, during the positioning and the subsequent detachment of the coils. The balloon’s aid takes into account the temporary remodeling of the wide-necked aneurysm during the release of the coils. This method requires the placement of a microcatheter with a non-detachable balloon in the artery at aneurysm origin along the aneurysm neck (Fig. 2). Another microcatheter is placed in the aneurysm sac. The balloon is inflated before releasing the coil and then, before the coil detachment, the balloon is gently deflated so that the stability of the mass of the coils can be evaluated. This procedure is repeated for each subsequent coil. The balloon serves three purposes during embolization: first, to stabilize the microcatheter into the aneurysm sac; second, to force the coil to assume the three-dimensional shape of the aneurysm; and third, to obtain haemostasis in case of intra-procedural rupture.

(a) Endovascular treatment with balloon-assisted coiling of a small ruptured carotid-cave aneurysm. (b) The balloon is temporary inflated during the coils’ deployment (c) Complete embolization at the end of the procedure
1.3.3 Stent-Assisted Coiling
The stent-assisted coiling is another endovascular technique used for the treatment of wide-necked aneurysms, as well as for the treatment of giant and dissecting aneurysms. The deployment of a stent at the aneurysm neck prevents the protrusion of the coils into the vessel and can help to prevent recurrence of the aneurysm (Shapiro et al. 2012) (Fig. 3).

(a) Endovascular treatment with stent-assisted coiling of a ruptured anterior communicating artery aneurysm. (b) A braided stent is deployed through the anterior communicating artery; then the sac is filled with coils
The first stent designed for the intracranial circle was made in Nitinol (an alloy of nickel and titanium that assumes a predetermined configuration under appropriate conditions). This flexible material allows the stent to reach the tortuous vessels of the intracranial circulation. The procedure consists in positioning the stent in the parent artery along the aneurysm neck; a microcatheter is then positioned through the stent struts into the aneurysm sac, and then the coils are deployed. Alternatively, the microcatheter can be jailed into the aneurysm sac, while the stent is deployed into the parent vessel, also known as “jailing technique”. With the possibility of having stents of various calibers and constructive characteristics (with open and closed cells, which can be recaptured and repositioned), interventional neuroradiologists have modified the technique, and with Y-stenting (Limbucci et al. 2016), all bifurcation aneurysms can be treated, allowing the reconstruction of the bifurcation.
Other newly developed devices, designed for the containment of the coils, are PulseRider® (Aguilar-Salinas et al. 2018) and pCONus® (Ulfert et al. 2018), which allow the treatment of large-bifurcation aneurysms without the need of deploying two intracranial stents.
The main drawback of this technique is the need of dual antiplatelet therapy, which represents a relative contraindication in the setting of SAH.
1.3.4 Intrasaccular Flow-Disruptors (WEB®)
The WEB® is a nitinol braided-wire intravascular device designed to disrupt blood flow at the aneurysmal neck.
This device has shown huge advantages in occluding difficult-to-treat aneurysms, such as wide-necked, and particularly for those located at bifurcation. These new devices consist in a high-attenuation micro-braided mesh constructed from a large number of nitinol wires (ranging from 19 to 38 μm) placed in the aneurysm sac to disrupt the intra-aneurysmal flow and create intra-aneurysmal thrombosis. Several studies have been focused on the treatment of unruptured cerebral aneurysms (Limbucci et al. 2018) (Fig. 4).

(a, b) A ruptured MCA trifurcation aneurysm; a bleb is highlighted on the superior portion of the sac. (c) Deployment of the WEB (d) Detachment of the WEB (e) Contrast stasis into the aneurysm sac (f) Complete occlusion of the aneurysm
However, some authors have demonstrated the safety of the WEB in the treatment of ruptured intracranial aneurysms (van Rooij et al. 2016).
Particularly, the unnecessity of antiaggregation, or adjunctive stents or balloons, makes this strategy a valuable alternative to coils in the treatment of acutely ruptured aneurysms.
1.3.5 Flow-Diverter Devices
FDD are new and important tools in the treatment of intracranial aneurysms (Briganti et al. 2014; Briganti et al. 2015; Briganti et al. 2017). They are able to form a high-coverage mesh that induces thrombosis of the aneurysmal sac, while preserving patency of the adjacent small vessels (Kallmes et al. 2007).
Although the available data for the FDD remain extremely encouraging, there remain several theoretical limitations of the device with respect to its application in the treatment of ruptured cerebral aneurysms.
First, as with any intracranial stent-like device, a course of dual-antiplatelet medications is required for prophylaxis against thrombosis, while the construct is becoming endothelialized and incorporated into the parent artery. The optimal duration of dual-antiplatelet therapy remains uncertain, but the current recommendation is for 6 months of aspirin with clopidogrel with aspirin alone thereafter (Briganti et al. 2016). For this reason, aneurysmal subarachnoid haemorrhage represents a relative contraindication to FDD placement, given the potential for complications related to the invasive procedures frequently required during the perioperative period in these patients (i.e. ventriculostomy catheters, percutaneous gastrostomy tubes, tracheostomies, etc.). Moreover, after FDD placement, without adjunctive coiling of the sac, the occlusion does not immediately occur and the patient is not theoretically protected by re-bleeding.
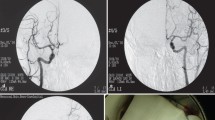
FDD are also used in ruptured aneurysms difficult to treat selectively either with the described endovascular techniques or with a microsurgical approach, such as very small aneurysms, blister-like aneurysms, dissecting aneurysms, or fusiform aneurysms (Zhu et al. 2018) (Figs. 5 and 6). However, it should be added that there are experiences of ruptured aneurysms treated with flow diverters in the acute phase, which demonstrate a rate of haemorrhagic complications not significantly different from that of other endovascular techniques and with a high percentage of complete occlusion at a distance.

(a) Ruptured dissecting aneurysm of the V4 segment of the vertebral artery. (b) Flow-diverter device deployment. (c) Contrast stasis at the end of the procedure. (d) 3-month angiography shows complete aneurysm occlusion

(a) A ruptured superior cerebellar artery aneurysm (b) Flow-diverter devices deployment into the basilar artery (c) Angiographic occlusion at 6 months
On the other side, some authors have proposed staged treatment of ruptured complex and giant intracranial aneurysms with coiling in the acute phase and FDD treatment following recovery from SAH (Brinjikji et al. 2016).
2 Endovascular Treatment of Haemorrhagic Intracranial Arteriovenous Malformations
2.1 Introduction
According to the National Stroke Association 2009 Fact Sheet, haemorrhagic stroke accounts for 13% of cases of acute stroke in the United States, with approximately 100,000 hospital admissions per year. Haemorrhagic stroke has a worse prognosis than ischemic stroke, with up to 50% 30-day mortality and very high rates of severe neurological disability among survivors (Qureshi et al. 2001).
There are two major types of haemorrhagic stroke: those that are due to an underlying vascular lesion such as a brain arteriovenous malformation (bAVM), aneurysm with intraparenchymal rupture, dural venous sinus (or cerebral vein) thrombosis (DVST), vasculitis, and Moya-Moya disease, which represent a minority of cases and are potentially treatable (secondary intracerebral haemorrhage); and those that are not due to an underlying vascular lesion (primary ICH).
The incidence of underlying vascular etiologies for an ICH varies significantly according to the patient’s clinical characteristics and noncontrast CT findings, with patient age being one of the most important variables. Indeed, in recent Computed Tomography Angiography (CTA) studies, the frequency of secondary ICH has ranged from 13% to 28% in patients older than 18 years (Gazzola et al. 2008) to 65% in patients of 40 years of age (Romero et al. 2009).
2.2 Brain Arteriovenous Malformations
A bAVM is an abnormal connection between arteries and veins with a characteristic nidus. In patients who present with a haemorrhage, the incidence of AVM re-bleeding is increased from 2–4%/year to 6–18%/year for at least a year following the initial haemorrhage.
The ideal treatment of a bAVM is complete obliteration of the lesion which removes the risk of further haemorrhage and reduces the seizure risk.
However, an alternative approach to cure is one where endovascular intervention is directed at specific angiographic target areas in an attempt to improve symptoms and reduce the associated morbidity.
As bAVM haemorrhage rate is significantly increased after a bleed, treatment of any weakness responsible for haemorrhage also offers an opportunity to lower this bleed rate to baseline or below (Sun et al. 2017).
Under general anaesthesia, a guiding catheter is commonly placed in the internal carotid artery or in the vertebral artery. Then a microcatheter is navigated in the nidus and a microangiography is usually performed.
The bleeding point is usually identified by looking for the presence of an intranidal or flow-related aneurysm. A flow-related aneurysm is defined as a saccular aneurysm in a vessel supplying the nidus, while an intranidal false aneurysm is identified as a defect with a smooth wall that was larger than the nidus channels with contrast often lingering within the defect.
In all of these case targets, endovascular embolization is usually performed (Fig. 7).

(a) Haemorrhagic cerebellar arteriovenous malformation fed by the right superior cerebellar artery. A pseudoaneurysm is highlighted on the feeders. (b) Microcatheterization of the feeder (c) Occlusion of the pseudoaneurysm with glue
Embolization with N-butyl cyanoacrylate (NBCA), i.e. acrylic glue, is faster in injection times and requires, with the same rates of occlusion, more access for session, and more sessions. Acrylic embolization is the first option in the case of high-flow arteriovenous fistulas within the nidus or in the case of deep feeders (lenticolostriate arteries) or functional “en passage” arteries. Flow-related aneurysm or intranidal aneurysm can be occluded also with coils or with the use of nonadhesive embolic agent like, Onyx® (Medtronic), Squid® (Emboflu), and Phil® (Microvention).
2.3 Dural Arteriovenous Fistulas (dAVF)
Intracranial dural arteriovenous fistulas (dAVF) are pathologic shunts between dural arteries and dural venous sinuses, meningeal veins, or cortical veins, which account for 10–15% of intracranial arteriovenous malformations (Kwon et al. 2005).
Intracranial DAVFs presenting with haemorrhage require early treatment aimed at complete and definitive fistula obliteration, considering the substantial risks of re-bleeding after the first haemorrhage (Duffau et al. 1999).
The choice of endovascular treatment depends on the angioarchitecture of each dAVF and, in this regard, each individual case requires a detailed angiographic study.
The general principle of endovascular treatment is the complete obliteration of the fistula drainage and the multiple arterial feeders.
The endovascular treatment should be realized by both arterial or venous routes using two types of liquid embolic agents: adhesive (NBCA) and not adhesive (Onyx®, Squid®, Phil®).
NBCA has been used as an adhesive embolic agent with relatively good results, but it requires quick and continuous injection technique to avoid catheter tip occlusion due to high thrombogenicity of the glue. The advent of new non-adhesive liquid embolic agent has changed the treatment strategy for DAVFs because of its greater safety and efficacy compared with NBCA in endovascular embolization (Sadeh-Gonike et al. 2018).
In the endovascular treatment, it is necessary to reach with the microcatheter a point as close as possible to the fistula (Fig. 8). The main target is the closure of the vein foot or the pathological tract of the dural sinus: a too proximal injection could not favour the penetration of the embolic agent at the fistula point, with the additional inconvenience to occlude the feeder, preventing any future treatments.

(a) MR of haemorrhagic dural arteriovenous fistula (DAVF) of the right occipital lobe. (b) The DAVF is fed by the transosseous branches of the right occipital artery and by posterior branch of the ipsilateral middle meningeal artery; the drainage occurs directly into an occipital vein (c, d) Occlusion of the fistula point with Onyx 18
The improvement of the microcatheters, however, has facilitated navigation of the meningeal vessels, almost always allowing a satisfactory injection point. A sure progress, in this sense, has been achieved with the introduction of detachable tip microcatheters, thanks to which an intermixed and prolonged injection technique of the chosen embolizing material could be implemented, avoiding the inconvenience of “gluing” of the distal end of the microcatheter, which force to leave the entire device in situ, cutting it at the level of the femoral access.
3 Endovascular Treatment of Acute Ischemic Stroke
3.1 Introduction
The efficacy of endovascular treatment in patients with acute ischemic stroke has been finally demonstrated in 2015 by 5 trials (ESCAPE, EXTEND-IA, SWIFT-PRIME, REVASCAT, and MR CLEAN) (Berkhemer et al. 2015; Campbell et al. 2016; Demchuk et al. 2014; Jovin et al. 2015; Saver et al. 2015), which have definitively established the usefulness of this type of reperfusion therapy after negative results obtained in previous published trial (MR RESCUE and SYNTHESIS) (Kidwell et al. 2013; Ciccone et al. 2013). The success of these studies is due not only to the use of new and more efficient endovascular devices, but also to the use of innovative neuroradiological techniques of computerized tomography (CT) and magnetic resonance (MR) between the inclusion and/or exclusion criteria: with the exception of MR CLEAN, in fact, in all the remaining trials, these advanced methods, represented above all by multi-phase CT angiography (multi-phase CT Angiography, mCTA), perfusion CT (CT Perfusion, CTP), and MR diffusion and perfusion, have been adopted instead of conventional CT scans without intravenous contrast medium and single-phase CTA in identifying patients for endovascular treatment. This approach has therefore shed new light on the strategies to be followed to achieve a more appropriate selection of patient candidates for endovascular therapy.
The importance of advanced neuroimaging in selecting for thrombectomy has been further demonstrated by two recent trials. In fact, according to the DAWN (Nogueira et al. 2018) (DWI or CTP Assessment with Clinical Mismatch in the Triage of Wake-Up and Late Presenting Strokes Undergoing Neurointervention with Trevo) and the DEFUSE 3 (Sheinberg et al. 2018) (Endovascular Therapy Following Imaging Evaluation for Ischaemic Stroke) trials, the therapeutic window has been extended up to 24 h in carefully selected patients.
3.2 Selection Criteria
Since endovascular intervention is indicated only in the cases of a primary intracranial artery occlusion, it is necessary to identify the patients to be investigated (Powers et al. 2018).
The selection is primarily made with reference to the clinical severity, according to National Institutes of Health Stroke Scale (NIHSS) clinical score.
Studies on the use of multimodal MR, which includes at least sequences in diffusion and perfusion and MR angiography (MRA), or multimodal CT, which includes perfusion study and CTA, however, have proved to be useful in defining the “salvable” brain tissue, particularly to better guide the indication to the endovascular intervention.
The use of multimodal imaging is particularly useful when the time interval from the onset of the symptoms is >4.5 h, when the endovascular treatment is performed at or above the time window, or when the stroke onset is unknown (stroke at the awakening).
The preliminary study before endovascular treatment with CTA or MRA can be very important in the planning of endovascular treatment. Careful evaluation of the angle between the aortic arch and the supra-aortic trunks and the caliber and tortuosity of the carotid artery, subclavian, and vertebral arteries make it possible to choose between a femoral or brachial/radial approach.
3.3 Endovascular Treatments and Techniques
All procedures are usually performed under conscious sedation in the angiography suite. No systemic heparinization is usually administered.
Femoral route is usually performed in almost cases.
The brachial/radial approach on the right should be considered in cases with marked tortuosity of the anonymous trunk (for vertebral and right internal carotid artery [ICA]) and with the origin of the left ICA from the anonymous trunk (for left ICA), while left brachial/radial approach in case of marked tortuosity of the left subclavian artery (for left vertebral artery).
Guiding catheters ranging from 6 to 9 Fr can be used depending on the caliber of carotid-vertebral arteries; it is important to obtain a stable position of the guiding catheter, trying not to block the flow if the catheterized artery supplies cerebral arteries or contribute to collateral circulation to the suffering brain region.
In the anterior circulation, it is possible to use an 8 F guiding catheter (or 9 in case of occlusion of the ICA at the origin) with a balloon to perform flow blockage and aspiration during the recovery of the stent-retriever in the ICA. It is advisable to use a coaxial system with a 5 Fr diagnostic intermediate catheter 125 cm long inside the 8 Fr catheter and 0.035 guide within the 5 Fr catheter.
3.3.1 Stent-retriever Thrombectomy
In the technique of thrombectomy with stent-retriever, the catheterization of the occluded artery is performed using the microwire. The occlusion point is passed with a “blind” navigation; in some cases, a wide loop at the microwire tip allows better recanalization of the vessel and reduces the engagement of collateral branches. Once the occlusion has been overcome, the microcatheter is advanced. This is followed by injection of the contrast medium from the microcatheter to confirm the position downstream of the occlusion.
Then a stent-retriever is deployed at the occlusion level; a control angiography is performed to verify the presence of the flow inside the stent-retriever. Then, the stent-retriever can be left in place for 5 min (Fig. 9).

(a) Embolic occlusion of the proximal M1 segment of the middle cerebral artery (MCA); (b) Deployment of a stent-retriever (c) After one thrombectomy attempt, complete flow restoration
It is advisable to remove the stent-retriever with flow block and in continuous aspiration, using a 60 cc syringe or an automatic pump; according to this technique, the balloon placed at the end of the guiding catheter is inflated by injection of contrast medium before starting the recovery of the stent-retriever which is slowly withdrawn together with the microcatheter, while the second operator carries out the aspiration of blood from the guiding catheter.
A variant of the stent-retriever retraction technique within the guiding catheter involves capture of the thrombus at the end of a large-caliber intermediate catheter, navigated in contact with the stent-retriever (Epic technique).
In cases where there is a significant vascular tortuosity, the vascular access is made by using an intermediate catheter of particular flexibility and softness that, if of appropriate caliber (5 or 6 Fr), allows the distal thromboaspiration during the concomitant maneuver of thrombectomy (Solumbra technique); in this case, thromboaspiration and stent-retriever work together (Fig. 10).

(a) Embolic occlusion of the proximal M1 segment of the middle cerebral artery (MCA); (b) Deployment of a stent-retriever into the M1-M2 segment of the MCA, while an aspiration catheter is placed in the M1, under continuous aspiration. (c) Complete flow restoration after the thrombectomy
3.3.2 Thromboaspiration
As an alternative to the technique with stent-retriever, it can also be used as a primary aspiration (ADAPT) with a 5 or 6 Fr catheter with a wide internal lumen (between 0.056 and 0.072 in.); this catheter must be taken immediately proximal to the thrombus using a microcatheter and microguide inside, keeping the system in continuous suction during the recovery maneuver.
This technique can also be used as a first intention (ADAPT), in some cases recanalizing the thrombectomy without using the stent-retriever (Fig. 11).

(a) Embolic occlusion of the mid-basilar artery. (b) An aspiration catheter is positioned in contact to the clot. (c) After one thromboaspiration maneuver, complete recanalization of the basilar artery
In 2017, ASTER trial compared efficacy and adverse events using the contact aspiration technique vs the standard stent-retriever technique as a first-line endovascular treatment for successful revascularization among patients with acute ischemic stroke and large vessel occlusion (Lapergue et al. 2017).
However, among patients with ischemic stroke in the anterior circulation undergoing thrombectomy, first-line thrombectomy with contact aspiration compared with stent-retriever did not result in an increased successful revascularization rate at the end of the procedure.
Extra-cranial carotid artery occlusion associated to intracranial occlusion (Tandem occlusion).
In case of carotid artery occlusion because of atherothrombotic or occlusive dissection (between 9% and 20% in the cases of the 5 recent trials), in most cases, after passing the occlusion by the 0.014 microwire, a stent is advanced and released at the cervical carotid occlusion, proceeding later to mechanical thrombectomy or thromboaspiration.
In the cases of stent-retriever use, it is necessary to pass the carotid stent with the guiding catheter (or with intermediate catheter 5 or 6 Fr with a large internal lumen) to prevent that stent-retriever get jailed with the carotid stent during the thrombectomy maneuver.
In the case of stent placement, antiaggregation therapy (double antiaggregation with clopidogrel loading, if the patient was not already on double antiaggregation therapy) is indicated even if fibrinolytic therapy is in progress or has just been completed.
4 Conclusion
The minimally invasive procedures used by interventional neuroradiologists accomplish a wide variety of treatments designed to provide correct life-threatening conditions, such as haemorrhagic or ischemic stroke. As alternatives to invasive surgery, these forms of therapy are often advantageous because they can lower the risk to patients, shorten hospital stays, and hasten recovery.
Some treatments, including emergency stroke care, are not feasible using an open surgery approach and can only be performed using a neurointervention procedure to increase patient outcomes.
Continuing improvement in imaging technology is also expected to enhance the therapeutic possibilities of this fascinating field.
Abbreviations
- bAVM:
-
Brain arteriovenous malformation
- CT:
-
Computed Tomography
- CTA:
-
Computed Tomography Angiography
- CTP:
-
CT Perfusion
- DVST:
-
Dural venous sinus thrombosis
- dAVF:
-
Dural arteriovenous fistulas
- FDD:
-
Flow-Diverter Devices
- GCS:
-
Glasgow Coma Scale
- GDC:
-
Guglielmi Detachable Coil
- HHS:
-
Hunt-Hess scale
- ICA:
-
Internal carotid artery
- ICH:
-
Intracerebral haemorrhage
- ISAT:
-
International Subarachnoid Aneurysm Trial
- MR:
-
Magnetic resonance
- MRA:
-
Magnetic Resonance angiography
- mRROC:
-
Modified Raymond-Roy occlusion classification
- mCTA:
-
Multi-phase CT angiography
- NIHSS:
-
National Institutes of Health Stroke Scale
- NBCA:
-
N-butyl cyanoacrylate
- SAH:
-
Subarachnoid haemorrhage
- SAC:
-
Stent-assisted coiling
References
Aguilar-Salinas P, Brasiliense LBC, Walter CM et al (2018) Current status of the PulseRider in the treatment of bifurcation aneurysms: a systematic review. World Neurosurg 115:288–294. https://doi.org/10.1016/j.wneu.2018.04.102. Epub 2018 Apr 24
Berkhemer OA, Fransen PS, Beumer D et al (2015) A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 372:11–20. [Erratum, N Engl J Med 2015;372:394]
Briganti F, Napoli M, Leone G et al (2014) Treatment of intracranial aneurysms by flow diverter devices: long term results from a single center. Eur J Radiol 83:1683–1690
Briganti F, Leone G, Marseglia M et al (2015) Endovascular treatment of cerebral aneurysms using flow-diverter devices: a systematic review. Neuroradiol J 28:365–375
Briganti F, Delehaye L, Leone G et al (2016) Flow diverter device for the treatment of small middle cerebral artery aneurysms. J Neurointerv Surg 8:287–294
Briganti F, Leone G, Ugga L et al (2017) Mid-term and long-term follow-up of intracranial aneurysms treated by the p64 flow modulation device: a multicenter experience. J Neurointerv Surg 9:70–76
Brinjikji W, Piano M, Fang S et al (2016) Treatment of ruptured complex and large/giant ruptured cerebral aneurysms by acute coiling followed by staged flow diversion. J Neurosurg 125:120–127
Campbell BC, Hill MD, Rubiera M et al (2016) Safety and efficacy of solitaire stent thrombectomy: individual patient data meta-analysis of randomized trials. Stroke 47:798–806. https://doi.org/10.1161/STROKEAHA.115.012360
Ciccone A, Valvassori L, Nichelatti M, SYNTHESIS Expansion Investigators et al (2013) Endovascular treatment for acute ischemic stroke. N Engl J Med 368:904–913
Demchuk AM, Goyal M, Menon BK et al (2014) ESCAPE Trial Investigators Endovascular treatment for Small Core and Anterior circulation Proximal occlusion with Emphasis on minimizing CT to recanalization times (ESCAPE) trial: methodology. Int J Stroke. https://doi.org/10.1111/ijs.12424
Duffau H, Lopes M, Janosevic V et al (1999) Early rebleeding from intracranial dural arteriovenous fistulas: report of 20 cases and re- view of the literature. J Neurosurg 90:78–84
Gazzola S, Aviv RI, Gladstone DJ et al (2008) Vascular and nonvascular mimics of the CT angiography “spot sign” in patients with secondary intracerebral hemorrhage. Stroke 39:1177–1183
Johnston SC, Dowd CF, Higashida RT, CARAT Investigators et al (2008) Predictors of rehemorrhage after treatment of ruptured intracranial aneurysms: the Cerebral Aneurysm Rerupture After Treatment (CARAT) study. Stroke 39:120–125. Epub 2007 Nov 29
Jovin TG, Chamorro A, Cobo E et al (2015) Thrombectomy within 8 hours after symptom onset in ischemic stroke. N Engl J Med 372:2296–2306. https://doi.org/10.1056/NEJMoa1503780
Kallmes D, Ding YH, Daying D et al (2007) A new endoluminal, flow-disrupting device for the treatment of saccular aneurysms. Stroke 38:2346–2352
Kidwell CS, Jahan R, Gornbein J, MR RESCUE Investigators et al (2013) A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med 368:914–923. https://doi.org/10.1056/NEJMoa1212793
Kwon BJ, Han MH, Kang HS et al (2005) MR imaging findings of intracranial dural arteriovenous fistulas: relations with venous drainage patterns. AJNR Am J Neuroradiol 26:2500–2507
Lapergue B, Blanc R, Gory B, ASTER Trial Investigators et al (2017) Effect of endovascular contact aspiration vs stent retriever on revascularization in patients with acute ischemic stroke and large vessel occlusion: the ASTER randomized clinical trial. JAMA 318:443–452. https://doi.org/10.1001/jama.2017.9644
Limbucci N, Renieri L, Nappini S et al (2016) Y-stent assisted coiling of bifurcation aneurysms with Enterprise stent: long-term follow-up. J Neurointerv Surg 8:158–162. https://doi.org/10.1136/neurintsurg-2014-011483
Limbucci N, Leone G, Rosi A et al (2018) Endovascular treatment of unruptured intracranial aneurysms by the woven EndoBridge device (WEB): are there any aspects influencing aneurysm occlusion? World Neurosurg 109:e183–e193. https://doi.org/10.1016/j.wneu.2017.09.136
Lozupone E, Piano M, Valvassori L et al (2018) Flow diverter devices in ruptured intracranial aneurysms: a single-center experience. J Neurosurg 128:1037–1043
Mayer SA, Kreiter KT, Copeland D et al (2002) Global and domain-specific cognitive impairment and outcome after subarachnoid hemorrhage. Neurology 59:1750–1758
Molyneux AJ, Kerr RS, Yu LM, International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group et al (2005) International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 366:809–817
Muto M, Giurazza F, Ambrosanio G et al (2017) Stent-assisted coiling in ruptured cerebral aneurysms: multi-center experience in acute phase. Radiol Med 122:43–52
Nogueira RG, Jadhav AP, Haussen DC, DAWN Trial Investigators et al (2018) Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med 378:11–21. https://doi.org/10.1056/NEJMoa1706442
Pierot L, Spelle L, Vitry F, for the ATENA investigators (2008) Immediate clinical outcome of patients harbouring unruptured intracranial aneurysms treated by endovascular approach: results of the ATENA trial. Stroke 39:2497–2504
Powers WJ, Rabinstein AA, Ackerson T, American Heart Association Stroke Council et al (2018) 2018 Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 49:e46–e110. https://doi.org/10.1161/STR.0000000000000158. Epub 2018 Jan 24. Review. Erratum in: Stroke. 2018;49:e138. Stroke. 2018 Apr 18
Qureshi AI, Tuhrim S, Broderick JP et al (2001) Spontaneous intracerebral hemorrhage. N Engl J Med 344:1450–1460
Romero JM, Artunduaga M, Forero NP et al (2009) Accuracy of CT angiography for the diagnosis of vascular abnormalities causing intraparenchymal hemorrhage in young patients. Emerg Radiol 16:195–201
Sadeh-Gonike U, Magand N, Armoiry X et al (2018) Transarterial onyx embolization of intracranial dural fistulas: a prospective cohort, systematic review, and meta-analysis. Neurosurgery 82:854–863
Saver JL, Goyal M, Bonafe A et al (2015) Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med 372(24):2285–2295. https://doi.org/10.1056/NEJMoa1415061
Shapiro M, Becske T, Sahlein D et al (2012) Stent-supported aneurysm coiling: a literature survey of treatment and follow-up. AJNR Am J Neuroradiol 33:159–163
Sheinberg DL, McCarthy DJ, Peterson EC, DEFUSE-3 Trial et al (2018) Reinforcing evidence for extended endovascular intervention time window for ischemic stroke. World Neurosurg 112:275–276. https://doi.org/10.1016/j.wneu.2018.02.064
Sun Y, Jin H, Li Y et al (2017) Target embolization of associated aneurysms in ruptured arteriovenous malformations. World Neurosurg 101:26–32. https://doi.org/10.1016/j.wneu.2017.01.081
Ulfert C, Pfaff J, Schönenberger S et al (2018) The pCONus device in treatment of wide-necked aneurysms: technical and midterm clinical and angiographic results. Clin Neuroradiol 28(1):47–54. https://doi.org/10.1007/s00062-016-0542-z
van Rooij WJ, Peluso JP, Bechan RS et al (2016) WEB treatment of ruptured intracranial aneurysms. AJNR Am J Neuroradiol 37:1679–1683. https://doi.org/10.3174/ajnr.A4811
Zhu D, Yan Y, Zhao P et al (2018) Safety and efficacy of flow diverter treatment for blood blister-like aneurysm: a systematic review and meta-analysis. World Neurosurg. https://doi.org/10.1016/j.wneu.2018.06.123. pii: S1878-8750(18)31339-1
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Briganti, F. et al. (2022). Basic Neuro-Interventional Therapeutic Approaches. In: Scaglione, M., Çalli, C., Muto, M., Wirth, S. (eds) Emergency Radiology of the Head and Spine. Medical Radiology(). Springer, Cham. https://doi.org/10.1007/978-3-030-91047-1_21
Download citation
DOI: https://doi.org/10.1007/978-3-030-91047-1_21
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-91046-4
Online ISBN: 978-3-030-91047-1
eBook Packages: MedicineMedicine (R0)