
Abstract
Clinically significant hearing loss is present in ~1 per 500 newborns and affects more than 30% of the population at some time in their lives. Empowered by the astounding progress in DNA sequencing technology, recent studies have brought the number of hearing loss genes to over 100. Despite these achievements, very few genes have been discovered that cause isolated inner ear malformations. In this review, we provide a summary of known genetic causes of inner ear malformations in humans.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
4.1 Introduction
Hearing loss (HL) is the most common sensory disorder in humans. It is estimated that 1.6 in every 1000 infants in the U.S. are born with sensorineural hearing loss (SNHL) [1]. One mechanism of congenital SNHL is developmental anomalies affecting the inner ear. Inner ear malformations (IEMs), detected by a computerized scan (CT) or magnetic resonance imaging (MRI) study, can be found in up to one-third of children with SNHL [2]. The presence of IEMs as well as the specific malformation detected may then have an impact on treatment options. For instance, if the cochlear nerve or the inner ear is absent in its entirety, placement of a cochlear implant would not be an effective treatment for the patient, although it is generally an effective treatment option for patients presenting with other forms of IEMs.
Despite studies suggesting over half of profound deafness has genetic causes [3], the genetic basis of IEMs still remains largely to be discovered. Understanding the genetic underpinnings of SNHL associated with IEMs is important in the diagnosis and timely management of patients presenting with SNHL. Not only would it help diagnose family members who may present with a milder form of IEMs and assist impacted individuals with family planning, but its diagnosis may also be an early indication of developmental abnormalities in other organ systems that would not have manifested until later in life. Both these implications of understanding the genetic basis of IEMs have the potential to greatly impact how a patient may be managed in a clinical setting. This review thus aims to summarize current understanding of the genetic etiology for IEMs, specifically its clinical presentation, the genes involved, and the roles they play in embryology.
4.2 A Brief Molecular Embryology of the Inner Ear
The embryological base of the inner ear originates from a thickening of the ectoderm known as the otic placode (OP), which then invaginates to form the otic vesicle. The OP, in turn, arises from a primitive embryological region that surrounds the neural plate known as preplacodal region (PPR).
4.2.1 Preplacodal Region
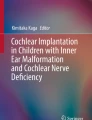
Inner ear development begins in the PPR. Studies in animal models have shown that the development of the PPR in the ectoderm of the developing embryo is determined mainly by the interaction of bone morphogenic protein (Bmp), Wnt and their antagonists, and proteins in the fibroblast growth factor (FGF) pathway [4] (Fig. 4.1a). The anterior-posterior differentiation of the PPR is further modulated by the mutual repression of transcription factors Gbx2 and Otx2, with Gbx2 playing an especially large role in the development of the OP [5] (Fig. 4.1b).

(a) The anterior-posterior differentiation of the preplacodal region at ~22 days. (b) Differentiation of the otic placode and relevant factors
The transcriptional co-activator Eya1 and homeobox gene Six1 function in the early differentiation and maintenance of neurons [6] and are thought to be regulated in turn by Foxi1 [7]. Eya1 and Six1 together with Dach form a regulatory network that leads to transcriptional activation, cell proliferation, and organogenesis of the inner ear [8].
4.2.2 Development of Otic Vesicle
The PPR develops into the OP, which invaginates to form the otic vesicle. The FGF pathway continues to be important in the induction of the OP and signaling of this factor has been shown to induce the expression of zebrafish otic genes such as pax8, pax2a, fgf24, and sox3 throughout the PPR, which is important in setting the pattern of the otic vesicle [9]. This transformation is believed to be, at least in part, regulated by the Hoxa1 gene [10]. The FGF pathway is also influenced by foxi1 and gata3 during otic development, with foxi1 shown to inhibit, and gata3 shown to promote its signaling [11].
In a study investigating the RhoA activity for apical constriction in inner ear placode invagination in a chick model, investigators showed that invagination of OP to form the otic vesicle occurs via the activation of myosin-II not only through FGF signaling, but also through the RhoA-ROCK pathway [12].
After the development of the otic vesicle, the otocyst then gives rise to the mature inner ear structures: the vestibular system in the dorsal plane and the auditory system in the ventral plane.
4.2.3 Molecules and Factors in the Neurogenesis of the Inner Ear
After the otic vesicle stage, many factors play important roles in the further development of neural inner ear structures. Previous studies indicate that high levels of Sox2 protein inhibit sensory cell development in the inner ear [13]. Thus in order for neuronal precursors to commit to a neuronal fate, Fgf10 signals the expression of Ngn1 and Neurod1, which act to inhibit the activity of Sox2 [13, 14] (Fig. 4.1b). Notch signaling then plays a role in specifying the sensory domains within the OP by inducing the proliferation of undifferentiated pre-sensory cells, upregulating Sox2, and inhibiting Ngn1 [15] (Fig. 4.1b). Furthermore, tfap2a is believed to modulate the activity of FGF and notch through activating the inhibitor bmp7a, playing a key role in neural development as well [16]. Another important neural aspect of the inner ear, the formation of the inner radial bundle, is mediated by Eph/Ephrin signaling, a target of Pou3f4 transcription factor activity [17, 18].
4.2.4 Cochlea Formation
The cochlea develops in the ventral plane in the antero-posterior development axis after the otic vesicle stage. Several factors and molecules are involved in the development of the cochlea, such as Jag1, Sox2, and Lfng [19]. Deletion of p27kip1 can cause changes in the cochlea, such as overproduction of hair cells, interestingly causing sensorineural hearing loss [20]. Atoh1 is the earliest discovered factor expressed in the prosensory domain associated with sensory hair cells. In the early period it can be detected in the whole cochlea but over time the expression of Atoh1 is restricted with hair cell progenitors. Numerous factors, which can up- or down-regulate Atoh1, have been described. Among them, Sox2 is one of the most investigated molecules. Although being required for the expression, Sox2 also down-regulates Atoh1. Other regulators of this transcription factor are the Id (inhibitor of differentiation) genes (Id1, Id2, and Id3). These genes are known to negatively regulate Atoh1 [21]. Cochlear lumen formation begins at the base of the cochlea and proceeds towards the apex. This is partly controlled by fluid secretion in the vestibular labyrinth, which is then absorbed into the endolymphatic sac, a process mediated by Slc26a4-encoded channels [22].
4.2.5 Semicircular Canal Development
The vestibular system is located in the dorsal plane of the inner ear. The semicircular canals and their neural elements are derived from the two prominences of the otocyst: the horizontal and vertical canal pouches. The hindbrain is the source of ventral-dorsal axial signaling for the inner ear and Wnts from the dorsal hindbrain are important signals for semicircular canal development [23]. Dlx5 has been shown to be one of the downstream genes that respond to Wnt signaling. Previous studies demonstrate that the lack of Dlx5 can affect canal and crista formation [24]. Also required for appropriate semicircular canal formation are the molecule Hmx3 and the gene Chd7, which encodes a chromodomain-containing helicase protein, and is proposed to act as a selector gene that encodes transcription factors essential for semicircular canal genesis [25].
4.3 Syndromic Causes of Inner Ear Malformations in Humans
Inner ear malformations can be found alone or as part of a syndrome involving other systems. While numerous syndromes can be associated with IEMs in humans, we summarize the most frequently diagnosed ones with clinical findings and causative genes in Table 4.1.
4.4 Non-syndromic Causes of Inner Ear Malformations
Non-syndromic deafness is a type of hearing impairment in which HL is the only clinical finding in the patient. Only a few gene mutations have thus far been discovered to cause non-syndromic IEMs and they are summarized below.
4.4.1 SLC26A4
In 1997, the gene responsible for Pendred syndrome was identified as SLC26A4 [26], which encodes a transmembrane protein named pendrin. Subsequently, SLC26A4 mutations were also discovered in individuals with autosomal recessive non-syndromic deafness associated with enlargement of the vestibular aqueduct (EVA). More than 200 mutations have since been reported related to sporadic and familial forms of Pendred syndrome and non-syndromic SNHL with EVA, and autosomal recessive mutations in the SLC26A4 gene is therefore currently one of the leading causes of non-syndromic SNHL. Although the number of mutant alleles of SLC26A4 has been shown to correlate with the auditory and thyroid phenotypes, no connections between the type of mutation and thyroid phenotype have been reported [27].
Recent studies with molecular testing for SLC26A4 mutations and radiologic imaging of temporal bones demonstrated that enlargement of the vestibular aqueduct (EVA) can be recognized as the most penetrant feature of Pendred syndrome [28]. EVA is the most common radiologic anomaly of the inner ear and is mostly identified in either of two different contexts, non-syndromic EVA or Pendred syndrome.
While variants in FOXI1 and KCNJ10 were reported to cause SNHL with EVA when the same person is heterozygous for an SLC26A4 mutation (i.e., digenic inheritance), this observation has not yet been confirmed by subsequent reports.
4.4.2 POU3F4
Variants in the POU3F4 gene are a major cause of X-linked deafness worldwide at locus DFN3. POU3F4 is the first nuclear gene implicated in non-syndromic deafness. The type of hearing loss found may be SNHL or mixed associated with IP-III (incomplete partition type 3) and stapes fixation (DFN3) [29,30,31,32]. In addition to mutations located within the gene, copy number variants not involving the coding part of the gene have been reported: de Kok and colleagues identified a hot spot for microdeletions in patients with X-linked deafness 900 kb proximal to the DFN3 gene [33]. Given the POU3F4’s uniqueness as an X-linked cause of IEMs, if hearing loss in a patient is found to be X-linked and associated with an inner ear malformation, mutations in POU3F4 gene must be part of the differential and evaluated.
As a clinical pearl, if POU3F4 is identified as the causative gene for hearing loss in a patient, the surgeon should be on the alert for perilymphatic gusher (in fact “cerebrospinal fluid”) during stapes surgery and avoid stapes surgery which may result in total hearing loss.
4.4.3 COCH
The COCH gene is located at 14q11.2-q13 and encodes a secretory protein called Cochlin [34]. The postulated pathogenetic mechanism of COCH gene-related hearing loss is the accumulation of acidophilic deposits in the area of the spiral osseous lamina, spiral ligament, and vestibular nerve channels [35]. Several reports indicate high probability of a link between mutations in the COCH gene and presentation of IEMs. Hildebrand et al. described a patient who presented with semicircular canal dehiscence (SSCD) associated with a mutation in the COCH gene [36]. Dodson et al. described a patient heterozygous for a mutation in the COCH gene and who showed an EVA upon CT imaging [37]. Finally, de Varebeke described nine patients with the same mutation in the COCH gene. On CT imaging, eight of them were found to have sclerotic lesions and/or narrowing of the semicircular canals, and in one patient, the posterior vestibule was also affected [38]. Based on these findings, COCH mutations are a possible autosomal dominant inherited cause of IEMs and are postulated to play a role, along with type II collagen bundles, in laying down the structure of the inner ear [39].
4.4.4 ROR1
ROR1 (receptor tyrosine kinase-like orphan receptor 1) is an integral transmembrane protein consisting of extracellular and intracellular conserved domains. A ROR1 gene mutation was found to be the cause of congenital autosomal recessive non-syndromic SNHL and common cavity anomaly in one reported family with two children [40].
References
Mehl AL, Thomson V. The Colorado newborn hearing screening project, 1992-1999: on the threshold of effective population-based universal newborn hearing screening. Pediatrics. 2002;109(1):E7.
Bamiou DE, Phelps P, Sirimanna T. Temporal bone computed tomography findings in bilateral sensorineural hearing loss. Arch Dis Child. 2000;82(3):257–60.
Nance WE. The genetics of deafness. Ment Retard Dev Disabil Res Rev. 2003;9(2):109–19.
Litsiou A, Hanson S, Streit A. A balance of FGF, BMP and WNT signalling positions the future placode territory in the head. Development. 2005;132(18):4051–62.
Steventon B, Mayor R, Streit A. Mutual repression between Gbx2 and Otx2 in sensory placodes reveals a general mechanism for ectodermal patterning. Dev Biol. 2012;367(1):55–65.
Zou D, Silvius D, Fritzsch B, Xu PX. Eya1 and Six1 are essential for early steps of sensory neurogenesis in mammalian cranial placodes. Development. 2004;131(22):5561–72.
Ishihara T, Sato S, Ikeda K, Yajima H, Kawakami K. Multiple evolutionarily conserved enhancers control expression of Eya1. Dev Dyn. 2008;237(11):3142–56.
Li X, Oghi KA, Zhang J, Krones A, Bush KT, Glass CK, et al. Eya protein phosphatase activity regulates Six1-Dach-Eya transcriptional effects in mammalian organogenesis. Nature. 2003;426(6964):247–54.
Padanad MS, Bhat N, Guo B, Riley BB. Conditions that influence the response to Fgf during otic placode induction. Dev Biol. 2012;364(1):1–10.
Makki N, Capecchi MR. Identification of novel Hoxa1 downstream targets regulating hindbrain, neural crest and inner ear development. Dev Biol. 2011;357(2):295–304.
Yao D, Zhao F, Wu Y, Wang J, Dong W, Zhao J, et al. Dissecting the differentiation process of the preplacodal ectoderm in zebrafish. Dev Dyn. 2014;243(10):1338–51.
Sai X, Yonemura S, Ladher RK. Junctionally restricted RhoA activity is necessary for apical constriction during phase 2 inner ear placode invagination. Dev Biol. 2014;394(2):206–16.
Evsen L, Sugahara S, Uchikawa M, Kondoh H, Wu DK. Progression of neurogenesis in the inner ear requires inhibition of Sox2 transcription by neurogenin1 and neurod1. J Neurosci. 2013;33(9):3879–90.
Alsina B, Abello G, Ulloa E, Henrique D, Pujades C, Giraldez F. FGF signaling is required for determination of otic neuroblasts in the chick embryo. Dev Biol. 2004;267(1):119–34.
Jeon SJ, Fujioka M, Kim SC, Edge AS. Notch signaling alters sensory or neuronal cell fate specification of inner ear stem cells. J Neurosci. 2011;31(23):8351–8.
Kantarci H, Edlund RK, Groves AK, Riley BB. Tfap2a promotes specification and maturation of neurons in the inner ear through modulation of Bmp, Fgf and notch signaling. PLoS Genet. 2015;11(3):e1005037.
Coate TM, Raft S, Zhao X, Ryan AK, Crenshaw EB III, Kelley MW. Otic mesenchyme cells regulate spiral ganglion axon fasciculation through a Pou3f4/EphA4 signaling pathway. Neuron. 2012;73(1):49–63.
Raft S, Coate TM, Kelley MW, Crenshaw EB III, Wu DK. Pou3f4-mediated regulation of ephrin-b2 controls temporal bone development in the mouse. PLoS One. 2014;9(10):e109043.
Wu D, Kelley MW. Molecular mechanisms of inner ear development. Cold Spring Harb Perspect Biol. 2012;4(8):a008409.
Chen P, Segil N. p27Kip1 links cell proliferation to morphogenesis in the developing organ of Corti. Development. 1999;126:1581–90.
Jones JM, Montcouquiol M, Dabdoub A, Woods C, Kelley MW. Inhibitors of differentiation and DNA binding (Ids) regulate Math1 and hair cell formation during the development of the organ of Corti. J Neurosci. 2006;26:550–8.
Kim HM, Wangemann P. Failure of fluid absorption in the endolymphatic sac initiates cochlear enlargement that leads to deafness in mice lacking pendrin expression. PLoS One. 2010;5(11):e14041.
Riccomagno MM, Takada S, Epstein DJ. Wnt-dependent regulation of inner ear morphogenesis is balanced by the opposing and supporting roles of Shh. Genes Dev. 2005;19:1612–23.
Acampora D, Merlo GR, Paleari L, Zerega B, Postiglione MP, Mantero S, Bober E, Barbieri O, Simeone A, Levi G. Craniofacial, vestibular and bone defects in mice lacking the distal-less-related gene Dlx5. Development. 1999;126:3795–809.
Hurd EA, Micucci JA, Reamer EN, Martin DM. Delayed fusion and altered gene expression contribute to semicircular canal defects in Chd7 deficient mice. Mech Dev. 2012;129(9-12):308–23.
Everett L, Glaser B, Beck J, Idol J, Buchs A, Heyman M, Adawi F, Hazani E, Nassir E, Baxevanis A, Sheffield V, Green E. Pendred syndrome is caused by mutations in a putative sulphate transporter gene (PDS). Nat Genet. 1997;17:411–22.
Ito T, et al. SLC26A4 genotypes and phenotypes associated with enlargement of the vestibular aqueduct. Cell Physiol Biochem. 2011;28(3):545.
Phelps PD, Coffey RA, Trembath RC, Luxon LM, Grossman AB, Britton KE, Kendall-Taylor P, Graham JM, Cadge BC, Stephens SG, Pembrey ME, Reardon W. Radiological malformations of the ear in Pendred syndrome. Clin Radiol. 1998;53:268–73.
Gong WX, Gong RZ, Zhao B. HRCT and MRI findings in X-linked non-syndromic deafness patients with a POU3F4 mutation. Int J Pediatr Otorhinolaryngol. 2014;78(10):1756–62.
Choi BY, An YH, Park JH, Jang JH, Chung HC, Kim AR, et al. Audiological and surgical evidence for the presence of a third window effect for the conductive hearing loss in DFNX2 deafness irrespective of types of mutations. Eur Arch Otorhinolaryngol. 2013;270(12):3057–62.
Anger GJ, Crocker S, McKenzie K, Brown KK, Morton CC, Harrison K, et al. X-linked deafness-2 (DFNX2) phenotype associated with a paracentric inversion upstream of POU3F4. Am J Audiol. 2014;23(1):1–6.
de Kok YJM, van der Maarel SM, Bitner-Glindzicz M, Huber I, Monaco AP, Malcolm S. Association between X-linked mixed deafness and mutations in the POU domain gene POU3F4. Science. 1995;267:685–8.
de Kok YJM, Vossenaar ER, Cremers CWRJ, Dahl N, Laporte J, Hu LJ. Identification of a hot spot for microdeletions in patients with X-linked deafness (DFN3) 900 b proximal to the DFN3 gene POU3F4. Hum Mol Genet. 1996;5:1229–35.
Parzefall T, Frohne A, Koenighofer M, et al. Identification of a rare COCH mutation by whole-exome Sequencing. Wien Klin Wochenschr. 2017;130:299. https://doi.org/10.1007/s00508-017-1230-y.
Robertson NG, Lu L, Heller S, Merchant SN, Eavey RD, et al. Mutations in a novel cochlear gene cause DFNA9, a human nonsyndromic deafness with vestibular dysfunction. Nat Genet. 1998;20:299–303.
Hildebrand MS, Tack D, Deluca A, Hur IA, Van Rybroek JM, McMordie SJ, et al. Mutation in the COCH gene is associated with superior semicircular canal dehiscence. Am J Med Genet A. 2009;149A(2):280–5.
Dodson KM, Georgolios A, Barr N, Nguyen B, Sismanis A, Arnos KS, et al. Etiology of unilateral hearing loss in a national hereditary deafness repository. Am J Otolaryngol. 2012;33(5):590–4.
de Varebeke SP, Termote B, Van Camp G, Govaerts PJ, Schepers S, Cox T, et al. Focal sclerosis of semicircular canals with severe DFNA9 hearing impairment caused by a P51S COCH-mutation: is there a link? Otol Neurotol. 2014;35(6):1077–86.
Shindo S, Ikezono T, Ishizaki M, Sekiguchi S, Mizuta K, Li L, et al. Spatiotemporal expression of cochlin in the inner ear of rats during postnatal development. Neurosci Lett. 2008;444(2):148–52.
Diaz-Horta O, Abad C, Sennaroglu L, Foster J, DeSmidt A, Bademci G, et al. ROR1 is essential for proper innervation of auditory hair cells and hearing in humans and mice. Proc Natl Acad Sci U S A. 2016;113(21):5993.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Liu, W., Ocak, E., Bademci, G., Tekin, M. (2022). Genetic Causes of Sensorineural Hearing Loss Associated with Inner Ear Malformations. In: Sennaroglu, L. (eds) Inner Ear Malformations. Springer, Cham. https://doi.org/10.1007/978-3-030-83674-0_4
Download citation
DOI: https://doi.org/10.1007/978-3-030-83674-0_4
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-83673-3
Online ISBN: 978-3-030-83674-0
eBook Packages: MedicineMedicine (R0)