
Abstract
A network theory of governance situates learning processes in the sharing of stories (which we might call ‘agency’) against a background of traditions and norms (which could be seen as ‘structure’). This perspective has implications for both the conceptualisation and study of learning and innovation as a distributed process within organisations. This chapter explores, and develops further, the role of stories in innovation by drawing on aspects of practice theory, in particular, John Shotter’s concept of ‘dialogical practice’ which explores the co-construction of agency through dialogue which represents a ‘third’ way of knowing that does not belong to any one individual, but is a shared, creative act. If such stories are co-constructed through interaction, rather than being formulated and shared by individuals, this has implications for how we conceptualise agency in learning and innovation processes. When considered dialogically, stories can be seen as enduring or ephemeral, and to support or impede change, depending on the networks though which they are co-constructed. This chapter explores this idea using ethnographic evidence from an NHS provider in England of specialist eye services managing a network of clinics. It examines the planning and implementation of innovation through this network and the ways in which the co-construction of stories draws on professional power, and the potential for both creativity and breakdown as they unfold, influence the resulting innovation processes. This perspective also has practical implications for the use of ethnography as a method for inquiring into innovation processes through stories.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Introduction
Innovation can be defined as the planning and implementation of new ideas, products, processes or organisational forms (Schumpeter 1934; Van de Ven 2017). While central to improving health care services, innovation is recognised as challenging to say the least in this context. Multiple reasons have been given for this, some of which include: professional power, complexity of ‘the product’, multiple organisational relationships, and system-wide regulatory processes. We also know that innovation at scale or major system change—where the number of stakeholders involved that need to coordinate their activities is multiplied—generates particular governance challenges in aligning the various professional groups and organisations involved (Turner et al. 2016a). For example, contemporary policy interest in different forms of ‘integrated care’ appear ambitious and fraught with difficulty, even in agreeing what is meant by ‘integration’ (Cameron et al. 2014). One reason for this is that such integrated initiatives, where different agents and organisations need to coordinate their behaviour, are set against decentred forms of governance, under which different organisations act with relative autonomy and in response to localised understandings of policy reforms and initiatives.
Some of the academic thinking on decentred governance offers a possible way forward in referring to the mechanisms, or ‘glue’, that might hold such networks together. For instance, Bevir and Richards (2009a) highlight the importance of the ‘stories’, ‘traditions’, and ‘dilemmas’ that bind together networks. Such ideas can be linked to social constructivism which rejects the primacy of top-down or hierarchical forms of governance by focussing on ‘the social construction of a practice through the ability of individuals to create and act on meanings’ (Bevir and Richards 2009a, p. 3). Governance is decentred because ideas about coordinating the planning or delivery of innovations are said to subsist as much in the responses of individuals involved in implementing change, the so-called ‘street level bureaucrats’ (Lipsky 1971), as the architects of policy or organisational reform that seek to influence change processes top-down by acting from other (often ‘higher’) parts of the system.
This chapter, while sympathetic to social constructivist approaches to understanding continuity and change in organisational and governance processes, seeks to question the status of the ‘individual’—as a key source of agency—in such accounts of policy or innovation processes. In order to do this, we turn to scholarship from within social psychology which takes issue with the idea of attributing ‘rationality’ or ‘cognition’ to an individual’s mind and, therefore, questions the notion of individuals having agency. Instead, this approach suggests a repositioning of the role of the individual in creating or acting on meanings or the stories in which those meanings are situated. Such thinking suggests that, while agency is similarly decentred or distributed, it can be attributed to shared or ‘joint action’ rather than individual’s cognitions. This move from individual to joint action suggests a greater degree of ambiguity and uncertainty in the negotiation of change, including potential for partial or non-implementation of innovation, than decentred governance theory currently proposes.
This chapter applies Bevir’s ideas concerning decentred governance to analyse the innovation processes observed within a specialist provider of eye care services that are organised and delivered through a network of clinics. The chapter then engages critically with the suggested mechanisms of decentred governance proposed by Bevir using the notion of ‘dialogical’ or shared practice drawn from John Shotter’s work. In doing this, the chapter addresses the following research question: what mechanisms influence the planning and implementation of innovations within decentred organisational networks?
In the next section, we outline the conceptual approach of decentred governance, especially the key role of stories, dilemmas, and traditions as mechanisms for holding networks together. We also discuss the status of the ‘individual’ in network theory and contrast this with scholarship from within social psychology that suggests agency comes from shared or ‘joint action’ to tease out the implications for conceptualising agency within innovation networks. These ideas are then explored in relation to an example of health care innovation, a decentralised network of outpatient clinics led by a specialist provider of ophthalmology services within the English National Health Service (NHS). The findings are described through vignettes based on observations of the planning and implementation of innovation by this provider; these are then discussed using decentred governance theory in order to identify key mechanisms that shape innovation within networks and, in particular, the conceptualisation of agency within such networks. The chapter concludes with implications for research and for policy and practice.
Stories, Dilemmas, and Traditions
Bevir and Richards (2009b) describe the theory of decentred governance as offering, “a micro‐theory based on individuals acting in accord with beliefs and desires forged against the background of specific traditions and dilemmas” (p. 140). They outline three mechanisms that allow networks of distributed individuals to coordinate their activities: stories, dilemmas, and traditions. Stories, as they are told and retold, are a by-product of social interaction wherein the narratives associated with networks are developed. By telling stories to one another, individuals share information and engage in learning activities (e.g. by comparing stories). Shared understanding is possible because story telling takes place against a common background of traditions and dilemmas. Traditions are a background of relevant interests and conventions associated with a network that help to inform individuals’ beliefs. Dilemmas or problems faced by individuals are an organising device as individuals develop responses to them. Failure to respond to dilemmas can cause individuals to reconsider their traditions and shared beliefs. There is interplay between dilemmas and traditions: beliefs help to guide individual’s approaches to the problems posed by dilemmas, while individual’s responses to dilemmas can lead to change in beliefs and traditions (Bevir and Waring 2018) . Ethnography is regarded as a key research method for uncovering how and why ‘everyday’ activities and practices come to be associated with decentred networks. Ethnographers construct stories about people’s stories.
Interaction as Shared or Dialogical Practice
The mechanisms of interaction within decentred networks offer a useful way of engaging with the ‘everyday’ practice of interaction. In this chapter, we wish to develop these ideas further, and to critically evaluate their influence on the coordination of innovations, by drawing on John Shotter’s work from the field of social psychology. A key area of contention is around the status of the individual, and their cognitions or rationality, as an agent of continuity and change in decentred network theory. Rather than beginning with the individual’s cognition (including consciousness, rationality, and beliefs), Shotter focusses on experience and interaction as a shared practice, and holds that this does not belong to any one individual. In particular, Shotter draws attention to the shared context of interaction and the ways in which this shapes practice. In describing such interactions, Shotter refers to a ‘third’ type of knowledge that does not belong to any one individual, but is emergent in the context of interaction itself. Shotter (1997) argues that, at the moment ‘when a second human being responds to the acts of a first’ (p. 349), their encounter becomes a spontaneous ‘dialogical’ practice. Such activity does not emerge from the knowledge that participants have acquired prior to their encounter, but depends instead on a non-cognitive response to the affordances of the encounter itself. Often, in the context of shared practice:
though we may be loathe to admit it - we all remain deeply ignorant as to what we are doing, or why we are doing it. Not because the ‘ideas’ or whatever, supposedly in us somewhere informing our actions, are too deeply buried to bring out into the light of day, but because the formative influences shaping our conduct are not wholly there, in our individual heads, to be brought out. Activity of this kind occurs in response to what others have already done, and we act just as much ‘into’ the opportunities and invitations, or ‘against’ the barriers and restrictions they offer or afford us, as ‘out of’ any plans or desires of our own. Thus, the stony looks, the nods of agreement, the failures of interest, the asking of questions, these all go towards what it is one feels one can, or cannot, do or say in such situations. This is joint action; it is spontaneous, unselfconscious, unknowing (although not unknowledgeable) kind of activity. (Shotter 1993, p. 47)
Shotter’s rejection of the idea of knowledge being ‘deeply buried’ could be seen as questioning the idea of individual’s subconscious or tacit knowledge informing activity. Instead, Shotter turns to social practice—and specifically social interactions—in order to understand how what we might term ‘knowledge’ is constructed. Thus, to understand the construction of knowledge in networks we need to inquire into how social interactions are organised. Shotter calls such interactions ‘joint action’.
The interpretation of social interaction as ‘joint action’ allows us to reimagine the key mechanisms of change described in decentred governance theory (dilemmas, stories, traditions). There is still an important role for dilemmas or problems facing actors in joint action. Shotter refers to a task, a difficulty, that is presupposed in joint activity, that such activity is responding to. There is something that needs to be ‘understood’; one proposed way of understanding is by ‘seeing connections’ in relation to one’s circumstances that had not been made before (Shotter 2010, p. 271). With regard to traditions, Shotter (2010) refers to the importance of a ‘larger activity’ (p. 210) or background in which utterances or gestures can be understood and allow the shared activity at hand to progress or ‘go on’. With respect to stories, Shotter (2010) points out the ‘unintended and unpredictable outcomes’ (p. 271) associated with joint action. Boje (1991) advocates the study of stories ‘as performance’ whereby they are observed directly in the context in which they take place, including the performance event, audience involved, and how one story is actively related to others. Utterances are shaped by both our past experiences and our immediate surroundings. In the construction of a story, therefore, what we experience is not the essence of a story—put together based on past experience—but something more creative and unpredictable, because it draws on the moment-to-moment sharing of agency available in the immediate situation.
Thus, the concept of joint action encourages us to examine the aspects of the social and material setting which appear to inform the construction of stories. Moreover, it suggests that the outcome of storytelling is unpredictable, meaning that it can direct activity in unexpected ways. In the rest of this chapter, we explore empirically the relevance of the mechanisms proposed in decentred theory for supporting the coordination of behaviour around innovations. Drawing on Shotter’s work, we also explore the relevance of seeing interactions as ‘joint action’ and how this influences the planning and implementation of innovations.
Methods
This chapter draws on a longitudinal case study of the planning and implementation of innovation by an NHS Foundation Trust in England that provides specialist eye services. This provider runs a network of clinics across multiple locations within a metropolitan area, the surrounding region, and internationally. The innovation related to the provision of outpatient clinics for the diagnosis and treatment of glaucoma, a chronic eye disease. Glaucoma is the second most common cause of irreversible blindness worldwide. Glaucoma affects almost 10% of England’s population over the age of 75, 2% of the population over 40, and accounts for over a million outpatient visits to health services annually. Once diagnosed, this potentially blinding condition requires lifelong and often complex treatment, which is necessary for preventing irreversible visual loss. Referrals to hospital of patients with suspected glaucoma have been increasing each year due to population ageing, and the introduction of national clinical guidelines that lowered the clinical threshold for referral (NICE 2009).
Increasing demand has placed pressure on hospital eye services; delays in glaucoma follow-up appointments have caused patient harm (National Patient safety Agency 2009). For glaucoma, the standard pathway involves the treatment of newly referred and follow-up patients in consultant-run clinics. Standard clinics are staffed by a consultant-led multidisciplinary team composed of nurses, optometrists, orthoptists, trainee ophthalmologists, technicians, clinic clerks, and liaison officers. A range of diagnostic tests is conducted, including eye pressure check, visual fields test, and imaging of the optic nerve. The consultant makes treatment decisions at the clinic, e.g. further monitoring, prescription of medication, laser treatment or discharge.
In order to improve patients’ experiences, an improvement programme was established across the Trust, which included a focus on reducing patient journey times through glaucoma clinics. New care pathways involve reorganising patient flow through the system with the aim of improving resource use to alleviate pressure on services caused by increasing demand. For instance, some patients with glaucoma may be allocated to different types of clinic based on their risk of progression of disease. This includes ‘virtual’ or ‘remote review’ clinics in which diagnostic tests are conducted face-to-face by ophthalmic technicians or other non-ophthalmologist staff. The consultant ophthalmologist then reviews these data electronically at a later point in time to make treatment decisions and prescribe medications. The wider studies from which this chapter derives involved analysing barriers and facilitators to the planning and implementation of innovations to improve the provision of outpatient services for glaucoma.
In the wider studies, data were collected during two periods of ethnographic fieldwork, one over the period 2013–2014, and the other over the period 2016–2017. In 2013–2014, 28 interviews and 40.5 hours of non-participants observations were conducted; in 2016–2017, there were a further 25 interviews and 9 hours of non-participant observations. The interviews included senior executives, operational managers, clinical academics, and a variety of clinical staff, including consultants, nurses, technicians, and clerks. Observations covered senior management level meetings, including board meetings, planning meetings by those leading innovations, communication and consultation meetings where updates on the improvement programme were shared and discussed, and the delivery of a number of outpatient clinics for glaucoma patients. All interviews were guided by a semi-structured topic guide, audio-recorded and professionally transcribed. Notes from observations were recorded contemporaneously.
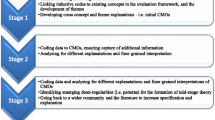
Data analysis for this chapter was geared toward existing ideas concerning both network-based governance (e.g. Bevir and Richards 2009a) and the characteristics of social interaction (e.g. Shotter 2010). Specifically, we constructed stylised vignettes based on observations and stakeholders that we felt represented key events in the planning and implementation of innovations. We then applied the three mechanisms of coordination from decentred governance theory (dilemmas, stories, and traditions) to analyse critically the events described through the vignettes, including the potential relevance of individual and joint action in both the empirical observations and theorised mechanisms of coordination. Thus, data analysis was relatively ‘deductive’ as these concepts were applied to the dataset systematically. However, we also compared and contrasted the fieldwork material with ideas from the literature and were attentive to ‘deviant’ cases, gaps in existing literature, and pointers for developing the literature further where the empirical work suggested new insights about the coordination of innovation in networks.
The meetings (2013–2014 dataset) were chosen as the basis for the vignettes because they were attended by a range of clinical and managerial staff, with differing degrees of authority, meaning that a variety of stakeholder views were shared, discussed and debated, allowing orientations toward dilemmas, traditions, and stories to be assessed across a multidisciplinary grouping.
Findings
In this section, we present two stylised vignettes concerning the planning and implementation of innovation respectively, which draw on interviews, non-participant observations, and documentary evidence relating to the innovation. We then apply three key ideas from Bevir’s work on network-based governance (dilemmas, traditions, stories) to the vignettes and also explore ideas about ‘shared practice’ or dialogical practice in explaining the empirical material.
Vignette 1: Deciding Whether to Roll Out Local Quality Improvement Work More Widely
Results are being shared from quality improvement work at one site within the Trust’s network of clinics. The consultant lead for the work at this site is presenting findings with other glaucoma consultants from across the Trust. Both senior and operational managers involved in the work are also sharing their views on the quality improvement work and contributing to the discussion. A representative from an external management consultancy that was employed to support the improvement work is also present. A multi-professional group from the hospital was established to reflect on the purpose and delivery of existing clinics. The improvement work involved mapping patient flows within different outpatient clinics at the site and experimenting with changes to patient flow and staff roles, before, during and after each clinic. The amount of time spent by each patient in the clinic, and what happened in this time, was measured. There was a new nurse ‘coordinator’ role that was used to allocate patients to different staff members. Rather than being allocated a list of patients, the consultant becomes a ‘floating resource’ available to advise on any patient’s care. This meeting is one in a number of events designed to gather consultants’ views that will be used to inform decision-making on rolling out this approach to quality improvement more widely within the Trust.
Vignette 2: Updating Front-Line Staff on the Quality Improvement Work
Members of the multidisciplinary team leading the improvement work are updating staff on progress at a clinical governance meeting at one of the Trust’s sites. The meeting is taking place in a large lecture theatre with rows of tiered seats. A formal presentation, with PowerPoint slides, is being used to give the update. The presentation, which is titled ‘transformation progress’, begins with an outline of the difficult times facing the NHS—chief among these, as described on the slide, include coping with demographic change, the need for financial savings, and responding to new commissioners and competitors. The presenter, an operational manager, also cites the Trust’s chief executive who had reportedly said: “it was time for a new approach”.
The presentation shares some of the principles being experimented with during the piloting of the new approach to delivering clinics, including ‘systems thinking’ (rather than focussing on individuals), minimising ‘handovers’ of patients among staff, telephoning patients prior to the clinic date to reduce those who ‘did not attend’ (DNA) appointments, and having a team briefing at the beginning of each clinic. The way that the pilot clinic operated was illustrated in a number of ways, including process maps of patient flow through the clinic, descriptions of how staff roles were performed within the clinics, and viewing each clinic in terms of profit and loss (although this was still being calculated), and the scheduling of patient appointments during the clinic.
Perceptions of how the pilot clinic had performed were then shared with the audience by members of the team. For example, it was noticeable that the lead consultant was being consulted a lot by other members of staff as ‘the expert’. Telephoning patients in advance had reduced the average DNA rate from 10–12 per clinic to 1–5. The clinics were also perceived to be ‘calmer’ in part due to the staff briefing at the beginning. The team did admit that only a small team had been involved in the transformation work and that others could be more involved in decision-making to avoid the current sense of change as a ‘process done to them, rather than with them’.
Interpretation: What’s the Dilemma?
Our observations suggested that the dilemma was related to overrunning outpatient clinics (the standard consultant-led clinics could overrun by up to two to three hours). Part of the reason that overrunning clinics had been a long-standing issue was because of the complexity of the problem. The complexity and intractability of the problem was acknowledged in the consultant meeting (vignette 1). In response to the consultant outlining the need for the service improvement work, the management consultant present chipped in by advocating the need for a thorough, deliberative approach because of the risk otherwise of ‘squeezing the balloon’ whereby one problem is solved and it pops up elsewhere. Another potential option raised at the consultant meeting was to introduce additional clinics. However, this was discounted because there was limited space for new clinics; additional clinics were already being offered on some evenings and on Saturdays.
Further ambiguity concerning the nature of the problem was introduced at the clinical governance meeting (vignette 2). Some frontline staff listening to the update on the improvement work queried the rationale for the changes to clinics. One doctor wanted to know, ‘what does success look like?’ The doctor argued that the background to the work describing challenges at Trust level was about ‘money’ rather than patient experience. They went on to suggest that, as a teaching hospital, there was a ‘tension between service and training’, and implying that the improvement work was having a negative impact on the latter. Were the changes more appropriate for independent sector treatment centres, that specialise in delivering more routine procedures, they posited. One of the management consultants responded by stating that the focus was on ‘value time’ whereby, he argued, if patients were seen more quickly, then this provided an opportunity to use the time in other ways, which could be seeing more patients or finishing the clinic at what could be considered a normal, reasonable time. The doctor responded by arguing that improvement work should not just be about benefiting patients, but also help to improve the workplace for staff. To underline his point, the doctor posed a rhetorical question to the wider audience, ‘when was the last time we had training in the lunch hour’? The management consultant responded by arguing that ‘improving morale’ was a benefit for staff and that making the Trust a great place to work also had a financial impact, e.g. reducing staff turnover can improve cost and revenue.
In summary, there was debate among front-line staff concerning the nature of the problem that the improvement was designed to address. However, given the variety of potential solutions, and differing views on the perceived efficacy of these, the challenges with the delivery of clinics can be seen as a ‘dilemma’. With regard to maintaining staff commitment to addressing the problem, representatives of the management consultancy played an important role in addressing concerns that front-line staff raised and by illustrating how the improvement work could be seen to address those, e.g. making the discursive link between improved staff morale and reducing cost.
Interpretation: What’s the Tradition?
There were traditions of inter- and intra-professional hierarchy. In the consultant meeting (vignette 1), staff had differing views on the new nurse ‘coordinator’ role that had been introduced to allocate patients to different members of staff across the clinic. Some nursing staff had taken to the role, others had not. The consultant leading the work suggested that a key issue was assertiveness among those in coordinator roles, that is, ‘can they tell doctors what to do, confidently?’ Those in the role were perceived to need particular capabilities, both clinical knowledge and a particular personality. It was suggested that it was not easy to find staff with ‘bossy nurse’ characteristics, and “with a matron’s hat”, another consultant added. Thus, while there was a suggestion that there was a lack of staff able to carry out the coordinator role, the challenge encountered of allocating patient cases to doctors also suggests underlying challenges associated with the negotiation of inter-professional relations. Hierarchy could also be invoked to support change, as illustrated by the reference to chief executive’s report endorsement of new ways of working by the operational manager in the clinical governance meeting (vignette 2).
There were traditions of resistance to change among staff. In the consultant meeting (vignette 1), the consultant leading the work suggested that resistance to changing work practices was not just an issue among doctors, but at all levels within the Trust. Another consultant responded with ‘that is normal’, seemingly questioning the idea that ‘resistance’ should be seen as problematic and as something that needed to be overcome. Thus, the two consultants agreed that ‘resistance’ existed and it could therefore be seen as a tradition within the Trust, but their views diverged on whether this was a ‘barrier’ to improvement work (first consultant) or that resistance should be seen as rational response to the changes being introduced (the second). In the clinical governance meeting (vignette 2), concerns were raised by staff about whether the changes would address concerns about staff training and the work environment. Resistance was also acknowledged as being understandable by the consultant leading the work because the changes being trialled could be perceived by some staff as a “process done to them”, especially where they were not involved in the initial discussions about making changes to the clinics.
There were also traditions of not sustaining change. One consultant stated in the consultant meeting (vignette 1) that, in response to managerial requests, they do make changes: “we do it, then it goes back to how it was”. This could be about change competing with traditional ways of working. For example, one staff member referred to an alternative approach to treating patients in which the ‘old mentality was get them in, get them out very quickly’.
There appeared to be interplay between the dilemma and traditions, in that traditions could be seen as playing a part in the dilemma of tackling overrunning outpatient clinics within the Trust. For example, the consultant leading the work appeared exasperated at times at the engagement of some staff with the improvement work. During the consultant meeting (vignette 1), the consultant stated that those involved “have to be open minded and go through this” and “have to challenge yourself about why changing process”. For example, the consultant argued that doctors should not be disengaging because they think that performing a particular diagnostic test within the clinic—one that measured visual acuity—“is beneath them”. Thus, the consultant’s statement could be interpreted as suggesting that staff needed to reflect on their own beliefs, on the reasons they had for holding those beliefs, and whether those reasons could be justified with regard to what was in patients’ interests.
In summary, we were able to distil through our observation of meetings a number of traditions that appeared to thwart the improvement activity. These point to a variety of professional responses to change, some of which can be linked to the approach to improvement (e.g. not sustaining improvement or involving staff sufficiently), others to inter and intra- professional power and hierarchy.
What’s the Story?
Multiple stories were told in relation to the dilemma of the overrunning clinics. Some stories were told about other settings outside the Trust. In response to concerns from a consultant about the lack of progress with addressing overrunning clinics over many years (vignette 1), a senior manager acknowledged that clinicians’ loyalty and commitment had been abused by management, adding that in other places where they have worked: “clinicians have called up management to tell patients in the waiting room why they can’t be seen after 5pm”. The reference to another workplace appeared to be used by the senior manager to underline the commitment of clinicians (i.e. in seeing the full list of patients even when clinics did overrun) in the current workplace. However, the consultant took issue with the sense that front-line staff were being held responsible for leaving work at the appropriate time (even in another workplace) and responded: “don’t blame clerks, it’s about the situation they’ve been put in”. The consultant then added that the problem for large clinics with a long list of patients was “firefighting”, with the consequence that it was “hard to make change”. The senior manager then responded that, for a period of time, they were interested in forgetting about demand and “deliberately running clinics to profile”. The consultant responds that they have “done it before and it works”.
Other stories were told to draw out the patient experience. In vignette 1, the consultant leading the work highlighted a quotation from a patient on their slide which summed up their experience of traditional clinics: “eye front, eye back, never the whole eye”. Another quote from a patient was used to highlight additional problems—in outlining these, the consultant adds that when staff undertaking the improvement work took a step back to reflect it was ‘quite shocking’. The quotes were supplemented with quantitative data collected by the management consultancy which suggested that patients spent 67% of their journey queuing. This information concerning the way that clinics had traditionally been run had affected patients was used to help build the case for change. There were then questions from members of the audience. For example, the approach of breaking the time spent by patients in clinics into ‘value’ versus ‘non-value’ time was questioned by some of the other staff present. They wanted to know what the two terms meant and, indeed, whether the activities allocated to ‘non-value’ time could accurately be described as a misuse of time. For instance, time spent by patients in between seeing clinicians could be necessary for eye drops to take effect.
Similarly, in the progress meeting with frontline staff (vignette 2), the purpose of the work was questioned by some staff especially with regard to the problem it was addressing. The management consultant present helped to turn the narrative back to one of ‘improvement’ in this setting by linking the objective of saving cost around another goal of improving staff working conditions, which a doctor had raised. In this context, it appeared easier for those leading the work to maintain a coherent narrative of improvement, relative to the consultant meeting (vignette 1) in which the approach to the work was fundamentally questioned.
In summary, stories were told through exchanges among the stakeholders present, with some appearing to become more accepted narratives, while others were challenged by alternative points of view or interpretations. There were examples of using evidence to add validity to particular stories (e.g. quotes from patients and time and motion studies to represent the patient experience), while others appeared to draw on authority to question alternative stories or reorient the narrative from their professional standing (e.g. senior doctors).
Individual Story or Joint Action?
The analysis of the vignettes suggests that stories, as well as traditions and dilemmas, are co-constructed. Stories are distributed across the spaces in which they are told. One utterance prompts other utterances; sometimes these appear to build upon the story being told, but more often than not these additions or qualifications take the story in unexpected directions. These movements both can amplify a story—to give it greater weight or credence in relation to the issue being discussed—or can work against the force of a story so its effect is dissipated or gets lost in the criss-crossing of dialogue. This raises the question of how and why some stories get heard—and appear to become influential—while others do not emerge or have less of an effect.
An important process in shaping the influence of stories appears to be the exercise of power. In the vignette, the tradition of inter- and intra-professional hierarchies within the Trust was noted as a mediator of responses to change or improvement activity. Such hierarchies can also influence the force with which stories are heard. In the meeting observed, it was consultants predominantly who sought to challenge both the other consultant leading the improvement work and the senior manager involved regarding the reasons for the problems with existing clinics and how the experiences with the new approaches to delivering clinics being trialled should be interpreted. Thus, power associated with occupying a senior role in the medical hierarchy was exercised in meetings to steer the stories that prevailed about the improvement work.
Discussion
How does decentred governance help us to understand innovation networks in health care? What does the concept of ‘joint action’ add, if anything, to this understanding? Decentred governance is about mechanisms that hold together, or coordinate, action over a distance (e.g. a network of outpatient clinics distributed across a metropolitan area). The empirical case study we used to explore decentred governance did not show strong tendencies toward coordination, that is, in addition to aspects of top-down organisation there were also aspects of autonomy among the organisations and agents involved in the delivery of this network of clinics. The stories, dilemmas, and traditions did not always add up, that is, they did not necessarily act as mechanisms of coordination.
Dilemmas were diffuse; they varied depending on who you spoke to and how they were negotiated in the course of social interaction. The sense of a ‘tradition’ was built on recognition of divisions within the Trust. There was a tradition of recognising these divisions and coping with them. This type of tradition could also be seen as a ‘dilemma’ given that they were not easily addressed. Stories were told to engage with the need for the improvement work, the approach being taken to improvement, and to evaluate progress or perceived success. Stories were co-constructed during interactions, suggesting that Shotter’s concept of ‘joint action’ is a useful way of describing how stories influence practice.
If story-telling is of a dialogical nature then this suggests greater ambiguity concerning its relationship to innovation processes. It means that the agency associated with story-telling is distributed beyond the individual story teller. This agency is held by others present who make contributions or interject, and through this, become co-authors of stories. Agency can also be attributed to the material context in which stories are told, including the particular space in which they are shared (which may contribute to a greater or lesser degree to interaction or debate that enables co-authorship) as well as the material resources that story-tellers draw on to lend authority, with examples including the use of audit findings, personal experiences of similar initiatives, and experiences gained in other organisations. Positional power also lends some participants greater authority to have their stories, or their views on others’ stories, heard.
The findings underlie the importance of medical professionalism, especially the practices of senior doctors, as a mediator of improvement processes (Best et al. 2012; Turner et al. 2016b). They highlight that an important mechanism through which senior doctors command power in relation to improvement processes is through their influence on the hum of narratives or stories that accompany improvement work. The prevailing stories that come to be associated with improvement work matter because they can influence decision-making concerning adoption or further spread. However, we can also see how other stakeholders such as management consultants attract credibility to their stories by drawing on ‘discursive resources’ (Bloomfield and Danieli 1995), including concepts that provide solutions to different dilemmas (e.g. ‘value time’), and by drawing on evidence from audit or research studies, including evidence of patient experience. This ability to attract discursive power around stories highlights an important facilitation role, whether this be management consultancy or other form of boundary spanner, that is able to counteract the positional power of senior doctors to ensure that other stories, and the voices they represent, are heard.
The approach outlined here also has methodological implications for practising ethnography. Firstly, the concept of stories, and other forms of interaction, being co-constructed rather than unilaterally constructed, should promote reflexivity concerning the collection of research ‘data’ for ethnography and what informs the analysis and writing up process. For example, the conduct of an interview or observation of a practice by the ethnographer shapes what happens during those interactions, including the ‘stories’ told. For example, one of the authors was collecting data within a hospital on ward-level responses to a medication safety ‘scorecard’ over a number of weeks as part of broader university and health care provider collaboration on patient safety. On arriving one week to share the data, a senior doctor said jokingly, ‘every time I see you my heart sinks’. This jibe could be interpreted in numerous ways (e.g. as a sign of general resource pressures, as a comment on the appropriateness of the ‘scorecard’, or as an attempt at humour or conviviality), but we include this example to highlight that the ethnographer is not invisible; their very presence, and research methods, influence practice in the field and should be recognised as a key part of the ‘stories’ being told.
Moreover, the ways in which those stories are retold by the ethnographer will be influenced by other factors, including their particular research question or hypothesis, reading material, conversations with colleagues, the presence of other corroborating or contradictory data, and the ethnographer’s style of writing and how ideas translate into a discursive argument that flows (or not) on the page. The apparatus of writing—and how this is informed by social and material interactions—should be explicit in accounts of ethnography, especially if insights from this approach to research are designed to inform future policy or practice.
Secondly, in attempting to describe the mechanisms underpinning innovations, there can be pressure to develop a coherent story or narrative of both the important events that were associated with the planning and implementation of the innovation and of the critical mechanisms that were influential in the empirical data that was collected. The mechanisms could vary depending on the hypothesis in which one is interested, and what is already known about the role of such mechanisms from previous research (e.g. how powerful stakeholders shape evidence use or how organisational culture might influence receptivity to innovations) and whether this is confirmed or better understood by the data collected. However, if we were to accept that stories are constructed, and such construction varies depending on who is involved, what is observed, and how such observations are rationalised into ‘stories’, then the story of innovation being told looks more precarious, arbitrary perhaps. It becomes more difficult to argue that the data highlights an empirical reality about innovation and, consequently, says something meaningful about “mechanisms” of innovation processes. The messy, co-construction of stories about practice suggests a need to hold back from mechanistic accounts of innovation and overly rationalised descriptions or interpretations of the accompanying interactions. Ethnographic findings, alone, are likely to be accused of being subjective and reliant on subjectivities. One way of addressing this is to combine ethnography with other methods of research, e.g. quantitative findings that add another layer to the story.
Conclusion
In conclusion, a decentred conception of governance represents a useful approach for analysing how a range of stakeholders make sense of and can help to shape innovation processes. This approach can complement more top-down perspectives of governance by showing how local actors play an important role in the negotiation of innovation processes. However, our analysis suggested that the decentred mechanisms through which innovations undergo triall and implementation are often not attributable to individuals’ stories—instead, such stories are co-constructed through social practice. Due to their co-construction, the information or perspective conveyed through such stories is dependent on the context in which they are told and the influence of the actors present who shape the telling of stories. In order to understand the influence of stories on innovation processes, it is important to admit a role for power in understanding how and why some stories carry influence, while others may be marginalised. The inclusion of power in the analysis also helps to develop Shotter’s concept of social practice as ‘joint action’ by highlighting that, while the formative influences on thought and behaviour are distributed and dependent on the context of interaction, the distribution of power plays an important role in shaping these.
References
Best, A., Greenhalgh, T., Lewis, S., Saul, J. E., Carroll, S., & Bitz, J. (2012). Large-system transformation in health care: A realist review. Milbank Quarterly, 90(3), 421–456.
Bevir, M.,& Richards, D. (2009a). Decentring policy networks: A theoretical agenda. Public administration, 87(1), 3–14.
Bevir, M., & Richards, D. (2009b). Decentring policy networks: Lessons and prospects. Public Administration, 87(1), 132–141.
Bevir, M., & Waring, J. (Ed.). (2018). Decentring health policy: Learning from British experiences in healthcare governance. London: Routledge.
Bloomfield, B. P., & Danieli, A. (1995). The role of management consultants in the development of information technology: The indissoluble nature of socio-political and technical skills. Journal of Management Studies, 32(1), 23–46.
Boje, D. M. (1991). The storytelling organization: A study of story performance in an office-supply firm. Administrative Science Quarterly, 36(1), 106–126.
Cameron, A., Lart, R., Bostock, L., & Coomber, C. (2014). Factors that promote and hinder joint and integrated working between health and social care services: A review of research literature. Health and Social Care in the Community, 22(3), 225–233.
Lipsky, M. (1971). Street-level bureaucracy and the analysis of urban reform. Urban Affairs Quarterly, 6(4), 391–409.
National Institute for Health and Clinical Excellence. (2009, April). Glaucoma diagnosis and management of chronic open angle glaucoma and ocular hypertension, NICE clinical guideline 85.
National Patient Safety Agency. (2009). Rapid response report NPSA/2009/RRR004: Preventing delay to follow up for patients with glaucoma. Available at https://www.rcophth.ac.uk/wp-content/uploads/2015/01/NPSA_RRR_on_glaucoma_2009_supporting_info.pdf. Accessed 7 April 2019.
Schumpeter, J. A. (1934). The theory of economic development. Cambridge, MA: Harvard University Press.
Shotter, J. (1993). Cultural politics of everyday life: Social constructionism, rhetoric and knowing of the third kind. Toronto, ON: University of Toronto Press.
Shotter, J. (1997). Dialogical realities: The ordinary, the everyday, and other strange new worlds. Journal for the Theory of Social Behaviour, 27(2–3), 345–357.
Shotter, J. (2010). Situated dialogic action research: Disclosing ‘‘beginnings’’ for innovative change in organizations. Organizational Research Methods, 13(2), 268–285.
Turner, S., Goulding, L., Denis, J. L., McDonald, R., & Fulop, N. J. (2016a). Major system change: A management and organisational research perspective. In Raine, R., Fitzpatrick, R., Barratt, H., Bevan, G., Black, N., Boaden, R. et al. Challenges, solutions and future directions in the evaluation of service innovations in health care and public health. Health Services and Delivery Research, 4(16), 85–104.
Turner, S., Ramsay, A., Perry, C., Boaden, R., McKevitt, C., Morris, S. et al. (2016b). Lessons for major system change: Centralization of stroke services in two metropolitan areas of England. Journal of health services research & policy, 21(3), 156–165.
Van de Ven, A. H. (2017). The innovation journey: You can’t control it, but you can learn to maneuver it. Innovation, 19(1), 39–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 The Author(s)
About this chapter

Cite this chapter
Turner, S., Wright, J.S.F. (2020). Sharing Stories or Co-Constructing Practice? Challenges to Undertaking and Researching Innovation Using Evidence from the English NHS. In: Bevir, M., Waring, J. (eds) Decentring Health and Care Networks. Organizational Behaviour in Healthcare. Palgrave Macmillan, Cham. https://doi.org/10.1007/978-3-030-40889-3_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-40889-3_7
Published:
Publisher Name: Palgrave Macmillan, Cham
Print ISBN: 978-3-030-40888-6
Online ISBN: 978-3-030-40889-3
eBook Packages: Business and ManagementBusiness and Management (R0)