
Abstract
The postoperative care unit at the Hospital for Special Surgery plays an important part in the overall perioperative care of the orthopedic patient. In order to optimize patient outcomes, the postoperative care of orthopedic patients should focus on observation of organ function, monitoring of the resolution of anesthesia, resuscitation of blood loss and its consequences, and adequate pain management. In order to assure best possible outcomes, physicians caring for orthopedic patients need to be familiar with common perioperative complications in order to address them expediently. The model of postoperative care at the Hospital for Special Surgery, which allows for the adjustment of recovery room resources to care for problems encountered at various stages of the hospitalization, has proven efficient and successful. In this chapter we describe and discuss the various functions of the postoperative care unit and how we address the challenges encountered.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Postanesthesia care unit
- Challenges
- Functions
- Organ function
- Pain management
- Resuscitation of blood loss
- Monitoring
- Resolution of anesthesia
-
To provide an overview of the goals of postoperative care and discuss commonly encountered challenges in the care of postoperative orthopedic patients
-
To discuss common perioperative complications and the care of specific patient populations as approached at the Hospital for Special Surgery
-
To introduce the concept of the model of postoperative care unique to the Hospital for Special Surgery
-
The traditional role of the postanesthesia care unit (PACU) is to provide a safe transition from the highly monitored operating environment to the routine management on the patient ward.
-
The goals of such transition include observation and monitoring of the resolution of anesthesia, resuscitation of blood loss and its consequences, and adequate pain management.
-
Common complications after orthopedic surgery affect the cardiopulmonary and other organ systems, requiring that perioperative physicians are familiar with diagnosis and treatment of these entities.
-
At the Hospital for Special Surgery, the PACU also functions as an extended monitored care facility, providing care and observation for specific surgical patient populations such as extensive spinal procedures and bilateral knee arthroplasties and patients with increased postoperative medical risks such as ischemic heart disease and pulmonary.
-
In the role as an intensive care unit, the recovery room at the Hospital for Special Surgery may also care for unstable patients, including those with respiratory failure.
Introduction
The orthopedic patient can be particularly challenging with regard to postoperative care. This patient group is diverse and may present with a variety of challenges. The spectrum includes the geriatric patient with multiple comorbidities scheduled for total joint replacement to the young deceptively healthy trauma patients who may have multiple associated injuries. Thus, it becomes clear that a host of different factors may significantly impact on an individual’s postoperative course.
Despite general concerns associated with any postoperative patient, the perioperative clinician’s greatest challenges continue to be related to the care of the elderly with significant medical problems who seek surgical resolution for their chronic musculoskeletal problems, most commonly osteoarthritis. As of 2016, 15.2% of the US population are over 65 years old, and 49% of these individuals have “physician” diagnosed arthritis. According to the Department of Health and Human Services, the number of US citizens over 65 years of age is expected to increase to 71.5 million by the year 2030. Hence, it is virtually certain that an increasing number of elderly patients with multiple comorbidities will seek orthopedic surgeries.
Traditionally, the role of the postanesthesia care unit (PACU) is to provide monitored care for the patient recovering from an anesthetic after surgery. It further represents the bridge between single practitioner monitoring in the operative theater environment and periodic observational monitoring in a hospital room.
The PACU at the Hospital for Special Surgery, however, serves multiple purposes with an expanded scope compared to more traditional recovery rooms. Although its primary functions focus on the recovery of patients after surgery and anesthesia, patients are admitted postoperatively for overnight observation for potential surgical or comorbidity-related complications. Further functions include those traditionally provided by a step-down unit (SDU) for patients who require additional physiological monitoring. Further it is used as an overflow unit for high-acuity and unstable patients with complications when the intensive care unit (ICU) is at capacity. The latter functions apply to complicated patients both directly admitted from the operating room and those transferred from patient wards within the hospital. During a 1-year period, approximately 2% of the patients discharged from the PACU after nonambulatory orthopedic surgery required readmission to a higher level of care, which includes ICU, SDU, and PACU [1]. Cardiac complications were the most common reason for transfer, followed by pulmonary and neurological adverse events.
The goal of this chapter is not to provide an in-depth discussion of components of routine postoperative care, such as monitoring the recovery from anesthesia, maintaining cardiopulmonary and hemodynamic stability, and controlling pain, but instead to entertain a brief overview of the most common problems and complications encountered in the care of specific orthopedic patient populations. Further, a specific objective of this chapter is to discuss the above points in the context of current practice at the Hospital for Special Surgery (HSS).
Recovery from Anesthesia and Fluid/Blood Management
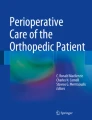
The role of the PACU is to provide patients with a safe transition of care from the operating room to the patient ward. During this transition, many acute effects of surgery and anesthesia, including traumatic and drug-related factors affecting patient physiology, need to be addressed. Since many PACUs care for patients after a variety of surgical procedures which often require general anesthesia, airway problems constitute a large number of complications, and hence respiratory management is often the focus of attention. In an Australian database of 419 recovery room incidents, 43% were related to airway and respiratory complications [2]. At this orthopedic institution, where the majority of the patients receive a regional anesthetic, although oxygenation and ventilation remain the most important concerns of the PACU staff, the incidence of PACU incidents related to the airway is much lower. Of the nonambulatory surgical procedures performed at HSS in 2010, the majority were performed under regional anesthesia (Fig. 9.1).

Distribution of types of anesthetics performed at the Hospital for Special Surgery
Since patients undergoing lower extremity surgery will usually have been anesthetized with neuraxial anesthesia, these individuals require PACU observation until both the hemodynamic and neural blockade effects of the local anesthetic have resolved. For patients undergoing a posterior approach total hip arthroplasty, the anesthetic often includes controlled hypotensive anesthesia via a neuraxial block which is dosed through the epidural catheter with the goal to achieve sympathectomy. In this particular patient population, the mean arterial blood pressure may decrease 25% with either no change or a slight decrease in heart rate [3]. With this technique, blood pressure and heart rate are controlled and stabilized using epinephrine infusions in the operating room, while in the PACU these patients are at risk for continued episodes of hypotension until the neuraxial block resolves. In the PACU, blood pressure is supported with ephedrine, intravenous fluids, and when applicable blood transfusions, respectively. Crystalloid infusions are limited because of the notion that once systemic vascular resistance is normalized and volume returns to the central circulation, elderly patients, especially those with preexisting cardiac dysfunction, may be at risk for postoperative congestive heart failure.
In the past, the majority of arthroplasty patients pre-donated autologous blood, and this blood was transfused in the PACU. However, an autologous blood donation system is expensive, and if the surgery is rescheduled, the donated blood is wasted. Further, there remains the risk of clerical transfusion errors and contamination of the blood units. Finally, preoperative anemia is a consequence of pre-donation and is associated with increased morbidity and mortality after orthopedic surgery [4]. Nevertheless, blood loss has been reduced through the combination of regional anesthesia with controlled hypotensive anesthesia and the perioperative administration of tranexamic acid [5]. Since the majority of the blood transfusions still take place in the PACU, our customary practice is to withhold homologous blood transfusion in asymptomatic adult patients with hemoglobin levels above 8gm/dl as per the results of the TRICC and FOCUS trials [6, 7]. A recent review supports a restrictive approach to blood transfusions after major orthopedic surgery [8]. The same conservative approach is applied to postoperative fluid management in the PACU, where the goal is to provide goal-directed therapy resulting in adequate tissue perfusion without inducing the complications of fluid overload, including pulmonary congestion, CHF, bowel edema and ileus, hyponatremia, and tissue edema [9]. In addition to the traditional methods of assessing intravascular volume status (physical examination, urine output, acid-base status), point-of-care, bedside transthoracic echocardiography (TTE) is frequently utilized [10]. Although the colloid-crystalloid debate continues, albumin is often considered as a resuscitation fluid to provide acute volume expansion with reduced interstitial edema.
Pain Management
Pain management should be addressed and planned in the operating room, but the PACU is where most of that plan is implemented. The goal is to establish an analgesic plan which will treat pain effectively, ameliorate the postoperative stress response, facilitate postoperative rehabilitation, minimize the side effects, improve outcome, and decrease hospital stay. This includes a multimodal approach, which will vary depending on the surgical procedure, but often includes acetaminophen, a NSAID, a gabapentinoid, and an opioid [11]. The initial dose of acetaminophen is frequently administered intravenously in the OR or PACU. At the Hospital for Special Surgery, many of the patients are followed by the Anesthesia Department managed with acute pain service, and the pain after lower extremity surgery may be managed with patient-controlled epidural analgesia (PCEA). An important element of this postoperative pain protocol is the institution of PCEA before the level of pain experienced by the patient becomes difficult to control and is usually initiated before complete resolution of the operative neuraxial blockade. Attention is paid, however, to frequent evaluation of the resolution of the motor blockade in order to detect rare neuraxial complications. Recently, a trend towards application of periarticular local anesthetic injections and/or more extensive combinations of peripheral nerve blocks has led to a decrease in the need for PCEA [12], which has also reduced the number of bladder catheters placed in the perioperative period.
Postoperative pain management is challenging in patients with preoperative narcotic dependency after spinal fusion surgery. The persistent nociceptive and neuropathic pain which these patients experience as well as perioperative opioid-induced hyperalgesia may in part be mediated through N-methyl-D-aspartate (NMDA) receptors. Ketamine is a noncompetitive NMDA receptor antagonist, which has been used in the treatment of chronic pain syndromes and at subanesthetic doses in the management of acute pain [13, 14]. At the Hospital for Special Surgery, we have shown that a perioperative infusion of subanesthetic ketamine is effective at reducing pain in narcotic-tolerant patients after posterior spinal fusions. It aids in counteracting unacceptable levels of pain in patients resistant to conventional narcotic treatment. These patients typically spend the night following surgery in the PACU on a ketamine infusion with concomitant use of a PCA with intravenous hydromorphone. On the first postoperative day, the chronic pain patients who were treated with ketamine continue to have improved analgesia during physical therapy compared to the non-ketamine-treated patients [15].
Common Complications
Cardiac Complications
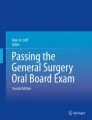
As previously discussed, our PACU serves not only as a recovery room but also as the location of care when SDU and ICU are at capacity. Analyzing institutional data, monitoring for cardiac complications – including myocardial ischemia – was the major reason patients remained in the PACU after having recovered from anesthesia. During a 1-year period, 7.6% of the patients undergoing major nonambulatory orthopedic procedures were entered into a rule-out myocardial infarction (ROMI) protocol [16]. Of these patients, 20% had elevated serum troponin levels and about one third had postoperative cardiac complications, the majority of which were arrhythmias. However, the incidence of a myocardial infarction was low (1.2%). Although speculative, it is feasible that aggressive postoperative management of these patients in the PACU (β-blockade; ASA, statin, treatment of anemia, and hemodynamic instability) assisted in achieving these results. The diagnosis of a postoperative myocardial ischemia is important in the orthopedic population since these events are often associated with further cardiac morbidity if not treated appropriately (Fig. 9.2). Two prospective studies of patients undergoing noncardiac surgery reported that postoperative cardiac troponin elevations were strongly associated with mortality within 30 days and 12 months after surgery [17, 18]. Furthermore, the decision to initiate postoperative physical therapy which is important for a favorable outcome in orthopedic patients may depend on the correct diagnosis of postoperative myocardial ischemia (PMI).

Troponin (cTnI) levels in postoperative patients with (yes) and without (no) cardiac complications
Arrhythmias, specifically atrial fibrillation (A-fib), is a common postoperative cardiac complication in the PACU. These patients are initially treated with either metoprolol or diltiazem to slow the ventricular response. A treatable etiology is then sought, including electrolyte abnormalities, anemia, hypovolemia, and myocardial ischemia. A pulmonary embolism is considered in those who present after the first postoperative day and have associated pulmonary signs and symptoms suggestive of a thrombotic event. Patients not converting to sinus rhythm are considered for amiodarone infusion. Since postoperative new-onset A-fib can be indicative of subclinical paroxysmal A-fib and an increased risk of an ischemic stroke within 1 year of surgery [19, 20], a cardiologist is consulted who can discuss the risks and benefits of long-term anti-coagulation.
Respiratory Complications
As most patients in a PACU will have received a variety of intraoperative medications and interventions which potentially compromise the respiratory system, related problems constitute some of the most commonly encountered postoperative complications. At an orthopedic institution where the majority of the patients receive a regional anesthetic with minimal to moderate sedation, the incidence of PACU complications related to the airway and respiratory system is relatively low. However, given the high prevalence of obesity and obstructive sleep apnea among patients undergoing arthroplasty and spine surgery, respiratory concerns and complications remain a primary concern. Furthermore, in patients with rheumatological diseases (i.e., rheumatoid arthritis, ankylosing spondylitis), both airway management and issues regarding oxygenation and ventilation secondary to restrictive lung disease can be particularly challenging. Elderly patients undergoing hip procedures are affected more commonly by hypoxic events compared to patients undergoing non-orthopedic procedures [21]. This hypoxia may reflect embolization of bone marrow debris into the pulmonary system. In some of these patients, preexisting pulmonary arterial hypertension will be exacerbated by the embolization of cement and bone marrow particles during hip and knee arthroplasty. Thus, our practice dictates that this patient population requires at least 12–24 hours of monitoring in the PACU.
Fat embolization is a well-known complication of skeletal trauma and surgery involving instrumentation of the femoral canal [22]. Patients undergoing bilateral hip and knee arthroplasty, revision hip arthroplasty, and pelvic reconstructions are at increased risk for fat (bone marrow) embolism syndrome [23]. The clinical manifestations of FES include respiratory symptoms, ranging from mild hypoxemia to adult respiratory distress syndrome; cardiac derangements, including tachycardia, arrhythmias to heart failure; neurologic abnormalities, ranging from somnolence and confusion to obtundation and coma; and hematologic symptoms, including thrombocytopenia and disseminated intravascular coagulation [24]. The signs and symptoms of FES in relation to the incidence of presentation are described in the Schonfeld Index [25] (Table 9.1). Since the management of the FES is supportive with early intervention resuscitation and stabilization to minimize the deleterious effects of the systemic inflammatory response to the initial insult, patients at increased risk are monitored in the PACU for 24 hours.
Renal Complications
In an analysis of 1636 patients undergoing lower extremity joint arthroplasty, acute renal failure (ARF) constituted one of the major postoperative life-threatening complications [26]. Using the RIFLE criteria to classify patients into ARF severity categories, many orthopedic patients fall into the group at risk for ARF [27]. Risk factors include advanced age, elevated body mass index, preoperatively elevated creatinine, and significant perioperative blood loss. The operative procedures which are most likely to result in ARF include bilateral knee arthroplasty, revision knee and hip arthroplasty, and posterior spine fusions. These procedures not only involve significant blood loss but may also induce FES and/or an inflammatory response which produces capillary leakage and decreased intravascular circulating volume. Hence, in the majority of cases, oliguria and anuria are the result of hypoperfusion of the kidney secondary to relative hypovolemia. Perioperatively, it is important to restore appropriate intravascular volume through the infusion of crystalloid, colloid, and when required blood products to prevent the development of acute renal dysfunction. Bedside TTE and laboratory tests are often utilized to assess intravascular volume status and determine subsequent care and interventions.
Obstructive Sleep Apnea
After the patient group with cardiac disease, the next largest category of patients who are monitored in the PACU for an extended period at the Hospital for Special Surgery are those with obstructive sleep apnea (OSA). OSA is a chronic condition resulting in partial or complete obstruction of the airway during sleep with potential adverse cardiovascular complications. The prevalence of OSA in our population may approach 10%. These patients may be at risk for adverse postoperative cardiorespiratory complications, including death. However, there are insufficient evidence-based data in the literature to provide guidelines with regard to the postoperative management of patients with diagnosed OSA. In a retrospective analysis of patients undergoing total hip or total knee arthroplasties, OSA was associated with increased incidence of postoperative transfer to an ICU [28]. The accepted diagnosis of OSA requires an overnight polysomnography analysis which generates an Apnea-Hypopnea Index, AHI, the number of pharyngeal collapses lasting more than 10 seconds per hour during sleep. However, the STOP-BANG questionnaire for OSA has been advocated by some as a simple bedside means of identifying those patients at risk for having OSA [29]. All patients for nonambulatory surgery at the Hospital for Special Surgery have a STOP-BANG score in their medical record; a score of ≥5 places a patient at high risk for OSA. Most clinicians agree that patients with severe OSA, AHI >30, or obesity hypoventilation syndrome (OHS) should be monitored with oximetry and adequate respirations for at least the night after surgery [30]. The postoperative management of those with mild-to-moderate OSA remains controversial; however, a conservative approach suggests a monitoring period of one sleep cycle. At the Hospital for Special Surgery, we have established an OSA unit which provides continuous pulse oximetry and respiratory rate monitoring with nurse-activated alarms. Patients who have known or suspected mild-to-moderate OSA, ASA 2, or BMI ≤45 and do otherwise not require SDU or ICU monitoring for additional diagnosis (ROMI, large EBL) are monitored in this unit (Box 9.1). Patients who use continuous positive airway pressure at home are asked to bring their masks to the hospital, thus facilitating continuation of care during their stay.
Box 9.1 Criteria for Admission to the OSA Unit
-
1.
Diagnosed OSA with stable, chronic use of CPAP at home
-
2.
Diagnosed OSA but noncompliant with CPAP
-
3.
Suspected OSA (STOP-BANG ≥5; clinician decision)
-
4.
BMI ≤45
-
5.
ASA ≤2 (unless ASA of 3 based on BMI only)
-
6.
Exclusion:
-
(a)
Requiring SDU monitoring other medical reasons
-
(b)
EBL >20%
-
(c)
Chronic pain patient
-
(a)
Patients After Bilateral Joint Arthroplasty and Revision Arthroplasty
Patients undergoing bilateral lower extremity or revision arthroplasty are observed overnight in our PACU, based on the fact that these operations are associated with increased blood loss, longer surgical duration, and an increase in the perioperative inflammatory response. Single-stage bilateral lower extremity arthroplasty, particularly that involving the knee joints (SBTKA), has been reported to be associated with increased morbidity and mortality [31]. The major postoperative complications after SBTKA include myocardial infarction, fat embolization, respiratory insufficiency, and thromboembolic events. As these complications may be the result of multiple comorbidities, increased blood loss and fluid shifts, pain, and cardiopulmonary stress compared to unilateral joint arthroplasty, careful patient selection and increased postoperative vigilance seem prudent in an attempt to improve outcomes. At our institution all SBTKA recipients are screened by an anesthesiologist preoperatively with the goal to restrict these higher-risk procedures to patients without significant comorbidities [32] (Box 9.2). Although younger patients are being selected for SBTKA, some of the complications are still increasing. The increased complication rate may be the result of the rising levels of obesity and associated, often undiagnosed, conditions like pulmonary hypertension [33].
Box 9.2 Exclusion Criteria for SBTKR
-
1.
Patients ≥80 y.o.
-
2.
ASA 3
-
3.
Active ischemic heart disease (h/o angina or positive stress test)
-
4.
Reduced LV function (LVEF<45%; DOE; h/o CHF)
-
5.
Poor functional capacity
-
6.
Pulmonary disease
-
(a)
Moderate to severe pulmonary hypertension
-
(b)
O2 dependent
-
(c)
Steroid-dependent asthma
-
(d)
Exercise-limiting COPD
-
(a)
-
7.
Morbid obesity
-
8.
Renal insufficiency: Cr >1.8
-
9.
Liver disease: child’s class B or greater
-
10.
Poorly-controlled DM; HbA1c >7%
-
11.
Cerebral vascular disease (h/o stroke)
-
12.
Major peripheral vascular disease
Data from Ref. [32]
Postoperative Delirium
Another significant patient population requiring extended postoperative monitoring and interventions is the population suffering from postoperative delirium. Delirium is a common complication in the geriatric population following orthopedic surgery, with a reported incidence of up to 50% particularly after the repair of femoral neck fractures [34]. Postoperative delirium usually presents after 24 hours post surgery and resolves within 48 hours. However, in some of the patients, evidence of confusion and cognitive dysfunction may persist for up to 6 months. Postoperative delirium is associated with longer hospital stay, increased risk for complications, poor recovery, increased mortality, and increased healthcare costs [35, 36]. The diagnosis can be challenging as postoperative delirium can present in various forms. A fluctuating hyperactive state is often associated with agitation, sweating, and tachycardia, but a hypoactive type may present with passive confusion and is often overlooked. Since in most cases patients present with a change in mental status without a clear etiology, they are often subjected to an extensive neurological evaluation including brain imaging. At the Hospital for Special Surgery, patients with delirium are identified by nurses using the CAM algorithm [37]. Next a neurological examination is conducted by a physician to rule out focal deficits. Further, blood laboratory analysis may be performed to exclude electrolyte abnormalities, hypercarbia, and hypoxemia. A review of all medications to eliminate unnecessary centrally acting medications is mandatory. And finally, care should be taken to assure adequate pain management [38].
At our institution over a 6-year period in a cohort of 78,492 adult patients undergoing nonambulatory orthopedic surgery, the incidence of POD was 1.2%. Many of the risk factors identified have been cited in previous reports and are not amendable to modification. They include advanced age, medical comorbidities, and a history of preexisting psychiatric disease. However, some risk factors such as preexisting narcotic dependence, alcoholism, and hyponatremia are potentially modifiable. In addition, the surgical procedure, type of anesthesia, and type of postoperative analgesia may affect the incidence of delirium, and as such these factors can be targeted in an attempt to reduce its incidence [39].
Once the diagnosis of postoperative delirium has been established, the managing physician is faced with the problem of treatment options. If removal of the delirium-inciting agents (i.e., narcotics, benzodiazepines) does not improve the confusion and/or the patient’s hyperactive state, pharmacological treatment has traditionally constituted in the use of neuroleptic medications such as haloperidol. At our institution, however, we have had significant success with low-dose (<0.5 μg/kg/h) infusions of dexmedetomidine for 6–8 hours. This approach is used primarily in hyperactive patients and produces mild-to-moderate sedation, control of agitation, and associated hypertension and tachycardia while allowing the patient to rest without significant depression of the respiratory system.
Readmission to the PACU
As mentioned previously, the PACU functions as the place for monitoring and treatment when the ICU and SDU are at capacity. As such its staff provides care for patients whose medical condition deteriorates during the remainder of their hospitalization. When studying all patients undergoing major orthopedic surgery over a 1-year period (n = 12,229) at our institution, 1.7% (n = 206) were readmitted to the PACU within 6 days of discharge. This represented 1.6% of all total hip arthroplasties, 1.8% of all total knee arthroplasties, and 3.4% of all spinal fusion surgeries (3.4%) [40]. Patients readmitted to the PACU after surgery had multiple comorbidities, including cardiac disease (40.3%), diabetes mellitus (18.4%), chronic renal insufficiency (14.1%), and pulmonary disease (12.6%) (Fig. 9.3). Approximately 9% of the returning patients had ≥3 comorbidities. Of the patients with a final diagnosis of myocardial ischemia, 80% had at least one cardiac risk factor. Patients requiring PACU readmission were also significantly older and had a longer length of hospital stay. Since there is increased pressure to reduce the length of the hospital stay after major orthopedic procedure, it is important to identify which patients are at risk for acute postoperative complications. This study represents the first step in identifying the incidence of postoperative complications after major orthopedic surgery, the patients at risk for these complications, and possible interventions which may reduce poor outcome.

Return to a monitored setting
Summary
The PACU at the Hospital for Special Surgery functions as a recovery room, SDU, and overflow ICU. Much of our emphasis is devoted to the recovery of patients from regional anesthesia and the institution of adequate postoperative analgesia. Common problems encountered in the orthopedic patient population often stem from blood loss and fluid resuscitation. Complications are infrequent but are often related to respiratory or cardiac events. In contrast to a traditional PACU, our recovery room devotes resources to the observation and management of patients after more invasive procedures, such as bilateral lower extremity arthroplasty, or patients with specific medical problems such as OSA and postoperative delirium as well as those at high risk for postoperative myocardial infarction. Our critical care is focused on complications prevalent among patients undergoing orthopedic surgery. Patients frequently found in this category are those requiring mechanical ventilation due to pulmonary insufficiency and those suffering large blood loss. Further, patient categories are those with severe complications related to fat embolism syndrome and those presenting with cardiopulmonary resuscitative emergencies. However, since many of our arthroplasty patients are geriatric, we also provide monitored care for the common medical complications associated with this age group. This careful attention to the postoperative issues of our specific patient population is paramount in attempting to reduce perioperative complications.
Summary Bullet Points
-
In order to optimize patient outcomes, the postoperative care of orthopedic patients should focus on observation of organ function, monitoring of the resolution of anesthesia, resuscitation of blood loss and its consequences, and adequate pain management.
-
Physicians caring for orthopedic patients need to be familiar with common perioperative complications in order to address them expediently.
-
The model of postoperative care at HSS which allows for the adjustment of recovery room resources to care for problems encountered at various stages of the hospitalization has proven to be efficient and successful.
Case Study
An 80-year-old female with a past medical history significant for hypertension, coronary artery disease, depression, and elevated cholesterol was scheduled for right total knee arthroplasty. The surgical course was uneventful, and the anesthesia was performed using a combined spinal epidural technique with 12 mg of bupivacaine and a femoral nerve block with 30 mL of 0.25% bupivacaine. The patient’s surgery ended at 10:30 am, and she was admitted to the PACU for an overnight stay for a rule-out myocardial infarction protocol and observation.
At 10 pm on the night of surgery, the patient was complaining of extensive pain despite an epidural infusion of 0.06% bupivacaine and 10 μg/mL of hydromorphone. The PACU team decided that the epidural was not adequately functioning, and she was switched to an intravenous patient-controlled pump containing hydromorphone.
By 1 am the PACU team was called to the patient’s bedside for assessment of aggressive and combative behavior. Her vital signs included a blood pressure of 190/100 mmHg, a heart rate 100 bpm, a temperature of 37.8 °C, and oxygen saturation of 90%. The patient complained that she was being held captive in a hotel in Chicago and demanded to have the police called so that she could be released immediately. An arterial blood gas was obtained and revealed a pH of 7.36, a CO2 of 44 mmHg, and an O2 of 66 mmHg. A chest radiograph demonstrated bilateral lower lobe atelectasis.
The differential diagnosis included pulmonary embolism, a cerebrovascular event, fat embolism syndrome, and postoperative delirium. Since the patient had been ambulatory prior to surgery and when taking the timing of events into account, a thromboembolic event was considered to be unlikely. The symptoms of hypertension and confusion could be the result of cerebrovascular occlusion and/or cerebral hemorrhage; however, the patient’s neurological exam was non-focal. In addition, the elevated blood pressure was more likely the result of her pain. With regard to infection, her chest radiograph was clear except for atelectasis, the knee incision was clean, and the wound was not hot or tense. Fat embolism syndrome was also considered, but as other signs like alveolar infiltrates on chest radiograph and hematologic signs such as thrombocytopenia were missing, this was also considered less likely.
The team decided that her primary problem was postoperative delirium, secondary the stress of surgery, inconsistent and inadequate analgesia, and sleep deprivation in the PACU. The patient was given intravenous enalapril and metoprolol for her elevated blood pressure and heart rate. An infusion of dexmedetomidine at 0.5 μg/kg/h was initiated, and once the patient was sedated, she was placed on noninvasive positive pressure ventilation. At 7 am the following morning, the infusion was stopped, and by 8 am the patient was awake, oriented, and alert. Her pain was well controlled with intravenous hydromorphone. Her vital signs had normalized and she was discharged to the ward.
References
Urban MK, Mangini-Vendal M, Lyman S, Pan TJ, Magid SK. The need for a step-up in postoperative medical care is predictable in orthopedic patients undergoing elective surgery. HSSJ. 2016;12:59–65.
Kluger MT, Bullock MF. Recovery room incidents: a review of 419 reports from the anesthetic incident monitoring study. Anaesthesia. 2002;57:1060–6.
Sharrock NE, Mineo R, Urquhart B. Hemodynamic effects and outcome analysis of hypotensive extradural anesthesia in controlled hypotensive patients undergoing total hip arthroplasty. Br J Anaesth. 1991;67:17–25.
Goodnough LT, Maniatis A, Earnshaw P, Benoni G, Beris P, Fergusson DA, et al. Detection, evaluation and management of preoperative anaemia in the elective orthopedic population: NATA guidelines. Br J Anaesth. 2011;106:13–22.
Melvin JS, Stryker LS, Sierra RJ. Tranexamic acid in hip and knee arthroplasty. JAAOS. 2015;23:732–40.
Hebert PC, Wells G, Blajchman MA, Marshall J, Martin C, Pagliarello G, et al. A multicenter randomized controlled clinical trial of transfusion requirements in critical care. N Eng J Med. 1999;340:409–17.
Carson JL, Terrin ML, Noveck H, Sanders DW, Chaitman BR, Rhoads GG, et al. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med. 2011;365:2453–62.
Mitchell MD, Betesh JS, Hume EL, Mehta S, Umshield CA. Transfusion thresholds for major orthopedic surgery: a systematic review and meta-analysis. J Arthroplast. 2017;32:3815–21.
Kayilioglu SI, Dinc T, Sozen I, Bostanoglu A, Cete M, Coskum F. Postoperative fluid management. World J Crit Care Med. 2015;4:192–201.
Adler AC, Greeley WJ, Conlin F, Feldman JM. Perioperative anesthesiology ultrasonographic analysis (PAUSE): a guided approach to perioperative bedside ultrasound. J Cardiothoracic Vasc Anesth. 2016;30:521–9.
Wick EC, Grant MC, Wu CL. Postoperative multimodal analgesic pain management with nonopioid analgesics and techniques. JAMA. 2017;152:691–7.
Gaffney CJ, Pelt CE, Gililland JM, Peters CL. Perioperative pain management in hip and knee arthroplasty. Orthop Clin N Am. 2017;48:407–19.
Hocking G, Cousins MJ. Ketamine in chronic pain management: an evidence-based review. Anesth Analg. 2003;97:1730–9.
Bell RF, Dahl JB, Moore RA, Kalso E. Peri-operative ketamine for acute post-operative pain: a quantitative and qualitative review (Cochrane review). Acta Anesthesiol Scand. 2005;49:1405–28.
Urban MK, Yadeau JT, Wukovits, Lipinitsky JY. Ketamine as an adjunct to postoperative management in opioid tolerant patients after spinal fusions: a prospective randomized trial. HSS J. 2008;4:62–8.
Urban MK, Wolfe SW, Sanghavi NM, Magid SK. The incidence of cardiac events after orthopedic surgery: a single I institutional experience of cases performed over one year. HSS J. 2017;13:248–54.
Devereaux PJ, Yang H, Yusuf S, Guyatt G, Leslie K, Villar JC, et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial. Lancet. 2008;371:1839–47.
Devereaux PJ, Chan MT, Alonso-Coello P, Walsh M, Berwanger O, Villar JC, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012;307:2295–304.
Healy JS, Stuart J, Connolly MD, Gold MR, Israel CW, Van Gelder IC, et al. Subclinical atrial fibrillation and the risk of stroke. N Engl J Med. 2012;366:120–9.
Khormaee S, Do HT, Mayr Y, Gialdini G, Lyman S, Cross MB. Risk of perioperative ischemic stroke after perioperative atrial fibrillation in total knee and hip arthroplasty patients. J Arthroplast. 2018;33:3016–9.
Sari A, Miyauchi Y, Yamashita S, Yokota K, Ogasahara H, Yonei A. The magnitude of hypoxemia in elderly patients with fractures of the femoral neck. Anesth Analg. 1986;65:892.
Gitin TA, Seidel T, Cera PJ, Glidewell OJ, Smith JL. Pulmonary microvascular fat: the significance? Crit Care Med. 1993;21:673–7.
Urban MK, Sheppard R, Gordon MA, Urquhart BL. Right ventricular function during revision total hip arthroplasty. Anesth Analg. 1996;82:1225–9.
Ereth MH, Weber JG, Abel MD, Lennon RL, Lewallen DG, Ilstrup DM, et al. Cemented versus noncemented total hip arthroplasty- embolism, hemodynamics, and intrapulmonary shunting. Mayo Clin Proc. 1992;67:1066–74.
Schonfeld SA, Ploysongsang Y, DiLisio R, Crissman JD, Miller E, Hammerschmidt DE, et al. Fat embolism prophylaxis with corticosteroids. A prospective study in high risk patients. Ann Int Med. 1983;99:438–43.
Parvizi J, Mui A, Purtill JJ, Sharkey PF, Hozack WJ, Rothman RH. Total joint arthroplasty: when do fatal or near-fatal complications occur? JBJS. 2007;89:27–32.
Bellomo R, Ronco C, Kellum JA, et al. Acute renal failure-definition, outcome measures, animal models, fluid therapy and information technology needs: the second international consensus conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:204–12.
Gupta RM, Parvizi J, Hanseen AD, Gay PC. Postoperative complications in patients with obstructive sleep apnea syndrome undergoing hip or knee replacement. A case-control study. Mayo Clin Proc. 2001;76:897–905.
Vasa TS, Doghramji K, Cavalizaai R, Grewal R, Hirani A, Leiby B, et al. Obstructive sleep apnea and postoperative complications: clinical use of the STOP-BANG questionnaire. Arch Otolaryngol Head Neck Surg. 2010;136(10):1020–4.
American Society of Anesthesiologists Task Force on Perioperative Management of patients with obstructive sleep apnea, Gross JB, Apfelbaum JL, Caplan RA, Connis RT, Coté CJ, et al. ASA practice guidelines for the perioperative management of patients with obstructive sleep apnea. Anesthesiology. 2014;120:268–86.
Memtsoudis S, Yan M, Della Valle G, Mazumdar M, Gaber-Baylis LK, MacKenzie CR, et al. Perioperative outcomes after unilateral and bilateral total knee arthroplasty. Anesthesiology. 2009;111:1206–16.
Urban MK, Chisolm M, Wukovitx B. Are postoperative complications more common with single-stage bilateral (SBTKR) than with unilateral knee arthroplasty: guidelines for patients scheduled for SBTKA. HSS J. 2006;2:78–82.
Memtsoudis SG, Mantilla CG, Parvizi J, Stundner O, Mazumdar M. Have bilateral knee arthroplasties become safer? A population based trend analysis. Clin Orthop Rel Res. 2012;471:2608–9.
Bruce AJ, Ritchie CW, Blizard R, Lai R, Raven P. The incidence of delirium associated with orthopedic surgery: a meta-analytic review. Intl Psychogeriatr. 2007;19(2):197–214.
Allen SR, Frankel HL. Postoperative complications: delirium. Surg Clin North Am. 2012;92(2):409–31.
Gleason LJ, Schmitt EM, Kosar CM, Tabloski P, Saczynski JS, Robinson T, et al. Effect of delirium and other major complications on outcomes after elective surgery in older adults. JAMA Surg. 2015;150:1134e40.
Wong CL, Holroyd-Leduc J, Simel DL, Straus SE. Does this patient have delirium; the value of bedside instruments? JAMA. 2010;304:779–86.
Vaurio LE, Sands LP, Wang Y, Mullen A, Leung JM. Postoperative delirium: the importance of pain and pain management. Anesth Analg. 2006;102:1267–73.
Winstein SM, Poulsides L, Baaklini LR, Morwald EE, Cozowicz C, Saleh JN, et al. Postoperative delirium in total knee and hip arthroplasty patients: a study of perioperative modifiable risk factors. Br J Anaesth. 2018;120:999–1008.
Urban MK, Magid S, Mangini M. One year incidence for admission to a critical care unit after major orthopedic surgery. Perioperative Medicine Summit, Miami Florida, 2011.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Urban, M.K. (2020). The Role of the Postanesthesia Care Unit in the Perioperative Care of the Orthopedic Patient. In: MacKenzie, C., Cornell, C., Memtsoudis, S. (eds) Perioperative Care of the Orthopedic Patient. Springer, Cham. https://doi.org/10.1007/978-3-030-35570-8_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-35570-8_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-35569-2
Online ISBN: 978-3-030-35570-8
eBook Packages: MedicineMedicine (R0)