
Abstract
Puberty is marked by changes in the threshold of GnRH pulse generator, and the loss of inhibition leads to pulsatile release of GnRH, which in turn stimulates the pituitary to release FSH and LH. Delayed puberty can be defined as failure to demonstrate signs of pubertal maturation by an age that is ≥2 standard deviations above the population mean. There is a wide range of conditions that can present with a delay in puberty, making a systematic tapered approach fundamental to the diagnostic process. In considering a patient with delayed puberty, the most important initial assessment is the gonadotropin status. Disorders of pubertal delay can be broadly categorized into hypogonadotropic, hypergonadotropic, and eugonadotropic hypogonadism. The failure to develop puberty in a normal and timely fashion can, therefore, cause profound anxiety in individuals and families. Furthermore, awareness that pubertal delay can indicate significant underlying pathology compels physicians to investigate any perceived deviation from a rigidly defined acceptable pattern of development.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Delayed puberty
- Hypogonadotropic hypogonadism
- Eugonadotropic hypogonadism
- Hypergonadotropic hypogonadism
- Hypogonadism
- Constitutional delay
- Kallmann syndrome
- Klinefelter syndrome
- GnRH
Introduction
Puberty is an indelible period of metamorphosis of the human lifecycle, which culminates in sexual maturation and reproductive capability. The failure to develop in a normal and timely fashion can, therefore, cause profound anxiety in individuals and families. Furthermore, awareness that pubertal delay can indicate significant underlying pathology compels physicians to investigate any perceived deviation from a rigidly defined acceptable pattern of development. The ability to distinguish between various causes of delay and to differentiate significant underlying pathology from common benign delay can be daunting often requiring prudent investigation. Depending on the ultimate diagnosis, treatment options vary, but most patients can ultimately expect to achieve pubertal maturation and fertility.
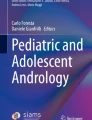
Puberty is initiated when the hypothalamic gonadotropin-releasing hormone (GnRH) pulse generator begins secreting brief nocturnal pulses of GnRH from the hypothalamic arcuate nucleus which subsequently stimulate the pituitary to release luteinizing hormone (LH) and follicle-stimulating hormone (FSH) [1]. Kisspeptin acts on the hypothalamic GnRH neurons, stimulating GnRH secretion [2]. The gonadotropins (LH and FSH) promote gonadal maturation, and gonads synthesize sex steroids, including testosterone and estrogen, and other proteins. LH acts on theca cells and interstitial cells to produce progestins and androgens which diffuse into adjacent granulosa cells. FSH acts on granulosa cells to stimulate aromatization of these androgens to estrogen. Estrogen and testosterone then promote pubertal changes throughout the body and provide negative feedback effect on the GnRH and gonadotropins (Fig. 17.1).

Schematic illustration of pubertal regulation
The first physical signs of puberty are typically breast development in girls and testicular enlargement in boys (testicular volume > 3 ml/ ≥ 2.5 cm in length). Some children, especially girls, have the appearance of pubic hair prior to the initiation of breast development, but in the absence of other puberty signs this usually represents adrenarche [adrenal source of androgens, independent of hypothalamic-pituitary-gonadal (HPG) axis maturation] and not true puberty. The trigger(s) for re-activation of the HPG axis is not completely understood, but modifying factors include general health, nutrition, genetic determinants, pubertal timing among primary relatives, endocrine-disrupting chemicals, and body mass index. Elevated body mass index (BMI) is often associated with delayed puberty in boys [3, 4]. Many of the genes involved in the HPG axis maturation are still unknown. Kisspeptin-1 and its cognate receptor (GPR54, a G protein-coupled receptor) are integral to the normal function of HPG axis and play critical role in the physiologic regulation of puberty [2, 5]. Kisspeptin is co-expressed with neurokinin B and dynorphin, and these signaling pathways are also important in physiologic regulation of puberty [6]. There is evidence that leptin, a 16 kDa hormone product of the Ob gene, synthesized by adipocytes, plays a permissive role [7, 8].
In delayed puberty, 16–40% of the population has loss of function mutation in the GnRH receptor. HS6ST1, FGFR1, KLB, and variants in several HH genes including GNRHR, TAC3, TACR3, IL17RD, and SEMA3A have been identified by whole exome sequencing; however, the exact pathogenicity of all these mutations is unknown [9,10,11,12]. Recently, in a Finnish family with delayed puberty, a gene of the immunoglobulin superfamily, IGSF10, has been described to cause delay by a defective neuroendocrine network of the GnRH pulse regulator [13].
Although the lower limit of normal for the onset of puberty is contestable, the average age for this process is generally accepted to be 9–10 years for girls and 10–11 years for boys [1, 14]. Delayed puberty can be defined as failure to demonstrate signs of pubertal maturation by an age that is ≥2 standard deviations above the population mean [1]. Delayed puberty is considered when there is lack of testicular enlargement by age 14 in males, lack of breast development by age 13 in females, absence of menarche by age 16 years in girls, or absence of menarche within 5 years of pubertal onset [15, 16]. Parenthetically, males present far more often for evaluation of delayed puberty, but it has been suggested that this is in part due to a referral bias [17, 18].
Key Points to the Diagnosis
There is a wide range of conditions that can present with a delay in puberty [17], which requires a systematic tapered approach fundamental to the diagnostic process. In considering a patient with delayed puberty, the most important initial assessment is the gonadotropin status. Disorders of pubertal delay can be broadly categorized into hypogonadotropic, hypergonadotropic, and eugonadotropic hypogonadism (Table 17.1).
Hypogonadotropic Hypogonadism (HH)
Hypogonadotropic hypogonadism (HH) is the commonest of the groups in both sexes and includes many pathologic disorders that can be further subdivided into constitutional delay of growth and puberty (CDGP), functional hypogonadotropic hypogonadism (FHH), and permanent hypogonadotropic hypogonadism (PHH). This classification can facilitate the diagnostic process by appropriately directing early evaluation efforts. HH is defined as lack of normal gonadal function secondary to low or absent gonadotropin secretion. In this case, the defect can be in the pituitary gland itself, or it can be related to hypothalamic dysfunction (delayed activation of the GnRH pulse generator). The delay in puberty can be either temporary or permanent. Isolated hypogonadotropic hypogonadism is diagnosed if there is no evidence of puberty by the age of 18 years [1].
Evaluation: In addition to low or absent LH/FSH, sex steroid concentrations will be in the pre-pubertal range, and bone age is typically delayed. Serum concentrations of adrenal androgens may be normal.
Constitutional Delay of Growth and Puberty (CDGP)
Constitutional delay of growth and puberty is the most common cause of delayed puberty, especially in males (65% of boys and 30% of girls with delayed puberty) [17]. It is a benign variant of normal growth and development and is, notably, a diagnosis of exclusion. Typically, a child will be normal size at birth and in infancy. At some point in early childhood, a decrease in growth velocity (GV) begets a decline in height centile for age. Normal growth then resumes with the child growing at an age-appropriate GV and at a consistent but low height percentile for age. This represents a global delay in biologic maturity affecting puberty and bone maturation. Height is usually appropriate for genetic potential when plotted for bone age. Often, there is a family history of “late bloomers” in the family history of delayed puberty in the patient’s parents or siblings (77%) [19]. Pedigree studies show that children with CDGP are mainly autosomal dominant with variable penetrance [20]. They exhibit a relatively normal pre-pubertal growth velocity and protracted pre-pubertal growth nadir. The discordance in height vs. peers is exacerbated by a relatively lower growth velocity compared to peers who are undergoing a pubertal growth spurt. The growth velocity and height, however, should remain normal for bone age and pubertal stage. After HPG axis maturation, secondary sexual characteristics appear in their natural sequence with normal secondary sexual characteristics development. In 93% of cases, spontaneous pubertal maturation occurs by 18 years and has an excellent height phenotype. In some cases, the constitutional delay of puberty superimposed on constitutional short stature and final height may be shorter than genetic potential [21].
Diagnosis of this common condition is ultimately a matter of watchful waiting with close monitoring of growth and development. However, judicious evaluation to rule out other conditions and support the likelihood of CDGP is important. Clustering of CDGP has been clearly established [17, 19], and the pericentromeric region of chromosome 2 harbors a gene predisposing to pubertal delay [19]. Growth charts, if available, should be reviewed to demonstrate typical CDGP pattern. In CDGP, both adrenarche and gonadal enlargement occur later than average. In isolated hypogonadotropic hypogonadism (IHH), there is dissociation of adrenarche and gonadarche, with adrenarche occurring at normal age [17, 22]. GV and serum somatomedin-c (IGF1) should be monitored and remain normal for pubertal status.
Evaluation: Patients can have low/normal serum gonadotropins and a delayed bone age. Even though gonadotropin-releasing hormone (GnRH) agonist stimulation testing is often ambiguous in differentiating CDGP and permanent HH [23], a positive response to GnRH agonist is suggestive of CDGP. To date, no single lab test or hormone stimulation protocol has the sensitivity and specificity to confirm this diagnosis. Response to sex steroid replacement therapy, which will often trigger activation of the HPG axis in CDGP but not permanent HH, may aid in the diagnosis. Baseline, morning testosterone concentration of ≥20 ng/dl suggests the appearance of pubertal signs within 12–15 months [24]. A very low basal serum FSH (<0.2 IU/L by ICMA and < 1.0 U/L by IFMA) infers permanent HH [25, 26]. Serum inhibin B (INHB) measurement will help to discriminate permanent HH from CDGP. INHB is produced by Sertoli cells upon FSH stimulation and is a reflection of Sertoli cell integrity [27]. A baseline INHB concentration of >35 pg/ml is highly suggestive of CDGP [27].
Functional Hypogonadotropic Hypogonadism (FHH)
Functional hypogonadotropic hypogonadism represents another form of temporary, reversible HH. It accounts for about 20% of children with delayed puberty [17]. Within this category is a broad range of pathology that highlights the complexity of the HPG axis and the diverse factors that must coordinate to initiate puberty. The most common diagnoses are related to chronic or underlying illnesses, such as hypothyroidism, cystic fibrosis, Crohn’s disease, inflammatory disorders that produce cytokines, immunosuppression seen in perinatally HIV-infected children, and chronic renal failure [17, 28, 29]. The mechanism of pubertal delay in the case of underlying illness is thought to be manifold, involving a combination of factors that include, but not limited to, undernutrition, stress, and medications such as corticosteroids resulting in abnormal gonadotropin secretion [28]. The implicated genetic variations are in genes that have been associated with idiopathic hypogonadotropic hypogonadism [30]. As aforementioned, a common cause of FHH is malnutrition, as seen in anorexia nervosa or intense exercise resulting in HPG dysfunction. The connection between weight, especially body fat mass and puberty, has been extensively studied [7, 31, 32]. On the other extreme, bulk training exercises, especially in sports like boxing and wrestling, may also lead to transient interruption in puberty.
Evaluation: A thorough and detailed history may disclose systemic complaints, eccentric eating habits, or an obsession with exercise and weight loss. Physical exam may be revealing at times: weight and BMI will typically be low for age, and erosion of dental enamel, lanugo hair, and callused knuckles may suggest eating disorders. Elevated sedimentation rate and/or other inflammatory markers may be detected. Further evaluation depends on general clinical picture.
Isolated Gonadotropin Deficiency
Isolated GnRH deficiency resulting in low or inappropriately normal gonadotropins and absent or incomplete puberty could be associated with abnormalities in craniofacial, skeletal, neurologic, renal, and olfactory systems. This could be due to molecular defects that alter the regulation of GnRH release, GnRH neurons, the action of GnRH or gonadotropins, or both GnRH and gonadotropins. Rare sequence variants (RSVs) in genes involved in GnRH neuronal migration (FGF8, FGFR1, KAL1, PROK2, PROKR2, and NELF), secretion (GNRH1, GPR54, TAC3, and TACR3), and receptivity (GNRHR) have been reported to contribute to GnRH deficiency in both men and women [33,34,35].
Kallmann syndrome (KS) is a well-known cause of gonadotropin deficiency due to abnormalities in the KAL1 gene and is inherited as X-linked dominant or autosomal recessive disorder [33, 36]. This condition is caused by abnormal migration of embryonic GnRH and olfactory neuronal cells to the hypothalamus, resulting in HH and anosmia or hyposmia.
FGFR1 mutations are autosomal dominant and are often associated with cleft lip/cleft palate, syndactyly, or skeletal abnormalities. Other cases of permanent isolated HH have historically been referred to as idiopathic HH (IHH). More recently, several genetic mutations have been reported in some of these cases.
Multiple GnRH receptor mutations causing GnRH insensitivity and G protein-coupled receptor 54 mutations causing impaired gonadotropin secretion have been identified [36]. At the time of puberty, the affected patients may have adrenarche – some pubic hair may be there, but little or no breast development or axillary hair and present with primary amenorrhea.
HH is reported in leptin deficiency and puberty can be induced by recombinant leptin [8]. HH has also been reported in DAX1 mutations. DAX1 is a nuclear receptor protein encoded by the NR0B1 and associated with X-linked congenital adrenal hypoplasia and HH, secondary to attenuated production of gonadotropins by the pituitary [37].
A reversible form of congenital GnRH deficiency also has been identified where the activation of the GnRH-gonadotropins axis is markedly delayed, yet the affected subject undergoes a sustained reversal of hypogonadotropism by the age of 18 [38].
A few neurological conditions are also known to be associated with delayed puberty. The 4H syndrome is caused by mutations in POLR3A/B and causes myelination defects (hypomyelination), hypodontia, and hypogonadotropic hypogonadism [39]. Gordon Holmes syndrome is associated with RNF216, OTUD4, and PNPLA6 mutations and presents as HH and ataxia [40]. A syndrome complex of polyneuropathy, endocrinopathies, and HH has been studied in children with DMXL2 mutation. Warburg Micro syndrome may be associated with ocular and neurodevelopmental issues and HH due to mutations in the RAB2GAP1 dysregulation of the RAB cycle.
Evaluation: In all cases of isolated HH, other pituitary hormones should be assessed to confirm that the defect is truly isolated to gonadotropin secretion. In KS there is often associated decreased olfaction, synkinesia (mirror movements), sensorineural deafness, unilateral renal agenesis, and pes cavus. Brain MRI with contrast imaging in cases of KS may show aplasia/hypoplasia of olfactory bulb and sulci. Some patients with isolated HH will have a positive family history, but most cases are sporadic. Genetic testing for associated mutations is possible, but frequently not diagnostic insofar as the majority of isolated HH is idiopathic, that is, not associated with identified genetic abnormalities [2]. It can be particularly challenging to differentiate between CD and isolated HH. Definitive diagnosis of GnRH deficiency cannot be established before 18 years.
Multiple Pituitary Hormone Deficiencies
Hypogonadotropic hypogonadism as part of a constellation of multiple pituitary hormone deficiencies (MPHDs) can occur in the setting of central nervous system (CNS) tumors (i.e., craniopharyngioma, germinoma, hypothalamic glioma, prolactinoma), non-tumoral lesions (i.e., histiocytosis, granuloma, hydrocephalus, vascular lesions, dermoid and epidermoid cysts), cerebral dysgenesis, CNS trauma or infection, and destructive medical therapies such as radiation therapy. Genetic mutations, including defects in transcription factors involved in pituitary formation such as PROP1, HESX1, LHX3 and LHX4, and SOX2, have also been incriminated [36].
In children, craniopharyngiomas are the predominant cause of permanent HH [17]. They are benign tumors that arise in the suprasellar region of the brain and may cause symptoms related to increased intracranial pressure and/or pituitary gland and optic nerve dysfunction [41]. Growth hormone deficiency is the most common endocrinologic disorder, but all pituitary hormones can be affected, and most adolescents presenting with these tumors will have delay in puberty [42]. Surgery and radiation therapy may further damage pituitary and hypothalamic function leading to permanent hormone deficiencies. Depending on dose and anatomical location, intracranial radiation therapy, in particular, causes irreversible damage to the hypothalamic-pituitary axis. It usually affects the hypothalamus to a greater extent than the pituitary gland; precocious puberty is more common than delayed puberty [43].
Septo-optic dysplasia (SOD) with midline cerebral dysgenesis can cause pubertal delay. It is characterized by congenital absence of the septum pellucidum, bilateral optic nerve hypoplasia, and hypopituitarism. There is significant variability in the severity of affected children but typically involves visual impairment and pituitary hormone deficiency with radiologic abnormalities of the septum pellucidum or corpus callosum. It is occasionally associated with HESX1 gene mutations [44]. The FGF8 mutation has been associated with Moebius syndrome and septo-optic dysplasia as well.
Histiocytosis X is a condition that usually presents with diabetes insipidus but may also present with multiple pituitary hormone abnormalities leading to pubertal delay.
Evaluation: In any case of MPHD, laboratory assessment of thyroid function, adrenal function, growth, and electrolyte balance is indicated. Physical exam should include a thorough neurologic examination. A careful history should include review of past or recent head trauma, CNS infection, or intracranial radiation therapy. A review of systems should be performed with particular attention to visual change, headache, vomiting, fever, polyuria, polydipsia, poor growth, and salt craving. In most cases of MPHD, brain and pituitary imaging is a requisite, and, if SOD is considered, an ophthalmologic exam is a requisite to evaluate optic nerves and vision. Genetic testing is not indicated in all patients, but for those with a family history of MPHD and specific radiographic findings, targeted testing for specific mutations may be indicated [45].
Genetic Syndromes
There are several congenital syndromes that have HH as one of the primary findings. The most well-known syndrome is Prader-Willi syndrome (PWS). It is caused by loss of imprinted genetic material from the paternally derived chromosome 15. In addition to HH, it is marked by neonatal hypotonia, feeding problems in infancy, obesity, hyperphagia, developmental delay, small hands/feet, and short stature. It is usually sporadic.
CHARGE syndrome is another common syndromic cause of HH [17]. This acronym stands for coloboma, heart defects, choanal atresia, impaired growth and development, genital hypoplasia, and ear abnormalities and/ or hearing loss.
Mutations in the CHD7 gene have recently been identified in approximately 2/3 of affected patients [46], and it has been suggested that the developmental abnormality causing HH in this condition may be similar to that seen in KS [47]. It can be an autosomal dominant mutation, but most cases are sporadic. Bardet-Biedl syndrome also includes HH as a primary feature. Other manifestations of this rare, autosomal recessive condition include rod-cone dystrophy, obesity, renal dysfunction, developmental delay, and postaxial polydactyly. Rud syndrome is also characterized by ichthyosis, HH, and epilepsy. Alstrom syndrome, associated with cardiomyopathy and cone rod abnormalities, and Bloom syndrome are other syndromes associated with HH.
The presence of other dysmorphic characteristics associated with a syndrome in addition to HH warrants further evaluation. For PWS, genetic testing, preferably with DNA-based methylation testing [48]. CHARGE and Bardet-Biedl syndromes are both diagnosed clinically. CHARGE syndrome diagnosis is based on major and minor criteria, but genetic testing for CHD7 mutation is available. Similarly, there is genetic testing for 14 associated genetic mutations for Bardet-Biedl, but the diagnosis is based on the presence of primary and secondary phenotypic features [49].
Hypergonadotropic Hypogonadism (HHG)
Hypergonadotropic hypogonadism (HHG) causes delayed puberty due to primary gonadal failure. By definition, these disorders have elevated levels of gonadotropins without concomitant increase in sex steroid concentrations and without signs of pubertal maturation. Within this category lie primarily disorders of gonadal dysgenesis and gonadal injury.
Gonadal Dysgenesis
Gonadal dysgenesis is the most common cause of hypergonadotropic hypogonadism in children [17]. It is usually related to chromosomal abnormalities, and hence chromosomal analysis is fundamental in the evaluation of children with HHG. In females, Turner’s syndrome (TS) is a condition of X-monosomy (45, X) or structural abnormalities of an X chromosome. Mosaicism is common (50% may have 45X/mosaic karyotype). Girls have short stature and lack of normal pubertal development secondary to streak ovaries and premature ovarian failure. The degree of pubertal maturation is variable with occasional spontaneous menarche and rare fertility [50]. Other characteristics include heart and renal abnormalities, webbed neck, and broad chest. Mixed gonadal dysgenesis (MGD) can also occur similarly with X-monosomy/XY mosaicism. This protean genetic disorder can range in phenotypic presentation depending on degree of mosaicism, from phenotypic female to phenotypic male.
Klinefelter syndrome is a chromosomal abnormality found in males presenting with delayed puberty. In this case the underlying karyotype is 47-XXY. Along with HHG, this condition is characterized by tall stature; gynecomastia; small, firm, fibrotic testes; decreased upper to lower segment body ratio; and learning disabilities. Klinefelter is typically characterized by declining inhibin B and AMH levels due to Sertoli cell dysfunction. Other less prevalent disorders of gonadal dysgenesis in 46XY karyotype are Swyer syndrome (46XY, streak gonads), Drash syndrome, Frasier syndrome, mutations of SOX-9, DAX1 with duplication of Xp21, and mutations in the SF1 [16]. 46,XX males, who may be SRY positive or negative, can present with hypergonadotropic hypogonadism, small testes, and normal-appearing external genitalia at birth.
Disorders of Sex Development
Certain disorders of sex development can present as hypergonadotropic hypogonadism. For example, children with AIS or 5-alpha reductase deficiency (5-ARD) are genetically XY but are often raised female because of ambiguous or female external genitalia. They may present with pubertal delay or primary amenorrhea when there is a failure to progress through normal female puberty.
Rare cases of gonadotropin receptor mutations (LH/FSH receptor mutation in XX females) with normal breast development, primary or secondary amenorrhea, elevated serum LH/ FSH [depending on mutation of LH/FSH receptor], low estradiol level, and infertility have been reported. LH receptor mutation (homozygous or compound heterozygous inactivating mutations of the LH receptor) in XY males presents with male pseudohermaphroditism – female external genitalia/micropenis, absence of Müllerian structures, Leydig cell hypoplasia, lack of breast development, or hypergonadotropic hypogonadism [15, 51, 52].
FSH-β subunit gene mutation presents with delayed puberty, primary amenorrhea, elevated LH, and low or undetectable FSH [53, 54]. FSH receptor mutation presents with primary gonadal failure and HHG in females [53]. FSH is required for follicular development and ovarian androgen and estrogen synthesis in females. Males present with oligospermia but are fertile as FSH is not necessary for spermatogenesis [54].
Recently, mutations in the HAX1 gene have been implicated as important in gonadal development and may present as premature ovarian failure in girls.
Gonadal Injury or Loss
Hypergonadotropic hypogonadism also occurs in children who have suffered gonadal damage. Some causes are iatrogenic (i.e., surgery, radiation, chemotherapy), environmental factors, viral infections, metabolic and autoimmune diseases, and genetic alterations. Gonadal tissue is particularly sensitive to radiation damage but can also be affected by many chemotherapeutic agents [17]. Testicular tissue is more sensitive to damage by these cytotoxic therapies compared to ovarian tissue, and in all cases the risk is agent and dose dependent [55].
Gonadal tissue can also be injured by a wide spectrum of other processes, including trauma, infarction, and infection. In addition, certain disease processes can affect gonadal tissue and lead to pubertal dysfunction and infertility. Autoimmune polyendocrine syndrome type 1 (APS 1), for example, is associated with autoimmune-induced damage to gonadal tissue. Gonadal failure is much more common in females with this disorder, and there is correlation between SCC autoantibodies and ovarian failure in women with APS1 [56]. Galactosemia is also associated with HHG in female patients, especially those for whom treatment was delayed. It is thought that this is caused by cellular galactose toxicity occurring very early in life [57].
Complete loss of gonadal tissue can also present with delayed puberty. There are several indications for gonadectomy in the prevention and treatment of malignancy, including mixed gonadal dysgenesis and selective cases of androgen insensitivity syndrome (AIS) [58]. Additionally, anorchia is a male condition in which testes form normally in utero, as evidenced by normal male genitalia, but are absent at the time of birth, indicating loss sometime after the 14th week gestational age. The cause is unknown. “Resistant ovary syndrome” is a condition due to abnormalities in gonadotropin receptors or antibodies to these receptors seen in 46,XX karyotypes, typically presenting with sexual immaturity and primary amenorrhea and small ovaries with primordial follicles despite elevated gonadotropin concentrations [59, 60].
Evaluation of Hypergonadotropic Hypogonadism: A careful history should disclose past surgeries, exposure to chemotherapy (especially of alkylating agents) or radiation, gonadal trauma or testicular torsion, prior episodes of orchitis, and the presence of other medical problems, including sickle cell disease, galactosemia, and autoimmune illnesses (especially hypoparathyroidism and Addison’s disease). If autoimmunity is suspected, certain autoantibodies associated with APS1 can be measured with those against 21-hydroxylase being the most common. If an undiagnosed underlying process is suspected based on history or physical examination, further evaluation should be tailored specifically as needed. Ultrasound examination of abdominal gonads and/or chromosomal analysis is often warranted.
Eugonadotropic Hypogonadism (EH)
There are several conditions that can present with normal, pubertal gonadotropin levels with delayed or abnormal pubertal progression. Hormonal imbalances, for example, can cause failure to mature appropriately despite normal gonadotropin levels. Females with polycystic ovarian syndrome (PCOS) can undergo puberty appropriately but fail to proceed to menarche. These girls, usually obese, have normal reproductive anatomy and secondary sex characteristics but may have signs of insulin resistance and hyperandrogenism including severe acne or hirsutism. Hyperprolactinemia can also present with hypogonadism. Males will often have gynecomastia and females can have galactorrhea. The most common cause of elevated prolactin levels is prolactinoma.
Anatomic abnormalities are another cause of delayed puberty. Vaginal outflow obstruction such as imperforate hymen can prevent menstrual outflow, a so-called pseudo-primary amenorrhea. Müllerian duct anomalies (MDAs) are another type of anatomic abnormality that can present with primary amenorrhea. MDAs are classified according to level and degree of malformation. Class 1 represents segmental or complete agenesis or hypoplasia that can involve any combination of the vagina, cervix, fundus, and fallopian tubes (American Fertility Society, 1988) and is referred to as Müllerian aplasia [61]. Mayer-Rokitansky-Küster-Hauser syndrome is associated with uterine and vaginal hypoplasia/aplasia, where ovaries and fallopian tubes are preserved [16].
Evaluation: A careful physical examination including assessment of weight, acanthosis, hirsutism, acne, gynecomastia or galactorrhea, neurologic or visual abnormalities, secondary sex characteristics, and external genitalia is warranted. Laboratory tests should include a serum prolactin. If PCOS is suspected, an elevated free testosterone level can strengthen the diagnosis, and a 17-OHP level should be obtained to rule out nonclassical congenital adrenal hyperplasia. Chromosomal analysis is warranted if a disorder of sex development is entertained. If serum prolactin level is elevated, an MRI of the brain/pituitary to detect prolactinoma is indicated. Abdominal and pelvic ultrasound is often helpful in EH cases and can identify polycystic ovaries, vaginal obstruction, and the presence of gonads and other internal reproductive organs.
Diagnostic Tests
Table 17.2 summarizes the diagnostic evaluation. A detailed history (especially of parental consanguinity, age of puberty and history of infertility in family members, anosmia, nutritional history, systemic illness), thorough physical examination (special attention to stature, BMI, accurate sexual maturity staging/Tanner staging, stigmata of known conditions and systemic illnesses, galactorrhea, etc.), bone age evaluation, and appropriate laboratory evaluations as indicated (i.e., karyotype, LH, FSH, estradiol/testosterone, other pituitary hormones, thyroid function and prolactin) will be a reasonable starting point. The aim of initial evaluation is to rule out underlying disorders causing delayed puberty. The assay methodology of serum LH and FSH determination is important as values obtained by immunochemiluminometric assays (ICMA) are less than half of those obtained by immunofluorometric assays (IFMA) [62]. Serum LH is a more specific marker of pubertal onset than FSH; the latter is a more specific marker of primary gonadal failure [62]. Basal levels of LH and FSH may discriminate between hypo−/eugonadotropic and hypergonadotropic causes.
A delay in bone age is commonly seen in delayed puberty. If the bone age is >2 years delayed, the height prediction by Bayley-Pinneau tables overestimate predicted target height in CDGP [1, 62]. Karyotype and/or comparative genomic hybridization is indicated in hypergonadotropic hypogonadism. Pelvic ultrasound (US) in girls will help to delineate the presence of absence of uterus and ovaries as well as any evidence of stimulation. Brain imaging is also indicated, especially in cases of hypogonadotropic hypogonadism. Serum INHB corroborates the functional integrity of the Sertoli cells. Depending on the clinical and laboratory assessment, imaging of brain and pelvic ultrasound is indicated. If basal gonadotropin levels are inconclusive, stimulation tests may assist in differentiating CDGP vs. HH. However, no single test has 100% specificity/sensitivity.
Role of stimulation tests
If basal gonadotropin levels are inconclusive, stimulation tests may be helpful in differentiating CDGP vs. hypogonadotropic hypogonadism (HH). However, no single test has 100% specificity/sensitivity.
-
1.
GnRH or a GnRH agonist stimulation test: This is the gold standard for biochemical evaluation of HPG axis activation determined by the LH response to a classical GnRH stimulation test. LHRH agonist stimulation test is more popular due to its wide availability and is also considered to be more discriminative than provocative LHRH test [63]. There is a significant overlap in LH and FSH responses between CDGP and HH patients. Persistence of low basal or GnRH agonist stimulated LH and FSH in a late teen with a bone age > 12 years may be suggestive of defective gonadotropin secretion. A positive response (i.e., predominant LH response over FSH response or peak LH >5 IU/L by ICMA and > 8 by IFMA) is more consistent with CDGP. In primary ovarian failure in which the gonadotropin levels are only mildly elevated, a GnRH agonist stimulation will reveal partial gonadal failure.
A variety of hormone stimulation protocols exist, but an often used one is leuprolide acetate injection 20mcg/kg (maximum 500mcg) administered subcutaneously. Draw blood levels for FSH, LH, and estradiol/testosterone. Some institutions use blood draws at 0 hour, 30 minutes, and 60 minutes. At our institution, blood is sampled at 0 hour, 4 hours, and 24 hours. If the HPG axis is activated, a two- to threefold rise in FSH and LH is observed with maximal pituitary response of LH >5 IU/L at 4 hours and maximal gonadal response of estradiol (E2) of >150 pmol/L (>40.86 pg/ml) and testosterone >3.15 nmol/L (>90 ng/dl) [64,65,66].
-
2.
Human chorionic gonadotropin (hCG) stimulation test: Likewise, there are disparate protocols for this test [67,68,69,70,71]. The protocol commonly used in our institution is hCG administered intra-muscularly at a dose of 3000 IU/m2 once a day for 3 days. Baseline LH, FSH, testosterone, as well as blood sampling for testosterone need to be drawn 24 hours after the third injection. An absolute serum testosterone concentration on day 4 of ≥150 ng/dl is normal and ≤ 50 ng/dl in HH.
-
3.
Growth hormone stimulation testing: In subjects with short stature, delayed puberty, poor growth velocity, and delayed bone age, evaluation of serum IGF1 and provocative growth hormone testing will be helpful to assess growth hormone deficiency. If there is significant short stature to warrant provocative growth hormone testing, sex steroid priming with estrogen/testosterone is recommended necessarily as this may restore the physiologic depressed growth hormone secretion associated with low estrogen levels [1].
Present and Future Therapies
Inadequate gonadal steroid secretion is the fundamental basis of delayed puberty.
Therapeutic goals are to develop secondary sex characteristics, to amass and sustain normal bone development, to maximize final height, and to restore fertility. Treatment of delayed puberty is variable and depends on diagnosis.
Observation
Most cases of temporary hypogonadism and EH do not require hormonal treatment to induce puberty. With GDGP, observation and “watchful waiting” are generally adequate, but short-term hormone therapy to “jump start” puberty is sometimes justified to prevent significant psychological distress, initiate a growth spurt, and/ or activate the HPG axis.
In functional HH related to exercise, eating disorder, or chronic illness, the treatment is to improve overall health and nutrition. In regard to disorders of sex development, there is significant controversy surrounding the appropriate time for cosmetic surgery, gonadectomy, and HRT – current recommendations are complex and beyond the scope of this review [58].
Hormone replacement therapy (HRT)
Permanent HH and HHG generally require sex steroid HRT to induce puberty and maintain physiologic hormone levels. Replacement of other pituitary hormones is also frequently required, especially in the case of MPHD. When using HRT to induce puberty, there are several important considerations. Initiation of therapy must be timed appropriately to balance the benefits of developing according to population and physiologic norms with risk of premature epiphyseal closure and attenuated final adult height. Studies on boys with CDGP and girls with TS have shown that initiation of hormone therapy at very low doses after around 14 years of age in boys or 12 years in girls has no significant negative impact on final adult height while simultaneously promoting a natural emergence in the development of secondary sex characteristics [72,73,74,75]. In girls with any type of hypogonadism, HRT is the best treatment option as this will result in adequate development of secondary sex characteristics as well as that of the uterus.
Estrogen therapy to induce female puberty is typically initiated with transdermal preparations of 17β-estradiol given the very low doses of hormone replacement that is required. Typically treatment starts with using half of the lowest dose patch with 3.1–6.2 μg daily (1/8–1/4 of the 25 μg patch) and increased gradually by 3.1–6.2 μg daily every 6 months [1] over the next 2 years to an adult dose of 100–200ug daily to mimic physiologic levels seen in puberty. Estradiol (E2) levels can be monitored to ensure appropriate dosing. On the other hand, HRT that is provided too rapidly tends to promote unnatural development, including breast growth that occurs disproportionately in the nipple and areola [76]. Once full E2 dosing is reached and breast maturation is almost complete, cyclic oral progesterone at normal adult dose is added every 1–3 months to induce menstruation, a necessity to decrease the risk of uterine cancer. Once menstruation has been established, contraception preparations can be used for HRT depending on patient preference [77]. In cases of HH in which permanent hypogonadism has not been confirmed, brief trials off HRT can be attempted once regular cycles occur in order to assess for activation of the HPG axis. If transdermal preparations are unavailable, HRT may be initiated with conjugated estrogens (Premarin®) 0.1625 mg daily, increase every 3–6 months to 0.325 mg daily or ethinylestradiol 2 μg daily and increase every 3–6 months up to 10 μg daily.
Initial therapy is with estrogen alone to maximize breast growth and to induce uterine and endometrial proliferation. Adding a progestin prematurely or administering combinations of estrogens and progestins early on may reduce ultimate breast size. Progestin is added to mimic the normal menstrual cycle after breast growth ceases (when full contour breast growth plateaus) or menses occur. Once menstruation established with cyclic hormone treatment, discontinue intermittently for 1–3-month periods to determine if spontaneous menstruation occurs (in girls with CD and FHH). In permanent hypogonadism, OCP should be continued till the average age of menopause, ~50 years.
Testosterone therapy to initiate male puberty is generally started at 50 mg of depot testosterone as intramuscular injection once monthly for 3–6 months [1]. This will result in pubertal activation in CDG P [38]. If testes do not grow and reach a volume of 4 ml within 1 year of treatment, it is highly likely that the patient will not develop puberty spontaneously (most likely, not CGDP). In that scenario, treatment may be discontinued for 3 months, and HPG axis activation may be re-evaluated. Subsequently, testosterone is increased to 100 mg per month with 25–50 mg increment in dose for approximately 18 months to complete the growth spurt (dosing should increase gradually to mimic physiologic puberty and prevent accelerated bone maturation). After growth is complete, further increase in dose can be made to 100 mg twice monthly. Testosterone levels and, in the case of hypergonadotropic hypogonadism, LH levels should be monitored and used to adjust dose up to a maximum adult dose of 200 mg twice monthly as needed to achieve serum concentrations in the normal range. Thereafter, the increment of testosterone is 250 mg, every 3–4 weeks. It has to be kept in mind that HRT in males only result in virilization without testicular development. Oral testosterone preparations provide less consistent serum testosterone levels, and there is a risk for hepatic damage or carcinogenesis. Testosterone topical products, nasal spray, and gels, frequently used in adults, are not well studied in children.
Pulsatile GnRH or gonadotropin therapy
Patients with permanent hypogonadism can occasionally achieve fertility through treatment with gonadotropin or GnRH-based therapies and should be referred to reproductive endocrinology as needed. When fertility is desired, treat with either exogenous gonadotropins or pulsatile GnRH. Pulsatile administration of exogenous GnRH is effective therapy for stimulation of endogenous gonadotropin secretion, follicular development, and ovulation in women with GnRH deficiency. Mutations in the GPR54 (encoding the kisspeptin receptor, also known as KISS1R) reportedly can be corrected by the administration of GnRH [5, 36]. In male hypogonadotropic hypogonadism, GnRH treatment will promote a physiologic puberty with testicular development, virilization, and spermatogenesis. When spermatogenesis is achieved, maintenance therapy consists of subcutaneous hCG injections once or twice a week [15].
Human chorionic gonadotropin (hCG)
HCG has been used to treat subjects with permanent HH. A typical starting dose of 500 IU is administered subcutaneously on Mondays, Wednesdays, and Fridays. Dilute the 10,000-unit vial of powder with 5 mL of diluent for a 2000 unit/mL concentration. Obtain serum testosterone measurement in 1 month on a Monday prior to an injection. If the testosterone is <200 ng/dL, increase the dose to 1000 units subcutaneously, up to a maximum dose of 1500 IU (on M-W-F) and repeat a “trough” testosterone in another month. The hCG treatment will result in testicular enlargement, testosterone production, Sertoli cell maturation, and spermatogenesis and thus offers better chances of future fertility.
Leptin has been used in the management of amenorrhea in adults, but there is no pediatric data available. Other treatment options such as combination of hMG/hCG or recombinant FSH/hCG [15] that are used in the management of hypogonadotropic males for fertility are beyond the scope of this chapter.
Future Therapies
Although current treatment of delayed puberty centers revolves around replacement of sex steroid hormones, advances in the identification of genetic mutations that underlie HH promise to increase our understanding of the physiology behind pubertal initiation [78]. This information could result in the development of improved targeted therapies and allow for normal pubertal progression. A potential future therapeutic agent for treatment of delayed puberty is agonists of kisspeptin peptides and neurokinin B agonists. In boys with CDGP and short stature, a potential therapeutic approach is aromatase inhibition, which may increase the final adult height [1, 79]. The treatments targeted to preserve future fertility such as cryopreservation of ovarian fragments prior to anticipated ovarian failure secondary to gonadotoxic treatment [10] and pulsatile hCG treatment for HH are not discussed in this chapter.
References
Palmert MR, Dunkel L. Clinical practice. Delayed puberty. N Engl J Med. 2012;366(5):443–53.
Seminara SB, Crowley WF Jr. Kisspeptin and GPR54: discovery of a novel pathway in reproduction. J Neuroendocrinol. 2008;20(6):727–31.
Lee JM, Kaciroti N, Appugliese D, Corwyn RF, Bradley RH, Lumeng JC. Body mass index and timing of pubertal initiation in boys. Arch Pediatr Adolesc Med. 2010;164(2):139–44.
Nathan BM, Sedlmeyer IL, Palmert MR. Impact of body mass index on growth in boys with delayed puberty. J Pediatr Endocrinol Metab. 2006;19(8):971–7.
Messager S, Chatzidaki EE, Ma D, Hendrick AG, Zahn D, Dixon J, et al. Kisspeptin directly stimulates gonadotropin-releasing hormone release via G protein-coupled receptor 54. Proc Natl Acad Sci U S A. 2005;102(5):1761–6.
Silveira LG, Noel SD, Silveira-Neto AP, Abreu AP, Brito VN, Santos MG, et al. Mutations of the KISS1 gene in disorders of puberty. J Clin Endocrinol Metab. 2010;95(5):2276–80.
Gueorguiev M, Goth ML, Korbonits M. Leptin and puberty: a review. Pituitary. 2001;4(1–2):79–86.
Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham CH, Prentice AM, et al. Effects of recombinant leptin therapy in a child with congenital leptin deficiency. N Engl J Med. 1999;341(12):879–84.
Tornberg J, Sykiotis GP, Keefe K, Plummer L, Hoang X, Hall JE, et al. Heparan sulfate 6-O-sulfotransferase 1, a gene involved in extracellular sugar modifications, is mutated in patients with idiopathic hypogonadotrophic hypogonadism. Proc Natl Acad Sci U S A. 2011;108(28):11524–9.
Poirot C, Vacher-Lavenu MC, Helardot P, Guibert J, Brugieres L, Jouannet P. Human ovarian tissue cryopreservation: indications and feasibility. Hum Reprod. 2002;17(6):1447–52.
Xu C, Messina A, Somm E, Miraoui H, Kinnunen T, Acierno J Jr, et al. KLB, encoding beta-klotho, is mutated in patients with congenital hypogonadotropic hypogonadism. EMBO Mol Med. 2017;9(10):1379–97.
Zhu J, Choa RE, Guo MH, Plummer L, Buck C, Palmert MR, et al. A shared genetic basis for self-limited delayed puberty and idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 2015;100(4):E646–54.
Howard SR, Guasti L, Ruiz-Babot G, Mancini A, David A, Storr HL, et al. IGSF10 mutations dysregulate gonadotropin-releasing hormone neuronal migration resulting in delayed puberty. EMBO Mol Med. 2016;8(6):626–42.
Parent AS, Teilmann G, Juul A, Skakkebaek NE, Toppari J, Bourguignon JP. The timing of normal puberty and the age limits of sexual precocity: variations around the world, secular trends, and changes after migration. Endocr Rev. 2003;24(5):668–93.
Delemarre EM, Felius B, Delemarre-van de Waal HA. Inducing puberty. Eur J Endocrinol. 2008;159(Suppl 1):S9–15.
Fenichel P. Delayed puberty. Endocr Dev. 2012;22:138–59.
Sedlmeyer IL, Palmert MR. Delayed puberty: analysis of a large case series from an academic center. J Clin Endocrinol Metab. 2002;87(4):1613–20.
Rosenfield RL. Clinical review 6: diagnosis and management of delayed puberty. J Clin Endocrinol Metab. 1990;70(3):559–62.
Wehkalampi K, Widen E, Laine T, Palotie A, Dunkel L. Association of the timing of puberty with a chromosome 2 locus. J Clin Endocrinol Metab. 2008;93(12):4833–9.
Sedlmeyer IL, Hirschhorn JN, Palmert MR. Pedigree analysis of constitutional delay of growth and maturation: determination of familial aggregation and inheritance patterns. J Clin Endocrinol Metab. 2002;87(12):5581–6.
Albanese A, Stanhope R. Predictive factors in the determination of final height in boys with constitutional delay of growth and puberty. J Pediatr. 1995;126(4):545–50.
Counts DR, Pescovitz OH, Barnes KM, Hench KD, Chrousos GP, Sherins RJ, et al. Dissociation of adrenarche and gonadarche in precocious puberty and in isolated hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 1987;64(6):1174–8.
Kelch RP, Hopwood NJ, Marshall JC. Diagnosis of gonadotropin deficiency in adolescents: limited usefulness of a standard gonadotropin-releasing hormone test in obese boys. J Pediatr. 1980;97(5):820–4.
Wu FC, Brown DC, Butler GE, Stirling HF, Kelnar CJ. Early morning plasma testosterone is an accurate predictor of imminent pubertal development in prepubertal boys. J Clin Endocrinol Metab. 1993;76(1):26–31.
Grinspon RP, Ropelato MG, Gottlieb S, Keselman A, Martinez A, Ballerini MG, et al. Basal follicle-stimulating hormone and peak gonadotropin levels after gonadotropin-releasing hormone infusion show high diagnostic accuracy in boys with suspicion of hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 2010;95(6):2811–8.
Resende EA, Lara BH, Reis JD, Ferreira BP, Pereira GA, Borges MF. Assessment of basal and gonadotropin-releasing hormone-stimulated gonadotropins by immunochemiluminometric and immunofluorometric assays in normal children. J Clin Endocrinol Metab. 2007;92(4):1424–9.
Coutant R, Biette-Demeneix E, Bouvattier C, Bouhours-Nouet N, Gatelais F, Dufresne S, et al. Baseline inhibin B and anti-Mullerian hormone measurements for diagnosis of hypogonadotropic hypogonadism (HH) in boys with delayed puberty. J Clin Endocrinol Metab. 2010;95(12):5225–32.
Simon D. Puberty in chronically diseased patients. Horm Res. 2002;57(Suppl 2):53–6.
Buchacz K, Rogol AD, Lindsey JC, Wilson CM, Hughes MD, Seage GR 3rd, et al. Delayed onset of pubertal development in children and adolescents with perinatally acquired HIV infection. J Acquir Immune Defic Syndr. 2003;33(1):56–65.
Caronia LM, Martin C, Welt CK, Sykiotis GP, Quinton R, Thambundit A, et al. A genetic basis for functional hypothalamic amenorrhea. N Engl J Med. 2011;364(3):215–25.
Kaplowitz P. Clinical characteristics of 104 children referred for evaluation of precocious puberty. J Clin Endocrinol Metab. 2004;89(8):3644–50.
Wyshak G, Frisch RE. Evidence for a secular trend in age of menarche. N Engl J Med. 1982;306(17):1033–5.
Semple RK, Topaloglu AK. The recent genetics of hypogonadotrophic hypogonadism – novel insights and new questions. Clin Endocrinol. 2010;72(4):427–35.
Shaw ND, Seminara SB, Welt CK, Au MG, Plummer L, Hughes VA, et al. Expanding the phenotype and genotype of female GnRH deficiency. J Clin Endocrinol Metab. 2011;96(3):E566–76.
Wang Y, Gong C, Qin M, Liu Y, Tian Y. Clinical and genetic features of 64 young male paediatric patients with congenital hypogonadotropic hypogonadism. Clin Endocrinol. 2017;87(6):757–66.
de Roux N, Genin E, Carel JC, Matsuda F, Chaussain JL, Milgrom E. Hypogonadotropic hypogonadism due to loss of function of the KiSS1-derived peptide receptor GPR54. Proc Natl Acad Sci U S A. 2003;100(19):10972–6.
Achermann JC, Gu WX, Kotlar TJ, Meeks JJ, Sabacan LP, Seminara SB, et al. Mutational analysis of DAX1 in patients with hypogonadotropic hypogonadism or pubertal delay. J Clin Endocrinol Metab. 1999;84(12):4497–500.
Raivio T, Falardeau J, Dwyer A, Quinton R, Hayes FJ, Hughes VA, et al. Reversal of idiopathic hypogonadotropic hypogonadism. N Engl J Med. 2007;357(9):863–73.
Wolf NI, Vanderver A, van Spaendonk RM, Schiffmann R, Brais B, Bugiani M, et al. Clinical spectrum of 4H leukodystrophy caused by POLR3A and POLR3B mutations. Neurology. 2014;83(21):1898–905.
Topaloglu AK, Lomniczi A, Kretzschmar D, Dissen GA, Kotan LD, McArdle CA, et al. Loss-of-function mutations in PNPLA6 encoding neuropathy target esterase underlie pubertal failure and neurological deficits in Gordon Holmes syndrome. J Clin Endocrinol Metab. 2014;99(10):E2067–75.
de Vries L, Weintrob N, Phillip M. Craniopharyngioma presenting as precocious puberty and accelerated growth. Clin Pediatr (Phila). 2003;42(2):181–4.
Halac I, Zimmerman D. Endocrine manifestations of craniopharyngioma. Childs Nerv Syst. 2005;21(8–9):640–8.
Darzy KH, Shalet SM. Pathophysiology of radiation-induced growth hormone deficiency: efficacy and safety of GH replacement. Growth Hormon IGF Res 2006;16 Suppl A:S30–40.
Dattani MT, Martinez-Barbera JP, Thomas PQ, Brickman JM, Gupta R, Martensson IL, et al. Mutations in the homeobox gene HESX1/Hesx1 associated with septo-optic dysplasia in human and mouse. Nat Genet. 1998;19(2):125–33.
Reynaud R, Gueydan M, Saveanu A, Vallette-Kasic S, Enjalbert A, Brue T, et al. Genetic screening of combined pituitary hormone deficiency: experience in 195 patients. J Clin Endocrinol Metab. 2006;91(9):3329–36.
Zentner GE, Layman WS, Martin DM, Scacheri PC. Molecular and phenotypic aspects of CHD7 mutation in CHARGE syndrome. Am J Med Genet A. 152A(3):674–86.
Pinto G, Abadie V, Mesnage R, Blustajn J, Cabrol S, Amiel J, et al. CHARGE syndrome includes hypogonadotropic hypogonadism and abnormal olfactory bulb development. J Clin Endocrinol Metab. 2005;90(10):5621–6.
Goldstone AP, Holland AJ, Hauffa BP, Hokken-Koelega AC, Tauber M. Recommendations for the diagnosis and management of Prader-Willi syndrome. J Clin Endocrinol Metab. 2008;93(11):4183–97.
Beales PL, Elcioglu N, Woolf AS, Parker D, Flinter FA. New criteria for improved diagnosis of Bardet-Biedl syndrome: results of a population survey. J Med Genet. 1999;36(6):437–46.
Pasquino AM, Passeri F, Pucarelli I, Segni M, Municchi G. Spontaneous pubertal development in Turner's syndrome. Italian study Group for Turner's syndrome. J Clin Endocrinol Metab. 1997;82(6):1810–3.
Latronico AC, Arnhold IJ. Inactivating mutations of LH and FSH receptors–from genotype to phenotype. Pediatr Endocrinol Rev. 2006;4(1):28–31.
Beranova M, Oliveira LM, Bedecarrats GY, Schipani E, Vallejo M, Ammini AC, et al. Prevalence, phenotypic spectrum, and modes of inheritance of gonadotropin-releasing hormone receptor mutations in idiopathic hypogonadotropic hypogonadism. J Clin Endocrinol Metab. 2001;86(4):1580–8.
Layman LC. Mutations in the follicle-stimulating hormone-beta (FSH beta) and FSH receptor genes in mice and humans. Semin Reprod Med. 2000;18(1):5–10.
Layman LC, Lee EJ, Peak DB, Namnoum AB, Vu KV, van Lingen BL, et al. Delayed puberty and hypogonadism caused by mutations in the follicle-stimulating hormone beta-subunit gene. N Engl J Med. 1997;337(9):607–11.
Howell SJ, Shalet SM. Spermatogenesis after cancer treatment: damage and recovery. J Natl Cancer Inst Monogr. 2005;34:12–7.
Myhre AG, Halonen M, Eskelin P, Ekwall O, Hedstrand H, Rorsman F, et al. Autoimmune polyendocrine syndrome type 1 (APS I) in Norway. Clin Endocrinol. 2001;54(2):211–7.
Kaufman FR, Kogut MD, Donnell GN, Goebelsmann U, March C, Koch R. Hypergonadotropic hypogonadism in female patients with galactosemia. N Engl J Med. 1981;304(17):994–8.
Lee PA, Houk CP, Ahmed SF, Hughes IA. Consensus statement on management of intersex disorders. International consensus conference on intersex. Pediatrics. 2006;118(2):e488–500.
Arici A, Matalliotakis IM, Koumantakis GE, Goumenou AG, Neonaki MA, Koumantakis EE. Diagnostic role of inhibin B in resistant ovary syndrome associated with secondary amenorrhea. Fertil Steril. 2002;78(6):1324–6.
Mueller A, Berkholz A, Dittrich R, Wildt L. Spontaneous normalization of ovarian function and pregnancy in a patient with resistant ovary syndrome. Eur J Obstet Gynecol Reprod Biol. 2003;111(2):210–3.
ACOG Committee Opinion No. 355: vaginal agenesis: diagnosis, management, and routine care. Obstet Gynecol. 2006;108(6):1605–9.
Wit JM, Rekers-Mombarg LT. Final height gain by GH therapy in children with idiopathic short stature is dose dependent. J Clin Endocrinol Metab. 2002;87(2):604–11.
Ibanez L, Potau N, Zampolli M, Virdis R, Gussinye M, Carrascosa A, et al. Use of leuprolide acetate response patterns in the early diagnosis of pubertal disorders: comparison with the gonadotropin-releasing hormone test. J Clin Endocrinol Metab. 1994;78(1):30–5.
Lanes R. A GnRH analog test in diagnosing gonadotropin deficiency in males with delayed puberty. J Pediatr. 2006;149(5):731; author reply –2
Wilson DA, Hofman PL, Miles HL, Unwin KE, McGrail CE, Cutfield WS. Evaluation of the buserelin stimulation test in diagnosing gonadotropin deficiency in males with delayed puberty. J Pediatr. 2006;148(1):89–94.
Zamboni G, Antoniazzi F, Tato L. Use of the gonadotropin-releasing hormone agonist triptorelin in the diagnosis of delayed puberty in boys. J Pediatr. 1995;126(5 Pt 1):756–8.
Segal TY, Mehta A, Anazodo A, Hindmarsh PC, Dattani MT. Role of gonadotropin-releasing hormone and human chorionic gonadotropin stimulation tests in differentiating patients with hypogonadotropic hypogonadism from those with constitutional delay of growth and puberty. J Clin Endocrinol Metab. 2009;94(3):780–5.
Dunkel L, Perheentupa J, Virtanen M, Maenpaa J. Gonadotropin-releasing hormone test and human chorionic gonadotropin test in the diagnosis of gonadotropin deficiency in prepubertal boys. J Pediatr. 1985;107(3):388–92.
Dunkel L, Perheentupa J, Virtanen M, Maenpaa J. GnRH and HCG tests are both necessary in differential diagnosis of male delayed puberty. Am J Dis Child. 1985;139(5):494–8.
Degros V, Cortet-Rudelli C, Soudan B, Dewailly D. The human chorionic gonadotropin test is more powerful than the gonadotropin-releasing hormone agonist test to discriminate male isolated hypogonadotropic hypogonadism from constitutional delayed puberty. Eur J Endocrinol. 2003;149(1):23–9.
Kauschansky A, Dickerman Z, Phillip M, Weintrob N, Strich D. Use of GnRH agonist and human chorionic gonadotrophin tests for differentiating constitutional delayed puberty from gonadotrophin deficiency in boys. Clin Endocrinol. 2002;56(5):603–7.
Arrigo T, Cisternino M, Luca De F, Saggese G, Messina MF, Pasquino AM, et al. Final height outcome in both untreated and testosterone-treated boys with constitutional delay of growth and puberty. J Pediatr Endocrinol Metab. 1996;9(5):511–7.
Buyukgebiz A. Treatment of constitutional delayed puberty with a combination of testosterone esters. Horm Res. 1995;44(Suppl 3):32–4.
Soliman AT, Khadir MM, Asfour M. Testosterone treatment in adolescent boys with constitutional delay of growth and development. Metabolism. 1995;44(8):1013–5.
Ankarberg-Lindgren C, Elfving M, Wikland KA, Norjavaara E. Nocturnal application of transdermal estradiol patches produces levels of estradiol that mimic those seen at the onset of spontaneous puberty in girls. J Clin Endocrinol Metab. 2001;86(7):3039–44.
Brook CG. Management of delayed puberty. Br Med J (Clin Res Ed). 1985;290(6469):657–8.
Bondy CA. Care of girls and women with turner syndrome: a guideline of the turner syndrome study group. J Clin Endocrinol Metab. 2007;92(1):10–25.
Achermann JC, Jameson JL. Advances in the molecular genetics of hypogonadotropic hypogonadism. J Pediatr Endocrinol Metab. 2001;14(1):3–15.
Wickman S, Sipila I, Ankarberg-Lindgren C, Norjavaara E, Dunkel L. A specific aromatase inhibitor and potential increase in adult height in boys with delayed puberty: a randomised controlled trial. Lancet. 2001;357(9270):1743–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Colvin, C., Devineni, G., Sunil, B., Ashraf, A.P. (2022). Delayed Puberty. In: Bandeira, F., Gharib, H., Griz, L., Faria, M. (eds) Endocrinology and Diabetes. Springer, Cham. https://doi.org/10.1007/978-3-030-90684-9_17
Download citation
DOI: https://doi.org/10.1007/978-3-030-90684-9_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-90683-2
Online ISBN: 978-3-030-90684-9
eBook Packages: MedicineMedicine (R0)