
Abstract
Breast cancer is the most commonly diagnosed cancer worldwide and the leading cause of cancer-related death in women. Approximately 10% of cases are hereditary, caused by mutations in genes responsible for cell growth and survival and DNA maintenance. Hereditary cancer predisposition is characterized by earlier age at onset, clustering in families, and association with various tumor types. Identifying patients with a genetic predisposition to cancer is important for the patient and their relatives, both affected and unaffected. Knowing the risk of developing cancer can help in clinical management both in terms of prevention and treatment. A number of genes have been identified which when mutated increase a carrier’s risk of developing breast and other cancers. Next-generation sequencing (NGS) allows for simultaneous analysis of all genes implicated in hereditary predisposition to breast cancer. In most cases, enough research has allowed the compilation of clinical management guidelines by large international working groups in order to individualize preventive and therapeutic management of at-risk individuals.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Cancer is a genetic disease. All tumors are the result of the accumulation of mutations and the subsequent deregulation of important genes involved in pathways which regulate cell growth, cell survival, and DNA maintenance [1]. Such mutations can arise in a given cell, in which case they are called somatic, or be inherited from a parent (germline), in which case they are present in all the cells of the body and the individual has an increased risk for developing cancer often at a younger age. In a small subset of patients, the mutation can be found to be de novo, in which case it has occurred for the first time in the individual, either in a parental germ cell (oocyte or sperm) or in early embryogenesis. In either case, the mutation is present in the majority, or all, of the cells of the individual and confers the same risk for cancer as an inherited mutation but in the absence of a family history.
Approximately 140 genes in the human genome have been identified in the pathways which control cell growth and stability, but only a subset of these have until now been implicated in hereditary cancer syndromes.
Hereditary cancer syndromes are caused by mutations in genes predisposing to high probability of developing specific cancers (Table 3.1) and are characterized by vertical transmission through a parent or association with other types of tumors in the individual or their family and often by an earlier age of diagnosis than that of the general population for the same type of tumor. They are generally inherited in a dominant manner, that is, they occur when one copy of the gene is mutated [2].
Familial cancers usually differ from hereditary forms in their inheritance patterns or age at onset. Familial cancers may be attributed to a combination of factors such as chance clustering of sporadic cancer cases in the family, genetic variation in low-penetrance genes, or a shared environment [3].
1.1 Genetic Risk Assessment
Historically, making a diagnosis of a hereditary cancer syndrome has relied on the clinician collecting a detailed personal and family history of the individual and recognizing the clinical hallmarks of a hereditary cancer syndrome [4]. Factors such as the number of affected relatives in the family, the closeness of the relationship to the individual, and the age at onset of cancer increase the likelihood of a hereditary predisposition to cancer in the family [5].
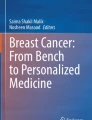
The construction of a detailed pedigree is the first step of this process, beginning with the health of the proband (index case) and proceeding outward to include first-, second- and, if possible, third- degree relatives on both sides of the family. All members of the family, affected and unaffected, are important, including their current age, or age at death. The information needed for all affected family members includes cancer diagnosis by primary site, age at diagnosis, bilaterality (when appropriate), and current age, or age at death. Other medical conditions that may be associated or predispose to cancer risk of the individual should also be recorded (Fig. 3.1).

Example of a pedigree with suspected hereditary predisposition to breast cancer. Arrow indicates proband, circles indicate females, squares indicate males, filled black symbols indicate affected individuals, diagonal line across a symbol indicates deceased individual. CaBr = breast cancer, y.o. = years old, d. = died (number indicates age at diagnosis, current age, or age at death)
However, variability in clinical phenotype and penetrance, as well as other environmental and lifestyle differences between individuals in the same family, can make it difficult to identify at-risk individuals, and the classic criteria originally used to define many of the hereditary cancer syndromes have limited sensitivity and specificity for detecting germline mutation carriers.
Factors that may limit the informativeness of the pedigree are [3, 6]:
-
Incomplete family history assessment.
-
Unavailable medical records.
-
Small family size.
-
Small number of individuals of the susceptible gender in sex-limited cancers.
-
Reduced penetrance.
-
Early death of key individuals in the family, from causes other than cancer, before the average age of onset of the phenotype.
-
Prophylactic surgeries that remove the organ at risk.
-
False paternity or adoption.
-
Inaccurate or incomplete information on family members.
-
Failure to investigate all types of cancer in the family.
Genetic testing for hereditary cancer predisposition should according to the American Society of Clinical Oncology (ASCO) be undertaken when [7]:
-
(a)
There is a personal or family history suggestive of genetic predisposition to cancer.
-
(b)
The test can be adequately interpreted.
-
(c)
Results will aid in the diagnosis or influence medical or surgical management of the patient or at-risk family members.
If the individual meets criteria for genetic testing, appropriate pre-test genetic counseling should be undertaken. Members of a number of specialties, including a genetic counsellor, medical geneticist, oncologist, surgeon, or oncology nurse, should be involved in the process in order to explain all aspects of the expected results and limitations of the test procedure, in addition to the possible implications both to the individual and their family [8]. A clear explanation of positive, negative, or inconclusive results should be made to the individuals. Furthermore, the distinction between the probability of being a mutation carrier and that of developing cancer should be made clear. Post-test counseling is also necessary in order to discuss the significance of the results, their impact on medical management, and the importance of sharing the results with family members who may also be at risk.
In families for whom genetic testing has not yet been performed, it is best to test an affected individual, if available, especially a family member with early onset of the disease, bilateral disease, or multiple primary cancers, as that individual has the highest risk of carrying a pathogenic mutation. Comprehensive analysis of the entire gene(s) should be carried out, including methods capable of detecting all types of mutations [9]. Possible mutations can be single base changes and small insertions/deletions, detected by sequencing [10,11,12], or large genomic rearrangements (insertions/deletions ranging in size from single exons to entire genes), detected by semi-quantitative methods such MLPA or qsmfPCR [13, 14] or more recently comparative genomic hybridization arrays (Fig. 3.2).

Types of DNA mutation and method of detection
Hereditary breast cancer is estimated to account for approximately 10% of all breast cancer cases [15, 16], while an additional 15–20% have a positive family history (one or more affected first and/or second-degree relatives). Identifying those cases with a hereditary basis of breast cancer is important as it provides the physician with improved management tools both in prevention and treatment of the disease not only for the patient but also for at-risk relatives.
Hereditary cancer predisposition genes can be categorized according to the relative risk for cancer that they confer. A relative cancer risk of 5 or higher is conferred by “high-penetrance genes,” 1.5 or lower by “low-penetrance genes,” and 1.5–5 by “intermediate-penetrance genes.”
2 Hereditary Breast and Ovarian Cancer Syndrome (HBOC)
Specific patterns of hereditary breast cancer, usually associated with ovarian cancer, are linked to mutations in the BRCA1 and BRCA2 genes [17, 18], which are the genes involved in HBOC.
BRCA1 and BRCA2 were first identified in 1994 [19] and 1995 [20], respectively, through linkage studies of multiple breast cancer families. These genes encode proteins involved in the Fanconi anemia pathway with crucial roles in DNA double-strand break repair [18, 21]. The carrier frequency of mutations in BRCA1 and BRCA2 is approximately 1 in 300 and 1 in 800 [22], respectively. However, this varies markedly between different ethnicities, due to the presence of founder mutations.
2.1 BRCA1
BRCA1 is located on chromosome 17 and encodes for a nuclear phosphoprotein, with key roles in DNA repair and regulation of cell cycle checkpoints in response to DNA damage. It combines with other tumor suppressor proteins, DNA damage sensors, and signal transducers, to form a complex associated with genome surveillance [23].
Female carriers of pathogenic mutations in BRCA1 have 44–78% breast cancer risk and ovarian cancer risk of 18–54% [24]. The risk for contralateral breast cancer by the age of 70 is up to 30% [25]. Male BRCA1 mutation carriers have 1.2% risk of developing breast cancer compared to 0.1% in the general male population. Cancers arising in BRCA1 mutation carriers are generally characterized by the absence of expression of human epidermal growth factor 2 (HER2), estrogen (ER), and progesterone receptors (PR), a phenotype commonly referred to as “triple negative” [26]. Indeed, studies have reported BRCA1 mutations in 7–28% of patients with triple-negative breast cancer. Furthermore, among patients with triple-negative breast cancer, BRCA1 mutation carriers were diagnosed at a younger age than non-carriers.
It has long been considered that biallelic mutations of BRCA1 are embryonic lethal. However, a recent report of one individual has shown that this is not the case [27].
2.2 BRCA2
The BRCA2 gene is located on chromosome 13. The protein product is involved in genomic stability maintenance through the homologous recombination (HR) pathway [18, 21].
Female carriers of BRCA2 mutations have up to 45% lifetime risk of developing breast cancer and up to 12% risk of ovarian cancer [24]. The risk for contralateral breast cancer by the age of 70 is up to 30% [25]. In addition, there is an increased risk for the development of pancreatic cancer (3%) and melanoma. Male carriers of BRCA2 mutations have a 7–8% risk of developing breast cancer and 20% risk for prostate cancer.
The pathological characteristics of BRCA2-related tumors are usually the same as those of sporadic breast carcinomas [21].
Individuals with biallelic pathogenic BRCA2 mutations have Fanconi anemia, a severe condition characterized by congenital anomalies, bone marrow failure, short stature, and increased risk for hematological and solid malignancies [28, 29].
2.3 Screening and Management
Based on the above observations regarding carriers of BRCA1 and BRCA2 mutations, various international collaborative groups, such as the National Comprehensive Cancer Network (NCCN), have put forward sets of criteria to help select those individuals/families who should be tested for mutations in these two highly penetrant genes.
Any individual with a personal history of breast cancer in addition to one or more of the following [9]:
-
Diagnosed at age 45 years or younger.
-
Diagnosed with at least two cancer primaries (i.e., bilateral tumors or two or more clearly separate ipsilateral tumors, occurring synchronously or asynchronously), the first at age 50 years or younger.
-
Diagnosed at age 50 years or younger with one or more close relatives with breast cancer at any age (or with unknown or limited family history), 1 or more close relatives with pancreatic cancer, or 1 or more close relatives with prostate cancer (Gleason score ≥ 7).
-
Diagnosed with triple-negative breast cancer at age 60 years or younger.
-
Diagnosed at any age with 1 or more close relatives with breast cancer diagnosed at age 50 years or younger.
-
Diagnosed at any age with 2 or more close relatives with breast cancer at any age.
-
Diagnosed at any age with 1 or more close relatives with invasive ovarian cancer (including fallopian tube and primary peritoneal cancers) diagnosed at any age.
-
Diagnosed at any age with two or more close relatives with pancreatic cancer and/or prostate cancer (Gleason score ≥ 7) at any age.
-
Having a close male relative with breast cancer at any age.
Since their discovery, BRCA1 and BRCA2 have been the best studied paradigms of the power of personalized genomics by highlighting how the information from genetic testing can be used in specific interventions to reduce morbidity and mortality. In this aspect, various collaborative groups have put forward general clinical management guidelines which include [9]:
-
Annual surveillance with breast MRI and mammograms starting at 25 years of age or younger based on family history.
-
Chemoprevention with agents such as tamoxifen.
-
Risk reducing bilateral salpingo-oophorectomy between 35 and 40 years of age.
-
Recommendation of risk-reducing bilateral mastectomy (RRM).
-
For male carriers, annual clinical breast examination starting at 35 years of age and prostate cancer screening starting at age 45 years.
Extensive studies on the function of the BRCA1 and BRCA2 proteins, and their role in DNA repair and stability, in addition to analyses as to how mutations in these proteins can disrupt these functions, have allowed for the development of novel therapeutic agents, such as inhibitors of the poly-ADP ribose polymerase (PARP inhibitors) which effectively target BRCA-deficient cells. Such agents are already approved and being used for the treatment of BRCA-deficient ovarian tumors and are being clinically tested for their efficacy in the treatment of BRCA- deficient breast carcinomas, thus adding new value to the clinical utility of BRCA1/2 genetic testing [30].
3 The New Era of Next-Generation Sequencing (NGS) and Gene Panels
Despite the fact that BRCA1 and BRCA2 are the two most significant genes in hereditary breast cancer predisposition, 20 years of analysis has highlighted the fact that mutations in these two highly penetrant genes are only present in approximately 20% of high-risk families [31].
Other genes, identified because of the strong association with familial cancer syndromes, in which breast cancer is one of the defining components, include TP53 (Li-Fraumeni syndrome), PTEN (Cowden Syndrome), STK11 (Peutz-Jeghers syndrome), CDH1 (hereditary diffuse gastric cancer syndrome—HDGC), and neurofibromatosis type 1 (NF1).
3.1 Li-Fraumeni Syndrome (LFS)
LFS is a rare hereditary cancer predisposition syndrome caused mainly by mutations in the TP53 gene [32], located on chromosome 17. The nuclear protein encoded by TP53 binds directly to DNA. It has been called “the guardian of the genome” and has an important role in controlling cell cycle and apoptosis [33].
LFS has been estimated to be responsible for only 1% of hereditary breast cancer cases [34]. However, the risk for breast cancer before the age of 45 is 18- to 60-fold greater in female carriers of TP53 pathogenic mutations, with a median age at diagnosis of breast cancer at 33 years. Breast tumors in individuals with LFS are usually HER2 positive and often also estrogen and progesterone receptor positive [35].
LFS is a highly penetrant hereditary cancer predisposition syndrome associated with a high lifetime risk of a wide spectrum of cancers, including soft tissue sarcomas, osteosarcomas, premenopausal breast cancer, acute leukemia, colon cancer, adrenocortical carcinoma, and brain tumors. These tumors usually present as early as childhood, and carriers of TP53 mutations have an increased risk of developing multiple primary cancers in their lifetime. Sarcoma, breast cancer, adrenocortical tumors, lung bronchoalveolar cancer, leukemia, and certain brain tumors have been referred to as the “core” cancers of LFS [36], as they account for the majority of cancers observed in carriers of TP53 germline pathogenic variants. A number of different sets of criteria for the selection of patients who warrant germline screening have been put forward and generally include the following points [9]:
-
A proband with a tumor belonging to the LFS spectrum before the age of 46 years and at least one first- or second-degree relative with a LFS tumor (except breast cancer if the proband has breast cancer) before the age of 56 years or with multiple tumors at any age.
-
A proband with multiple tumors (except multiple breast tumors), two of which belong to the LFS tumor spectrum and the first of which occurred before the age of 46 years.
-
Proband with adrenocortical carcinoma or choroid plexus tumor, regardless of family history.
-
A woman with a personal history of early-onset breast cancer (age at diagnosis ≤31 years), with or without family history of core tumor types.
Approximately 7–20% of LFS cases result from de novo mutations in TP53. As a result, strict adherence to these guidelines, which are mostly based on family history, may result in LFS cases being missed [36].
Based on the high cancer risk associated with LFS, specific surveillance and management guidelines have been proposed. In this aspect, surveillance includes annual comprehensive physical examination starting in childhood and enhanced colorectal and breast cancer surveillance beginning at 20–25 years (based on family history). Based on the wide spectrum of tumors associated with LFS, screening through total-body MRI may be warranted for these individuals in addition to annual dermatologic examination starting at age 18 years [9].
As far as clinical management is concerned, for women with breast cancer diagnosis, mastectomy is recommended instead of lumpectomy due to the high risk of developing a second tumor in the radiation field. Discussion about preventive bilateral mastectomy is also recommended for female TP53 mutation carriers [9].
3.2 Cowden Syndrome (CS)
CS is part of a spectrum of disorders known as PTEN hamartoma tumor syndrome (PHTS) [37]. PHTS is caused by mutations in the PTEN tumor suppressor gene, located on chromosome 10. The PTEN protein is a tyrosine phosphatase with a role in cell cycle arrest, apoptosis, and genomic stability [38]. The incidence of CS has been reported to be 1 in 200,000 although this may be an underestimate [39].
Carriers of PTEN germline mutations usually present with benign characteristics of the disease by their late 20s, including oral papillomas, facial trichilemmomas, macrocephaly, uterine fibroids, and fibrocystic breast. In addition, carriers of pathogenic PTEN mutations are at increased risk of a number of different cancers, including breast (lifetime risk of 77–85%), thyroid (3–10%), endometrial (5–10%), colorectal cancer (9–16%), renal cancers (15%), and melanoma. Two male cases with CS who developed breast cancer have also been reported [40, 41].
Based on the high cumulative lifetime risk of 85% for the development of any cancer [40], guidelines on the clinical management and surveillance of PTEN mutation carriers have been formulated and include breast imaging beginning at age 30–35 years (or younger based on family history), endometrial cancer surveillance, thyroid and renal ultrasound, and colonoscopy starting at age 35 years. In addition, RRM and hysterectomy are recommended for female PTEN mutation carriers [9].
3.3 Peutz-Jegher’s Syndrome (PJS)
PJS is caused by inherited mutations in the STK11 gene, also known as LKB1, on chromosome 19. The serine/threonine kinase protein encoded regulates cell polarity and functions as a tumor suppressor. Mutations in this gene are found in 50–70% of individuals affected by PJS, although in approximately half of the cases, these mutations are de novo [42].
PJS is characterized by multiple hamartomatous polyps of the gastrointestinal (GI) tract, mucocutaneous pigmentation, and increased risk of multiple cancer types, including gastrointestinal, breast, and non-epithelial ovarian cancer. Symptoms often present in childhood or early adolescence. The risk of breast cancer in women with PJS ranges from 8% at age 40–45% at age 70 [43].
Clinical surveillance guidelines for STK11 mutation carriers include mammograms and MRI beginning at age 25 and colonoscopies and upper GI endoscopies beginning in late teens [9].
3.4 Hereditary Diffuse Gastric Cancer (HDGC)
HDGC is caused by inherited mutations in the CDH1 gene, located on chromosome 16 and encoding for E-cadherin, a protein responsible for calcium-dependent epithelial cell adhesion [44]. In addition to gastric cancer, female carriers of pathogenic mutations in CDH1 are at increased risk of lobular breast cancer. The lifetime risk of gastric cancer is 67% for men and 83% for women, with an average age at diagnosis at 37 years. The risk of breast cancer in female mutation carriers is 39–52%. Furthermore, lobular breast cancer may arise in the absence of diffuse gastric cancer in the family [45].
Preventive management guidelines for carriers of germline CDH1 mutations include endoscopic surveillance for high-risk gastric cancer, with preventive gastrectomy between the ages of 18 and 40 being preferable. As far as breast cancer is concerned, enhanced breast surveillance by mammogram and MRI is recommended beginning at 30 years (or earlier, based on family history). In addition, RRM should be offered to female carriers of germline CDH1 mutations [9].
3.5 Neurofibromatosis Type 1 (NF1)
NF1 is caused by inherited mutations in the NF1 gene, which is located on chromosome 17. The Neurofibromin 1 protein acts as a tumor suppressor regulating the function of the ras protein and therefore preventing cell overgrowth.
Patients with NF1 are at increased risk of developing malignant peripheral nerve sheath tumors, as well as other central nervous system (CNS) and gastrointestinal tumors. The estimated lifetime risk of cancer in NF1 patients is almost 60% [46]. Several studies have indicated that female carriers of NF1 mutations also have up to 8.4% risk of developing breast cancer until the age of 50. However, the same studies have shown that the risk after the age of 50 is not significantly elevated compared to that of the general population [47].
Based on these risk estimates, clinical surveillance guidelines for NF1 mutation carriers include annual screening with mammography and MRI starting at age 30, but MRI screening should be discontinued after the age of 50 [9].
4 Other Genes
In addition to these high-penetrance genes, technological advances in DNA sequencing, commonly designated as “next-generation sequencing (NGS),” have aided in the concentrated efforts to identify new genes responsible for the missing heritability. These efforts have relied on the analysis of likely candidate genes, based on prior knowledge of functional association, their involvement in the same cellular pathways as the high-penetrance proteins, and the phenotypic evidence in carriers of autosomal recessive syndromes.
4.1 Partner and Localizer of BRCA2 (PALB2)
The PALB2 protein was first identified as a nuclear partner of BRCA2 and was later shown to bind directly and collaborate with BRCA2 in double-strand-break repair [48]. Biallelic mutations of PALB2, located on chromosome 16, were initially identified in the more severe form of the hereditary syndrome Fanconi anemia type D1 (FANCD1) who lacked mutations in BRCA2 [48]. Analysis of large numbers of breast cancer patients subsequently revealed the frequency of PALB2 mutations to be between 1.1% and 3.4%, while this frequency in men with breast cancer was found to range between 1% and 2% of men testing negative for a BRCA2 pathogenic mutation.
The risk for breast cancer in female carriers of a PALB2 pathogenic mutations increased with age reaching 35% by age 70. Furthermore, the risk was shown to increase with the increasing number of affected relatives, reaching as high as 58% by age 70 in families with two first-degree relatives. In addition to breast cancer, PALB2 mutations have been associated with an increased risk for pancreatic cancer as well as melanoma, while the risk for ovarian and prostate cancer is not yet established [49].
The discovery of the involvement of PALB2 in hereditary breast cancer is relatively recent. As a result, data is still limited. Therefore, clinical management guidelines for carriers of PALB2 pathogenic mutations are at the time being based only on the increased breast cancer risk conferred and indicate the need for enhanced breast screening by MRI beginning at the age of 30 years. In addition, RRM should be offered to female carriers of germline PALB2 mutations [9].
4.2 Checkpoint Kinase 2 (CHEK2)
CHEK2 is a tumor suppressor gene, located on chromosome 22, which encodes for a serine/threonine kinase protein, which is activated by the ATM protein in response to double-stranded DNA breaks.
Mutations in CHEK2 are more prevalent in Northern and Eastern Europe. The lifetime risk for breast cancer in female carriers of CHEK2 pathogenic variants is dependent upon family history ranging from 28% to 44% in individuals with a strong family history. In addition, women are at increased risk of developing a second breast cancer. Furthermore, association of CHEK2 pathogenic variants and risk of colorectal and other cancers has been suggested.
Individuals homozygous for CHEK2 mutations have been shown to have a sixfold increased risk of breast cancer compared to the general population. In addition, such individuals are at an increased risk of developing a second breast cancer and may therefore warrant more intensive breast cancer surveillance than heterozygote mutation carriers [50].
Management of CHEK2 mutation carriers is largely guided by family history, but is primarily based on increased screening. Women with CHEK2 mutations are more likely to develop estrogen receptor-positive breast cancer and may, therefore, benefit from tamoxifen chemoprevention and screening with mammogram and MRI starting at age 40 [9, 50].
4.3 Ataxia Telangiectasia Mutated (ATM)
The ATM gene, located on chromosome 11, encodes for a protein kinase which functions in cellular signaling in response to DNA damage and acts with the MRN protein complex. Biallelic mutations in ATM were first identified in the ataxia-telangiectasia (AT) syndrome, an autosomal recessive disorder with childhood-onset progressive neurodegeneration, telangiectasia, immunodeficiency, gonadal atrophy, and predisposition to malignancy. The carrier frequency of ATM mutations in the general population is about 0.5–1% [50].
Women with a single pathogenic mutation in ATM were shown to have 38–69% risk of developing breast cancer by the age of 70. Other cancers associated with ATM mutations include pancreatic and prostate cancer [9].
The increased risk of breast cancer in carriers of ATM mutations has prompted recommendation for increased surveillance by mamogram and MRI starting at age 40 and the option of risk-reducing bilateral mastectomy based on family history [9].
4.4 MRN Complex
This complex is made up of the proteins MRE11A-RAD50-NBN and has a crucial role in the detection and early processing of double-strand breaks, maintaining in this way DNA integrity. This is achieved by interaction with the ATM, BRCA1, and CHEK2 proteins. Based on the complex’s crucial role in maintaining DNA stability through interaction with well-established breast cancer predisposition proteins, various sequencing studies sought out to investigate the role of these proteins in breast cancer susceptibility. Potentially pathogenic mutations have been identified in the NBN gene, while the contribution of mutations in RAD50 and MRE11A is still in dispute [9, 50]. Mutations in the MRN complex genes, although very rare, can be population specific.
4.4.1 Nibrin (NBN)
The NBN gene (also known as NBS1), located on chromosome 8, encodes for the protein Nibrin.
Homozygous or compound heterozygous mutations in NBN are responsible for the autosomal recessive Nijmegen breakage syndrome (NBS), characterized by childhood-onset microcephaly, short stature, immunodeficiency, and high risk of cancer, especially lymphoid malignancy [50].
Heterozygous carriers of pathogenic NBN mutations have been shown to have a moderately increased risk for breast and possibly ovarian cancer. The overall risk of breast cancer in females with a NBN pathogenic mutation is 3.1, and limited evidence suggests that the risk of prostate cancer in male carriers is also elevated.
Mutations predisposing to NBN-associated breast cancer are most prevalent in Eastern European populations. Most pathogenic variants described until today are frameshift or truncating mutations, while missense mutations have only been described in childhood acute lymphoblastic leukemia (ALL).
Again, recommendations for enhanced breast cancer screening by annual mammogram and MRI after the age of 40 have been proposed for female carriers of pathogenic mutations [9].
5 Multi-Gene Testing
Gene panels or “multi-gene testing” as it is more commonly referred to is increasingly favored as first-choice testing. This approach allows for the simultaneous screening of multiple risk loci associated with a specific family cancer phenotype or multiple phenotypes at no or little added cost.
Multiple studies have shown the added value of multi-gene testing as in the majority only about half the pathogenic variants identified in high-risk patients were located in BRCA1 and BRCA2 [51].
Currently, a concern in the use of multi-gene testing is that there is only limited data for some of the genes included in most panels [52]. This is translated to uncertainty regarding the degree of cancer risk associated with these genes and in turn to luck of clear clinical management guidelines. Another drawback of testing genes for which data is limited is the high rate of “variants of uncertain significance” (VUS) identified. A number of studies have shown that the rate of VUS detection may be as high as 40%. When such a variant is detected, it adds complexity in counselling the patients and uncertainty as to their clinical management [9].
Despite these concerns, knowing if a pathogenic variant is present is still advantageous, since it allows for the identification of at-risk relatives, who may then pursue more active cancer evaluation and surveillance. Furthermore, with the rapid adoption of multi-gene testing of at-risk individuals, data is rapidly accumulating enabling the continuous formulation of clinical management guidelines for more genes. An example of this rapid growth of “knowledge” is seen in the fact that international working groups, such as NCCN, are updating their guidelines 3–4 times per year in order to include the new evidence becoming available [9].
6 Male Breast Cancer (MBC)
Although rare, breast cancer can be diagnosed in men as well. MBC makes up <1% of all breast cancer cases and < 1% of all cancers in men in the Western world. Risk factors, such as genetic, hormonal, and environmental factors, are involved in the pathogenesis of both female and male breast cancer, but the major predisposing factor of MBC is a positive family history. A positive first-degree family history can increase a man’s risk twofold, and this risk may reach up to fivefold as the number of relatives increases, especially early onset [53].
Epidemiologically, MBC resembles more closely postmenopausal female breast cancer, and therefore treatment follows the same indications as postmenopausal female breast cancer.
As in female breast cancer, mutations in a number of genes, with high, moderate, and low penetrance, have been implicated.
From the high-penetrance genes, mutations in BRCA2 are much more common than those in BRCA1, with an estimated 60–76% MBCs being attributed to mutations in BRCA2 and only from 10 to 16% to BRCA1 mutations [53]. Overall, mutations in BRCA1 and BRCA2 are more commonly found in men with a positive first-degree family history. Furthermore, it seems that large genomic rearrangements in BRCA2 are more frequent in families with MBC, although this association has not been explained biologically [53].
Analysis of moderate-penetrance genes, known to be associated with female breast cancer, in men with breast cancer has revealed a number of associations. One of the best studied moderate-penetrance genes is CHEK2, especially the mutation c.1100delC (p.Thr367Metfs). This mutation has been shown to confer as much as tenfold increase of MBC in men lacking a BRCA1/BRCA2 mutation and has been estimated to be responsible for up to 9% of all MBC cases. Once again, this association is more evident in men with a positive family history [53].
Another moderate-penetrance gene found to be associated with male breast cancer is PALB2. Mutations in PALB2 have been found in families with both male and female breast cancer, and PALB2 female carriers were shown to be 4 times more likely to have a male relative with breast cancer [53].
References
Vogelstein B, Kinzler KW. The multistep nature of cancer. Trends Genet. 1993;9:138–41.
Pharoah PD, Day NE, Duffy S, Easton DF, Ponder BA. Family history and the risk of breast cancer: a systematic review and meta-analysis. Int J Cancer. 1997;71:800–9.
Berliner JL, Fay AM, Practice Issues Subcommittee of the National Society of Genetic Counselors' Familial Cancer Risk Counseling Special Interest Group. Risk assessment and genetic counseling for hereditary breast and ovarian cancer: recommendations of the National Society of genetic Counselors. J Genet Couns. 2007;16:241–60.
Murff HJ, Spigel DR, Syngal S. 2004 does this patient have a family history of cancer? An evidence-based analysis of the accuracy of family cancer history. JAMA. 2004;292:1480–9.
Slattery ML, Kerber RA. A comprehensive evaluation of family history and breast cancer risk. The Utah Population Database. JAMA. 1993;270:1563–8.
Calzone KA, Soballe PW. Genetic testing for cancer susceptibility. Surg Clin North Am. 2008;88:705–21.
Robson ME, Storm CD, Weitzel J, Wollins DS, Offit K, American Society of Clinical Oncology. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2010;28:893–901.
Lancaster JM, Powell CB, Chen LM, Richardson DL, SGO Clinical Practice Committee. Society of Gynecologic Oncology statement on risk assessment for inherited gynecologic cancer predispositions. Gynecol Oncol. 2015;136:3–7.
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Genetic/familial high-risk assessment: breast and ovarian. Version 3.2019. https://www.nccn.org/. Accessed 18 January 2019.
Gross E, Arnold N, Goette J, Schwarz-Boeger U, Kiechle M. A comparison of BRCA1 mutation analysis by direct sequencing, SSCP and DHPLC. Hum Genet. 1999;105:72–8.
Apessos A, Agiannitopoulos K, Pepe G, Tsaousis GN, Papadopoulou E, Metaxa-Mariatou V, Tsirigoti A, Efstathiadou C, Markopoulos C, Xepapadakis G, Venizelos V, Tsiftsoglou A, Natsiopoulos I, Nasioulas G. Comprehensive BRCA mutation analysis in the Greek population. Experience from a single clinical diagnostic center. Cancer Genet. 2018;220:1–12.
Weiss M, Van der Zwaag B, Jongbloed J, Vogel M, Brüggenwirth H, Lekanne Deprez R, et al. Best practice guidelines for the use of next-generation sequencing applications in genome diagnostics: a National Collaborative Study of Dutch Genome Diagnostic Laboratories. Hum Mutat. 2013;34:1313–21.
Schouten JP, McElgunn CJ, Waaijer R, Zwijnenburg D, Diepvens F, Pals G. Relative quantification of 40 nucleic acid sequences by multiplex ligation-dependent probe amplification. Nucleic Acids Res. 2002;30:e57.
Casilli F, Di Rocco ZC, Gad S, Tournier I, Stoppa-Lyonnet D, Frebourg T, Tosi M. Rapid detection of novel BRCA1 rearrangements in high-risk breast-ovarian cancer families using multiplex PCR of short fluorescent fragments. Hum Mutat. 2002;20:218–26.
Foulkes WD. Inherited susceptibility to common cancers. NEJM. 2008;359:2143–53.
Pharoah PD, Antoniou A, Bobrow M, Zimmern RL, Easton DF, Ponder BA. Polygenic susceptibility to breast cancer and implications for prevention. Nat Genet. 2002;31:33–6.
Blackwood MA, Weber BL. BRCA1 and BRCA2: from molecular genetics to clinical medicine. J Clin Oncol. 1998;16:1969–77.
Venkitaraman AR. Cancer susceptibility and the functions of BRCA1 and BRCA2. Cell. 2002;108:171–82.
Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavtigian S, Liu Q, Cochran C, Bennett LM, Ding W, Bell R, Rosenthal J, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994;266:66–71.
Wooster R, Bignell G, Lancaster J, Swift S, Seal S, Mangion J, Collins N, Gregory S, Gumbs C, Micklem G, Barfoot R, Hamoudi R, et al. Identification of the breast cancer susceptibility gene BRCA2. Nature. 1995;378:789–92.
Narod SA, Foulkes WD. BRCA1 and BRCA2: 1994 and beyond. Nat Rev Cancer. 2004;4:665–76.
Ford D, Easton DF, Peto J. Estimates of the gene frequency of BRCA1 and its contribution to breast and ovarian cancer incidence. Am J Hum Genet. 1995;57:1457–62.
Wang Y, Cortez D, Yazdi P, Neff N, Elledge SJ, Qin J. BASC, a super complex of BRCA1-associated proteins involved in the recognition and repair of aberrant DNA structures. Genes Dev. 2000;14:927–39.
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A, Pasini B, Radice P, Manoukian S, Eccles DM, Tang N, Olah E, Anton-Culver H, Warner E, Lubinski J, Gronwald J, Gorski B, Tulinius H, Thorlacius S, Eerola H, Nevanlinna H, Syrjäkoski K, Kallioniemi OP, Thompson D, Evans C, Peto J, Lalloo F, Evans DG, Easton DF. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003;72:1117–30.
van den Broek AJ, van’t Veer LJ, Hooning MJ, Cornelissen S, Broeks A, Rutgers EJ, Smit VT, Cornelisse CJ, van Beek M, Janssen-Heijnen ML, Seynaeve C, Westenend PJ, Jobsen JJ, Siesling S, Tollenaar RA, van Leeuwen FE, Schmidt MK. Impact of age at primary breast cancer on contralateral breast cancer risk in BRCA1/2 mutation carriers. J Clin Oncol. 2016;34:409–18.
Fostira F, Tsitlaidou M, Papadimitriou C, Pertesi M, Timotheadou E, Stavropoulou AV, Glentis S, Bournakis E, Bobos M, Pectasides D, Papakostas P, Pentheroudakis G, Gogas H, Skarlos P, Samantas E, Bafaloukos D, Kosmidis PA, Koutras A, Yannoukakos D, Konstantopoulou I, Fountzilas G. Prevalence of BRCA1 mutations among 403 women with triple-negative breast cancer: implications for genetic screening selection criteria: a Hellenic Cooperative Oncology Group Study. Breast Cancer Res Treat. 2012;134:353–62.
Sawyer SL, Tian L, Kähkönen M, Schwartzentruber J, Kircher M, University of Washington Centre for Mendelian Genomics, FORGE Canada Consortium, Majewski J, Dyment DA, Innes AM, Boycott KM, Moreau LA, Moilanen JS, Greenberg RA. Biallelic mutations in BRCA1 cause a new Fanconi anemia subtype. Cancer Discov. 2015;5:135–42.
The Breast Cancer Linkage Consortium. Cancer risks in BRCA2 mutation carriers. JNCI. 1999;91:1310–6.
Offit K, Levran O, Mullaney B, Mah K, Nafa K, Batish SD, Diotti R, Schneider H, Deffenbaugh A, Scholl T, Proud VK, Robson M, Norton L, Ellis N, Hanenberg H, Auerbach AD. Shared genetic susceptibility to breast cancer, brain tumors, and Fanconi anemia. JNCI. 2003;95:1548–51.
Nesic K, Wakefield M, Kondrashova O, Scott CL, McNeish IA. Targeting DNA repair: the genome as a potential biomarker. J Pathol. 2018;244:586–97.
Newman B, Austin MA, Lee M, King MC. Inheritance of human breast cancer: evidence for autosomal dominant transmission in high-risk families. PNAS. 1988;85:3044–8.
Malkin D, Li FP, Strong LC, Fraumeni JF Jr, Nelson CE, Kim DH, et al. Germ line p53 mutations in a familial syndrome of breast cancer, sarcomas, and other neoplasms. Science. 1990;250:1233–8.
Levine AJ. p53, the cellular gatekeeper for growth and division. Cell. 1997;88:323–31.
Walsh T, Casadei S, Coats KH, Swisher E, Stray SM, Higgins J, Roach KC, Mandell J, Lee MK, Ciernikova S, Foretova L, Soucek P, King MC. Spectrum of mutations in BRCA1, BRCA2, CHEK2, and TP53 in families at high risk of breast cancer. JAMA. 2006;295:1379–88.
Masciari S, Dillon DA, Rath M, Robson M, Weitzel JN, Balmana J, et al. Breast cancer phenotype in women with TP53 germline mutations: a Li-Fraumeni syndrome consortium effort. Breast Cancer Res Treat. 2012;133:1125–30.
Gonzalez K, Noltner KA, Buzin CH, Gu D, Wen-Fong CY, Nguyen VQ, Han JH, Lowstuter K, Longmate J, Sommer SS, Weitzel JN. Beyond Li Fraumeni syndrome: clinical characteristics of families with p53 germline mutations. J Clin Oncol. 2009;27:1250–6.
Orloff MS, Eng C. Genetic and phenotypic heterogeneity in the PTEN hamartoma tumour syndrome. Oncogene. 2008;27:5387–97.
Nelen MR, Padberg GW, Peeters EA, Lin AY, van den Helm B, Frants RR, et al. Localization of the gene for Cowden disease to chromosome 10q22-23. Nat Genet. 1996;13:114–6.
Nelen MR, Kremer H, Konings IB, Schoute F, van Essen AJ, Koch R, Woods CG, Fryns JP, Hamel B, Hoefsloot LH, Peeters EA. Padberg GW novel PTEN mutations in patients with Cowden disease: absence of clear genotype-phenotype correlations. Eur J Hum Genet. 1999;7:267–73.
Pilarski R. Cowden syndrome: a critical review of the clinical literature. J Genet Couns. 2009;18:13–27.
Pilarski R, Burt R, Kohlman W, Pho L, Shannon KM, Swisher E. Cowden syndrome and the PTEN hamartoma tumor syndrome: systematic review and revised diagnostic criteria. JNCI. 2013;105:1607–16.
Jenne DE, Reimann H, Nezu J, Friedel W, Loff S, Jeschke R, Müller O, Back W, Zimmer M. Peutz-Jeghers syndrome is caused by mutations in a novel serine threonine kinase. Nat Genet. 1998;18:38–43.
Hearle N, Schumacher V, Menko FH, Olschwang S, Boardman LA, Gille JJ, Keller JJ, Westerman AM, Scott RJ, Lim W, Trimbath JD, Giardiello FM, Gruber SB, Offerhaus GJ, de Rooij FW, Wilson JH, Hansmann A, Möslein G, Royer-Pokora B, Vogel T, Phillips RK, Spigelman AD, Houlston RS. Frequency and spectrum of cancers in the Peutz-Jeghers syndrome. Clin Cancer Res. 2006;12:3209–15.
Guilford P, Hopkins J, Harraway J, McLeod M, McLeod N, Harawira P, et al. E-cadherin germline mutations in familial gastric cancer. Nature. 1998;392:402–5.
Pharoah PD, Guilford P, Caldas C, International Gastric Cancer Linkage Consortium. Incidence of gastric cancer and breast cancer in CDH1 (E-cadherin) mutation carriers from hereditary diffuse gastric cancer families. Gastroenterology. 2001;121:1348–53.
Uusitalo E, Rantanen M, Kallionpää RA, Pöyhönen M, Leppävirta J, Ylä-Outinen H, Riccardi VM, Pukkala E, Pitkäniemi J, Peltonen S, Peltonen J. Distinctive cancer associations in patients with neurofibromatosis type 1. J Clin Oncol. 2016;34:1978–86.
Seminog OO, Goldacre MJ. Age-specific risk of breast cancer in women with neurofibromatosis type 1. Br J Cancer. 2015;112:1546–8.
Southey MC, Teo ZL, Winship I. PALB2 and breast cancer: ready for clinical translation! Appl Clin Genet. 2013;6:43–52.
Antoniou AC, Casadei S, Heikkinen T, Barrowdale D, Pylkäs K, Roberts J, Lee A, Subramanian D, De Leeneer K, Fostira F, Tomiak E, Neuhausen SL, Teo ZL, Khan S, Aittomäki K, Moilanen JS, Turnbull C, Seal S, Mannermaa A, Kallioniemi A, Lindeman GJ, Buys SS, Andrulis IL, Radice P, Tondini C, Manoukian S, Toland AE, Miron P, Weitzel JN, Domchek SM, Poppe B, Claes KB, Yannoukakos D, Concannon P, Bernstein JL, James PA, Easton DF, Goldgar DE, Hopper JL, Rahman N, Peterlongo P, Nevanlinna H, King MC, Couch FJ, Southey MC, Winqvist R, Foulkes WD, Tischkowitz M. Breast-cancer risk in families with mutations in PALB2. NEJM. 2014;371:497–506.
Rainville IR, Rana HQ. Next-generation sequencing for inherited breast cancer risk: counseling through the complexity. Curr Oncol Rep. 2014;16:371.
Susswein LR, Marshall ML, Nusbaum R, Vogel Postula KJ, Weissman SM, Yackowski L, Vaccari EM, Bissonnette J, Booker JK, Cremona ML, Gibellini F, Murphy PD, Pineda-Alvarez DE, Pollevick GD, Xu Z, Richard G, Bale S, Klein RT, Hruska KS, Chung WK. Pathogenic and likely pathogenic variant prevalence among the first 10,000 patients referred for next-generation cancer panel testing. Genet Med. 2016;18:823–32.
Apostolou P, Fostira F. Hereditary breast cancer: the era of new susceptibility genes. Biomed Res Int. 2013;2013:747318.
Rizzolo P, Silvestri V, Tommasi S, Pinto R, Danza K, Falchetti M, Gulino M, Frati P, Ottini L. Male breast cancer: genetics, epigenetics, and ethical aspects. Ann Oncol. 2013;24(Suppl 8):viii75–82.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Apessos, A., Nasioulas, G. (2021). Breast Cancer Genetics. In: Rezai, M., Kocdor, M.A., Canturk, N.Z. (eds) Breast Cancer Essentials. Springer, Cham. https://doi.org/10.1007/978-3-030-73147-2_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-73147-2_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-73146-5
Online ISBN: 978-3-030-73147-2
eBook Packages: MedicineMedicine (R0)