
Abstract
The human oral cavity is colonized by one of the densest bacterial communities on the planet, with consistent microbial composition throughout life and in response to perturbations such as tooth cleaning. The oral microbiome has important associations with health in the context of gingivitis and even heart disease and preterm birth. In this chapter, we will provide an overview of what is known about the human oral microbiome, starting from the first glimpse of microbes when van Leeuwenhoek looked at his own oral microbes with the first microscope, to recent expansion of knowledge with both high-throughput sequencing and microscopy. We will describe what is known about healthy oral microbial communities, including how they develop in childhood and become shared within families and others who cohabitate, and how the biogeographic and biophysical forces drive construction of largely anaerobic microbial communities unique to each tooth. Finally, we touch on what is known about health-and disease-associated human oral microbial communities and briefly discuss the potential for using saliva samples to monitor health.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Saliva comprises millions or billions of human and microbial cells along with molecules and proteins of various sizes. Salivary microbes are contributed from a variety of intraoral surfaces; there are about a thousand different kinds of bacteria in an average healthy mouth (Lazarevic, Whiteson, Francois, & Schrenzel, 2011), and more bacteria in one person’s mouth than people on the Earth. The study of microbes living in our mouths began with the birth of microbiology, when in the late 1600s Antonie van Leeuwenhoek first observed a microbe in his dental plaque scrapings with a home-made microscope. Since that time, microbiologists have developed numerous methods for isolating and characterizing the microbes inhabiting the oral cavity. These centuries of research have taught us that oral microbial communities are dominated by Bacteria, along with their viruses, known as bacteriophages, and with some Archaea and Fungi. Oral microbial communities include a surprising proportion of anaerobic bacteria, are some of the most densely situated and most diverse communities on Earth, do not typically support pathogenic microbes, and sustain themselves through an incredible diversity of metabolisms.
Characterizing the interactions of oral microbes with each other and the human host is essential for improving oral and overall health, and offers a window into the functioning of one of the most diverse ecosystems on Earth. Fortunately, oral microbes can usually be studied with noninvasive sampling by swab or saliva collection, which provides aggregate material from the microhabitats within the oral cavity and is easily accessible and obtainable.
In this chapter, we will discuss the microbes and molecules found in the human oral cavity, along with the historical and modern approaches used to study them. We then look at the structure of oral microbial communities at several scales, starting from a single microbial cell on a tooth and then zooming out to view the oral microbial communities in individual people, families, and within a geographic region. Finally, we touch on the ways in which oral microbes influence our general health, and whether manipulating oral communities is feasible.
2 Methods for Sampling and Studying the Microbiome and Metabolome in Saliva
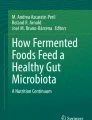
Since van Leeuwenhoek’s first glimpse at oral microbes in the 1600s, sophisticated methods have been developed to sample and examine both live and dead microbes that reside in the oral cavity. Of particular importance is the development of culture techniques that enable isolation and study of anaerobic bacteria, and the development of high-throughput DNA sequencing methods for culture-independent identification of microbes (Fig. 7.1).

Timeline of milestones in oral microbiology. Beginning at the top in the 1600s and finishing in the present, major advances in the detection and characterization of microbes are shown. The top of the timeline focuses on the first microbiologists who invented some of the techniques still used today. Following in their footsteps were several major technological advances that enabled detection of microbes that had previously been elusive (e.g., anaerobes or other difficult to culture bacteria). Finally, the bottom of the timeline shows multinational collaborations formed to produce and house unprecedented levels of -omics data. Bars in the timeline are not to scale. Illustration credit: Dr. Eliza Wolfson (https://lizawolfson.co.uk)
Sampling Microbes in Saliva and Plaque
Saliva and dental plaque are the most common samples obtained for studies of oral microbes. Saliva sampling is easier to carry out and is preferred in situations where teeth are not present (edentulous infants or adults) or when training someone to take a dental plaque sample consistently is not feasible. Saliva includes a mix of microbes contributed from several distinct niches in the oral cavity, along with others that arrive with food or drink. For this reason, saliva is sometimes considered a less stable sample. [However, in comparison to fecal microbiomes, saliva microbiomes are relatively stable (David et al., 2014)]. Tooth surfaces offer microbes more permanent and distinct microenvironments that are dictated by local conditions, especially steep gradients of oxygen and pH. The human intraoral cavity maintains a steady temperature (~34 °C, with some distinct daily circadian patterns as shown in Choi, Lyons, Kieser, & Waddell, 2017); microbes in saliva experience greater mixing, which may lead to more continuous access to nutrients and fewer extremes of oxygen and pH. Physical and chemical conditions, combined with the characteristics of the microbes themselves, provide ample opportunities for individual cells to aggregate into clumps and/or adhere to the tooth surface directly or on top of other microbes that were already there. This aggregation and adhesion provide variation in physical structuring that enables niche formation and additional microbes to join the community.
2.1 Studying Oral Microbes Through Culturing
The ability to isolate and grow one microbial strain or species at a time was essential for the development of microbial culturing methods by Robert Koch and others, and has formed the foundation of clinical microbiology since the late 1800s. The agar plates developed by Fannie Hesse (in Koch’s laboratory) inspired by agar containing desserts from Indonesia, a Dutch colony at the time, are still standard in modern clinical microbiology labs in hospitals worldwide. In the early 1900s techniques were developed to culture anaerobic bacteria, which greatly facilitated the study of oral microbes (Finegold, 1993).
Although agar plate culturing has been essential for our current understanding of microbiology, and in fact large numbers of the microbes found in saliva can be cultured on them, it only works for a small fraction of microbes, and has thus biased our view of the microscopic world. For example, when a physician takes an oral swab to search for the cause of Strep throat, the swab contents are then spread on an agar plate designed to favor the growth of a particular pathogen. For these clinical microbiology tests, it is necessary to eliminate the “background signal” of bacteria that are nonpathogenic so that the physician can identify the infecting pathogen and treat their patient. For this reason, many bacteria in saliva had been overlooked, particularly those with fastidious nutritional requirements and anaerobes unable to survive even small amounts of oxygen exposure. In recent years, we have significantly improved culturing techniques in order to grow more of the microbes that inhabit the human body (Browne et al., 2016; Sibley et al., 2011).
Instead of the iconic culture flask or petri dish used to isolate a single strain of microbe, many investigators are improving culture models to closely mimic the structure of the oral cavity. One important component is to offer the microbes naturally occurring gradients of pH, oxygen, and nutrients, which have been shown to affect transcription and production of metabolites in oral microbes (Edlund et al., 2015; McLean et al., 2012). These gradients have been recreated in a fermentation model that uses rotating disks in rich media, which were then inoculated with pooled saliva samples; the microbes eventually formed stable and diverse populations (Hope & Wilson, 2006).
Another important aspect of culture is to offer conditions that promote the formation of biofilms, which are polysaccharide and protein-rich matrices that offer bacteria a structured environment; biofilms are a natural state for many oral microbes, e.g., plaque is biofilm. Classic biofilm culturing has relied on bacteria adhering to the walls in plastic 96-well plates. This method works for some bacterial types, such as Pseudomonas aeruginosa (O’toole & Kolter, 1998). However, some strains do not attach to a surface, but rather form small aggregates, which are hard to study in a surface attachment assay. New efforts to allow biofilms and aggregates of cells to form have been shown to recreate physiologically relevant gradients of oxygen and pH (Sonderholm et al., 2018).
Finally, efficiency is a key to making progress with culturing. Anna Edlund at the Craig Venter Institute has a higher throughput and well-characterized oral microbiome model culture system with saliva pooled from 10 people and growing in 96-well plates (Edlund et al., 2013). This system produced highly replicable data and enabled culturing of stable oral communities in biofilms, including many taxa that were previously considered unculturable.
2.2 Studying Oral Microbes Through Culture-Independent Approaches
The discrepancy between what we routinely grow in the lab and the diversity of microbes observed in the native environment has been referred to as the “great plate anomaly” by environmental microbiologists since the mid-twentieth century. Scientists would observe enormous numbers of microbes in a natural sample, but only a few would grow on an agar plate in the lab. Attempting multiple culturing techniques was sometimes successful, but it was the revolution in DNA sequencing capacity that truly enabled our current high-tech inventories of the thousands of microbes living in saliva. In this section, we describe what we have learned from such high-throughput approaches that provide a relatively unbiased view of the microbes.
Omics
While sequencing the first human genome in the late twentieth century took multiple governments and nearly a billion dollars (National Human Genome Institute, 2016), today it requires only a desktop machine and hundreds of dollars. Indeed, new high-throughput sequencing methods have reduced the cost and time investment requirements at rates that surpass even the pace of improvements in computing power (Muir et al., 2016; Wetterstrand, 2019). Some of our most important glimpses at oral microbial communities came from DNA sequencing. Most of the data have come from amplicon sequencing, where a segment of a universal bacterial gene (the 16S rRNA gene) is targeted and sequenced from each bacterial genome in a sample. The resultant hundreds to millions of sequences are then analyzed to identify, and infer abundances for, the bacteria present, and to infer characteristics of the community’s ecology using statistics. Amplicon-based approaches have also been used to identify Fungi and Archaea in oral samples, but do not work for viruses, as there are no universal viral genes. Instead, viruses are usually physically separated from the rest of the sample using filtration or density gradient ultracentrifugation, and then all the viral DNA is sequenced (Reyes, Semenkovich, Whiteson, Rohwer, & Gordon, 2012). Note that sequencing all of the DNA in microbial communities is also a commonly used approach for identifying all microorganisms present and inferring their functional or metabolic abilities (Belda-Ferre et al., 2012).
16S rRNA sequencing has shown us that saliva in most people includes Streptococcus, among other facultative anaerobes such as Rothia mucilaginosa, and also a diversity of anaerobic bacteria, including Prevotella, Veillonella, and Gemella (Human Microbiome Project, 2012; Lazarevic, Whiteson, Hernandez, Francois, & Schrenzel, 2010; Lim, Totsika, Morrison, & Punyadeera, 2017; Stahringer et al., 2012). Large comparative studies have shown that the resilience of oral communities after antibiotic treatment is high, and that saliva communities are less affected by antibiotics than gut communities (Zaura et al., 2015). In one study of more than 2000 Japanese adults, oral microbiomes were found to cluster into two main types that are associated with overall health, and confirm the widespread nature of the observations made to date with regard to the typical composition of bacteria in saliva, dominated by Streptococcus spp. and other facultative anaerobes (Takeshita et al., 2016).
Fungi frequently found (through ITS amplicon sequencing) include members of the genera Candida and Aspergillus (Ghannoum et al., 2010; Peters, Wu, Hayes, & Ahn, 2017), though a diversity of fungi were present in all sampled individuals. Fungal diversity or phyla present do not seem to vary with oral health (Peters et al., 2017). Archaea are also present, although they may be more common in cases of reduced immune health (Lepp et al., 2004).
Microscopy
Although microscopy was the first method used for examining bacteria and other microorganisms, it is normally hindered by the limited morphological differences between bacterial taxa. However, new microscopy methods that combine nucleic acid-binding fluorescent probes with confocal microscopy have quickly propelled microscopy to the forefront of microbiome research. Microscopy allows us to examine the physical structure, or biogeography, of microbial communities to see which cells are neighbors and whether cells are organized or random (discussed more in the next section). For example, Kolenbrander (Kolenbrander, 2011) used confocal microscopy to follow colonization dynamics of bacteria growing in flow cells with saliva as their only nutrient source.
Metabolomics
Saliva comprises small molecules/metabolites produced by the microbes and human host. Over a thousand such molecules have been identified with a variety of methods, including NMR, GC–MS and LC–MS, and they are profiled in the Saliva Metabolome Database (Dame et al., 2015). The saliva metabolome is a promising tool for disease diagnosis and health monitoring; biomarkers in saliva have been identified for many diseases or conditions, including diabetes, dementia, and cancer (Barnes et al., 2014; Figueira et al., 2016; Ishikawa et al., 2016). The importance and promise of using saliva metabolomes to inform clinical research is evidenced by the NIH Common Fund Metabolomics Program, which supports a metabolome database and multiple institutes for generating metabolomics data.
In summary, culture-dependent and culture-independent methods have provided the identities of microbes that live in the oral cavity, resulting in a catalog of species that are commonly found and maintained throughout an individual’s life. Some of the metabolites produced by these microbes are also being investigated. These studies have resulted in the creation of several public repositories of data related to oral microbes. The expanded HOMD includes genomic and taxonomic information for over 700 microbial species detected in the oral cavity, pharynx, nasal passages, sinuses, and esophagus (Chen et al., 2010; Escapa et al., 2018). The Human Microbiome Project includes amplicon sequence data, shotgun metagenomic sequence data, and a repository of bacterial cultures that can be requested (Human Microbiome Project, 2012). The Oral Microbe Bank of China (OMBC) (Xian et al., 2018) houses hundreds of bacterial strains and human samples, both available for research purposes.
Box 7.1 Sampling and Processing Saliva: Tips and Best Practices
Standardization of sampling and methods is an important priority in the microbiome and metabolome fields (Knight et al., 2018). This is because DNA, RNA, metabolites, or even whole cells, are often altered upon sample storage. Decisions about the strategy for sample collection, storage, processing, and analysis can all alter the downstream results. During the early days of the human microbiome project, samples were processed and sequenced at four facilities, and the biggest signal in the early datasets emerged as the core facility and processing methods, rather than anything biological. Batch effects are still important, as are positive and negative controls. Comparisons of each step in the process of saliva analysis suggest that the earlier experimental steps, such as DNA extraction from saliva samples, have a bigger impact on the resulting data than later data processing steps (Lazarevic, Gaia, Girard, Francois, & Schrenzel, 2013). Regular meetings have been held at the National Institute of Standards and Technology, where an International Metagenomics and Microbiome Standards Alliance (IMMSA, 2019) has been established (Standards).
The top considerations when characterizing the salivary microbiome and metabolome include:
-
1.
Keep everything consistent within a batch of samples that will be compared to one another. This includes sample collection timing, method, storage, and processing. Several studies suggest abstaining from food or drink for 1 h before collecting saliva, and collecting at the same time of day, usually in the morning (Dame et al., 2015; Lazarevic et al., 2010, 2011, 2013; Lim et al., 2017). Lim et al. (2017), show that food or drink does not affect DNA quality and quantity. Although optimal microbiome and metabolome focused saliva collection times have not been established, microbiome profiles are quite consistent for an individual over the course of months to years (David et al., 2014; Human Microbiome Project Consortium, 2012; Lazarevic et al., 2010). Standardized collection kits for passive drool or swabs are available—it is important to save the entire swab and not just the flow through, because several common swabbing materials trap microbes.
-
2.
Saliva collected with the intention of sequencing microbial DNA can be stored in a commercially available nucleic acid preservation buffer that will be frozen, preferably within 1 h of collection. For metabolomics, there are not commercial buffers to preserve metabolome composition at room temperature, and freezing the samples within an hour is the gold standard. Limited storage studies with similar samples, such as sputum from Cystic Fibrosis patients, have shown that metabolome composition shifts significantly within a few hours of storage at 4 °C (Wandro, Carmody, Gallagher, Lipuma, & Whiteson, 2017).
-
3.
Including positive and negative controls, along with batch controls. Running blank samples using the same collection tubes and reagents to understand the background, especially for microbiome samples that will include DNA amplification steps, is more important for very low abundance samples. Saliva is densely colonized by microbes, but negative controls are still an important way to understand the background. Positive controls with known mixtures of microbes are commercially available and can be included with each batch. In a big study with many batches, making many aliquots of a large pooled representative sample that can be stored and included in every batch will allow for some comparison across batches.
3 Biogeography of Microbial Communities of the Oral Cavity
While most studies of the oral microbiome have relied on saliva samples, there are a few studies using 16S rRNA amplicon sequencing or microscopy that have highlighted the variability in microbial communities at several scales. Examining where particular species or genera of bacteria reside in comparison to others, i.e., their biogeography, is the first step to using these oral communities as signatures of health or markers of disease.
Structured microbial communities form around a single tooth
Mark Welch, Rossetti, Rieken, Dewhirst, and Borisy (2016) used fluorescently tagged bacteria and confocal microscopy to determine the structure of bacteria living in dental plaque. They found that filamentous cells of Corynebacteria, which formed central pillars, and nine other bacterial species radially emanated from the tooth surface (Fig. 7.2). The positions of these species suggested that this environment was structured according to each species’ niche, as oxygen and carbon sources used by particular species could predict their position in the plaque (e.g., anaerobes were furthest from the surface).

Architecture of the oral microbiome at different scales. Variation in microbial communities at differing scales. Beginning at the top in the oral cavity, levels of diversity are represented by orange circles. The tooth inset shows the organization of bacterial cells of different species based on microscopy data from Mark Welch et al. (2016). In the middle, diversity levels within an individual and variation in community diversity between individuals are shown with orange and blue circles, respectively. At the bottom, variation in community diversity between individuals of a family unit, a local population, and global populations are indicated by blue circles. Illustration credit: Dr. Eliza Wolfson (https://lizawolfson.co.uk)
Tooth by Tooth Environment
Each tooth has its own microbial community and which microbes are present depends most on type of tooth (e.g., molar versus incisor), though other things that could affect community structure included whether the buccal or lingual side of the tooth was sampled, and distance from submandibular/sublingual glands (Callahan, Proctor, Relman, Fukuyama, & Holmes, 2016; Proctor et al., 2018; Proctor & Relman, 2017). An ecological gradient from the front to the back of mouth has also been revealed (Proctor et al., 2018). Along this gradient microbial communities varied on teeth, mucosa (buccal and alveolar), and keratinized gingiva according to their anterior–posterior position. Moreover, evidence indicated that the flow of saliva was at least partly responsible for gradient structure (Proctor et al., 2018).
Colonization of the Oral Cavity
Although still a very active research field, current data suggest that in young infants, environmental and physiochemical conditions, perhaps even mode of delivery, select for oral microbes (Costello et al., 2009; Holgerson et al., 2013). Breastfed babies usually have Lactobacilli in their oral microbial communities (Vestman et al., 2013). In general, younger babies have oral microbiota similar to their mother’s skin or breast milk, and then as babies age, phyla such as Fusobacteria and the potentially pathogenic TM7 colonize. Once mature, Neisseria, Rothia, S. mutans, and others (Bik et al., 2010; Contreras et al., 2010; Lazarevic et al., 2010) follow and this mature community remains relatively stable (Rasiah, Wong, Anderson, & Sissons, 2005).
Nature Versus Nurture and Oral Microbiota
Multiple groups have tried to understand whether oral communities are predicted by human genetics or whether other factors are more important. Stahringer et al. (2012) profiled the bacteria living in over 200 saliva samples, including some taken longitudinally and from twins, and found that similarities in saliva bacteria were more accurately predicted by a shared environment than genetics. Gomez et al. (2017) compared the oral bacteria in dizygotic or monozygotic twins and showed that although genetics predicted the presence of a few bacterial species, there was a strong environmental component particularly with respect to cariogenic bacteria. When these cariogenic bacteria increased in frequency (due to sugar consumption), other genetically determined bacteria decreased in frequency. Shaw et al. (2017) looked at family units that were cohabiting and found that cohabitation was the strongest predictor of oral microbial communities. This is consistent with results from other studies that found that sharing households was associated with very similar oral microbiota (e.g., Abeles et al., 2016; Song et al., 2013). Cohabitation was also associated with similar bacteriophage communities (Ly et al., 2016). Not surprisingly, diet plays a strong role in community composition (Hansen et al., 2018).
Global and Ethnic Differences in the Oral Microbiota
Four ethnic groups in the USA were shown to have specific bacterial signatures in their oral microbiomes; the distinct saliva microbiomes of Caucasian and African-Americans who shared a longer history of US diet and lifestyle heritage (in comparison to Chinese and Latino saliva donors who more recently immigrated to the USA) suggested that this was not due to environmental or dietary differences alone, although this is difficult to disentangle (Mason, Nagaraja, Camerlengo, Joshi, & Kumar, 2013). Thus, although within an ethnic group there is a weak influence of genetics on oral microbiota (e.g., twin study discussed above), comparisons between ethnic groups suggest that genetics may play some broader role. For example, Gupta, Paul, and Dutta (2017) suggested that differences in root and tooth morphologies and innate immunity between ethnic groups, and hunter-gatherer versus urban lifestyles, may influence which microbes can colonize and persist in the oral cavity.
Individuality
However, despite these comparisons at many levels, i.e., between twins, cohabiting relatives or strangers, and ethnic groups across the globe, the most important source of variation in any microbiome or metabolome study comes from which individual the sample was taken from. For example, Mukherjee, Beall, Griffen, and Leys (2018) showed that oral microbiomes are highly personalized. Although each person’s oral microbiome did change over the year, they resulted in differences that were minimal compared to the differences between individuals. Thus, for studies that involve oral bacteria, carrying out cross-sectional studies is difficult because each individual is quite unique. This point reiterates the importance of having baseline samples as part of a longitudinal study.
4 The Oral Microbiota’s Influence on Overall Health
Two major conceptual advances regarding oral microbes have occurred in the last few decades. First, doctors are beginning to understand that disease may be caused by a change in community structure, rather than the presence of an individual pathogen. In other words, Koch’s postulates are not applicable to all infectious diseases. Second, we have recently begun to understand how oral health affects our overall health. There is reasonable evidence that oral microbes can enter the bloodstream via lesions in the oral cavity (associated with periodontitis) and then travel to various regions in the body (e.g., blood vessels, placenta, and colon). Oral microbes may also travel through inhalation (to the lungs) and swallowing (to the stomach/gut). Once these oral microbes arrive in their new home, they can significantly affect health.
Streptococcus species are a major cause of dental caries, along with a collection of other microbes (Belda-Ferre et al., 2012). These bacteria cause caries by consuming dietary sugar and producing acids that degrade tooth enamel. Inflammation of the gums (i.e., gingivitis, which can progress to periodontitis) is also typically a response to the bacterial biofilms lining the teeth. The cause of periodontitis was originally attributed to shifts in all microbes or due to infection by individual pathogens. However, investigations into oral communities of microbes have resulted in an ecological model of caries and periodontitis (reviewed in Kilian et al., 2016) where complex microbial communities interact with the immune system and dietary factors to eventually determine oral health.
In addition to the obvious influence of oral microbes on caries and periodontitis, these microbes and/or their associated oral diseases have been shown to affect overall health. For example, periodontitis is associated with progression to cardiovascular disease (Leishman, Do, & Ford, 2010), preterm and low birth weight (Puertas et al., 2018). Abundances of Veillonella and Streptococcus in atherosclerotic plaque correlated with their oral abundances (Koren et al., 2011). The presence of specific oral microbes may eventually be a useful predictor of atherosclerosis (Chhibber-Goel et al., 2016); however, at this point, more data are needed.
Oral bacteria have also been shown to colonize the intestines, which can cause issues in individuals with IBD (Atarashi et al., 2017) or colon cancer (Flynn, Baxter, & Schloss, 2016). In individuals with colon cancer, biofilms described as “oral-like” were identified on the colonic mucosa (Flemer et al., 2018). Finally, respiratory infections are also affected by oral microbes. Half of all cases of pneumonia have oral etiology (Yamasaki et al., 2013), and the proximity of the densely colonized oral cavity to the airways has important implications, especially when immune health and airway clearance are compromised. Part of health is maintaining distinct microbial communities in different parts of the oropharynx and the airways. Aging and alcoholism have both been shown to lead to blurred microbial communities (Samuelson et al., 2018; Thevaranjan et al., 2018), where the oropharynx and the nasopharynx, for example, are no longer distinct.
The diversity of microbes present in and on the human body may be important for health, although defining the composition and diversity of a microbiome that promotes health is still an underexplored frontier. In some regions of the body, for example, in the gut, greater microbial diversity is associated with health. This also appears to be the case for the distinct communities of microbes colonizing dental plaque in the oral cavity, where increased diversity was found in healthy individuals compared to those with caries (Espinoza et al., 2018). However, in saliva, the opposite has been found to be true, where greater diversity is associated with gingivitis (Takeshita et al., 2016).
5 Summary of Current Knowledge and a Look to the Future
In summary, the oral microbiome is a diverse population of microbes that live in various niches within the oral cavity. Often the community of microbes is specific for each individual, and cohabiting individuals tend to share many oral microbes. Saliva samples are accessible, and have contributed to our knowledge of oral microbes, in addition to samples of dental plaque and other oral specimens.
Although we have learned a lot since Antonie van Leeuwenhoek first gazed at his oral microbes under the microscope, there is still much to learn. First, we have a good idea of which bacteria are common oral inhabitants, but we know less about what these diverse organisms are doing in the mouth and whether they are beneficial, detrimental, or neutral, and if their roles change as health improves or declines. Second, associations between the presence of particular microbes and health need to be better understood. Improved culturing, high-throughput sequencing, metabolic analyses, and microscopy will no doubt enable a deeper look into these associations to tease apart correlation and causation. Third, as we identify particular microbes that have a significant role in oral or overall health, we can begin to manipulate their abundances to improve health. Saliva will no doubt play a crucial role in all of these future endeavors.
Definitions of key terms:
-
Microbiome: The microbes living in a given environment, including viruses, bacteria, archaea, and small eukaryotes.
-
Metabolome: The metabolites produced by all organisms living in a given environment.
-
16S rRNA gene: A gene that is highly conserved in all organisms and is often amplified and sequenced to identify microorganisms. It is the gene most often used for culture-independent study of microbial communities.
-
Metagenome: All of the genes encoded by the organisms living in a given environment.
-
High-throughput sequencing: DNA sequencing technologies that produce large amounts of sequence data in short amounts of time. These technologies are typically much lower in cost than earlier methods.
References
Abeles, S. R., Jones, M. B., Santiago-Rodriguez, T. M., Ly, M., Klitgord, N., Yooseph, S., … Pride, D. T. (2016). Microbial diversity in individuals and their household contacts following typical antibiotic courses. Microbiome, 4, 39.
Atarashi, K., Suda, W., Luo, C., Kawaguchi, T., Motoo, I., Narushima, S., … Honda, K. (2017). Ectopic colonization of oral bacteria in the intestine drives TH1 cell induction and inflammation. Science, 358, 359–365.
Barnes, V. M., Kennedy, A. D., Panagakos, F., Devizio, W., Trivedi, H. M., Jonsson, T., … Scannapieco, F. A. (2014). Global metabolomic analysis of human saliva and plasma from healthy and diabetic subjects, with and without periodontal disease. PLoS One, 9, e105181.
Belda-Ferre, P., Alcaraz, L. D., Cabrera-RUBIO, R., Romero, H., Simon-Soro, A., Pignatelli, M., & Mira, A. (2012). The oral metagenome in health and disease. The ISME Journal, 6, 46–56.
Bik, E. M., Long, C. D., Armitage, G. C., Loomer, P., Emerson, J., Mongodin, E. F., … Relman, D. A. (2010). Bacterial diversity in the oral cavity of 10 healthy individuals. The ISME Journal, 4, 962–974.
Browne, H. P., Forster, S. C., Anonye, B. O., Kumar, N., Neville, B. A., Stares, M. D., … Lawley, T. D. (2016). Culturing of ‘unculturable’ human microbiota reveals novel taxa and extensive sporulation. Nature, 533, 543–546.
Callahan, B., Proctor, D., Relman, D., Fukuyama, J., & Holmes, S. (2016). Reproducible research workflow in R for the analysis of personalized human microbiome data. Pacific Symposium on Biocomputing, 21, 183–194.
Chen, T., Yu, W. H., Izard, J., Baranova, O. V., Lakshmanan, A., & Dewhirst, F. E. (2010). The Human Oral Microbiome Database: a web accessible resource for investigating oral microbe taxonomic and genomic information. Database (Oxford), 2010, baq013.
Chhibber-Goel, J., Singhal, V., Bhowmik, D., Vivek, R., Parakh, N., Bhargava, B., & Sharma, A. (2016). Linkages between oral commensal bacteria and atherosclerotic plaques in coronary artery disease patients. NPJ Biofilms Microbiomes, 2, 7.
Choi, J. E., Lyons, K. M., Kieser, J. A., & Waddell, N. J. (2017). Diurnal variation of intraoral pH and temperature. BDJ Open, 3, 17015.
Contreras, M., Costello, E. K., Hidalgo, G., Magris, M., Knight, R., & Dominguez-Bello, M. G. (2010). The bacterial microbiota in the oral mucosa of rural Amerindians. Microbiology, 156, 3282–3287.
Costello, E. K., Lauber, C. L., Hamady, M., Fierer, N., Gordon, J. I., & Knight, R. (2009). Bacterial community variation in human body habitats across space and time. Science, 326, 1694–1697.
Dame, Z. T., Aziat, F., Mandal, R., Krishnamurthy, R., Bouatra, S., Borzouie, S., … Wishart, D. S. (2015). The human saliva metabolome. Metabolomics, 11, 1864–1883.
David, L. A., Materna, A. C., Friedman, J., Campos-Baptista, M. I., Blackburn, M. C., Perrotta, A., … Alm, E. J. (2014). Host lifestyle affects human microbiota on daily timescales. Genome Biology, 15, R89.
Edlund, A., Yang, Y., Hall, A. P., Guo, L., Lux, R., He, X., … Mclean, J. S. (2013). An in vitro biofilm model system maintaining a highly reproducible species and metabolic diversity approaching that of the human oral microbiome. Microbiome, 1, 25.
Edlund, A., Yang, Y., Yooseph, S., Hall, A. P., Nguyen, D. D., Dorrestein, P. C., … Mclean, J. S. (2015). Meta-omics uncover temporal regulation of pathways across oral microbiome genera during in vitro sugar metabolism. The ISME Journal, 9, 2605–2619.
Escapa, I. F., Chen, T., Huang, Y., Gajare, P., Dewhirst, F. E., & Lemon, K. P. (2018). New insights into human nostril microbiome from the expanded Human Oral Microbiome Database (eHOMD): A resource for the microbiome of the human aerodigestive tract. mSystems, 3, e00187.
Espinoza, J. L., Harkins, D. M., Torralba, M., Gomez, A., Highlander, S. K., Jones, M. B., … Dupont, C. L. (2018). Supragingival plaque microbiome ecology and functional potential in the context of health and disease. MBio, 9, e01631.
Figueira, J., Jonsson, P., Nordin Adolfsson, A., Adolfsson, R., Nyberg, L., & Ohman, A. (2016). NMR analysis of the human saliva metabolome distinguishes dementia patients from matched controls. Molecular BioSystems, 12, 2562–2571.
Finegold, S. M. (1993). A century of anaerobes: A look backward and a call to arms. Clinical Infectious Diseases, 16(Suppl 4), S453–S457.
Flemer, B., Warren, R. D., Barrett, M. P., Cisek, K., Das, A., Jeffery, I. B., … O’toole, P. W. (2018). The oral microbiota in colorectal cancer is distinctive and predictive. Gut, 67, 1454–1463.
Flynn, K. J., Baxter, N. T., & Schloss, P. D. (2016). Metabolic and community synergy of oral bacteria in colorectal cancer. mSphere, 1, e00102.
Ghannoum, M. A., Jurevic, R. J., Mukherjee, P. K., Cui, F., Sikaroodi, M., Naqvi, A., & Gillevet, P. M. (2010). Characterization of the oral fungal microbiome (mycobiome) in healthy individuals. PLoS Pathogens, 6, e1000713.
Gomez, A., Espinoza, J. L., Harkins, D. M., Leong, P., Saffery, R., Bockmann, M., … Nelson, K. E. (2017). Host genetic control of the oral microbiome in health and disease. Cell Host and Microbe, 22(269–278), e3.
Gupta, V. K., Paul, S., & Dutta, C. (2017). Geography, ethnicity or subsistence-specific variations in human microbiome composition and diversity. Frontiers in Microbiology, 8, 1162.
Hansen, T. H., Kern, T., Bak, E. G., Kashani, A., Allin, K. H., Nielsen, T., … Pedersen, O. (2018). Impact of a vegan diet on the human salivary microbiota. Scientific Reports, 8, 5847.
Holgerson, P. L., Vestman, N. R., Claesson, R., Ohman, C., Domellof, M., Tanner, A. C., … Johansson, I. (2013). Oral microbial profile discriminates breast-fed from formula-fed infants. Journal of Pediatric Gastroenterology and Nutrition, 56, 127–136.
Hope, C. K., & Wilson, M. (2006). Biofilm structure and cell vitality in a laboratory model of subgingival plaque. Journal of Microbiological Methods, 66, 390–398.
Human Microbiome Project Consortium. (2012). Structure, function and diversity of the healthy human microbiome. Nature, 486, 207–214.
International Metagenomics and Microbiome Standards. (2019). Accessed January 2019, from https://microbialstandards.org/
Ishikawa, S., Sugimoto, M., Kitabatake, K., Sugano, A., Nakamura, M., Kaneko, M., … Iino, M. (2016). Identification of salivary metabolomic biomarkers for oral cancer screening. Scientific Reports, 6, 31520.
Kilian, M., Chapple, I. L., Hannig, M., Marsh, P. D., Meuric, V., Pedersen, A. M., … Zaura, E. (2016). The oral microbiome – An update for oral healthcare professionals. British Dental Journal, 221, 657–666.
Knight, R., Vrbanac, A., Taylor, B. C., Aksenov, A., Callewaert, C., Debelius, J., … Dorrestein, P. C. (2018). Best practices for analysing microbiomes. Nature Reviews. Microbiology, 16, 410–422.
Kolenbrander, P. E. (2011). Multispecies communities: Interspecies interactions influence growth on saliva as sole nutritional source. International Journal of Oral Science, 3, 49–54.
Koren, O., Spor, A., Felin, J., Fak, F., Stombaugh, J., Tremaroli, V., … Backhed, F. (2011). Human oral, gut, and plaque microbiota in patients with atherosclerosis. Proceedings of the National Academy of Sciences of the United States of America, 108(Suppl 1), 4592–4598.
Lazarevic, V., Gaia, N., Girard, M., Francois, P., & Schrenzel, J. (2013). Comparison of DNA extraction methods in analysis of salivary bacterial communities. PLoS One, 8, e67699.
Lazarevic, V., Whiteson, K., Francois, P., & Schrenzel, J. (2011). The salivary microbiome assessed by a high-throughput and culture-independent approach. Journal of Integrated Omics, 1, 28–35.
Lazarevic, V., Whiteson, K., Hernandez, D., Francois, P., & Schrenzel, J. (2010). Study of inter- and intra-individual variations in the salivary microbiota. BMC Genomics, 11, 523.
Leishman, S. J., Do, H. L., & Ford, P. J. (2010). Cardiovascular disease and the role of oral bacteria. Journal of Oral Microbiology, 2.
Lepp, P. W., Brinig, M. M., Ouverney, C. C., Palm, K., Armitage, G. C., & Relman, D. A. (2004). Methanogenic archaea and human periodontal disease. Proceedings of the National Academy of Sciences of the United States of America, 101, 6176–6181.
Lim, Y., Totsika, M., Morrison, M., & Punyadeera, C. (2017). The saliva microbiome profiles are minimally affected by collection method or DNA extraction protocols. Scientific Reports, 7, 8523.
Ly, M., Jones, M. B., Abeles, S. R., Santiago-Rodriguez, T. M., Gao, J., Chan, I. C., … Pride, D. T. (2016). Transmission of viruses via our microbiomes. Microbiome, 4, 64.
Mark Welch, J. L., Rossetti, B. J., Rieken, C. W., Dewhirst, F. E., & Borisy, G. G. (2016). Biogeography of a human oral microbiome at the micron scale. Proceedings of the National Academy of Sciences of the United States of America, 113, E791–E800.
Mason, M. R., Nagaraja, H. N., Camerlengo, T., Joshi, V., & Kumar, P. S. (2013). Deep sequencing identifies ethnicity-specific bacterial signatures in the oral microbiome. PLoS One, 8, e77287.
Mclean, J. S., Fansler, S. J., Majors, P. D., Mcateer, K., Allen, L. Z., Shirtliff, M. E., … Shi, W. (2012). Identifying low pH active and lactate-utilizing taxa within oral microbiome communities from healthy children using stable isotope probing techniques. PLoS One, 7, e32219.
Muir, P., Li, S., Lou, S., Wang, D., Spakowicz, D. J., Salichos, L., … Gerstein, M. (2016). The real cost of sequencing: Scaling computation to keep pace with data generation. Genome Biology, 17, 53.
Mukherjee, C., Beall, C. J., Griffen, A. L., & Leys, E. J. (2018). High-resolution ISR amplicon sequencing reveals personalized oral microbiome. Microbiome, 6, 153.
National Human Genome Research Institute. (2016). The cost of sequencing a human genome. Accessed January 2019, from https://www.genome.gov/27565109/the-cost-of-sequencing-a-human-genome/
O’toole, G. A., & Kolter, R. (1998). Initiation of biofilm formation in Pseudomonas fluorescens WCS365 proceeds via multiple, convergent signalling pathways: A genetic analysis. Molecular Microbiology, 28, 449–461.
Peters, B. A., Wu, J., Hayes, R. B., & Ahn, J. (2017). The oral fungal mycobiome: Characteristics and relation to periodontitis in a pilot study. BMC Microbiology, 17, 157.
Proctor, D. M., Fukuyama, J. A., Loomer, P. M., Armitage, G. C., Lee, S. A., Davis, N. M., … Relman, D. A. (2018). A spatial gradient of bacterial diversity in the human oral cavity shaped by salivary flow. Nature Communications, 9, 681.
Proctor, D. M., & Relman, D. A. (2017). The landscape ecology and microbiota of the human nose, mouth, and Throat. Cell Host Microbe, 21, 421–432.
Puertas, A., Magan-Fernandez, A., Blanc, V., Revelles, L., O’valle, F., Pozo, E., … Mesa, F. (2018). Association of periodontitis with preterm birth and low birth weight: A comprehensive review. The Journal of Maternal-Fetal & Neonatal Medicine, 31, 597–602.
Rasiah, I. A., Wong, L., Anderson, S. A., & Sissons, C. H. (2005). Variation in bacterial DGGE patterns from human saliva: Over time, between individuals and in corresponding dental plaque microcosms. Archives of Oral Biology, 50, 779–787.
Reyes, A., Semenkovich, N. P., whiteson, K., Rohwer, F., & Gordon, J. I. (2012). Going viral: Next-generation sequencing applied to phage populations in the human gut. Nature Reviews. Microbiology, 10, 607–617.
Samuelson, D. R., Burnham, E. L., Maffei, V. J., Vandivier, R. W., Blanchard, E. E., Shellito, J. E., … Welsh, D. A. (2018). The respiratory tract microbial biogeography in alcohol use disorder. American Journal of Physiology. Lung Cellular and Molecular Physiology, 314, L107–L117.
Shaw, L., Ribeiro, A. L. R., Levine, A. P., Pontikos, N., Balloux, F., Segal, A. W., … Smith, A. M. (2017). The human salivary microbiome is shaped by shared environment rather than genetics: Evidence from a large family of closely related individuals. MBio, 8, e01237.
Sibley, C. D., Grinwis, M. E., Field, T. R., Eshaghurshan, C. S., Faria, M. M., Dowd, S. E., … Surette, M. G. (2011). Culture enriched molecular profiling of the cystic fibrosis airway microbiome. PLoS One, 6, e22702.
Sonderholm, M., Koren, K., Wangpraseurt, D., Jensen, P. O., Kolpen, M., Kragh, K. N., … Kuhl, M. (2018). Tools for studying growth patterns and chemical dynamics of aggregated Pseudomonas aeruginosa exposed to different electron acceptors in an alginate bead model. NPJ Biofilms Microbiomes, 4, 3.
Song, S. J., Lauber, C., Costello, E. K., Lozupone, C. A., Humphrey, G., Berg-Lyons, D., … Knight, R. (2013). Cohabiting family members share microbiota with one another and with their dogs. eLife, 2, e00458.
Stahringer, S. S., Clemente, J. C., Corley, R. P., Hewitt, J., Knights, D., Walters, W. A., … KRAUTER, K. S. (2012). Nurture trumps nature in a longitudinal survey of salivary bacterial communities in twins from early adolescence to early adulthood. Genome Research, 22, 2146–2152.
Takeshita, T., Kageyama, S., Furuta, M., Tsuboi, H., Takeuchi, K., Shibata, Y., … Yamashita, Y. (2016). Bacterial diversity in saliva and oral health-related conditions: The Hisayama study. Scientific Reports, 6, 22164.
Thevaranjan, N., Puchta, A., Schulz, C., Naidoo, A., Szamosi, J. C., Verschoor, C. P., … Bowdish, D. M. E. (2018). Age-associated microbial dysbiosis promotes intestinal permeability, systemic inflammation, and macrophage dysfunction. Cell Host Microbe, 23, 570.
Vestman, N. R., timby, N., Holgerson, P. L., Kressirer, C. A., Claesson, R., Domellof, M., … Johansson, I. (2013). Characterization and in vitro properties of oral lactobacilli in breastfed infants. BMC Microbiology, 13, 193.
Wandro, S., Carmody, L., Gallagher, T., Lipuma, J. J., & Whiteson, K. (2017). Making it last: Storage time and temperature have differential impacts on metabolite profiles of airway samples from cystic fibrosis patients. mSystems, 2, e00100.
Wetterstrand, K. A. (2019) Data from the NHGRI Genome Sequencing Program (GSP). Accessed January 2019, from www.genome.gov/sequencingcostsdata .
Xian, P., Xuedong, Z., Xin, X., Yuqing, L., Yan, L., Jiyao, L., … Ga, L. (2018). The Oral Microbiome Bank of China. International Journal of Oral Science, 10, 16.
Yamasaki, K., Kawanami, T., Yatera, K., Fukuda, K., Noguchi, S., Nagata, S., … Mukae, H. (2013). Significance of anaerobes and oral bacteria in community-acquired pneumonia. PLoS One, 8, e63103.
Zaura, E., Brandt, B. W., Teixeira DE Mattos, M. J., Buijs, M. J., Caspers, M. P., Rashid, M. U., … Crielaard, W. (2015). Same exposure but two radically different responses to antibiotics: Resilience of the salivary microbiome versus long-term microbial shifts in feces. MBio, 6, e01693–e01615.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Maughan, H., Whiteson, K. (2020). Saliva as a Window into the Human Oral Microbiome and Metabolome. In: Granger, D., Taylor, M. (eds) Salivary Bioscience. Springer, Cham. https://doi.org/10.1007/978-3-030-35784-9_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-35784-9_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-35783-2
Online ISBN: 978-3-030-35784-9
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)