
Abstract
Traditionally, standard practice has been to delineate the target volumes for radiotherapy planning on a CT dataset, sometimes after fusion with other modalities such as magnetic resonance imaging, but recently PET/CT has been used as the functional imaging tool such that planning volumes are based on the metabolic uptake. Hence, PET may be used to modify the GTV and has the potential to identify hypermetabolic regions that may be smaller than the morphological appearance of the tumour. In addition, the size of the clinical target volume (CTV) may be modified by the inclusion or absence of PET avid lymph nodes. In this chapter, we briefly describe PET based radiotherapy planning.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


The role of radiotherapy is to deliver a prescribed radiation dose to a target volume whilst minimising the dose to surrounding organs at risk (OAR). The tumour control probability (TCP) increases with absorbed dose until certain local control is achieved. However, the escalation of absorbed dose is generally limited by normal-tissue-complication probability (NTCP).
Advanced radiotherapy techniques such as intensity modulated radiation therapy (IMRT) and proton/ion therapy offer a high degree of conformity to a target volume, with much less normal tissue receiving a high dose for a given target dose. These may allow dose escalation to the target for the same NTCP as conventional radiotherapy, thus providing the potential for better disease control.
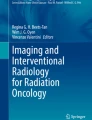
The most important component of radiation therapy treatment planning is the delineation of the gross tumour volume (GTV), Fig. 3.1. The GTV is the macroscopically demonstrable extent and location of the tumour. The clinical target volume (CTV) is extended from the GTV to include subclinical malignant disease with a certain probability of occurrence considered relevant for therapy. The planning target volume (PTV) is a larger volume that takes account of geometrical uncertainties such as organ motion and setup variations.

Target volumes used in radiotherapy treatment planning. GTV gross tumour volume, CTV clinical target volume, PTV planning target volume
Traditionally, standard practice has been to delineate the target volumes on a CT dataset, sometimes after fusion with other modalities such as magnetic resonance imaging, but recently PET/CT has been used as the functional imaging tool such that planning volumes are based on the metabolic uptake. Hence, PET may be used to modify the GTV and has the potential to identify hypermetabolic regions that may be smaller than the morphological appearance of the tumour. In addition, the size of the clinical target volume (CTV) may be modified by the inclusion or absence of PET avid lymph nodes.
The most commonly used radiopharmaceutical is 2-[18F] fluoro-2-d-deoxyglucose (18F-FDG). Other radiopharmaceuticals to assess various molecular pathways in tumour biology are summarised in Table 3.1.
A major advantage of PET imaging is the quantitative assessment of tumour uptake by standardised uptake value (SUV). This is defined as the uptake of a radiopharmaceutical, normalised to the injected dose and body weight. It is commonly used for prognosis, response monitoring and definition of treatment volumes. There are a number of biological and technical factors that influence the measure of SUV, and guidelines to minimise the error have been published [1, 2].
The widespread availability of large-bore integrated PET/CT systems, together with fixed radiation therapy positioning laser systems has enabled radiotherapy planning of metabolic target volumes to be realised. A single-scan approach can be used that enables the radiotherapy plan to be generated on the PET and/or CT dataset.
With the advent of wide bores, a flat therapy couch top with a carbon fibre overlay can be securely fitted to the PET/CT couch to achieve the same geometry as the radiotherapy couch top (Fig. 3.2). The rigidity of the couch top should ensure minimal sag in the extended PET position. Immobilisation devices can be attached to the couch top consistent with the table tops in the treatment unit. The dedicated radiotherapy laser system is generally positioned in front of the PET/CT gantry and provides a coordinate system in three axes such that appropriate marks can be placed on the patient’s skin or immobilisation device to reproduce the position in the treatment room.

PET/CT with radiotherapy planning setup. The laser light system is mounted in front of the gantry. A flat-top couch is attached to the bed, with immobilisation device for consistency with the treatment unit
Appropriate QA, generally performed by the radiotherapy physics team needs to be performed to ensure consistency with the treatment room lasers.
Because of the inherent resolution limitation and partial volume effect in PET systems, accurate delineation of the gross tumour volume (GTV) is a major consideration in the application of PET/CT for radiotherapy planning [3,4,5]. Delineation errors may result in sub-optimal loco-regional disease control because of inadequate coverage or to increased toxicity of the treatment because of excessive coverage of normal tissues.
Manual delineation of PET images is the easiest method, but is very operator-dependent, particularly since altering the window levels can vary the perception of tumour volume, despite using the CT images as anatomic boundaries.
More accurate methods utilise automatic or semi-automatic segmentation methods that reduce the GTV significantly and reduce interobserver variability. A thresholding method is easy to implement with all voxels having an intensity higher than threshold (SUV = 2.5) considered as target [6]. Alternatively, for regions of reduced signal-to-noise, a percentage threshold may be used, with a commonly used value of 40% of the maximum value in the target region [7].
Gradient based auto-contouring methods utilise image processing techniques such as edge enhancement using partial volume correction methods. Gradient based segmentation is then performed by evaluating the image gradient of a line profile across a tumour region of the PET image.
Respiratory motion is another technical challenge for lesions located in the thorax and upper abdomen. As breath-hold techniques are not achievable in long acquisition time PET protocols, respiratory motion may manifest in a visual appearance of smearing of the activity distribution in the tumour, with a loss of contrast and overestimation of the lesion volume.
There are several respiratory monitoring systems available for gating purposes based on different physical properties [8].
-
1.
Pressure sensitive belt.
-
2.
Spirometry system.
-
3.
Strain-gauge belt.
-
4.
Temperature sensor.
-
5.
Opto-electronic system.
These techniques work by synchronising the PET and CT acquisitions to the patient’s respiratory cycle, with the result that well-registered PET and CT images are produced corresponding to specific phases of the breathing cycle. This has the effect of potentially reducing the PTV, with increased effectiveness of radiotherapy treatment and less side-effects.
-
The role of radiotherapy is to deliver a prescribed radiation dose to a target volume whilst minimising the dose to surrounding organs at risk (OAR).
-
The most important component of radiation therapy treatment planning is the delineation of the gross tumour volume (GTV).
-
The GTV is the macroscopically demonstrable extent and location of the tumour.
-
The clinical target volume (CTV) is extended from the GTV to include subclinical malignant disease with a certain probability of occurrence considered relevant for therapy.
-
The planning target volume (PTV) is a larger volume that takes account of geometrical uncertainties such as organ motion and setup variations.
-
Delineation errors may result in sub-optimal loco-regional disease control because of inadequate coverage.
-
Manual delineation of PET images is the easiest method, but is very operator-dependent.
-
More accurate methods utilise automatic or semi-automatic segmentation methods that reduce the GTV significantly and reduce interobserver variability.
References
Boellaard R, et al. EANM procedure guidelines for tumour PET imaging: version 1.0. Eur J Nucl Med Mol Imaging. 2010;37:181–200.
Sattler B, et al. PET/CT (and CT) instrumentation, image reconstruction and data transfer for radiotherapy planning. Radiother Oncol. 2010;96:288–97.
Caldwell CB, et al. Observer variation in contouring gross tumor volume in patients with poorly defined non-small-cell lung tumors on CT: the impact of 18FDG-hybrid PET fusion. Int J Radiat Oncol Biol Phys. 2001;51(4):923–31.
Schinagl DA, Vogel WV, Hoffmann AL, van Dalen JA, Oyen WJ, Kaanders JH. Comparison of five segmentation tools for 18F-fluorodeoxy-glucose-positron emission tomography-based target volume definition in head and neck cancer. Int J Radiat Oncol Biol Phys. 2007;69:1282–9.
Zaidi H, Naqa IE. PET-guided delineation of radiation therapy treatment volumes: a survey of image segmentation techniques. Eur J Nucl Med Mol Imaging. 2010;37:2165–87.
Nestle U, Kremp S, Schaefer-Schuler A, et al. Comparison of different methods for the delineation of 18F-FDG PET-positive tissue for target volume definition in radiotherapy of patients with non-small cell lung cancer. J Nucl Med. 2005;46:1342–8.
Biehl KJ, Kong F-M, Dehdashti F, et al. 18F-FDG PET definition of gross tumor volume for radiotherapy of non-small cell lung cancer: is a single standardized uptake value threshold approach appropriate? J Nucl Med. 2006;47:1808–12.
Nehmeh SA, Erdi YE. Respiratory motion in positron emission tomography/computed tomography: a review. Semin Nucl Med. 2008;38:167–76.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2022 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Aldridge, M. (2022). The Physics of PET/CT for Radiotherapy Planning. In: Agrawal, K., Skillen, A., Esmail, A., Usmani, S. (eds) PET/CT Imaging. Clinicians’ Guides to Radionuclide Hybrid Imaging(). Springer, Cham. https://doi.org/10.1007/978-3-030-75476-1_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-75476-1_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-75475-4
Online ISBN: 978-3-030-75476-1
eBook Packages: MedicineMedicine (R0)