
Abstract
Child development is an extremely complex process, which results from the interaction between the biological and psychological, located in a sociocultural and historical framework. It is normally described through the set of transformations produced during childhood in the personal-social, emotional, linguistic, psychomotor, cognitive, and playful areas. Much of the research that has examined it offers evidence about the decisive influence it has on the overall health of people throughout life. For this reason, various countries consider it extremely necessary, first, including child development as a central dimension to approximate the index of well-being or quality of life of girls and boys and, second, to expand access and continuity in child development intervention programs, especially in at-risk populations. This chapter proposes to present a review of the studies referring to the development of girls and boys who belong to groups in vulnerable situations in Latin America and the metropolitan area of Buenos Aires, Argentina. The review is organized around four axes of analysis: (1) Approaching the study of child development in populations in vulnerable situations; (2) Instruments for the evaluation of child development; (3) Characteristics of child development in the populations under study; (4) Contributions and limitations of the child development study in the region. This chapter is expected to offer an integrative view of child development and contributes to focusing on activities to strengthen the mechanisms of approach and intervention in priority problems that affect girls and boys from vulnerable sectors.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Recently, scientific evidence has shown the decisive influence of childhood development on the integral health of people throughout life. For this reason, various countries recognize that it is extremely necessary, first, to include early childhood development as a central dimension to approximate the index of well-being or quality of life of girls and boys and, second, to expand access and continuity in intervention programs in child development, especially in populations in situations of social vulnerability.
Particularly in Latin America, where millions of households are going through a serious social situation (CEPAL, 2021), population studies on child development are essential to estimate children’s abilities, skills and knowledge in relation to what is expected at different ages, and to count with useful elements that serve to design promotion strategies and/or intervention in the development of children.
Conceptualizations About Child Psychological Development
In the history of psychology, there have been various proposed conceptions of psychological development. Although these conceptions agree in defining it as a complex process that involves a set of changes produced during the first years of life, they differ with regard to describing and explaining how these changes occur.
Traditionally, the theoretical models that have predominated in psychological discipline have been the mechanistic and the organicist. The first, framed in behaviorist theory, maintains that psychological development lacks its own internal dynamics and is limited to being a succession of learning. The organicist emphasizes internal processes more than external ones and proposes the existence of an “evolutionary need” that makes development pass through certain phases or stages that constitute evolutionary universals in all people (Palacios, 1991).
Currently, the dialectical contextual model has become the frame of reference that includes a great variety of approaches and theoretical perspectives that assume a set of postulates related to development (Palacios & Mora, 2017; UNICEF, 2016):
-
1.
The extension of the development throughout the life of the subject, understanding it as a multidimensional, multidirectional, and contextualized process (Martí Sala, 1991).
-
2.
The relativity of chronological age, as by itself it is not a causal, descriptive, or explanatory factor.
-
3.
The action of a multiplicity of factors (normative graduated by age, normative graduated by history and non-normative events) that interact with each other in determining the changes (Pérez Pereira, 1995).
-
4.
The attribution of the active role of the subject, while insisting on the importance of sociocultural conditions to which a decisive influence is given in shaping the course of individual development (Gutiérrez Martínez, 2005).
The way of interpreting these postulates differs in the different theoretical perspectives, of which we can mention the ecological, the ethological, the cognitive-evolutionary, the information processing (with its most up-to-date versions such as connectionism), and the historical-cultural (Gutiérrez Martínez & Vila Chavez, 2011).
The historical-cultural approach, in which our own studies reported below are inscribed, conceives human development as the synthesis between the biological and the psychological, in a sociocultural and historical framework. On a psychobiological basis, ontogenetic development consists of the progressive appropriation of symbolic instruments and cultural competencies that enable interaction with others. In the words of Vygotsky (2006 [1930]), “it is a complex dialectical process, characterized by periodicity, irregularity in the development of different functions, metamorphosis or qualitative transformation from one form to another, the interrelation of external factors and internal and adaptive processes that overcome the obstacles that the one little crosses” (p. 116).
In the first 6 years of life, good nutrition and the quality of intersubjective activity take on a transcendental significance for children to unfold their full potential in terms of health and cognitive and socio-emotional capacities (Young, 2002).
During this period, opportune biological conditions are produced for the acquisition and construction of capacities and abilities in different areas of development. From neuroscience, the most current research on the subject provides abundant evidence for the massive increase in plastic and malleable neural networks, which change and evolve in relation to family and school contexts (García & Juanes, 2013; Barrios-Tao, 2016).
From the cultural-historical perspective, child development is a process located and crossed by cultural contexts and products that mediate its construction. In this sense, the context ceases to be an incident variable and becomes an inherent variable in the development and learning processes: the cultural practices in which these processes are situated are the conditions for their realization (Castellaro, 2017; Moreno Zavaleta, 2020). Specifically, the macrocontext (economic, political, and social context) defines the nature and scope of social policies that directly influence the well-being of families and children; the microcontext, that is, the interactions between the child and his caregivers, mediated mainly by language, originate a guided development process, thanks to which the infant appropriates the culture of his environment. In other words, the intersubjective activity, both in upbringing and in school practices, configures modes of socially, culturally, and historically situated development.
The availability of programs, services, and policies directed at children, their caregivers, or both, affect the quality of these interactions and, therefore, the course of development in childhood (Vegas & Santibáñez, 2010). As Tuñón and Salvia (2011) have mentioned, child development requires having a set of favorable economic, social, and cultural factors that allow children to live fully in terms of the full deployment of their human capacities. It is the obligation of the State and society to take care of and attend to the material, formative, and emotional conditions of children, including respect for their person, their family, and their culture. Hence, it is essential to diagnose the situation of children regarding their development and expand access to quality interventions, especially in populations that are living under vulnerable conditions.
Population Studies of Child Development in Latin America and Argentina
As can be inferred from the above, child development constitutes a great challenge for the countries of Latin America. Concerning the cognitive, linguistic, socio-emotional and motor dimensions, large gaps are observed between social groups of different socioeconomic status. Currently, information regarding child development assessments in our region is very limited, generally resulting from specific studies and not from systematic measurements. Additionally, it is mainly based on the areas of health and nutrition, with less knowledge about other areas such as cognitive and language development, socio-emotional and motor development of children under 6 years of age (Fiszbein et al., 2016).
One of the projects aimed at generating knowledge to promote public policies in the countries of the region is the Regional Program of Child Development Indicators (Engle et al., 2011), in which Costa Rica, Nicaragua, Paraguay, and Peru participate. It recognizes child development as a holistic and comprehensive process that brings together several interrelated dimensions including cognitive, language, emotional, health, social, motor skills, executive functioning, among others.
Within the framework of this program, new child development assessment instruments were created, built from items common to scales applied in the region (for example, Nelson Ortiz Pinilla’s Abridged Scale, the Comprehensive Child Development Scale) and items found in recent international assessments. These instruments include the Engle Scale (Verdisco et al., 2009), valid and reliable for examining cognitive, linguistic, socio-emotional, and motor development, aimed at children between 24 and 59 months of age from the four countries. Among the main results, the existing inequality in child development for 24 months of age stands out: inequalities between countries, between populations within countries, and between dimensions of development. Particularly in the cognitive and language/communication dimensions, the gaps are evident from the early years and increase with age. Additionally, they indicate strong correlations of the mother’s wealth and education index with the cognitive and language/communication dimensions. The home environment, which refers to indicators of family care, including the number of books per child in the home, the number of adults and the frequency with which they interact with the child, the routines implemented at home, and basic hygiene routines, appears with particular importance in all dimensions of child development (Verdisco et al., 2015).
With the same purpose of investigating the influence of home on the development of children, in Uruguay (López Bóo et al., 2019) some items of the subscales of Parental Response Capacity and Parental Sensitivity of the HOME inventory were implemented within the Survey of Nutrition, Child Development and Health (ENDIS) (Cabella et al., 2015). In this way, emotional aspects of the home environment were evaluated, and it was found that children from families with greater socioeconomic vulnerability are exposed to a lower quality environment (more punitive environments and with less capacity to respond to their needs). Additionally, it was found that the results obtained correlate with the level of child development.
For its part, to have an instrument of local value, Mexico has developed the Infant Development Assessment (EDI) test in 2013 (Instituto Nacional de Perinatología, 2013). It consists of a developmental screening for children under 5 years of age that assesses the areas of fine and gross motor skills, language, social, and adaptive skills. It returns the following possible outcomes:
-
1.
Normal development (classified as “green”), that is, the child has reached the developmental milestones corresponding to their age group.
-
2.
Developmental delay (classified as “yellow”), when the child has not reached the developmental milestones corresponding to its age group, but does meet the milestones of the previous age; there are no red flags and the neurological examination are normal.
-
3.
Risk of delay (classified as “red”), the child has not reached the milestones of the age group to which it belongs or those of the immediate previous group, or because it presents an alteration in the neurological examination or has warning signs (Instituto Nacional de Perinatología, 2013).
In order to test validity and reliability, Rizzoli-Córdoba et al. (2014) conducted a cross-sectional study that included a total of 438 children from different regions of the country with and without risk of developmental delay (biological risk: n = 197, 45%), environmental risk (n = 137, 31.3%), and no risk (n = 104, 23.7%). They considered diagnostic tests, the Battelle Developmental Inventory-2 (Newborg, 2004) and Bayley-III (Bayley, 2006), finding that the EDI has adequate properties and similar to the tests most used in the USA (Rizzoli-Córdoba et al., 2013, 2014). Of the 438 participants, 41.3% (n = 181) obtained a normal result (green). The remainder had results indicating developmental delay (yellow) or alertness (red) (56% [n = 144] and the remaining 44% [n = 113] respectively). Among children with delay, 86.8% had at least one affected domain and 50% had three or more affected domains, compared with the group at risk (red), which presented 93.8% and 78.8% correspondingly, allowing the identification of different magnitudes of the problems and, consequently, promoting differentiated interventions (Rizzoli-Córdoba et al., 2014).
In Colombia, there is the Abbreviated Development Scale (EAD) (Ortiz Pinilla, 1999), an instrument nationally validated by the Colombian Ministry of Health and the United Nations Children’s Fund (UNICEF), and standardized for its population. This scale has been updated and revised twice, the current iteration being the EAD-3 (PUJ Facultad Medicina, 2016). Its objective is to identify, early, the risk of delays in the development of Spanish-speaking Colombian children up to 7 years of age, through the areas of hearing-language, personal-social, and fine and gross motor skills. It allows the comparison of the guidelines approved by the child with a normative reference group being expected to pass through most of the items in their age range. Studies that used this scale in children under 5 years with associated risk factors (Castaño et al., 2019; Suárez Sanabria & García Paz, 2017) have found a high number of cases with development problems. Castaño et al. reported that 27.7% of the children evaluated (54 healthy children aged 1–5 years) presented a level of alertness in the global characteristics of psychomotor development, language being the area of development most affected (37%). Similar results are those expressed by Suárez Sanabria and García Paz (2017), who evaluated 60 children under 5 years of age with malnutrition, finding a prevalence of the risk of delay of 38.3%.
In Chile, starting in the 1990s, the evaluation of psychosocial development was incorporated into pediatric control through the implementation of a program to stimulate and evaluate psychomotor development in children under 6 years of age, which used standardized instruments and a scale of clinical screening: the Brief Guideline for Development Assessment and Psychomotor Development Assessment Scale (EEDP) (Rodríguez et al., 1976) for children under 2 years of age and the Psychomotor Development Test (TEPSI) (Haeussler & Marchant, 2003) for children between 2 and 5 years of age (Bedregal, 2008). During 2007, they started the child protection program “Chile Grows with You,” which aimed to offer the child population an integrated system of interventions and social services that support the biopsychosocial development of children and their families, from pregnancy to their schooling, to reduce inequities (Bedregal et al., 2016). In a study where the results of evaluations of psychomotor development within the framework of the program are exposed, between 2008 and 2011 (Atalah et al., 2014), they found a 5% prevalence of developmental delay or risk in children. The children evaluated had a recovery rate close to 50% and there was a slight increase in the prevalence of lag in children under 2 years of age (0.6%). In the period reported, the average number of children under 3 years of age controlled by the program was 505,471 (67.4% of the Chilean population of that age), which corresponds to the annual application of about 350,000 tests to assess psychomotor development.
In 2006, Argentina added a specific module to the Social Debt Survey (EDSA) with the aim of evaluating the level of compliance with the rights of the child, as well as the social and human development of children and adolescents (Tuñon & Fourcade, 2019). This survey was designed to collect data on households and individuals in the most significant urban conglomerates in the country.Footnote 1 In the case of the module for childhood, the mother, father, or guardian of children from 0 to 17 years old who live in the home answered the questions. Tuñon (2018) presented the results obtained for children from 0 to 12 years old, whose families participated in the EDSA in 2017. Indicators of emotional, social, and intellectual stimulation were analyzed as a way of approaching child development through the characteristics of their parenting and socialization context. The seven indicators included were:
-
1.
Sharing of a bed or mattress.
-
2.
Sharing of stories and/or oral histories as a family.
-
3.
Presence of children’s books in the home.
-
4.
Birthday celebrations.
-
5.
Parenting styles (homes in which physical, verbal aggression or penance is used to discipline).
-
6.
Access to extracurricular sports activities.
-
7.
Access to extracurricular artistic activities.
Among the most relevant results, it was found that 4 out of 10 children are not usually told oral stories and that this percentage increases as the children grow older. Furthermore, when the child belongs to families of the marginal working stratum, they are twice as likely not to be a recipient of oral histories than a peer in the middle professional stratum. Regarding the deficit of books at home, it affects 40% of children and the percentage is higher in children and boys. The inequality gap with respect to this indicator increases up to six times when the child belongs to the marginal worker stratum. The absence of a birthday celebration affects 17% of children with a regressive inequality gap of nine times for children from the most vulnerable sector. Regarding extracurricular socialization activities, the 2017 measurement showed that 60% of children and adolescents between 5 and 17 years old do not practice sports or physical activity outside school, whereas in the case of artistic activities, this percentage grows to 85%.
Also in Argentina, Horacio Lejarraga and collaborators conducted various studies on child development in vulnerable populations in different areas of the Buenos Aires metropolitan area (AMBA).Footnote 2 Part of these studies consisted of creating and validating, in our country, the National Research Test (PRUNAPE, acronym in Spanish of Prueba Nacional de Pesquisa) developed by Lejarraga et al. (Jumbo Salazar et al., 2021; Lejarraga et al., 2013, 2018b) that conceives the development process as the course of changes in sensory-motor behavior, emotional response, intelligence, language, and learning. It is a screening or research instrument that allows identification of the presence of risk in psychomotor development from 0 to 6 years of age. The instrument assesses 78 development guidelines grouped and ordered into four areas: personal-social (PS), fine motor skills (MF), language (L), and gross motor skills (MG), based on the increasing compliance with the guidelines as they advance in chronological age. The items are differentiated according to whether they are type A or B guidelines and are determined according to the chronological age of the children evaluated; all the B guidelines and three guidelines must be evaluated in each area. Type A patterns are those that exceeded the normative sample by 90%, whereas type B guidelines are between the 75 and 90 percentiles. Therefore, noncompliance with a type A guideline is always at a higher risk than noncompliance with a type B guideline. Any child who passes all type A guidelines or who fails only one type B guideline is classified as normal. Otherwise, the child is classified as at risk.
During the period 2004–2005, a study was carried out in three health centers in the town of San Isidro, belonging to the AMBA, which served populations from different socioeconomic contexts (Lejarraga et al., 2008). Two of them served communities in the center of the locality where either the level of unemployment was high (Center A), or the families had more stable jobs but had a low income (Center B). The third center (C) served the middle-class population. In each center, the first five children who attended on a particular day of the week were selected and who met the two inclusion criteria: being under 6 years of age and having no chronic or acute diseases. The participating children were evaluated through PRUNAPE and those who did not pass the test were referred to the San Isidro Maternal and Child Hospital where a multidisciplinary team was made available to conduct in-depth developmental evaluations and offer diagnosis and follow-up. Among the most relevant results, the authors found a high prevalence of children who did not pass the test (20%; 24% Center A, 19% Center B, and 16% Center C). Furthermore, a significant percentage of children either did not attend or did not complete the diagnostic process when they were referred to the Maternal and Child Hospital (43%). When exploring the socioeconomic characteristics of those families that did not complete the diagnostic process, the authors found a higher prevalence of high-risk families (families in vulnerable situations). Alternatively, among the children who were referred to the hospital and completed the process, the diagnosis of global developmental disorder was predominantly found. Finally, four risk factors for development were identified (risk of failing the PRUNAPE): the mother’s educational level, male gender, pregnancies with complications, and the age of the child (the older the child, the higher the risk).
Lejarraga and his group of researchers (2014) also participated in the implementation of a series of surveys conducted from 2010 on families with unsatisfied basic needs in the region known as Cuenca Matanza Riachuelo and in the town of Florencio Varela (both belonging to the AMBA). Through these, it was sought to evaluate, among other aspects, the risk of suffering inapparent developmental problems in children under 6 years of age and to be able to identify determinants associated with said risk. The 7844 participating children were evaluated either through a selection of 13 PRUNAPE guidelines, or through the PRUNAPE Pre-Screening Questionnaire (CPPP), which consists of a series of questions that the mother or caregiver must answer about the skills that PRUNAPE investigates. The analysis of the results obtained allowed us to find a high proportion of children at risk of developmental problems (34.8%) and a higher prevalence in males. Likewise, the results showed a marked delay in development and a progressive trend of this delay until the age of 4 years. Strong relationships were found with birth weight, gestation duration, and the mother’s literacy skills in terms of possible risk determinants (Lejarraga et al., 2014).
In 2018, based on Gesell’s (Ames, 1940) concept of “developmental tempo” (the speed at which a child achieves one pattern after another), Lejarraga et al. (2018a) analyzed the data obtained in the previous study to describe these “tempos” when environmental conditions are unfavorable. The analysis allowed three phases to be identified: a first phase between birth and 270 days with normal development, in which the median age of compliance with the guidelines was like that of the national reference; a second phase of progressive developmental delay; and the third recovery phase from 1260 days. Lejarraga attributed the normal development time during the first year of life to maternal care, which appears to constitute protective factors. After the first year, maternal and family care is not enough to protect the child from unfavorable environmental factors, which would explain why a slower maturation time appears in the second phase. The recovery that characterizes the third phase is associated, according to the authors, with the attendance of children from 4 years of age at kindergarten or care centers (Lejarraga et al., 2018a).
Another of the lines of research that address the issue of vulnerability and child cognitive development in Argentina is that of the works of Lipina and collaborators. Recently, they have investigated the influence of poverty on child development, analyzing its effects and relationship with alterations in the growth and development of different cognitive skills (Lipina, 2008). From this perspective, they propose studying the influence of poverty on cognitive development using a comprehensive and multidisciplinary approach (Lipina, 2017). Concerning studies with local children in this group, some of their most outstanding current works are described below.
In 2017, Prats et al. conducted a cross-sectional study to evaluate the relationship between children’s cognitive performance in different tasks and various individual and contextual factors. With this objective, they evaluated 46 children aged 5 years from homes with unsatisfied basic needs (UBNs), with no history of developmental disorder, concurrently with a public kindergarten in the La Boca neighborhood of the Ciudad Autónoma de Buenos Aires (CABA). They administered the following instruments:
-
Session 1. (a) Expressive vocabulary (K-BIT) , which assesses processes of verbal intelligence (Kaufman & Kaufman, 1983); (b) Heart-flower stroke, which assesses cognitive flexibility, inhibitory control (Davidson et al., 2006); (c) K-ABC Digit Repetition Sub-Test, which evaluates working memory (Kaufman & Kaufman, 2002).
-
Session 2. (d) Matrices (K-Bit), which evaluate fluid thinking (Kaufman & Kaufman, 1983).
-
Session 3. (e) Attention network test (ANT), which evaluates attentional processes (Rueda et al., 2004); (f) Corsi blocks, which assess spatial working memory (Pickering, 2001).
For individual factors, they took a saliva sample to measure cortisol and measured EEG activity; they also conducted an interview with mothers and observed a game situation (parenting practices and language complexity). For contextual subjects, they considered insufficient income, based on the concept of UBN. Among the main results, they found that the factors with the greatest association with cognitive performance were neural connectivity/power and the mother tongue. The findings of this study are in connection with those found in the literature on the subject.
In line with this work, Hermida et al. (2019) conducted a comparative study between two groups of children with UBN, a group from a rural context and another from an urban context. A total of 131 participating children, attending two public schools in Buenos Aires and two public schools in Santiago del Estero, were evaluated at age 5 with cognitive tasks and individual and environmental variables. In this way, they investigated how poverty and rural or urban environments affect children’s cognitive performance. For the same level of UBN, children from rural settings performed worse than those from urban settings. Such differences could be mainly attributed to the months of preschool attendance and the complete level of parental education. As in the aforementioned work, the authors point out that the results obtained indicate that they should promote policies and programs for children living in rural poverty throughout the world, and especially in Latin America (Hermida et al., 2019; Prats et al., 2017).
In 2017, the Facultad Latinoamericana de Ciencias Sociales (FLACSO), conducted an assessment of the effects of the Centros de Primera Infancia Program (Early Childhood Centers) that operate in CABA and created in 2009 by civil society organizations meeting with the Ministerio de Desarrollo Humano y Hábitat (Ministry of Human Development and Habitat) of Buenos Aires City. It consists of 76 centers serving children from 45 days to 4 years of age providing food and educational service in 8-h days. The study was conducted on 456 children aged 3 years and included, among other variables, the developmental assessment using the Battelle 2 test (Newborg, 2004). From the 13 centers selected for the show, six were in vulnerable neighborhoods attended exclusively by children living there and seven were in more heterogeneous neighborhoods, although the children attending were from families living under conditions of significant social vulnerability. Among the most relevant results regarding developmental assessment, one in four children were found to have a risk of developmental delay. The area where the greatest risk was found was cognitive, whereas the adaptive area had the lowest frequency of at-risk cases. Analyzing the presence of factors associated with better development scores, it was found that attendance time at centers for more than 1 year involved improvements in all areas of development evaluated. Other factors associated with better scores were the educational level of the parents and the parenting style. In contrast, factors identified as higher developmental risk partners were male life, attending centers in vulnerable neighborhoods, living in overcrowded conditions, having moved three times in the past 3 years, preterm birth, hospital stays of at least 15 days, and the presence of postpartum mother depression (Fondo de las Naciones Unidas para la Infancia, 2019).
Most Popular Child Development Assessment Tools in Latin America
The child development assessment is normally aimed at investigating the presence or absence of risk. Individually, if a risk is detected, a psychological examination will be deepened with specific tests, and it will be decided whether a professional intervention is necessary (Castro Solano, 2017). At the population level, it will allow information to be used to design and implement actions aimed at promoting development, especially for children at socioeconomic disadvantage. Thus, the evaluation and monitoring of development in the first years of life consist of:
-
1.
Developmental monitoring corresponds to systematic observations of children conducted by professionals, during health control, and encompasses all activities related to the promotion of normal development and the detection of developmental problems in primary health care.
-
2.
Screening is a tool that identifies children at risk in their development in a supposedly healthy population.
-
3.
Developmental assessment is a more detailed investigation of children with suspected developmental problems (Vericat & Orden, 2010).
To conduct these actions there are different techniques and methods, such as surveys of parents or caregivers, direct observation of the child, screening tests, and developmental scales.
Table 4.1 shows a register of early childhood development assessment tools created or adapted in Latin America. From the bibliographic study performed and presented in the previous section, it has been possible to select those tests that, by their characteristics, are suitable, effective, and suitable for the regional and local populations, both for research activities and for professional practice.
Findings and Contributions from Our Line of Research
The study on child growth and development at the local level was opened with the “Estrategias de Alimentación, Crianza y Desarrollo Infantil (Child feeding, parenting, and development strategies)” project carried out during 1986–1989, with financial support from Canada’s International Development Research Center (IDRC), the Scientific Research Commission of Buenos Aires, Argentina, and UNICEF’s technical and financial assistance. This project focused on the research of the characteristics of families living in settlements in Gran La Plata and Gran Buenos Aires, under the hypothesis that poverty did not shape a homogeneous condition, with differences linked to the psychological development and nutritional status of children from 0 to 5 years (Piacente et al., 1990).
This research, which was pioneering in the area and in the region, opened up a line of investigation that continued years later with the impact assessment of the Plan más Vida,Footnote 3 by the Scientific Research Commission of Buenos Aires. This evaluation consisted of the administration of a series of surveys and psychological tests by cross-sections of representative samples of families in the suburbs of Buenos Aires, aimed at examining food, nutrition, upbringing, child psychological development, and literacy (CIC, 2008). Against this background, in 2017 the project “Infancia y derechos sociales. Condiciones de vida, cuidados, estado nutricional y desarrollo infantil en el Gran La Plata”Footnote 4 had the objective of assessing the conditions of domestic and extra-domestic care in children attending the initial level of public schools of Gran La Plata and evaluating their nutritional status and psychological development.
The results set out here correspond to one of the studies of the project, more specifically that dedicated to describing and analyzing the psychomotor and socio-emotional development of 5-year-olds of the Gran La Plata. Two sources of information were used: the direct evaluation and observation of children and the parent survey. It was also proposed to relate the results obtained from these sources to family practices reported by caregivers. The interest of this work lies in the importance of having an up-to-date diagnosis of child development in the Gran La Plata because, first, it is considered an essential dimension for approaching the child welfare index and an indicator of the quality of life of children from the perspective of human rights (Brooks & Hanafin, 2005; Colacce & Tenenbaum, 2018); second, the scarcity of such studies at the local level. This diagnosis is essential to ensure that all children have access to quality early childhood development care and preschool education, so that they are prepared for primary education (UNESCO, 2019).
Our research involved 728 children and their families concurrent with the last initial public education level of the Gran La Plata. The distribution of the participants according to the locality of residence of the kindergarten respected the current census information, being formed as follows: 35 from Ensenada, 77 from Berisso, and 616 from La Plata. It should be clarified that the population who attends these educational institutions is of low average and low socioeconomic status. It was observed that the participating children had a chronological age of less than 6 years (mean = 65.5, SD = 3.53) and did not present apparent alterations in development, whereas the research used allows risk to be detected in a presumably healthy population.
To assess psychomotor development, the PRUNAPE (Lejarraga et al., 2013) was used. To examine socio-emotional development, we used the Ages & Stages Questionnaires: Socio-Emotional Second Edition (ASQ: SE 2) (Squires et al., 2015). The questionnaire for parents was attached to the “Encuesta sobre Condiciones de Cuidado y Crianza” (“Survey on Care and Parenting Conditions”), developed for this project to inquire about household data, as well as knowledge and practices related to food, health, child development, and childcare.
In the case of the PRUNAPE, between 12 and 16 items were evaluated. The items considered for the ages studied are presented in Table 4.2. Compliance with the guidelines qualifies the development of children as “normal” or “at risk.” It should be clarified that the test is a screening, so it does not thoroughly explore each component of development and does not produce diagnostic categories. The administration of PRUNAPE consisted of an individual session of approximately 20 min, held in the school establishments that collaborated in the study. The results were personally returned to parents and in cases detected as being “at risk,” an offer was made to replicate and deepen the evaluation.
On the other hand, ASQ:SE 2 is a screening of American origin, adapted into Spanish. It consists of nine multiple choice questionnaires to complete per parent or primary caregiver of the child, which examines the socio-emotional development of 1–72 months of age. The questions that make up these questionnaires address seven areas:
-
1.
Self-regulation (calming down, reassuring, or adjusting to psychological or environmental conditions).
-
2.
Compliance (obeying orders and complying with instructions given by others).
-
3.
Adaptive operation (dealing with needs such as sleeping, eating, going to the bathroom, etc.).
-
4.
Autonomy (initiating some action by itself or responding to others without instructions).
-
5.
Affection (showing your own feelings and empathy for others).
-
6.
Communication (responding to or initiating verbal or nonverbal signals indicating feelings, affections, or internal states).
-
7.
Interaction with persons (responding to or initiating social responses to parents, other adults or peers).
The scores obtained are added up and the total is compared with a cut-off point set by age. This cut-off point delimits qualitative categories:
-
1.
Below the cut-off point, socio-emotional development is within expectations.
-
2.
Close to the cut-off point, the child requires additional monitoring and follow-up actions.
-
3.
Above the cut-off point, is at risk, requires a more thorough evaluation and eventually, an intervention.
In this study, it was decided to work with dichotomic categories, grouping the 2 and 3: “within what is expected” and “should be observed and/or thoroughly evaluated.”
Psychomotor and Socio-Emotional Development
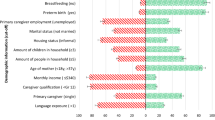
The administration of the PRUNAPE in the Gran La Plata yielded the following results: 72.1% of participants achieved the expected psychomotor development guidelines for age, whereas 27.9% did not, ranking in the risk category. Children identified as being at risk had a higher number of faults in the language areas (33.8%) and the fine motor skills (23.1%) (Fig. 4.1), particularly in type A guidelines, i.e., those that are approved by more than 90% of the population of that age range: “use two objects” and “fold a piece paper diagonally,” respectively.

Most affected psychomotor development areas
As for the results obtained from the administration of ASQ:SE 2, it was found that in the Gran La Plata 77.2% of caregivers report child behaviors that place children within what is expected in socio-emotional development, whereas 22.8% manifest the presence of socio-emotional behaviors that require monitoring and/or thorough evaluation. This percentage is lower than that reported by the authors of the questionnaire (Squires et al., 2015): from the normative sample 31.1% were placed in the at-risk category.
Comparing the overall results of both tests (N728), of children passing the PRUNAPE (72.1%), 78% get an outcome within what is expected and 22% require follow-up in socio-emotional development. These proportions are maintained among those who do not pass the PRUNAPE (Table 4.3).
Factors Associated with Psychomotor and Socio-Emotional Development
The associations between the qualitative categories of PRUNAPE (normal to at risk) and ASQ: SE 2 (within expected to observe/consult) and the variables “gender,” “maternal education level,” “family practices with children,” “characteristics of children,” and “family concerns regarding the development of the child” were analyzed.
-
1.
Gender and psychomotor/socio-emotional development. Differences in child development were observed according to gender, being significantly in favor of girls in psychomotor development (Table 4.4).
-
2.
Maternal education level and psychomotor/socio-emotional development. The maternal educational level has been used as a proxy variable of the socioeconomic level of families, a variable widely used in Argentina and in the region (General Directorate of Statistics and Censuses [DGEyC], 2017). It is noted that as the years of maternal education increase, the percentages of children at risk decrease, with a noticeable positive difference being made for the children of mothers with an education over 16 years of age (Table 4.5).
-
3.
Family practices with children and psychomotor/socio-emotional development. From the data collected in the family surveys, composite variables were developed that refer to different practices of caregivers with children. These practices were categorized into appropriate/inadequate, according to their presence and how often they are performed (Table 4.6).
Concerning family development promotion practices, they were considered appropriate when performing three or four of the following activities: singing songs, playing with the child, telling the child stories, reading stories to the child, offering pencil and paper and other materials, taking the child for a walk, and offering the child children’s books, provided that present among them was “play with the child.” Of the total practices reported, 49% were adequate and 51% were inadequate. In terms of psychomotor development, among families reporting appropriate development promotion practices, 66.4% passed the psychomotor development assessment and 77% obtained results within what is expected for ASQ: SE 2.
For the home literacy context, the following practices were particularly considered: reading stories, offering pencil and paper, and children’s books. Just over two-thirds (67.8%) of the parents reported adequate practices. There were no significant differences between children who qualify as being at risk and those who do not, in relation to literacy practices reported by parents.
-
4.
Characteristics of children and psychomotor/socio-emotional development. Children’s characteristics include the variables “pre-reading knowledge,” “motivation for reading,” “socialization,” an×d “play.”
The association between the pre-reading knowledge (for example, recognizing some letters, reading familiar words, distinguishing letters from numbers), and psychomotor development was significant (×2 = 9.95, p = 0.002). In Table 4.6, it can be seen that children with knowledge and pre-reading practices suitable for their school level (83%) also had psychomotor development suitable for their chronological age.
Among children with suspected risk in their psychomotor development, 33.8% of the pre-reading knowledge was inadequate. Moreover, the four variables included in the “Child Characteristics” dimension were significantly associated with socio-emotional development. Among children who were within what is expected in socio-emotional and psychomotor development, the families carried out greater appropriate play and socialization activities.
-
5.
Family concerns and psychomotor/socio-emotional development. Most of the families who answered the survey did not express concern about the development of their children (85%). In these cases, where parents were not concerned, 25% did not pass the PRUNAPE. Regarding socio-emotional development, it was noted that for families who did not express concerns about development, 19.4% were not within what is expected, whereas for those whose parents were concerned, 39% should have had a follow up (Table 4.7).
Table 4.8 presents the percentages of parents reporting concerns about their children’s habits and development, based on the results obtained in the different assessments. It should be clarified that of all the responses from parents who claim to be concerned, 47% refer to developmental problems, 21.8% to developmental delays, and the remaining 15.9% to habits (absence or presence of inappropriate habits) .
Final Considerations and Perspective
This chapter presented a powerful overview of population child development studies in Latin America and the metropolitan area of Buenos Aires (Argentina), particularly for children with social vulnerability. This review has delved into our own research, which has been carried out in recent years.
The information reported by the literature consulted provides empirical evidence about the at-risk situation that is recorded very early in the psychological development of children. However, the situation is not the same in the various Latin American countries and between populations within each country: the percentages of children at risk with regard to development vary within a range of 20–40%. Concerning developmental dimensions, the research agrees to point to language as the most affected area of child development.
Another highlight of the bibliographic review is the elaboration of a register of child development assessment tools used in Latin America. This list provides information about up-to-date tests that, because of their characteristics, are suitable, effective, and appropriate for the regional and local population, both for research activities and for professional practice.
As for our research, coinciding with the range reported by Latin American studies, it has been observed that 27.9% of the children evaluated are at risk regarding psychomotor development and 22.8% regarding socio-emotional development. These percentages are similar to the proportions reported by the studies by Lejarraga and collaborators (2014, 2018a) with children of 0–6 years of age carried out in primary care facilities in different locations of the Buenos Aires suburbs and CABA, which show that between 20% and 35% of the population has developmental disorders (SAP, 2016). However, it should be emphasized that the percentages found in our study are close to the upper limit of that range.
The area that has been recorded as the most sensitive to risk in childhood development has been language. This is consistent with regional findings that mention language and cognition as the dimensions most affected by social vulnerability (Verdisco et al., 2015).
As for the results in the PRUNAPE and ASQ:SE 2, in addition to the discrepancies recorded in the at-risk percentages, the subjects who were at risk were not the same in both tests: of the group of children who did not pass the PRUNAPE, 26% also did not pass ASQ:SE 2.
This is possibly linked, first, to the assessment of diverse psychological constructs, so that risk in psychomotor development does not pose a risk in socio-emotional development and vice versa. Second, it could be because the latter instrument is a questionnaire for caregivers, which requires certain parental skills to observe, perceive, and identify behaviors that indicate developmental delays or alterations early. This is in continuity with the low percentage of caregivers (15%) that raises concerns about the development of their children.
In line with what has been reported in previous research carried out in other regions of the AMBA (Lejarraga et al., 2008; UNICEF, 2019), the child’s male gender appears to be associated with an increased risk of developmental problems. Similarly, our study shows that as the mother’s educational level increases, there is a significant decrease in the percentage of children at risk of developing developmental problems. This coincides with the findings of the two studies mentioned, as well as the Regional Programme of Child Development Indicators (Engle et al., 2011).
On the other hand, it was recorded that psychomotor development and socio-emotional development correlate significantly with child characteristics such as the presence of pre-reading knowledge, motivation for reading, socialization, and play with other children. Not so with family practices promoting development and literacy, as reported by the Regional Programme of Child Development Indicators (Engle et al., 2011; Verdisco et al., 2015) and Uruguayan studies (López Bóo et al., 2019). After analyzing these results, it is possible to suggest that in the ages under study in our research, which correspond to the last year of preschool, the factors linked to school contexts have a greater impact on children’s development than family factors.
We believe that a considerable contribution from our study is the fact that it delivers results obtained both from a specific developmental test administered to children and from parental reporting tools that consider contextual factors, which greatly enriches the evaluations carried out. In this sense, it is necessary to recall the importance of multi-forming child evaluation, i.e., include different sources such as information given by the child’s parents, caregivers, and observers; multicontext, taking into account how different contexts assume different roles and influence child behavior; multitechnical and multimethod, i.e., that the approach to the psychology of the child is through different techniques that respond to different levels of inference (Castro Solano, 2017).
Finally, it should be noted that studies of child development in our region, including our own, have so far been cross-cutting, given the difficulties involved in longitudinal studies at the population level in unfavorable contexts. We agree with Lejarraga et al. (2018a) on the importance of starting to implement longitudinal research to confirm the incidence of protective factors for child development, such as assistance to schools and care, which are detached from the studies carried out so far.
Notes
- 1.
Metropolitan Area of Gran Buenos Aires, Gran Córdoba, Gran Rosario, Gran Mendoza y San Rafael, Gran Salta, Gran Tucumán y Tafí Viejo, Mar del Plata, Gran Paraná, Gran San Juan, Gran Resistencia, Neuquén-Plottier, Zárate, Goya, La Rioja, Comodoro Rivadavia, Ushuaia, and Río Grande.
- 2.
Metropolitan Area of Buenos Aires (AMBA): is the common urban area that makes up the Autonomous City of Buenos Aires (CABA) and 40 municipalities of the Province of Buenos Aires, including La Plata, Berisso, and Ensenada, which make up in turn the urban conglomerate “Gran La Plata.”
- 3.
Food program under the Ministerio de Desarrollo Social (Ministry of Social Development) of the Government of the province of Buenos Aires. Its objective is to ensure the basic feeding of the living-child population at risk through the nutritional reinforcement of pregnant women and children.
- 4.
Oriented Research Project, Consejo Nacional de Investigaciones Científicas y Técnicas – CONICET (National Council for Scientific and Technical Research) and Comisión de Investigaciones Científicas – CIC (Scientific Research Commission of Buenos Aires). Directora: Dr. Susana Ortale; Codirector: Mg. Javier Santos.
References
Accardo, P. J., & Capute, A. J. (2005). The capute scales: Cognitive adaptive test/clinical linguistic & auditory milestone scale (CAT/CLAMS). Brookes Publishing.
Ames, L. B. (1940). The constancy of psychomotor tempo in individual infants. Pedagogical Seminary and Journal of Genetic Psychology, 57, 445–450.
Atalah, E., Cordero, M., Guerra, M. E., Quezada, S., Carrasco, X., & Romo, M. (2014). Monitoreo de los indicadores del programa “Chile Crece Contigo” 2008–2011 [Monitoring indicators of the program “Chile Grows with you” 2008–2011]. Revista Chilena de Pediatría, 85(5), 569–577. https://doi.org/10.4067/S0370-41062014000500007
Barrios-Tao, H. (2016). Neurociencias, educación y entorno sociocultural [Neurosciences, education and sociocultural environment]. Educación y Educadores, 19(3), 395–415. https://doi.org/10.5294/edu.2016.19.3.5
Bayley, N. (2006). In N. Bayley (Ed.), Bayley scales of infant and toddler development (3rd ed.). Pearson.
Bedregal, P. (2008). Instrumentos de medición del desarrollo en Chile [Development measurement instruments in Chile]. Revista Chilena de Pediatría, 79, 32–36. https://doi.org/10.4067/S0370-41062008000700006
Bedregal, P., Hernández, V., Mingo, M. V., Castañón, C., Valenzuela, P., Moore, R., & Castro, D. (2016). Desigualdades en desarrollo infantil temprano entre prestadores públicos y privados de salud y factores asociados en la Región Metropolitana de Chile [Inequalities in early childhood development between public and private health providers and associated factors in the Metropolitan Region of Chile]. Revista Chilena de Pediatría, 87(5), 351–358. https://doi.org/10.1016/j.rchipe.2016.02.008
Brooks, A. M., & Hanafin, S. (2005). Report on the development of a national set of child well-being indicators in Ireland. The National Children’s Office.
Cabella, W., De Rosa, M., Failache, E., Fitermann, P., Katzkowicz, N., Mila, J., Nathan, M., Nocetto, A., Pardo, I., Perazzo, I., Salas, G., Salmentón, M., Severi, C., & Vigorito, A. (2015). Salud, Nutrición y Desarrollo en la Primera Infancia en Uruguay, Primeros resultados de la ENDIS [Health, nutrition and development in early childhood in Uruguay, first results of ENDIS]. OPP, INE, FCEA.
Castaño, P., Duarte, S., Gelves, M., Gálvez, N., & Pérez, J. (2019). Perfil psicomotor y factores de riesgo pre, peri y postnatales en preescolares [Psychomotor profile and pre, peri and postnatal risk factors in preschool children]. Revista de Investigación e Innovación en Ciencias de la Salud, 1(2), 32–37. https://doi.org/10.46634/riics.20
Castellaro, M. (2017). La interacción social como clave del desarrollo cognitivo: Aportes del socioconstructivismo a la Psicología [Social interaction as a key to cognitive development: Contributions of socio-constructivism to psychology]. Revista de Psicología Digital, 4(9), 1–14. https://ri.conicet.gov.ar/handle/11336/67301
Castro Solano, A. (2017). La evaluación psicológica infantil. Aspectos conceptuales [Child psychological evaluation. Conceptual aspects]. In A. Castro Solano & M. Fernández Liporace (Eds.), La evaluación psicológica en niños. Técnicas de screening y diagnóstico (pp. 21–40). Paidós.
Castro Solano, A., & D’Anna, A. (2017). El Screening Neuropsicológico para Niños (SNN-UBA) [Neuropsychological screening for children]. In A. Castro Solano & M. Fernández Liporace (Eds.), La evaluación psicológica en niños. Técnicas de screening y diagnóstico (pp. 227–253). Paidós.
CEPAL. (2021). Panorama social de América Latina, 2020 [Social Panorama of Latin America, 2020]. Naciones Unidas.
Colacce, M., & Tenenbaum, V. (2018). Las dimensiones del bienestar infantil y la focalización de los programas dirigidos a la primera infancia [The dimensions of child well-being and the targeting of programs aimed at early childhood]. CEPAL.
Comisión de Investigaciones Científicas (CIC). (2008). Evaluación de impacto Plan Más Vida [Impact evaluation of the Plan Más Vida]. Ministerio de Desarrollo Social, Provincia de Buenos Aires, Argentina.
Davidson, M. C., Amso, D., Anderson, L. C., & Diamond, A. (2006). Development of cognitive control and executive functions from 4 to 13 years: Evidence from manipulations of memory, inhibition, and task switching. Neuropsychologia, 44(11), 2037–2078. https://doi.org/10.1016/j.neuropsychologia.2006.02.006
Dirección General de Estadísticas y Censos (DGEyC). (2017). Población de Buenos Aires [Population of Buenos Aires]. Revista Semestral de Datos y Estudios Sociodemográficos Urbanos, 14(26), 1. Gobierno de la Ciudad de Buenos Aires, Argentina.
Edwards, M., & Pardo, M. (2013). Test de Aprendizaje y Desarrollo Infantil (TADI) [Child learning and development test (TADI)]. Editorial Universitaria.
Engle, P., Cueto, S., Ortíz, M. L., & Verdisco, A. (2011). Programa Regional de Indicadores de Desarrollo Infantil (PRIDI): Marco conceptual [Regional programme for child development indicators: Conceptual framework], pp. 1–32. https://publications.iadb.org/en/publication/15178/programa-regional-de-indicadores-de-desarrollo-infantil-pridi-marco-conceptual
Fiszbein, A., Guerrero, G., & Rojas, V. (2016). Medición del desarrollo infantil en América Latina: construyendo una agenda regional [Measuring child development in Latin America: Building a regional agenda]. Diálogo Interamericano.
Fondo de las Naciones Unidas para la Infancia (UNICEF). (2019). Informe sobre evaluación de efectos del Programa CPI: un estudio muestral [Report on the evaluation of the effects of the CPI Program: A sample study]. https://www.unicef.org/argentina/media/5701/file/Evaluaci%C3%B3n%20de%20efectos%20del%20Programa%20CPI.pdf
Frankenburg, W. K., Dodds, J., Archer, P., Shapiro, H., & Bresnick, B. (2003). DENVER II. In Assessing children’s well-being: A handbook of measures (p. 83).
García, J., & Juanes, J. A. (2013). El cerebro y las TIC [The brain and ICT]. Teoría de la Educación Educación y Cultura en la Sociedad de la Información, 14(2), 42–84. https://dialnet.unirioja.es/servlet/articulo?codigo=4350893
Gutiérrez Martínez, F. (2005). Teorías del desarrollo cognitivo [Theories of cognitive development]. UNED.
Gutiérrez Martínez, F., & Vila Chavez, J. (2011). Psicología del desarrollo II [Developmental psychology II]. UNED.
Haeussler, I. M., & Marchant, T. (2003). Tepsi. Test de Desarrollo Psicomotor 2–5 años [Tepsi. Psychomotor development test 2–5 years] (10th ed.). Universidad Católica de Chile.
Hermida, M. J., Shalom, D. E., Segretin, M. S., Goldin, A. P., Abril, M. C., Lipina, S. J., & Sigman, M. (2019). Risks for child cognitive development in rural contexts. Frontiers in Psychology, 9, 2735. https://doi.org/10.3389/fpsyg.2018.02735
Himmel, E. (1994). Estandarización y validación del Denver Developmental Screening Test (DDST) [Standardization and validation of the Denver developmental screening test (DDST)]. Pontificia Universidad Católica de Chile.
Instituto Nacional de Perinatología. (2013). Manual para la aplicación de la prueba Evaluación del Desarrollo Infantil, EDI [Manual for the application of the child development assessment, EDI test]. Comisión Nacional de Protección Social en Salud.
Jumbo Salazar, F. F., Salazar Villacis, M. G., Acosta Gavilánez, R. I., & Torres Constante, D. V. (2021). Test de Denver y el test PRUNAPE, instrumentos para identificar alteraciones del desarrollo psicomotor [Denver test and PRUNAPE test, instruments to identify alterations in psychomotor development]. Revista Científica UISRAEL, 8(1), 123–136. https://doi.org/10.35290/rcui.v8n1.2021.401
Kaufman, A. S., & Kaufman, N. L. (1983). Kaufman assessment battery for children. John Wiley & Sons.
Kaufman, A., & Kaufman, N. (2002). K-ABC: Batería de evaluación para niños [K-ABC: assessment battery for children]. Ediciones TEA.
Lejarraga, H., Menéndez, A. M., Menzano, E., Guerra, L., Biancato, S., Pianelli, P., Del Pino, M., Fattore, M. J., & Contreras, M. M. (2008). Screening for developmental problems at primary care level: A field programme in San Isidro, Argentina. Paediatric and Perinatal Epidemiology, 22, 180–187. https://doi.org/10.1111/j.1365-3016.2007.00897.x
Lejarraga, H., Kelmansky, D., Pascucci, M., & Salamanco, G. (2013). Prueba Nacional de Pesquisa – PRUNAPE. Manual Técnico [National Research Test – PRUNAPE. Technical manual]. Ediciones de la Fundación Hospital de Pediatría Garrahan.
Lejarraga, H., Pascucci, M. C., Masautis, A., Kelmansky, D., Lejarraga, C., Charrúa, G., Insua, I., & Nunes, F. (2014). Desarrollo psicomotor infantil en la Cuenca Matanza-Riachuelo: pesquisa de problemas inaparentes del desarrollo [Child psychomotor development in the Matanza-Riachuelo Basin: Investigation of inapparent developmental problems]. Revista Argentina de Salud Pública, 5(19), 17–24. https://ojsrasp.msal.gov.ar/index.php/rasp/article/view/266
Lejarraga, H., Kelmansky, D. M., & Nunes, F. (2018a). Developmental tempo in children aged 0–5 years living under unfavourable environmental conditions. Archivos Argentinos de Pediatría, 116(2), e210–e215. https://sap.org.ar/uploads/archivos/files_ao_lejarraga_in_14-2pdf_1518629932.pdf
Lejarraga, H., Kelmansky, D., Masautis, A., & Nunes, F. (2018b). Índice de desarrollo psicomotor en menores de seis años en las provincias argentinas [Psychomotor development index in children under six years of age in the Argentine provinces]. Archivos Argentinos de Pediatría, 116(2), 251–256. https://www.sap.org.ar/docs/publicaciones/archivosarg/2018/v116n2a17.pdf
Lipina, S. J. (2008). Vulnerabilidad social y desarrollo cognitivo [Social vulnerability and cognitive development]. Jorge Baudino Ediciones; UNSAM.
Lipina, S. J. (2017). Critical considerations about the use of poverty measures in the study of cognitive development. International Journal of Psychology, 52(3), 241–250. https://doi.org/10.1002/ijop.12282
López Bóo, F., Cubides Mateus, M., Sorio, R., Garibotto, G., & Berón, C. (2019). Measuring the quality of the home environment of young children in Uruguay: Socioeconomic gradients in the home inventory. Institute of Labor Economics. IZA Discussion Papers, No. 12110.
Martí Sala, E. (1991). Psicología Evolutiva: teorías y ámbitos de investigación [Evolutionary psychology: Theories and research areas]. Anthropos.
Ministerio de Salud de la República Argentina. (2017). IODI. Instrumento para la observación del desarrollo infantil [Instrument for the observation of child development]. http://www.msal.gob.ar/images/stories/bes/graficos/0000000844cnt-iodi-variables-y-bibliografia.pdf
Moreno Zavaleta, M. T. (2020). Aprendizaje y desarrollo en la primera infancia [Early childhood learning and development]. Educación, 26(1), 63–72. https://doi.org/10.33539/educacion.2020.v26n1.2186
Newborg, J. (2004). Battelle developmental inventory, second edition (BDI-2). Riverside Publishing.
Oiberman, A., Mansilla, M., & Orellana, L. (2002). Nacer y Pensar. Construcción de la Escala Argentina de Inteligencia Sensorio-Motriz de 6 meses a 2 años [To be born and to think. Construction of the argentine sensory-motor intelligence scale from 6 months to 2 years]. Ediciones CIIPME, CONICET.
Ortiz Pinilla, N. (1999). Escala Abreviada de Desarrollo – EAD [Abbreviated development scale – EAD]. Ministerio de Salud de Colombia.
Palacios, J. (1991). Introducción a la Psicología Evolutiva: historia, conceptos básicos y metodología [Introduction to evolutionary psychology: History, basic concepts and methodology]. In J. Palacios, A. Marchesi, & C. Coll (Eds.), Desarrollo psicológico y educación, Tomo 1. Psicología Evolutiva (pp. 15–35). Alianza.
Palacios, J., & Mora, J. (2017). Crecimiento físico y desarrollo psicomotor hasta los 2 años [Physical growth and psychomotor development up to 2 years]. In A. Marchesi, J. Palacios, & C. Coll (Eds.), Desarrollo psicológico y educación, Tomo 1. Psicología Evolutiva (pp. 81–97). Alianza.
Pérez Pereira, M. (1995). Nuevas perspectivas en psicología del desarrollo. Un enfoque histórico crítico [New perspectives in developmental psychology. A critical historical approach]. Alianza.
Piacente, T., Talou, C., & Rodrigo, A. (1990). Piden pan… y algo más. Un estudio sobre crecimiento y desarrollo infantil [They ask for bread … and something else. A study on child growth and development]. UNICEF.
Pickering, S. J. (2001). The development of visuo-spatial working memory. Memory, 9, 423–432. https://doi.org/10.1080/09658210143000182
Portellano, J. A., Mateos, R., Martínez, R., Granados, M., & Tapia, A. (2000). Cuestionario de madurez neuropsicológica infantil (Cumanin) [Child neuropsychological maturity questionnaire]. TEA Ediciones.
Prats, L., Segretin, M. S., Fracchia, C., Kamienkowski, J., Pietto, M., Hermida, J., & Lipina, S. (2017). Asociaciones entre factores individuales y contextuales con el desempeño cognitivo en preescolares de hogares con necesidades básicas insatisfechas (NBI) [Associations between individual and contextual factors with cognitive performance in preschoolers from households with unsatisfied basic needs (UBN)]. Cuadernos de Neuropsicología/Panamerican Journal of Neuropsychology, 11(2), 42–77. https://doi.org/10.7714/CNPS/11.2.201
PUJ Facultad Medicina, E. C. (2016). Escala Abreviada de desarrollo-3 [Abbreviated Development Scale-3]. https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/VS/PP/ENT/Escala-abreviada-de-desarrollo-3.pdf
Rizzoli-Córdoba, A., Schnaas-Arrieta, L., Liendo-Vallejos, S., Buenrostro-Márquez, G., Romo-Pardo, B., Carreón-García, J., & Muñoz-Hernández, O. (2013). Validación de un instrumento para la detección oportuna de problemas de desarrollo en menores de 5 años en México [Validation of an instrument for the timely detection of developmental problems in children under 5 years of age in Mexico]. Boletín Médico del Hospital Infantil de México, 70(3), 195–208.
Rizzoli-Córdoba, A., Ortega-Ríosvelasco, F., Villasís-Keever, M. Á., Pizarro-Castellanos, M., Buenrostro-Márquez, G., Aceves-Villagrán, D., & Muñoz-Hernández, O. (2014). Confiabilidad de la detección de problemas de desarrollo mediante el semáforo de la prueba de Evaluación del Desarrollo Infantil: ¿es diferente un resultado amarillo de uno rojo? [Reliability of detecting developmental problems using the child development assessment test traffic light: Is a yellow result different from a red result?]. Boletín Médico del Hospital Infantil de México, 71(5), 277–285. https://doi.org/10.1016/j.bmhimx.2014.10.003
Rodríguez S., Arancibia V., & Undurraga, C. (1976). Escala de evaluación de desarrollo psicomotor para niños entre 0 y 2 años [Psychomotor development assessment scale for children between 0 and 2 years old]. Galdoc.
Rueda, M. R., Fan, J., McCandliss, B. D., Halparin, J. D., Gruber, D. B., Lercari, L. P., & Posner, M. I. (2004). Development of attentional networks in childhood. Neuropsychologia, 42(8), 1029–1040. https://doi.org/10.1016/j.neuropsychologia.2003.12.012
Sociedad Argentina de Pediatría (SAP). (2016). Detección oportuna de los problemas de desarrollo. La Prueba Nacional de Pesquisa PRUNAPE [Timely detection of development problems. The PRUNAPE National Research Test]. http://www.sap.org.ar/docs/profesionales/recomendaciones/prueba_nacional_de_pesquisa.pdf
Squires, J., Bricker, D. D., & Twombly, E. (2009). Ages & stages questionnaires (pp. 257–182). Paul H. Brookes.
Squires, J., Bricker, D., & Twombly, E. (2015). Cuestionario Ages & Stages: Socio-Emocional (ASQ: SE 2) [Ages & stages questionnaire: Socio-emotional (ASQ: SE 2)]. Brookes Publishing.
Suárez Sanabria, N., & García Paz, C. B. (2017). Implicaciones de la desnutrición en el desarrollo psicomotor de los menores de cinco años [Implications of malnutrition in the psychomotor development of children under five years of age]. Revista Chilena de Nutricion, 44(2), 125–130. https://doi.org/10.4067/S0717-75182017000200002
Tuñon, I. (2018). (In)equidades en el ejercicio de los derechos de niñas y niños. Derechos humanos y sociales en el período 2010-2017 [(In)equity in the exercise of the rights of girls and boys. Human and social rights in the period 2010–2017]. In Documento Estadístico. Barómetro de la Deuda Social de la Infancia. Serie EDSA. Agenda para la equidad (2017–2025). Universidad Católica Argentina.
Tuñon, I., & Fourcade, H. (2019). Disparidades sociales en los procesos de crianza y cuidado de la primera infancia desde una perspectiva de derechos: Área Metropolitana de Buenos Aires [Social disparities in the processes of upbringing and early childhood care from a rights perspective: Metropolitan Area of Buenos Aires]. In M. Paredes & L. Monteiro (Eds.), Desde la niñez a la vejez: nuevos desafíos para la comprensión de la sociología de las edades (pp. 57–79). Teseo.
Tuñón, I., & Salvia, A. (2011). Apuntes sobre la construcción de indicadores de desarrollo humano de la infancia: Perspectivas teóricas desde donde mirar el desarrollo humano de la Infancia [Notes on the construction of childhood human development indicators: Theoretical perspectives from which to look at the human development of childhood]. In Centro Interdisciplinario de Infancia y Pobreza. Seminario Internacional: Modelos e indicadores de desarrollo y bienestar infantil. Universidad de la República.
UNESCO. (2019). SDG 4 Data digest, how to produce and use the global and thematic education indicators. UNESCO. Institute for Statistics. http://uis.unesco.org/sites/default/files/documents/sdg4-data-digest-2019-en_0.pdf
UNICEF. (2016). Apoyando el desarrollo en la primera infancia: de la ciencia a la aplicación a gran escala [Supporting early childhood development: From science to large-scale application]. In Executive summary of The Lancet. https://www.unicef.org/nicaragua/informes/apoyando-el-desarrollo-en-la-primera-infancia-de-la-ciencia-la-aplicaci%C3%B3n-gran-escala
Unidad Nacional de CEN-CINAI, Unidad de Investigación y Vigilancia del Crecimiento y Desarrollo. (2013). Manual operativo de la Escala simplificada de Evaluación del Desarrollo Integral del niño de 0-6 años para su implementación en los CEN-CINAI [Operational manual of the simplified Comprehensive Development Assessment Scale for children aged 0–6 years for its implementation in the CEN-CINAI]. https://issuu.com/uticcen-cinai/docs/escala_simplificada_de_evaluaci__n_
Uribe Ferrari, M. C. (2009). Adaptation and Standardization of Cuestionario para Madurez Neurológica Infantil (CUMANIN) at the State of Mexico. Doctoral dissertation, School of Social and Human Studies, Atlantic International University, Institutional repository Atlantic International University.
Vegas, E., & Santibáñez, L. (2010). La promesa del desarrollo en la primera infancia en América Latina y el Caribe [The promise of early childhood development in Latin America and the Caribbean]. Banco Mundial, Mayol Ediciones SA. https://doi.org/10.1596/978-9-5883-0778-7
Verdisco, A., Cueto, S., Thompson, J., Engle, P., Neuschmidt, O., Meyer, S., González, E., Oré, B., Hepworth, K., & Miranda, A. (2009). Urgency and possibility. Results of PRIDI. A first initiative to create regionally comparative data on child development in four Latin American countries. Technical annex. Inter-American Development Bank. https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.712.3773&rep=rep1&type=pdf
Verdisco, A., Cueto, S., Thompson, J., & Neuschmidt, O. (2015). PRIDI, urgencia y posibilidad: una primera iniciativa para crear datos comparables a nivel regional sobre desarrollo infantil en cuatro países latinoamericanos [PRIDI, urgency and possibility: A first initiative to create regionally comparable data on child development in four Latin American countries]. Inter-American Development Bank. http://repositorio.minedu.gob.pe/handle/20.500.12799/4488
Vericat, A., & Orden, A. B. (2010). Herramientas de screening del desarrollo psicomotor en Latinoamérica [Screening tools for psychomotor development in Latin America]. Revista Chilena de Pediatría, 81(5), 391–401. https://doi.org/10.4067/S0370-41062010000500002
Vygotsky, L. (2006). El desarrollo de los procesos psicológicos superiores [The development of higher psychological processes]. Biblioteca de Bolsillo.
Young, M. E. (2002). From early child development to human development. The World Bank. https://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.199.2092&rep=rep1&type=pdf
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Querejeta Echegoyen, M., Romanazzi Colombo, M.J., Laguens Harnan, A. (2021). Studies on Child Development in Vulnerable Groups in the Metropolitan Area of Buenos Aires, Argentina. In: Barcelata Eguiarte, B.E., Suárez Brito, P. (eds) Child and Adolescent Development in Risky Adverse Contexts. Springer, Cham. https://doi.org/10.1007/978-3-030-83700-6_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-83700-6_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-83699-3
Online ISBN: 978-3-030-83700-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)