
Abstract
For years, the term “Mondini dysplasia” was used to describe virtually every type of congenital inner ear malformation detected in imaging tests. More recently, histopathologic and imaging studies led to the description of several novel morphologic features, which were categorized into new groups according to morphologic patterns of the inner ear abnormalities. In addition, those new findings made possible to hypothesize potential pathophysiologic and embryogenic mechanisms involved in the genesis of each specific type of malformation. However, there are still obscure areas that still need to be better understood, such as quantitative and qualitative pathologic changes in the cellular, sensorial, and neural elements in the inner ear of patients with inner ear abnormalities. Therefore, histologic analysis of human temporal bones from patients who had inner ear malformations constitutes a tool of invaluable value. The clinical impact of past studies involving inner ear malformations is clear: today, cochlear implants or auditory brainstem implants are well indicated to treat hearing loss in patients with inner ear malformations, who were previously excluded from candidacy criteria. In the future, a broader understanding of yet obscure aspects of those malformations may increase even further the candidacy for those implants and create strategies for improved functional results. Thus, the objective of this chapter is to report, based on a review of the literature, otopathologic findings in human temporal bones from donors with inner ear malformations and to correlate the findings with embryogenic factors and their clinical implications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
2.1 Introduction
The study of the ear structures has been a matter of great interest among anatomists, researchers, and physicians throughout the centuries [1]. Before the introduction of the first functional microscope in the 1660s, descriptions of the ear anatomy were limited to gross macroscopic studies of the external ear [1]. But the introduction of microscopy equipment and tissue staining techniques in the 1670s allowed the study of microscopic aspects of several diseases and malformations affecting the ear [1].
The first author to describe an inner ear abnormality was Carlo Mondini [2], in 1791, who reported the first gross anatomic features of a malformation which was later named by Siebenmann [3], in 1904, as “typus Mondini.” [4] In his descriptions, Mondini [2] describes dilatation of the vestibule and vestibular aqueduct and several cochlear abnormalities, including incomplete interscalar septum, incomplete development of the modiolus, and hypoplasia of the upper turns, limiting the cochlea to one and a half turns [4]. Later, in 1838, Edward Cock [5] reported a wide communication between the cochlea and the vestibule in four human temporal bones, a deformity that is now known as “common cavity.” In 1863, P. Michel [6] described another inner ear malformation characterized by bilateral absence of inner ear structures, which were later named after him (Michel aplasia). Other malformations affecting the membranous labyrinth have been described as well, including complete membranous labyrinthine dysplasia [7], cochleosaccular dysplasia [8], and cochlear basal turn dysplasia [9]. Since membranous abnormalities are not seen in the available imaging tests, those are not included in most current classification systems of malformations [10].
For years, the term “Mondini dysplasia” has been used to describe virtually every type of congenital inner ear malformation detected by imaging tests [10]. However, further histopathologic and imaging have made possible the development of classification systems and to hypothesize potential pathophysiologic and embryogenic mechanisms involved in the genesis of each malformation [10, 11]. In addition, those new findings allowed the development of several hearing rehabilitation solutions for patients who have severe-to-profound hearing loss secondary to inner ear malformations [12,13,14]. Initially, these patients were excluded from the candidacy criteria for cochlear implantation, mostly due to concerns about potential complications and low expectations of a successful stimulation of the cochlear nerve [7, 12]; in addition, the auditory brainstem implants were not indicated for children under 12 years [15]. But technological advancements as well as the growing number of surgeons who successfully performed those implants in pediatric and adult patients with cochleovestibular malformations have led to gradual change to their indications [13, 14, 16]. Analysis of inner ears from donors who had cochlear malformations has a tremendous value to achieve a better understanding of the embryologic, pathophysiologic, morphologic, and developmental features associated with those malformations [1, 17].
2.2 Classification of Inner Ear Malformations
The introduction of high-resolution computed tomography (CT) and magnetic resonance imaging (MRI) in the late 1980s, as well as further histopathologic analysis of human temporal bone specimens, resulted in detailed descriptions of new morphologic aspects and malformations that do not completely fit the initial descriptions of Mondini [2], Siebenmann [3], and Terrahe [17]. Moreover, new classifications became a necessity with the development of cochlear and brainstem implants—selection of potential candidates to those implants includes a thorough evaluation of the type and degree of malformations, considering their impact in the surgical decisions and potential prognosis of the rehabilitation [18].
Jackler et al. [10] were the first authors to describe a classification system for inner ear malformations based upon their radiologic appearance. The authors also described potential embryologic mechanisms (developmental arrest, aberrant development) involved in their genesis, and correlated the findings with the audiologic patterns and prognosis. Their classification has divided the bony malformations in 2 groups, one with absent or malformed cochlea and one with normal cochlea (Table 2.1). As a general rule, the authors observed a correlation between severity of the structural abnormalities and worse audiologic results [10].
Marangos [19], in 2002, developed a new classification method and highlighted some of the arrests in the embryogenic development that may cause each type of malformation. The authors also claim that some of the malformations may be considered as absolute contraindications to cochlear implant, due to potential complications and very low expectation of hearing rehabilitation. Marangos’ [19] classification also includes other types of abnormalities not contemplated by Jackler et al. [10], such as long crista transversa, internal auditory canal tripartitus, and X-linked hearing loss (Table 2.1).
Sennaroglu and Saatci [11], in 2002, reported a classification method for cochlear malformations based on radiologic findings in 23 patients. The authors classified the abnormalities according to their locations in the inner ear and severity of the abnormalities in the inner and outer architecture. They also demonstrated that abnormalities in each labyrinthine compartment may occur in isolation or in association with malformations of other portions of the bony labyrinth (Table 2.1). With their findings, they hypothesized potential pathophysiologic mechanisms and embryogenic factors associated with the development of each abnormality [11, 20]. Later, in 2006, Sennaroglu et al. [12] modified their classification to accommodate the X-linked deafness as “incomplete partition type 3.”
More recently, Jeong and Kim [21] suggested a new classification system, claiming that previous classifications have embryogenic implications but lack clinical application. Reviewing clinical, imaging, and surgical data of 59 patients with cochleovestibular malformations subjected to cochlear implantation, the authors suggested the following classification: (1) type A, normal cochlea and modiolus; (2) type B, malformed cochlea and partial modiolus; (3) type C, malformed cochlea and no modiolus.
2.3 Embryology of Inner Ear Malformations
After 3 weeks of development, the ectoderm on each side of the rhombencephalon thickens to form the otic placodes, which will later invaginate and form the otocysts [22]. Arrest in the development before formation of the otocyst leads to labyrinthine aplasia (Michel aplasia) [20]. The labyrinthine aplasia may occur either with presence or absence of the petrous bone and otic capsule [20]. If the arrest occurs in the initial stages of the otocyst formation, the resultant deformity is called “rudimentary otocyst.” [23] At Week 5, the pars utriculovestibularis grows dorsocranially to later form the utricle, semicircular canals, and endolymphatic duct [22, 24]. The earlier formation of the posterior labyrinth explains why some cochlear malformations are not necessarily followed by abnormalities in the posterior labyrinth [20]. An arrest in development which occurs between the fourth and fifth week (before differentiation of the otocyst into cochlea and vestibule) will result in common cavity malformation. On the other hand, an insult affecting the inner ear within the fifth week (before development of the cochlear duct) will lead to an abnormality characterized by cochlear aplasia with hypoplastic or normal vestibular/endolymphatic structures [10, 20, 22].
During the sixth week, the cochlear duct starts to develop from the saccule, reaching the size of one turn at 7 weeks, 1.5 turns at 8 weeks, and the full 2.5 turns before the 11th week [10, 20, 22]. If there is any developmental arrest between sixth and 11th week, the cochlea will be hypoplastic with some degree of underdeveloped internal architecture depending on the time the insult happens [10, 20, 22]. After the cochlea reaches the full size of 2.5 turns, it will slowly continue to grow in caliber until it reaches adult size between the 22nd and 24th weeks. Thus, defects in the development occurring after the tenth week will result in a cochlea with normal or near-normal external dimensions [10, 20, 22].
After the cochlea reaches 2.5 turns around the tenth week, the mesenchyme surrounding the cochlear duct differentiates into cartilage, which will later become the perilymphatic cochlear ducts; in addition, epithelial cells of the cochlear duct differentiate into the spiral limbus and organ of Corti [10, 20, 22]. The development of the vestibulocochlear nerve occurs in parallel to the membranous labyrinth—before the eighth week, nerve fibers from the neuroblasts grow towards the labyrinth and vestibulocochlear nerve area at the brainstem [10, 20, 22]. Vestibulocochlear nerve is present by seventh week, while the hair cells in the basal turn of the cochlea receive nerve fibers around the tenth week [10, 20, 22]. The modiolus develops from the membranous bone within the cochlea, and bone deposition occurs exponentially around 20–21st week in the basal and middle turns of the cochlea and towards the apical turn by the 25th week. Thus, any cochlear developmental arrest after the tenth week will not affect the cochlear size, but may have a significant impact on the development of the internal architecture of the cochlea and vestibulocochlear nerve, comprising both incomplete partitions and membranous labyrinth anomalies [10, 20, 22].
2.4 Histopathologic Findings of Inner Ear Malformations and Their Clinical Implications
Histopathologic studies of human temporal bone from donors who had inner ear malformations provided (and will continue to provide) invaluable contributions to the current knowledge on several features of labyrinthine anomalies [1]. Throughout the years, several different types of inner ear malformations have been described, but adequate assessment of several of them was only made possible after introduction of high-resolution CT [10]. It is known today that over 20% of all cases of congenital sensorineural hearing loss are secondary to bony malformations, while the remaining 80% are probably membranous malformations located at the cellular level [11]. However, for many years, the term “Mondini deformity” has been used in such a way to encompass any type of bony malformation affecting the cochlea [10].
After the first demonstration of a cochlear implant in a patient with inner ear malformation by Mangabeira-Albernaz [16], in 1983, in addition to other following successful experiences [13, 14], the candidacy for cochlear implants has changed to accommodate patients with cochlear malformations, who were initially excluded from its indications [12]. The possibility for hearing restoration in this specific population brought the need for a broader and deeper understanding of the anatomic, morphologic and functional aspects of each specific type of inner ear malformation [10, 11]. In this regard, imaging and histopathologic studies already provided advances, demonstrating several different types of malformations and their respective morphologic features [25, 26]. The clinical implications of those new findings are clear, considering that some types of malformations are associated with neural and structural abnormalities that may either predict the results or even contraindicate cochlear implantation at all, as in cases of labyrinthine aplasia—those patients may benefit from brainstem auditory implants [12].
The classification systems proposed for inner ear malformations after the 1980s mostly comprised of bony malformations, considering that they can be identified in imaging tests [10]. However, descriptive histopathologic analysis of human temporal bones also demonstrated several malformations affecting only the membranous labyrinth as well [27, 28].
2.4.1 Malformations of the Membranous Labyrinth
In this group of malformations, the otic capsule and bony labyrinth are well developed and normal in size, but there is abnormal development of the internal architecture of the membranous labyrinth. The three main types of exclusive membranous malformations are:
-
1.
Cochleosaccular dysplasia (Scheibe dysplasia): This type of malformation involves only the saccule and cochlea, while the utricle and semicircular canals are spared [29]. Several abnormalities secondary to this malformation were observed, such as degeneration of the stria vascularis and organ of Corti, loss of inner and outer hair cells, and collapsed Reissner’s membrane; signs of hydrops may also be observed [28, 29]. However, there seem to be no significant decrease in the number of neuron cells. The saccular membrane is usually collapsed and its sensorial epithelium is deformed [29]. Some degree of atrophy of the cochlear and vestibular nerve have been reported as well [28]. This abnormality may occur as part of several syndromes (Down, keratitis-ichthyosis-deafness, Refsum, Waardenburg, Jervell and Lange, trisomy of 18), following viral infections (congenital rubella), or in isolation [28, 29].
-
2.
Cochlear basal turn dysplasia (Alexander dysplasia): In his original description in 1904 [9], Alexander describes the abnormalities affecting the inner ear of a 38-year-old man who was deaf mute. The author describes normal pars inferior, while the cochlea had several abnormalities affecting the basal turn, including atrophy of the stria vascularis, defect of the interscalar septum from above the upper basal turn, loss of hair and pillar cells in the organ of Corti, and loss of spiral ganglion neurons. In the middle and apical turns, minor changes were observed, such as atrophy of the stria vascularis and spiral ligament and absence of helicotrema. However, no subsequent report of a malformation limited to the basal turn of the cochlea has been later described [7].
-
3.
Complete membranous labyrinth aplasia (Siebenmann-Bing): The description of a complete dysplasia of the membranous labyrinth was first published by Siebenmann and Bing, in 1907 [10]. This type of malformation is exceedingly rare, with very few reports in the literature. The bony labyrinth has a normal development, and thus such abnormality cannot be seen in the currently available imaging tests [7]. It has also been suggested that it may be a severe variant of the Scheibe’s dysplasia. An association with genetic syndromes such as Jervell and Lange, Usher, and oculo-auriculo-vertebral spectrum has been reported in the past [7].
2.4.2 Malformations of the Bony Labyrinth
In this group of malformations, abnormalities affect the otic capsule and internal/external cochlear and vestibular bony architecture, which may be accompanied by membranous abnormalities [10, 11, 20]. It comprises a wide range of abnormalities, ranging from complete labyrinthine aplasia (Michel aplasia) to near-normal inner ear. The most important bony malformations, as reported by Sennaroglu and Saatci [11], include labyrinthine aplasia, rudimentary otocyst, common cavity, cochlear aplasia, cochlear hypoplasia, and incomplete partition. Those malformations may be bilateral (more frequently) or unilateral, and the contralateral side may be normal or have a different type of malformation [11, 24]. In addition, they may occur in isolation, associated with middle ear or other organ anomalies, or in association with several syndromes, such as Wildervanck, Pendred, DiGeorge, and the trisomies [29]. The currently available histopathologic findings of human bone studies in the literature are listed below and in Table 2.2.
Labyrinthine aplasia and rudimentary otocyst comprise a group of malformations resulting from very early arrest in embryologic development, before the fifth week. To date, there are no histopathologic descriptions of those abnormalities in human temporal bones. Radiologic and clinical characteristics are described below:
2.4.2.1 Labyrinthine Aplasia (Michel aplasia)
It is characterized by the absence of both anterior and posterior labyrinth [6]. Petrous bone, as well as otic capsule, may be hypoplastic, aplastic, or normal [30]. There are no histopathologic human temporal bone descriptions of this malformation in the literature [20]. Patients with this abnormality have absence of response in all clinical audiologic tests and may benefit only from brainstem auditory implants [15, 31].
2.4.2.2 Rudimentary Otocyst
In the initial stages of embryologic development, an arrest in development may occur right after formation of the otocyst—such arrest results in a small, millimetric round or ovoid cavity, which may have parts of semicircular canals, called rudimentary otocyst. It is an earlier malformation as compared with the common cavity, which is larger in size and may have nerve connections through the internal auditory canal. Audiologic tests in patients with this abnormality are absent, and the only hearing rehabilitation option is brainstem auditory implant [15, 31]. Although (to the best of our knowledge) no human temporal bone description of this type of abnormality exists, studies in mice demonstrated the first maturational stages of the otocyst [32,33,34]. At Day 12 of embryologic development, areas of sensory structures can be identified [32,33,34], and at this stage, the otocyst is composed of pseudostratified columnar epitheliae surrounded by undifferentiated mesenchymal cells [32]. In some areas, there may be initial differentiation of those mesenchymal cells in chondrocytes [32, 33]. There are definite perilymphatic spaces, with respective projections resembling rudimentary semicircular canals; those canals sometimes have identifiable cristae, which usually end in a blind sac into the cartilaginous capsule [32]. No endolymphatic duct or sac is identified [32]. There may be formation of utriculosaccular spaces in a few cases, with or without sensorial macula [32]. In over 50% cases, there may be partial development of a cochlear duct, which does not coil and become a swollen sac [32,33,34]. Rudimentary cochlear sensory epithelia and tectorial membrane may also be present [32,33,34].
2.4.2.3 Common Cavity
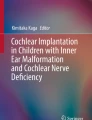
The common cavity deformity, first described in 1838 by Cock [5, 7, 35], comprises a single, ovoid or round chamber as seen in imaging tests. It seems to occur secondary to an arrest in development around the fourth and fifth weeks [5]. It is important to differentiate a common cavity from a rudimentary otocyst due to the clinical implications. In both situations, a round or ovoid cavity is seen in the otic capsule, but in the rudimentary otocyst, the cavity is smaller in size and there is no internal auditory canal [5, 36]. In the common cavity, there is an internal auditory canal (Fig. 2.1) and also neural spiral ganglion cells in the lateral wall, which allow cochlear implantation.

Common cavity deformity. The cavity is bigger in size as compared with a rudimentary otocyst, and there is an internal auditory canal. (Source: Image kindly provided by Dr. Levent Sennaroglu, reproduced under his authorization)
Patients with common cavity deformity usually have profound sensorineural hearing loss [30]. Considering the possibility of the presence of a viable cochlear nerve, cochlear implants may be indicated [5, 30]; nonetheless, it is imperative to perform an extensive audiologic assessment prior to surgery [5, 30]. In cases that a cochlear implant is indicated, the selected electrode should be short and expand against the external borders of the cochlea to reach the neural epithelium [5, 30, 36]; curved electrodes (designed to “hug” the modiolus) should be avoided [5, 37]. In cases of cochlear nerve aplasia or failure of cochlear implants, auditory brainstem implants may be offered [5, 15, 30].
2.4.2.4 Cochlear Aplasia
In this type of malformation, although the otic capsule is present and posterior labyrinth is formed, no cochlea is developed [10, 11, 20]; labyrinthine segment of the cochlear nerve is usually dislocated anteriorly. The arrest in development leading to this abnormality must occur before the development of the cochlear duct at fifth week. Frequently, the abnormality is bilateral and symmetric, suggesting a genetic origin. The vestibule and vestibular canals may be hypoplastic or dilated.
2.4.2.5 Cochlear Hypoplasia
Cochlear hypoplasia is defined as the presence of an identifiable cochlea with smaller external dimensions. The prevalence of cochlear hypoplasia accounts for 15–23.5% among all types of inner ear malformations [23, 38]. They may occur in isolation or associated with several syndromes, such as branchio-oto-renal syndrome, trisomy of 13, and triploidy [39]. The degree of structural abnormalities depends largely on the time and severity of arrest during the embryologic period [7, 10, 20]. The arrest in development leading to cochlear hypoplasia occurs between the sixth and eighth week, after the cochlear duct is formed but has not yet completed their development in caliber [20]. The only exception is cochlear hypoplasia type IV, in which the arrest seems to occur in a later developmental stage [10, 20].
There may be some coincidence in the morphologic appearance of cochlear hypoplasia, cochlear aplasia with enlarged vestibule and common cavity malformations [20]. The difference between those entities is that in the cochlear hypoplasia, the cochlea and the vestibule are distinct. Although morphologically similar, it is imperative to identify the type of malformation in the preoperative evaluation of patients with potential cochlear implant indication: patients with common cavity and cochlear hypoplasia may achieve good results with cochlear implants, but patients with cochlear aplasia only benefit from brainstem implants [20, 23].
When cochlear implants are indicated, there are some morphologic features that have to be assessed in the preoperative evaluation [18]. Patients who have bony cochlear nerve canal aplasia always have severe-to-profound hearing loss and do not benefit from cochlear implantation [37]. If the canal is hypoplastic, the hearing levels vary from mild (less frequently) to profound hearing loss [23, 40,41,42]. The presence of normal cochlear nerve canal also does not necessarily represent better hearing levels as compared with cochlear aperture hypoplasia, considering the other structural and membranous abnormalities present in cochlear hypoplasia and also the status of the cochlear nerve fibers, which may be normal, hypoplastic, and aplastic in both conditions [20, 30, 37, 40]. Intraoperatively, considering the anatomic aberrations associated with the hypoplasia, identification of the round window niche/membrane through facial recess approach may be difficult; therefore, an additional transmeatal approach or a labyrinthotomy is needed in some cases [37, 43]. The course of the facial nerve may be abnormal as well [20, 23, 44]. It is recommended to use thin (0.8 mm) and short (<20 mm) electrodes, given the smaller cochlear size and fragility of its internal architecture [12, 30, 37].
Sennaroglu and Bajin [30] have categorized the group of malformations nominated as cochlear hypoplasia in four subgroups:
-
1.
Cochlear hypoplasia type I: The cochlea is either oval- or round-shaped, and its internal architecture is severely deformed [11, 20, 23].
-
(a)
Internal cochlear architecture: The modiolus is absent or hypoplastic, with defective neural connections into the interior of the cochlea [11, 20, 23]. There is no interscalar septum or internal membranous structures [11, 20, 23, 30].
-
(b)
Bony cochlear nerve canal/cochlear nerve: The canal for the cochlear nerve may be aplastic (no cochlear nerve), or hypoplastic, with coincident cochlear nerve hypoplasia [11, 20, 23].
-
(c)
Vestibular system: The vestibular system may be hypodeveloped as well—there were reports of aplasia or hypoplasia of the vestibule and semicircular canals and dilatation of the utricle [20].
-
(d)
Other associated malformations: fixation of the footplate and aplastic oval window [11, 20].
-
(e)
Clinical implications: Most patients with cochlear hypoplasia type I have severe-to-profound sensorineural or mixed hearing loss [23]. Therefore, there are not many treatment options other than cochlear or auditory brainstem implants [30, 37]. In preoperative evaluation, the morphology of the bony cochlear nerve canal should be assessed carefully, considering that the cochlear implant may not provide good hearing outcomes if the canal is aplastic [30]. In cases of hypoplastic cochlear nerve and subtotal/total modiolar defect, it is recommended to first perform cochlear implants—although their functional results may be poorer than in normal patients, they are still better than brainstem implants, which should be performed in the contralateral side if cochlear implantation does not provide sufficient hearing restoration [30, 37]. If cochlear implants are indicated, short, straight electrodes are warranted for two reasons: (1) the neural epithelium is usually localized at the lateral cochlear wall, and thus the electrode should expand against these; and (2) if there is a communication between the cochlea and internal auditory canal, curved electrodes may be misplaced inside the meatus, increasing the risks for damaging the facial nerve [31, 37, 45].
-
(a)
-
2.
Cochlear hypoplasia type II: The cochlea has an external shape that, although rounder, is more closely related to a normal cochlea as compared with cochlear hypoplasia type I.
-
(a)
Internal architecture: The internal architecture of the cochlea is also more developed in the cochlear hypoplasia type II as compared with type I [20]. The modiolus is always absent or hypoplastic (no development in the upper half of the cochlea) (Fig. 2.2) [20, 46]. The interscalar septum may be either hypoplastic or absent, giving the cochlea a rounder shape (Fig. 2.2) [20]. It has also been demonstrated the possibility of absence or loss in the population of spiral ganglion cells [20, 46,47,48]. Lateral wall in the basal turn is frequently normal in the basal turn, with varying degrees of hypoplasia/atrophy in the upper regions of the cochlea [20, 46].
-
(b)
Bony cochlear nerve canal/cochlear nerve: There were reports of complete absence of bony cochlear nerve canal and hypoplastic nerve, but they may also be normal (Fig. 2.2) [20].
-
(c)
Vestibular system: The vestibule may be hypoplastic, normal, or minimally dilated; vestibular aqueduct is sometimes enlarged [20, 46].
-
(d)
Other associated malformations: Aplasia of the oval window and stapes fixation are frequent features of cochlear hypoplasia type II [20].
-
(e)
Clinical implications: The frequent abnormalities of the oval window and stapes may add a conductive component onto the sensorineural hearing loss, although pure sensorineural hearing loss is much more frequent than mixed hearing loss among patients with cochlear hypoplasia type II [23]. The majority of patients (over 80%) have severe-to-profound hearing loss, while moderate-to-severe hearing loss is less frequently observed [23, 30]. If functional hearing is observed, some patients may benefit from stapedectomy with postoperative hearing aids [23, 30]. In cases of severe-to-profound hearing loss, cochlear or auditory brainstem implants are warranted considering the presence or absence of aplasia of the bony cochlear nerve canal [31, 37, 45]. In cases with complete absence of the modiolus, surgeons must be aware of the possibility of intraoperative gusher and misplacement of the cochlear implant electrode inside of the internal auditory canal [49,50,51]. The high prevalence of stapes abnormalities secondary to this malformation may increase the risks of recurrent meningitis as well [36, 52, 53].
-
(a)
-
3.
Cochlear hypoplasia type 3: In this type of hypoplasia, the external shape of the cochlea is very similar to normal, given the presence of interscalar septum [20]. In a case series published by Cinar et al. [23], this type of hypoplasia was the most frequent among all patients with cochlear hypoplasia. Although external architecture is near normal, the cochlea is limited to one and a half turns internally—this particular morphologic feature may have led authors in the past to classify patients with this abnormality as Mondini dysplasia [39]. Given that ossification of the cochlea begins only after the membranous labyrinth reaches full size, it is possible that, in this type of malformation, the cochlea is genetically predetermined to have a smaller size [20].
-
(a)
Internal architecture: [20] The modiolus is usually well developed but shorter than in a normal cochlea (Fig. 2.3). Interscalar septum is always present. The anatomic configuration of the cochlear scalas, organ of Corti, and lateral wall is normal (Fig. 2.3)
-
(b)
Bony cochlear nerve canal/cochlear nerve: [20] Although frequently normal, the bony cochlear nerve canal may be aplastic or hypoplastic.
-
(c)
Vestibular system: [20] vestibule and semicircular canals are frequently hypoplastic.
-
(d)
Other associated malformations: [20] oval window may be normal or aplastic, and stapes fixation is seen in some cases.
-
(e)
Clinical implications: Given the near-normal internal cochlear architecture and potential abnormalities in the oval window, patients may present with virtually any type and degree of hearing loss [23, 30]; however, pure sensorineural, moderate-to-severe, and severe-to-profound hearing loss are the most frequent types of observed hearing loss among patients with cochlear hypoplasia type 3 [23]. Mixed hearing loss may be treated by stapedectomy and/or hearing aids, mild-to-moderate sensorineural hearing loss with hearing aid or middle ear implants and severe-to-profound hearing loss should receive cochlear or auditory brainstem implants [14, 30, 37, 54].
-
(a)
-
4.
Cochlear hypoplasia type 4: Defined as normal basal turn, but hypoplastic middle and apical turn [20]. Descriptions of this type of abnormality are very recent [11, 20]. There is no current histopathologic description available for this type of cochlear hypoplasia [20]. Given the normal diameter of the basal turn, it is possible that the insult leading to this type of malformation occurs between the tenth and 20th weeks of embryologic development, and the cochlea is probably genetically determined to have such morphology [20]. From imaging observations, it has been noted that the upper 1.5 turns of the cochlea are severely hypoplastic and dislocated to an anterior position [20, 44]. Among the available reports, none of the patients with this type of malformation had bony cochlear nerve canal aplasia. There may be fixation of the stapes and aplasia of oval window as well.
-
(a)
Clinical implications: Considering the normal cochlear basal turn development, patients with his type of cochlear hypoplasia may have a mild hearing loss [23]. The frequency of moderate-to-severe hearing loss is also higher than in other types of cochlear hypoplasia. Those patients frequently have sensorineural or mixed hearing loss, but the presence of pure conductive hearing loss has also been demonstrated as well—for the other types of hypoplasia, there are no clinical descriptions of pure conductive hearing loss [23]. Treatment options are similar to what is described for cochlear hypoplasia type 3 [30].
-
(a)

A horizontal section of a human temporal bone with cochlear hypoplasia type II, harvested from a 5-year-old male patient (Hematoxylin and Eosin). The patient had congenital bilateral profound hearing loss, congenital heart problems, and complete cleft lip and palate. He also had a history of chronic otitis media bilaterally, as diagnosed by physical exam and type B tympanograms. Interestingly, he had a cochlear hypoplasia type III on the contralateral ear. Conditional audiometry revealed residual bone conduction thresholds at the frequencies of 250 and 500 Hz. In this section, it is possible to observe mucoid-purulent effusion, fibrous strands, and granulation tissue in the middle ear. The facial nerve is dehiscent in its tympanic segment. There is a clear abnormality in the footplate. The cochlea is hypoplastic, with a cystic apex; slight hydrops in the upper part of the scala media is observed. The modiolus is hypoplastic, absent in its upper portion. Interscalar septa are absent in the upper part of the cochlea as well. There are identifiable spiral ganglion cells in the Rosenthal’s canal in the lower basal turn and in the lateral posterior wall of the cochlea. There is rudimentary organ of Corti in the basal turn of the cochlea, with adjacent normal stria vascularis and spiral ligament. The bony cochlear nerve canal is hypoplastic, with no cochlear nerve fibers within. Vestibule is hypoplastic, and semicircular canals are aplastic. Saccular wall is slightly dilated. Endolymphatic sac and duct are aplastic. (Source: Human temporal bone archive from the Otopathology Laboratory at the University of Minnesota (USA))

A horizontal section of a human temporal bone with cochlear hypoplasia type III, harvested from a 50-year-old female patient (Hematoxylin and Eosin). The donor died of acute myeloid leukemia, renal failure, gastrointestinal bleeding, and sepsis. At physical examination prior to death, she had retracted tympanic membranes but no signs of inflammation. She complained of a mild hearing loss in the past, which got worse after she was started on ototoxic antibiotics to treat the infection in the moment of admission. Left side: In this panoramic view of the middle and inner ear, it is possible to observe mucoid-purulent effusion, fibrous strands, and granulation tissue in the middle ear and mastoid antrum. The facial nerve is partially dehiscent in its tympanic segment; footplate is normal. Vestibule, saccule, utricle, and semicircular canals are normal; endolymphatic duct and sac are also normal. Right side: A 4× magnification view of the cochlea, at the same level as the figure in the left. The cochlea is hypoplastic, with decreased number of turns as compared to a normal cochlea. The modiolus is normal (as per the size of the cochlea). Interscalar septa are present. Organ of Corti, basilar membrane, Reissner’s membrane, and structures of the lateral wall are normal. There is no apparent decrease in the number of spiral ganglion cells in Rosenthal’s canal; cochlear aperture for the cochlear nerve, internal auditory canal, and cochlear nerve are normal. (Source: Human temporal bone archive from the Otopathology Laboratory at the University of Minnesota (USA))
2.4.2.6 Incomplete Partition Anomalies
In this type of malformation, the cochlea is well defined, with normal or near-normal size, and clearly distinct from the vestibule. According to Sennaroglu and Bajin [30], incomplete partitions account for 41% of all inner ear malformations. In their initial classification published in 2002, Sennaroglu and Saatci [11] initially reported that incomplete partition type I had more severe cochlear abnormalities as compared with cochlear hypoplasia and incomplete partition type II. However, those findings have been later questioned with the description of a wide range of potential types of hypoplasia, as previously mentioned [20]. In terms of development, cochlear hypoplasia seems to occur in an earlier developmental stage as compared with incomplete partition malformations, given that after the cochlea reaches its full size after the eighth week of development, it is not possible to have cochlear hypoplasia (except type IV) [20, 39].
The difference between the types of incomplete partitions is the degree of abnormalities affecting the internal cochlear architecture. Sennaroglu and Saatci [11] classified these abnormalities into three groups:
-
1.
Incomplete partition type I: Externally, the shape of the cochlea is similar to the cochlear hypoplasia type II (round or oval shaped) (Fig. 2.4) [20, 55]. Considering its similarities with other malformations (such as common cavity, rudimentary otocyst, cochlear hypoplasia type I, and even Mondini dysplasia), some of the past clinical descriptions of the incomplete partition type I have been erroneously described under other type of malformation [37, 39]. The difference of the incomplete partition type I from those other abnormalities is that, in this type of malformation, it is possible to clearly identify the cochlea and vestibule (as opposed to common cavity) and the external size of the cochlea is normal (as opposed to cochlear hypoplasia type II and rudimentary otocyst) [39]. Previous histopathologic descriptions of malformations which fit the characteristics of incomplete partition type I were nominated “empty cochlea,” [56] “severe incomplete partition,” [10] “severely dysmorphic cochlea,” [57] and “pseudo-Mondini.” [58]
-
(a)
Internal architecture: The incomplete partition type I is characterized by the absence or subtotal development of the modiolus and absence of interscalar septum (Fig. 2.4). In some cases, there is no bony separation from the cochlear base and internal auditory canal. Lateral cochlear wall structures are hypoplastic or aplastic. The organ of Corti may or not be present—when present, it is rudimentary (Fig. 2.3) [5]. Those findings suggest an earlier developmental arrest than in incomplete partition type II [39].
-
(b)
Bony cochlear nerve canal/cochlear nerve: There is usually a wide communication between the cochlea and internal auditory canal. The cochlear nerve may be aplastic (Fig. 2.4). There seems to be a distribution of spiral ganglion cells along the lateral wall of the cochlea, similarly to what is found in common cavity and cochlear hypoplasia type I deformities [5, 36].
-
(c)
Vestibular system: Vestibule and semicircular canals are frequently grossly dilated (Fig. 2.5), but some cases of aplasia of the posterior semicircular canal have also been described [20]. Enlargement of vestibular aqueduct is very rare—in fact, imaging studies demonstrated that the vestibular aqueduct is not seen at all in some cases [59]. This may be explained by the fact that the vestibular aqueduct is the last structure of the posterior labyrinth to develop, suggesting a developmental arrest before this structure is completely formed [39]. The vestibule is separated from the cochlea by only a very thin membrane (Fig. 2.4), but in some cases a wide communication between the cochlea and vestibule can be seen [5, 20].
-
(d)
Vestibular system: Vestibule and semicircular canals are frequently grossly dilated (Fig. 2.5), but some cases of aplasia of the posterior semicircular canal have also been described [20]. Enlargement of vestibular aqueduct is very rare—in fact, imaging studies demonstrated that the vestibular aqueduct is not seen at all in some cases [59]. This may be explained by the fact that the vestibular aqueduct is the last structure of the posterior labyrinth to develop, suggesting a developmental arrest before this structure is completely formed [39]. The vestibule is separated from the cochlea by only a very thin membrane (Fig. 2.4), but in some cases a wide communication between cochlea and vestibule can be seen [5, 20].
-
(e)
Other associated malformations: Abnormalities in the stapes with areas of absent bone cover on the oval window have been described [20].
-
(f)
Clinical implications: Most patients with incomplete partition type I have severe-to-profound hearing loss—it has been noted by Sennaroglu and Saatci [39] that none of their patients benefit from hearing aids. If a cochlear implant is indicated, considering that the modiolus is absent and the neuron cells are located in the marginal areas of the cochlea, straight electrodes should be used rather than ones designed to “hug” the cochlea, which may lead to poor results and displacement of the electrode into the internal auditory canal [30, 55, 60]. The surgery may be performed using the traditional transmastoid-facial recess approach, but the transmeatal approach may be used considering the possibility of aberrant facial nerve course [37, 55]. The surgeon must be prepared for profuse gusher due to the frequently observed large communication between the cochlea and the internal auditory canal, which should be sealed accordingly [30, 51, 55]. In cases of cochlear nerve aplasia, an auditory brainstem implant is indicated [15, 31]. Due to the anomalies in the footplate, recurrent meningitis is frequent among patients with incomplete partition type I [30, 55].
-
(a)
-
2.
Incomplete partition type II (Mondini dysplasia): In this type of incomplete partition, the upper portion of the modiolus is absent [26]. This has been described by Mondini [2], in addition to the observations of enlarged vestibular aqueduct and dilated vestibule [20, 25, 26]. The association between enlarged vestibular aqueduct and partial modiolar defect has been demonstrated by several authors [27, 57, 61]. There are several histopathologic reports in the literature describing findings in human temporal bones with Mondini dysplasia, including absent vestibular labyrinth and vestibular nerve, enlarged vestibular aqueduct and sac, loss of both vestibular and cochlear hair cells, and atrophy of the stria vascularis [25, 26, 46, 62, 63]. However, it has to be considered that in the past most malformations (including common cavity, cochlear hypoplasia, and incomplete partition type I) were classified as Mondini’s dysplasia [10].
-
(a)
Internal architecture: The apex of the cochlea is frequently cystic and dilated, given the absence of the upper part of the modiolus and its adjacent interscalar septa (Figs. 2.5 and 2.6). The scala vestibuli in the basal turn of the cochlea may be dilated with its corresponded interscalar septum bulged upwards due to increased CSF pressure transmitted through an enlarged vestibular aqueduct (Figs. 2.5 and 2.6) [20, 64]. Some cases of bony defects in the base of the modiolus have been described as well [20, 27]. The internal architecture of the cochlea, especially in the basal turn, may be normal; however, different degrees of hair cell loss have been observed (Figs. 2.4 and 2.5) [26]. There were reports of spots of spiral ligament and stria vascularis atrophy as well, which were more pronounced in the upper cochlear turns (Figs. 2.5 and 2.6) [26].
-
(b)
Bony cochlear nerve canal/cochlear nerve: Normal (Fig. 2.5).
-
(c)
Vestibular system: Vestibule is frequently minimally dilated, and the vestibular aqueduct and sac are enlarged in virtually all cases (Figs. 2.5 and 2.7). The development of the vestibular aqueduct suggests that incomplete partition type II malformations occur in a later embryologic stage as compared with incomplete partition type I.
-
(d)
Other associated malformations: The stapes footplate, oval window, and round window are usually unremarkable [20].
-
(e)
Clinical implications: The degree of hearing loss resulting from the incomplete partition type II varies greatly—Özbal Batuk et al. [59] reported that those patients may have normal hearing or virtually any degree of conductive, mixed, or sensorineural hearing loss. However, in their casuistic, most patients (>75%) had severe-to-profound hearing loss. It is usually observed that patients with incomplete partition type II may have progressive hearing loss, possibly due to further sensorial and neural degeneration caused by the transmission of CSF pressure to the cochlea through the enlarged vestibular aqueduct and sac. Furthermore, it has been observed a positive relationship between the size of the vestibular aqueduct and presence of progressive hearing loss. At young age, patients may have near-normal or normal hearing, but as hearing degeneration progresses they eventually benefit from hearing aids. Most patients progress to (or are born with) severe-to-profound hearing loss, and thus become candidates for cochlear implants. Given the normal-sized cochlea and the normal development of the basal part of the modiolus, any type of electrode may be used. Due to the possible modiolar defects and the increased CSF pressure, either gusher, oozing, or pulsation is frequently observed intraoperatively. The cochlear nerve is always present, and therefore auditory brainstem implants are not indicated [37]. In comparison with patients with incomplete partition type I, patients with incomplete partition type II do have better functional hearing outcomes [60, 65], possibly due to the lesser architectural abnormalities in the cochlear neural structures [60].
-
(a)
-
3.
Incomplete partition type III (X-linked deafness): To date, there are no histopathologic analysis of specimens with this type of malformation in the literature [20]. It is considered to be the least frequent form of inner ear malformation, accounting for 2% of all cases [30]. de Kok et al. [66] have mapped the gene responsible for the characteristic abnormalities to the Xq21 region by linkage analysis, more specifically the POU3F4 gene, located at the Xql3-q22 interval. High-resolution computed tomography scans demonstrate that the otic capsule around the cochlea is very thin, following the outline of the membranous labyrinth. The interscalar septum is present, but cochlear base and modiolus are completely absent. The lateral end of the internal auditory canal is dilated, bulbous, and directly connected to the vestibule and cochlea, while in other cases there is a very thin separation [52, 67]. Such connection between internal auditory canal and the basal turn of the cochlea may transmit pressure from the internal auditory canal to the perilymphatic spaces, increasing the risks of gusher during surgical procedures; however, spontaneous fistulae have never been reported [20, 30]. The vestibular aqueduct is frequently abnormal, with varying degrees of dilatation [30, 68]. Cochlear nerve and cochlear nerve canal are normal. Stapes fixation is also frequent [52].
-
(a)
Clinical implications: Most patients with incomplete partition type 3 have profound mixed or sensorineural hearing loss [30, 52] and also impaired vestibular function, as demonstrated by caloric and head impulse testing [52]. There are three possible explanations for the conductive component in the hearing loss: (1) stapes fixation [52, 66, 69]; (2) increase in the perilymphatic pressure due to the communication between cochlea and internal auditory canal and consequent pressure towards the footplate [70]; and (3) third-window phenomenon [71]. Given the increased pressure in the perilymphatic compartments, it is not recommended to perform stapedectomy in those patients due to the possibility of gusher and difficulties in placing the prosthesis [30, 69]. A loss in residual hearing secondary to this procedure could also be a potential complication [30, 69]. Thus, in patients with severe-to-profound hearing loss, a cochlear implant is indicated [49, 50]. Intraoperatively, the surgeon must be prepared to profuse gusher, which occurs in virtually all cases, which should be fully controlled during the procedure [69]. The literature suggests several different techniques to prevent continuous CSF leak: (1) using cochlear electrode with silicon or “cork type” stoppers to be placed in the site of cochleostomy [69]; (2) sealing around the cochleostomy site with temporalis muscle and fascia grafts [50]; (3) sealing cochleostomy site with muscle and fascia grafts followed by obliteration of the Eustachian tube and middle ear cleft [72]; and (4) subtotal petrosectomy and blind end closure of the external ear canal. In addition, considering the absence of the modiolus and separation from the cochlea and IAC, the electrode may be displaced into the internal auditory canal [69]. Therefore, ideally, the electrode to be selected should be short and have full rings or contact surfaces on both sides [69]. Pre-curved electrodes or other designs aimed to “hug” the cochlea should be avoided, due to increased risks of displacement into the internal auditory canal and damage to the facial nerve [69]. Intraoperative imaging tests must be used to ensure correct electrode positioning [50, 69]. Postoperatively, the patients should be followed periodically due to the increased risks of meningitis or intracranial infection [53].
-
(a)

A horizontal human temporal bone section from a donor who had incomplete partition type I malformation (Hematoxylin and Eosin). The size of the cochlea and vestibule is normal. However, there is no cochlear internal architecture, including modiolus and interscalar septa. In addition, there is a communication between the base of the cochlea and the internal auditory canal. The cochlea is separated from the vestibule by only a small thin membrane. (Source: Reproduced with permission of the “Massachusetts Eye and Ear Infirmary” and “Cochlear Implants International” journal)

A panoramic horizontal section of a right human temporal bone with bilateral incomplete partition type II, harvested from a 90-year-old female donor who died of pneumonia (Hematoxylin and Eosin). She had progressive hearing loss until she became completely deaf at the age of 6. Middle ear and mastoid are normal; cochlea is of normal size, flattened in the upper regions due to abnormal interscalar septum. Bony cochlear nerve aperture and internal auditory canal are normal. Vestibule is also normal, but lateral and posterior semicircular canals seem slightly dilated. The endolymphatic duct and sac are severely enlarged. There is a partial defect in the footplate, which is covered by membranous/fibrous tissue. (Source: Human temporal bone archive from the Otopathology Laboratory at the University of Minnesota (USA))

A 4× cochlea-centered magnification of the human temporal bone section depicted in this figure (incomplete partition type II). The cochlea is of normal size, oddly shaped in the upper regions due to the abnormal interscalar septum. Scala vestibuli looks hydropic, especially in the upper basal turn, which reflects on the flattening of the Reissner’s membrane (arrows pointing down) and the bulging of the interscalar septum upwards (arrows pointing up). The organ of Corti is absent in all cochlear turns, and there is atrophy of the stria vascularis and spiral ligament. The number of spiral ganglion cells is also decreased. (Source: Human temporal bone archive from the Otopathology Laboratory at the University of Minnesota (USA))

A computed tomography scan of a female patient who had progressive bilateral mixed hearing loss, affecting the low frequencies. Figure in the left side: cochlea with cystic apex, Figure in the right side: Enlarged vestibular aqueduct
2.4.2.7 Enlarged Vestibular Aqueduct
The first large study published demonstrating enlargement of the vestibular aqueduct was published by Valvassori and Clemis [73], in 1978. The authors demonstrated, using polytomography, presence of dilatation (>1.5 mm) of the vestibular aqueduct. It is known today that large vestibular aqueducts occur in combination with incomplete partition type II deformities [20]. However, in their series, Valvassori and Clemis found that the enlarged aqueduct was the only abnormal feature in 40% of their cases [73]. An enlarged vestibular aqueduct syndrome may lead to a variety of clinical presentations, from normal hearing to profound hearing loss [27, 65]. The hearing loss may be conductive at the beginning (affecting preferentially the low frequencies, probably due to a third window effect) [29], but over time sensorineural hearing loss progresses, potentially leading to profound hearing loss [29]. It may occur in isolation, association with incomplete partition type II (more frequently) [20], or in association with Pendred syndrome [29]. Treatment of the hearing loss secondary to enlarged vestibular aqueducts should be performed in accordance with the degree of hearing loss (hearing aids or cochlear implants) [65].
2.4.2.8 Cochlear Aperture Abnormalities
The bony cochlear nerve canal, which allows passage of the cochlear nerve from the IAC into the cochlea, may be hypoplastic/narrow (<1.4 mm) or aplastic (canal closed by bone) [30]. They may be followed or not by narrowing of the internal auditory canal [30]. If the internal auditory canal or the bony cochlear nerve canal are hypoplastic, it is necessary to perform T2-weighted magnetic resonance imaging in axial and sagittal oblique planes to evaluate whether cochlear nerve is normal, hypoplastic, or absent [37]. Patients with absent or hypoplastic bony cochlear nerve aperture may have severe-to-profound hearing loss and may be treated with cochlear implants (cochlear nerve present) or auditory brainstem implants (absent cochlear nerve) [37].
2.5 Conclusions
Histopathologic studies of human temporal bones from donors who had malformations, in addition to improvements in the imaging tests, have brought new insights and developments in the current knowledge of inner ear malformations. However, there are still gaps to be filled regarding several anatomic and functional features associated with those abnormalities. Nonetheless, recently, information provided by those histopathologic and imaging studies allowed clinical advances in the treatment of the hearing loss associated with several of those malformations. To ensure continuous improvement in the rehabilitation of those patients, future histopathologic and imaging studies may shed additional light in the hidden aspects of the inner ear malformations.
References
Monsanto RC, Pauna HF, Paparella MM, Cureoglu S. Otopathology in the United States: history, current situation, and future perspectives. Otol Neurotol. 2018;39(9):1210–4. https://doi.org/10.1097/MAO.0000000000001942.
Mondini C. Anatomica hati sectio. De Bononiensi Scientarum et Artium Instituto atque Academia Commentarii. Anat Hati Sect. 1791;7(28):419.
Siebenmann F. Grundzüge der Anatomie und Pathogenese der Taubstummheit. Wiesbaden: J.F. Bergmann; 1904.
Illum P. The Mondini type of cochlear malformation: a survey of the literature. Arch Otolaryngol. 1972;96(4):305–11. https://doi.org/10.1001/archotol.1972.00770090481002.
Khan AM, Levine SR, Nadol JB. The widely patent cochleovestibular communication of Edward Cock is a distinct inner ear malformation: implications for cochlear implantation. Ann Otol Rhinol Laryngol. 2006;115(8):595–606. https://doi.org/10.1177/000348940611500805.
Michel P. Mémoire sur les anomalies congénitales de l’oreille interne. Gaz Méd Strasbg. 1863;23:55–8.
Jackler RK. Chapter 152: Congenital malformations of the inner ear. In: Otolaryngology-head and neck surgery. 2nd ed. Mosby-Yearbook: Chicago, IL; 1993.
Scheibe A. Ein Fall von Taubstummheit mit Acusticusatrophie und Bildungsanomalien im häutigen Labyrinth beiderseits. Z Ohrenheilkd. 1892;22:11–24.
Alexander G. Zur Pathologie und pathologischen Anatomie der kongenitalen Taubheit. Arch Für Ohrenheilkd. 1904;61(3):183–219. https://doi.org/10.1007/BF01808972.
Jackler RK, Luxford WM, House WF. Congenital malformations of the inner ear: a classification based on embryogenesis. Laryngoscope. 1987;97(3 Pt 2 Suppl 40):2–14.
Sennaroglu L, Saatci I. A new classification for cochleovestibular malformations. Laryngoscope. 2002;112(12):2230–41. https://doi.org/10.1097/00005537-200212000-00019.
Sennaroglu L, Sarac S, Ergin T. Surgical results of cochlear implantation in malformed cochlea. Otol Neurotol. 2006;27(5):615–23. https://doi.org/10.1097/01.mao.0000224090.94882.b4.
Silverstein H, Smouha E, Morgan N. Multichannel cochlear implantation in a patient with bilateral Mondini deformities. Am J Otol. 1988;9(6):451–5.
Tucci DL, Telian SA, Zimmerman-Phillips S, Zwolan TA, Kileny PR. Cochlear implantation in patients with cochlear malformations. Arch Otolaryngol Head Neck Surg. 1995;121(8):833–8.
Monsanto RC, Bittencourt AG, Neto NJB, et al. Auditory brainstem implants in children: results based on a review of the literature. Int J Adv Otol. 2014;10(2):284–90.
Mangabeira-Albernaz PL. The Mondini dysplasia--from early diagnosis to cochlear implant. Acta Otolaryngol. 1983;95(5–6):627–31.
Terrahe K. Missbildungen des Innen- und Mittelohres als Folge der Thalidomidembryopathie: Ergebnisse von Röntgenschichtuntersuchungen. Fortschr Röntgenstr. 1965;102:14.
Papsin BC. Cochlear implantation in children with anomalous cochleovestibular anatomy. Laryngoscope. 2005;115(1 Pt 2 Suppl 106):1–26. https://doi.org/10.1097/00005537-200501001-00001.
Marangos N. Dysplasien des Innenohres und inneren Gehörganges. HNO. 2002;50:866–81.
Sennaroglu L. Histopathology of inner ear malformations: do we have enough evidence to explain pathophysiology? Cochlear Implants Int. 2016;17(1):3–20. https://doi.org/10.1179/1754762815Y.0000000016.
Jeong S-W, Kim L-S. A new classification of cochleovestibular malformations and implications for predicting speech perception ability after cochlear implantation. Audiol Neurootol. 2015;20(2):90–101. https://doi.org/10.1159/000365584.
Rodriguez K, Shah RK, Kenna M. Anomalies of the middle and inner ear. Otolaryngol Clin N Am. 2007;40(1):81–96. https://doi.org/10.1016/j.otc.2006.10.006, vi.
Cinar BC, Batuk MO, Tahir E, Sennaroglu G, Sennaroglu L. Audiologic and radiologic findings in cochlear hypoplasia. Auris Nasus Larynx. 2017;44(6):655–63. https://doi.org/10.1016/j.anl.2016.12.002.
Bartel-Friedrich S, Wulke C. Classification and diagnosis of ear malformations. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2008;6:Doc05. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3199848/. Accessed 26 Nov 2018.
Kaya S, Hızlı Ö, Kaya FK, Monsanto RD, Paparella MM, Cureoglu S. Peripheral vestibular pathology in Mondini dysplasia. Laryngoscope. 2017;127(1):206–9. https://doi.org/10.1002/lary.25995.
Paparella MM. Mondini’s deafness. A review of histopathology. Ann Otol Rhinol Laryngol Suppl. 1980;89(2 Pt 3):1–10.
Hirai S, Cureoglu S, Schachern PA, Hayashi H, Paparella MM, Harada T. Large vestibular aqueduct syndrome: a human temporal bone study. Laryngoscope. 2006;116(11):2007–11. https://doi.org/10.1097/01.mlg.0000237673.94781.0a.
Cureoglu S, Schachern PA, Paparella MM. Scheibe dysplasia. Otol Neurotol. 2003;24(1):125.
Merchant SN. Genetically determined and other developmental defects. In: Schuknecht’s pathology of the ear. 3rd ed. New Heven, CT: People’s Medical Publishing House; 2010.
Sennaroğlu L, Bajin MD. Classification and current management of inner ear malformations. Balkan Med J. 2017;34(5):397–411. https://doi.org/10.4274/balkanmedj.2017.0367.
Sennaroglu L, Ziyal I. Auditory brainstem implantation. Auris Nasus Larynx. 2012;39(5):439–50. https://doi.org/10.1016/j.anl.2011.10.013.
Li CW. Congenital malformation of inner ear. Dev Neurosci. 1979;2(1):7–18. https://doi.org/10.1159/000112434.
Ruben RJ. Development and cell kinetics of the kreisler (kr-kr) mouse. Laryngoscope. 1973;83(9):1440–68. https://doi.org/10.1288/00005537-197309000-00006.
Van De Water TR. Effects of removal of the statoacoustic ganglion complex upon the growing otocyst. Ann Otol Rhinol Laryngol. 1976;85(6 Suppl 33 Pt 2):2–31. https://doi.org/10.1177/00034894760850S602.
Schmidt RS, Sismanis A. Common cavity deformity. Otol Neurotol. 2008;29(4):567. https://doi.org/10.1097/MAO.0b013e31815ae9ef.
Graham JM, Phelps PD, Michaels L. Congenital malformations of the ear and cochlear implantation in children: review and temporal bone report of common cavity. J Laryngol Otol Suppl. 2000;25:1–14.
Sennaroglu L. Cochlear implantation in inner ear malformations--a review article. Cochlear Implants Int. 2010;11(1):4–41. https://doi.org/10.1002/cii.416.
Joshi VM, Navlekar SK, Kishore GR, Reddy KJ, Kumar ECV. CT and MR imaging of the inner ear and brain in children with congenital sensorineural hearing loss. Radiogr Rev. 2012;32(3):683–98. https://doi.org/10.1148/rg.323115073.
Sennaroglu L, Saatci I. Unpartitioned versus incompletely partitioned cochleae: radiologic differentiation. Otol Neurotol. 2004;25(4):520–9; discussion 529.
Freeman SR, Sennaroglu L. Management of cochlear nerve hypoplasia and aplasia. Adv Hear Rehabil. 2018;81:81–92. https://doi.org/10.1159/000485542.
Glastonbury CM, Davidson HC, Harnsberger HR, Butler J, Kertesz TR, Shelton C. Imaging findings of cochlear nerve deficiency. Am J Neuroradiol. 2002;23(4):635–43.
Peng KA, Kuan EC, Hagan S, Wilkinson EP, Miller ME. Cochlear nerve aplasia and hypoplasia: predictors of cochlear implant success. Otolaryngol Neck Surg. 2017;157(3):392–400. https://doi.org/10.1177/0194599817718798.
Beltrame MA, Frau GN, Shanks M, Robinson P, Anderson I. Double posterior labyrinthotomy technique: results in three Med-El patients with common cavity. Otol Neurotol. 2005;26(2):177–82.
Sennaroğlu L, Bajin MD, Pamuk E, Tahir E. Cochlear hypoplasia type four with anteriorly displaced facial nerve canal. Otol Neurotol. 2016;37(10):e407–9. https://doi.org/10.1097/MAO.0000000000001220.
Tahir E, Bajin MD, Atay G, Mocan BÖ, Sennaroğlu L. Bony cochlear nerve canal and internal auditory canal measures predict cochlear nerve status. J Laryngol Otol. 2017;131(8):676–83. https://doi.org/10.1017/S0022215117001141.
Schuknecht HF. Mondini dysplasia; a clinical and pathological study. Ann Otol Rhinol Laryngol Suppl. 1980;89(1 Pt 2):1–23.
Otte J, Schunknecht HF, Kerr AG. Ganglion cell populations in normal and pathological human cochleae. Implications for cochlear implantation. Laryngoscope. 1978;88(8 Pt 1):1231–46. https://doi.org/10.1288/00005537-197808000-00004.
Pollak A, Felix H. Histopathological features of the spiral ganglion and cochlear nerve in temporal bones from three patients with profound hearing loss. Acta Otolaryngol Suppl. 1985;423:59–66.
Cosetti MK, Friedmann DR, Heman-Ackah SE, Perez R, Waltzman SB, Roland JT. Surgical techniques and outcomes of cochlear implantation in patients with radiographic findings consistent with X-linked deafness. Int J Pediatr Otorhinolaryngol. 2015;79(10):1689–93. https://doi.org/10.1016/j.ijporl.2015.07.027.
Saeed H, Powell HRF, Saeed SR. Cochlear implantation in X-linked deafness - how to manage the surgical challenges. Cochlear Implants Int. 2016;17(4):178–83. https://doi.org/10.1080/14670100.2016.1180018.
Cabbarzade C, Sennaroglu L, Süslü N. CSF gusher in cochlear implantation: the risk of missing CT evidence of a cochlear base defect in the presence of otherwise normal cochlear anatomy. Cochlear Implants Int. 2015;16(4):233–6. https://doi.org/10.1179/1754762813Y.0000000048.
Phelps PD, Reardon W, Pembrey M, Bellman S, Luxom L. X-linked deafness, stapes gushers and a distinctive defect of the inner ear. Neuroradiology. 1991;33(4):326–30.
Incesulu A, Adapinar B, Kecik C. Cochlear implantation in cases with incomplete partition type III (X-linked anomaly). Eur Arch Otorhinolaryngol. 2008;265(11):1425–30. https://doi.org/10.1007/s00405-008-0614-z.
Pulcherio JOB, Bittencourt AG, Burke PR, et al. Carina® and Esteem®: a systematic review of fully implantable hearing devices. PLoS One. 2014;9(10):e110636. https://doi.org/10.1371/journal.pone.0110636.
Berrettini S, Forli F, De Vito A, Bruschini L, Quaranta N. Cochlear implant in incomplete partition type I. Acta Otorhinolaryngol Ital. 2013;33(1):56–62.
Reisner K. Tomography in inner and middle ear malformations: value, limits, results. Radiology. 1969;92(1):11–20. https://doi.org/10.1148/92.1.11.
Davidson HC, Harnsberger HR, Lemmerling MM, et al. MR evaluation of vestibulocochlear anomalies associated with large endolymphatic duct and sac. AJNR Am J Neuroradiol. 1999;20(8):1435–41.
Phelps PD. Mondini and “pseudo Mondini”. Clin Otolaryngol Allied Sci. 1990;15(2):99–101.
Özbal Batuk M, Çınar BÇ, Özgen B, Sennaroğlu G, Sennaroğlu L. Audiological and radiological characteristics in incomplete partition malformations. J Int Adv Otol. 2017;13(2):233–8. https://doi.org/10.5152/iao.2017.3030.
Kontorinis G, Goetz F, Giourgas A, Lenarz T, Lanfermann H, Giesemann AM. Radiological diagnosis of incomplete partition type I versus type II: significance for cochlear implantation. Eur Radiol. 2012;22(3):525–32. https://doi.org/10.1007/s00330-011-2301-5.
Lemmerling MM, Mancuso AA, Antonelli PJ, Kubilis PS. Normal modiolus: CT appearance in patients with a large vestibular aqueduct. Radiology. 1997;204(1):213–9. https://doi.org/10.1148/radiology.204.1.9205250.
Zheng Y, Schachern PA, Cureoglu S, Mutlu C, Dijalilian H, Paparella MM. The shortened cochlea: its classification and histopathologic features. Int J Pediatr Otorhinolaryngol. 2002;63(1):29–39.
Sampaio ALL, Cureoglu S, Schachern PA, Kusunoki T, Paparella MM, Oliveira CACP. Massive endolymphatic sac and vestibular aqueduct in Mondini dysplasia. Arch Otolaryngol Head Neck Surg. 2004;130(5):678–80. https://doi.org/10.1001/archotol.130.5.678.
Holden PK, Linthicum FH. Mondini dysplasia of the bony and membranous labyrinth. Otol Neurotol. 2005;26(1):133.
Sefein I, Younes A, Omara A, Hamada S, Sami A, El Rouby I. Outcome of cochlear implantation in children with enlarged vestibular aqueduct (EVA) and Mondini dysplasia (incomplete partition type II). J Med Sci Res. 2018;1(1):17. https://doi.org/10.4103/JMISR.JMISR_7_18.
de Kok YJ, van der Maarel SM, Bitner-Glindzicz M, et al. Association between X-linked mixed deafness and mutations in the POU domain gene POU3F4. Science. 1995;267(5198):685–8.
Cremers CW, Hombergen GC, Scaf JJ, Huygen PL, Volkers WS, Pinckers AJ. X-linked progressive mixed deafness with perilymphatic gusher during stapes surgery. Arch Otolaryngol. 1985;111(4):249–54.
Talbot JM, Wilson DF. Computed tomographic diagnosis of X-linked congenital mixed deafness, fixation of the stapedial footplate, and perilymphatic gusher. Am J Otol. 1994;15(2):177–82.
Sennaroğlu L, Bajin MD. Incomplete partition type III: a rare and difficult cochlear implant surgical indication. Auris Nasus Larynx. 2018;45(1):26–32. https://doi.org/10.1016/j.anl.2017.02.006.
Tang A, Parnes LS. X-linked progressive mixed hearing loss: computed tomography findings. Ann Otol Rhinol Laryngol. 1994;103(8 Pt 1):655–7. https://doi.org/10.1177/000348949410300814.
Snik AF, Hombergen GC, Mylanus EA, Cremers CW. Air-bone gap in patients with X-linked stapes gusher syndrome. Am J Otol. 1995;16(2):241–6.
Wootten CT, Backous DD, Haynes DS. Management of cerebrospinal fluid leakage from cochleostomy during cochlear implant surgery. Laryngoscope. 2006;116(11):2055–9. https://doi.org/10.1097/01.mlg.0000240286.43289.87.
Valvassori GE, Clemis JD. The large vestibular aqueduct syndrome. Laryngoscope. 1978;88(5):723–8.
Acknowledgements
This project was funded by the NIH grant number: 1 UG3 NS107688-01, the International Hearing Foundation; the 5M Lions International; and the Starkey Foundation. The authors have no other funding, financial relationships, or conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 Springer Nature Switzerland AG
About this chapter

Cite this chapter
da Costa Monsanto, R., Cureoglu, S., Sancak, I.G., Sennaroglu, L., Paparella, M.M. (2022). Histopathologic Findings in Inner Ear Malformations. In: Sennaroglu, L. (eds) Inner Ear Malformations. Springer, Cham. https://doi.org/10.1007/978-3-030-83674-0_2
Download citation
DOI: https://doi.org/10.1007/978-3-030-83674-0_2
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-83673-3
Online ISBN: 978-3-030-83674-0
eBook Packages: MedicineMedicine (R0)