
Abstract
The atrioventricular complex (A-V complex) consists of the left atrial wall, the leaflets of the Mitral valve, its cords and tendons, the papillary muscles from which they arise, and the ventricular wall through which the Mitral apparatus is connected in a continuous loop. Anteriorly, from the surgeons’ view, the Aortic leaflet is continuous with the fibrous aorto-mitral curtain, which abuts the non- and left coronary cusp of the Aortic valve. The integrity of the A-V complex secures normal left ventricular and Mitral valve function. If any of these elements break down Mitral regurgitation will ensue. If the lesion is primarily that of the valve and/or sub-valvar apparatus, uncorrected the left ventricle will fail. If the lesion is of the left atrium or the left ventricle, mitral regurgitation will commonly develop. This chapter explores the pathogenesis and pathophysiology of the valve-ventricular complex and the fact of embryogenesis as the progenitor of primary mitral valve lesions.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Introduction
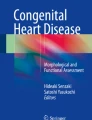
The Mitral valve is so much more than a singular structure. A better term for it is the Mitral valve complex, or more precisely the left atrioventricular valve complex (A-V complex), the term “complex” perhaps first coined by J. K. Perloff and W. C. Roberts in 1972 [1]. This left A-V valve complex consists of the left atrial wall (e), the mural mitral valve leaflet (b), the tendinous cords (c), the papillary muscles (d), and the postero-superior and infero-basal left ventricular free wall (g). In addition, the Aortic leaflet (a), for most of its circumferential length, becomes the Aorto-Mitral curtain (f), which forms just over one-third of the circumference of the left ventricular outflow tract and in turn merges with the ventricular side of the aortic valve (Fig. 7.1).


(a) The Mitral valve complex [FCW sketch]. a. Aortic leaflet, b. Mural leaflet, c. Tendinous cords, d. Papillary muscles, e. Left Atrial wall, f. Aorto-Mitral curtain, g. L.V. free wall, h. L.A. appendage. (b) Anatomical demonstration of the same attitudinal region as in the sketch. These images reveal the innate saddle shape of the aorto-mitral curtain and the aortic leaflet/aorto-mitral curtain continuity and atrial convexity of the LV outflow tract impressed upon this structure. [Figure 46-1&2 McAlpine WA. Heart and Coronary arteries]. (b) The saddle shape of the Aortic leaflet and the Aorto-mitral curtain of the mitral valve. Anatomical demonstration of the same attitudinal region as in sketch. These images reveal the innate saddle shape of the aorto-mitral curtain and the aortic leaflet/aorto-mitral curtain continuity and atrial convexity\ of the LV outflow tract impressed upon this structure. [Figure 46-1&2 McAlpine WA. Heart and Coronary arteries]
At the conjunction of the Aortic, Tricuspid, and Mitral valves lies a condensation of connective tissue that is at its most dense as a result of the forces that are exerted at this point through the cardiac cycle. This region is referred to, by some authorities, as the central fibrous body of the heart, from which more dense condensation of the membrane runs part way around the antero-superior circumference of the Mitral valve. These variable but incomplete extensions were first described by Henle J. and were referred to as the left and right fila of Henle 1873 [2]. In some species cartilage or even bone may be found at these most dense areas of membranous condensation, reflecting the stress and strain exerted at these regions through the cardiac cycle. Contrary to dogma, the atrioventricular junction (annulus) is not a complete fibrous ring around the orifice of the valve, but simply the boundary between atrium and ventricle; there is no formal discrete structure that can be defined as the annulus. For most of its circumference, it contains fat and superiorly the Circumflex coronary artery and inferiorly the coronary sinus has relatively close proximity. For most of this junction, the fibrous extension from the antero-superior Trigone does not form a complete ring, more of which later [3]. Thus a better description of this region is the atrioventricular junction, which is more complex than the use of the simple term annulus implies.
For normal physiological function, each of the components of the atrioventricular complex must be structurally and functionally normal. The use of the more comprehensive descriptive term, the atrioventricular complex that we refer to as the Mitral valve, is important in trying to help physicians and surgeons make sense of the lesions that are encountered. Indeed, the atrioventricular valvar complex is really a machine in the strict sense of the definition of that word. That is, an apparatus using or applying mechanical power, having several parts, each with a definite function, and together performing certain kinds of work; or an instrument that transmits a force or directs its application [4].
The key to the maintenance of this machine’s function is the way that the leaflets of the valve meet at the commissure.Footnote 1 As is well established the leaflets do not close edge-to-edge. They meet and, supported by the primary cords, they coapt over a height of 5–8 mms (Fig. 7.2a & b). Just as the keystone is the vital component of an arch, so coaptationFootnote 2 is for the full and pressurised closure of the Mitral valve. Each normal closed and fully developed leaflet forms a somewhat complex sinusoidal shape as it extends from the left atrial wall or aorto-mitral curtain, into the body of the leaflet and then turning downward into the ventricle where it meets its counter-part (Fig. 7.2c).

(a) Sketch showing atrioventricular valve coaptation. [FCW] (b) Detail from RL 19080 recto revealing coaptation of the mitral valve. [Copywrite Her Majesty the Queen. Royal Collection Windsor]. (c) Schematic representation of the Sinusoidal shape of the coapting Mitral leaflets. [FCW]
Disrupt any part of the mechanism of a machine complex and the machine cannot function normally. As so often is the case in failing machinery, the failure of one part will lead to a slow and steady, or on occasions, a catastrophic failure of the whole. So it is in the heart, disruption of any part of the atrioventricular complex can lead to a slow or catastrophic failure of valve and heart function. Left atrial dilatation, as a result of atrial fibrillation, will often lead to distraction of the atrial/ventricular junction, drawing the mural leaflet away from coaptation with the aortic leaflet and slowly developing mitral regurgitation [5]. In contrast, papillary muscle rupture, as a result of myocardial infarction, will usually lead to catastrophic and life-threatening pulmonary oedema and rapid onset left ventricular failure with a high mortality. Between these extremes is the most common form of atrioventricular dysfunction, caused by slowly worsening mitral valve leaflet prolapse, with progressive left atrial and ventricular volume loading and heart failure. As a result of increasing wall stress, this more chronic form of disease of the valve incurs fibrous tissue deposition within the left ventricular myocardium, worsening the prognosis for the patient and reducing the chance of a full recovery of ventricular function. In this chapter we will explore the functional aspects of the structure of the left atrioventricular valve and the importance of each component in its performance.
The Atrioventricular Complex Through the Cardiac Cycle
The normal Mitral valve is a highly dynamic structure. It is subject to significant and complicated movement in all components, under rapid pressure changes, throughout the cardiac cycle. The valve has to achieve all of this with surfaces that have to prevent surface thrombus formation, with an average life span of 70 + years. A challenge, which to date, no man-made structure has been able to reliably reproduce.
Let us begin at the end of systole . At this point, the left ventricular muscle is maximally contracted with significant twisting of the apex from the base as well as the apex being pulled upward toward the base. The papillary muscles are tensioned and the atrioventricular valve is tightly closed with full leaflet coaptation. The Aortic valve is beginning to close with the leaflets beginning to unfurl as a result of the vortices in the aortic sinuses. As muscular tension abates, diastole begins , the ventricle begins to untwist and to fill with blood from the left atrium across the opening Mitral orifice. The mass of blood entering the ventricle accelerates the untwisting of the chamber. As the dilatation of the ventricle accelerates a suction effect is created further enhancing the flow of blood from the atrium to ventricle. The Mitral valve leaflets are opening with the longer Aortic leaflet guiding the flow of blood towards the apex [6]. Vortices have begun above the valve leaflets by the end of systole which then roll down into the ventricle and as the blood reaches the apex of the ventricle larger vortices develop which begin to float the leaflets away from the ventricular walls and upwards towards each other [7, 8]. Leonardo suggested that the bulk of the Papillary muscles prevent the mitral mural leaflet from reaching the ventricular wall which enables the blood to get behind it and begin to billow the leaflet towards coaptation which fits with modern understanding of the vortices getting behind the skirts of the valve and drifting the leaflets towards each other.Footnote 3 The veracity of this suggestion has been borne out by recent studies. Left atrial contraction drives the final blood flow into the ventricle across the valve further stretching the left ventricular myocardium, recruiting the innate elastic recoil that exists in the myocardial walls.
A particular property of the Mitral valve during diastole, that enhances maximum flow under all conditions [9], is the ability of the atrioventricular junction to dilate beyond the orifice area at which the leaflets fully coapt. This occurs as the oxygen and nutrient demands of exercise are met by an increasing cardiac output and thus, venous return. The heart evolved through times when we as a species relied upon being able to go from rest to maximum exercise quickly, when chasing our prey, or escaping the preying jaws of the sabre-toothed Tiger! To carry the machine/mechanical analogy further, we can compare the exercise-driven dilating atrioventricular orifices to the wide exhausts on sports cars to allow exiting of burnt gases as speedily as possible to allow the following cycle of fuel ignition and energy release. The atrioventricular orifice changes its circumference by up to 40% through the cardiac cycle.
In addition to the expansile A-V junction, the leaflets have developed in such a way, that there are interruptions in leaflet continuity of varying depth, to allow it to open rather like the pleats of a lady’s skirt, thereby, allowing greater freedom of movement, and in this case, enhanced flow of blood to the ventricle. These normal interruptions have supportive cords that extend into their depths revealing that they must be interruptions in development of the atrioventricular cushions (Fig. 7.3 cords to the depth of the mural leaflet interruptions). The terminology used to name these interruptions has been various, with the common use of the word cleft to describe them. Cleft is the past participle of the verb to cleave and endorses the idea of a splitting or cutting of the tissues which is not the case. Indentations, (implying a dentate appearance with the notches seen along a dental line) does not quite match the bluntness or the depth of these normal interruptions, found in development. Perhaps a better term is a recess but the word interruption implies not only the anatomical finding but also the probable aetiology. Interruptions of normal depth do not reach as deeply as the A-V junction and usually extend for no more than one-third of the height of the leaflet. Thinking back to the embryology of the valve it raises the question that these leaflet interruptions are where the atrioventricular cushions have not grown as far forwards as the part on either side (Fig. 7.4, Deficient leaflet development at the centre of the P2 region).

Tendinous cords extending into the depths of the abnormally deep clefts

Deficient leaflet development at the centre of the P2 region
It is true to say that the detailed knowledge of the full development of the components of the mitral valve remains unknown. Therefore, any description of the detailed development has to remain in the world of speculation at the moment. However, if one is to, in a sense, reverse engineer what is found at surgery in patients with mitral valve prolapse, certain tentative conclusions may be drawn. The detailed development of the valve apparatus is enormously complex. The development of the papillary muscles from the non-compacted myocardium is a highly complex process and it is to be expected that nature gets it wrong from time to time. Similarly, the development of the tendinous cords and their relationship to the leaflet and the papillary muscles is yet another example of the huge complexity of the development of this structure. Hence interruptions in the advancement of the atrioventricular cushions would give rise to the recesses found at surgery. As the development of the cords and the papillary muscles must be a conjoined process it is not at all surprising to find that the cords reach to the very depths of the interrupted leaflets. Variations from the normal horseshoe-shaped papillary muscles are also to be expected and are regularly found. These anatomical variations will disrupt the normal distribution of forces around the conjoined aortic and mural leaflets.

(a & b) Overgrowth of Aortic leaflet to match under-development of Mural leaflet
It is common to find the extension of the opposing portion of the Aortic leaflet in valves where the mural leaflet is underdeveloped (Fig. 7.5a & b, Overgrowth of Aortic leaflet to match under-development of the mural leaflet). If this assumption of abnormal development with severe retardation in growth of parts of the A-V cushions is true then it will likely lead to the morbid anatomy of deep interruptions in the leaflet reaching to the atrioventricular junction of the orifice. Here we see that the cords reach into the depths of these undeveloped leaflet interruptions indicating a retardation of growth of these parts of the leaflets (Fig. 7.4). These are features that we commonly find in the regurgitant valve, more of which later.
At the end of the diastole, the ventricular muscle begins to contract with a twisting motion and the conical ventricle shortens from apex to base. The papillary muscles are tensioned, exerting a restraining force on the tendinous cords, which in turn prevent eversion of the mitral leaflets as they begin to move towards coaptation. It is the primary cords that prevent eversion of the valve leaflets and as the force on the leaflets grow, the secondary cords come into play, spreading the load through their arching extensions extending onto the underside of the leaflets. This area of cordal distribution on the ventricular side of the valve has become known as the “rough zone” (Fig. 7.6). This is not a good name as it is not rough in the true meaning of that word. The leaflet is covered with endothelium and thus inherently smooth but has the rippled, raised insertions of the tendinous cords as they merge with the leaflet tissue. These arching terminations of the secondary cords spread the load of the pressurised ventricle. As the intra-ventricular pressure continues to rise the area of coaptation of the two leaflets develops over 0.5–0.8 cms. At this point in the cycle, the load is transferred from the primary cords to the secondary cords, the primary cords, even vibrating in these later stages of systole. They have done their job in preventing prolapse of the leaflet. This differentiation of primary and secondary cords is not absolute but relative as there is some residual fusion of the two cordal types near the edge of the leaflet. At this point, the blood continues to swirl in vortices under the now almost completely closed valve developing the coaptation of the leaflets until complete closure is achieved.

So-called rough zone underneath the Aortic leaflet [Bovine specimen]
Once the leaflets meet and coaptation is complete the energy expended in ventricular contraction can be spent on driving the blood along the left ventricular outflow tract and out into the aorta. From the time of complete closure of the Mitral leaflets the force of intra-ventricular pressure is exerted on the underside of the valve leaflets which then becomes in engineering terms a force field . They have to distribute this energy evenly across both leaflet surfaces to prevent undue strain in local parts. The valve has grown and developed with these stresses continuously at work, shaping them and forming the response to stress. The leaflets bear the strain through several mechanisms.
The key component is the surfaces of coaptation, that are present in a fully closed normal valve. This coaptation has developed through the restraint of the primary cords preventing leaflet prolapse. The closing of the sphincter-like muscle at the base of the ventricle enhances this closure pushing the leaflets towards each other further supporting coaptation. The load is further shared through the tendinous cords and the tensed papillary muscles through to the ventricular muscle wall and back to the base of the heart at the atrioventricular junction. The distribution of the tendinous cords, arising from the two main horseshoe-shaped papillary muscles spatially arranged around each end of the commissure (closure line) of the leaflets is vital in load sharing. It will be noted that the two leaflets are not completely separated at the ends of the commissures and this allows the load to be shared between them at these junctional regions. The tendinous cords are most dense in these regions.
The secondary tendinous cords arch across the underside of the leaflets spreading the load evenly as do the arches under the roof in a large building (Fig. 7.6: So-called rough zone underneath the Aortic leaflet [Bovine specimen]).
In the normal arrangement, the direction of tension from leaflet to papillary muscle is vertical. Imagine walking to the airport carrying your luggage at 45 degrees to your body! It could not be maintained for long. And so it is with the papillary muscles and the tendinous cords. Abnormal development of the Papillary muscles causing the insertion of the cords at an angle from the vertical puts undue strain on them further increasing the likelihood of stretch and rupture. The Papillary muscles as with all other parts of the atrioventricular complex are liable to congenital malformation. A description of papillary muscle variations can be found in a paper by Roberts and Cohen [10]. The most common extreme version is the parachute mitral valve where all of the cords arise from one papillary muscle head. Whilst this can produce regurgitation it usually produces stenosis.
It would appear that condensations of the non-compacted myocardium give rise to the Papillary muscles. (see the chapter on development R H Anderson et al) Therefore, it is not surprising to find a multitude of possibilities arising from abnormal development. Some variations observed at the surgery are shown in Fig. 7.7. When operating on these valves it is striking how frequently one sees these forms of abnormality. Papillary muscle malalignment can be through abnormal embryogenesis giving rise to the kinds of abnormalities illustrated in Fig. 7.7, or through left ventricular distortion through ischaemic lesions or other cardiomyopathies resulting in functional mitral regurgitation. A proper appreciation of papillary muscle geometry is important in approaching mitral valve reconstruction.

Intraoperative photographs of abnormal papillary muscle morphology
As systole develops, the pressure inside the left ventricular outflow tract (LVOT) increases, and the pliable aorto-mitral curtain, which forms one-third of the LVOT, naturally takes up a cylindrical shape. Also the junction of the A-M curtain flexes on the aortic leaflet that then turns upwards as the leaflets close in coaptation. This is how the so-called Saddle shape of the valve develops [11]. The aorto-mitral curtain forming the “pommel” of the saddle and the aortic leaflet the seat of the saddle (Fig. 7.1b). These forces have helped to shape the aortic leaflet and maintenance of its three-dimensional shape through which the strain of ventricular closure is distributed. The fundamental importance of this distinct morphology is discussed by Salgo IS, Gorman JH, and colleagues. They point out how the curvature of the Aortic leaflet reduces mechanical stress [12]. Of significant interest is the fact that this observation seems to hold across mammalian species. They suggest quite reasonably that their data strongly suggest that nature conserves the 3-dimensional geometric changes brought about by the highly dynamic sphincter-like closure of the basal ventricular muscle and the conformation of the aorto-mitral curtain, which alters the orifice surface area dimensions by up to 40% [13]. The annulus (the ring orifice) is a descriptive term rather than a singular and identifiable structure. It responds to these pressure and force changes rather than exerting them. The dynamism of the atrioventricular orifice and the leaflet morphology is well demonstrated in an exhaustive MRI study of the mitral orifice and leaflets by Shuan Leng and colleagues [14]. The normal annular dynamics were significantly reduced in patients with mitral regurgitation over valves in the normal group. This reflects the basal dilatation of the ventricle in response to increasing volume overload with the progression of the mitral regurgitation.
There is the suggestion that by mapping the saddle shape in a complete annuloplasty ring and re-imposing it on the orifice of the valve that this can impart improved physiological morphology. Contrary to this thought is the fact that by leaving the inter-trigonal space (aorto-mitral curtain) free of device, as in a C band (Trigone to Trigone) the annulus can and will take up naturally the saddle shape for the reasons described previously. Miller and colleagues demonstrated with three-dimensional computer modelling that “regardless of their three dimensional shape, rigid and complete annuloplasty rings, but not a partial flexible band, increased maximum principal anterior mitral leaflet strains predominantly in the belly and edge regions in the normal beating Ovine heart [15].” Thus emphasising the natural tendency of this dynamic conformation of the Aortic leaflet to the pressurised ventricle and outflow tract to allow the optimal configuration.
The stress and strain found within the Mitral valve during isovolumetric contraction have been studied in vivo in both animals and man. Several studies have demonstrated the beautiful adaptation of this structure to the forces that are exerted upon it in all stages of the cardiac cycle [16, 17]. Moreover, the histological adaptation to the distributed stresses on the leaflets has been shown to occur as well [18]. The authors of this paper (Blomme et al. [18]) demonstrated that CTGF (a profibrotic growth factor promoting the synthesis of extracellular matrix (ECM) components) is up-regulated in many pathological processes involving mechanically challenged organs, promotes ECM accumulation and is considered as a hallmark of fibrotic diseases. They demonstrate that abnormal perception and responsiveness of valvular interstitial cells to mechanical stress may induce an inappropriate adaptative remodelling of the valve progressively leading to a myxomatous mitral valve. The authors were able to show that mechanical stretching induced the nuclear translocation of myocardin-related transcription factor-A (MRTF-A) which forms a transcriptional complex with SRF to promote the expression of target genes, notably CTGF.
Recently Calafiore et al have made the case for structural remodelling of the mitral valve through molecular stimulation and cellular change as a result of altered forces and flow on ischaemic mitral valves [19]. It is becoming ever more clear that restoration of a normal force distribution throughout the valve leaflets, cords, and papillary muscles as well as restoring normal flow patterns is the key to sustainable return to normal mitral valve function and structural remodelling.
Piecing all of this information together it would appear that the abnormal formation of the mitral valve complex will lead to the abnormal distribution of the forces that act upon it throughout the cardiac cycle and that these abnormal forces will bring about pathological stress and strain distribution in the leaflets, cords, and papillary muscles. These excess forces in areas of the valve that are not well supported can and almost certainly do lead to the changes that are seen histologically with collagen and elastin disruption and the laying down of myxoid material. Fundamentally the valvular interstitial cells (VIC’s) control the nature of the extracellular matrix. Their phenotype is regulated by signals from the environment and thus in turn, they are responsible for the homeostasis in normal circumstances and remodelling of the ECM in pathological states of abnormal stress and strain [20,21,22].
In a paper addressing the spectrum of normality of the Mitral valve relevant to Mitral prolapse, as long ago as 1979, Becker and De Wit wrote, “ If one considers the fact that the Mitral valve sustains considerable pressures for a prolonged time, one may perhaps speculate on the effects of an irregular distribution of cordal support on leaflets”. This is to be found in valves from patients in increasing age and they defined them as ballooning deformities. They go on to point out that study of the body of the leaflets from these conditions, reveal an increase in mucopolysaccharides, probably an expression of tissue injury [23]. One of the central tenants of their paper is that “minor variations in architecture of the cordal apparatus may leave some parts of the leaflets less well supported than others, a phenomenon which could then result in deformity of the leaflet at that particular site.” Furthermore, they note that these abnormalities are most commonly found at the site of the posteromedial commissure and related parts of the mural leaflet. In summary, they state that, weakening of the central core of the leaflet, may act as a final common pathway to a process of chronic injury and in some cases, a floppy and ultimately prolapsing valve leaflet [24].
This assertion that unbalanced forces on a biological structure will lead to a change in cellular signalling and thence to a change in leaflet morphology and thence to a failure of valve structural integrity is a modern take on sage intelligent deduction. In a now lesser known work, (but still recognised by significant minds in Science and the Arts as among the finest academic books of the twentieth century), On Growth and Form [25], D’Arcy Thompson, its polymath author, powerfully makes the case in his words that the form of any objects in nature are diagrams of the forces that act upon them. In other words, “that in general no organic form exists save as are in conformity with physical and mathematical laws.” He declared that physiology is vastly strengthened and enlarged by making use of the chemistry and of the physics of the age. All should be supported by mathematical explanation. These ultra-modern thoughts are coming to pass in the modern scientific age as the understanding of the regurgitant/degenerating mitral valve evolves. He wrote in his beautiful Edwardian prose, “For the harmony of the world is made in Form and Number, and the heart and soul and all the poetry of Natural Philosophy are embodied in the concept of mathematical beauty.” He alludes to the power of measurement and understanding in a biblical quote from Isiah wherein he sates “Who has measured the waters in the hollow of his hand and metered out heaven with the span, and comprehended the dust of the earth in a measure and weighed the mountains in scales and the hills in a balance.”.Footnote 4 These profound statements recognise the fundamental determination of structure by natural forces, normal or abnormal on the structure in question. Let us then consider the impact of abnormal morphology of the valve on its structure and function.
The Malfunctioning Mitral valve
We have discussed the normal structure and function of the left-sided atrioventricular complex, the Mitral valve, and the great importance of normal structural integrity and form. Let us now consider the impact of the abnormal morphology that is to be found in the malformed valve which leads to an inability to control the normal unidirectional flow of blood. As stated at the beginning of this chapter failure of any component of the atrioventricular complex will lead to various degrees of incompetence.
The most common lesion presenting to the cardiologist/surgeon is that of Mural leaflet prolapse. This is accompanied by cordal elongation and frequently cordal rupture (Fig. 7.8).

Ruptured cord. Note the excess height of the leaflet and the deep clefts on either side
As discussed earlier, closer inspection of the valve will almost always reveal accompanying papillary muscle abnormalities and/or deep interruptions on either side of the prolapsing segment. If we think of the need to distribute forces evenly across the closed and tensioned valve it is easily visualised that deep recesses, extending to the atrioventricular junction and abnormal papillary muscle distribution will prevent normal force distribution.
In addition, it is common to find that the prolapsing portion is much taller (sometimes x2 or x3) than the height of the rest of the mural leaflet (Fig. 7.9)

Eccentric excessive height of the mural leaflet in the P3 region. Note the scalloping of the P1/P2 regions also turning the mural leaflet into four segments
At the commissural ends, there may be a significant paucity of cordal support usually associated with papillary muscle abnormalities and leaflet prolapse (Fig. 7.10)

Antero-superior commissural prolapse with highly abnormal papillary muscle and a significant paucity of cords
All of these and many other combinations of abnormalities will confront the mitral valve surgeon who should be versed in all of the possible techniques of repair and reconstruction to reach a 95% repair rate which should be possible in the modern state of knowledge.
As these are all congenital developmental lesions and the valve is so complex any combination of anatomical abnormalities may be encountered. The degenerative component in the leaflet histology is a result of sustained maldistribution of forces on the valve leaflets and not a primary disease process.
Conclusions
The mitral valve complex is one of the most complicated developmental processes that the body has to undertake. Its many components and the mode of embryogenesis is such that it should surprise no one that nature makes mistakes that lead to the lesions that we find inside the heart at surgery. The increased frequency of these lesions within families reinforces the congenital nature of these lesions. The fact that the “degenerative” changes and the manifestation of these morphogenic problems do not present until later in life fits with the presented hypothesis that it is the congenital malformation that is the primary lesion in these valves and not a later and secondary disease process as has been suggested by some. The inability to distribute the exerted forces of systolic closure lead to the morphological cahnges encountered in the prolapsing segments of the valve.
Notes
- 1.
The line of coaptation of the leaflets throughout the closure line is correctly named the commissure, not just the marginal junctions.
- 2.
Coaptation: derived from the Latin, coaptare meaning to fit closely together.
- 3.
Leonardo da Vinci. Windor Royal Library. Royal Collection RL 19073 recto.
- 4.
Isiah. Chapter 40 verse 12. The Old Testament. King James’s bible.
References
Perloff JK, Roberts WC. The mitral valve apparatus: functional anatomy of mitral regurgitation. Circulation. August 1972;XLVI:227–39.
Henle J. Handbuch der Gefasslehre des Menschen. Braunschweig, 1876.
Angelini A, Ho SY, Anderson RH, Davies M, Becker AE. A histological study of the atrioventricular junction in hearts with normal and prolapsed leaflets of the mitral valve. Br Heart J. 1988;59:712–6.
Thompson D, editor. Oxford concise dictionary of current English. 9th ed. Oxford: Clarendon Press; 1995.
Ring L, Dutka DP, Wells FC, et al. Mechanisms of atrial mitral regurgitation: insights using 3D trans esophageal echo. Eur Heart J Cardiovasc Imaging. 2014;15:500–8.
Faludi RF, Szulik M, D’hooge J, et al. Left ventricular flow patterns in healthy subjects and patients with prosthetic mitral valves: An in vivo study using echocardiographic particle image velocimetry. JTCVS. 2010;39(6):1501–10.
Bao T, Sotiropolous F, Coffey D, Keefe D. Vortex formation and instability in the left ventricle. Phys Fluids. 2012;24:091110.
Elbaz ME, Calkoen EE, et al. Vortex flow during early and late left ventricular filling in normal subjects: quantitative characterization using retrospectively-gated 4D flow cardiovascular magnetic resonance and three-dimensional vortex core analysis. J Cardiovasc Magn Reson. 2014;78:16.
Glasson JR, Komeda M, Daughters GT, Niczyporuk MA, Bolger AF, Ingels NB, Miller DC. Three-dimensional regional dynamics of the normal mitral anulus during left ventricular ejection. J Thorac Cardiovasc Surg. March 1996;111(3):574–85.
Roberts WC, Cohen LS. Left ventricular papillary muscles. Description of the normal and a survey of conditions causing them to be abnormal. Circulation. July 1972;XLVI:138–54.
Chun X, Brinster CJ, et al. A novel approach to in vivo mitral valve stress analysis. Am J Physiol Heart Circ. 2010 Dec;299(6):H1790–4.
Salgo IS, Gorman JH III, Gorman RC, Jackson BM, Bowen FW, Plappert T, St John Sutton MG, Henry Edmunds L Jr. Effect of annular shape on leaflet curvature in reducing mitral leaflet stress. Circulation. August 2002;106(6):711–7.
Levack MM, Jassar AS, Shang EK, et al. Three-dimensional echocardiographic analysis of mitral annular dynamics. Circulation. 2012;S184:S183–8.
Leng S, Zhang S, Jiang M, et al. Imaging 4D morphology and dynamics of mitral annulus in humans using cardiac cine MR feature tracking. Sci Rep. 2018;8:81. https://doi.org/10.1038/s41598-017-18354-2.
Bothe W, Kuhl E, et al. Rigid, complete annuloplasty rings increase anterior mitral leaflet strains in the normal beating ovine heart. Circulation. 2011 Sep 13;124(11 Suppl):S81–96.
Rausch MK, Famaey N, et al. Mechanics of the mitral valve: a critical review, an in vivo parameter identification, and the effect of prestrain. Biomech Model Mechanobiol. 2013 Oct;12(5):1053–71.
Amini R, Eckert CE, Koomalsingh K, McGarvey J, Minakawa M, Gorman JH, Gorman RC, Sacks MS. On the in vivo deformation of the mitral valve anterior leaflet: Effects of annular geometry and referential configuration. Ann Biomed Eng. 2012;40:1455–67.
Blomme B, Deroanne C, et al. Mechanical strain induces a pro-fibrotic phenotype in human mitral valvular interstitial cells through RhoC/ROCK/MRTF-A and Erk 1/2 signalling. JMCC. October 2019;135:149–59.
Calafiore AM, Totaro A, et al. Mimicking natural mitral adaptation to ischaemic regurgitation: a proposed change in the surgical paradigm. Eur J Cardiothorac Surg. 2020;58:35–9.
Ayoub S, Ferrari G, Gorman RC, Gorman JH, Schoen FJ, et al. Heart valve biomechanics and underlying mechanobiology. Compr Physiol. 2016;6(4):1743–80.
Waxman AS, Kornreich BG, Gould RA, Moïse NS, Butcher JT. Interactions between TGFβ1 and cyclic strain in modulation of myofibroblastic differentiation of canine mitral valve interstitial cells in 3D culture. J Vet Cardiol. 2012;14(1):211–21.
Aupperle H, März I, Thielebein J, Schoon HA. Expression of transforming growth factor-beta1, -beta2 and -beta3 in normal and diseased canine mitral valves. J Comp Pathol. 2008;139(2–3):97–107.
Becker AE, De Wit AP. Mitral valve apparatus. A spectrum of normality relevant to mitral valve prolapse. Br Heart J. 1979;42:680–9.
Becker AE, De Wit AP. Mitral valve apparatus. A spectrum of normality relevant to mitral valve prolapse. Br Heart J. 1979;42:688.
Thompson DA. On growth and form. Cambridge University Press. First edition 1917. Second enlarged edition 1942.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 The Author(s), under exclusive license to Springer Nature Switzerland AG
About this chapter

Cite this chapter
Wells, F.C. (2021). The Atrioventricular Complex: Function and Dysfunction. In: Wells, F.C., Anderson, R.H. (eds) Mitral Valve Disease. Springer, Cham. https://doi.org/10.1007/978-3-030-67947-7_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-67947-7_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-67946-0
Online ISBN: 978-3-030-67947-7
eBook Packages: MedicineMedicine (R0)