
Abstract
The aging process is associated with social changes, among all the modifications that it entails. Relationship networks are transformed and/or impoverished, they may decrease. A decrease in social activity is possible and all these accumulated changes contribute, or can contribute, to increase the vulnerability of the elderly to experience loneliness. Loneliness is a concept that has been studied by several areas of knowledge, however it remains difficult to define. Objective: describe the dimensions and indicators of the concept of loneliness perceived by elderly who use social and health institutions. Methodology: Systematic Literature Review, through research at EBSCO, selecting the CINAHL and MEDLINE databases. Results: After analyzing the chosen studies, 5 dimensions of the concept of loneliness were identified. Indicators were also identified by the use of expressions/reports by the elderly in the analyzed studies. Conclusion: The “Absence of significant relationships”, “the lack of distraction” and “social isolation” are referred in the majority of the 9 articles analyzed. We can affirm that the relational and social isolation dimensions are valued, compared to the other dimensions identified. Health professionals must know the concept of loneliness perceived by the elderly to intervene. Moving to nursing homes can bring security and social support, but when it fails it can aggravate some of the indicators of loneliness of various dimensions. All participants in the studies analyzed were able to collaborate in the investigations, the non-verbal component was not explored, revealing a limitation in this review.
Access provided by Autonomous University of Puebla. Download conference paper PDF
Similar content being viewed by others


Keywords
1 Introduction
Someone is considered elderly if he/she is aged 65 years old or more in developed countries [1] and the arrival at this age is also linked to the retirement age, being a reference for old age. Portugal is in the same demographic evolution trend of the worldwide, there is a continued increase in elderly population. Corroborating this, data from the National Statistics [2] show that, in 2018, the resident population in Portugal was composed of 13.7% of young people, 64.5% of people of working age and 21.8% elderly. In this study we will consider that people with 65 years or more are elderly.
Aging is a process and it is associated with multiple consequences or effects of time in people. This process depends on multiple factors [3], such as: genetics; the context where the person is inserted and develops his lifestyle. This complexity makes the research in the aging field a priority area of action in its various dimensions.
Some of the changes that occur in the aging process are associated with social changes. Over the years there is a loss of members of the social network due to the death of family and friends, leading to a relationship network that is transformed and/or impoverishes, a network of contacts that decreases. On the other hand, there is a decrease in social activity and thereby all these accumulated changes contribute, or can contribute, to increase the vulnerability of the elderly to experience loneliness [4].
The concept of loneliness has been studied by several areas of knowledge; however, it remains difficult to define. Harry Stack Sullivan, in 1950, defined loneliness as an extremely unpleasant experience that leads to an extreme and inadequate need for human intimacy [5].
In 1973, Weiss defends that each individual needs to establish and/or maintain solid and binding interpersonal relationships and that these are essential to their well-being; when the relationship is not able to satisfy these needs inherent to the human condition, the individual experience loneliness [5]. Loneliness is seen as a multidimensional experience, both for the various causes and for the many contexts in which it manifests itself.
Also in 1973, Carl Rogers considered that loneliness is more acute and blunt in the individual who, for one reason or another, finds himself without some of his habitual defenses, a vulnerable self, alone, but real, safe from rejection in a world that judge and criticize [5].
Bastos, in 2005 [6] refers to loneliness as an important experience of aging, especially in adults of advanced age, due to the consequences it has on the quality of life and well-being of these people.
Loneliness can also be defined as a painful experience that often happens when social relationships are not adequate, in which the person feels lonely, even when surrounded by people, because there is a feeling of lack of affective support [7]. This type of loneliness in the elderly seems to be related more to losses, which mean a decrease of the feeling of belonging, than to social isolation [8], with an impact in 3 main dimensions: affection; cognition; and behavior [9].
The progressive loss of autonomy is linked to the increase in the level of loneliness in the elderly living with a disease [10], such as heart failure, that increases the probability of the inability to maintain an active social life, threatening health and well-being. Functional deterioration and an increase in the self-care deficit resulting from the aging process is limitating and this can mean an inability to leave the house or have the urge of being admitted in a nursing home. The effect of being in nursing homes on loneliness varies according to the conditions of the institution itself, the quality of social moments and moments shared with the family members [8].
Paulo Santos, a CINTESIS researcher, and Catarina Rocha-Vieira, from ARS Norte, argue that it is important to realize that loneliness in the elderly leads to a greater sum of their suffering and increases the risk of being over-medicated [11]. According to the same study, loneliness leads to an increase in the use of health services, as we can see through its relationship with chronic drug consumption, especially among the elderly over 80 years of age, explain the researchers of the study, which was published in the scientific journal Family Medicine & Primary Care Review [11].
All these data raised the interest and the importance of studying the way in which the elderly perceive loneliness in order to be able to make appropriate interventions later.
In addition to the more traditional interventions, technology can be an ally of health professionals in situation diagnosis, prevention and control of loneliness in the elderly.
However, as loneliness is a concept perceived individually, it is necessary to transform it into a universal concept.
This systematic review of the literature aims to describe the dimensions and indicators of the perceived concept of loneliness by elderly people, who use social and health institutions.
2 Methodology
The systematic review of the literature which, as referred by Cochrane Handboo [12], tries to collect all the empirical evidence that meets the pre-specified eligibility criteria, in order to answer a specific research question. Systematic and explicit methods are used, selected with the aim of minimizing bias, thus providing more reliable results from which conclusions can be drawn and then informed decisions can be made.
The research question was elaborated through the formulation PICO (P patient and/or problem of interest; I main intervention; C control, or if any, comparison intervention; O outcomes): Which are dimensions and the loneliness indicators that are perceived by elderly, users of social and health institutions?
In October 2019, research was carried out for this review, in the EBSCOhost - Research Databases database, through the reserved area of the University of Évora, Portugal. From this it was possible to access the following databases: CINAHL, MEDLINE with the descriptors: [(elderly) OR (aging) OR (frail elderly)], [(solitude) OR (loneliness) OR (isolation)], [(long term care) OR (nursing homes) OR (homes for the aged) OR (housing for the elderly)]. Subsequently, more descriptors were introduced: [(result of elderly) OR (aging) OR (frail elderly)] AND [(solitude) OR (loneliness) OR (isolation)] AND [(long term care) OR (nursing homes) OR (homes for the aged) OR (housing for the elderly)]. Inclusion criteria were defined: full text, in English and Portuguese, and scientific articles dated from 2014/01/01 to 2019/12/31.
As participants, only elderly adults receiving home care or living in nursing homes were included in the study.
Repeated articles were excluded and to make the preliminary selection of the articles, two readings were performed: first, two authors excluded some articles by reading their titles and later by reading their abstracts; second, the articles were analyzed by all the authors of this article, they were read in full in order to answer the research question as defined.
The methodological quality and reliability of the articles was elaborated through the critical analysis of the articles, for which the level of evidence presented was used, according to Melnyk and Fineout-Overhold [13], which indicate seven levels of evidence: level I (Referring to systematic literature reviews or meta-analysis), level II (randomized controlled studies), level III (randomized controlled study), level IV (case-control study or cohort study), level V (review systematic quantitative or descriptive studies), level VI (qualitative or descriptive study) and level VII (opinion or consensus). In this study the articles included had a level of evidence V or VI.
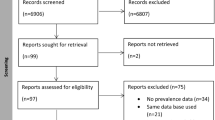
In total, 9 articles were analyzed using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) [13] recommendations were used to perform the Fig. 1.

Flowchart: selection of articles for SRL.
3 Results
The results of the articles found and selected for the preparation of this systematic review were summarized in the Table 1:
4 Discussion
After analyzing the chosen articles, five dimensions and seventeen concept indicators of loneliness were identified. These indicators were obtained by of expressions/reports used by the elderly, as well as interpretations by the authors in the analyzed studies. These are summarized in the Table 2.
Regarding the place where they live, only three articles refer to studies with elderly people living at home [14, 16, 21], the rest were carried out with institutionalized elderly people. This systematic review is in line with the previously consulted literature, when loneliness is referred to as a multidimensional experience. Therefore, it was possible to identify 5 dimensions and to each one of them indicators have been found and these indicators can help understand how the elderly perceive loneliness in the analyzed studies. In their study, Sjöberg, M., Edberg, AK, Rasmussen, BH, Beck, I. [14] identified two categories and seven subcategories of conditions that help in the experience of loneliness felt by the elderly: being recognized by others, with the subcategories being the focus of others' concerns, finding intimacy and having a meaningful exchange of thoughts and feelings; another category is to group negative thoughts and feelings with the subcategories adaptation and acceptance of the current situation, see life in the rear view mirror, get in touch with the spiritual dimensions and having the opportunity to get away and be distracted [14]. The shortcomings of these conditions are inserted in the relational and mental dimensions of the perception of loneliness. In the same sense, the study by Medvene, LJ, Nilsen, KM, Smith, R., Ofei-Dodoo, S., DiLollo, A., Webster, N.[16], mention the importance of social networks composed by family, diversified, restricted, religious, as these are more protective of loneliness than restricted networks. These concepts of social networks fit not only in the relational dimensions, but also in the isolation dimension.
In the dimension of health perception (named this way because it includes physical and psychological aspects of the health status perceived by the elderly), the study by Taube, E., Kristensson, J., Sandberg, M., Midlöv, P., Jakobsson, U. [21], revealed that depressed mood [22] was associated only with seeking outpatient care. In addition to this, the same study states that those who feel more lonely have more health complaints and consequently seek more this type of care. Predisposition to the disease, physical fragility associated with falls are indicators of loneliness for the elderly in the analyzed studies.
Lotvonen et al. [22] found significant differences in the elderly when moving to nursing homes, both physically and psychically. This study offers clues as to how this change, if not successful, can bring added problems to the elderly if they are not able to make the necessary transition to the new condition [14, 22]. We must highlight the lack of autonomy reported by the elderly in the study.
Lack of satisfaction about life [20], negative thoughts and feelings [14, 18] are other indicators that professionals should recognize as predictors of loneliness. The problem is that they are not subject to direct observation by professionals, because the mental dimension is the most difficult to access.
All the indicators found in this review can be observed by professionals, some directly and some indirectly. For example, professionals can observe directly: changes in the social network [20], in situations of loss, change in accommodation; social isolation [15,16,17, 19]; predisposition to diseases [19], due to the vulnerability of the organism and co-morbidities; health complaints and increased demand for physical and mental health services [21]. The observation of indicators such as negative thoughts and feelings – [14, 18]; lack of satisfaction about life – [20]; quality of life related to health perception –[22]; can be done through available instruments, namely interviews, questionnaires and scales. However, it is necessary that the elderly are able to participate in these types of investigation.
In five studies [15,16,17,18, 20] the evaluation of loneliness was carried out with the support of the UCLA-loneliness scale. This scale was developed by Russel, Peplau and Ferguson in 1978 in order to assess loneliness and was originally made up of items created with phrases/expressions used by lonely individuals that characterized feelings of loneliness [23].
All the elderly who participated in the nine studies analyzed were able to collaborate in the investigations. Despite this collaboration, the non-verbal component was not explored in the search for indicators of loneliness.
5 Conclusion
The most repeated concept indicators were: “Absence of significant relationships”; “The lack of distraction” and “social isolation”. Therefore, it can be said that the elderly value the relational and social isolation dimensions, compared to the other dimensions of the perceived concept of loneliness.
The move to a nursing home can bring social support and security, but when it is not successful it can aggravate some of the indicators of loneliness of various dimensions. It is important that professionals, in addition to assessing physical and psychological performance, consider the various components of the body’s well-being during the adjustment to the accommodation by the elderly [22].
It is known that nowadays technology provides several tools to improve the quality of life of the elderly, namely in cognitive stimulation, since it allows the development of the necessary skills to control and regulate our thoughts, emotions and actions [24]. This type of stimulation promotes not only well-being [25] in general, but also emotional well-being [26,27,28].
All the elderly who participated in the analyzed studies were able to collaborate in the investigations, but the non-verbal component of communication was not explored, revealing a limitation in this review.
6 Professional Practice Implications
Health professionals must understand the concept of loneliness perceived by the elderly to intervene and they should also be able to distinguish the dimensions that exist and affect that person. The intervention will be more efficient, in our understanding, because it will be based on the elderly person and the loneliness, he/she experiences and not a general concept. This is providing person-centered care. On the other hand, it should be possible to conceptualize the concept of loneliness perceived by the elderly. A common language is necessary and for this to happen, extensive studies must be carried out in the different social contexts where elderly people are included.
The positive relationship between the use of technological means in maintaining and even strengthening social relationships, especially with family and friends [27] offers new tools to health professionals. There are also studies on the use of robots as an alternative to therapies such as animal-assisted therapy in the promotion of the health and social well-being of elderly people in elderly care facilities [29].
Health professionals should use all available resources to provide efficient care.
References
Fonseca, A., Caldeira, E., Lopes, M.J., Marques, C., Casas-Novas, V.: Velhice: Representações Sociais Construídas por Estudantes de Enfermagem e Idosos. In: Lopes, M., Mendes, F.,Silva, A., Envelecimento- Estudos e Perspectivas, pp. 131–145, Martinari, São Paulo (2014)
Instituto Nacional de Estatística: Estatísticas Demográficas 2018, Instituto Nacional de Estatística, IP, Lisboa (2019). ISSN: 0377-2284
Lopes, D.: Solidão e Bem-estar Subjetivo na Terceira Idade: Estudo comparativo de idosos institucionalizados e não institucionalizados, Dissertação de Mestrado em Psicologia da Educação, Desenvolvimento e Aconselhamento, Faculdade de Psicologia e de Ciências da Educação, Universidade de Coimbra (2012)
Gomes, C.: A influência do meio ambiente ecológico na experiência da solidão e no bem-estar subjetivo, numa amostra de adultos mais velhos. Tese para obtenção de Grau de Mestre em Psicologia. Universidade de Lisboa, Faculdade de Psicologia Gomes (2015)
Pocinho, M. e Macedo, E.: Solidão: Um Construto Complexo. Interações: Sociedade e as novas modernidades 32, 53–66 (2017)
Bastos, M.: A solidão e os processos de vinculação nos jovens e sua inter-relação com a utilização da internet (Tese de doutoramento não publicada). Faculdade de Psicologia e de Ciências da Educação da Universidade do Porto (2005)
Azeredo, Z., Afonso, M.: Solidão na perspectiva do idoso. Revista Brasileira de Geriatria e Gerontologia 19(2), 313–324 (2016). https://doi.org/10.1590/1809-98232016019.150085
Rodrigues, R.: Solidão, Um Fator de Risco. Revista Portuguesa de Clínica Geral 34(5), 334–338 (2018). https://doi.org/10.32385/rpmgf.v34i5.12073
Stall, N.M., Savage, R.D., Rochon, P.A.: Loneliness in older adults. CMAJ 191(17), E476 (2019). https://doi.org/10.1503/cmaj.181655
Calha, A., Arriaga, M., Cordeiro, R.: Prevalência da solidão e depressão na população idosa residente na zona histórica da cidade de Portalegre, pp. 9–14. Revista Portuguesa de Enfermagem de Saúde Mental (spe1) (2014)
Seviço Nacional de Saúde in (2019). https://www.sns.gov.pt/noticias/2019/07/22/estudo-impacto-da-solidao-em-idosos/
Donato, H., Donato, M.: Etapas na Condução de uma Revisão Sistemática Acta Med. Port. 32(3), 227–235 (2019). https://doi.org/10.20344/amp.11923
Pompeo, D., Rossi, L., Galvão, C.: Revisão integrativa: etapa inicial do processo de validação de diagnóstico de enfermagem. Acta Paul Enferm. 22(4), 434–438 (2009)
Sjöberg, M., Edberg, A.K., Rasmussen, B.H., Beck, I.: Being acknowledged by others and bracketing negative thoughts and feelings: Frail older people’s narrations of how existential loneliness is eased. Int. J. Older People Nurs. 1–9 (2019). ISSN: 1748-3743
Drum, J.L., Medvene, L. J.: The social convoys of affordable senior housing residents: fellow residents and “Time Left”. Educ. Gerontol. 43, 540–551 (2017). ISSN: 1521-0472
Medvene, L.J., Nilsen, K. M., Smith, R., Ofei-Dodoo, S., DiLollo, A., Webster, N.: Social networks and links to isolation and loneliness among elderly HCBS clients. Aging Ment. Health 20, 485–493 (2016). ISSN: 1364-6915
Eskimez, Z., Demirci, P.Y., TosunOz, I.K., Oztunç, G., Kumas, G.: Loneliness and social support level of elderly people living in nursing homes. Int. J. Caring Sci. 12, 465–474 (2019). ISSN: 1791-5201
Gan, P., Xie, Y., Duan, W., Deng, Q., Yu, X.: Rumination and loneliness independently predict six-month later depression symptoms among Chinese elderly in nursing homes. PLoS ONE 10, 11 (2015). ISSN: 1932-6203
Cavalcante, E.S., Freire, I.L.S., Gomes, A.T.L., Fonseca, M.F., Miranda, F.A.N., Torres, G.V.: La percepción del envejecer en una población de ancianos. Cultura de los Cuidados (Edición digital) 21(47) (2017)
Andrew, N., Meeks, S.: Fulfilled preferences, perceived control, life satisfaction, and loneliness in elderly long-term care residents. Aging Ment. Health 22, 183–189 (2018). ISSN: 1364-6915
Taube, E., Kristensson, J., Sandberg, M., Midlöv, P., Jakobsson, U.: Loneliness and health care consumption among older people. Scand. J. Caring Sci. 29, 435–443 (2015). ISSN: 1471-6712
Lotvonen, S., Kyngäs, H., Koistinen, P., Bloigu, R., Elo, S.: Mental well-being of older people in finland during the first year in senior housing and its association with physical performance. Int. J. Environ. Res. Public Health 15, 1–20 (2018). ISSN: 1660-4601
Russel, D., Peplau, L., Ferguson, M.: Developing a measure of loneliness. J. Pers. Assement 42, 290–294 (1978)
Lousa, E.: Benefícios da estimulação cognitiva em idosos: um estudo de caso. Coimbra, Portugal: Dissetação apresentada ao Instituto Superior Miguel torga para obtenção do grau de Mestre em Psicologia (2016). https://repositorio.ismt.pt/bistream/123456789/682/1/DISSERTA%C3%87%C3%83O.pdf
Páscoa, G., Gil, H.: Envelhecimento e tecnologia - Desafios do Século XXI. In: Coimbra, Portugal, 14th Iberian Conference on Information Systems and Technologies (CISTI) 1–6 (2019). https://repositorio.ipcb.pt/bitstream/10400.11/6627/1/Atas_IEEExplore_GP_HG_CISTI_2019_.pdf
Hung, L., Liu, C., Woldum, E., Au-Yeung, A., Berndt, A., Wallsworth, C., Horne, N., Gregorio, M., Mann, J., Chaudhury, H.: The benefits of and barriers to using a social robot PARO in care settings: a scoping review. BMC Geriatr. 19, 10 (2019). https://doi.org/10.1186/s12877-019-1244-6
Ferreira, S., Veloso, A.: Reflexões sobre o impacto da utilização das TIC nas redes sociais de apoio do indivíduo sénior. In: Carioca, V. (Coord.). Envelhecer em tempos de Matrix – Metáforas, Reflexões e Práticas em Gerontecnologia, pp. 93–106. Repositório Científico do Instituto Politécnico de Viseu. Capítulo em obra nacional, como autor (2020). https://hdl.handle.net/10400.19/6269
Fonseca, C., Lista, A., Lopes, M., Mendes, F., Marques, C., Garcia-Alonso, et al.: Dependence in self-care with comorbidity, indicators of nursing care and contributions to an ontology of aging: systematic review of the literature. In: 13th Iberian Conference on Information Systems and Technologies (CISTI), pp. 1–6. IEEE (2018). https://doi.org/10.23919/CISTI.2018.8399236
Hung, L., Liu, C., Woldum, E., et al.: The benefits of and barriers to using a social robot PARO in care settings: a scoping review. BMC Geriatr. 19, 232 (2019). https://doi.org/10.1186/s12877-019-1244-6
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this paper

Cite this paper
Gomes, S., Lopes, M., Fonseca, C. (2021). Perceived Loneliness by Elderly a Systematic Literature Review. In: García-Alonso, J., Fonseca, C. (eds) Gerontechnology III. IWoG 2020. Lecture Notes in Bioengineering. Springer, Cham. https://doi.org/10.1007/978-3-030-72567-9_37
Download citation
DOI: https://doi.org/10.1007/978-3-030-72567-9_37
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-72566-2
Online ISBN: 978-3-030-72567-9
eBook Packages: MedicineMedicine (R0)