
Abstract
In healthcare, training is an important mechanism to facilitate organizational change and can be understood using the input-mediator/moderator-output-input (IMOI) model. Using the examples of teamwork training and cultural competency training, we show that training in all its many forms is an input that is intended to influence change in organizations, such as improving team performance or increasing equity in care provision. This occurs by influencing changes in attitudes, behaviors, and cognitions on the job (i.e., mediators), which then result in outcomes for both patients and organizations (e.g., patient safety, worker well-being). In addition, the organization plays a critical support role in its own change process because organizational efforts to support training (e.g., conducting needs analyses, adhering to training best practices, providing resources to support training) serve as moderators of these relationships. Together, such factors feed into continued organizational change efforts (subsequent inputs). We summarize this area of research, presenting key messages about implications and recommendations for practice grounded in these areas, and comment about opportunities for future research.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


1 Introduction
The healthcare industry is evolving rapidly to respond to changing conditions and demands. In order to keep pace, effective organizational change, defined as creating or responding to differences in structures, processes, and roles over time (Martins, 2011), is essential in healthcare. Many of the changes impacting the healthcare industry require clinicians to think and act in new ways. Thus, training is an important way to promote organizational change. In this chapter we will describe the role of training in the context of organizational change, and provide specific examples of teamwork training and cultural competency training. We will describe the outcomes that such training programs can achieve, how they can facilitate organizational change, and how they can impact patient safety and worker wellbeing.
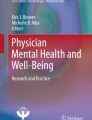
The chapter is framed by the input-mediator/moderator-outcome-input (IMOI) model (modified from Ilgen, Hollenbeck, Johnson, & Jundt, 2005, who put forth the input-mediator-outcome-input model). This model posits that an input (e.g., training) leads to one or more mediators (e.g., changed attitudes, behaviors, and cognitions on the job, also known as transfer of training), that are impacted by moderators (e.g., conducting a training needs analyses, adhering to training best practices, and providing organizational support for training). This should then lead to outcomes (e.g., improved patient safety and worker well-being). Finally, the outcomes, in turn, feed into future inputs (e.g., continued organizational change through subsequent training). Figure 16.1 displays this process in full.

Theoretical model of training in the context of organizational change, following the IMOI model
In the remainder of this chapter, we will discuss each section of this IMOI model in the context of organizational change. First, we will define the input of interest—training—and describe examples of two types of training intended to facilitate change in organizations: teamwork training and cultural competency training. Next, we will discuss the mediators, including learning and changed attitudes, behaviors and cognitions on the job (i.e., transfer of training). We will then discuss outcomes of training, with a particular focus on patient safety and worker wellbeing. Finally, we will discuss moderators in the model that facilitate subsequent training efforts (e.g., refresher training), including adherence to training best practices, organizational support, and the use of a training needs analysis. We conclude with an overall discussion and key messages for research and practice.
2 Input: Training
Broadly defined, training is “the systematic acquisition of attitudes, concepts, knowledge, rules, or skills that result in improved performance at work,” (Goldstein, 1991, p. 508). Training can be provided for task and/or interpersonal skills related to a job, and can take various forms including traditional face-to-face training sessions, online modules (e.g., computer-based learning), or simulation (e.g., role playing, virtual reality). While there are various types of training that can influence organizational change, the current chapter focuses on two specific types that are distinct from each other yet very common in healthcare settings: (a) teamwork training, defined as “a learning strategy in which a learner or group of learners systematically acquire(s) teamwork KSAs [knowledge, skills, and attitudes] to impact cognitions, affect, and behaviors of a team” (Hughes et al., 2016, p. 1267); and (b) cultural competency training, which seeks to improve clinicians’ KSAs around working with patients from different cultures (Gallagher & Polanin, 2015). Cultural competency training is often designed to increase awareness about healthcare disparities, defined as “a particular type of health difference that is closely linked with economic, social, or environmental disadvantage,” (US Department of Health and Human Services, 2010) that are attributed to cultural differences and thereby can be used to address inequities in healthcare.
2.1 Teamwork Training: An Overview
As the number of clinicians and allied health professionals required to care for a single patient increases (e.g., Gawande, 2012), teamwork training is becoming increasingly necessary for organizations to effectively and safely accommodate this change. Teamwork training programs teach clinicians to engage in behaviors such as back-up behavior (e.g., providing task assistance and support), situation assessment, more effective communication, and focused efforts to prevent human error. As a result, teamwork training is associated with improved outcomes for hospitals (e.g., better safety climate, increased patient satisfaction, and lower mortality rates; Hughes et al., 2016). There is also evidence supporting the concept that there is a trickle-down effect such that training leads to learning, which impacts training transfer, and this ultimately yields improved outcomes such as those mentioned previously (Hughes et al., 2016). Popular choices for teamwork training programs in healthcare settings include crew resource management (CRM) and the Agency for Healthcare Research and Quality (AHRQ)’s publicly-available TeamSTEPPS® program (Agency for Healthcare Research and Quality, 2019). One study found that in 2015, over 1.5 million people had been trained on TeamSTEPPS® alone (Global Diffusion of Healthcare Innovation Working Group, 2015).
2.2 Cultural Competency Training: An Overview
In healthcare, implicit bias, defined as “associations outside conscious awareness that lead to a negative evaluation of a person on the basis of irrelevant characteristics such as race or gender” (FitzGerald & Hurst, 2017, p. 19), has been found to be correlated with lower quality of care and disparities in care provision (FitzGerald & Hurst, 2017). This correlation is likely due to the impact that these implicit judgments have on providers’ behaviors towards and treatment decisions about different patients (Drewniak, Krones, Sauer, & Wild, 2016). Through cultural competency training, a type of training designed to reduce implicit bias and increase individuals’ sensitivity to and knowledge about cross-cultural interactions (Betancourt, Green, Carrillo, & Ananeh-Firempong, 2003), the likelihood of these negative evaluations and their subsequent impacts on care quality may be reduced. Cultural competency training can be focused on individual or a combination of economic, social, or environmental factors such as race or ethnicity, religion, socioeconomic status, gender, age, mental health status, disability status, sexual orientation or gender identity. Interventions to improve cultural competency can be delivered at an individual or organizational level, thus the target of such training may be on health care providers, patients, hospitals, communities, or even government agencies (e.g., introduction of new policies; Chin, Walters, Cook, & Huang, 2007). Here we focus specifically on training healthcare workers. In this context, training to increase cultural competency around race and ethnicity in medical student and medical resident curricula has been proposed and implemented (Jacobs, Kohrman, Lemon, & Vickers, 2003; Smith et al., 2007; Vela, Kim, Tang, & Chin, 2008), as well as cultural competency training through continuing education programs for practicing physicians (Like, 2011). While cognitive knowledge and skills training are usually the focus of these curricula, including training focused on developing cultural competency can help to change cultural attitudes among these healthcare workers. For instance, incorporating experiential training such as a poverty simulation can increase awareness of and influence attitudes about socioeconomic disparities for healthcare workers who may need to address socioeconomic factors in providing care to their patients (Nickols & Nielsen, 2011).
3 Mediator: Learning, Changed Attitudes, Behaviors, and Cognitions on the Job
The goal of training is to impart new knowledge, skills, and/or attitudes (KSAs) onto workers (i.e., learning), with the intention that these new KSAs will be utilized by workers on the job (i.e., transfer of training). Outcomes targeted for improvement through training cannot be achieved if (a) the necessary KSAs are not learned in training, or (b) the KSAs are not used back on the job. While learning is a key proximal goal of training, not all training is effective—that is, not all training yields changes in KSAs. Similarly, not all KSAs that are learned are transferred back to the workers’ job environments. We next describe moderators of these relationships.
3.1 Moderator: Adhering to Training Best Practices to Facilitate Learning
There are a number of best practices that should be employed to ensure that training is as effective as possible (Gregory, Feitosa, Driskell, Salas, & Vessey, 2013). As such, adherence to training best practices serves as a moderator, such that the degree to which trainees learn the intended KSAs is driven by the extent to which training is designed and delivered according to recommended practices. Specific best practices regarding instructional design and delivery include: (1) use of multiple delivery methods, including information (e.g., lectures, slides, handouts), demonstration (e.g., videos, in-person skits), and practice (e.g., role plays, simulations) (Salas & Cannon-Bowers, 2001); and, (2) gauging trainees’ understanding and providing timely, specific feedback (both positive and negative) (Kluger & DeNisi, 1996).
3.2 Moderator: Organizational Support for Training Transfer
Another moderator that influences training effectiveness is organizational support. More specifically, the support the organization (including leadership, supervisors, and peers) provides (or does not provide) impacts the extent to which learned KSAs are transferred to and used in the job environment (Baldwin & Ford, 1988). This support comes in multiple forms, including both practical support (e.g., providing resources needed to use what was learned in training such as providing access to an interpreter service after training providers to be sensitive about the needs of non-English speaking patients), and culturally supporting the training in the practice setting (e.g., leaders and supervisors reinforcing the use of trained KSAs through verbal statements and rewards) (Hughes, Zajac, Spencer, & Salas, 2018).
4 Outcomes
While learning and transfer are more proximal outputs of training, the ultimate goal of training is to produce some type of change. In the context of healthcare, training that is intended to produce organizational change may be focused on improving outcomes for employees, and/or improving outcomes for patients. In this section, we will describe how training can positively impact both patient safety (a patient outcome) and worker wellbeing (an employee outcome).
4.1 Patient Safety
Patient safety, defined as “freedom from accidental or preventable injuries produced by medical care” (Agency for Healthcare Research and Quality Patient Safety Network), is one of the six domains of quality defined by the Institute of Medicine (2001). Patient safety incidents are complex and multi-causal; however, frequent contributors include medical error (e.g., diagnostic error), human factors (e.g., lack of attention), teamwork and coordination issues (e.g., miscommunication), environmental and equipment factors (e.g., malfunctions, missing equipment, disruptions), system issues (e.g., understaffing), patient-related issues (e.g., failure to follow medical advice) and training-related issues (e.g., lack of training, failure to recall) (Chaneliere et al., 2018; Joint Commission, 2016). As such, teamwork training designed to target such issues can help to reduce patient safety incidents. For instance, teamwork training (as defined previously, and inclusive of various programs such as TeamSTEPPS®, crew resource management, and Medical Team Training) has been shown meta-analytically to be associated with improved patient safety (Hughes et al., 2016). More specifically, in one study, Morey et al. (2002) implemented a teamwork training program in nine hospitals using a quasi-experimental, untreated control group design and found that clinical errors decreased 30.9% to 4.4% from pre- to post-teamwork training for the experimental group. Similarly, a teamwork training program implemented in a combat support hospital in Iraq was associated with significant reductions in communication-related errors, medication and transfusion errors, and needle stick incidents (Deering et al., 2011). Improved safety is likely due to the content that is taught in such training programs: communication, coordination, and assertiveness—concepts directly related to the contributors to patient safety, as mentioned above.
While evidence suggests a relationship between teamwork training and patient safety, research linking cultural competency training to patient safety outcomes is sparse (Shepherd, 2019). Nonetheless, it is likely that such training would have positive impacts on safety outcomes. For example, a core competency taught in many cultural competency training programs is that of reducing implicit bias. Implicit bias can influence decision making, which is an important precursor to the provision of safe care (Croskerry & Nimmo, 2011). While the link between implicit bias training and patient safety is understudied, research on training to reduce other types of biases (e.g., bias blind spot, confirmation bias, fundamental attribution error) has been shown to be effective in reducing bias in decision-making immediately after training and 2 months post-training for tasks similar to the training scenarios and generalizing to novel tasks that had a different format or context not present in the training (Morewedge et al., 2015). Further, there are theoretical reasons to believe that cultural competency training of healthcare workers can lead to improved patient safety. For instance, an analysis of adverse events across six hospitals compared adverse events for patients fluent in English to patients with low-English proficiency (Divi, Koss, Schmaltz, & Loeb, 2007). When patients with low-English proficiency experience an adverse event, it more often leads to physical harm, and the physical harm experienced is typically more severe. Communication errors contributed to the adverse events experienced by low-English proficiency patients more often than to events experienced by fluent patients, specifically disclosure (i.e., sharing care delivery and outcomes information) and assessment of patient needs. The possibility of harm can be reduced for patients with low-English proficiency when physicians and nurses are trained on how to identify language proficiency issues, to follow guidelines about when to use translation services, and to access and use the special services that are available to patients (Coren, Filipetto, & Weiss, 2009). Further, the type of interpreter used (i.e., professionally trained, paid interpreters, vs. ad hoc family members or hospital staff who speak the patient’s language) has a clear impact on patient safety: professional interpreters are more effective at reducing clinically significant translation problems, compared to ad hoc interpreters (Flores, Abreu, Barone, Bachur, & Lin, 2012). Training for workers on how to use translation services including how to integrate an interpreter into the clinical encounter, or providing workers with experience in clinics serving these populations during medical school can improve patient safety and ultimately reduce disparities in care (Marion, Hildebrandt, Davis, Marín, & Crandall, 2008). In similar work related to cultural competency training, Lewin, Skea, Entwistle, Zwarenstein, and Dick (2001) conducted a systematic review of seventeen studies that trained providers to use more patient-centered communication techniques and concluded that such training programs can, in fact, enhance provider communication skills such that they are more inclusive of patient needs and preferences. This evidence supports the idea that it is possible to train providers to communicate with patients in a way that their unique needs (e.g., cultural needs/preferences) are taken into account, and this can ultimately lead to safer care (Epstein & Street, 2007).
4.2 Worker Wellbeing
Worker wellbeing is a broad concept that includes concepts such as affect, mental health, emotional exhaustion, and satisfaction with work (Wright & Doherty, 1998). Within the scope of worker wellbeing, researchers have examined more specific constructs such as burnout (defined as “a psychological syndrome of emotional exhaustion, depersonalization, and reduced personal accomplishment” at work; Maslach, Jackson, Leiter, Schaufeli, & Schwab, 1986, p. 192), job stress (defined as “a perceived substantial imbalance between demand and response capability, under conditions where failure to meet demands has important perceived consequences;” McGrath, 1970, p. 20), job engagement (defined as “a high level of energy and strong identification with one’s work;” Bakker, Demerouti, & Sanz-Vergel, 2014, p. 391), and job satisfaction (defined as “a positive (or negative) evaluative judgment one makes about one’s job or job situation” (Warr & Nielsen, 2018; Weiss, 2002, p. 6). The job demands-resources model suggests that job demands (e.g., workload, emotional demands) can lead to poor wellbeing outcomes, while job resources (e.g., support, feedback) can improve motivation and other wellbeing outcomes (Bakker & Demerouti, 2017).
With increases in healthcare provider workload attributed to different causes including increased numbers of patient visits (Fu, Schwebel, & Hu, 2018) and consultations (Hobbs, Bankhead, & Mukhtar, 2016), as well as time demands related to the use of electronic health records (Arndt et al., 2017), worker wellbeing is becoming a major global issue in healthcare. Studies have found that almost half of physicians report burnout symptoms (e.g., Shanafelt et al., 2012; Soler et al., 2008), and recent estimates suggest that burnout costs healthcare organizations $7600 per physician per year (Han et al., 2019), or $4.6 billion nationally in the United States. The job demands-resources model (Bakker & Demerouti, 2017) suggests that providing workers with support and resources in their jobs can mitigate some of the negative effects of job demands (e.g., patient workload, electronic health record alerts), and training programs are one way to give workers the capacity to address job demands. For instance, Xanthopoulou et al. (2007) found that offering professional development opportunities to home healthcare workers buffered the negative effects of their job demands. This may be due to the new knowledge and skills built through training and professional development programs that enable workers to more efficiently and effectively complete job tasks. Teamwork training can similarly enhance knowledge and skills to improve efficiency and/or work conditions, and contribute to worker wellbeing. For example, interventions to improve team communication, such as communication between clinicians and staff members, can lead to increased clinician satisfaction (Linzer et al., 2015). Teamwork training programs have additionally been associated with lower turnover for nurses and with less sick leave time for nurse assistants (Meurling, Hedman, Sandahl, Felländer-Tsai, & Wallin, 2013), as well as with increased staff morale (West et al., 2012).
Cultural competency training, as a resource for providers, can also potentially serve to help providers better meet the demands of their jobs, yet studies disagree about the impact of these trainings on worker wellbeing. For instance, in practice, workers may view new training as another job demand. Further, as workers are already experiencing widespread levels of burnout and stress, cultural competency training will increase their awareness about expectations to deliver culturally competent care, but they may not feel appropriately supported to do so, thus adding to their stress and workload (Solberg, 2016). Also, workers may perceive that some factors contributing to care disparities are outside their control (Runyan, 2018); as a result, they may be frustrated and feel “that they cannot provide the good care they wish—and believe is their duty—to give” (Glasberg, Eriksson, & Norberg, 2007). However, in one study where clinicians were trained to increase their awareness about healthcare disparities and the factors that contribute to these disparities, they also learned about available community resources and how to screen patients to identify risk factors associated with these disparities (Tong et al., 2018). Although burnout was not specifically measured, the study found that providers modified the care they delivered based on the screenings and felt this improved their communication with patients. Thus, training that increases provider awareness about how to deliver culturally competent care for their patients may be able to build providers’ skills to address risk factors related to economic, social, or environmental disadvantages, and potentially serve as a job resource to reduce burnout among these workers.
4.3 The Relationship Between Worker Wellbeing and Patient Safety
Research has identified important connections between worker wellbeing and patient safety. Using a longitudinal design, West et al. (2006) sought empirically to examine the directionality of the relationship between wellbeing and patient safety (i.e., does poor worker wellbeing lead to patient safety incidents, or do patient safety incidents lead to poor worker wellbeing?). They found that there was a reciprocal relationship between the two constructs such that being involved in a medical error led to reduced wellbeing, which subsequently led to an increased likelihood of being involved in another medical error. More recently, Tawfik et al. (2018) surveyed 6586 physicians and found that more than 10% of respondents reported a major medical error in the prior 3 months, and these rates were even higher among physicians who had symptoms of burnout (e.g., emotional exhaustion, depersonalization), even after adjusting for personal (e.g., age, sex, relationship status) and practice factors (e.g., specialty, practice setting, hours worked per week). In a meta-analysis of 21 studies linking burnout and patient safety, Panagioti et al. (2018) found that physician burnout was associated with twice the odds of being involved in a patient safety incident. Future work in this area should seek to examine the role training can play, including both training targeted at increasing worker wellbeing and at improving patient safety, as both would likely be beneficial.
4.4 Moderator: Training Needs Analysis
In order for a training program to get the outcomes it intends (including improved patient safety and worker wellbeing), a training needs analysis should be conducted prior to the development of training (Goldstein, 1991). The goal of a training needs analysis is to understand what content should be included in training, who should be trained, when and how training should occur, and the extent to which the organization is ready for and will support training (see Table 16.1). An appropriate training needs analysis can thus facilitate development of an effective training program. In practice, a training needs analysis is often a mixed-methods process that includes surveys and/or interviews and/or observations to understand (1) the organization’s support for training (e.g., understanding what resources they are willing to provide for workers to attend training; the extent to which attending training and using trained KSAs on the job will be rewarded; tangible support such as provision of materials and personnel [e.g., white boards for training on team briefs, interpreters for training on non-English speaking patients, etc.] in order to use trained skills); (2) the job environment and context (e.g., rapid-paced emergency room providing 24/7 staffing vs. rural primary care clinic with more traditional business hours); (3) tasks that workers perform independently, and/or interdependent tasks that team members work together to complete (to help identify where specific needs are for targeting training; e.g., it is not effective to focus training around handoff mnemonics when these are already frequently used); and (4) who the potential trainees are (e.g., perhaps a particular issue is most salient in intensive care, rendering the training of employees in ambulatory and medical-surgical units unnecessary). This process can also be used as an opportunity to increase buy-in from workers for the change that is desired to be achieved via training, and to allow them to help shape the direction of the change program—an approach recommended in contrast to a fully top-down change model (Tams, 2018). While a training needs analysis process should be the first step in developing a training initiative (Goldstein, 1991), its importance becomes evident after training has transferred. For instance, while training transfer may occur (i.e., employees use newly learned KSAs back on the job), this transfer will not yield improved outcomes if the training did not address the KSA needs of those employees (i.e., a needs analysis was not done to understand what training content was needed in order to improve the outcomes an organization wished to change.)
5 Input: Continued Organizational Change
Following the logic of the IMOI framework, the last link of the model in Fig. 16.1 depicts a recursive arrow feeding back to the input of training thus showing that training is not a one-time event. In order to ensure continued attention to organizational change efforts over time, training evaluation should be ongoing to monitor the need for refresher training or for training on new content as new issues and needs arise. This is necessary for multiple reasons including: (1) evidence shows that people do not retain much of the information learned in training over time (Arthur, Bennett, Stanush, & McNelly, 1998); and (2) new workers will continue to join the organization after the training takes place and thus will have not been exposed to it. In addition to providing refresher training, sustainment of trained KSAs on the job can be increased by provision of supervisor, peer, and organizational support (Hughes, Zajac, Woods, & Salas, 2019).
6 Discussion
In this chapter, we discussed the role of training to improve patient safety and worker wellbeing in the context of organizational change. Throughout the chapter we interwove specific examples of two training programs deployed in healthcare settings: teamwork training and cultural competency training. In so doing we reviewed the state of the science in these areas as they relate to our modified IMOI model. Broadly, both teamwork training programs and cultural competency training programs are associated with improvements in worker wellbeing and patient safety. However, while the science on teamwork training is relatively well-developed (e.g., Hughes et al., 2016; Marlow et al., 2017; Weaver, Dy, & Rosen, 2014), the evidence for cultural competency training is more limited with respect to its impact on worker wellbeing and patient safety.
6.1 Future Research
As previously noted, more research is needed to investigate the link between training and worker/patient outcomes. Overall, very few training programs are evaluated at this level; most evaluators collect simple participant reactions (Association for Talent Development, 2009). We noted above the paucity of high-quality evidence linking cultural competency training with improved outcomes. Further, while the science of teamwork training is further developed, only 3% of healthcare teamwork training programs collect data on how the training impacts patient outcomes (Marlow et al., 2017). Future research on training to promote organizational change should assess the impact of training on both organizational (e.g., worker wellbeing) and patient (e.g., patient safety, patient satisfaction) outcomes. At the same time, although evidence linking cultural competency training to improved worker wellbeing is still emerging, it is unknown through what causal pathways (i.e., how) this may occur. More research should be done to investigate the causal mechanisms of these relationships so that future cultural competency training can be designed to achieve positive outcomes.
7 Conclusion
Training can be a key driver to produce organizational change that improves patient safety and worker wellbeing. However, many training programs do not achieve their intended outcomes and are unsuccessful in inducing organizational change (e.g., Vedantam, 2008). For instance, factors such as failure to align the training content with learners’ training needs and desires (Tannenbaum & Yukl, 1992), suboptimal, passive delivery methods (e.g., death by PowerPoint) (Salas & Cannon-Bowers, 2001), failure to align training content with desired outcomes (Salas & Cannon-Bowers, 2001), and lack of organizational and/or supervisor support and resources for using trained KSAs (Rouiller & Goldstein, 1993) can contribute to less successful training efforts. We have presented a modified IMOI model positing that for training to achieve its goals, it must be designed in accordance with training best practices, be supported by the organization, and be grounded in a training needs analysis. As effective training is not a one-time event, it is important for organizations (and supervisors) to continue to support use of the trained KSAs on the job and provide refresher training over time to increase the likelihood that organizational changes to increase patient safety and wellbeing succeed.
7.1 Key Messages for Researchers
-
Investigate the causal pathways that lead from training to improved outcomes; i.e., how does training change knowledge, skills, and attitudes on the job (e.g., via motivation, when effective interactive training methods are used, and when organizations/supervisors are supportive?).
-
Evaluate training programs at multiple levels (e.g., learners’ reactions, learning, transfer of training, outcomes/results): Invest in assessing the impact of training on organizational and patient outcomes.
7.2 Key Messages for Healthcare Delivery
-
Conduct a training needs analysis before designing training in order to tailor training content and methods to the specific needs of the learners.
-
Design training in accordance with training best practices; key tips include using multiple delivery methods (e.g., information, demonstration, practice), providing feedback, and ensuring training is provided when it is needed most.
-
Organizations and supervisors should provide support for the training by providing time to complete training, and resources to support use of trained knowledge, skills, and attitudes on the job.
References
Agency for Healthcare Research and Quality. (2019). TeamSTEPPS 2.0. Retrieved from https://www.ahrq.gov/teamstepps/instructor/index.html
Agency for Healthcare Research and Quality Patient Safety Network. Patient safety. Retrieved from http://psnet.ahrq.gov/glossary.aspx#P
Arndt, B. G., Beasley, J. W., Watkinson, M. D., Temte, J. L., Tuan, W.-J., Sinsky, C. A., et al. (2017). Tethered to the EHR: Primary care physician workload assessment using EHR event log data and time-motion observations. The Annals of Family Medicine, 15(5), 419–426.
Arthur, W., Bennett, W., Stanush, P. L., & McNelly, T. L. (1998). Factors that influence skill decay and retention: A quantitative review and analysis. Human Performance, 11(1), 57–101.
Association for Talent Development. (2009). ASTD: New study shows training evaluation efforts need help. Retrieved from https://www.td.org/insights/astd-new-study-shows-training-evaluation-efforts-need-help
Bakker, A. B., & Demerouti, E. (2017). Job demands–resources theory: Taking stock and looking forward. Journal of Occupational Health Psychology, 22(3), 273–285.
Bakker, A. B., Demerouti, E., & Sanz-Vergel, A. I. (2014). Burnout and work engagement: The JD–R approach. Annual Review of Organizational Psychology and Organizational Behavior, 1(1), 389–411.
Baldwin, T. T., & Ford, J. K. (1988). Transfer of training: A review and directions for future research. Personnel Psychology, 41(1), 63–105.
Betancourt, J. R., Green, A. R., Carrillo, J. E., & Ananeh-Firempong, O. (2003). Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Reports, 118(4), 293–302. https://doi.org/10.1093/phr/118.4.293
Chaneliere, M., Koehler, D., Morlan, T., Berra, J., Colin, C., Dupie, I., et al. (2018). Factors contributing to patient safety incidents in primary care: A descriptive analysis of patient safety incidents in a French study using CADYA (categorization of errors in primary care). BMC Family Practice, 19(1), 121–134. https://doi.org/10.1186/s12875-018-0803-9
Chin, M. H., Walters, A. E., Cook, S. C., & Huang, E. S. (2007). Interventions to reduce racial and ethnic disparities in health care. Medical Care Research and Review, 64(5 Suppl), 7S–28S. https://doi.org/10.1177/1077558707305413
Coren, J. S., Filipetto, F. A., & Weiss, L. B. (2009). Eliminating barriers for patients with limited English proficiency. The Journal of the American Osteopathic Association, 109(12), 634–640.
Croskerry, P., & Nimmo, G. (2011). Better clinical decision making and reducing diagnostic error. The Journal of the Royal College of Physicians of Edinburgh, 41(2), 155–162.
Deering, S., Rosen, M. A., Ludi, V., Munroe, M., Pocrnich, A., Laky, C., et al. (2011). On the front lines of patient safety: Implementation and evaluation of team training in Iraq. The Joint Commission Journal on Quality and Patient Safety, 37(8), 350–356.
Divi, C., Koss, R. G., Schmaltz, S. P., & Loeb, J. M. (2007). Language proficiency and adverse events in US hospitals: A pilot study. International Journal for Quality in Health Care, 19(2), 60–67. https://doi.org/10.1093/intqhc/mzl069
Drewniak, D., Krones, T., Sauer, C., & Wild, V. (2016). The influence of patients’ immigration background and residence permit status on treatment decisions in health care. Results of a factorial survey among general practitioners in Switzerland. Social Science & Medicine, 161, 64–73.
Epstein, R., & Street, R. (2007). Patient-centered communication in cancer care: Promoting healing and reducing suffering. National Cancer Institute; Bethesda. Retrieved from https://cancercontrol.cancer.gov/brp/docs/pcc_monograph.pdf
FitzGerald, C., & Hurst, S. (2017). Implicit bias in healthcare professionals: A systematic review. BMC Medical Ethics, 18(1), 19. https://doi.org/10.1186/s12910-017-0179-8
Flores, G., Abreu, M., Barone, C. P., Bachur, R., & Lin, H. (2012). Errors of medical interpretation and their potential clinical consequences: A comparison of professional versus ad hoc versus no interpreters. Annals of Emergency Medicine, 60(5), 545–553. https://doi.org/10.1016/j.annemergmed.2012.01.025
Fu, Y., Schwebel, D., & Hu, G. (2018). Physicians’ workloads in China: 1998–2016. International Journal of Environmental Research and Public Health, 15(8), 1649.
Gallagher, R. W., & Polanin, J. R. (2015). A meta-analysis of educational interventions designed to enhance cultural competence in professional nurses and nursing students. Nurse Education Today, 35(2), 333–340. https://doi.org/10.1016/j.nedt.2014.10.021
Gawande, A. (2012). Big med. The New Yorker. Retrieved from https://www.newyorker.com/magazine/2012/08/13/big-med
Glasberg, A.-L., Eriksson, S., & Norberg, A. (2007). Burnout and ‘stress of conscience’ among healthcare personnel. Journal of Advanced Nursing, 57(4), 392–403.
Global Diffusion of Healthcare Innovation Working Group. (2015). Global diffusion of healthcare innovation study: Accelerating the journey. Retrieved from http://wish-qatar.org/summit/2015-summit/global-diffusion-of-healthcare-innovation
Goldstein, I. L. (1991). Training in work organizations. In M. D. Dunnette & L. M. Hough (Eds.), Handbook of industrial and organizational psychology (pp. 507–619). Palo Alto, CA: Consulting Psychologists Press.
Gregory, M., Feitosa, J., Driskell, T., Salas, E., & Vessey, W. (2013). Designing, delivering, and evaluating team training in organizations: Principles that work. In Developing and enhancing high-performance teams: Evidence-based practices and advice. San Francisco, CA: Jossey-Bass.
Han, S., Shanafelt, T. D., Sinsky, C. A., Awad, K. M., Dyrbye, L. N., Fiscus, L. C., et al. (2019). Estimating the attributable cost of physician burnout in the United States. Annals of Internal Medicine. https://doi.org/10.7326/M18-1422
Hobbs, F. R., Bankhead, C., & Mukhtar, T. (2016). On behalf of the National Institute for Health Research School for Primary Care Research. Clinical workload in UK primary care: A retrospective analysis of 100 million consultations in England, 2007–14. Lancet, 387(10035), 2323–2330.
Hughes, A. M., Gregory, M. E., Joseph, D. L., Sonesh, S. C., Marlow, S. L., Lacerenza, C. N., et al. (2016). Saving lives: A meta-analysis of team training in healthcare. Journal of Applied Psychology, 101(9), 1266–1304. https://doi.org/10.1037/apl0000120
Hughes, A. M., Zajac, S., Spencer, J. M., & Salas, E. (2018). A checklist for facilitating training transfer in organizations. International Journal of Training and Development, 22(4), 334–345.
Hughes, A. M., Zajac, S., Woods, A. L., & Salas, E. (2019). The role of work environment in training sustainment: A meta-analysis. Human Factors, Online First. https://doi.org/10.1177/0018720819845988
Ilgen, D. R., Hollenbeck, J. R., Johnson, M., & Jundt, D. (2005). Teams in organizations: From input-process-output models to IMOI models. Annual Review of Psychology, 56, 517–543. https://doi.org/10.1146/annurev.psych.56.091103.070250
Institute of Medicine. (2001). Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academy Press.
Jacobs, E. A., Kohrman, C., Lemon, M., & Vickers, D. L. (2003). Teaching physicians-in-training to address racial disparities in health: A hospital-community partnership. Public Health Reports, 118(4), 349–356. https://doi.org/10.1093/phr/118.4.349
Joint Commission. (2016). Sentinel event statistics released for 2015. The Joint Commission Online.
Kluger, A. N., & DeNisi, A. (1996). The effects of feedback interventions on performance: A historical review, a meta-analysis, and a preliminary feedback intervention theory. Psychological Bulletin, 119(2), 254–284.
Lewin, S., Skea, Z., Entwistle, V. A., Zwarenstein, M., & Dick, J. (2001). Interventions for providers to promote a patient-centred approach in clinical consultations. Cochrane Database of Systematic Reviews, 4.
Like, R. C. (2011). Educating clinicians about cultural competence and disparities in health and health care. The Journal of Continuing Education in the Health Professions, 31(3), 196–206. https://doi.org/10.1002/chp.20127
Linzer, M., Poplau, S., Grossman, E., Varkey, A., Yale, S., Williams, E., et al. (2015). A cluster randomized trial of interventions to improve work conditions and clinician burnout in primary care: Results from the Healthy Work Place (HWP) Study. The Journal of General Internal Medicine, 30(8), 1105–1111. https://doi.org/10.1007/s11606-015-3235-4
Marion, G. S., Hildebrandt, C. A., Davis, S. W., Marín, A. J., & Crandall, S. J. (2008). Working effectively with interpreters: A model curriculum for physician assistant students. The Medical Teacher, 30(6), 612–617. https://doi.org/10.1080/01421590801986539
Marlow, S. L., Hughes, A. M., Sonesh, S. C., Gregory, M. E., Lacerenza, C. N., Benishek, L. E., et al. (2017). A systematic review of team training in health care: Ten questions. The Joint Commission Journal on Quality and Patient Safety, 43(4), 197–204. https://doi.org/10.1016/j.jcjq.2016.12.004
Martins, L. L. (2011). Organizational change and development. In S. Zedeck (Ed.), APA handbook of industrial and organizational psychology, Vol 1: Building and developing the organization (Vol. 3, pp. 691–728). Washington, DC: American Psychological Association.
Maslach, C., Jackson, S. E., Leiter, M. P., Schaufeli, W. B., & Schwab, R. L. (1986). Maslach burnout inventory (Vol. 21). Palo Alto, CA: Consulting Psychologists Press.
McGrath, J. E. (1970). A conceptual formulation for research on stress. Social and Psychological Factors in Stress, 10, 21.
Meurling, L., Hedman, L., Sandahl, C., Felländer-Tsai, L., & Wallin, C. J. (2013). Systematic simulation-based team training in a Swedish intensive care unit: A diverse response among critical care professions. BMJ Quality & Safety, 22(6), 485–494. https://doi.org/10.1136/bmjqs-2012-000994
Morewedge, C. K., Yoon, H., Scopelliti, I., Symborski, C. W., Korris, J. H., & Kassam, K. S. (2015). Debiasing decisions: Improved decision making with a single training intervention. Policy Insights from the Behavioral and Brain Sciences, 2(1), 129–140.
Morey, J. C., Simon, R., Jay, G. D., Wears, R. L., Salisbury, M., Dukes, K. A., et al. (2002). Error reduction and performance improvement in the emergency department through formal teamwork training: Evaluation results of the MedTeams project. Health Services Research, 37(6), 1553–1581.
Nickols, S. Y., & Nielsen, R. B. (2011). “So many people are struggling”: Developing social empathy through a poverty simulation. Journal of Poverty, 15(1), 22–42.
Panagioti, M., Geraghty, K., Johnson, J., Zhou, A., Panagopoulou, E., Chew-Graham, C., et al. (2018). Association between physician burnout and patient safety, professionalism, and patient satisfaction: A systematic review and meta-analysis. The Journal of the American Medical Association Internal Medicine, 178(10), 1317–1331.
Rouiller, J. Z., & Goldstein, I. L. (1993). The relationship between organizational transfer climate and positive transfer of training. Human Resource Development Quarterly, 4(4), 377–390.
Runyan, C. N. (2018). Assessing social determinants of health in primary care: Liability or opportunity? Families, Systems, & Health, 36(4), 550–552.
Salas, E., & Cannon-Bowers, J. A. (2001). The science of training: A decade of progress. Annual Review of Psychology, 52, 471–499. https://doi.org/10.1146/annurev.psych.52.1.471
Shanafelt, T. D., Boone, S., Tan, L., Dyrbye, L. N., Sotile, W., Satele, D., et al. (2012). Burnout and satisfaction with work-life balance among US physicians relative to the general US population. Archives of Internal Medicine, 172(18), 1377–1385. https://doi.org/10.1001/archinternmed.2012.3199
Shepherd, S. M. (2019). Cultural awareness workshops: Limitations and practical consequences. BMC Medical Education, 19(1), 14. https://doi.org/10.1186/s12909-018-1450-5
Smith, W. R., Betancourt, J. R., Wynia, M. K., Bussey-Jones, J., Stone, V. E., Phillips, C. O., et al. (2007). Recommendations for teaching about racial and ethnic disparities in health and health care. Annals of Internal Medicine, 147(9), 654–665. https://doi.org/10.7326/0003-4819-147-9-200711060-00010
Solberg, L. I. (2016). Theory vs. practice: Should primary care practice take on social determinants of health now? No. Annals of Family Medicine, 14(2), 102–103. https://doi.org/10.1370/afm.1918
Soler, J. K., Yaman, H., Esteva, M., Dobbs, F., Asenova, R. S., Katić, M., et al. (2008). Burnout in European family doctors: The EGPRN study. Family Practice, 25(4), 245–265.
Tams, C. (2018). Why we need to rethink organizational change management. Forbes. Retrieved from https://www.forbes.com/sites/carstentams/2018/01/26/why-we-need-to-rethink-organizational-change-management/#53923035e93c
Tannenbaum, S. I., & Yukl, G. (1992). Training and development in work organizations. Annual Review of Psychology, 43(1), 399–441.
Tawfik, D. S., Profit, J., Morgenthaler, T. I., Satele, D. V., Sinsky, C. A., Dyrbye, L. N., et al. (2018). Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clinic Proceedings, 93(11), 1571–1580. https://doi.org/10.1016/j.mayocp.2018.05.014
Tong, S. T., Liaw, W. R., Kashiri, P. L., Pecsok, J., Rozman, J., Bazemore, A. W., et al. (2018). Clinician experiences with screening for social needs in primary care. The Journal of the American Board of Family Medicine, 31(3), 351–363. https://doi.org/10.3122/jabfm.2018.03.170419
US Department of Health and Human Services. (2010). Healthy people 2020. Retrieved from https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities
Vedantam, S. (2008). Most diversity training ineffective, study finds. Washington Post. Retrieved from http://www.washingtonpost.com/wp-dyn/content/article/2008/01/19/AR2008011901899.html
Vela, M. B., Kim, K. E., Tang, H., & Chin, M. H. (2008). Innovative health care disparities curriculum for incoming medical students. The Journal of General Internal Medicine, 23(7), 1028–1032. https://doi.org/10.1007/s11606-008-0584-2
Warr, P., & Nielsen, K. (2018). Wellbeing and work performance. In E. Diener, S. Oishi, & L. Tay (Eds.), Handbook of well-being. Salt Lake City, UT: DEF.
Weaver, S. J., Dy, S. M., & Rosen, M. A. (2014). Team-training in healthcare: A narrative synthesis of the literature. BMJ Quality & Safety, 23(5), 359–372. https://doi.org/10.1136/bmjqs-2013-001848
Weiss, H. M. (2002). Deconstructing job satisfaction: Separating evaluations, beliefs and affective experiences. Human Resource Management Review, 12(2), 173–194.
West, C. P., Huschka, M. M., Novotny, P. J., Sloan, J. A., Kolars, J. C., Habermann, T. M., et al. (2006). Association of perceived medical errors with resident distress and empathy: A prospective longitudinal study. The Journal of the American Medical Association, 296(9), 1071–1078.
West, P., Sculli, G., Fore, A., Okam, N., Dunlap, C., Neily, J., et al. (2012). Improving patient safety and optimizing nursing teamwork using crew resource management techniques. The Journal of Nursing Administration, 42(1), 15–20. https://doi.org/10.1097/NNA.0b013e31823c17c7
Wright, T. A., & Doherty, E. M. (1998). Organizational behavior ‘rediscovers’ the role of emotional well-being. Journal of Organizational Behavior, 19(5), 481–485.
Xanthopoulou, D., Bakker, A. B., Dollard, M. F., Demerouti, E., Schaufeli, W. B., Taris, T. W., et al. (2007). When do job demands particularly predict burnout? The moderating role of job resources. Journal of Managerial Psychology, 22(8), 766–786.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gregory, M.E., Rothwell, C.D., McAlearney, A.S. (2020). Training as a Facilitator of Organizational Change in Health Care: The Input-Mediator/Moderator-Outcome-Input Model. In: Montgomery, A., van der Doef, M., Panagopoulou, E., Leiter, M.P. (eds) Connecting Healthcare Worker Well-Being, Patient Safety and Organisational Change. Aligning Perspectives on Health, Safety and Well-Being. Springer, Cham. https://doi.org/10.1007/978-3-030-60998-6_16
Download citation
DOI: https://doi.org/10.1007/978-3-030-60998-6_16
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-60997-9
Online ISBN: 978-3-030-60998-6
eBook Packages: Behavioral Science and PsychologyBehavioral Science and Psychology (R0)