
Abstract
Facial nerve paralysis is the single most common cranial neuropathy. The course of the nerve is long with the nerve traversing potential sites of injury, and the slightest change in facial symmetry is often promptly noted. Most of the time, an exact etiology of the facial nerve paralysis is never found, which is the phenomenon called Bell’s palsy. The next most common cause is herpes zoster oticus, also known as Ramsay Hunt syndrome. Facial paralysis can be due to central causes, which causes an upper motor neuron pattern of weakness that spares the forehead muscles. A lower motor neuron pattern of weakness, as in the case of facial nerve paralysis, involves the forehead muscles. Facial nerve paralysis presents with weakness of the muscles of facial expression on the ipsilateral side, with inability to close the eye, inability to wrinkle the forehead, and a drooping mouth. The facial nerve has numerous functions in addition to moving the muscles of facial expression, and patients may also complain of altered lacrimation, taste, salivation, and hearing. Despite the fact that the etiology is often unknown, or so-called idiopathic, there is proven benefit for a short course of steroids when started within 3 days of onset. There is also additional benefit of treatment with antiviral agents in individuals with Ramsay Hunt syndrome in addition to steroids.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The facial nerve, cranial nerve VII, innervates the muscles of facial expression and supplies innervation for lacrimation, salivation, taste on the anterior two-thirds of the tongue, dampening of sound, as well as sensation for the auricle. Bell’s palsy is the term for facial nerve paralysis of unknown cause, and it is named after Sir Charles Bell who first identified the syndrome and the function of the facial nerve [1]. The facial nerve has an extended course which involves an intracranial and extracranial path, with some areas of difficulty along its course, particularly the temporal bone and at its entrance to the bony facial canal. In addition to the psychological toll of facial nerve paralysis, there is risk of corneal abrasion due to inability to blink, along with alterations of speech and smiling, and inadequate facial animation.
Epidemiology
Bell’s palsy is more common in those aged 15–45 years old; those with diabetes, upper respiratory disease, or immune compromise; and during pregnancy. It has an estimated incidence of 11.5–53.3 per 100,000 person-years [2]. In a retrospective study which looked at 1989 patients referred for facial nerve palsy, Bell’s palsy was the diagnosis in 38%, acoustic neuroma resection in 10%, malignancy in 7%, iatrogenic injury in 7%, varicella zoster virus infection in 7%, Lyme disease in 4%, and other etiologies in 17% [3]. Women made up a majority of cases at 62% and the mean age was 44.5 years [3].
In a study of 1701 patients with Bell’s palsy, 71% eventually achieved normal facial nerve function, with a majority of patients having a complete recovery by 2 months [4]. Complete recovery is less likely if there has been no or minimal improvement after 3 months from symptom onset. Prognosis is better for those with incomplete Bell’s palsy as compared to those with complete Bell’s palsy [4].
The occurrence of bilateral facial nerve palsy is rare; an estimated 0.3–2.0% of facial nerve palsies are bilateral [5]. Of those with facial diplegia, 20% are idiopathic. The causes of facial diplegia include Guillain-Barre syndrome, sarcoidosis, multiple sclerosis, HIV, Lyme disease, diabetes, acute leukemia, and porphyria [6].
Facial Nerve Anatomy
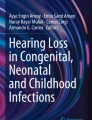
An understanding of the anatomy of the facial nerve’s course is immensely helpful in understanding the pathogenesis of facial nerve palsy (Fig. 7.1). The facial nerve has a motor division and a sensory division. Within the sensory root of the facial nerve are sensory fibers which end in the spinal nucleus of cranial nerve V and preganglionic parasympathetic fibers and taste axons [7]. The facial nucleus is in the lateral pons, and the motor fibers exit the brainstem ventrolaterally at the pontomedullary junction. The sensory division of the facial nerve is separate from the motor division between the brainstem and the internal acoustic canal, but the two divisions join to enter the internal auditory meatus and course through the auditory canal of the petrous temporal bone. Cranial nerve VIII also travels through the auditory canal with cranial nerve VII. The facial nerve path through the temporal bone can be separated into four parts: the meatus, labyrinthine, tympanic, and mastoid parts. The meatus is the narrowest portion of the facial canal and is implicated as the site of facial nerve compression in Bell’s palsy as it is quite narrow at 0.68 mm, with little room for the facial nerve to swell from any potential inflammation [8]. The labyrinthine segment is named for its proximity to the superior semicircular canal. This segment ends at the geniculate ganglion, which contains sensory neurons for taste of the anterior two-thirds of the tongue and general somatic sensation for the region near the external auditory meatus. The greater petrosal nerve branches out from the geniculate ganglion, and this eventually supplies lacrimation through parasympathetic fibers. In the tympanic segment, the stapedius nerve branches off to supply the stapedius muscle, which works to dampen sound by stabilizing the stapes bone. The stapedius muscle is interesting as it is the smallest muscle in the human body, and the stapes is the smallest bone in the human body. The mastoid segment descends to the stylomastoid foramen to proceed extracranially. The chorda tympani branches off the facial nerve in the mastoid segment, and this ultimately supplies parasympathetic fibers to the sublingual and submandibular glands, along with relaying taste from the anterior two-thirds of the tongue [9]. Most saliva production (about 70 percent) originates from the submandibular salivary glands [10]. The facial nerve then travels through the parotid gland and branches into the five major branchial motor branches which control the muscles of facial expression: the temporal, zygomatic, buccal, mandibular, and cervical branches [9].

Anatomy of the seventh cranial nerve. (Reproduced from Gilchrist [51])
The facial nerve has four main functional subdivisions: special visceral efferent, general visceral efferent, special afferent, and general somatic afferent subdivisions. The special visceral efferent subdivision, also known as the branchial branch, supplies motor innervation to the muscles of facial expression, the stylohyoid, stapedius, and the posterior belly of the digastric muscle. The general visceral efferent subdivision supplies parasympathetic innervation to the submandibular, sublingual, and lacrimal glands. The special sensory afferent subdivision of facial nerve supplies taste from the anterior two-thirds of the tongue. General somatic afferents provide sensory information from the tympanic membrane, external auditory canal, and the auricle [11].
Pathophysiology and Pathogenesis
As Bell’s palsy is the term for acute facial nerve paralysis when no other medical etiology of facial weakness is determined, it is therefore a diagnosis of exclusion. There are a vast number of etiologies for facial nerve paralysis (Table 7.1). The two broad main categories are an acquired deficit of the facial nerve, such as infection or injury to the nerve, or congenital malformations [12]. True developmental anomalies are rare and include Moebius syndrome and neonatal asymmetric crying facies. Moebius syndrome is a rare neurologic condition, with an incidence of about one in 50,000 in which children have trouble with muscles of facial expression and eye movement, along with micrognathia and microstomia [13].
Acquired facial nerve paralysis is much more common than congenital. The most common infectious causes of facial nerve paralysis are herpes simplex virus and varicella zoster virus. Infectious causes can lead to inflammation which compresses the nerve in the small enclosures of the facial canal. Both viruses are acquired in childhood and can reactivate from their latent state in the trigeminal or geniculate ganglia causing inflammation and paralysis [14]. McCormick first suggested that herpes simplex virus was a cause of acute facial nerve paralysis in 1972, hypothesizing that the virus remained in nerve cell endings and axons [15]. Using PCR testing on autopsy specimens, herpes simplex virus was present in 94 percent of trigeminal ganglia and 88 percent of geniculate ganglia [16]. There is increased incidence of facial paralysis in diabetic patients, and it has been suggested based on an animal study that reactivation of HSV-1 in the geniculate ganglion may be responsible for the increased incidence in diabetic patients [17].
Ramsay Hunt syndrome is peripheral facial neuropathy with an accompanying vesicular rash of the ear (herpes zoster oticus) or mouth. The cause of Ramsey Hunt syndrome is varicella zoster virus. Patients presenting with Ramsay Hunt syndrome may also complain of tinnitus, hearing loss, nausea, and vertigo, and they tend to have a severe facial paralysis with poor recovery [18]. Hunt described the proximity of the vestibulocochlear nerve to the geniculate ganglion in the confines of the bony facial canal [19], and this explains the symptoms of tinnitus, hearing loss, nausea, and vertigo seen in Ramsay Hunt syndrome.
Borrelia burgdorferi, the tick-born spirochete that causes Lyme disease, can cause a unilateral or bilateral facial nerve paralysis. Lyme disease should be considered in those presenting with facial palsy as well tick exposure, arthralgia, or the classic bull’s eye skin rash of erythema nodosa associated with Lyme disease. It is reported that 10 percent of patients with Lyme disease have facial nerve palsy [20], and a study from the UK found that younger patients with Lyme disease were more likely to develop facial paralysis, possibly due to a younger population of hikers and campers [21]. Facial nerve paralysis due to Lyme disease has a good prognosis, with 95 percent of patients having a complete recovery if diagnosed early [22].
Facial nerve palsy in pregnancy is hypothesized to be due to relative immunosuppression that allows for reactivation of herpes virus, or increased extracellular volume, hypertension, or changes in hormone levels [23]. Retrospective data has shown that pregnant women may have a worse prognosis of facial nerve paralysis, as pregnant women are more likely to have a complete facial nerve paralysis [24].
Central processes are also responsible for facial palsy and include ischemia, tumor, stroke, and multiple sclerosis, among others. Facial palsy sometimes is the first sign of multiple sclerosis, but will typically present with other brainstem signs [25]. Bilateral and unilateral facial paralysis has been described in neurosarcoidosis, which can also present with myelopathy, optic neuropathy, cerebral mass lesions, and polyneuropathy. The treatment is 1 milligram per kilogram per day of prednisone or, in severe cases, intravenous methylprednisolone [26].
Clinical Presentation
The onset of acute facial nerve paralysis is typically less than 72 h [2]. Patients often present with inability to close the eye, drooping of the corner of the mouth, and loss of the nasolabial fold. There is a facial asymmetry on examination of the face: the facial creases and the nasolabial fold disappear; the affected side also may have a drooping mouth, eyelid widening, and lagophthalmos, all of which are static signs. Dynamic signs include the inability to whistle, puff the checks, frown, and close the eyelid [27]. Paralysis of all muscles of facial expression on one side is consistent with a lower motor neuron pathology, while an upper motor neuron pathology, such as a stroke, spares the frontalis muscle of the forehead.
Many experience a Bell’s phenomenon, which is the rolling of the eye upwards upon trying to close the eyelid. Patients may complain of food and beverage spilling out of their mouth, and some complain of subjective numbness of the paralyzed area [28]. A postulated mechanism for this numbness is herpetic viral spread along an anatomical course involving the trigeminal nerve [29].
Along with facial muscle weakness, patients can experience impaired salivation and lacrimation due to compromise of the parasympathetic fibers of the seventh cranial nerve. Hearing loss is not a typical sign, although hyperacusis does occur as the seventh cranial nerve supplies innervation to the stapedius muscle. Damage to the chorda tympani nerve can result in dysgeusia.
Bell’s palsy is a complication of pregnancy with an incidence in pregnant women of 45.1 per 100,000 births, while nonpregnant women of the same age group is 17.4 in 100,000. Of 42 cases of Bell’s palsy in pregnancy, 31 of those cases occurred in the third trimester [30]. It is important to distinguish an upper motor neuron facial nerve palsy, such as a stroke, from a lower motor neuron facial nerve palsy in a pregnant woman with facial weakness as the management is distinctly different.
As a general rule, a complete facial paralysis on initial presentation carries a poorer prognosis for recovery as compared to partial facial paralysis. The presence of complete facial paralysis, hypertension, and non-ear pain all are associated with incomplete recovery [28]. A cohort study of 368 patients with Bell’s palsy found that normal stapedius reflex testing and no pathological spontaneous activity in EMG were significant prognostic factors of recovery, and prednisolone therapy initiated after 96 h had a decreased recovery rate then when it was started earlier in the course. In the same study, the median onset of treatment was 1.5 days, and the median recovery time was 2.6 months [31].
In the process of recovery, regenerating fibers can reach the wrong target, leading to phenomena such as crocodile tears, in which a person exhibits lacrimation instead of salivation at the sight of food [10]. Abnormal recovery of motor fibers can lead to synkinesis, which is an abnormal involuntary movement that occurs during voluntary movement of another muscle. For example, a patient may try to volitionally close the eye, but instead, the muscles of the mouth contract.
The presence of bilateral facial nerve palsy, which is far more rare than unilateral facial nerve palsy, should broaden the differential diagnosis to include Lyme disease, Guillain-Barré syndrome, HIV, sarcoidosis, multiple sclerosis, diabetes, or leukemia [6].
Diagnosis
The diagnosis of acute facial nerve palsy does not typically require a plethora of testing and can be made with bedside examination. The ear should be examined to assess for herpes zoster oticus, which presents as vesicles on the external auditory canal, concha, or helix, although the absence of visible lesions does not exclude Ramsay Hunt syndrome [32]. Imaging is not absolutely required, and clinicians can rely mostly on history and physical to establish the diagnosis readily. The most important question to answer in an acute setting is whether the facial weakness is due to a central or peripheral cause. An upper motor neuron pattern of weakness, or a central cause of weakness, spares the forehead of weakness; this pattern of facial weakness should alarm clinicians for a stroke or other central causes.
Upper motor neuron facial weakness will not have accompanied hyperacusis or dysgeusia, and stroke or other upper motor neuron dysfunction will likely present with other deficits beyond the face. The muscles that supply the forehead receive bilateral supranuclear innervation, while the facial muscles of the middle and lower face receive unilateral innervation from contralateral upper motor neurons [33]. A lower motor neuron pattern of weakness causes paralysis of an entire side of the face, including the forehead. This weakness is ipsilateral to the facial nerve paralysis.
Imaging is not necessary if there is high suspicion for isolated facial nerve paralysis. However, if facial weakness if suspected to be secondary to another cause, then imaging can be helpful in evaluating for pontine lesions or an internal acoustic canal mass. Bilateral facial paralysis or the involvement of multiple cranial nerves should also prompt imaging and examination of cerebrospinal fluid evaluation, as this can be the presentation of multiple sclerosis, neurosarcoidosis, or cancer with central nervous system involvement.
Testing for Lyme disease is warranted if there is suspicion that the patient has been exposed to a tick, especially in areas where the disease is more prevalent. The first is an enzyme immunoassay (EIA) or immunofluorescence assay of antibodies to the spirochete Borrelia burgdorferi. A positive result may indicate past or current infection, or it may be a false positive. If the result of this first step is positive or equivocal, then obtain a Western blot (immunoblot) assay for IgM and IgG; this test is more specific for Lyme disease than the EIA. The Western blot for IgM is particularly helpful when symptoms have been present for less than 4 weeks [34]. After 1 month into the course of the disease, there should be an IgG response and so an isolated IgM antibody is most likely a false positive [35]. False positives may occur with testing of IgM, the largest antibody, as there can be cross-reactivity with other pathogens [36]. The sensitivity of this two-step testing method is 70–100 percent with above 95 percent specificity [37].
EMG can be considered in those with complete facial nerve paralysis, as those with greater than 90 percent axonal loss of facial nerve can be considered for facial nerve decompression [38]. However, strong evidence for the efficacy of surgical decompression of the facial nerve is lacking, as there are limited randomized controlled trials with low power [39]. Risks of the surgery include persistent vertigo [39] and unilateral sensorineural hearing loss, with one study reporting deafness in 15 percent of patients who underwent surgical decompression [40].
MRI can be considered in those with multiple cranial nerve dysfunction or other neurologic signs. Gadolinium enhancement of the facial nerve can be seen on MRI in some patients with facial nerve paralysis, but the presence of this enhancement does not indicate a worse prognosis [41].
Management and Treatment
The main pearls of management of acute facial nerve palsy are corticosteroids with the use of eye lubricants to prevent corneal abrasion [1]. Antiviral therapy may also be beneficial (see below).
Steroids in the treatment of acute facial nerve palsy have proven to be an effective treatment. Earlier studies, including a 2004 meta-analysis of four randomized controlled trials, showed no benefit of facial nerve paralysis treatment with corticosteroids [42]. A 2009 meta-analysis of 18 randomized controlled trials, which involved 2786 patients, concluded that corticosteroids were associated with greater benefit (reduced risk of unsatisfactory recovery) than antivirals alone, and there was added benefit if corticosteroids and antivirals were used together [43].
A randomized, double-blind, placebo-controlled, multicenter trial was conducted with the primary outcome of time to complete recovery of facial function. Patients were randomized to placebo, prednisolone 60 milligrams per day for 5 days then reduced by 10 milligrams per day plus placebo, 1000 milligrams valacyclovir three times a day for 7 days plus placebo, or prednisolone for 10 days plus valacyclovir for 7 days. Time to recovery was shorter in patients who received prednisolone compared to those who did not (hazard ratio 1.40, 95 percent CI 1.18–1.64; p < 0.0001). There was no difference in time to recovery in those treated with valacyclovir and those who did not receive valacyclovir [44].
Additional treatment with antivirals appears to have a very modest effect on recovery, with a reported 7 percent increase in probability of facial functional recovery. A large review of 14 trials showed that corticosteroid monotherapy was probably more effective than monotherapy with antivirals, and antivirals with corticosteroids were more effective than placebo or no treatment [45]. The antiviral of choice is valacyclovir 1 gram three times per day for 7 days. Prednisone is administered at a dose of 60 milligrams per day for 10 days. Complications of prednisone can include dyspepsia, duodenal ulcer activation, uncontrolled diabetes, and acute psychosis; however, these complications occur in less than 4 percent of patients who received prednisone [46].
Early medical attention is preferred as there is no benefit of medications administered after 4 days of onset of symptoms [1]. Patients should be prescribed eye lubrication to be used hourly throughout the day, and those with corneal abrasions should be referred to ophthalmology.
For those with Lyme disease as the identified cause of facial paralysis, doxycycline is the recommended antibiotic. Doxycycline is given in a dose of 100 milligrams orally twice daily for 10–21 days. Alternatively, other antibiotic regimens include cefuroxime 500 milligrams orally twice daily or amoxicillin 500 milligrams orally three times daily for 14–21 days [47].
For pregnant women who present with acute facial nerve paralysis, the risks and benefits should be evaluated in the clinical context. Although recovery tends to be worse in pregnant women with facial paralysis, there is extra risk with use of steroids in the presence of concurrent hyperglycemia and hypertension. Steroids are FDA pregnancy category C and are probably safe during lactation. In the absence of clear viral infection, antiviral therapy, which is category B and considered safe in breast-feeding, can probably be held in pregnant women with facial nerve paralysis as the benefit is modest [24].
There lack sufficient data and consensus as to the benefit of decompressive surgery as a therapy for facial paralysis, along with a lack of uniformity of who should get surgery and when during the disease surgery is most efficacious [48]. A small non-randomized, non-blinded study did show benefit of surgical treatment with decompression in patients with severe facial paralysis. Patients who were offered surgery had total facial paralysis with greater than 90 percent decrease in motor amplitude compared to the unaffected side and no voluntary motor unit potentials on needle EMG exam [49]. However, the benefit of surgical decompression has been a controversial topic [50].
Conclusion
Facial neuropathy manifests as unilateral facial weakness, and an unknown cause of facial nerve paralysis is a Bell’s palsy. Clinicians should make the distinction between acute stroke and facial nerve paralysis. In facial nerve paralysis, there is weakness of the entire unilateral side of the face, while stroke produces an upper motor neuron pattern of weakness which spares the forehead muscles. Patients with facial nerve palsy commonly have a drooping mouth and inability to close the eye and may have alterations in lacrimation, taste, salivation, and hearing. Common causes of facial nerve palsy include infectious etiologies, such as herpes zoster oticus (Ramsay Hunt syndrome) or herpes simplex virus. Treatment should be initiated within 3 days of onset, and this consists of at least a 5-day course of corticosteroids at a suggested dose of 60 milligrams per day of prednisone. There is some additional benefit in treating with valacyclovir. Diagnostic workup should be tailored to each clinical scenario, and generally imaging and cerebrospinal fluid analysis should be reserved for those presenting with multiple cranial nerve deficits or other neurologic signs.
References
Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997–1002.
Baugh RF, Basura GJ, Ishii LE, Schwartz SR, Drumheller CM, Burkholder R, et al. Clinical practice guideline: Bell’s palsy. Otolaryngol Head Neck Surg. 2013;149(3 Suppl):S1–27.
Hohman MH, Hadlock TA. Etiology, diagnosis, and management of facial palsy: 2000 patients at a facial nerve center. Laryngoscope. 2014;124(7):E283–93.
Peitersen E. Bell’s palsy: the spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002;549:4–30.
Jung J, Park DC, Jung SY, Park MJ, Kim SH, Yeo SG. Bilateral facial palsy. Acta Otolaryngol. 2019;139(10):934–8.
Kumar P, Charaniya R, Bahl A, Ghosh A, Dixit J. Facial diplegia with paresthesia: an uncommon variant of guillain-barre syndrome. J Clin Diagn Res. 2016;10(7):Od01–2.
DeMyer W. Neuroanatomy. 2nd ed. Baltimore: Williams & Wilkins; 1998. p. xi, 463 p.
Kochhar A, Larian B, Azizzadeh B. Facial nerve and parotid gland anatomy. Otolaryngol Clin N Am. 2016;49(2):273–84.
Gilchrist JM. Seventh cranial neuropathy. Semin Neurol. 2009;29(1):5–13.
Blumenfeld H. Neuroanatomy through clinical cases. 2nd ed. Sunderland: Sinauer Associates; 2010. ©2010; 2010.
Chu EA, Byrne PJ. Treatment considerations in facial paralysis. Facial Plast Surg. 2008;24(2):164–9.
Owusu JA, Stewart CM, Boahene K. Facial nerve paralysis. Med Clin North Am. 2018;102(6):1135–43.
Domeshek LF, Zuker RM, Borschel GH. Management of bilateral facial palsy. Otolaryngol Clin N Am. 2018;51(6):1213–26.
Schirm J, Mulkens PS. Bell’s palsy and herpes simplex virus. APMIS. 1997;105(11):815–23.
McCormick DP. Herpes simplex virus as a cause of Bell’s palsy. 1972. Rev Med Virol. 2000;10(5):285–9.
Takasu T, Furuta Y, Sato KC, Fukuda S, Inuyama Y, Nagashima K. Detection of latent herpes simplex virus DNA and RNA in human geniculate ganglia by the polymerase chain reaction. Acta Otolaryngol. 1992;112(6):1004–11.
Esaki S, Yamano K, Katsumi S, Minakata T, Murakami S. Facial nerve palsy after reactivation of herpes simplex virus type 1 in diabetic mice. Laryngoscope. 2015;125(4):E143–8.
Sweeney CJ, Gilden DH. Ramsay hunt syndrome. J Neurol Neurosurg Psychiatry. 2001;71(2):149–54.
Hunt JR. On herpetic inflammation of the geniculate ganglion: a new syndrome and its complications. J Nerv Mental Dis. 1907;34(2):73–96.
Masterson L, Vallis M, Quinlivan R, Prinsley P. Assessment and management of facial nerve palsy. BMJ. 2015;351:h3725.
Cooper L, Branagan-Harris M, Tuson R, Nduka C. Lyme disease and Bell’s palsy: an epidemiological study of diagnosis and risk in England. Br J Gen Pract. 2017;67(658):e329–e35.
Duncan CJ, Carle G, Seaton RA. Tick bite and early Lyme borreliosis. BMJ. 2012;344:e3124.
Evangelista V, Gooding MS, Pereira L. Bell’s palsy in pregnancy. Obstet Gynecol Surv. 2019;74(11):674–8.
Massey EW, Guidon AC. Peripheral neuropathies in pregnancy. Continuum (Minneap Minn). 2014;20(1 Neurology of Pregnancy):100–14.
Fukazawa T, Moriwaka F, Hamada K, Hamada T, Tashiro K. Facial palsy in multiple sclerosis. J Neurol. 1997;244(10):631–3.
Jain V, Deshmukh A, Gollomp S. Bilateral facial paralysis: case presentation and discussion of differential diagnosis. J Gen Intern Med. 2006;21(7):C7–C10.
Ciorba A, Corazzi V, Conz V, Bianchini C, Aimoni C. Facial nerve paralysis in children. World J Clin Cases. 2015;3(12):973–9.
Katusic SK, Beard CM, Wiederholt WC, Bergstralh EJ, Kurland LT. Incidence, clinical features, and prognosis in Bell’s palsy, Rochester, Minnesota, 1968–1982. Ann Neurol. 1986;20(5):622–7.
Vanopdenbosch LJ, Verhoeven K, Casselman JW. Bell’s palsy with ipsilateral numbness. J Neurol Neurosurg Psychiatry. 2005;76(7):1017–8.
Hilsinger RL Jr, Adour KK, Doty HE. Idiopathic facial paralysis, pregnancy, and the menstrual cycle. Ann Otol Rhinol Laryngol. 1975;84(4 Pt 1):433–42.
Urban E, Volk GF, Geissler K, Thielker J, Dittberner A, Klingner C, et al. Prognostic factors for the outcome of Bells’ palsy: a cohort register-based study. Clin Otolaryngol. 2020;45(5):754–61.
Wagner G, Klinge H, Sachse MM. Ramsay hunt syndrome. J Dtsch Dermatol Ges. 2012;10(4):238–44.
Sanders RD. The trigeminal (V) and facial (VII) cranial nerves: head and face sensation and movement. Psychiatry (Edgmont). 2010;7(1):13–6.
Marques AR. Laboratory diagnosis of Lyme disease: advances and challenges. Infect Dis Clin N Am. 2015;29(2):295–307.
Halperin JJ. Neurologic manifestations of lyme disease. Curr Infect Dis Rep. 2011;13(4):360–6.
Lager M, Dessau RB, Wilhelmsson P, Nyman D, Jensen GF, Matussek A, et al. Serological diagnostics of Lyme borreliosis: comparison of assays in twelve clinical laboratories in Northern Europe. Eur J Clin Microbiol Infect Dis. 2019;38(10):1933–45.
Branda JA, Linskey K, Kim YA, Steere AC, Ferraro MJ. Two-tiered antibody testing for Lyme disease with use of 2 enzyme immunoassays, a whole-cell sonicate enzyme immunoassay followed by a VlsE C6 peptide enzyme immunoassay. Clin Infect Dis. 2011;53(6):541–7.
Zandian A, Osiro S, Hudson R, Ali IM, Matusz P, Tubbs SR, et al. The neurologist’s dilemma: a comprehensive clinical review of Bell’s palsy, with emphasis on current management trends. Med Sci Monit. 2014;20:83–90.
McAllister K, Walker D, Donnan PT, Swan I. Surgical interventions for the early management of Bell’s palsy. Cochrane Database Syst Rev. 2011;(2):CD007468.
Brown JS. Bell’s palsy: a 5 year review of 174 consecutive cases: an attempted double blind study. Laryngoscope. 1982;92(12):1369–73.
Engstrom M, Abdsaleh S, Ahlstrom H, Johansson L, Stalberg E, Jonsson L. Serial gadolinium-enhanced magnetic resonance imaging and assessment of facial nerve function in Bell’s palsy. Otolaryngol Head Neck Surg. 1997;117(5):559–66.
Salinas RA, Alvarez G, Ferreira J. Corticosteroids for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2004;(4):CD001942.
de Almeida JR, Al Khabori M, Guyatt GH, Witterick IJ, Lin VY, Nedzelski JM, et al. Combined corticosteroid and antiviral treatment for Bell palsy: a systematic review and meta-analysis. JAMA. 2009;302(9):985–93.
Engstrom M, Berg T, Stjernquist-Desatnik A, Axelsson S, Pitkaranta A, Hultcrantz M, et al. Prednisolone and valaciclovir in Bell’s palsy: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet Neurol. 2008;7(11):993–1000.
Gagyor I, Madhok VB, Daly F, Sullivan F. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;9:CD001869.
Adour KK, Wingerd J, Bell DN, Manning JJ, Hurley JP. Prednisone treatment for idiopathic facial paralysis (Bell’s palsy). N Engl J Med. 1972;287(25):1268–72.
Hu LT. Lyme disease. Ann Intern Med. 2016;164(9):Itc65–itc80.
Adour KK. Decompression for Bell’s palsy: why I don’t do it. Eur Arch Otorhinolaryngol. 2002;259(1):40–7.
Gantz BJ, Rubinstein JT, Gidley P, Woodworth GG. Surgical management of Bell’s palsy. Laryngoscope. 1999;109(8):1177–88.
Bodenez C, Bernat I, Willer JC, Barre P, Lamas G, Tankere F. Facial nerve decompression for idiopathic Bell’s palsy: report of 13 cases and literature review. J Laryngol Otol. 2010;124(3):272–8.
Gilchrist JM. Facial nerve palsy. New York: Springer Nature; 2012.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Siriwardane, J. (2021). Facial Nerve Palsy. In: Roos, K.L. (eds) Emergency Neurology. Springer, Cham. https://doi.org/10.1007/978-3-030-75778-6_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-75778-6_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-75777-9
Online ISBN: 978-3-030-75778-6
eBook Packages: MedicineMedicine (R0)