
Abstract
On January 12, 2010, a magnitude 7.0 earthquake struck Haiti 25 km west of Port-au-Prince. The event was catastrophic, killing 200,000 people and displacing more than a million others. Ten months later, a cholera outbreak was confirmed on the island nation for the first time in more than 100 years. Early emergency responses included treatment of those infected with hydration and antibiotics, improvements in sanitation, training of health-care workers, public education, and improved surveillance. Despite these efforts, cases continued to rise. The outbreak grew to one of the worst cholera epidemics in recent history, causing 665,000 cases and 8183 deaths. In response, mass immunization campaigns with cholera vaccine were launched. Disease transmission became less efficient, and the number of new cases week to week began to slow. Field studies estimated vaccine effectiveness at 97.5%. Cholera remains endemic to Haiti, fueled by the high rates of poverty, crowded living conditions, and incomplete recovery from infrastructure that was decimated a decade ago. Vigilance, outbreak surveillance, improvements in infrastructure, more reliable access to clean water, and cholera vaccine campaigns are key components to preventing future large epidemics.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Cholera
- Vibrio cholerae
- Rice water diarrhea
- Live attenuated bacterial vaccine
- Oral rehydration solution
Cholera
Etiology
Cholera is a small intestinal infection caused by certain toxin-producing strains of the Gram-negative bacillus, Vibrio cholerae . The organism is a facultative anaerobe with a single unipolar flagellum that occurs in both freshwater and marine habitats where they attach themselves to the chitin-containing exoskeletons of crabs, shrimp, and other shellfish. Cholera occurs when toxigenic strains of V. cholerae are ingested, colonize the small intestine, and begin to express the 2-subunit cholera toxin cyxA/cyxB. The toxin stimulates the movement of fluid and electrolytes across the epithelium into the intestinal lumen, causing profuse watery diarrhea . Cholera is endemic in areas with poor sanitation where sporadic cases can quickly lead to epidemics. Disease is uncommon in developed countries, where occasional small outbreaks are easily controlled.
Many serogroups of V. cholerae have been identified, but only serogroups O1 and O139 cause cholera epidemics. Before 1992, when serogroup O139 was first identified in Bangladesh as the cause of a regional outbreak, serogroup O1 was the only pathogen known to cause cholera. V. cholerae serogroup O1 continues to be responsible for nearly all cholera outbreaks and epidemics globally. Sporadic cases of infections caused by serogroup O139 continue to be reported from Asia, with only rare reports from other areas of the world. During cholera epidemics, both disease incidence and mortality are highest among children younger than 5 years of age.
Epidemiology of Cholera
Globally, cholera epidemics are caused by toxigenic strains of Vibrio cholerae serogroup O1. Outbreaks and sporadic cases caused by serogroup O139, first identified from Bangladesh, have not spread outside of Asia. The World Health Organization has identified cholera as pandemic in Africa, Asia, and Latin America for more than 50 years. Sub-Saharan Africa carries the greatest global burden accounting for 60% of the world’s nearly 12 million cases between the years of 2008 and 2012. Southeast Asia carries the second highest burden globally, accounting for 30% of cases. In 2017, case fatality rates were highest in the African nations of Chad (6.8%), Angola (5.2%), and Zambia (3.2%). Densely populated areas of the Indian subcontinent, especially across India and Bangladesh, are home to the world’s greatest numbers of individuals at risk for developing cholera. Outbreaks and epidemics of cholera are indicators of inadequate access to clean water and sanitation and a general lack of social development. Globally, 2.4 billion people live in unsanitary conditions, 2 billion use water sources that are contaminated with human and animal waste, and 950 million practice open defecation due to the lack of toilets or latrines. The highest risk areas for cholera outbreaks include urban slums and camps for displaced persons or refugees. Of the estimated 1.3–4 million people infected with cholera each year worldwide, between 21,000 and 143,000 die. In 2017, 34 countries reported cases of cholera to the WHO, but a single large epidemic in Yemen, related to civil unrest, conditions of war, and ongoing conflicts with neighboring countries, was responsible for causing 84% of all cases and 41% of deaths worldwide that year.
Global Cholera Pandemics 1 Through 7
Cholera is one of the oldest known diseases with potential to cause pandemics. Cholera-like illnesses are described in ancient writings from India and Greece dating back as early as the fifth century BC. Throughout recorded history, endemic cholera is described from areas of the Ganges and Brahmaputra river deltas in Eastern India and Bangladesh.
The first pandemic to be described began in 1817 at the Ganges River delta, then spread via trade routes, across Asia to the Persian Gulf, and throughout Southern Europe over a 6-year period, ending in 1823. The world’s second pandemic endured much longer, again originating in India from the delta of the Ganges River. From 1829 to 1851, cholera spread throughout Asia to the Middle East, and for the first time crossed the Atlantic spreading to North America and Latin America. The third global pandemic proved to be the deadliest to date. Its origin was again traced to India, this time spreading through Europe, including Great Britain where the infection killed more than 23,000 people. In 1854, British physician John Snow carefully mapped out cases of cholera that were occurring in a London neighborhood, subsequently identifying contaminated water from the public well on Broad Street as the source of the outbreak. Global pandemics 4 (1863–1875), 5 (1881–1896), and 6 (1899–1923) also had their origins in India. Robert Koch first isolated the bacterium in culture in 1883, during the fifth pandemic.
More than a half million people died from cholera in India alone between 1918 and 1919. The world’s seventh and current cholera pandemic , caused by V. cholerae O1 El Tor biotype, began in 1961. Its origin was in Indonesia, not India. After spreading through Asia, the pandemic reached Africa, the Middle East, southern Europe, and the former USSR in 1971. Punctuated by periods of emergence and re-emergence, the O1 El Tor biotype was first identified in Latin America in 1991.
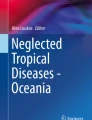
The global burden from cholera during 2018 is shown in Fig. 8.1. During 2018, outbreaks continued throughout much of Africa where 16 nations reported a total of 120,000 cases to the WHO. Nigeria, Zimbabwe, and the Democratic Republic of the Congo were disproportionately affected. An epidemic in Yemen that began in late 2016, fueled by ongoing conflict with Saudi Arabia, civil war, famine, and lack of access to clean water and basic health care, saw an additional 370,000 cases of cholera in 2018 alone. Cholera in the Western Hemisphere paled in comparison during 2018, but notable for the 3777 cases reported from Haiti where thousands of cases continue to be reported annually since 2010. In stark contrast, 3 sporadic cases of cholera were reported in 2018 from Vancouver, Canada. The infections were acquired locally following the consumption of herring eggs collected in a nearby creek. Disease did not spread beyond the 3 primary cases.

Global burden of cholera 2018. Shown is a world map indicating the total numbers of cholera cases reported during 2018 by country. Note that “0” is used to indicate either that no cases were reported (no report submitted), or that 0 cases were reported. (Source of data used to generate the original figure: https://www.who.int/immunization/diseases/typhoid/en/)
Cholera in the USA
During the early and mid-1800s, cholera was endemic to the USA . By the mid-1800s, the introduction of modern water and sewage treatment systems had virtually eliminated the spread of disease via contaminated water. Reports of sporadic cases tapered quickly. Currently, with one exception, fewer than 20 cases per year are reported. Identified cases over the past six decades are usually in travelers returning from areas where disease remains endemic, or from the ingestion of raw or undercooked seafood from the Gulf Coast. At-risk individuals include health-care workers who treat cholera patients, mission response workers in areas where cholera has been identified, and travelers to endemic regions who do not practice safe food and water precautions.
In 1989, the US Centers for Disease Control and Prevention started COVIS, a Cholera and Other Vibrio Illness Surveillance program , in close collaboration with the FDA and the Gulf Coast states of Alabama, Florida, Louisiana, and Texas. From 1989 to 2006, only infections shown to be caused by toxigenic V. cholerae serogroup O1 or O139 were nationally notifiable. In 2007, surveillance expanded to include all infections caused by members of the Vibrionaceae family. Such infections are classified as vibrioses to distinguish them from cholera. Between 2010 and 2014, 96 cases of cholera were reported in the USA through COVIS. The majority of cases were associated with travel to endemic regions and/or consumption of seafood. The higher than expected numbers during this period of time were caused, at least in part, by the close proximity of the USA to Haiti where cholera had become epidemic following the earthquake of 2010. Of the 96 cases of cholera reported to COVIS in the USA, between 2010 and 2014, 64 (67%) had a history of recent travel to Haiti or the Dominican Republic. Given the magnitude of the epidemic in Haiti, and the close geographic proximity between Haiti and the US A, it is surprising that more cases have not spread to the USA.
Transmission
Fresh, brackish, and marine waters are the natural environment for Vibrio cholerae where the organism closely associates itself with crustaceans and mollusks. Infection is transmitted through ingestion of contaminated food or water via the fecal-oral route , often where sanitation practices are poor. The majority of individuals who become infected with V. cholerae do not develop symptoms, but still shed bacteria in their stool for as long as 10 days. Crowded living conditions , especially those with poor sanitation, facilitate spread. Bacteria closely associate with zooplankton and chitin-containing shells of crustaceans (crabs, shrimps, lobsters) and molluscs (clams, oysters) shellfish, explaining why individuals who consume raw or undercooked seafood have an increased risk for infection.
Clinical Presentation
The clinical presentation of cholera ranges from asymptomatic infection with shedding to life-threatening, rapidly progressive secretory diarrhea. Approximately 10% of those infected develop severe manifestations of disease. Severe infection is characterized by profuse watery diarrhea with very frequent, large volume rice-water stools with or without vomiting. Fever is usually absent. Untreated, between 25 and 50% of those with severe disease develop complications that may include severe electrolyte imbalances, renal failure, hypovolemic shock, circulatory collapse, and death. Young children, pregnant women, and their fetuses are at highest risk for mortality.
Following exposure, the median incubation period is 1.4 days with a range between 8 hours and 5 days. Re-exposure can lead to reinfection, but the infection is not associated with the development of a carrier state.
Management
Rehydration is paramount. The most severe cases require rapid treatment with intravenous fluids and antibiotics . Mild-to-moderate, and some severe, infections are managed successfully with oral rehydration solution supplemented with intravenous fluids with electrolytes as needed. With fluid and electrolyte support and replacement, rapid recovery is expected without long-term sequelae. Zinc therapy for children under 5 years of age reduces the duration of the illness. Antibiotics should be used in combination with hydration therapy . When choosing an antibiotic, it is important to consider local antibiotic susceptibility patterns, because antimicrobial resistance is becoming more common. In most circumstances, the first-line antibiotic options are doxycycline for adults and azithromycin for children and pregnant women . The use of antibiotic prophylaxis is generally discouraged during outbreaks. Prevention of spread requires careful attention to toileting practices and personal hygiene.
Cholera Vaccine
WHO-qualified cholera vaccines include the brand names Dukoral (SBL Vaccin AB), Shanchol (Biotechnics Limited), Euvichol-Plus (Eubiologics), and Vaxchora (PaxVax Bermuda Ltd). Vaxchora is the only cholera vaccine available for use in the USA where it was approved for use by the FDA on June 10, 2016. It is licensed for use as an orally administered active immunization against Vibrio cholerae serogroup O1. The recipient should avoid eating or drinking for 60 minutes before and after ingesting the vaccine. Each dose is supplied as 2 components. Packet 1 contains a vaccine buffer and packet 2 contains the live attenuated bacteria. Both components should be stored at 2 °C to 8°, protected from light and moisture. Prior to administration, the vaccine must be reconstituted. Using a clean disposable cup, 100 mL cold water is added to the contents of the buffer packet. Effervescence will occur. The buffer solution is stirred until completely dissolved. Next, the contents of packet 2, containing the lyophilized attenuated bacteria, are added to the buffer solution, and stirred for a minimum of 30 seconds. The final suspension is slightly cloudy and may contain white particulates. The entire 100 mL volume should be consumed within 15 minutes of reconstitution. The vaccine is licensed for use as a single dose in adults to be administered at least 10 days prior to potential exposure. Booster doses are not recommended. Vaccine strain , live attenuated bacteria are shed in stools of recipients for at least 7 days.
Immunizing Antigen
The immunizing antigen included in cholera vaccine is a live attenuated serogroup O1 classical Inaba strain of V. cholerae. Attenuation was achieved by deleting the catalytic domain sequence of both copies of the ctxA toxin gene, thereby preventing the synthesis of active cholera toxin. The immunogenic nontoxic B subunit of cholera toxin encoded by ctxB is unaltered. For epidemiologic purposes, a marker has been inserted into the hemolysin gene locus (hlyA) to facilitate the differentiation between vaccine strain and wild type V. cholerae in the laboratory.
The attenuated bacteria are grown in fermenters in a culture medium containing casamino acids, yeast extract, mineral salts, and an antifoaming agent. Bacteria are then collected by filtration, diafiltered, and concentrated. The formulation is stabilized using a solution containing the antioxidant ascorbic acid, and 2 cryoprotectants: hydrolyzed casein and sucrose. The bacteria are lyophilized, milled, and blended with dried lactose as a desiccant and bulking agent. The vaccine buffer component consists of sodium bicarbonate to neutralize gastric acid, sodium carbonate, ascorbic acid, and dried lactose.
Additives and Excipients
The final formulation of cholera vaccine contains no more than 8.6 mg ascorbic acid, 17.1 mg hydrolyzed casein, 165 mg sucrose, 2 g dried lactose, 2.4 g sodium bicarbonate, and 0.5 g sodium carbonate per dose. It is preservative-free.
Vaccine Recommendations
A single, one-time dose of cholera vaccine is recommended for adults 18 to 64 years of age who will be traveling to an area with any cholera activity reported within the last year unless otherwise contraindicated. Vaccination is not required as a condition for entry into any country or region.
Contraindications to Vaccine
Cholera vaccine is contraindicated in those individuals who developed a life-threatening allergic reaction to a previous dose, and those with a known severe allergy to any vaccine component. Individuals with a moderate or severe acute illness should postpone immunization until they recover.
Warnings and Precautions for Vaccine Use
Cholera vaccine should not be administered to individuals who are currently being treated with or were treated with systemic antibiotics in the last 14 days. If needed for malaria prophylaxis, treatment with chloroquine should not be started until at least 10 days after cholera vaccination. Vaccine strain bacteria are shed in feces for at least 7 days after receipt, indicating the potential for transmission to nonvaccinated close contacts. Attention to proper hand washing, especially after bathroom use and during food handling, is important to prevent transmission to others. Safety and effectiveness have not been established in immunocompromised people, and careful consideration should be given when administering vaccine to individuals with immunocompromised close contacts.
Side Effects and Adverse Events
Cholera vaccine is well tolerated. When side effects occur, the vast majority are mild and self-limiting, resolving within a few days. In clinical trials, the most common AEs (incidence >3%) occurring within 7 days of vaccination included fatigue (31%), headache (29%), abdominal pain (19%), nausea/vomiting (18%), decreased appetite (17%), and diarrhea (4%). Pooled analyses of results from 4 randomized, controlled clinical trials indicated that the overall rate of severe adverse events was 0.6% in vaccine recipients and 0.5% in control groups. None of the serious adverse events were considered to be related to the vaccination.
Estimated Effectiveness or Efficacy from Clinical Vaccine Trials
A placebo-controlled efficacy trial of cholera vaccine that included 197 healthy adult volunteers showed 90.3% efficacy at 10 days post vaccination, and 79.5% efficacy at 3 months post vaccination. An immunogenicity trial in US and Australian adult volunteers showed that 93.5% of all vaccine recipients developed protective antibody responses.
Impact of Vaccine on Disease Burden
Mathematical modeling suggests that maintaining community immunization rates of 70% or higher among residents of Bangladesh 1 year of age and older is sufficient to interrupt cholera transmission. Since the creation of a global oral cholera vaccine stockpile in 2013, more than 50 million doses have been used in mass vaccination campaigns in efforts to interrupt transmission during outbreaks. Between 2014 and 2017, 18 million doses of vaccine were shipped to 15 countries including Cameroon, Democratic Republic of the Congo, Ethiopia, Guinea, Haiti, Iraq, Malawi, Mozambique, Nepal, Niger, Somalia, South Sudan, Sudan, Tanzania, and Zambia. The rationale for distribution included humanitarian crises (37%), outbreak control (36%), and ongoing endemic disease (27%). Targeted shipments to the most affected regions of Africa continued through 2018 and 2019.
Civil war and ongoing conflict with neighboring Saudi Arabia quickly escalated to a massive humanitarian crisis in the Middle Eastern country of Yemen. The associated unsanitary and crowded living conditions , famine, and malnutrition incited the largest and fastest spreading cholera outbreak in recorded history. From late 2016 to the end of 2019, nearly 2.5 million cases and 4000 deaths have occurred in Yemen. Approximately 25% of those affected are children under 5 years of age. During early October 2018, a pause in fighting, known as the “Days of Tranquility,” allowed the opportunity for public health workers to vaccinate more than 300,000 individuals, including 164,000 children. The campaign was life-saving for many, but the benefits will be short-lived unless or until the root cause of the massive crisis can be solved.
References and Suggested Readings
Contagion live: https://www.contagionlive.com/outbreak-monitor?z=no&type=sub&category=cholera.
Deen J, Mengel MA, Clemens JD. Epidemiology of cholera. Vaccine. 2019; https://doi.org/10.1016/j.vaccine.2019.07.078.
Desai SN, Pezzoli L, Alberti KP, et al. Achievements and challenges for the use of killed oral cholera vaccines in the global stockpile era. Hum Vacc Immunother. 2017;13:579–87.
Frozen formulation: https://www.fda.gov/media/98688/download.
Hsiao A, Desai SN, Mogasale V, Excler JL, Digilio. Lessons learnt from 12 oral cholera vaccine campaigns in resource-poor settings. Bull World Health Organ. 2017;95:303–12.
Islam MT, Chowdhury F, Qadri F, et al. Trials of the killed oral cholera vaccine in India and Bangladesh: lessons learned and way forward. Vaccine. https://doi.org/10.1016/j.vaccine.2019.06.082.
Refrigerated formulation: https://www.fda.gov/media/128415/download.
Severe K, Rouzier V, Anglade SB, et al. Effectiveness of oral cholera vaccine in Haiti: 37-month follow-up. Am J Trop Med Hyg. 2016;94:1136–42.
U.S. Centers for Disease Control and Prevention: https://www.cdc.gov/cholera/index.html.
Vaccine Information Sheet: https://www.cdc.gov/vaccines/hcp/vis/vis-statements/cholera.html.
Vaxchora package inserts.
Weil AA, Ryan ET. Cholera: Recent updates. Curr Opin Infect Dis. 2018;31:455–61.
Wierzba TF. Oral cholera vaccines and their impact on the global burden of disease. Hum Vaccin Immunother. 2019;15:1294–301.
World Health Organization: https://www.who.int/health-topics/cholera#tab=overview. https://www.who.int/topics/cholera/impact/en/.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bonville, C., Domachowske, J. (2021). Cholera. In: Domachowske, J., Suryadevara, M. (eds) Vaccines. Springer, Cham. https://doi.org/10.1007/978-3-030-58414-6_8
Download citation
DOI: https://doi.org/10.1007/978-3-030-58414-6_8
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-58413-9
Online ISBN: 978-3-030-58414-6
eBook Packages: MedicineMedicine (R0)