
Abstract
Surgical management of the cervical lymph nodes represents an essential element of comprehensive care for patients with oral/head and neck cancer. The histopathologic status of these lymph nodes remains the primary prognostic index for patients with squamous cell carcinoma of this anatomic region. It is therefore essential for ablative surgeons to establish and apply a scientific and sound philosophical approach to neck surgery to improve the potential for long-term survival, and possible cure of patients with oral/head and neck cancer. Such an approach is applicable to both the clinically positive neck (cN+) and the clinically negative neck (cN0). In fact, a distinct survival advantage exists when executing selective neck dissections for occult neck disease. This chapter reviews the history, classification, and indications for neck dissection in patients with oral/head and neck squamous cell carcinoma.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Oncologic levels of the neck
- Occult neck disease
- Selective neck dissection
- Supraomohyoid neck dissection
- Functional neck dissection
- Comprehensive neck dissection
- Modified radical neck dissection
History of Neck Dissections for Oral/Head and Neck Cancer
Surgical removal of the cervical lymph nodes plays a very important role in the comprehensive management of squamous cell carcinoma of the oral/head and neck anatomic region. Two of the most important aspects of the assessment of patients with these cancers, therefore, include the clinical evaluation of the lymph nodes of the neck, and the prediction of occult neck disease in the case of a clinically negative neck examination (cN0). Occult neck disease can be defined as disease that is present microscopically in cervical lymph nodes, but cannot be palpated clinically and may elude identification by special imaging studies including positron emission tomography/computed tomography (PET/CT) scans [1,2,3]. As such, oral/head and neck cancer patients who are statistically likely (>20%) [4] to harbor occult disease in their cervical lymph nodes are clinically staged as cN0 and should undergo elective neck dissections with the frequent and resultant histopathologic identification of metastatic disease in the cervical lymph nodes (pN+). Enhanced survival outcome assessments indicate that elective surgical removal of occult cervical lymph nodes should be executed with curative intent [5, 6].
Oral cancer is most commonly treated surgically, so it is most appropriate that the neck be simultaneously addressed surgically while reserving radiotherapy, and possibly chemotherapy for the adjuvant setting when adverse pathologic features so dictate [7]. Indeed, observing the N0 neck, only to operate the neck in the case of future, clinically apparent nodal disease, is detrimental from a survival perspective in a large majority of cases of oral squamous cell carcinoma [8]. This statement is based on the realization that salvage rates for these patients are unfavorable [9, 10]. To this end, in 1839, Warren recommended removal of lymph nodes in the submandibular triangle associated with tongue cancer with the expressed intention of improving the curability of cancer at that site [11]. One of the first systematic descriptions of the importance of cervical lymph nodes in head and neck cancer was reported by Maximilian von Chelius in 1847 [12]. In 1906, a frequently quoted paper was published in The Journal of the American Medical Association by Dr. George Crile of the Cleveland Clinic in Ohio that reviewed the execution of neck dissection in head and neck cancer patients [13]. The paper was entitled Excision of cancer of the head and neck – With special reference to the plan of dissection based on one hundred and thirty-two operations. Interestingly, Crile’s 1906 paper is the most commonly quoted treatise regarding this discipline and is thought to represent the first of his works on this subject, yet it was in fact his second paper published on this exercise. His first paper was published on this topic in 1905, entitled On the surgical treatment of cancer of the head and neck – With a summary of one hundred and twenty-one operations performed upon one hundred and five patients, in which Crile initially described an en bloc dissection of the neck [14, 15]. In the 1905 paper, Crile created an analogy between breast cancer, where regional lymph nodes are routinely excised, and head and neck cancer where a similar approach should therefore be applied. He stated that a dissection of lymph nodes of the neck is indicated whether the “glands are or are not palpable.” Crile stated, “palpable glands may be inflammatory and impalpable glands may be carcinomatous.” “A strict rule of excision should therefore be followed.” He further recommended against handling of the malignant tissue due to the lymphatic channels remaining intact that would encourage dissemination of the malignancy. Finally, he indicated that a tracheostomy was “doubly indicated” since aside from the short-circuiting of respiration and fixing the trachea, it produced a wall of protective granulations across the top of the precarious mediastinal area that therefore forestalled dissemination of disease into the chest.
Early in the introduction of his 1906 paper, Crile astutely identified that the immediate extension from the primary malignant focus principally occurred by permeation and metastasis in the regional lymphatics. As such, Crile summarized his recommendations for surgical management of the neck by stating that an incomplete operation would lead to dissemination of disease, stimulate the growth of the cancer, shorten the patient’s life , and diminish comfort. He re-emphasized his philosophy that isolated excision of the primary focus of the cancer was “as unsurgical as excision of a breast” in the case where the regional lymph nodes remained unaddressed. Further, he offered support of en bloc removal of cervical lymph nodes in that excision of individual lymphatic glands would not result in cure of the patient, but it would rather be followed by greater dissemination and more rapid growth. He emphasized that a block dissection of the regional lymphatics and the primary malignancy was necessary, therefore, for effective treatment of these patients. This block dissection included lymph nodes in levels I–V of the neck (Table 1.1), the sternocleidomastoid muscle , the internal jugular vein, and the spinal accessory nerve. Crile performed this treatment in the management of patients in whom lymph nodes were enlarged (cN+ neck) as well as in those patients whose lymph nodes were not clinically enlarged (cN0 neck). Crile’s comments were collectively directed to head and neck cancer of a variety of anatomic sites. In his 1906 discussion, oral cavity cancers represented only a minority, including four cases of floor of mouth cancer, two alveolar ridge cancers, and 12 cancers of the tongue. Four cases of oropharyngeal cancer were reported including two cases of tonsillar cancer and one case each of soft palate cancer and pharyngeal cancer. This notwithstanding, this paper served as a model for treatment of the neck in patients with oral cancer. Interestingly, the most common cancer treated by Crile in his report of 132 cancers was that of the lips, accounting for 31 of these cases. By twenty-first century standards, most of these lip cancers could likely have been managed without neck dissection. There were no deaths related to these 31 lip cancers. Moreover, while the frequently quoted theme of Crile’s paper was radical neck dissection, only 36 patients underwent such treatment in his report. Ninety-six patients reportedly did not undergo “radical block dissection.”
In his 1923 paper [16] entitled Carcinoma of the jaws, tongue, cheek, and lips, Crile elaborated on his recommendations for excision of the cervical lymph nodes. He emphasized that early cancer of the gingiva or cheek that metastasizes late does not demand excision of the lymph nodes, while cancer of the lip, however early, demands the complete excision of all lymph nodes that drain the involved area. Further, cancer of the tongue or of the lip calls for the complete removal of the lymph nodes of the neck on both sides [16]. Crile’s 1923 paper reiterated many of the statements made in the 1905 and 1906 papers, including comments about a review of 4500 reported autopsies of patients with head and neck cancer in which only 1% identified distant metastases. He emphasized that when death results from a cancer of the head and neck that local and regional disease was responsible for death rather than distant disease.
Dr. Crile’s three papers represented the landmark articles regarding neck dissections for head and neck cancer until Dr. Hayes Martin published his paper entitled Neck dissection [17] in 1951. This extensive review commented on an experience of 1450 neck dissections performed from 1928 to 1950, although statistics were derived from 665 operations performed in 599 patients. One hundred forty-four patients with tongue cancer constituted the most common primary site, and these patients underwent 131 unilateral neck dissections and 13 bilateral neck dissections. Dr. Martin did not believe that a routine prophylactic radical neck dissection (RND) was practical in managing patients with cancer of the tongue and lip and presented data from a survey sent to 75 of his colleagues, the consensus of which supported his contentions. His conclusion regarding the RND was that routine prophylactic neck dissection was considered “illogical and unacceptable” for cancer of the oral cavity. He made these comments, due to his thoughts about oncologic safety and not about functional consequences, stating that no one could carry out prophylactic neck dissection to a degree sufficient to effect significant improvements in cure rates. He believed that the RND was an excessively radical technique performed electively and routinely. Stated differently, the RND should not be employed for the N0 neck, a philosophy that is largely observed in the twenty-first century. Regarding the elective neck dissection, Martin reported that this concept was not performed on the Head and Neck Service of Memorial Hospital at the time. Rather, he believed that definite clinical evidence that cancer was present in the lymph nodes represented one criterion for neck dissection. Other criteria included the requirement of control of the primary lesion giving rise to the metastasis, or if not controlled, there should be a plan to remove the primary cancer simultaneously with the neck dissection. Moreover, Martin indicated that there should be a reasonable chance of complete removal of the cervical metastatic cancer, there should be no clinical or radiographic evidence of distant metastasis, and the neck dissection should offer a greater chance of cure than radiation therapy.
While the RND has proved to be a reliable method of treating patients with oral/head and neck cancer, it is associated with substantial morbidity. Nahum [18] described a syndrome of pain and decreased range of abduction in the shoulder following RND . These symptoms constitute shoulder syndrome and relate to the sacrifice of the spinal accessory nerve (SAN) . Preservation of the SAN during neck dissection ameliorates the syndrome [19]. The morbidity of the RND, therefore, gave way to the development of the numerous modifications of the RND that maintain oncologic safety while also reducing morbidity of the RND. These modifications of the RND were designed to preserve one or more of the sternocleidomastoid muscle, spinal accessory nerve, and internal jugular vein and have been realized in the form of the modified radical neck dissection (MRND) proper, and the selective neck dissections were represented primarily by the supraomohyoid neck dissection and secondarily by the functional neck dissection . By twenty-first century standards, radical and MRNDs are most commonly performed as therapeutic neck dissections for clinically N+ disease, while selective neck dissections are most commonly performed as elective neck dissections for clinically N0 disease.
Cervical Lymph Nodes in Relation to Oral Cancer and Classification of Neck Dissections
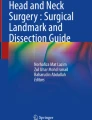
Surgical management of the cervical lymph nodes in patients with oral/head and neck squamous cell carcinoma requires a thorough understanding of the lymphatic anatomy of the neck and the patterns of nodal metastasis from these cancers. Classifications for neck dissections by the American Head and Neck Society [20, 21] reviewed six lymph node levels (Table 1.1) for defining the boundaries of neck dissection, levels I–V of which are potentially involved with oral squamous cell carcinoma (Fig. 1.1). In addition, lymph nodes in levels I–III are designated as sentinel, or first echelon lymph nodes for oral cavity cancers. Specifically, these are the first lymph nodes that will typically contain metastatic squamous cell carcinoma when the cervical lymph nodes in fact contain cancer. This well-accepted concept forms the basis for elective neck dissections where the likelihood of occult neck disease exceeds 20% [4].

The oncologic lymph node levels of the neck as applied to oral cavity squamous cell carcinoma. (With permission from Regezi et al. [70])
To develop uniformity regarding nomenclature, Robbins et al. [20] developed standardized neck dissection terminology in 1991 and updated the classification in 2002 [21] (Table 1.2). Their original classification was based on the following concepts: (1) the RND is the fundamental procedure to which all other neck dissections are compared, (2) MRND denotes preservation of one or more nonlymphatic structures, (3) selective neck dissections denote preservation of one or more group(s) of lymph nodes, and (4) extended RND denotes removal of one or more additional lymphatic and/or nonlymphatic structure(s). A modified radical neck dissection refers to the excision of all lymph nodes routinely removed by radical neck dissection with preservation of one or more nonlymphatic structures such as the spinal accessory nerve, internal jugular vein, and sternocleidomastoid muscle. Therein, lymph node levels I–V are removed in this neck dissection (Table 1.1). Typically, a type I MRND involves preservation of the spinal accessory nerve; a type II MRND involves preservation of the spinal accessory nerve and the internal jugular vein; and a type III MRND involves preservation of the spinal accessory nerve, internal jugular vein, and the sternocleidomastoid muscle [22]. It seems that most authors favor the type I MRND for the cN+ neck in oral/head and neck cancer [23] (Fig. 1.2), and this modification of the traditional RND does not compromise oncologic safety [24].



A 71-year-old man (a and b) presented with a 2.5 cm area of mucosal ulceration and submucosal induration in the left tongue (c). Evaluation of the cervical lymph nodes identified a palpable 1.5 cm left level II mass. An incisional biopsy of the left tongue identified squamous cell carcinoma. Staging was consistent with a T2N1M0 cancer. PET/CT scans demonstrated hypermetabolic activity in the left tongue (d) and level II nodes of the left neck (e and f). Due to the patient’s cN+ designation, a type I modified radical neck dissection was planned. A Crile incision was designed (g) and the MRND neck dissection specimen is noted (h and i). The resultant defect in the neck is appreciated (j). The patient simultaneously underwent left partial glossectomy with 1.5 cm margins (k). Three of 41 lymph nodes contained metastatic squamous cell carcinoma on microscopic examination. The tongue specimen demonstrated perineural invasion. The patient underwent postoperative radiation therapy and demonstrated no evidence of disease at 3 years postoperatively (l, m, and n)
Neck dissections are additionally classified as comprehensive or selective. Comprehensive neck dissections are those where cervical lymph nodes are removed in levels I–V. Such neck dissections are represented by the radical and modified radical neck dissections for N+ disease, and commonly also remove nonlymphatic tissue. Selective neck dissections are those where cervical lymph nodes are selectively removed, and most commonly for cN0 disease. The most commonly performed selective neck dissection for oral cavity cancer is the supraomohyoid neck dissection that removes lymph nodes in levels I, II, and III. The anterolateral neck dissection removes lymph nodes in levels II, III, and IV, and the posterolateral neck dissection removes lymph nodes in levels II, III, IV, and V. The functional neck dissection is a poorly understood and often misquoted neck dissection in terms of sacrifice of lymph node levels but typically removes lymph nodes in levels II, III, IV, and V.
Comprehensive Neck Dissections for the Clinically Positive Neck
Type I Modified Radical Neck Dissection
The surgical concepts of modified radical neck dissections (MRNDs) are based on the understanding that the aponeurotic system of the neck encases the internal structures that are usually removed during RND. The MRND works within these planes of dissection and still results in an en bloc lymphadenectomy while preserving structures including the spinal accessory nerve, the sternocleidomastoid muscle, and the internal jugular vein. By definition, the type I modified radical neck dissection sacrifices lymph node levels I–V, the sternocleidomastoid muscle, and underlying internal jugular vein while intentionally preserving the spinal accessory nerve (Fig. 1.2). Most head and neck cancer surgeons preferentially execute this neck dissection for surgical management of the cN+ neck.
Selective Neck Dissections for the Clinically Negative Neck
Functional Neck Dissection (II–V)
In 1967, Bocca and Pignataro published their work on a more conservative neck dissection [25] that has been referred to as the functional neck dissection (FND). Lymph nodes in levels II–V are removed with intentionality in this selective neck dissection. Bocca and Pignataro indicated, “if the submaxillary fossa must be included in the dissection, the sacrifice of the submaxillary gland can generally be avoided because the gland itself may be easily stripped of its aponeurotic sheath.” These authors also reported the flexibility of inclusion of a level I dissection in this procedure in 1980, indicating “the superficial cervical fascia is cut along the lower border of the submaxillary fossa against the lateral surface of the submaxillary gland , preserving the marginal mandibular nerve” [26]. Clearly, it was not the author’s intention to execute a complete dissection of level I structures including lymph nodes in this region [27]. Feldman and Applebaum [28] provided justification for the exclusion of level I lymph nodes in their evaluation of 51 neck dissections, 26 of which were performed for cancer of the larynx and 12 of which were performed for cancer of the oral cavity. The results of their study identified three of the 51 neck dissections containing metastatic disease in level I of the neck. Of those three cases with metastatic level I disease, one specimen was a stage II floor of mouth cancer and one specimen was a stage IV retromolar cancer. None of the 12 laryngeal cancers demonstrated metastatic level I disease. By twenty-first century standards, ablative surgeons cannot equate the lymph node drainage patterns of oral cancer and laryngeal cancer such that a functional neck dissection, while scientifically justified for the treatment of laryngeal cancer, cannot be similarly justified for the treatment of oral cancer.
The first author to describe the functional neck dissection was Osvaldo Suarez from the University of Cordoba Medical School in Argentina. He published the first, original, systematic approach to this neck dissection in 1963 [15]. History indicates that Bocca learned the technique from Suarez and later published numerous observations on this technique as an elective neck dissection. Prior to that time, the elective neck dissection was the RND. In their report, the authors described absence of lymphatic recurrences in about 100 neck dissections where only the lymphatic tissue of the neck was sacrificed and the sternocleidomastoid muscle, internal jugular vein, and spinal accessory nerve were preserved. In 1984, these authors published their findings of 1500 functional neck dissections in 843 patients operated between 1961 and 1982 [29]. Cancer of the larynx comprised 87% of the patients in this series. Twelve hundred of these neck dissections were elective (cN0), while 300 were therapeutic (cN+). Neck recurrences occurred in 68 cases (8.1%). Of these, 16 occurred in the elective FND patients (2.38%) for N0 disease, and 52 recurrences occurred in the 171 therapeutic FND patients (30.4%) for N+ disease. Calearo and Teatini reviewed 476 functional neck dissections that were performed in 211 patients with only nine recurrences (3.5%) during a 3-year follow-up period [30]. Other authors [31, 32] have expressed similar satisfaction with this neck dissection.
Supraomohyoid Neck Dissection (I–III)
The supraomohyoid neck dissection is the ideal solution to the dilemma for some surgeons as to how to properly manage the cN0 neck associated with oral cavity cancer [33] (Fig. 1.3). A significant body of literature supports the performance of elective neck dissections for T1N0 and T2N0 squamous cell carcinomas of the oral cavity, identifying the incidence of occult neck disease in these cases of 36–42% [34,35,36]. As such, numerous authors have enthusiastically recommended the supraomohyoid neck dissection as a staging procedure in the management of the N0 neck associated with oral cavity squamous cell carcinoma [37,38,39,40,41].



A 37-year-old man (a and b) with a 5-cm left tongue mass (c) that was tender to palpation. An incisional biopsy was performed that identified squamous cell carcinoma. Staging was consistent with a T3N0M0 cancer. A PET/CT (d) was obtained that did not identify hypermetabolic activity associated with the cervical lymph nodes. The patient underwent a left supraomohyoid neck dissection (e and f) with identification and preservation of branches of the external carotid artery and internal jugular vein (g). A left hemi-glossectomy with 1 cm linear margins was performed (h, i, and j) and reconstructed with a radial forearm free microvascular flap (k). The patient’s final pathology identified 1/20 lymph nodes with metastatic squamous cell carcinoma and perineural invasion in the tongue specimen. He underwent postoperative radiation therapy and remains free of disease at 4 years postoperatively (l, m, and n)
The supraomohyoid neck dissection removes lymph node levels I–III while preserving the spinal accessory nerve, internal jugular vein, and sternocleidomastoid muscle. This author shares the opinion of many others that delaying elective surgery of the cN0 neck and adopting the watchful approach to the cN0 neck is deleterious in most cases. This is particularly true for tongue cancer where survival in the watchful waiting group has been noted to be 33% compared to 55% in the neck dissection group, and that locoregional control increased from 50% to 91% when neck dissection was performed [42]. The supraomohyoid neck dissection is a straightforward surgical procedure that requires little time to perform and offers prognostically significant information to the patient, as well as to the radiation oncologist who might otherwise be unable to render treatment based on objective information. Most importantly, it addresses neck disease in an occult stage whereby survival is improved [8]. Its scientific basis is the observation that lymph nodes in levels I–III are sentinel nodes.
In a study by Shah examining the specimens of 501 patients undergoing radical neck dissection, only 9% of patients showed histopathological evidence of cervical lymph node metastases in level IV when the neck dissection was elective in nature [43]. The incidence of positive nodes in level V was only 2%. These data indicate that levels IV and V probably do not require removal in the management of the cN0 neck. This notwithstanding, Shah [44] recommended the excision of level IV lymph nodes along with levels I, II, and III when operating the cN0 neck related to primary cancers of the lateral border of the oral tongue. Crean et al. [45] found occult metastases in level IV in 5 of 49 cases of oral cavity cancers. The conclusion of these authors was that extending the traditionally performed SOHND to include the easily accessible level IV should be adopted as standard treatment in the management of the cN0 neck. Byers et al. [46] identified an overall frequency of skip metastases in squamous cell carcinoma of the oral tongue in 15.8% of their patients studied. These patients either demonstrated level IV metastases as the only manifestation of disease in the neck or the level III node was the only positive node present without disease in level I and II. The authors’ conclusions were that the usual supraomohyoid neck dissection is inadequate for a complete pathologic evaluation of all the nodes at risk for patients with squamous carcinoma of the oral tongue. Feng et al. [47] retrospectively studied 637 patients with oral squamous cell carcinoma, particularly regarding skip metastases at level IV or V. Clinically negative necks were identified in 447 patients. The highest rate of occult metastasis was located at level II in these 447 patients, accounting for 74 cases (16.6%), while level I was involved in 67 cases (15.0%), and level III was involved in 16 cases (3.6%). Skip metastases were identified in 5 of the 447 cN0 patients (1.1%). No skip metastasis to level IV alone was observed in this study. The authors concluded that the supraomohyoid neck dissection is the preferred neck dissection in cN0 patients with oral squamous cell carcinoma.
Some authors have recommended performing the supraomohyoid neck dissection with frozen section analysis of the lymph nodes to permit intraoperative extension of the neck dissection in the form of a modified radical neck dissection [48, 49]. Other authors have stressed the importance of including level IV beyond the traditional supraomohyoid neck dissection when managing the cN0 neck where the primary tumor is located in the tongue [46, 50]. While many surgeons do not advocate the use of the supraomohyoid neck dissection in the management of the N+ neck, some recent evidence suggests the efficacy of this type of neck dissection with postoperative radiation therapy in the management of head and neck cancer patients with a cN+ neck [51]. This approach remains controversial and not oncologically safe if extracapsular extension of metastatic cervical lymph node disease is diagnosed microscopically. The supraomohyoid neck dissection is therefore not recommended by this author for the management of the cN+ neck.
Indications for Neck Dissection and Their Outcomes
This author performs surgical treatment of the neck primarily utilizing two main neck dissections. In patients with a clinically N0 neck, the sentinel or first echelon nodes are present in levels I, II, and III. As such, a supraomohyoid neck dissection as described would adequately address the neck in these patients (Fig. 1.3). As discussed, stage I and II squamous cell carcinoma of the tongue is a disease with a threshold incidence of occult neck disease thereby warranting elective treatment of the neck. This author does not adopt the wait-and-watch approach in such circumstances. The use of the supraomohyoid neck dissection in patients who have pathologically negative nodes has resulted in excellent control of disease in the neck with failure rates of less than 10% [43]. In the 30% of patients who are found to have pathologically proved occult neck disease , the failure rate with the supraomohyoid neck dissection alone ranges from 10% to 24% depending on the number of positive nodes and the presence of extracapsular spread [52]. When postoperative radiation therapy is added to this scenario, the failure rates drop to 0–15%, again depending on the extent of nodal metastases [53].
In patients with palpable cervical metastasis (N+), the levels at highest risk are levels I–IV. In the opinion and experience of this author, the most prudent operation to perform is the type I modified radical neck dissection, thereby sparing the spinal accessory nerve provided it is not involved with tumor (Fig. 1.2). This approach is recommended since palpable nodes smaller than 3 cm in diameter have a substantial incidence of extracapsular spread of disease [54]. The presence of extracapsular spread may breech the aponeurotic planes relied upon when the SCM and IJV are otherwise preserved. As such, a selective neck dissection is probably contraindicated in managing the cN+ neck related to oral cavity cancer [52]. In patients with clinically palpable neck disease, the results of type I MRND followed by postoperative radiation therapy depend upon the bulk of disease in the neck, the presence of extracapsular spread in the lymph node, and the radiosensitivity of microscopic disease remaining in the neck. When patients receive radiation therapy following a type I MRND for an N+ neck, neck failure rates in N1 patients are 7–10% and approximately 12% in N2 patients [55]. These results compare favorably to those obtained with RND in similar patients [52]. It is therefore oncologically safe and appropriate to preserve cranial nerve XI as part of a modified radical neck dissection.
While a great deal of thought must be exerted in determining which neck dissection is best suited for patients with oral cancer, perhaps the more controversial aspect of oral cancer care surrounds the small cohort of patients who do not require a neck dissection for effective management of their oral cancer. Due to the relative lack of morbidity and high yield of the supraomohyoid neck dissection in managing the cN0 neck, it seems reasonable to perform this neck dissection in most, if not all patients with squamous cell carcinoma of the oral cavity. This notwithstanding, there are some patients with early oral cancer for whom elective neck dissection is not necessary. In general terms, this author believes that the risk of occult neck disease is less than 20% in some patients with primary T1N0 and T2N0 cancers of the lip and anterior maxillary and anterior mandibular gingiva squamous cell carcinoma. As such, elective neck dissections may not be required in these patients in specific clinical circumstances. Robbins and Samant [56] indicate that a supraomohyoid neck dissection should be performed for all T1–T4 tongue cancers, T2–T4 at all other sites, and where there is identified perineural or lymphatic invasion in the primary specimen. Zhan et al. [57] analyzed 2,623 cases of primary cT1N0 squamous cell carcinoma in the National Cancer Database from 1998 to 2012, all of which underwent surgical resection and elective neck dissection. Most patients in the cohort were white (93%), men (60%), and operated at an academic medical center (58%). Forty-two percent of the cancers were primarily located in the oral tongue. Concordance with clinical and pathologic stage I designations occurred in 86% of cases. Occult nodal disease was 15% in this cohort. The incidence of occult nodal disease was higher in women (16.7%) than in men (13.9%; P = 0.049), and in moderately differentiated (17.4%) and poorly differentiated tumors (28.5%) than well-differentiated disease (5.9%; P < 0.001). Incidence did not vary significantly by age groups, race, academic versus community hospital, insurance type, or medical comorbidity. The authors concluded that elective neck dissection should be performed for moderately differentiated or poorly differentiated cT1N0 squamous cell carcinoma of the oral cavity, regardless of depth of invasion, and especially in women with tongue cancer. They also indicated that sentinel lymph node biopsy might represent a viable alternative for high-risk patients.
Brockoff et al. [58] investigated the threshold tumor depth of invasion of oral squamous cell carcinoma that would predict a 20% or greater risk of cervical lymph node metastases. The authors analyzed 286 patients in their database from 2009 to 2014. Most patients (94%) were white and the most common primary tumor site was the oral tongue (37%). The authors performed 390 neck dissections for these 286 patients, and 115 patients (40%) demonstrated cervical lymph node metastases. At 1-mm depth of invasion, the authors determined that none of the seven neck dissections demonstrated a positive node. At the 2-mm depth of invasion, there were 12 patients with node negative necks and 3 patients with node positive necks for an overall percentage of 20%. An increasing depth of invasion of greater than 2 mm resulted in a greater than 20% node positivity. The authors determined that the depth of invasion required for a 20% positivity rate of cervical lymph node metastases was 2 mm for tongue, 3 mm for floor of mouth, 3 mm for retromolar trigone, and 4 mm for alveolus/hard palate. The authors concluded that depth of invasion is an important factor to consider when establishing surgical recommendations for patients with T1N0 disease. This notwithstanding, the ultimate decision should be based on both the depth of invasion and the anatomic site of the primary tumor.
Kuo et al. [59] established guidelines for lymph node yield in patients with oral cavity squamous cell carcinoma while indicating that quality metrics were established for lymph node yield in regional node dissections for bladder, colorectal, esophageal, penile, and skin cancers. The authors analyzed 13,143 eligible cases of oral cavity cancer in the National Cancer Database . Patient factors that predicted a higher lymph node yield were male gender, young age, and African American race status. Of the patients who had known clinical lymph node staging (n = 6147), 71.1% underwent neck dissection. Most patients (79%) had cN0 disease, and the rate of neck dissection was 63.9% in these patients and 98.3% of cN+ patients underwent neck dissection. The lymph node yield was 21 lymph nodes overall, with 20 lymph nodes in the cN0 group and 25 lymph nodes in the cN+ group. Patients had significantly decreased survival when fewer than 16 lymph nodes were present in the neck dissections for cN0 patients and fewer than 26 lymph nodes in the neck dissections for cN+ patients.
The next genre of neck dissection is designated the superselective neck dissection utilizing sentinel node biopsies [60]. This technique was first described in melanoma patients [61], and it analyzes lymphoscintigraphy-guided biopsies of sentinel nodes in the neck to determine the histologic status of first echelon cervical lymph nodes and whether a neck dissection is indicated. Careful examination of a specific lymph node, as occurs in the evaluation of sentinel lymph node biopsies, but not elective neck dissections, may increase the utility of sentinel lymph node mapping. Ambrosch analyzed a series of 76 neck dissection specimens from patients originally staged as histologically negative [62]. The authors utilized ten-micron serial sections and hematoxylin-eosin staining and cytokeratin staining to re-assess the lymph nodes previously reported as negative. Eight previously undiagnosed micrometastases were identified in 6 specimens from 6 patients resulting in upstaging. Another study revealed 36 of 96 (37%) pathologically negative elective neck dissection specimens to contain micrometastases upon serial resectioning [63]. Similar findings have been noted by other authors [64, 65]. The consensus conclusion is that elective neck dissections might be therapeutic in a larger number of cases than previously thought. Serial sectioning is therefore essential in the processing of a sentinel lymph node [60].
In a study investigating the accuracy of sentinel lymph node biopsies in patients with squamous cell carcinoma, Shoaib [66] identified sentinel lymph nodes in 36 of 40 necks (90%). In four necks, nonsentinel lymph nodes contained tumor in the presence of pathologically positive sentinel lymph nodes. One case demonstrated a nonsentinel lymph node containing tumor, thereby giving the impression of a false-negative neck based on sentinel lymph node biopsies. Werner [67] reported that sentinel lymph node biopsies correctly identified metastatic disease in 97% of their 90 patients with head and neck squamous cell carcinoma. They indicated that if only the lymph node with the highest tracer activity was excised, 39% of cancer-positive necks would not be diagnosed. Payoux et al. [68] examined 30 patients with 37 neck dissections for N0 necks. Preoperative lymphoscintigraphy was performed and sentinel nodes were identified. In 29 necks, the sentinel node and neck dissection were negative for metastatic disease. Lymph node mapping allowed for identification of six of seven positive necks (86%). The authors concluded that lymphoscintigraphic sentinel node detection might have a role in the management of squamous cell carcinoma of the head and neck. The authors recommended that randomized clinical trials be performed before the technique is widely used.
Loree et al. [69] retrospectively analyzed the outcomes of sentinel lymph node biopsies in the management of previously untreated 108 patients with clinically negative necks related to oral squamous cell carcinoma. There were 56 T1, 49 T2, and two T3 tumors studied. The primary anatomic locations were 65 tongue, 7 floor of mouth, 13 buccal mucosa, 1 retromolar trigone, 15 lip, and 7 gingival cancers. The mean number of sentinel lymph nodes harvested per patient was two. Twenty-one patients (18.5%) had disease that was staged as SLN positive, and 82 patients (75.9%) had disease staged as SLN negative. The most common SLN site was ipsilateral level II (61 patients). Ten patients (9.7%) had their SLN identified outside of the boundaries of the supraomohyoid neck dissection . Sixteen patients (76%) with a positive SLN demonstrated lymph node metastases greater than or equal to 2 mm in size. Of these patients, five patients (31%) had additional nodal metastases on subsequent neck dissection. Of the 21 patients with positive SLN, all underwent selective or comprehensive neck dissection, six of whom demonstrated further positive lymph nodes. Eight patients with positive SLN and either further positive lymph nodes, extracapsular extension or vascular invasion or perineural invasion at the primary site underwent chemoradiation therapy in the adjuvant setting. Of the 108 patients studied, 20 (19%) developed local, regional, or distant metastatic disease. Seven recurrences (6%) were nodal recurrences as false-negative SLN. The disease-specific survival (DSS) and disease-free survival (DFS) rates for the 108 patients were 93% and 81%, respectively. The DSS and DFS for patients with positive SNB were 91% and 76%, respectively. The authors concluded their study by indicating that sentinel lymph node biopsies may represent the superior modality for the management of the cN0 neck in oral cavity squamous cell carcinoma.
Conclusion
Significant technical and philosophical refinement has occurred in neck dissections since 1905 in patients with oral/head and neck cancer. These refinements have been described and implemented in the best interests of enhancing the potential cure of these patients while also maintaining the patient’s functional capacity and quality of life. One should anticipate that further developments will occur in this compelling surgical discipline in the future. In the meantime, ablative surgeons must strategically execute surgical treatment for the clinically negative neck with the same degree of enthusiasm as is performed for the clinically positive neck, although clearly with different techniques.
References
Nahmias C, Carlson ER, Duncan L, et al. Positron emission tomography/computerized tomography (PET/CT) scanning for preoperative staging of patients with oral/head and neck cancer. J Oral Maxillofac Surg. 2007;65:2524–35.
Carlson ER, Schaefferkoetter J, Townsend D, et al. The use of multiple time point dynamic positron emission tomography/computed tomography in patients with oral/head and neck cancer does not predictably identify metastatic cervical lymph nodes. J Oral Maxillofac Surg. 2013;71:162–77.
Schaefferkoetter JD, Carlson ER, Heidel RE. Can 3′-deoxy-3′-(18F) fluorothymidine outperform 2-deoxy-2-(18F) fluoro-D-glucose positron emission tomography/computed tomography in the diagnosis of cervical lymphadenopathy in patients with oral/head and neck cancer? J Oral Maxillofac Surg. 2015;73:1420–8.
Weiss MH, Harrison LB, Isaacs RS. Use of decision analysis in planning a management strategy for the stage N0 neck. Arch Otolaryngol Head Neck Surg. 1994;120:699–702.
Carlson ER, Cheung A, Smith BC, Pfohl C. Neck dissections for oral/head and neck cancer 1906–2006. J Oral Maxillofac Surg. 2006;64:4–11.
Carlson ER, Miller I. Management of the neck in oral cancer. Oral Maxillofac Surg Clin North Am. 2006;18:533–46.
Koyfman SA, Ismaila N, Crook D, et al. Management of the neck in squamous cell carcinoma of the oral cavity and oropharynx: ASCO clinical practice guideline. J Clin Oncol. 2019;37:1753–74.
D’Cruz AK, Vaish R, Kapre N. Elective versus therapeutic neck dissection in node-negative oral cancer. N Engl J Med. 2015;373:521–9.
Hamoir M, Holvoet E, Ambroise J, et al. Salvage surgery in recurrent head and neck squamous cell carcinoma: oncologic outcome and predictors of disease free survival. Oral Oncol. 2017;67:1–9.
Chung EJ, Park MW, Kwon KH, Rho YS. Clinical outcomes and prognostic factor analysis after salvage surgery for recurrent squamous cell carcinoma of the oral cavity. Int J Oral Maxillofac Surg 2020;49:285–91. September 4, Epub ahead of print.
Smith GI, O’Brien CJ, Clark J, Shannon KDF, Clifford AR, McNeil EB, et al. Management of the neck in patients with T1 and T2 cancer in the mouth. Br J Oral Maxillofac Surg. 2004;42:494–500.
Shah JP. Head and neck surgery in crisis. Preparing for the future (commentary). Arch Otolaryngol Head Neck Surg. 2005;113:556–60.
Crile G. Excision of cancer of the head and neck – with special reference to the plan of dissection based on one hundred and thirty-two operations. JAMA. 1906;47:1780–6.
Crile GW. On the surgical treatment of cancer of the head and neck. With a summary of one hundred and twenty-one operations performed upon one hundred and five patients. Trans South Surg Gynecol Assoc. 1905;17:108–27.
Ferlito A, Rinaldo A. Errare humanum est, in errore perseverare stultum: this is true also for neck dissection. Oral Oncol. 2005;41:132–4.
Crile GW. Carcinoma of the jaws, tongue, cheek, and lips. Surg Gynecol Obstet. 1923;36:159–62.
Martin H, Del Valle B, Ehrlich H, et al. Neck dissection. Cancer. 1951;4:441–99.
Nahum AM, Mullally W, Marmor L. A syndrome resulting from radical neck dissection. Arch Otolaryngol. 1961;74:82–6.
Short SO, Kaplan JN, Laramore GE, et al. Shoulder pain and function after neck dissection with or without preservation of the spinal accessory nerve. Am J Surg. 1984;148:478–84.
Robbins KT, Medina JE, Wolfe GT, Levine PA, Sessions RB, Pruet CW. Standardizing neck dissection terminology. Official report of the Academy’s Committee for Head and Neck Surgery and Oncology. Arch Otolaryngol Head Neck Surg. 1991;117:601–5.
Robbins KT, Clayman G, Levine PA, Medina J, Sessions R, Shaha A, et al. Neck dissection classification update. Revisions proposed by the American Head and Neck Society and the American Academy of Otolaryngology – Head and Neck Surgery. Arch Otolaryngol Head Neck Surg. 2002;128:751–8.
Medina JE. A rational classification of neck dissections. Otolaryngol Head Neck Surg. 1989;100:169–76.
Myers EN, Fagan JJ. Treatment of the N+ neck in squamous cell carcinoma of the upper aerodigestive tract. Otolaryngol Clin North Am. 1998;31:671–86.
Khafif RA, Gelbfish GA, Asase DK. Modified radical neck dissection in cancer of the mouth, pharynx, and larynx. Head Neck. 1990;12:476–82.
Bocca E, Pignataro O. A conservation technique in radical neck dissection. Ann Otol Rhinol Laryngol. 1967;76:975–87.
Bocca E, Pignataro O, Sasaki CT. Functional neck dissection. A description of operative technique. Arch Otolaryngol. 1980;106:524–7.
Ferlito A, Rinaldo A, Robbins KT, et al. Changing concepts in the surgical management of the cervical node metastasis. Oral Oncol. 2003;39:429–35.
Feldman DE, Applebaum EL. The submandibular triangle in radical neck dissection. Arch Otolaryngol. 1977;103:705–6.
Bocca E, Pignataro O, Oldini C, et al. Functional neck dissection: an evaluation and review of 843 cases. Laryngoscope. 1984;94:942–5.
Calearo CV, Teatini G. Functional neck dissection. Anatomical grounds, surgical technique, clinical observations. Ann Otol Rhinol Laryngol. 1983;92:215–22.
Ariyan S. Functional radical neck dissection. Plast Reconstr Surg. 1980;65:768–76.
Gavilan J, Gavilan C, Herranz J. Functional neck dissection: three decades of controversy. Ann Otol Rhinol Laryngol. 1992;101:339–41.
Persky MS, Lagmay VMP. Treatment of the clinically negative neck in oral squamous cell carcinoma. Laryngoscope. 1999;109:1160–4.
Yuen APW, Lam KY, Chan CL, et al. Clinicopathological analysis of elective neck dissection for N0 neck of early oral tongue carcinoma. Am J Surg. 1999;177:90–2.
Ho CM, Lam KH, Wei WI. Occult lymph node metastasis in small oral tongue cancers. Head Neck. 1992;14:359–63.
Beenken SW, Krontiras H, Maddox WA. T1 and T2 squamous cell carcinoma of the oral tongue: prognostic factors and the role of elective lymph node dissection. Head Neck. 1999;21:124–30.
Henick DH, Silver CE, Heller KS, et al. Supraomohyoid neck dissection as a staging procedure for squamous cell carcinomas of the oral cavity and oropharynx. Head Neck. 1995;17:119–23.
Medina JE, Byers RM. Supraomohyoid neck dissection: rationale, indications, and surgical technique. Head Neck. 1989;11:111–22.
Kligerman J, Lima RA, Soares JR. Supraomohyoid neck dissection in the treatment of T1/T2 squamous cell carcinoma of oral cavity. Am J Surg. 1994;168:391–4.
Kowalski LP, Magrin J, Waksman G, et al. Supraomohyoid neck dissection in the treatment of head and neck tumors. Arch Otolaryngol Head Neck Surg. 1993;119:958–63.
Spiro JD, Spiro RH, Shah JP, et al. Critical assessment of supraomohyoid neck dissection. Am J Surg. 1988;156:286–9.
Jalisi S. Management of the clinically negative neck in early squamous cell carcinoma of the oral cavity. Otolaryngol Clin N Am. 2005;38:37–46.
Shah JP, Candela FC, Poddar AK. The patterns of cervical lymph node metastasis from squamous carcinoma of the oral cavity. Cancer. 1990;66:109–13.
Shah JP, Singh SG. Cervical lymph nodes. In: Head and neck surgery and oncology. 3rd ed. Edinburgh: Elsevier; 2003. p. 353–94.
Crean SJ, Joffman A, Potts J, Fardy MJ. Reduction of occult metastatic disease by extension of the supraomohyoid neck dissection to include level IV. Head Neck. 2003;25:758–62.
Byers RM, Weber RS, Andrews T, McGill D, Kare R, Wolf P. Frequency and therapeutic implications of “skip metastases” in the neck from squamous carcinoma of the oral tongue. Head Neck. 1997;19:14–9.
Feng Z, Li JN, Niu LX, Guo CB. Supraomohyoid neck dissection in the management of oral squamous cell carcinoma: special consideration for skip metastases at level IV or V. J Oral Maxillofac Surg. 2014;72:1203–11.
Manni JJ, van den Hoogen FJA. Supraomohyoid neck dissection with frozen section biopsy as a staging procedure in the clinically node-negative neck in carcinoma of the oral cavity. Am J Surg. 1991;162:373–6.
Van den Hoogen FJA, Manni JJ. Value of the supraomohyoid neck dissection with frozen section analysis as a staging procedure in the clinically negative neck in squamous cell carcinoma of the oral cavity. Eur Arch Otorhinolaryngol. 1992;249:144–8.
Woolgar JA. Pathology of the N0 neck. Br J Oral Maxillofac Surg. 1999;37:205–9.
Muzaffar K. Therapeutic selective neck dissection: a 25-year review. Laryngoscope. 2003;113:1460–5.
Shah JP, Andersen PE. Evolving role of modifications in neck dissection for oral squamous carcinoma. Br J Oral Maxillofac Surg. 1995;33:3–8.
Byers RM. Modified neck dissection. A study of 967 cases from 1970–1980. Am J Surg. 1985;150:414–21.
Snow GB, Annyas AA, Van Slooten EA, et al. Prognostic factors of neck node metastasis. Clin Otolaryngol. 1982;7:185–92.
Anderson PE, Spiro RH, Cambronero E, Shah JP. The role of comprehensive neck dissection with preservation of the spinal accessory nerve in the clinically positive neck. Am J Surg. 1994;168:499–502.
Robbins KT, Samant S. Neck dissection. In: Cummings CW, editor. Cummings otolaryngology head & neck surgery, Chapter 116. 4th ed. Philadelphia: Mosby; 2005. p. 2614–45.
Zhan KY, Morgan PF, Neskey DMP. Preoperative predictors of occult nodal disease in cT1N0 oral cavity squamous cell carcinoma: review of 2623 cases. Head Neck. 2018;40:1967–76.
Brockhoff HC, Kim RY, Braun TM, et al. Correlating the depth of invasion at specific anatomic locations with the risk for regional metastatic disease to lymph nodes in the neck for oral squamous cell carcinoma. Head Neck. 2017;39:974–9.
Kuo P, Mehra S, Sosa JA, et al. Proposing prognostic thresholds for lymph node yield in clinically lymph node-negative and lymph node-positive cancers of the oral cavity. Cancer. 2016;122:3624–31.
Myers EN, Gastman BR. Neck dissection: an operation in evolution. Arch Otolaryngol Head Neck Surg. 2003;129:14–25.
Morton DL, Wen D, Wong JH, Economou JS, Cagle LA, Storm FK, Foshag LJ, Cochran AJ. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg. 1992;127:392–9.
Ambrosch P, Kron M, Pradler O, Steiner W. Efficacy of selective neck dissection: a review of 503 cases of elective and therapeutic treatment of the neck in squamous cell carcinoma of the upper aerodigestive tract. Otolaryngol Head Neck Surg. 2001;124:180–7.
Van den Brekel MWM, van der Wall I, Meijer CJLM, et al. The incidence of micrometastases in neck dissection specimens obtained from elective neck dissections. Laryngoscope. 1996;106:987–91.
Enepekides DJ, Sultanem K, Hguyen C. Occult cervical metastases: immunoperoxidase analysis of the pathologically negative neck. Otolaryngol Head Neck Surg. 1999;120:713–7.
Woolgar JA. Micrometastasis in oral/oropharyngeal squamous cell carcinoma: incidence, histopathological features and clinical implications. Br J Oral Maxillofac Surg. 1999;37:181–6.
Shoaib T, Soutar DS, MacDonald DG, et al. The accuracy of head and neck carcinoma sentinel lymph node biopsy in the clinically N0 neck. Cancer. 2001;91:2077–83.
Werner JA, Dunne AA, Ramaswamy A, et al. The sentinel node concept in head and neck cancer: solution for the controversies in the N0 neck? Head Neck. 2004;26:603–11.
Payoux P, Dekeister C, Lopez R, Lauwers F, Esquerre JP, Paoli JR. Effectiveness of lymphoscintigraphic sentinel node detection for cervical staging of patients with squamous cell carcinoma of the head and neck. J Oral Maxillofac Surg. 2005;63:1091–5.
Loree JT, Popat SR, Burke MS. Sentinel lymph node biopsy for management of the N0 neck in oral cavity squamous cell carcinoma. J Surg Oncol. 2019;120:101–8.
Regezi J, Sciubba J, Jordan RCK, editors. Oral pathology – clinical pathologic correlations, chapter 2. 7th ed. Philadelphia: WB Saunders Co.; 2017. p. 64. Figure 2-80
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Carlson, E.R. (2021). Neck Dissections: History, Classification, and Indications. In: Schlieve, T., Zaid, W. (eds) Complications in Neck Dissection. Springer, Cham. https://doi.org/10.1007/978-3-030-62739-3_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-62739-3_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-62738-6
Online ISBN: 978-3-030-62739-3
eBook Packages: MedicineMedicine (R0)