
Abstract
Additive manufacturing or 3D printing, otherwise known as rapid prototyping (RP), originally developed in the late 1980s as a technique for manufacturing engineering, has evolved rapidly over the years to create a niche in the field of biomedical engineering. From the manufacturing of medical devices to customized micro-architectural implants, the manufacturing flexibility and capabilities of AM systems make it one of the most favorable systems for such biomedical applications.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
19.1 Introduction
Additive manufacturing (AM) or 3D printing, otherwise known as rapid prototyping (RP) , originally developed in the late 1980s as a technique for manufacturing engineering, has evolved rapidly over the years to create a niche in the field of biomedical engineering. From the manufacturing of medical devices to customized micro-architectural implants, the manufacturing flexibility and capabilities of AM systems make it one of the most favorable systems for such biomedical applications.
AM technology made its debut in the market during the late 1980s with the introduction of the stereolithography system (SLA-1) by 3D Systems Inc. (Valencia, CA). As opposed to conventional fabrication processes which involve the subtraction or removal of materials from stock (e.g., conventional machining) and casting or molding (e.g., investment casting, injection molding, etc.), all AM techniques are material addition processes which employ a similar fabrication concept of layer-by-layer additive building to produce three-dimensional physical parts from wood, plastics, metals, and ceramics. AM fabrication starts with the creation of a three-dimensional volumetric computer model of the desired part that can be derived from output data generated by surface digitizers or medical imaging systems (e.g., computed tomography (CT) or magnetic resonance imaging (MRI)). The digital model is then computationally sliced into thin layers having a constant thickness that is user-defined. Using AM fabrication, layers of material representing the cross-sectional profiles of the desired part as obtained from the computer-generated slices are formed by processing solid sheet, liquid, or powder material feedstocks. The material layers are automatically and precisely stacked and fused on top of one another to create the desired physical part. Detailed descriptions of the principles and operations of the various AM techniques can be found in existing text [1].
This chapter aims at providing readers with an overview into the biomedical applications of AM. It would be divided into two main sections: (1) tissue engineering scaffolds and (2) prostheses.
19.2 Biomedical Applications of AM-Tissue Engineering Scaffolds
Human has always been intrigued by the possibility of being able to grow new, fully functional tissues and organs to replace damaged, injured, or worn parts of the human body. It is not until recently that such an aspiration is considered mere science fiction when the emergence of tissue engineering (TE) has turned this “aspiration” into medical reality [2,3,4,5]. The vast interest generated among clinicians as well as engineers seeking biologic replacements to treat malfunctioned human tissues and organs rapidly and effectively is incited by the immense potential and promise to overcome the severe shortage of donor organs and the limitations of alternative short-term therapies including drug, mechanical prosthetics, etc. [6]. The scarcity of donor organs [7, 8] has created huge demands for laboratory-produced biologic alternatives and, hence, paved the way for unprecedented growth and advances in TE research and applications.
Scaffold-guided TE is a major TE strategy or approach that is attracting wide interest and research effort from the scientific community. Scaffold-guided TE can facilitate the extensive building and growth of cell masses in three-dimensional forms to achieve successful cell transplantation of either hard (e.g., bone and cartilage) [9, 10] or soft (e.g., liver and blood vessels) [11, 12] tissues and organs. Using this approach, progenitor cells are harvested from the patient or a donor and expanded in population through cell culture systems [13]. Once sufficient quantities of cells are obtained, they are seeded directly onto scaffolds that would allow the cells to attach and proliferate. The cell-seeded scaffolds are subjected to an additional period of in vitro culturing in an environment (e.g., bioreactors [14, 15]) which mimics the biochemical and physical signals that regulate in vivo tissue development, to allow full colonization of the scaffold in order to achieve homogeneous and healthy tissue regeneration.
This section focuses on the application of AM for creating such TE scaffolds. The main objectives are to compile the information available to date on the characteristics, parameters, and applications or potential applications of these new and novel AM fabrication techniques for scaffold creation and to highlight their advantages as well as their limitations. The characteristics of the AM-fabricated scaffolds are assessed and compared. Research to develop CAD strategies to be applied in conjunction with AM to design, customize, and control the internal architectures of the scaffolds is also described. It is the authors’ aim to provide the TE community the essential information on the critical parameters and factors that are to be considered in choosing the appropriate automated fabrication techniques for specific TE applications.
19.3 Roles and Prerequisites for Tissue Engineering Scaffolds
In scaffold-guided TE, the scaffolds serve as temporary surrogates for the native extracellular matrix (ECM) that mechanically supports cellular anchorage and reorganization of cells in three dimensions and maintains differentiated phenotypes and tissue-specific functions once implanted. Scaffolds for TE applications must be produced from scaffolding materials that exhibit good biocompatibility and as such are limited to materials that are non-mutagenic, nonantigenic, noncarcinogenic, nontoxic, and non-teratogenic. To date, a variety of natural biological substances (e.g., collagens, chitosan, fibrin, etc.) [16, 17] have been used as scaffolding materials with promising results. The need for large quantities of scaffolding materials to cater for clinical applications as well as assurance of pathogen removal [18, 19] has led to the investigations and inclusions of synthetic biocompatible polymers (e.g., poly(glycolic acid), poly(l-lactic acid), etc.), copolymers (e.g., poly(dl-lactic-co-glycolic acid)) [20,21,22], and bioceramics (e.g., hydroxyapatite, tricalcium phosphate) [23, 24] as scaffolding materials. Besides being formed from a suitable biomaterial, the scaffolds must possess appropriate three-dimensional forms that are spatially and anatomically consistent with the defect and micro-architectural properties [25, 26] that will support tissue regeneration. The scaffold’s micro-architecture affects not only cell survival, signaling, growth, propagation, and reorganization but also plays major roles in influencing cell shape modeling and gene expressions that relate to cell growth and the preservation of native phenotypes [27, 28]. In order for a scaffold to be effective in its intended TE application, the scaffold must possess a large surface area to volume ratio to achieve high yields of attached cells [29]. It must also have a highly porous microstructure (>90% porosity [30,31,32]) with interconnected porous networks that will allow the in-growth of cells and provide uninhibited diffusion pathways to facilitate nutrient, gas, and waste exchange with cells that have penetrated into the scaffold. In these porous constructions, the pore sizes must be large enough so that the cells can penetrate and grow within the pores without occluding the pore spaces [33, 34]. Besides architectural designs, scaffolds fashioned from degradable biomaterials must be tailored such that sufficient mechanical strengths and properties are preserved in the degrading construct to maintain the pore spaces for the in-growth of cells and to support early mobilization of the implant site.
19.4 Conventional Manual-Based Scaffold Fabrication Techniques
A wide variety of manual-based fabrication methods and techniques are available that can be used to transform the biomaterials into scaffold structures [18, 35,36,37,38]. These manual-based techniques include fiber bonding [39], phase separation [40, 41], solvent casting with particulate leaching [42], membrane lamination [43, 44], melt molding [45], gas foaming with high-pressure processing [46, 47], hydrocarbon templating [48], freeze drying [49, 50], and combinations of these techniques (e.g., gas foaming with particulate leaching [51], etc.). As different cell types require different sets of structural requirements, the fabrication techniques mentioned have been tailored to produce scaffolds with their particular and optimized characteristics for specific TE applications. As such, none of the techniques is sufficiently generic to be suitable for all TE applications. Although most of these techniques have been used in preliminary investigations for engineering a variety of tissues with varying degrees of success, most carry some forms of imperfection that restrict the scope of their applications. The extensive use of porogens and toxic solvents in most of these techniques results in adverse drawbacks due to the risk of inadvertent residual solvents and porogen entrapped in the polymer matrix. Another highly detrimental weakness in manual-based techniques is their high dependency and sensitivity to manual skills, experiences, and procedures, often resulting in poor consistency and poor repeatability. Other factors such as high labor involvement, lengthy processing time, and poor flexibility to produce complex macro-architectures lead to increased production costs. The processing procedures, advantages, and limitations of the various manual-based conventional fabrication techniques can be found in several published reviews [35,36,37,38].
19.5 Computer-Controlled AM Techniques for Tissue Engineering Scaffolds
Although immense research efforts have been placed in developing new biocompatible scaffolding materials and processing techniques for converting such materials into useful scaffold structures, relatively little work had been carried out towards the development of rapid and automated procedures for designing and producing TE scaffolds. Recently, a group of computer-controlled fabrication techniques, namely, AM techniques, have been identified and recognized to possess significant potentials for TE scaffold fabrication. The manufacturing flexibility and fabrication capabilities of AM systems permit complex irregular three-dimensional scaffold geometries with designed or customized internal micro-architectures to be fabricated. Such capabilities are highly advantageous since the ideal scaffold should replicate the geometry and size of the patient’s original anatomy and its internal micro-architecture should support cell proliferation and spreading. The fact that each tissue and organ in the human body has their own unique geometry that varies in size between individuals undermines the applicability of most conventional fabrication techniques that are restricted to the fabrication of scaffolds with highly simplified geometries. Although the application of AM for the production of TE scaffolds is still very much in the laboratories, the vast amounts of interest generated by AM for TE scaffold fabrication are demonstrated by the number of publications generated over the last 5 years [52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72]. Research conducted with existing commercial and noncommercial AM systems has laid down a firm foundation in generating scaffolds with unprecedented quality, accuracy, and reproducibility and is fast in establishing AM as a fabrication method of choice in TE scaffold production.
To date, only a small number of AM techniques have been exploited for scaffold fabrication. Since most AM systems available commercially are designed to cater mostly for engineering-related industries, work conducted to date had mainly been focused on adapting and modifying such systems for processing biomaterials and scaffold production. Detailed descriptions of the principles and operations of the various AM techniques can be found in some publications [1]. The following sections describe the major AM techniques that have been extensively researched for fabricating TE scaffolds. The section is divided into three main subsections: (1) solid-based techniques, (2) powder-based techniques, and (3) liquid-based techniques.
19.5.1 Solid-Based Techniques
Solid-based AM systems are meant to encompass all forms of material in solid state that can be in the form of a wire, roll, laminates, and pellets. Most of such systems fabricate parts by means of cutting and joining method or melting and fusing/solidifying method.
19.5.1.1 Fused Deposition Modeling (FDM)
The fused deposition of material technique uses the concept of material extrusion to deposit thin filaments of liquids, pastes, melts, solutions, or reactive material to form the cross-sectional profiles of the desired part. The technique was first introduced by Stratasys Inc. (Eden Prairie, MN), as fused deposition modeling (FDM), and is based on the extrusion of polymer melts. Among the variants of the FDM technique are fused deposition of ceramics (FDC), precise extrusion manufacturing (PEM), low-temperature deposition manufacturing (LDM), rapid prototyping robotic dispensing (RPBOD), and Bioplotter. In these techniques, the scaffolding materials are extruded from a nozzle in thin filament forms known as material roads. The nozzle is attached to a moving mechanism (e.g., robotic arm, x-y table) that translates in the horizontal plane to direct the deposition of the material roads onto a building platform. The material roads are arranged in parallel with a pre-defined spacing (i.e., raster gap setting) to form the individual material layers which are then stacked on top of one another to replicate the third (height) dimension of the scaffold object. Variations in the angle or direction of material deposition (i.e., lay-down pattern) for each individual layer can be utilized to create scaffolds with varying honeycomb-like micro-architectures.
The FDM systems available commercially impose many constraints on scaffold fabrication. The nature and operating limits of the FDM systems reduce the choice of scaffolding materials to thermoplastics with low melting points and relatively low melt viscosities. Further to this, there is a need to convert the polymeric scaffolding materials that are usually supplied by the material vendors as pellets, powders, or flakes into filament form with good diametrical consistency before they can be processed on the FDM. Currently, the FDM had been successfully adapted by Zein et al. [57] for fabricating poly(ε-caprolactone) (PCL) scaffolds with pore sizes (channel widths) and porosity values ranging from 160–700 μm and 48–77%, respectively, that were subsequently seeded with primary human fibroblast and osteoblast cells [60]. Complete in-growth and colonization of the scaffolds by cellular tissues were reported after a 3- to 4-week culture period. Cornejo et al. [63] developed the fused deposition of ceramic (FDC) system that processes ceramic-loaded thermoplastic filaments for producing ceramic scaffolds from β-tricalcium phosphate (TCP) . The polymeric binder was removed via a burnout process, and the ceramic component was sintered at 1250 °C to yield scaffolds with minimum pore widths of 300 μm.
To address the limitations imposed on the choice and physical forms of the scaffolding materials that can be processed by existing FDM systems, different research groups have developed their own material extrusion systems that are dedicated for scaffold fabrication. Xiong et al. [61] developed the precise extrusion manufacturing (PEM) system that is suited for the processing of biopolymers. While the FDM system requires filament feedstock, the PEM system is capable of accepting polymer powder, pellet, or granule feedstock. The pressure to extrude the polymer melt is generated by compressed air. Xiong et al. utilized the PEM system for fabricating porous cylindrical poly(l-lactic acid) (PLLA) scaffolds with porosities of around 60.3% and varying channel widths of between 200 and 500 μm. Further developments achieved by Xiong et al. [73] led to a low-temperature deposition manufacturing (LDM) system that was specially developed for producing composite PLLA/TCP scaffolds for bone tissue engineering applications. The LDM fabrication process is carried out within a subzero environment using a slurry feedstock with a composition of 15 wt% PLLA, 15 wt% TCP, and 70 wt% dioxane. For their evaluation, hollow tubular PLLA/TCP scaffolds with internal and external diameters measuring 5 and 10 mm, respectively, and channel widths of 400 μm were produced. The average porosity of the scaffolds was around 89.6%. To assess their biocompatibility and efficacy, the LDM-fabricated PLLA/TCP composite scaffolds preloaded with about 150 μL of bovine bone morphogenic protein (bBMP) at 200 g/L concentration were used to repair a 20 mm segmental defect in canine radiuses. Results of radiology and physical examinations after 24 weeks of implantation showed complete regeneration of new bone tissues over the entire scaffold.
Ang et al. [53] developed a rapid prototyping robotic dispensing (RPBOD) system that is capable of processing gel material feedstock (chitosan and chitosan/HA mixtures). To evaluate the RPBOD system, rectangular chitosan and chitosan/HA composite scaffolds measuring 5 × 5 × 3 mm were fabricated. In vitro cell culture studies were carried out to assess the biocompatibility of the scaffolds. Samples of the scaffolds measuring were seeded with human osteoblast cells and cultured for a 4-week period. The cells exhibited healthy morphology and strong proliferative ability throughout the culture period for all seeded scaffolds, therefore ascertaining scaffold cell biocompatibility.
A commercial machine, Bioplotter , developed separately by Freiburg Materials Research Centre, Germany, and marketed by Envision Technologies GmBH, Germany, [71] has similar design concepts and working principles as the RPBOD system. The Bioplotter is capable of processing a wide range of biomaterials including thermoplastic polymers, reactive resins (i.e., silicone resins), structured hydrogels (composed of alginic acid, gelatin, collagen, fibrin, or other hydrogels), and thermos-reversible hydrogels. In the Bioplotter setup, an 80-μm needle is employed as the extrusion nozzle where liquids, pastes, melts, solutions, hot melts, reactive oligomers, or dispersions which are initially stored in a heated cartridge are extruded into a temperature controlled liquid dispensing medium. The dispensing medium induces solidification of the deposited material by cooling and heating or through chemical reaction. Also, by using a dispensing solution of similar density as the building material, the buoyancy exerted by the medium on the building can prevent the collapse of complex structures, thus eliminating the need for sacrificial support structures which are typical in conventional FDM systems.
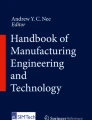
The authors have successfully built and studied the micro-architectures of different scaffold constructions produced using high-density polyethylene (HDPE) with the FDM. These scaffolds were built with lay-down patterns supplied in the system software or from the works of Too et al. [56] and Hutmacher et al. [65]. There are no restrictions to the number of lay-down patterns that can be created by changing the direction of material extrusion for each consecutive layer of a FDM structure. However, as demonstrated by Too et al. [56] and Hutmacher et al. [65], the lay-down pattern employed has its own set of mechanical and physical characteristics that may generate specific or unique cell or host tissue response. The pore interconnectivity of FDM-fabricated structures is observed from the morphology of a sliced structure taken at a 90° angle to the y-axis (Fig. 19.1).

Micrograph showing three-dimensional pore interconnectivity within FDM-fabricated structure
Although the FDM is capable of fabricating various honeycomb-like architectures, the pore morphologies obtained for FDM-fabricated scaffolds are not consistent along the three dimensions (x-, y-, and z-axes) when built using the standard build patterns provided by the system software as illustrated in Fig. 19.2. The pore openings facing the z-direction are determined by the lay-down pattern employed during fabrication that is directly controlled by user-defined parameters. Pore openings facing the x- and y-directions (both are similar) are created by the stacking of material layers and material layer. In addition, the pore openings in both the x- and y-directions are partially occluded by the deposited material that bridges consecutive roads. A method to circumvent such limitation to attain consistent pore openings along all three axes is to stack consecutive layers of materials that are built with the same lay-down pattern until the desired pore morphology is formed before changing the lay-down pattern for the deposition of subsequent layers. Specimens built using this improved method are presented in Fig. 19.3. Other limitations encountered with the FDM include the need for supporting structures to be constructed alongside scaffold with channels or overhanging features. Moreover, the need to convert the scaffolding materials to filament forms before FDM processing increases the risk of material contamination or can cause degradation in material properties.

Micrographs showing the inconsistency in pore sizes on the surfaces of a cubic scaffold when viewed from the (a) z-direction and (b) x- and y-directions

Micrographs showing the surfaces of a cubic scaffold produced with the improved building technique when viewed from the (a) z-direction and (b) x- and y-directions
A different approach for scaffold production using FDM-fabricated sacrificial molds in conjunction with casting methods (lost mold technique) to obtain porous ceramic implants has also been developed. In this process, wax molds made from a commercial modeling material, ICW06 (Stratasys Inc., MN), were produced on a commercial FDM system [68]. The molds were designed based on the negative profile of the desired implant structure. Water-based alumina slurry was infiltrated into the mold cavities and allowed to dry before the mold is pyrolyzed. The resulting ceramic structure was then sintered at a higher temperature. Sample scaffolds with porosities between 33% and 50% and various pore sizes ranging from 300 to 750 μm have been fabricated with this method. In order to convert the bioinert alumina implants into bioactive and osteoconductive devices, the implants were dip-coated with HA [74] and fired to consolidate the coating. In vitro cell culture assessment carried out with human osteosarcoma cells yielded high numbers of attached cells and good uniformity in the distribution of the attached cells throughout the entire structure of the implants.
19.5.2 Powder-Based Techniques
Though powder-based systems are strictly considered as solid-based because they are in solid state, it is intentionally created as a category to highlight the fusion techniques employed to fuse them together which often includes binder or laser. This category is meant to mean powder in grain-like form.
19.5.2.1 Color Jet Printing (CJP)
The CJP process , formerly known as 3D printing (3DP), is a binder jetting process that employs ink jet printing technology for processing powder materials. The versatility and simplicity of CJP allow the processing of a wide variety of powder materials including polymers, metals, and ceramics. During fabrication, a printer head is used to print a liquid binder onto thin layers of powder following the object’s profile as generated by the system computer. The subsequent stacking and printing of material layers to the top of previously printed layer recreates the full structure of the desired object. The completed object is embedded inside a cake of unprocessed powders and is extracted simply by brushing away the loose powders.
CJP is perhaps the most widely investigated AM technique for scaffold fabrication. Kim et al. [70] employed CJP with particulate leaching technique to create porous polylactide-coglycolide (PLGA) scaffolds with interconnected 800-μm porous channels and microporosities of 45–150 μm. The scaffolds were subsequently seeded with hepatocytes (HCs). The successful attachment of a large numbers of HCs to the scaffolds’ surfaces and in-growth of HCs into the pore spaces of the scaffolds were reported. Zeltinger et al. [62] successfully built poly(l-lactic acid) (L-PLA) scaffolds with varying pore sizes (38–150 μm) and porosities (75–90%) to investigate the influence of scaffold microstructure on the adhesion, proliferation, and matrix deposition of canine dermal fibroblasts, vascular smooth muscle cells, and microvascular epithelial cells. Cell culture results demonstrated the suitability of scaffolds built with CJP in supporting cell proliferation for the different cell types. Park et al. [71] investigated using CJP with surface modification methods to create scaffolds with controllable poly(lactide-co-glycolic)/poly(l-lactide) (PLGA/PLLA) anisotropic microstructures and regionally selective scaffolds with diverse receptor systems to enable selective cell adhesion. Lam et al. [55] developed a blend of starch-based powder containing cornstarch (50%), dextran (30%), and gelatin (20%) that can be bound by printing distilled water. However, to improve the strength and water resistance of the scaffolds, a secondary infiltration process with copolymer solution consisting of 75% poly(l-lactide) acid and 25% polycaprolactone in dichloromethane is necessary.
One other application of CJP in the fabrication of scaffolds was to print a blend of cellulose and starch powders containing 40 and 50 wt% HA loading. A water-based polymeric solution was employed as the binder in producing the scaffolds. The structures obtained yield high degrees of pore interconnectivity within the scaffolds. Control of the scaffolds’ microstructural characteristics can be achieved by varying the printing speed, the flow rate, drop position of the liquid binder, and the particle size distribution and composition of the powders. As CJP fabrication involves the utilization of a powder bed, a scaffold with complex shapes containing overhanging or hollow features can be carried out since the unprocessed powders surrounding the part can provide the necessary support for such features. The simplicity and versatility of CJP allow the processing of a wide range of biomaterials including polymers and ceramics. As CJP fabrication is conducted at room temperature, the processing of temperature-sensitive materials can be conducted.
Limitations encountered with CJP-fabricated scaffolds using the standard building styles provided by the system software include the limited pore sizes achievable (<50 μm) and their widely distributed values. More consistent pore sizes including larger pores can be generated by mixing porogens (with predetermined sizes) into the powders prior to scaffold fabrication [62, 70]. Despite the improvements achievable with porogens, their application carried the risk of inadvertent residues remaining within the scaffolds as a result of incomplete leaching. For producing polymeric scaffolds, the use of organic solvents as binders to dissolve the polymer powders in the printed regions will create difficulties in solvent removal and risks of residues. However, the formulation and application of water-based binders and specialized powder blends as described previously may lead to the elimination of solvent application. The use of water-based binders in conjunction with room temperature processing may also allow the incorporation of biologically active and pharmaceutical agents into the scaffolds during fabrication [55, 62]. The mechanical properties and accuracy of CJP-fabricated scaffolds are other considerations that need to be further addressed [72].
19.5.2.2 Selective Laser Sintering (SLS)
The SLS technique , a powder bed fusion process, employs a carbon dioxide, CO2, laser beam to sinter selectively thin layers of powdered polymeric materials. The powders that are preheated to a temperature close to melting point will encounter a rise in temperature beyond melting point when exposed to the laser spot, causing them to melt and fuse together into a solid mass. Subsequent layers of powders that are sintered directly on top of previously formed layers will cause the fusion of adjacent layers to form the height of the build object. The supportless feature makes SLS an ideal process for fabricating multilayered porous structures [75].
Lee and Barlow [76, 77] developed various forms of poly(methyl methacrylate-co-n-butyl methacrylate) (PMMA)-coated calcium phosphate powders for processing on a commercial SLS system for producing ceramic scaffolds for hard tissue regeneration. The SLS-fabricated parts were fired in a furnace to remove the polymeric binder and subsequently to sinter the ceramic structures. To improve the density and strengths of the ceramic structures, infiltration of the structures with a phosphoric acid-based inorganic cement was carried out before and after the sintering cycle. The final ceramic scaffolds were reported to possess pore sizes ranging from 60 to 200 μm and an overall porosity of about 30%.
Biocompatibility assessment conducted by implanting SLS-fabricated oral implants on the dog model revealed excellent integration of the implant with the host bone after only 4 weeks of implantation.
In the authors’ research [78, 79], an investigation is being conducted to identify and assess the suitability of different biopolymers for processing via the SLS technique. So far, preliminary sintering experiments conducted on a commercialized SLS system, Sinterstation 2500 (3D Systems, Valencia, CA, USA), have ascertained the feasibility of processing poly-l-lactide acid (PLLA), polycaprolactone (PCL), and polyetheretherketone (PEEK) powder stocks with varying degrees of success. Figure 19.4 illustrates the microstructures of SLS-fabricated scaffold specimens produced from the sintering of PEEK powders and a powder blend of PEEK/HA. Figure 19.5 presents the microstructures obtained from the sintering of PLLA and PCL powders. Due to the use of powder stocks and the relatively low compaction forces exerted on the powder bed during the layering of the powders, high porosity and pore interconnectivity were obtained for all the specimens. The porosity of the specimens can be changed by varying the SLS process parameters such as laser power (or exposure density), scan speed, and part bed temperature. Similar to the 3D-P technique, the SLS is highly capable of producing scaffolds with irregular three-dimensional shapes including structures containing channels and overhanging features due to support provided by the powder bed. Other advantages of SLS for polymer processing include the fact that it is solvent-free and does not require any secondary binder system, hence minimizing any risk of material contamination.

Microstructure of SLS-fabricated scaffolds , (a) PEEK and (b) PEEK with 10 wt% HA

SLS-fabricated scaffolds obtained from the sintering of (a) PLLA and (b) PCL powders
Limitations encountered with the SLS technique include the fact that the pores created in SLS-fabricated scaffolds are dependent on the particle size of the powder stock used and the compaction pressure exerted onto the powder bed while depositing the powder layers. As with the scaffolds fabricated by CJP , scaffolds fabricated by SLS possess pores with sizes that are distributed over a wide range of values. Since the SLS technique involves high processing temperatures, the technique is limited to the processing of thermally stable polymers.
19.5.2.3 Selective Laser Melting (SLM)
Like SLS, SLM , also a powder bed fusion process, employs a laser to selectively fuse powder bed layer-by-layer to form a final part, but SLM is designed for processing mainly metallic powder and its composites [1, 80]. The solidification of powder is due to rapid heating and cooling of metal particles during laser scanning. This mechanism is different from sintering; hence, the word “melting” is given to the name. The main advantage of using metals for tissue engineering is their superior mechanical properties compared to polymer scaffolds. Moreover, as SLM is more precise and accurate than SLS due to the use of fiber laser, smaller pores can be produced. Furthermore, surface roughness is important for host tissue integration. SLM process can naturally introduce different levels of roughness depending on printing parameters or even make different roughness on different surfaces by using strategies such remelting [81]. Therefore, the as-printed parts could be used as the final products for sterilization and implantation.
The use of SLM for tissue engineering comes in two forms. One is printing biocompatible titanium alloys (e.g., medical grade Ti6Al4V) into customized implants with lattice structures such that the implants match the shape, geometry, density, and modulus of native bone tissues [82]. This approach is very helpful in improving conventional implant designs. However, this type of metal scaffolds is still permanent in the body and different from the original concept of tissue engineering scaffolds, which is a biodegradable temporary implant. The other approach focuses on the biodegradation of metal scaffolds by using absorbable metal elements such as magnesium, zinc, iron, and their combinations [83]. As this approach is new, the effects of SLM process on these alloys require further investigation. In addition, the high cost of SLM process and material could be another limitation.
19.5.3 Liquid-Based Techniques
Liquid-based AM systems have the initial form of its material in liquid form. Through a process known as curing, the liquid is converted into solid state; hence, the physical part is obtained.
19.5.3.1 Stereolithography Apparatus (SLA)
The SLA process , a liquid-based rapid prototyping system that has a vat polymerization process, builds parts in a vat of photo-curable liquid resin that solidifies upon exposure to laser radiation usually in the UV range [1]. The process begins with the vat filled with the photo-curable liquid resin and the elevator table set just below the surface of the liquid resin. The computer-controlled optical scanning system then directs the focused laser beam so that it solidifies the two-dimensional cross section corresponding to the slice data on the surface of the resin to a depth greater than one-layer thickness with the elevator descending with each layered scanned. The elevator table then descends enough to cover the solid part that is just fabricated with another layer of resin on the surface. The laser proceeds to draw the next layer, and the process is repeated until the whole part is fabricated. The accuracy and precision of SLA process make it suitable for fabricating not only scaffold lattices but also complex cellular constructs such as triple periodic minimal surface (TPMS) structures [84].
Research on SLA using ceramic materials [85,86,87,88] shows the feasibility of using ceramic in SLA systems. Brady et al. [85] and Hinczewski et al. [86] in their research used a ceramic suspension containing alumina powder, UV curable monomer, diluent, photoinitiator, and dispersant in the process to produce three-dimensional ceramic parts. Upon polymerization, the photopolymer was subjected to heating to remove the organic phase. Subsequent sintering (by means of heating) was carried out to obtain the final dense ceramic piece. The key requirement in these researches is that the suspension must be UV curable that is required for all stereolithography (SL) processes. Other concerns include the ability to obtain a resin with a low viscosity (1200 cps or less [59]) and a curing depth sufficient for typical layer thickness of 100 μm [1].
In the need to seek for alternative materials to be used on SLA, various research teams looked into the possibility of using HA [59, 64, 89] and polymers such as poly (propylene fumarate), PPF [54]. Chu et al. [59, 89] in their research explored the possibility of using an aqueous HA suspension in acrylamides to fabricate custom made ceramic implants by SL. By using different volume percentage of HA powder and different weight percentage of dispersant, different varying viscosities of the resin were obtained. A higher volume percentage of HA powder would result in a higher viscosity making it impossible to be used for SL. Parts fabricated using ceramic suspensions tended to be nonporous which are not desirable for tissue scaffolds because a porous structure is required for cell proliferation.
Hollister et al. [64] combined an image-based approach (based on computed tomography (CT) or magnetic resonance imaging (MRI) data) with SLA to fabricate custom designed TE scaffolds for application in craniofacial surgery. Computer software was used to read the CT data of the area of defect that was to be reconstructed and the data was regenerated to form the external shape. With the shape of the defect obtained, internal pore architecture based on the defect was generated, taking into consideration crucial factors such as tissue infiltration and mechanical behavior and was combined via Boolean combination to obtain the image of the scaffold. The image of the scaffold was exported to a format readable by SLA (in this case .stl) and was ready to be fabricated using the two techniques proposed by the team. In the first technique, casting used as HA slurry was poured into the molds that were fabricated by SL and cured. The second technique used by the team is similar to the one carried out by Chu who is also a member of this research team. Both techniques are capable of fabricating scaffolds that allow control over the external shape as well as internal pore architecture.
The presence of double bonds in PPF allows the polymer to be cross-linked into a solid using a thermal initiator, making it a suitable material for use in SL for the work carried out by Fisher et al. [54]. Soft and hard tissue response to the scaffolds was investigated upon in a rabbit model and results showed that such scaffolds elicited a mild tissue response in both soft and hard tissue making PFF a viable material for use in TE.
Due to the need to obtain resins that are UV curable, the application of SL on TE is limited. Furthermore, the process involves various other sub-components (such as diluent and dispersant), making it a tedious and complex process if HA powders are to be introduced. This inevitably prolongs the fabrication time because parts fabricated by SL process need further curing in the UV chamber. The usage of organic solvent also hinders its application for TE scaffolds. Like FDM, SL process would include the need to allocate supports in parts with overhang that need to be removed during the post processing stage.
19.5.3.2 Bioprinting
Bioprinting , also known as 3D bioprinting or organ printing, is a multidisciplinary research area that emerged in the early 2000s when tissue engineering and 3D printing crossed each other’s path. Bioprinting is defined as a robotic additive biomanufacturing of functional 3D human tissues and organs using living materials (e.g., biological cells) primarily for pharmaceutical and medical applications such as disease modeling, drug discovery, and organ transplantation [90]. In recent years, this family of technologies has rapidly evolved into four main process categories, namely, material jetting, vat photopolymerization, material extrusion, and free-form spatial bioprinting [91]. Many bioprinters developed based on these principles are already commercially available [92, 93].
The ability of manipulating living materials is a unique feature of bioprinting. Compared to scaffold-guided tissue engineering, bioprinting is scaffold-free. Cells are no longer manually seeded onto scaffolds; instead they are directly printed into the shape of a scaffold or a tissue. Therefore, the concepts involved in conventional scaffolds such as porosity, pore size, and pore connectivity become less relevant. The more important considerations are printability of bio-inks, postprinting cell viability, and complex tissue architectures with vascularization.
There are two main forms of living materials used in bioprinting: low cell density materials and high cell density materials . Low cell density materials include cell suspensions and cell-laden hydrogels, especially those printable hydrogels loaded with stem cells [94], which represents a promising strategy for tissue regeneration without much concern on the source of cells, such as heart cells and nerve cells that have very limited division capability in adults. High cell density materials include cell spheroids and organoids [95,96,97]. They are aggregates of either homogeneous or heterogeneous cell populations through mixing or differentiation. The main advantage of using high cell density materials in bioprinting is their close resemblance of native tissue composition (e.g., similar cell density and extracellular matrices) and tissue behaviors (e.g., tissue fusion and cell sorting). Low cell density materials are easily manipulated in terms of printability, shape fidelity, build size, and mechanical properties. Even complex tissue architectures, such as branched 2D and 3D channels [98, 99], could be considered at the design stage when printing low cell density materials, but it would be challenging if cell aggregates are used. Nevertheless, both types of living materials are not as strong as polymeric and ceramic scaffolds. In addition, polymeric and ceramic scaffolds can be stored for later use, while it is expensive and challenging to keep a reasonable shelf life for bioprinted tissue constructs.
Despite of the challenges, bioprinting continues to advance with new applications, for example, guidance for cell alignment [100], new cancer models for pathological study [101], and a novel placental model for developmental biology [102]. Looking into the future, some researchers proposed to solve the issue of support materials in order to build vascular system and complex tissue structures [103], while others envisioned 4D bioprinting [104], in which a bioprinted tissue changes its property over time or matures upon simulation (Table 19.1).
19.6 Development of CAD Strategies and Solutions for Automated Scaffolds Fabrication
Research on AM techniques for scaffold fabrication has ascertained their potential in overcoming many of the limitations encountered using manual-based fabrication techniques. Among the main advantages derivable with AM are the ability to produce spatially and anatomically accurate scaffolds with complex irregular three-dimensional geometries. However, AM systems are optimized for producing highly dense prototypes for engineering applications and as such are limited when it comes to the fabrication of porous structures with consistent pore morphologies and characteristics that are essential for TE scaffolds. Therefore, to enhance better AM scaffold fabrication, new building strategies would have to be developed. One solution is to design the internal micro-architecture of the scaffolds using CAD modeling before committing the scaffold designs to AM fabrication [64, 105, 106]. However, due to the minute and intricate details of possible scaffold micro-architectures, preparation of the computer model of the scaffold using traditional CAD techniques for AM fabrication can be extremely prohibitive even at the hands of experienced CAD operators. The task of having to design, assemble, and integrate individual pore geometries to form a consolidated three-dimensional architecture can be highly tedious and time-consuming, making the entire process impractical for supporting customized production. The need to shape the assembled micro-architectural design to conform to the anatomic shape of the organ or tissue adds to the difficulty of CAD modeling.
In order to overcome the complications of the CAD modeling process, several automated image-based approached for scaffold assembly had been reported. In the work carried out by Hollister et al. [64] which is focused on the fabrication of scaffolds for bone tissue engineering in craniofacial reconstructive surgery, a digital model possessing the external shape of the defect is first reconstructed based on surface profile data acquired at the region of interest on the patient using CT or MRI scans. An internal micro-architecture model is then created using voxel density distribution approach. Both the defect model and the micro-architectural models are then combined to create the final scaffold model that is then fabricated on an AM system.
The authors have developed an automated image-based technique [105,106,107] that can be used to construct and assemble scaffold micro-architectures from a set of selected polyhedral shapes to yield open cellular solids that can be applied for TE applications. Figure 19.6 presents the process chain for the automated process. To allow a wide range of scaffold micro-architectures to be generated, a parametric library of open polyhedral unit shapes was first established. With the library, the user is given the option to select the shape of the polyhedral or combinations of polyhedras to be used and to size the selected polyhedras to yield the correct pore sizes. Control is also provided for the user to determine and build model with desired surface area to volume ratio, porosity, and pore sizes of the scaffold that can be assembled from the selected polyhedra.

Process chain for automated approach to scaffold fabrication
Once an appropriate polyhedra unit shape has been selected and sized, a scaffold assembly algorithm is developed to assemble and link multiple copies of the selected and modified polyhedra shape into a three-dimensional scaffold structure that conforms to the external surface profiles of the defect. Figure 19.7 presents the CAD images of several assembled structures that were generated using the scaffold assembly algorithm and photographs of their physical counterparts that were fabricated using the SLS as compared to a millimeter scale rule. The assemblies shown in Fig. 19.7a, b were obtained by combining two different polyhedra forms using an alternating pattern arrangement, while the assemblies shown in Fig. 19.7c, d were assembled from a single polyhedra form. High macro-porosity values ranging from 83% to 93% are achieved with the different cell configurations presented in Fig. 19.7. This is done without encountering any adverse effects on the structural integrity of the AM-fabricated structures. Figure 19.8 presents a scaffold structure that was assembled to conform to the external and internal shape of the bone segment shown in the same figure.

CAD-generated scaffold assemblies and their AM-fabricated counterparts. (a) Octahedron-tetrahedron. (b) Octahedron-truncated cube. (c) Square prism. (d) Square pyramid

(a) Surface model for bone segment reconstructed from CT data. (b) CAD-generated scaffold structure for the bone segment
Besides the benefits of AM fabrication that have been described earlier, the application of CAD strategies for designing scaffold micro-architectures will enhance the capabilities of the AM techniques. With such strategies, a wide variety of internal architectural designs to facilitate experiments that can be used to characterize the different micro-architectures can be derived. The results of such experiments are necessary inputs for determining the optimal parameters to be used in the RP process and cell culture. The wide variety of internal micro-architectures will also facilitate in vitro and in vivo experiments to determine the suitability and to optimize the designs of the various micro-architectures for different TE applications.
19.7 Prostheses
Prostheses are man-made substitutes fabricated for body parts that have been removed either for traumatic or medical reasons. The main aim of prosthesis is to help a person appear as if the body part has not been removed, hence restoring the confidence of the person in their social lives. While there are numerous prostheses such as hip and artificial legs, breasts, or facial, this section will only explore the applications of AM techniques on facial prostheses.
Facial deformities due to acquired (e.g., surgical excision of diseased tissues or trauma) or congenital (e.g., microtia) causes have always been a concern for plastic surgeons. Patients with defects in the facial region may often be subjected to ridicule or self-isolation, and very often prostheses would be required to provide psychological benefit in the rehabilitation of the patient. With the advancements in modern surgical procedures, instruments, and equipment, plastic surgery may improve a defect in the facial region, but in some cases, it may not be possible to create the lost anatomy with sufficient detail. In addition, patients who do not have the option of surgery due to age, medical condition and preference of the patients, or in cases whereby surgery would not yield satisfactory results, facial prostheses seem to provide the best esthetical solution.
In this section, an integrated manufacturing system for producing extraoral facial prostheses utilizing laser surface scanning/digitizing, computer-aided design (CAD) (e.g., three-dimensional modeling), and computer-aided manufacturing (CAM) (e.g., rapid prototyping) technologies is introduced [108,109,110,111]. Two case studies involving the making of different facial prostheses (forehead and auricular prostheses) using the integrated manufacturing system are briefly described.
19.7.1 Integrated Approach to Prostheses Production
The integrated approach encompasses a series of steps (Fig. 19.9) that include (1) data acquisition, (2) CAD remodeling, (3) fabrication of prosthesis via AM, and (4) trial fitting and casting of actual prosthesis.

Process chains of the new integrated manufacturing system
19.7.1.1 Data Acquisition
The first step in the integrated approach is to obtain topographic data of both the defective region and a healthy “donor” organ upon which the design of the prosthesis would be based. In order to capture anatomic details and profiles, surface scanning is carried out by means of a laser surface scanners or digitizers. Surface scanning is being used more frequently now in the medical field, and its usefulness is evident in studies related to data capture of surface morphology and quantitative assessment of surface changes. Data obtained from such surface scanners are three-dimensional point cloud data sets stored in various formats (e.g., IGES, DXF, ACIS, etc.). Such data are read by specialized CAD software so as to reconstruct the surfaces of the scanned object from the output digitized data to yield a computer model of the object that can then be exported to the relevant AM systems. One key advantage of such scanners is that the digitizers utilize low power lasers that produce no harmful radiations. Moreover, scanning times are in the order of 0.6–7 s per scan which eliminates the need for the patient to remain perfectly still for a lengthy period of time. However, one of the limitations with most surface scanners is the need for special darkroom environment or special rooms with the scanning components forming permanent fixtures in these environments .
19.7.1.2 CAD Remodeling
CAD software is often utilized to edit and manipulate the point cloud data generated by a digitizer. The ability of such software to convert CAD models to STL data format is important since the STL format is the de facto standard for data interfacing between CAD and AM systems. Although most CAD software are capable of generating STL data, not all are capable of reading-in, editing, or manipulating STL data. As such, the authors have used Surfacer Version 9 (Imageware Inc., USA) for the purpose of their research. The point cloud data is triangulated or polygonized to reconstruct the surface profiles of the site of deformity or the facial organ. Any missing data patches or blind spots on the polygonized point cloud model can be regenerated using a number of CAD editing and data manipulation methods. The computer models generated by both techniques are converted into STL data for fabrication in an AM system.
19.7.1.3 Fabrication of Prosthesis Via AM
Most AM systems generally adopt the additive fabrication technique whereby the part to be fabricated is built layer-by-layer. The individual layer is represented and determined by its corresponding slice file that stores the geometric detailed data of the model to be built. For the purpose of discussion in this section, selective laser sintering (SLS) would be described.
19.7.1.4 Casting of Actual Prosthesis
Casting of the prostheses starts from the master model of the prototype. Vacuum casting is often preferred in prototype making because low-cost components can be obtained. Furthermore, slight adjustments to their shapes which can be achieved by removing materials or adding wax where desired are conducted to improve the comfort of the prostheses. The AM replicas can also serve as patterns to produce the negative molds necessary to cast the actual prostheses.
19.8 Case Studies
The authors have focused on producing facial prostheses using computerized imaging techniques, CAD, and AM on facial organs (such as ear) and deformity (forehead) in their research [110, 111].
19.8.1 Case Study 1: Prosthetic Ear
In this case study, the patient suffers from unilateral microtia involving the total loss of the right external ear. As such, the profile of the deformity as well as the patient’s contralateral external normal ear was scanned using the laser digitizer. For the purpose of comparison between the healthy ear and the prosthetic ear that is to be created, the anterolateral and posterior surfaces of both sides of the normal ear were scanned. Figure 19.10a shows the point cloud data of the healthy ear as acquired by the digitizer, and Fig. 19.10b illustrates the application of the three-dimensional curve generation technique in Surfacer Version 9.0 environment to restore missing areas that were not captured during scanning. Figure 19.10c shows the fully patched and completed computer model of the ear. Upon the completion for the patching of the point cloud data in the Surfacer Version 9.0 environment, the completed model was mirror-imaged to obtain a contralateral version, which provided for the prosthetic ear pattern to be fabricated. A point to note is that, in order to create an accurate prosthetic ear with good surface fitting attributes, the positioning and fitting of the prosthesis were conducted in the CAD environment. Factors taken into consideration in creating a natural looking prosthesis include the inclination of the ear and the size and the degree of erection. Moreover, to ensure perfect fitting between the undersurface of the prosthesis and the face of the patient, the surface profile of the site of deformity was extracted and used to create the undersurface of the prosthetic ear model. When a satisfactory model of the prosthetic ear was reached, it was converted into the STL format and fabricated using the SLS system.

(a) Point cloud data of the healthy ear. (b) Surface regeneration using three-dimensional curve generating technique. (c) Completed CAD model (before mirror-imaging). (d) SLS-fabricated pattern
Figure 19.10d presents the prosthetic ear pattern built from polyamide (Duraform™, 3D Systems Inc., USA) material. It was observed that the undercuts around the helix and concha regions of the ear were reproduced with high degrees of realism using the surface patching technique . The duration of the entire process from data acquisition to completion of the pattern was approximately 5.5 h including the 3-h SLS fabrication time.
19.8.2 Case Study 2: Prosthetic Forehead
For this case study, the patient has a congenital defect in the form of a depression on her forehead . The objective was to create a forehead prosthesis that can be worn by the patient to cover the depression. Conventional procedures for such deformity include facial implants or local flap [112, 113]. The first technique, facial implants, requires the raising of skin flap down to the skull bone. Thereafter, a pocket is created, and the implant, usually made of silastic or methyl methacrylate, is embedded into the pocket. The implant is anchored in place by placing sutures around the enveloping muscles and tissues. After ensuring that the implant is secured, the skin flap is returned to its original position. In the second technique, areas such as the supraorbital and supratrochlear vessel-based island flap are used to cover the unilateral forehead defects. Detailed preoperative dimensioning is needed to determine the size and shape of the forehead skin to be replaced by portion of the forehead island flap. Full thickness of skin is incised around the inverted pattern of the defect, outlining the skin portion of the island flap [104]. Such conventional techniques are often dependable on the condition of the patient as well as the availability of donor site for such operations. Furthermore, such surgical procedures often require up to 3 h. Compared to the conventional procedures, AM-fabricated prosthetic forehead is noninvasive, hence reducing the duration of the surgical procedures and recovery time for the patient.
This particular prosthesis presents a challenge to the CAD operator as the profile of the forehead prosthesis had to be empirically recreated based on anthropometrical measurements and visual assessments made at the site of deformity. A full-face scan was conducted on the patient using a hand-held laser scanner to obtain the full profile of the depression. The scanned data was then imported into Surfacer software environment where it was triangulated to generate the surface model of the patient’s face. Figure 19.11a shows the surface model generated using Surfacer with the congenital forehead depression visible on the patient’s left.

(a) Subject with congenital forehead depression. (b) Creating the forehead prosthesis via three-dimensional surface patching. (c) Model of forehead prosthesis fitted onto the patient’s face
The facial profile on the unaffected side of the patient’s forehead was extracted and mirror-imaged to serve as a template for the CAD operator to capture and recreate the profile of the missing forehead. Using the CAD tools in Surfacer, the forehead prosthesis was created based on the boundaries as defined in Fig. 19.11b. Surface lofting was then used to generate a series of external surfaces as well as the undersurfaces of the forehead prosthesis based on the set of defined curves which can be further adjusted to match the profile of the forehead depression. The realism of the prosthesis was enhanced with the aid of the unaffected side of the patient’s forehead as the external surface contours of the prosthesis were adjusted to match the curvature of the unaffected side.
This was made possible in the Surfacer environment as the prosthetic model can be viewed from different projection angles to assess its fitting and to assist in carrying out editing works to smoothen or camouflage the junction lines formed at the edge of the prosthesis when it is worn by the patient. This was carried out to create the illusion of a continuous forehead surface. By doing so, the edges of the resulting prosthesis model are usually thin in order for the prosthesis to blend flawlessly onto the face of the patient. Figure 19.11c shows the completed model of the prosthesis fitted onto the patient’s face.
As thin edges were noted on the prosthetic forehead, the direct fabrication of the prosthetic forehead would result in an AM-fabricated pattern with edges that were brittle and hence easily damaged through handling. Hence, instead of creating a master pattern to cast a silicon rubber mold to produce the actual prosthesis, the direct mold production approach was followed to produce a negative AM-fabricated mold set for casting the forehead prosthesis. Fabrication of the mold set was carried out on a SLS system (Sinterstation 2500, 3D Systems Inc., USA) to yield a negative mold that can be cast using silastic material to obtain the prosthetic forehead .
19.9 Conclusion
The biomedical applications of AM in two main fields have been explored. The applications of scaffolds fabricated using conventional, manual-based fabrication techniques are limited due to imperfections encountered in their macro- and micro-architectures and the poor flexibility and control offered by the fabrication techniques. Computer-controlled fabrication via AM technology has been recognized and established as having the potential for providing a generic solution in automating customized scaffold production. A review of the different AM methods that have been evaluated and employed for scaffold fabrication together with the work conducted by different research teams worldwide has been presented. The use of image-based approaches and CAD strategies for designing scaffold structures also has been highlighted and discussed. It is clear that the application of AM techniques in conjunction with the proposed building strategies will enable new cost-effective and rapid solutions to customize “made-to-order” scaffold production to meet the needs of most TE applications.
Furthermore, the integration of a manufacturing system consisting of a laser digitizer, CAD software, and AM system for making facial prostheses was detailed. From the case studies presented, it can be noted that the novel integrated manufacturing system is able to shorten the time needed to acquire digitized data of a patient’s facial deformity, as well as to minimize patient involvement throughout the prosthesis fabrication process. The application of computer-aided techniques will undoubtedly allow reproducible and consistently high-quality prostheses to be achieved.
References
Chua CK, Leong KF. 3D printing and additive manufacturing: principles and applications fifth edition of rapid prototyping fifth edition. Singapore: World Scientific Publishing; 2017.
Bell E. Tissue engineering in perspective. In: Lanza RP, Langer RS, Vacanti JP, editors. Principles of tissue engineering. 2nd ed. Academic Press: San Diego; 2000.
Mooney DJ, Mikos AG. Growing new organs. Sci Am. 1999;280:60–5.
Patrick CWJ, Mikos AG, Mcintire LV. Prospectus of tissue engineering. In: Patrick CWJ, Mikos AG, Mcintire LV, editors. Frontiers in tissue engineering. New York: Elsevier; 1998. p. 1–11.
An J, Teoh JEM, Suntornnond R, Chua CK. Design and 3D printing of scaffolds and tissues. Engineering. 2015;1:261–8.
Thomson R, Wake M, Yaszemski MJ, Mikos A. Biodegradable polymer scaffolds to regenerate organs. Adv Polym Sci. 1995:245–74.
United Network for Organ Sharing Website: http://www.unos.org
Scientific Registry of Transplant Recipients. Annual report of the U.S. Scientific registry for organ transplantation and the Organ Procurement and Transplant Network R, VA, 2000.
Whang K, Healy K, Elenz D, Nam E, Tsai D, Thomas C, Nuber G, Glorieux F, Travers R, Sprague S. Engineering bone regeneration with bioabsorbable scaffolds with novel microarchitecture. Tissue Eng. 1999;5:35–51.
Kim WS, Vacanti JP, Cima L, Mooney D, Upton J, Puelacher WC, Vacanti CA. Cartilage engineered in predetermined shapes employing cell transplantation on synthetic biodegradable polymers. Plast Reconstr Surg. 1994;94:233–7. discussion 238–240
Davis MW, Vacanti JP. Toward development of an implantable tissue engineered liver. Biomaterials. 1996;17:365–72.
Niklason L, Gao J, Abbott W, Hirschi K, Houser S, Marini R, Langer R. Functional arteries grown in vitro. Science. 1999;284:489–93.
Karmiol S. Cell isolation and selection. In: Atala A, Lanza R, Lanza RP, editors. Methods of tissue engineering. Academic Press: San Diego; 2002. p. 19–36.
Freed L, Hollander A, Martin I, Barry J, Langer R, Vunjak-Novakovic G. Chondrogenesis in a cell-polymer-bioreactor system. Exp Cell Res. 1998;240:58–65.
Freed L, Vunjak-Novakovic G, Langer R. Cultivation of cell-polymer cartilage implants in bioreactors. J Cell Biochem. 1993;51:257–64.
Weinberg CB, Bell E. A blood vessel model constructed from collagen and cultured vascular cells. Science. 1986;231:397–400.
Madihally SV, Matthew HW. Porous chitosan scaffolds for tissue engineering. Biomaterials. 1999;20:1133–42.
Mikos AG, Temenoff JS. Formation of highly porous biodegradable scaffolds for tissue engineering. Electron J Biotechnol. 2000;3:23–4.
Temenoff JS, Mikos AG. Tissue engineering for regeneration of articular cartilage. Biomaterials. 2000;21:431–40.
Mooney DJ, Vacanti JP. Tissue engineering using cells and synthetic polymers. Transplant Rev. 1993;7:153–62.
Cima L, Vacanti J, Vacanti C, Ingber D, Mooney D, Langer R. Tissue engineering by cell transplantation using degradable polymer substrates. J Biomed Eng. 1991;113:143.
Cima LG, Langer R, Vacanti JP. Polymers for tissue and organ culture. J Bioact Compat Polym. 1991;6:232–40.
Cornell CN. Osteoconductive materials and their role as substitutes for autogenous bone grafts. Orthop Clin. 1999;30:591–8.
Beruto D, Mezzasalma S, Capurro M, Botter R, Cirillo P. Use of α-tricalcium phosphate (TCP) as powders and as an aqueous dispersion to modify processing, microstructure, and mechanical properties of polymethylmethacrylate (PMMA) bone cements and to produce bone-substitute compounds. J Biomed Mater Res. 2000;49:498–505.
Liu X, Ma PX. Polymeric scaffolds for bone tissue engineering. Ann Biomed Eng. 2004;32:477–86.
Ingber DE. Mechanical and chemical determinants of tissue development. In: Principles of tissue engineering. 2000. pp. 101–110.
Mooney DJ, Cima L, Langer R, Johnson L, Hansen LK, Ingber DE, Vacant JP. Principles of tissue engineering and reconstruction using polymer-cell constructs. In: MRS online proceedings library archive, 252. 1991.
Chen CS, Mrksich M, Huang S, Whitesides GM, Ingber DE. Geometric control of cell life and death. Science. 1997;276:1425–8.
McClary KB, Ugarova T, Grainger DW. Modulating fibroblast adhesion, spreading, and proliferation using self-assembled monolayer films of alkylthiolates on gold. J Biomed Mater Res. 2000;50:428–39.
Freed LE, Vunjak-Novakovic G, Biron RJ, Eagles DB, Lesnoy DC, Barlow SK, Langer R. Biodegradable polymer scaffolds for tissue engineering. Bio/Technology. 1994;12:689–93.
Freed L, Grande D, Lingbin Z, Emmanual J, Marquis J, Langer R. Joint resurfacing using allograft chondrocytes and synthetic biodegradable polymer scaffolds. J Biomed Mater Res. 1994;28:891–9.
Mikos AG, Sarakinos G, Lyman MD, Ingber DE, Vacanti JP, Langer R. Prevascularization of porous biodegradable polymers. Biotechnol Bioeng. 1993;42:716–23.
Wake MC, Patrick CW Jr, Mikos AG. Pore morphology effects on the fibrovascular tissue growth in porous polymer substrates. Cell Transplant. 1994;3:339–43.
Rout P, Tarrant S, Frame J, Davies J. Interaction between primary bone cell cultures and biomaterials. Part 3: a comparison of dense and macroporous hydroxyapatite. In: Pizzoferratto A, Ravaglioli PG, Lee AJC, editors. Biomaterials and clinical applications. Amsterdam: Elsevier; 1988. p. 591–6.
Yang S, Leong KF, Du Z, Chua CK. The design of scaffolds for use in tissue engineering. Part I Traditional factors. Tissue Eng. 2001;7:679–89.
Thomson RC, Shung AK, Yaszemski MJ, Mikos AG. Polymer scaffold processing. In: Principles of tissue engineering, vol. 2; 2000. p. 251–62.
Widmer MS, Mikos AG. Fabrication of biodegradable polymer scaffolds for tissue engineering. In: Frontiers in tissue engineering: Elsevier; 1998. p. 107–20.
Lu L, Mikos AG. The importance of new processing techniques in tissue engineering. MRS Bull. 1996;21:28–32.
Mikos AG, Bao Y, Cima LG, Ingber DE, Vacanti JP, Langer R. Preparation of poly (glycolic acid) bonded fiber structures for cell attachment and transplantation. J Biomed Mater Res. 1993;27:183–9.
Lo H, Ponticiello M, Leong K. Fabrication of controlled release biodegradable foams by phase separation. Tissue Eng. 1995;1:15–28.
Nam YS, Park TG. Porous biodegradable polymeric scaffolds prepared by thermally induced phase separation. J Biomed Mater Res. 1999;47:8–17.
Mikos AG, Thorsen AJ, Czerwonka LA, Bao Y, Langer R, Winslow DN, Vacanti JP. Preparation and characterization of poly (L-lactic acid) foams. Polymer. 1994;35:1068–77.
Mikos AG, Sarakinos G, Leite SM, Vacant JP, Langer R. Laminated three-dimensional biodegradable foams for use in tissue engineering. Biomaterials. 1993;14:323–30.
Mikos AG, Sarakinos G, Vacanti JP, Langer RS, Cima LG. Biocompatible polymer membranes and methods of preparation of three dimensional membrane structures. US Patent 5,514,378. 1996.
Thomson RC, Yaszemski MJ, Powers JM, Mikos AG. Fabrication of biodegradable polymer scaffolds to engineer trabecular bone. J Biomater Sci Polym Ed. 1996;7:23–38.
Mooney DJ, Baldwin DF, Suh NP, Vacanti JP, Langer R. Novel approach to fabricate porous sponges of poly (D, L-lactic-co-glycolic acid) without the use of organic solvents. Biomaterials. 1996;17:1417–22.
Baldwin DF, Shimbo M, Suh NP. The role of gas dissolution and induced crystallization during microcellular polymer processing: a study of poly (ethylene terephthalate) and carbon dioxide systems. J Eng Mater Technol. 1995;117:62.
Shastri VP, Martin I, Langer R. Macroporous polymer foams by hydrocarbon templating. Proc Natl Acad Sci. 2000;97:1970–5.
Whang KTC, Nuber G, Healy KE. A novel method to fabricate bioabsorbable scaffolds. Polymer. 1995;36:837–42.
Healy KE, Whang K, Thomas CH. Method of fabricating emulsion freeze-dried scaffold bodies and resulting products. Patent 5,723,508. 1998.
Harris LD, Kim BS, Mooney DJ. Open pore biodegradable matrices formed with gas foaming. J Biomed Mater Res. 1998;42:396–402.
Yang S, Leong KF, Du Z, Chua CK. The design of scaffolds for use in tissue engineering. Part II. Rapid prototyping techniques. Tissue Eng. 2002;8:1–11.
Ang T, Sultana F, Hutmacher D, Wong YS, Fuh J, Mo X, Loh HT, Burdet E, Teoh S-H. Fabrication of 3D chitosan–hydroxyapatite scaffolds using a robotic dispensing system. Mater Sci Eng C. 2002;20:35–42.
Fisher JP, Vehof JW, Dean D, van der Waerden JPC, Holland TA, Mikos AG, Jansen JA. Soft and hard tissue response to photocrosslinked poly (propylene fumarate) scaffolds in a rabbit model. J Biomed Mater Res. 2002;59:547–56.
Lam CXF, Mo X, Teoh S-H, Hutmacher D. Scaffold development using 3D printing with a starch-based polymer. Mater Sci Eng C. 2002;20:49–56.
Too MH, Leong KF, Chua CK, Du ZH, Yang SF, Cheah CM, Ho SL. Investigation of 3D non-random porous structures by fused deposition modelling. Int J Adv Manuf Technol. 2002;19:217–23.
Zein I, Hutmacher DW, Tan KC, Teoh SH. Fused deposition modeling of novel scaffold architectures for tissue engineering applications. Biomaterials. 2002;23:1169–85.
Hollister SJ, Maddox R, Taboas JM. Optimal design and fabrication of scaffolds to mimic tissue properties and satisfy biological constraints. Biomaterials. 2002;23:4095–103.
Chu T-M, Halloran J, Hollister SJ, Feinberg SE. Hydroxyapatite implants with designed internal architecture. J Mater Sci Mater Med. 2001;12:471–8.
Hutmacher DW, Schantz T, Zein I, Ng KW, Teoh SH, Tan KC. Mechanical properties and cell cultural response of polycaprolactone scaffolds designed and fabricated via fused deposition modeling. J Biomed Mater Res. 2001;55:203–16.
Xiong Z, Yan Y, Zhang R, Sun L. Fabrication of porous poly (L-lactic acid) scaffolds for bone tissue engineering via precise extrusion. Scr Mater. 2001;45:773–9.
Zeltinger J, Sherwood JK, Graham DA, Müeller R, Griffith LG. Effect of pore size and void fraction on cellular adhesion, proliferation, and matrix deposition. Tissue Eng. 2001;7:557–72.
Cornejo I. Development of bioceramic tissue scaffolds via fused deposition of ceramics. Ceram Trans. 1999;110:183–95.
Hollister SJ, Levy RA, Chu TM, Halloran JW, Feinberg SE. An image-based approach for designing and manufacturing craniofacial scaffolds. Int J Oral Maxillofac Surg. 2000;29:67–71.
Hutmacher DW. Scaffolds in tissue engineering bone and cartilage. Biomaterials. 2000;21:2529–43.
Hattiangadi A, Bandyopadhyay A. Processing, characterization and modeling of non-random porous ceramic structures. In: Proceedings of solid freeform fabrication symposium, Austin, TX, 1999. pp. 319–326.
Steidle C, Klosterman D, Chartoff R, Graves G, Osborne N. Automated fabrication of custom bone implants using rapid prototyping. In: Proceedings of the 44th international SAMPE symposium and exhibition. Long Beach, CA, May 1999, 1866–1877.
Bose S, Avila M, Bandyopadhyay A. Processing of bioceramic implants via fused deposition process. In: Proceedings of solid freeform fabrication symposium. Austin, TX, 1998. pp. 629–636.
Danforth S, Safari A, Jafari M, Langrana N. Solid freeform fabrication (SFF) of functional advanced ceramic components. Naval Res Rev. 1998;50:27–38.
Kim SS, Utsunomiya H, Koski JA, Wu BM, Cima MJ, Sohn J, Mukai K, Griffith LG, Vacanti JP. Survival and function of hepatocytes on a novel three-dimensional synthetic biodegradable polymer scaffold with an intrinsic network of channels. Ann Surg. 1998;228:8.
Park A, Wu B, Griffith LG. Integration of surface modification and 3D fabrication techniques to prepare patterned poly (L-lactide) substrates allowing regionally selective cell adhesion. J Biomater Sci Polym Ed. 1998;9:89–110.
Giordano RA, Wu BM, Borland SW, Cima LG, Sachs EM, Cima MJ. Mechanical properties of dense polylactic acid structures fabricated by three dimensional printing. J Biomater Sci Polym Ed. 1997;8:63–75.
Xiong Z, Yan Y, Wang S, Zhang R, Zhang C. Fabrication of porous scaffolds for bone tissue engineering via low-temperature deposition. Scr Mater. 2002;46:771–6.
Bose S, Darsell J, Hosick HL, Yang L, Sarkar DK, Bandyopadhyay A. Processing and characterization of porous alumina scaffolds. J Mater Sci Mater Med. 2002;13:23–8.
Yang W, Bai X, Zhu W, Kiran R, An J, Chua CK, Zhou K. 3D printing of polymeric multi-layer micro-perforated panels for tunable wideband sound absorption. Polymers. 2020;12:360.
Lee G, Barlow J. Selective laser sintering of calcium phosphate powders. In: Proceedings of the solid freeform fabrication symposium. Austin, TX, 1994. pp. 376–380.
Lee G, Barlow J. Selective laser sintering of bioceramic materials for implants. In: Proceedings of the solid freeform fabrication symposium. Austin, TX, 1993. pp. 376–380.
Tan KH, Chua CK, Leong KF, Cheah CM, Cheang P, Bakar MA, Cha SW. Scaffold development using selective laser sintering of polyetheretherketone–hydroxyapatite biocomposite blends. Biomaterials. 2003;24:3115–23.
Tan KH, Chua CK, Leong KF, Cheah CM, Gui WS, Tan WS, Wiria FE. Selective laser sintering of biocompatible polymers for applications in tissue engineering. Biomed Mater Eng. 2005;15:113–24.
Yu W, Sing S, Chua C, Kuo C, Tian X. Particle-reinforced metal matrix nanocomposites fabricated by selective laser melting: a state of the art review. Prog Mater Sci. 2019.
Yu W, Sing SL, Chua CK, Tian X. Influence of re-melting on surface roughness and porosity of AlSi10Mg parts fabricated by selective laser melting. J Alloys Compd. 2019;792:574–81.
Popovich A, Sufiiarov V, Polozov I, Borisov E, Masaylo D. Producing hip implants of titanium alloys by additive manufacturing. Int J Bioprinting. 2016;2:7.
Carluccio D, Demir AG, Bermingham MJ, Dargusch MS. Challenges and opportunities in the selective laser melting of biodegradable metals for load-bearing bone scaffold applications. Metall Mater Trans A. 2020.
Yang W, An J, Chua CK, Zhou K. Acoustic absorptions of multifunctional polymeric cellular structures based on triply periodic minimal surfaces fabricated by stereolithography. Virtual Phys Prototyping. 2020;15:242–9.
Brady GA, Halloran JW. Stereolithography of ceramic suspensions. Rapid Prototyp J. 1997.
Hinczewski C, Corbel S, Chartier T. Stereolithography for the fabrication of ceramic three-dimensional parts. Rapid Prototyp J. 1998.
Brady GA, Chu T-M, Halloran JW. Curing behavior of ceramic resin for stereolithography. In: Proceedings of solid freeform fabrication symposium. Austin, TX. 1996. pp. 403–410.
Himmer T, Nakagawa T, Noguchi H. Sterelithography of ceramics. In: Proceedings of solid freeform fabrication symposium. Austin, TX. 1997. pp. 363–369.
Chu T-MG, Orton DG, Hollister SJ, Feinberg SE, Halloran JW. Mechanical and in vivo performance of hydroxyapatite implants with controlled architectures. Biomaterials. 2002;23:1283–93.
Chua CK, Yeong WY. Bioprinting: principles and applications. Singapore: World Scientific Publishing; 2015.
Lee JM, Sing SL, Zhou M, Yeong WY. 3D bioprinting processes: a perspective on classification and terminology. Int J Bioprinting. 2018; 4.
Lee H, Koo Y, Yeo M, Kim S, Kim GH. Recent cell printing systems for tissue engineering. Int J Bioprinting. 2017;3:15.
Choudhury D, Anand S, Naing MW. The arrival of commercial bioprinters – towards 3D bioprinting revolution! Int J Bioprinting. 2018;4
Mehrban N, Teoh GZ, Birchall MA. 3D bioprinting for tissue engineering: stem cells in hydrogels. Int J Bioprinting. 2016;2:14.
Sriphutkiat Y, Kasetsirikul S, Zhou Y. Formation of cell spheroids using Standing Surface Acoustic Wave (SSAW). Int J Bioprinting. 2018; 4.
Mironov V, Khesuani YD, Bulanova EA, Koudan EV, Parfenov VA, Knyazeva AD, Mitryashkin AN, Replyanski N, Kasyanov VA, DASF P. Patterning of tissue spheroids biofabricated from human fibroblasts on the surface of electrospun polyurethane matrix using 3D bioprinter. Int J Bioprinting. 2016;2:8.
Zhuang P, Sun AX, An J, Chua CK, Chew SY. 3D neural tissue models: from spheroids to bioprinting. Biomaterials. 2018;154:113–33.
Yeong WY, Chua CK, Leong KF, Chandrasekaran M, Lee MW. Comparison of drying methods in the fabrication of collagen scaffold via indirect rapid prototyping. J Biomed Mater Res B Appl Biomater. 2007;82:260–6.
Suntornnond R, Tan EYS, An J, Chua CK. A highly printable and biocompatible hydrogel composite for direct printing of soft and perfusable vasculature-like structures. Sci Rep. 2017;7:1–11.
Bhuthalingam R, Lim PQ, Irvine SA, Agrawal A, Mhaisalkar PS, An J, Chua CK, Venkatraman S. A novel 3D printing method for cell alignment and differentiation. Int J Bioprinting. 2015;1:9.
Knowlton S, Joshi A, Yenilmez B, Ozbolat IT, Chua CK, Khademhosseini A, Tasoglu S. Advancing cancer research using bioprinting for tumor-on-a-chip platforms. Int J Bioprinting. 2016;2:6.
Mandt D, Gruber P, Markovic M, Tromayer M, Rothbauer M, Krayz SRA, Ali F, van Hoorick J, Holnthoner W, Mühleder S, Dubruel P, Van Vlierberghe S, Ertl P, Liska R, Ovsianikov A. Fabrication of placental barrier structures within a microfluidic device utilizing two-photon polymerization. Int J Bioprinting. 2018; 4.
Suntornnond R, An J, Chua CK. Roles of support materials in 3D bioprinting – present and future. Int J Bioprinting. 2017;3:4.
An J, Chua CK, Mironov V. A perspective on 4D bioprinting. Int J Bioprinting. 2016;2:3.
Cheah CM, Chua CK, Leong KF, Chua SW. Development of a tissue engineering scaffold structure library for rapid prototyping. Part 1: investigation and classification. Int J Adv Manuf Technol. 2003;21:291–301.
Cheah CM, Chua CK, Leong KF, Chua SW. Development of a tissue engineering scaffold structure library for rapid prototyping. Part 2: parametric library and assembly program. Int J Adv Manuf Technol. 2003;21:302–12.
Cheah CM, Chua CK, Leong KF, Cheong CH, Naing MW. Automatic algorithm for generating complex polyhedral scaffold structures for tissue engineering. Tissue Eng. 2004;10:595–610.
Ck C, Chou SM, Lin SC, Lee ST, Saw CA. Facial prosthetic model fabrication using rapid prototyping tools. Integr Manuf Syst. 2000;11(1):42–5.
Chua CK, Chou SM, Ng WS, Chow KY, Lee ST, Aung SC, Seah CS. An integrated experimental approach to link a laser digitiser, a CAD/CAM system and a rapid prototyping system for biomedical applications. Int J Adv Manuf Technol. 1998;14:110–5.
Cheah CM, Chua CK, Tan KH, Teo CK. Integration of laser surface digitising with computer-aided design and manufacturing for developing facial prostheses—part 1: design and fabrication of prosthesis replicas. Int J Prosthodont. 2003;16:435–41.
Cheah CM, Chua CK, Tan KH, Teo CK. Integration of laser surface digitising with computer-aided design and manufacturing for developing facial prostheses—part 2: development of moulding techniques for casting prosthetic parts. Int J Prosthodont. 2003;16:543–8.
Whitaker LA. Facial implants. Plast Surg. 1:439–40.
Guerrerosantos J. Frontalis Musculocutaneous Island flap for coverage of forehead defect. Plast Reconstr Surg. 2000;105:18–22.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2021 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Chua, C.K., Leong, K.F., An, J. (2021). Additive Manufacturing and 3D Printing. In: Narayan, R. (eds) Biomedical Materials. Springer, Cham. https://doi.org/10.1007/978-3-030-49206-9_19
Download citation
DOI: https://doi.org/10.1007/978-3-030-49206-9_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-49205-2
Online ISBN: 978-3-030-49206-9
eBook Packages: Chemistry and Materials ScienceChemistry and Material Science (R0)