
Abstract
This chapter considers skin cancer as an emerging health challenge. The causes are analyzed in terms of population, lifestyle, and epidemiological factors. Certain facial skin cancers have high-risk factors which are considered in pathological, clinical, and metastatic risk categories. Other facial skin cancers are high-risk by virtue of their anatomical site, clinical and radiological extent, and reconstructive challenge. Patients presenting with high-risk facial skin cancers require proper oncological and reconstructive management. Certain facial cancers are best managed by multidisciplinary teams, with tailored treatment by surgeons and specialists trained to a very high standard. Specific clinical examples are illustrated, but principally the concepts of complete local excision + aesthetic reconstruction (CLEAR) or delayed reconstruction after pathological examination (DRAPE) are emphasised. High-risk facial cancers include those of the skin and cancer of the upper aerodigestive tract arising from the mucosal surface, most commonly squamous cell carcinoma with poor differentiation, perineural invasion, and malignant melanoma. Less commonly basal cell carcinoma with morphoeic patterns, basosquamous carcinomas, de-differentiated basal cell carcinoma and even rarer but very aggressive cancers such as sebaceous carcinoma, Merkel cell cancer and sarcoma.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Extreme facial skin cancer
- The size of the problem
- Complete local excision
- Aesthetic reconstruction (CLEAR)
-
High-risk cancers of the face are best managed by experienced plastic surgeons in a multidisciplinary setting.
-
These cancers are relatively rare compared to the very common occurrence of skin cancer as a prevalent cancer in the general population, but require a unique surgical skill set.
-
Accurate diagnosis and a precise surgical plan of management should be co-ordinated with adjuvant therapies including radiation, medical, and immunotherapy oncological protocols.
1 Introduction
Australia and New Zealand with a combined population of about 31 million citizens, many of Celtic heritage, who live in a region with very high solar ultraviolet index, are characterised by the highest incidence of skin cancer in the world. These cancers result in a significant health, economic, and social burden.
Two in three people in Australia and New Zealand will develop skin cancer in their lifetime [1]. While the majority of these are the relatively indolent and slow-growing basal cell carcinomas (BCCs), there are a certain number of more aggressive skin cancers that present to plastic surgeons and other specialists. These include high-grade squamous cell carcinomas (SCCs), de-differentiated (basosquamous) carcinomas, malignant melanoma (MM), and rarer entities such as Merkel cell carcinoma, sebaceous carcinoma, adnexal carcinoma, and sarcoma. Cancer of the upper aerodigestive tract arising from the mucosal surface is also a significant entity affecting the head and neck. A distinctive feature of extreme facial cancers is perineural spread along the cranial nerves.
Australia and New Zealand have the highest incidence of skin cancer in the world. In 2014, Australia recorded 959,243 Medicare claims for the treatment of non-melanoma skin cancer (NMSC). This is an underestimate. The annual incidence of NMSC in the USA has been recorded as 3.5 million [2], with a population in 2020 of 331 million—one tenth the incidence of NMSC in Australia and New Zealand.
The risk of developing skin cancer in Australia and New Zealand is greater for men than for women (70% versus 58%). Deaths from skin cancer exceed those caused by road trauma with 2162 recorded for Australia in 2015, 1520 of which were attributed to MM. In 2017, 310 deaths were caused by MM in New Zealand.
Although mortality rates of skin cancer have been increasing in Australia and New Zealand since 2000, recent trends suggest stabilization of the numbers for those citizens <45 years of age. This is a result of reduced ultraviolet exposure resulting from successful and very prominent public education programs.
The ultraviolet levels in New Zealand are very high especially in summer months. The ozone “hole” over Antarctica, Celtic skin types, and a sun-seeking outdoor lifestyle of the population, all contribute to the high incidence of skin cancer. The National Institute of Water and Atmospheric Research has shown that ultraviolet levels are 40% higher in New Zealand than at a corresponding latitude in the northern hemisphere [3]. The highest levels of annual ultraviolet exposure in New Zealand are in the Eastern Bay of Plenty region of the North Island, where the lead author (MFK) has provided a provincial plastic surgery service for the last decade. This in part triggered his interest in writing about the extreme forms of facial skin cancer. The second author (IB), a general surgeon practicing for over 30 years in a similar high-ultraviolet exposure regions (Gisborne, East Cape), has also managed patients with skin cancers affecting the face and other body sites, during his long surgical career.
The pathogenesis and molecular biology of extreme facial cancer are well detailed in later chapters by pathologists and research scientists. It involves genetic predisposition and solar ultraviolet radiation damage as well as complex mutations in tumor suppressor genes. There has been a paradigm shift in the theories of oncogenesis involving complex molecular pathways and the role of cancer stem cells.
From a day-to-day clinical management perspective, it is important to be aware of the risk stratification of skin cancers. BCCs with a morphoeic (sclerosing) histological pattern have a much higher risk of local recurrence and therefore require wider excision margins than the standard 4 mm. SCCs with poor histological differentiation and perineural and/or lymphovascular invasion have a predicted metastatic risk of 37% compared to the 0.3% risk for low-risk lesions in the head and neck [4]. Perineural spread caused by head and neck cancer is most often caused by skin SCC, and a high index of suspicion is needed. This also applies to radiological imaging studies of such patients [see Chap. 5 “The Team Approach in Cancer Care” on Applied Anatomy]. MM, the third most common skin cancer in Australia and New Zealand, is responsible for almost 2000 deaths per annum.
2 Why Do Patients Present with Extreme Facial Cancer?
This is perhaps the most important question in this chapter, given the knowledge and expertise in the management of skin cancer generally and the public awareness of this common acquired disease. The reasons are multiple and include personal fear and social isolation, cultural practices such as chewing of carcinogens, lifestyle and workstyle practices, initial mis-diagnosis and or mis-management, specific tumour characteristics, immunosuppression, and/or previous radiation therapy.
All skin cancers of the human face start as small tumours.
Figure 1 shows a typical BCC of the face in a middle-aged woman, which was completely excised and repaired with a postauricular full-thickness skin graft.

(a–c) An infiltrating BCC of the left mid-cheek treated by the late Sir William Manchester (1913–2001) in the 1960s with wide excision and a post-auricular full-thickness graft
Figure 2 shows a 71-year-old man with an infiltrating micronodular BCC of his left infraorbital region, widely excised and immediately repaired with a Mustardé cheek rotation flap. The final image shows the result at 4 years, when he was re-referred with an SCC on his right eyebrow.

(a–c) A case of the lead author – infiltrating BCC of the left infraorbital region widely excised and repaired with a Mustardé cheek rotation flap at 3 days and result at 4 years
Figure 3 shows the extreme disfiguring appearance of a locally advanced BCC in an elderly man who neglected this cancer because of his fear. He was eventually encouraged to seek specialist attention by his wife, who was concerned about food, drink, and saliva spilling out of his left cheek. Sadly, the BCC was very extensive with infiltration of the facial soft tissues and skeleton and was considered inoperable. Appropriate palliative care was provided.

A neglected inoperable BCC with extensive involvement of the left hemi-face and invading the left maxilla and orbit in an elderly retired chemist seen by the lead author during his post-fellowship training in southern England circa 1990
3 Alternative Medical Misadventure: A Salutary Lesson
A 65-year-old woman sought advice from an alternative medicine practitioner regarding a 3 cm ulcerated lesion on her scalp who allegedly diagnosed the lesion as an “infected sebaceous cyst” and reassured the patient that it was benign. The patient was commenced on a skin treatment regimen involving the daily application of a herbal poultice and dressing changes. After 6 months of treatment, the lesion had grown to 8 cm and developed a purulent discharge. When the patient’s family became concerned that the treatment was ineffective, the alternative medicine practitioner allegedly dismissed these concerns and reiterated that the lesion was benign and advised against seeking conventional medical advice. After 16 months of treatment, the lesion had grown to 20 cm and eroded through the calvarium and involved the dura, confirmed by MRI and CT scans (Fig. 4). The tumour was treated by wide local excision including the underlying skull, the greater wing of sphenoid, and dura. Reconstruction included dural repair with a dura substitute, split rib grafts to span the bony defect, and an overlying latissimus dorsi muscle free flap covered with a split thickness skin graft (Fig. 4).

An extensive scalp SCC with destruction of the soft tissues and underlying skull and invasion of the dura (a) also demonstrated on MRI (b) and CT (c) scans, treated with surgery and adjuvant radiotherapy (d). (Reprinted from Mistry et al. [5]; with permission)
These four clinical cases contrast the relative simplicity of successfully managing early facial skin cancers, as opposed to only being able to offer palliation in the advanced cases. The third and fourth cases clearly illustrate the oncological and reconstructive challenges of the neglected skin cancer. A case report of five patients from Hungary in 2011 shows that delays in the diagnosis and late presentation are usually because of the patient’s fears of the diagnosis and treatment. In some cases, the patient just becomes accustomed to the usually slow-growing tumour [6].
Dr. Milton Edgerton MD (1928–2018) of Johns Hopkins Hospital and Virginia University considered the problem of advanced BCC in his Hayes Martin Lecture to the American Society of Head and Neck Surgeons in 1982 [7]. Invasion of deep facial tissues by a BCC and especially the mucous membranes is not a trivial matter, and the patient may never again be tumour-free. His case presentation of a young woman treated with radiotherapy in the 1930s for facial acne chronicles the more than 30 years (1949–1980) of multiple complete reconstructions of her nose, cheeks, lips, and chin. One important principle remains: if the destructive effects of the tumour and the surgical treatment result in the removal of one or more major facial features, it is essential that reasonably prompt reconstruction be undertaken.
This is true for non-facial regions as well and was certainly the case in this retired gentleman, shown in Fig. 5, who presented with a large ulcerated BCC of his left posterior shoulder in 1990. The infiltration had extended into the left shoulder joint, and definitive surgical management necessitated a left forequarter amputation. A radial forearm free flap harvested from the amputated extremity and used to repair the extensive soft tissue defect.

(a, b) A case of neglected BCC in a retired London accountant witnessed by the lead author in Southern England circa 1990. The extensive ulcerated tumour invaded the left shoulder joint and required a forequarter amputation and reconstruction with a free radial forearm flap harvested from the amputated left upper extremity
4 Guiding Principles of Surgical Management
Whatever the cancer challenge, the guiding principles (Sir Harold Gillies 1882–1960) for the plastic surgeon remain the same, specifically:
-
1.
Diagnose before you treat.
-
2.
Make a plan and a pattern for this plan (incorporating the choice of reconstruction).
-
3.
Treat the primary defect first.
-
4.
Never let routine methods become your master.
-
5.
Have a lifeboat.
-
6.
Consult other specialists.
-
7.
The aftercare is as important as the planning.
These principles are of course derived from some of the many fundamental truths that became intuitive for pioneers in plastic surgery like Sir Harold Gillies [8].
5 Management/Technique
This 68-year-old man with alcohol addiction (Fig. 6) presented with a neglected, locally advanced ulcerated SCC affecting his left posterior neck. He did not seek medical attention for several months. At one stage, he decided against the wishes of his family to drive to a remote location in North Queensland and attempted to drink himself to death under a eucalyptus tree. When this failed, he drove back to his home city thousands of kilometers away and sought medical attention.

(a–c) A neglected fungating SCC of the posterior neck in a 60-year-old gentleman with alcoholism, treated with wide local excision, radical left neck dissection and a pedicled trapezius myocutaneous flap reconstruction
On presentation, the extensive fungating tumor was inhabited by maggots. Physical examination and a CT scan indicated that surgical excision was feasible. A wide local excision along with a radical neck dissection resulted in a significant neck defect which was repaired with a pedicled trapezius myocutaneous flap. The large secondary defect was repaired with a meshed split skin graft. A keystone double advancement flap would also have been a reasonable option for closing the secondary defect. A free flap could have been considered as an alternative reconstructive option, but Professor Michael Poole of Sydney, Australia, who led the surgery for this patient, and the lead author felt that his pre-surgical general condition and relative malnutrition resulting from alcoholism were a contraindication to lengthy microvascular surgery.
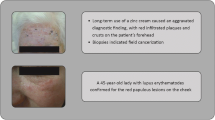
Figure 7 shows a 50-year-old woman who presented with an extensive ulcerated lesion of her right upper lip and nasolabial area, which had been treated as an inflammatory lesion for several months. A “delayed” biopsy showed an infiltrating BCC. After margin controlled wide excision and DRAPE (delayed reconstruction after pathology examination) protocol, a term coined by Professor Felix Behan FRACS of Melbourne, Australia, a staged reconstruction of her medial cheek, right alar base, and right upper lip was completed using a cheek rotation local flap, a paramedian forehead local flap, and a lower lip Abbé flap, with satisfactory results.

(a–c) A misdiagnosed infiltrating BCC of the right upper lip and nasolabial area, widely excised and reconstructed with multiple local flaps (cheek rotation, paramedian forehead and Abbé lower lip-switch flap)
The 60-year-old man in Fig. 8 presented with extensive facial sun damage and a recurrent Merkel cell carcinoma of his right cheek and required a very extensive hemi-face resection and ipsilateral parotidectomy. A loco-regional flap was considered unreliable, so an ulnar forearm free flap was used for reconstruction. This proximal forearm flap initially described by Dr. Maxwell Lovie FRACS (1939–2000) et al. [9] provided sufficient soft tissue volume compared to the more frequently used radial forearm flap. The patient underwent post-operative adjuvant radiotherapy.

(a–d) A recurrent Merkel cell carcinoma on the cheek in a 60-year-old man, was widely excised including a facial nerve-preserving superficial parotidectomy and immediate reconstruction with an ulnar forearm fasciocutaneous free flap, followed by adjuvant radiotherapy
MM rarely presents with extensive facial lesions, but occasionally metastatic spread can pose a challenge, as in this a 70-year-old man (Fig. 9), who developed a nodal metastasis in his left neck, which involved the overlying skin and was adherent to the common carotid artery. In collaboration with the vascular surgeons, a wide local excision and neck dissection including resection of a segment of his carotid artery were performed, with a temporary carotid by-pass shunt to preserve brain perfusion. A reversed saphenous vein bypass graft was utilized. The graft was then protected with a pedicled loco-regional pectoralis major myocutaneous flap.

(a, b) Metastatic malignant melanoma in a 70-year-old man’s left neck adherent to the left common carotid artery. Salvage surgery with local excision, neck dissection, bypass shunt, saphenous vein bypass graft of the excised carotid artery and reconstruction with a pedicled left pectoralis major myocutaneous flap
6 Indications
Innovative reconstruction methods are required when the cancer burden is extensive, the resection defect considerable, and where traditional methods of repair are inadequate.
6.1 Loco-Regional Combined Flaps
This 45-year-old pastor from Papua New Guinea (Fig. 10), with extensive SCC affecting the lips and right cheek caused by longstanding betel nut chewing, was referred to our Interplast Humanitarian team. The betel nut was mixed with an alkali lime powder from crushed seashells to reduce the acidity of the ingestion. Chewing betel nut is a traditional social practice in many Pacific Islands including the Solomon Islands, Papua New Guinea, and Vanuatu. Transfer to Australia or New Zealand for resection and free flap reconstruction was not an option, so the team planned a combination of loco-regional keystone flaps from his left cheek and anterior neck. An opinion was urgently requested by the Interplast Team leader (MFK), from Professor Felix Behan FRACS in Melbourne, Australia, via the Internet. The planned total forehead flap was not required for lining. The secondary defect of his submental region was repaired with a skin graft. The case was lost to follow-up.

(a–e) An extensive perioral SCC of the lips in a 40-year-old Papua New Guinean pastor, referred to a New Zealand based Interplast surgical team. Wide excision in Port Moresby and immediate reconstruction with keystone perforator island loco-regional flaps from the cervicomental and left cheek regions
6.2 Free-Flap Option
This 43-year-old man (Fig. 11) presented to the oral and maxillofacial surgeons with a rapidly growing chondrosarcoma of his right maxilla. An initial right hemimaxillectomy was followed by rapid and aggressive recurrence, which therefore required a wide orbital-heminasal midface resection, immediate reconstruction with a bi-paddled latissimus dorsi myocutaneous free flap, and post-operative adjuvant radiotherapy. Subsequent attempts were made to reconstruct his right hemi-nose defect with a staged forehead flap and bone grafts. He is now 20 years post-treatment and free of disease.

(a–d) An aggressive chondrosarcoma of the right maxilla in a 43-year-old man, treated radically with right hemiface resection (right orbit, maxilla and heminose), staged reconstruction with a free bi-paddled latissimus dorsi flap and expanded forehead flap. Alive and well 20 years later
7 Contraindications
There are rare extensive facial cancers that are inoperable as shown in Fig. 3, in an elderly man with longstanding and neglected midface BCC. For some patients, their comorbidities and general medical status as defined by the American Society of Anesthesiology (ASA) Physical Status classification may preclude curative surgery [10]. Professor Michael Poole MD, FRCS (Fig. 12), plastic, craniofacial, and head and neck plastic surgeon in Sydney, Australia with whom the lead author collaborated for 3 years (2004–2006), was a firm and passionate advocate for palliative surgery in selected patients, to improve their quality of life (Fig. 13). The concept of palliative surgery is detailed by Dr. Rafael Acosta-Rojas FRACS, EBOPRAS, in Chap. 15 “Palliative Surgery”.

Professor Michael Poole MD, FRCS – former director of the Oxford Craniofacial Unit, Radcliffe Infirmary, Oxford, UK and plastic surgeon/craniofacial surgeon Sydney, Australia. He mentored the lead author from 1999 to 2008

(a–c) A 78-year-old man with a fungating metastatic skin SCC on the right side of his neck following primary radiotherapy (a), underwent right radical neck dissection and superficial parotidectomy with wide local excision of the involved skin including partial amputation of the right ear (b). The resection defect was reconstructed with a large pedicled pectoralis myocutaneous flap and the donor site defect was repaired with a transpositional subcostal fasciocutaneous flap (c)
8 Palliative Surgery as an Option
Figure 13 shows a 78-year-old man with a metastatic skin SCC to the right side of his neck which failed to respond to primary radiotherapy. The fungating tumour resulted in a constant discharge and odour requiring daily dressings, affecting his quality of life significantly. Following a multidisciplinary discussion, the patient was offered and proceeded with salvage surgery. This involved a right radical neck dissection and superficial parotidectomy with wide local excision of the involved overlying skin and amputation of the lower pole of the right ear. The extensive defect was repaired with a large pedicled pectoralis myocutaneous flap (with removal of the nipple). The donor site was closed with an anteriorly based transpositional subcostal fasciocutaneous flap.
9 Innovations
The keystone perforator island loco-regional flaps of Professor Felix Behan continue to challenge our modern concepts of free flap surgery for major facial cancers. The keystone flap concept was based on clinical observation and the intuition that dermatomal planning of flaps guarantees a supportive vascular supply. Vessels follow nerves. The workhorse perforator flap concept has stood the test of time, for a quarter of a century. The lead author learned this flap from Dr. Simon Donahoe FRACS, a colleague of Behan in Melbourne at the Peter MacCallum Cancer Institute and has been a champion of its application for over a decade [11]. The keystone flap and its variants (Omega, double, Yin-Yang) provide a simple, quick, and reliable option with pain-free recovery, aesthetic reconstruction, low complications, and economy of effort and resources: Behan’s PACE acronym. They are applicable anywhere on the face and neck including the scalp but in the latter experience is required [9]. Professor Behan et al. expand on the application of the keystone flaps in Chap. 9 “Keystone Flap Concepts”.
10 Management of Complications
All surgery must balance the advantages of a given method with the risk of treatment. Complications can occur pre-operatively because of poor decision-making and planning (e.g., aspiration pneumonitis or sepsis). Problems may also arise peri-operatively because of imperfect technique, unheralded findings, and anaesthetic emergencies as well as post-operatively. The key post-operative complications include hematoma from bleeding which may compromise flap viability, partial or complete flap necrosis due to vascular insufficiency (most commonly venous outflow problems), injury to vital anatomical structures (e.g., facial nerve, thoracic duct), and sepsis. Incomplete cancer excision or cancer recurrence are also challenging complications. Knowledge of and situational awareness about complications are stressed to plastic surgeon trainees for their professional exam preparation. This becomes a mandatory skill set with consultant experience post final examinations! The philosophy with respect to complications may be a conservative approach, but sometimes a pro-active re-operative approach and salvage are required. The timing and judgment required for this are critical and follow the dictum of Sir Harold Gillies: Don’t do today what can be honorably be put off until tomorrow. Professor Michael Poole MD, FRCS, from whom the lead author learned so much in the 2000s, would argue that He who hesitates is lost.
11 Controversies
Mohs micrographic surgery, a technique popularized by dermatologists in North America and pioneered by a Wisconsin medical student in the 1940s, has been described as a “precise” surgical technique for the treatment of skin cancer. During Mohs surgery, thin layers of cancer-containing skin are serially removed and examined until only cancer-free tissue remains. Although published studies comparing Mohs’ surgery with conventional surgical excision claim superior results for BCC specifically, plastic surgeons worldwide question the oncological legitimacy and cost-effectiveness of this approach and its role in extreme facial cancers [12]. The technique is tedious, expensive, painful, and costly, although it may have a role in achieving clear resection margins for certain challenging BCCs, such as those with a morphoeic pattern and/or certain anatomic sites. Chap. 12 “Extreme Cancer of the Periorbital Region” in this Atlas describes cancers of the periorbital region, and Dr. Stephen Ng FRANZCO, an ophthalmic surgeon with a special interest in oculoplastic surgery, who collaborated with the lead author and third author (EB) for that chapter, has significant experience in reconstructing periorbital defects after Mohs micrographic surgery by dermatologists in his region.
12 Conclusion/Summary
Skin cancer is prevalent among the Caucasian population of Australia and New Zealand, with an incidence ten times that of other major developed countries such as the USA. During their careers, plastic surgeons can expect to be confronted with many challenges in the management of skin cancer and occasionally extreme, advanced, and even more challenging cases. Why these rarer cases ever present in the first place is an interesting and vexed question, for which the explanation is often complex and associated with multiple patient personality disorders. It is left for the experts in the field of cancer care to grapple with the challenge and conundrums of extreme facial cancer.
A surgical approach is suggested based on sound surgical principles including a definitive diagnosis, staging, and a multidisciplinary plan of management. Immediate reconstruction with the most appropriate method is ideal, but this may be delayed due to oncological concerns. A range of loco-regional and distant free flap options exist in the surgeon’s toolkit, backed up by the adjuvant therapies of radiation and medical oncology. The team includes radiologists, pathologists, prosthetic specialists, specialized nurses, anaesthetists, psychologists, and palliative care specialists as well as surgeons.
References
Cancer Council of Australia: skin cancer statistics and issues. 2012 & 2014. wiki.cancer.org.au.
Connolly KL, Nehal KS, Disa JJ. Evidence-based medicine: cutaneous facial malignancies: nonmelanoma skin cancer. Plast Reconstr Surg. 2017;139(1):181–90.
NIWA (National Institute of Water and Atmospheric Research). niwa.co.nz.
Peat B, Insull P, Ayers R. Risk stratification for metastasis from cutaneous squamous cell carcinoma of the head and neck. ANZ J Surg. 2012;82:230–3.
Mistry R, Wademan B, Avery G, Tan ST. A case of misdiagnosed squamous cell carcinoma due to alternative medical misadventure - time for tightening regulation? N Z Med J. 2010;123:61–7.
Varga E, Korom I, Rasko Z, Kis E, Varga J, Ol’ah J, et al. Neglected basal cell carcinomas in the 21st century. J Skin Cancer. 2011;2011:392151. https://doi.org/10.1155/2011/392151.
Edgerton MT. Advanced basal cell cancer: prognosis and treatment philosophy. Am J Surg. 1982;1444(4):392–400.
Klaassen MF, Brown E. An examiner’s guide to professional plastic surgery exams. Springer Nature. https://doi.org/10.1007/978-981-13-06689-1.
Lovie MJ, Duncan GM, Glasson DW. The ulnar artery forearm flap. Br J Plast Surg. 1984;37:486–92.
Klaassen MF, Brown E, Behan FC. Simply local flaps. Heidelberg: Springer; 2018. https://doi.org/10.1007/978-3-319-59400-2.
Behan FC. The keystone solution for major head and neck defects: audio-visual case presentations. Australas J Plastic Surg. 2019;2(2):79–83.
van Loo E, Mosterd E, Krekels GA, Roozeboom MH, Ostertag JU, Dirksen CD, et al. Surgical excision versus Mohs’ micrographic surgery for basal cell carcinoma of the face: a randomized clinical trial with 10 year followup. Eur J Cancer. 2014;50:3011–20.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Klaassen, M.F., Burton, I., Brown, E., Beehan, P.J., Tan, S.T. (2022). The Skin Cancer Epidemic. In: Burton, I., Klaassen, M.F. (eds) Atlas of Extreme Facial Cancer. Springer, Cham. https://doi.org/10.1007/978-3-030-88334-8_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-88334-8_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-88333-1
Online ISBN: 978-3-030-88334-8
eBook Packages: MedicineMedicine (R0)