
Abstract
Two decades following the cloning of the heparanase gene, the significance of this enzyme for tumor growth and metastasis cannot be ignored. Compelling pre-clinical and clinical evidence tie heparanase with all steps of tumor formation namely, initiation, growth, metastasis, and chemo resistance, thus confirming and significantly expanding earlier observations that coupled heparanase activity with the metastatic capacity of tumor cells. This collective effort has turned heparanase from an obscure enzyme to a valid target for the development of anti-cancer drugs, and led basic researchers and biotech companies to develop heparanase inhibitors as anti-cancer therapeutics, some of which are currently examined clinically. As expected, the intense research effort devoted to understanding the biology of heparanase significantly expanded the functional repertoire of this enzyme, but some principle questions are still left unanswered or are controversial. For example, many publications describe increased heparanase levels in human tumors, but the mechanism underlying heparanase induction is not sufficiently understood. Moreover, heparanase is hardly found to be increased in many studies utilizing methodologies (i.e., gene arrays) that compare tumors vs (adjacent) normal tissue. The finding that heparanase exert also enzymatic activity-independent function significantly expands the mode by which heparanase can function outside, but also inside the cell. Signaling aspects, and a role of heparanase in modulating autophagy are possibly as important as its enzymatic aspect, but these properties are not targeted by heparanase inhibitors, possibly compromising their efficacy. This Book chapter review heparanase function in oncology, suggesting a somewhat different interpretation of the results.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Activity capable of cleaving macromolecular heparin at a limited number of sites was first reported in 1975 by Ögren and Lindahl [1]. Soon thereafter, Höök et al. reported an endoglycosidase activity that degrades heparan sulfate (HS)-polymers into oligosaccharides [2]. Given the structural role of HS proteoglycans (HSPG) in the assembly of extracellular matrix (ECM) and basement membrane, it was hypothesized that HS-degrading activity would loosen the ECM, thus promoting cell dissemination. Indeed, heparanase activity was found to correlate with the metastatic potential of tumor cells [3,4,5], a correlation that still direct and guide heparanase research. Subsequent years can be divided to before and after the cloning of the heparanase gene. Until 1999, progress in the field was slow and studies were restricted to measures of heparanase activity in different normal and malignant cells and tissues under various experimental settings [6, 7]. Also, the lack of a simple assay and purified enzyme in sufficient amounts lead to conflicting reports on the biochemical properties and substrate specificity of the enzyme(s) [8]. Heparanase activity was attributed to proteins with a molecular weight ranging from 8 to 130 kDa, raising the possible existence of several HS-degrading endoglycosidic enzymes [8,9,10,11]. This confusion was solved when the cloning of a single human heparanase cDNA sequence was independently reported by several groups in 1999 [12,13,14,15]. So far, and unlike many other classes of enzymes, no other cDNA sequence encoding an active heparanase enzyme has been identified, indicating that mammalian cells express primarily one single dominant heparanase enzyme (historic perspective is presented by Vlodavsky et al., Gaskin et al., and Khanna and Parish, Chaps. 1, 3 and 7 in this volume). With the availability of appropriate tools, heparanase research entered a new era. In the last 20 years, we are experiencing a burst in heparanase research, evident by an average of 100 new citations in PubMed each year. This collective effort has turned heparanase from an obscure enzyme to a valid target for the development of anti-cancer drugs, some of which are under clinical evaluation [16,17,18,19].
In 2007, Vreys and David published a comprehensive review article entitled “Mammalian heparanase-What is the message?” [20]. A similar phrase was entitled by Rickles: “If heparanase is the answer, what is the question?” [21]. The ‘message’, or ‘answer’, over ten years later, can be summarized as a pleiotropic enzyme that plays an important role in cancer and inflammation, two major facets that are often interconnected. While the pro-tumorigenic properties of heparanase are well taken, some aspects of heparanase biology and its mode of action are still unclear. Here, we review heparanase function in oncology, suggesting a somewhat different interpretation of the results.
2 Heparanase and Cancer Progression
2.1 Heparanase Induction in Human Cancer
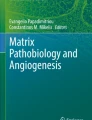
Soon after the cloning of the HPSE gene and the development of anti-heparanase antibodies and probes, many studies examined its expression in human tumors compared with adjacent normal tissue. Immunohistochemistry, in situ hybridization, RT-PCR, real time-PCR and enzymatic activity analyses revealed that heparanase is up regulated in essentially all human tumors examined. In most cases, elevated levels of heparanase were detected in about 50% of the tumor specimens, with a higher incidence in pancreatic (78%) and gastric (80%) carcinomas, and in multiple myeloma (86%) [20, 22,23,24]. Generally, the normal looking tissue adjacent to the malignant lesion expressed little or no detectable levels of heparanase, suggesting that epithelial cells do not normally express the enzyme. This is in agreement with the notion that under normal conditions heparanase expression is restricted primarily to the placenta and platelets, and to lower extent keratinocytes, lymphocytes, neutrophils, and macrophages [9, 10]. In several carcinomas, most intense heparanase staining was localized to the invasive front of the tumor [25,26,27,28], supporting a role for heparanase in cell invasion. Furthermore, patients that were diagnosed as heparanase-positive exhibited a significantly higher rate of local and distant metastasis as well as reduced postoperative survival, compared with patients that were diagnosed as heparanase-negative [25, 26, 29,30,31,32] (Fig. 9.1). These and more recent studies [33,34,35,36,37,38,39,40,41,42,43] provide strong clinical support for the pro-metastatic function of heparanase. Subsequent studies provided compelling evidence that tie heparanase levels with all steps of tumor formation including tumor initiation, angiogenesis, growth, metastasis, and chemoresistance [40, 44,45,46,47,48,49]. These and other results (i.e., the critical role of heparanase in the tumor microenvironment) [49, 50] (See also Chapter by Elkin et al., Chap. 17 in this volume) indicate that heparanase is causally involved in cancer progression and collectively provide strong clinical support for the pro-tumorigenic function of heparanase and put forward the concept that heparanase is a valid target in cancer.

Reduced overall survival curves of patients with tongue (left), head and neck (middle) and lung (right) carcinomas according to heparanase immunostaining intensity. Formalin-fixed paraffin-embedded sections of tumors and adjacent normal head and neck and lung tissues were subjected to immunostaining of heparanase, applying anti-heparanase pAb 733. Staining was graded as 0 (negative), 1 (weak) and 2 (strong). Note that adjacent normal head and neck and lung tissues are stain negative for heparanase. Shown are representative immunostaining at low (upper panels) and high (x100) magnifications (middle panels). Kaplan-Meier analysis showed poor survival of patients with strong (score 1 & 2) heparanase staining or high staining extent (i.e., percent of heparanase-positive cells), compared with patients who were diagnosed as heparanase-negative (score 0) (lower panels)
The molecular mechanism(s) underlying heparanase induction in tumor cells is not entirely clear, but evidently involves epigenetic alterations (i.e., DNA methylation), hormones, oncogenes, and post-transcriptional regulation [51]. The involvement of SNPs [52, 53] and an enhancer region that activates the promoter [54] is discussed in details by Ostrovsky et al., Chap. 8 in this volume.
2.2 Basal and Inducible Heparanase Gene Transcription
A 3.5-kb promoter region of the heparanase gene was cloned by Jiang et al. [55]. Somewhat surprisingly, sequence analysis revealed that the TATA-less, GC-rich promoter of the heparanase gene belongs to the family of housekeeping genes. This may suggest that heparanase is being expressed at low levels by all cells in order to maintain homeostasis (see below). The above-mentioned lack of heparanase detection by immunostaining of normal epithelium adjacent to the tumor lesion may thus result from low levels under the detection of anti-heparanase antibodies. Further analysis revealed three Sp1 sites and four Ets-relevant elements (ERE) within the heparanase promoter [55, 56]. SP1 is a zinc-finger transcription factor that binds GC-rich motif of many gene promoters and is abundantly expressed by all mammalian cell types. Thus, it was long thought to be a regulator of housekeeping genes. Indeed, knockout of Sp1 in mice causes embryonic lethality at an early stage of development (around day 10.5 of gestation) with a broad range of phenotypic abnormalities, suggesting a general function in many cell types [57]. Unlike SP1 and Ets, which are associated with basal heparanase transcription levels [55], Early growth response 1 (Egr1) appears to be related to inducible transcription of heparanase. Egr1 has been shown to bind the human and mouse heparanase gene promoters and to induce heparanase expression in tumor cells [58,59,60] and in primary T lymphocytes, facilitating their infiltration into the CNS to promote EAE [61]. Egr1 has been shown to bind to the promoters of a range of genes to mediate responses such as wound healing and neo-vascularization, and has been strongly associated with vascular proliferative disorders [60]. Moreover, Egr1 has been implicated in tumor angiogenesis, growth, and metastasis, closely resembling heparanase pro-tumorigenic properties. Egr1 was also noted to inhibit heparanase expression in pancreatic carcinoma cells exposed to radiation [62], suggesting that heparanase gene regulation by Egr1 is cell-type and context-dependent. The clinical significance of heparanase regulation by Egr1 emerged in the study of DNA methylation (Gaskin et al., Chap. 7 in this volume).
2.3 Gene Methylation and Egr1
In addition to multiple genetic alterations that govern cell transformation, epigenetic processes, marked by hypermethylation of the promoter region, contribute significantly to gene transcription and cancer progression, likely by down-regulation of tumor suppressor and DNA repair genes. Several studies have convincingly shown that promoter methylation status plays an important role in heparanase gene transcription. By examining a series of tumor-derived cell lines, Shteper et al. found that cells which exhibit heparanase activity also harbor at least one unmethylated allele [63]. In contrast, cell lines which exhibit no heparanase expression or activity, such as C6 rat glioma and JAR human choriocarcinoma, were found to harbor fully methylated alleles [63]. Treating these cells with demethylating agents such as 5-azacytidine restored heparanase activity accompanied by augmented metastatic capacity [63]. This augmentation was suppressed in mice treated with heparanase inhibitor [63], thus critically relating to heparanase expression and metastasis. Subsequent studies revealed a similar correlation with prostate and bladder cancer-derived cell lines, and, moreover, with prostate and bladder tissue. Hence, significantly higher promoter methylation was found in benign prostatic hyperplasia (BPH) and in normal bladder than in bladder carcinomas, inversely correlating with heparanase expression [64, 65]. Interestingly, Ogishima et al. have noted a correlation between heparanase expression by bladder and prostate carcinomas and the expression levels of Egr1, regulating heparanase expression in a stepwise manner. Hence, heparanase expression was the lowest in methylation-positive and EGR1-negative samples and the highest in methylation-negative and EGR1-positive samples [64, 65]. It should be noted, nonetheless, that while DNA methylation and Egr1 likely play an important role in regulating heparanase transcription, the magnitude of heparanase induction by these factors seems lower than the induction often observed by immunostaining. This may suggest that heparanase expression is also regulated post-transcriptionally.
2.4 ARE and Post-Transcriptional Gene Regulation
In mammalian cells, sequence elements rich in adenosine and uridine, called AU-rich elements (ARE) , were identified for their ability to target mRNAs for rapid degradation [66,67,68]. Many ARE-bearing mRNAs encode oncoproteins, cytokines, growth factors and transcription factors [66, 69]. Arvatz et al. have shown that heparanase expression is regulated at the post-transcriptional level by sequences at the 3′ untranslated region (3′UTR) of the gene [51]. Introducing the 3′UTR immediately following the heparanase cDNA reduces heparanase enzymatic activity and protein levels, resulting in decreased cellular invasion capacity. Furthermore, a 185 bp sequence was identified within the 3′UTR that mediates heparanase down-regulation, and an ARE motif has been recognized within this region. Deletion of the entire 185 bp region or the ARE motif eliminated the inhibitory effect of the 3′UTR, resulting in more stable heparanase mRNA, elevated heparanase levels and formation of larger tumor xenografts indistinguishable from those produced by heparanase over-expressing cells in terms of size, vascularization and Akt activation [51]. These results suggest that loss of the ARE is an important regulatory mechanism and driving force contributing to heparanase induction and tumor growth [51].
2.5 Heparanase Regulation by Hormones, Tumor Suppressors, Oncogenes and Micro-RNA
Systemic and local mediators are also likely to participate in heparanase gene regulation. The presence of functional estrogen response elements within the heparanase promoter suggests a systemic mechanism by which hormones control heparanase transcription [70, 71]. Indeed, administration of estrogen markedly enhanced heparanase gene transcription in breast cancer cells, which was completely abolished by estrogen receptor antagonist [72]. Furthermore, a correlation between heparanase and estrogen receptor levels was confirmed by analyzing breast carcinoma tissue array [72], signifying its clinical relevance.
Normal epithelia exhibit relatively low levels of heparanase activity, suggesting that the heparanase promoter may possibly be transcriptionally repressed. This is due, at least in part, to binding of the p53 tumor suppressor and recruitment of histone deacetylases [73]. Mutational inactivation of p53 during cancer development leads to transcriptional activation of heparanase, providing a possible molecular mechanism for the frequent increase in heparanase levels observed in the course of tumorigenesis [73]. Likewise, heparanase expression was found to be under the regulation of oncogenes. For example, overexpression of mutant BRAF (V600E) and mutant Ras (G12 V) resulted in a marked increase in heparanase expression, accompanied by reduced HS on the cell surface [74]. Similarly, knockdown of BRAF expression in a BRAF-mutated KAT-10 tumor cell line led to the suppression of heparanase gene expression, subsequently leading to increased cell surface HS levels [74]. Analyses of the heparanase promoter revealed that the Ets relevant elements are critical for BRAF-induced heparanase expression, in a manner that involves GABPβ (but not Egr1) [74].
More recent studies reported the involvement of several micro-RNAs in heparanase gene regulation. For example, miR-1258 levels inversely correlated with heparanase expression in non-small cell lung cancer and breast cancer cells [75,76,77]. Functionally, heparanase downregulation by miR-1258 resulted in reduced cell invasiveness in vitro, and brain metastasis of breast cancer cells in vivo [75,76,77], emphasizing the relevance of miRNA-dependent heparanase regulation for cancer metastasis. In contrast, Mir-558 was noted to induce heparanase expression, and knockdown of endogenous miR-558 decreased the growth, invasion, metastasis, and angiogenesis of neuroblastoma cells in vitro and in vivo [78].
Collectively, the results suggest that heparanase expression is tightly regulated [20]; its induction in tumor cells is not mediated by one common cue but rather by complexed mechanisms that can operate in concert [65] but may vary among cells, type of tumor, and patients. Somewhat surprisingly, the detailed experimental results described above are not reflected in many array-type analyses that compare gene signatures in disease states and mainly cancer. We expected that given the common induction of heparanase in human tumors and consequently its bad prognosis (Fig. 9.1), heparanase will be found among the genes increased in tumors vs. normal tissue. This is not commonly observed. The reason is unclear, but may suggest that post-transcriptional mechanisms are more dominant than anticipated, or that mechanisms that were identified in cell lines do not sufficiently mimic tumors in patients. It is also possible that the heterogeneity of human tumors and sampling of a small area of the lesion for RNA extraction does not sufficiently reflect the tumor mass. Common inclusion of heparanase in patients’ gene analyses would strengthen the significance of heparanase in cancer, and recruit more investigators to the field.
3 Heparanase Signaling-A Message from within
Heparanase up-regulation in primary human tumors correlated in some cases not only with tumor metastasis but also with tumors larger in size [26, 79,80,81,82,83]. The clinical findings have been recapitulated in many pre-clinical models in which overexpression of heparanase promotes tumor growth [20, 22,23,24, 84, 85]. Likewise, heparanase gene silencing or administration of heparanase inhibitors attenuated tumor growth [20, 22,23,24, 84, 85] (See chapters 19, 22, 23, 21 by Chhabra and Ferro; Hammond and Dredge; Giannini et al. and Noseda and Barbieri, This book for a detailed discussion on heparanase inhibitors). In addition, recent studies revealed that high levels of heparanase in the tumor metastases predict poor prognosis in stage IVc melanoma patients [39]. This result implies that heparanase not only enhances tumor cells dissemination but also promotes the growth and aggressiveness of the resulting metastases. Notably, larger tumors were produced also by cells engineered to overexpress heparanase mutants and forms (i.e., C-domain, splice variants) that lack heparanase enzymatic activity [45, 46, 86,87,88,89] (Fig. 9.2), clearly implying that heparanase function beyond its enzymatic aspect.

Heparanase promotes the formation of disorganized acinar structures by MCF10A cells and tumorigenicity of MCF10AT1 cells. (A). Acinar structures formation. Control (Mock), heparanase (Hepa), and 8C-infected MCF10A cells were plated on, and overlaid with Matrigel for 10 days. Formation of three-dimensional acini-like structures was evaluated by fluorescent confocal imaging applying DAPI nuclei counterstaining. (B). Tumorigenicity of MCF10AT1 cells. MCF10AT1 cells were infected with control (Mock), heparanase, or 8C gene constructs and inoculated into SCID/beige mouse mammary fat pad (n = 6). Xenografts were harvested 12 weeks after cell transplantation and formalin-fixed, paraffin-embedded 5-micron sections were subjected to histological analyses. Shown are representative images of whole sections scanned by 3DHISTECH Pannoramic MIDI System attached to HITACHI HV-F22 color camera (3dhistech kft, Budapest, Hungary). (C). Immunostaining. Xenografts produced by MCF10AT1 infected cells were stained with anti-vimentin (upper panels) and anti-E-cadherin (second panels) antibodies. Original magnifications: x100
The mechanisms underlying the capacity of heparanase to promote tumor growth are not entirely clear. Conceptually, heparanase activity can potentially release a wide range of biological mediators that are sequestered by HSPG and turn on their activity. Among the proteins sequestered by the ECM are typical pro-angiogenic mediators such as PDGF, HGF, bFGF, HB-EGF, and VEGF-A [90, 91]. Indeed, heparanase exerts a strong pro-angiogenic response in pre-clinical models and clinical settings [20, 22, 84, 85, 92, 93]. Experimentally, Elkin et al. have demonstrated that heparanase can release ECM-bound 125I-bFGF in a highly active form that promotes the proliferation of BaF3 cells [93]. Similarly, the addition of recombinant heparanase could release VEGF-A from cardiomyocytes, but this effect was also exerted by latent heparanase, suggesting displacement rather than cleavage of HS [94]. Similar considerations may also hold for the increase of soluble VEGF receptor 1 (sVEGF-R1) in heparanase-transgenic mice [95]. However, the release of ECM-bound angiogenic- and growth- promoting factors was not demonstrated unequivocally in the context of tumor growth, most probably due to the low levels of protein being released and its local nature. Instead, we and others have shown that heparanase induces the expression of VEGF-A [50, 96,97,98] and VEGF-C [99, 100], leading to increased blood and lymph vessel density. This implies that heparanase not only facilitates tumor cell invasion by loosening the ECM and basement membrane but also increases the density of vessels that mobilize the disseminating cells to distant organs. Subsequent studies revealed that heparanase down-regulates the expression of tumor suppressors [i.e., CXCL10; [45]] and induces the transcription of pro-angiogenic (i.e., COX-2, MMP-9), pro-thrombotic (i.e., tissue factor), pro-inflammatory (i.e., TNFα, IL-1, IL-6, MIP-2), pro-fibrotic (i.e., TGFβ), mitogenic (i.e., HGF), osteolytic (RANKL) and various other genes [22, 50, 99, 101,102,103,104,105,106,107], thus significantly expanding its functional repertoire and mode of action in promoting aggressive tumor behavior. The mode by which heparanase regulates gene transcription is largely unclear but possibly results from its ability to stimulate signal transduction, best exemplified by Src-mediated VEGF-A induction by heparanase [96]. Stimulation of signaling (i.e., increased phosphorylation and activity of protein kinases intrinsic in signal transduction pathways) by heparanase can be indirect, due to the release of HS-bound growth factors. As discussed above, this possibility has not been convincingly proven in preclinical and clinical studies. Alternatively, heparanase was noted to enhance signaling in HS-dependent and -independent manners [89].
3.1 HS-Dependent Signaling
Heparanase interacts with syndecans by virtue of their HS content and the typical high affinity that exists between the enzyme and its substrate. This high-affinity interaction directs clustering of syndecans followed by a rapid and efficient uptake of heparanase [108] (see below). Mechanistically, syndecan clustering by heparanase or the KKDC peptide [corresponding to the heparin binding domain of heparanase [109]] enhanced cell spreading and was associated with PKC, Src, and Rac1 activation [110], molecular determinants shown to be induced by syndecans [111,112,113,114]. This mode of action likely represents a non-enzymatic signaling function of heparanase in its simplest term [89].
3.2 HS-Independent Signaling
Heparanase was noted nonetheless to elicit signaling also in a manner that does not involve HS. Signaling is considered to be HS-independent if it occurs in HS-deficient cells (i.e., CHO 745) or in the presence of heparin, as has been demonstrated for enhanced Akt phosphorylation by heparanase [115]. In fact, heparin, a potent inhibitor of heparanase enzymatic activity, when added together with heparanase, augmented Akt phosphorylation [115], critically implying that heparanase enzymatic activity is not required for Akt activation. In several cases, where tumor xenograft development was examined, heparanase over-expression resulted in tumors bigger in volume and weight [51, 70, 116, 117] coupled with increased Akt phosphorylation [51, 88, 116, 117]. Importantly, heparanase gene silencing was associated with reduced Akt phosphorylation levels [118], further substantiating a role for endogenous heparanase in Akt modulation. Moreover, Akt phosphorylation was markedly attenuated by heparanase inhibitors [46, 119, 120] (also see below). Subsequent studies revealed that heparanase stimulates the phosphorylation of STAT3 and STAT5, Src, EGFR, Erk and the insulin receptor, and moreover activates G-protein receptor signaling [121,122,123,124], all function to promote tumorigenesis. Importantly, enhanced EGFR phosphorylation by heparanase was restricted to selected tyrosine residues (i.e., 845, 1173) thought to be direct targets of Src rather than a result of receptor auto-phosphorylation [125]. Indeed, enhanced EGFR phosphorylation on tyrosine residues 845 and 1173 by heparanase was abrogated in cells treated with Src inhibitors or anti-Src siRNA [121]. Notably, heparanase gene silencing was accompanied by a decrease in cell proliferation, while heparanase overexpression resulted in enhanced cell proliferation and formation of larger colonies in soft agar, in Src- and EGFR-dependent manner [121].
Fux et al. predicted the structure of enzymatically active, single chain, heparanase enzyme, in which the linker segment was replaced by three glycine-serine repeats (GS3) , resulting in a constitutively active enzyme [126]. The structure clearly illustrates a TIM-barrel fold, in agreement with previous predictions [109, 127]. Notably, the structure also delineates a C-terminus fold positioned next to the TIM-barrel structure [88]. Fux et al. thus, hypothesized that the seemingly distinct protein domains observed in the three-dimensional model, namely the TIM-barrel and C-domain regions, mediate enzymatic and non-enzymatic functions of heparanase, respectively [88]. Interestingly, cells transfected with the TIM-barrel construct (amino acids 36–417) failed to display heparanase enzymatic activity, suggesting that the C-domain is required for the establishment of an active heparanase enzyme, possibly by stabilizing the TIM-barrel fold [88]. Deletion and site-directed mutagenesis approach further indicated that the C-domain plays a decisive role in heparanase enzymatic activity and secretion [88, 128, 129]. Remarkably, Akt phosphorylation was stimulated by cells overexpressing the C-domain (amino acids 413–543), while the TIM-barrel protein variant yielded no Akt activation compared with control, mock transfected cells [88]. These findings clearly indicate that the non-enzymatic signaling function of heparanase leading to activation of Akt is mediated by the C-domain. Because the C-domain gene construct lacks the 8 kDa segment which, according to the predicted model, contributes one beta strand to the C-domain structure, the resulting protein may exhibit suboptimal Akt activation. Indeed, Akt phosphorylation was markedly enhanced in cells transfected with a mini gene comprising a segment of the 8 kDa subunit, predicted by the model to contribute a beta strand (Gln36-Ser55) to the C-domain structure, linked to the C-domain sequence. These findings further support the predicted three-dimensional model, indicating that the C-domain is indeed a valid functional domain responsible for Akt phosphorylation (see Chapter 5 by Wu and Davies for a detailed discussion of heparanase crystal structure and new insights regarding structural relationships between the latent and active enzyme). The cellular consequences of C-domain overexpression are best revealed by monitoring tumor xenograft growth. Notably, tumor xenografts produced by C-domain-transfected glioma cells appeared comparable to those produced by cells transfected with the full-length heparanase, while the growth of tumors produced by TIM-barrel-transfected cells appeared comparable with control mock-transfected cells [88].
While signaling through HS clustering appears straightforward in its rational, HS-independent signaling by heparanase requires a mediator, possibly in the form of cell surface receptor(s). The existence of cell surface heparanase receptor is supported by binding experiments. Applying iodinated heparanase to HeLa cells revealed the presence of two distinct types of binding sites exhibiting low-affinity (Kd = 3 mM), high abundant (βmax = 1x108), and high affinity (Kd = 2 nM), low abundant (βmax = 1.7x104) characteristics [130]. Binding studies performed with wild type CHO-KI cells and their HS-deficient CHO-745 counterpart cells have demonstrated that heparanase binding to the high-affinity binding sites is almost identical in both cell types. In contrast, the number of low-affinity binding sites was significantly reduced in CHO-745 vs. CHO-KI cells, and a similar decrease was noted in CHO-KI cells treated with bacterial heparinase III [130]. These studies reinforce the notion that while HSPG serve as low affinity, high abundant binding sites, heparanase also associates with high affinity, low abundant cell surface receptor(s). A first indication for the protein nature of this receptor and its molecular weight emerged from cross-linking experiments, revealing two distinct complexes representing 130 and 170 kDa proteins associated with heparanase [88]. Moreover, Akt phosphorylation by heparanase was found to be mediated by a lipid raft resident protein [118]. Such a receptor has not been isolated and characterized yet. Also, Wood and Hulett have reported that the 300 kDa Cation-independent Mannose 6-Phosphate Receptor (CIMPR; CD222) can bind enzymatically active heparanase [131] and may serve as a heparanase receptor. The affinity of this interaction and the consequences of heparanase binding in term of signaling has not been reported. Alternatively, heparanase may facilitate signaling from within the lysosome.
4 Heparanase Uptake – Is the Message within Lysosomes?
A number of studies have shown that secreted or exogenously added latent heparanase rapidly interacts with normal and tumor-derived cells, followed by internalization and processing into a highly active enzyme [108, 115, 130, 132,133,134,135,136], collectively defined as heparanase uptake. Several approaches, including HS-deficient cells, addition of heparin or xylosides, and deletion of HS-binding domains of heparanase, provided compelling evidence for the involvement of HS in heparanase uptake [109, 132]. While syndecans are regarded as the primary receptors for heparanase endocytosis, low-density lipoprotein receptor-related protein (LRP) and the cation-independent mannose-6-phosphate receptor (CIMPR) have been identified as heparanase-binding proteins [131, 136] that contribute to heparanase uptake. Heparanase uptake is regarded as a pre-requisite for the delivery of latent 65 kDa heparanase to lysosomes and its subsequent proteolytic processing and activation into 8 and 50 kDa that compose the active enzyme. Following uptake, heparanase was noted to reside primarily intracellularly within endocytic vesicles, assuming a polar, peri-nuclear localization and co-localizing with lysosomal markers [133, 137] (Fig. 9.3A). Indeed, heparanase processing was blocked by chloroquine and bafilomycin A1 which inhibit lysosomal proteases by raising the lysosome pH [108]. Subsequent studies employing lysosomal preparation, site-directed mutagenesis, gene silencing, and pharmacological inhibitors have identified cathepsin L as the primary lysosomal protease responsible for heparanase processing and activation [138,139,140]. Moreover, syndecan-1 and 4 are internalized by cells following addition of heparanase, co-localizing with heparanase in endocytic vesicles [132, 141] (Fig. 9.3A). Since syndecans mediate the uptake of a large number of molecules including atherogenic lipoproteins [142, 143] and microorganisms such as bacteria and viruses [144], mechanisms that mediate internalization of syndecan ligands are of interest and clinical significance. Structurally, all syndecans are composed of an extracellular domain, membrane domain, and a conserved short C-terminal cytoplasmic domain divided into the first conserved region (C1), the variable domain (V), and the second conserved region (C2). Each of these cytoplasmic domains has been shown to interact with specific adaptor molecules and to mediate cellular functions [113, 145]. To examine the role of syndecan-1 cytoplasmic domain in heparanase processing, Shteingauz et al. transfected cells with full-length mouse syndecan-1 or deletion constructs lacking the entire cytoplasmic domain (delta), the conserved (C1 or C2) or variable (V) regions [146]. Heparanase uptake was markedly increased following syndecan-1 over expression (Fig. 9.3B, WT), thus challenging the notion that cell surface HS is at saturation and does not limit ligand binding. In contrast, heparanase was retained at the cell membrane, and its processing was impaired in cells overexpressing syndecan-1 deleted for the entire cytoplasmic tail [146] (Fig. 9.3B, Delta). Subsequent studies revealed that the C2 and V regions of syndecan-1 cytoplasmic tail mediate heparanase processing. Furthermore, syntenin, known to interact with syndecan C2 domain, and α actinin were shown to be essential for heparanase processing [146]. These results illustrate the tight regulation of heparanase activation and shed light on syndecan-mediated endocytosis. Interestingly, syndecans and syntenin, via interaction with ALIX, have been implicated in regulating the biogenesis of exosomes [147]. Importantly, heparanase facilitates the production of exosomes and regulates their secretion and composition [148, 149], implying that heparanase-syndecan-syntenin establish a linear axis that regulates exosome formation and the related effects on tumor progression [146] (see Chapters 12, 10 by Sanderson et al., and David and Zimmermann for detailed discussion on heparanase and exosomes).

(A). Altered syndecan localization in response to heparanase addition. U87 glioma cells were incubated with Myc-tagged latent heparanase (10 μg/ml) for 15 min. Cells were then fixed and stained with anti-syndecan-1 (upper panel, green) monoclonal antibody and with anti-Myc polyclonal antibody (Hepa, second panel, red). Merge images are shown in the lower panel. Note internalization of syndecan into endocytic vesicles upon heparanase addition. (B). Heparanase uptake requires the syndecan cytoplasmic tail. Heparanase (1 μg/ml) was added to U87 glioma cells over-expressing wt syndecan-1 or syndecan-1 lacking the entire cytoplasmic tail (delta) for 1 hour at 37 °C. Cells were then fixed with cold methanol and subjected to immunofluorescent staining applying anti-heparanase mouse monoclonal antibody (lower panels, green). Merged images with rat anti-syndecan-1 staining (red) are shown in the upper panels. Note increased heparanase-positive endocytic vesicles in cells overexpressing wild type (WT) syndecan-1, but retention of heparanase at the cell membrane, co-localizing with syndecan lacking the entire cytoplasmic tail (Delta). (C). Heparanase co-localizes with LC3-II. Heparanase (1 μg/ml) was added exogenously to HeLa cells stably expressing a GFP-LC3 gene construct for 24 hours. Cells were then deprived of amino acids in the presence of chloroquine (50 μg/ml; AA+Chl) for 3 hours or were incubated under serum-free conditions as control (Con). Cells were then fixed with methanol and subjected to immunofluorescent staining applying anti-heparanase (middle panels, red) antibody. Co-localization of heparanase and GFP-LC3 appears yellow (lower panel). (D). Electron microscopy. Pancreas tissues from control (Con) and heparanase transgenic mice (Hpa-Tg) were fixed in glutaraldehyde and processed for EM. Shown are representative images at x10,000 magnification. Note a substantial increase in the number and size of autophagosomes in the pancreas of heparanase-transgenic mice
The efficient uptake mechanism and accumulation of heparanase in endocytic vesicles suggest that heparanase is not normally present in association with the ECM, the site of its recognized activity. Active heparanase can get to the cell exterior by one of three mechanisms: 1. Secretion of endocytic vesicles/lysosomes; 2. Processing of latent heparanase into active enzyme outside the cell, and 3. Release by lysosomes/micro-vesicles. The latter, however, is thought to mediate communication between cells and transfer the membrane-enclosed protein and/or its mRNA from one cell to another rather than to release the enzyme. The former mechanisms have been substantiated experimentally [150,151,152], but the secreted enzyme will be subjected to the same principles of uptake (or re-uptake) described above [20]. The rapid and efficient uptake mechanism of heparanase and its accumulation in lysosomes likely serve as an important regulatory mechanism that limit its extracellular retention, due to the damage that this activity may cause to tissues and cells. The instrumental role of the lysosome in signaling raises the possibility that heparanase accumulation in this organelle not only serves as a reservoir for the enzyme but rather plays an important role in its function.
4.1 The Lysosome as a Signaling Organelle
For the past five decades, the lysosome has been characterized as an unglamorous cellular recycling center. This notion has undergone a radical shift in the last 10 years, with new research revealing that this organelle serves as a major hub for metabolic signaling pathways. The discovery that master growth regulators, including the protein kinase mTOR (mechanistic target of rapamycin), make their home at the lysosomal surface has generated intense interest in the lysosome’s key role in nutrient sensing and cellular homeostasis [153,154,155,156]. The transcriptional networks required for lysosomal maintenance and function are a subject of intense research activity, and their connection to lysosome-based signaling pathways was revealed. Much is now understood about how the lysosome contributes to amino acid sensing by mTORC1, the function of the energy-sensing kinase, AMP-activated protein kinase (AMPK) , at the lysosome and how both AMPK and mTORC1 signaling pathways feedback to lysosomal biogenesis and regeneration following autophagy [153,154,155,156]. In fact, the lysosome is intimately involved in each of the classic hallmarks of cancer [154], and compounds that impact lysosomal function are under clinical evaluation [154].
In spite of its localization in a highly active protein degradation environment such as the lysosome, heparanase appears stable [108, 137] and exhibits a half-life of about 30 hours [132], relatively long compared with a t1/2 of 2–6 h, and 25 min for transmembrane and GPI-anchored HSPG, respectively [157]. Residence and accumulation of heparanase in lysosomes indicate that the enzyme may function in the normal physiology of this organelle. In a search for such function, we revealed a role of heparanase in modulating autophagy [48]. Autophagy is an evolutionarily conserved catabolic pathway through which cytoplasmic components, including macromolecules such as proteins and lipids as well as whole organelles, are sequestered into double-membrane vesicles called autophagosomes. Autophagosomes are subsequently fused with lysosomes, where the intracellular material is degraded and recycled. This process occurs in every cell at a basal level and is required to remove unfolded proteins and damaged organelles, thus maintaining cellular homeostasis. Autophagy is further induced by starvation and stress, promoting cancer cells survival by providing their metabolic needs [158, 159]. Our results indicate that heparanase is localized within autophagosomes (Fig. 9.3C) and promotes autophagy. Moreover, enhanced tumor growth and chemo-resistance exerted by heparanase are mediated in part by augmenting autophagy [48]. This was concluded because reduced LC3-II (a protein that specifically associates with autophagosomes) levels are found in cells and tissues obtained from heparanase knockout mice as opposed to elevated LC3-II levels found in transgenic mice that overexpress heparanase. Even higher induction of autophagy was evident in head and neck carcinoma and glioma cells overexpressing heparanase [48], in accordance with a strong pre-clinical and clinical significance of heparanase in the progression of these malignancies [36, 51, 81, 88, 99, 103, 121, 122]. Notably, electron microscopy analyses of cells overexpressing heparanase revealed not only a higher number of autophagic vacuoles (Fig. 9.3D), but also abundant release of vesicles, likely exosomes, from the cell surface [48], further supporting the notion that heparanase enhances exosome secretion that contributes to tumor growth [148, 149]. These results imply that heparanase function is not limited to the extracellular milieu but can function inside the cell [48, 160].
The mechanism underlying autophagy induction by heparanase is not entirely clear, but likely involves mTOR1 that plays a pivotal role in nutrient-sensing and autophagy regulation [161]. mTOR1 activity inhibits autophagy, but under starvation, its activity is repressed, leading to autophagy induction. Shteingauz et al. found that heparanase overexpression associates with reduced mTOR1 activity, evident by decreased levels of p70 S6-kinase phosphorylation, an mTOR1 substrate. In contrast, heparanase-knockout cells exhibited increased mTOR1 activity and p70 S6-kinase phosphorylation [48]. Notably, mTOR1 appears more diffusely scattered in control cells, whereas in cells with a high content of heparanase, mTOR1 is found mostly in peri-nuclear regions, co-localizing with heparanase and LysoTracker that labels acidic lysosomal vesicles. This agrees with the notion that activation of mTOR1 by nutrients is associated with peripheral lysosomes, whereas starvation leads to peri-nuclear clustering of lysosomes and decreased mTOR1 activity [162]. These results imply that autophagy induction contributes to the pro-tumorigenic function of heparanase. This emerges from in vitro and in vivo experiments utilizing inhibitors of autophagy (chloroquine) and heparanase (PG545) alone or in combination [48]. Thus, combining PG545 and chloroquine in a tumor xenograft model resulted in significantly smaller and more differentiated tumors, suggesting that heparanase activity drives cancer cell de-differentiation as part of its pro-tumorigenic properties. Equally important is the ability of heparanase overexpression to confer resistance to stress, chemotherapy and targeted drugs [47], mediated, at least in part, by enhancing autophagy [48]. Indeed, diverse classes of anticancer drugs induce autophagy [163, 164], thus attenuating tumor cell elimination, while autophagy inhibitors overcome chemo-resistance [165, 166]. Based on this concept, chloroquine is currently evaluated in several clinical trials in combination with different classes of chemotherapeutic agents [165, 167].
Modulation of mTOR activity and autophagy by heparanase likely represents only the tip of the iceberg; lysosomal heparanase possibly modulate many other aspects of lysosome function in health and disease, but this notion awaits in-depth validation. Moreover, it is possible that lysosomal heparanase needs to be targeted in order to attenuate tumor growth.
5 Heparanase Inhibitors – Are We Targeting Well?
The search for heparanase inhibitors started soon after the appreciation of its pro-metastatic properties [168, 169]. Since then, many heparanase inhibitors have been developed (Discussed in detail by Chhabra & Ferro; Hammond & Dredge; Giannini et al. and Noseda and Barbieri, Chaps. 19, 21, 22 and 23; in this volume). These include, among others, heparin/HS mimetics (i.e., SST0001 = Roneparstat, M402 = Necuparanib, PI-88 = Mupafostat), synthetic, fully sulfated HS mimetic (PG545 = Pixatimod), neutralizing antibodies, small molecules, oligonucleotides (i.e., defibrotide), natural products and their derivatives, and many others [23, 85, 120, 170,171,172,173]. Of these, Mupafostat, Roneparstat, Necuparanib, and Pixatimod were examined clinically [16,17,18,19]. These compounds as well as the anti-heparanase neutralizing monoclonal antibodies that show some potency in pre-clinical models [49], do not penetrate the cell and their inhibition potential is restricted to the cell exterior. This likely explains the low toxicity of these compounds [16, 17]. Given the above considerations and the seemingly low abundance of heparanase outside the cells, the eminent question would be what exactly are these inhibitors targeting? A possible explanation comes from the observation that the heparin/HS mimetics as well the neutralizing antibodies not only inhibit heparanase activity but also attenuate its uptake, resulting in accumulation of heparanase in the cell culture medium, accompanied with reduced lysosomal content [[49, 50] and our unpublished results]. This may suggest that attenuation of tumor growth results in whole or in part from reduced intracellular content of heparanase. Thus, the ideal inhibitor should target heparanase both inside and outside the cell, attenuating HS cleavage and signaling, in order to neutralize its diverse functions and bring heparanase inhibitors closer to the clinic.
6 Is Hpa2 the Answer?
Cloning of a single human heparanase cDNA sequence independently reported by several groups [12,13,14,15] implied that one active heparanase enzyme exists in mammals. Further analysis of human genomic DNA led researchers to conclude that the heparanase gene is unique and that the existence of related proteins is unlikely [174]. Based on amino acid sequence, McKenzie and colleagues nonetheless reported the cloning of heparanase homolog termed heparanase 2 (Hpa2) [174]. The full-length HPSE2 gene consists of 2353 bp encoding a protein of 592 amino acids; Alignment of the coding region of heparanase and Hpa2 reveals an overall identity of 40% and sequence resemblance of 59%, including conservation of residues critical for heparanase enzymatic activity (Glu225 and Glu343) [174]. The segment corresponding to the linker region and cleavage sites of pro-heparanase are not conserved in Hpa2 [20]. Importantly, Hpa2 lacks intrinsic HS-degrading activity, the hallmark of heparanase [141], and seems not to undergo processing in a manner required for heparanase activation. This may be due to differences in the cellular localization of Hpa2 and its sequestration from the lysosome. Wild type Hpa2 (Hpa2c) [141, 174] is secreted and markedly accumulates in the cell conditioned medium following the addition of heparin or HS but not hyaluronic acid, indicating that Hpa2 retains the capacity to interact with HS despite the lack of HS-degrading activity [141]. In fact, Hpa2 exhibits even higher affinity towards heparin and HS than heparanase [141], thus competing for HS binding and thereby inhibiting heparanase enzymatic activity [141]. Moreover, co-immunoprecipitation studies revealed physical association between Hpa2 and heparanase proteins [141], providing an additional route by which Hpa2 can inhibit heparanase enzymatic activity. Immunofluorescent staining illustrates Hpa2 localization on the cell surface following its exogenous addition, co-localizing with and clustering of syndecan-1 and -4 (Fig. 9.5, left image). Unlike heparanase, Hpa2 does not appear to get internalized into endocytic vesicles but rather remains on the cell surface for a relatively long period of time [141]. This result clearly indicates that the rapid and efficient internalization of heparanase together with syndecans (Fig. 9.3A) [108, 109, 175] is unique and not purely a consequence of HS-ligand binding. Moreover, the lack of Hpa2 processing may be due to its sequestration from the lysosome and lysosomal enzymes. Thus, while Hpa2 can inhibit heparanase activity extracellularly, it cannot affect lysosomal heparanase directly. However, Hpa2 attenuate heparanase uptake, possibly due to its high affinity to HS, resulting in depletion of lysosomal heparanase [141]. In this regard, Hpa2 function in a manner similar to HS-mimetic heparanase inhibitors [48]. In addition to the full-length Hpa2 protein (Hpa2c), several variants have been identified as a result of alternative splicing of the HPSE2 transcript, including Hpa2a (480 aa) and Hpa2b (534 aa) [174]; Another splice variant of Hpa2, composed of only 528 amino acids, was described by Vreys and David [20]. Notably, only wild type Hpa2 is secreted, likely due to extra glycosylation sites that are lost in the splice variants [141]. The biological significance and cellular localization of Hpa2 splice variants are yet to be revealed. Localization of Hpa2 splice variants to the lysosome will imply that whereas wild type Hpa2 can modulate heparanase activity in the cell exterior, its splice variants will modulate heparanase activity inside cells.
6.1 Hpa2 in Cancer Progression-an Opposite Answer
Very little attention was given to Hpa2 in general, and only a few studies attempted to reveal its significance in cancer (see Chapters by Roberts and Woolf, and by Mckenzie, Chaps. 34 and 35; in this volume). However, the emerging results clearly suggest that Hpa2 function in cancer is the exact opposite of heparanase. The notion that Hpa2 function as a tumor suppressor is supported by the following observations. Unlike heparanase, Hpa2 staining is evident in the normal epithelium of the bladder, breast, gastric and ovarian tissues. Notably, Hpa2 levels are reduced substantially in the resulting carcinomas (Fig. 9.4), a staining pattern typical of a tumor suppressor. In other cases, such as head and neck cancer, the opposite is observed [141]. The reason for this behavior is unclear. Importantly, nonetheless, head and neck cancer patients exhibiting high levels of Hpa2 showed prolonged time to disease recurrence (follow-up to failure) and inversely correlated with tumor cell dissemination to regional lymph nodes [141], thus providing clinical relevance for the antitumor properties of Hpa2. Notably, overexpression of Hpa2 in head and neck cancer cells resulted in a marked reduction in tumor growth, associating with a prominent reduction in tumor vascularity (blood and lymph vessels) likely due to reduced Id1 expression [176], a transcription factor highly implicated in VEGF-A and VEGF-C gene regulation [177]. Moreover, growth of tumor xenografts produced by Hpa2 over-expressing cells was not affected by a monoclonal antibody that targets a heparin binding domain of Hpa2 [176], implying that Hpa2 functions in HS-independent manner. Tumor produced by cells over-expressing Hpa2 were not only smaller but also exhibited a higher degree of cell differentiation (i.e., cytokeratin expression) [176]. Likewise, high levels of Hpa2 in bladder cancer patients correlated inversely with tumor grade and stage [178], further strengthening the significance of Hpa2 as a tumor suppressor and its role in cell differentiation. Thus, heparanase and Hpa2 not only exhibit opposite function in term of tumor growth but also in term of the underlying mechanism. For example, while heparanase induces VEGF-A and VEGF-C expression and promote angiogenesis, Hpa2 attenuate the expression of VEGF-A and VEGF-C and decrease tumor vascularity; whereas heparanase reduce cell differentiation and promote epithelial to mesenchymal transition (EMT) (Fig. 9.2; [179]), Hpa2 increase cell differentiation [176, 178]. This mirrored functionality strongly suggests that Hpa2 exert these properties by modulating heparanase, but we could not demonstrate decreased heparanase activity in cells overexpressing Hpa2 [176], possibly due to the semi-quantitative assay being employed. Given the above considerations, however, it is possible that the main function of Hpa2 is not to inhibit heparanase activity extracellularly, but rather to deplete heparanase from the lysosome.

Hpa2 immunostaining appears strong in normal epithelium and is decreased substantially in the resulting carcinomas. Biopsies of gastric (upper panels), ovarian (second panels), breast (third panels), and bladder (lower panels) carcinomas were subjected to immunostaining applying anti-Hpa2 polyclonal antibody. Strong Hpa2 staining is detected in normal epithelium of the gastric, ovarian, breast and bladder tissues adjacent the tumor lesion (left panels) which is decreased substantially in the carcinomas (right panels)

Schematic presentation of heparanase and Hpa2 biosynthesis and trafficking. Pre-pro-heparanase (red circles) and Hpa2 (green triangles) are first targeted to the ER lumen via their own signal peptides (1). The proteins are then shuttled to the Golgi apparatus and are subsequently secreted via vesicles that bud from the Golgi (2). Once secreted, heparanase rapidly interacts with syndecans, resulting in their clustering and signaling (3), followed by rapid endocytosis of the heparanase-syndecan complex (5) that accumulates in late endosomes (6). Hpa2 interacts with cell membrane HSPG (i.e., syndecans) with higher affinity but unlike heparanase, is not subjected to uptake but rather remains on the cell membrane for a relatively long period of time (4 & left inset). Accumulation of Hpa2 in the extracellular compartment is enhanced by heparin or anti-Hpa2 (1c7) monoclonal antibody. Heparanase uptake is inhibited by heparin/heparin mimetics, anti-heparanase monoclonal antibodies, or Hpa2, resulting in extracellular accumulation of the latent enzyme ( , 5). Conversion of endosomes to lysosomes results in heparanase processing and activation (primarily by cathepsin L). Typically, heparanase appears in perinuclear lysosomes (right inset) and is thought to promote autophagy (7) and tumor growth, metastasis, angiogenesis, and chemo-resistance due to its enzymatic and signaling (8) functions whereas Hpa2 appear to attenuate tumor growth and vascularity. Novel heparanase inhibitors are hoped to target extracellular latent (signaling) and active heparanase as well as the intracellular, lysosomal, enzyme
, 5). Conversion of endosomes to lysosomes results in heparanase processing and activation (primarily by cathepsin L). Typically, heparanase appears in perinuclear lysosomes (right inset) and is thought to promote autophagy (7) and tumor growth, metastasis, angiogenesis, and chemo-resistance due to its enzymatic and signaling (8) functions whereas Hpa2 appear to attenuate tumor growth and vascularity. Novel heparanase inhibitors are hoped to target extracellular latent (signaling) and active heparanase as well as the intracellular, lysosomal, enzyme
7 Heparanase Message Revisited
Twenty years after cloning the HPSE gene, heparanase research has made substantial progress, clearly revealing the clinical significance of the enzyme and turning heparanase into a valid target for the development of anti-cancer therapeutics. Progress was also made in deciphering the role of heparanase in inflammation, viral infection, diabetes, and other pathologies (see chapters by Elkin et al., Simeonovic et al., Masola et al., and Agelidis and Shukla, Chaps. 17, 24, 27 and 32; in this volume). Disclosing its mode of action and the translation of the knowledge into clinical practice is nonetheless insufficient. In this Review, we challenge some of the concepts that guided the field, hoping that new ideas and thinking will advance basic and translational aspects of heparanase.
Based on the house-keeping nature of its gene promoter, we suggest that heparanase is expressed at low levels by all cells, modulating autophagy and possibly other functions of the lysosome. According to this notion, heparanase function in the lysosome is equally, or possibly more important than its function extracellularly. This may turn most relevant in platelets, neutrophils, lymphocytes and macrophages that show relatively high levels of heparanase expression/activity [13, 50, 60], and also in normal epithelium [180]. Beyond serving as a cellular recycling center, recent evidence suggests that the lysosome is involved in homeostasis, generating building blocks for cell growth, mitogenic signaling, angiogenesis and metastasis, and activation of transcriptional programs [154, 156], repertoire that closely resembles those of heparanase. The PI3-kinase/Akt/mTOR is highly implicated in the regulation of cell metabolism, protein homeostasis, and cell growth due, in part, to the localization of mTOR at the lysosome membrane which is required for its activation [153, 181]. In fact, Akt is the most common kinase activated by heparanase [46, 51, 88, 101, 115,116,117,118,119, 121, 122, 182,183,184,185], and its instrumental role in the regulation of mTOR would likely convey to the lysosome [181]. Clearly, more work is required to critically resolve the significance of heparanase in modulating lysosomal function in normal cells and in tumor growth, metastasis, and chemo-resistance.
As already described above, heparanase inhibitors were solely directed to neutralize its enzymatic activity and most often yielded disappointing results in pre-clinical models, with the exception of PG545 (Pixatimod). The specificity of this compound is, nonetheless, questionable, because it also exerts heparanase-independent functions and attenuates the growth of tumor xenografts produced by heparanase-negative lymphoma cells [186]. A new generation of heparanase inhibitors, possibly in the form of small molecules, should also target its signaling activity at the cell membrane and inside the lysosome in order to better neutralize all aspects of heparanase function. This will lead to better appreciation of heparanase role in health and disease and, hopefully, will enable improved clinical application of these compounds in cancer, inflammation, and other pathologies.
References
Ogren, S., & Lindahl, U. (1975). Cleavage of macromolecular heparin by an enzyme from mouse mastocytoma. The Journal of Biological Chemistry, 250, 2690–2697.
Hook, M., Wasteson, A., & Oldberg, A. (1975). A heparan sulfate-degrading endoglycosidase from rat liver tissue. Biochemical and Biophysical Research Communications, 67, 1422–1428.
Nakajima M, Irimura, T., DiFerrante, D., DiFerrante, N., Nicolson, G. L. Heparan sulfate degradation: Relation to tumor invasion and metastatic properties of mouse B 16 melanoma sublines. Science (Wash DC). 1983;220:611–613.
Nakajima, M., Irimura, T., Di Ferrante, N., & Nicolson, G. L. (1984). Metastatic melanoma cell heparanase. Characterization of heparan sulfate degradation fragments produced by B16 melanoma endoglucuronidase. The Journal of Biological Chemistry, 259, 2283–2290.
Vlodavsky, I., Fuks, Z., Bar-Ner, M., Ariav, Y., & Schirrmacher, V. (1983). Lymphoma cells mediated degradation of sulfated proteoglycans in the subendothelial extracellular matrix: Relation to tumor cell metastasis. Cancer Research, 43, 2704–2711.
Bar-Ner, M., Kramer, M. D., Schirrmacher, V., Ishai-Michaeli, R., Fuks, Z., & Vlodavsky, I. (1985). Sequential degradation of heparan sulfate in the subendothelial extracellular matrix by highly metastatic lymphoma cells. International Journal of Cancer, 35, 483–491.
Matzner, Y., Bar-Ner, M., Yahalom, J., Ishai-Michaeli, R., Fuks, Z., & Vlodavsky, I. (1985). Degradation of heparan sulfate in the subendothelial extracellular matrix by a readily released heparanase from human neutrophils. Possible role in invasion through basement membranes. The Journal of Clinical Investigation, 76, 1306–1313.
Bame, K. J. (2001). Heparanases: endoglycosidases that degrade heparan sulfate proteoglycans. Glycobiology, 11, 91R–98R.
Vlodavsky, I., & Friedmann, Y. (2001). Molecular properties and involvement of heparanase in cancer metastasis and angiogenesis. The Journal of Clinical Investigation, 108, 341–347.
Parish, C. R., Freeman, C., & Hulett, M. D. (2001). Heparanase: A key enzyme involved in cell invasion. Biochimica et Biophysica Acta, 1471, M99–M108.
Dempsey, L. A., Brunn, G. J., & Platt, J. L. (2000). Heparanase, a potential regulator of cell-matrix interactions. Trends in Biochemical Sciences, 25, 349–351.
Hulett, M. D., Freeman, C., Hamdorf, B. J., Baker, R. T., Harris, M. J., & Parish, C. R. (1999). Cloning of mammalian heparanase, an important enzyme in tumor invasion and metastasis. Nature Medicine, 5, 803–809.
Kussie, P. H., Hulmes, J. D., Ludwig, D. L., Patel, S., Navarro, E. C., Seddon, A. P., et al. (1999). Cloning and functional expression of a human heparanase gene. Biochemical and Biophysical Research Communications, 261, 183–187.
Toyoshima, M., & Nakajima, M. (1999). Human heparanase. Purification, characterization, cloning, and expression. The Journal of Biological Chemistry, 274, 24153–24160.
Vlodavsky, I., Friedmann, Y., Elkin, M., Aingorn, H., Atzmon, R., Ishai-Michaeli, R., et al. (1999). Mammalian heparanase: Gene cloning, expression and function in tumor progression and metastasis. Nature Medicine, 5, 793–802.
Dredge, K., Brennan, T. V., Hammond, E., Lickliter, J. D., Lin, L., Bampton, D., et al. (2018). A phase I study of the novel immunomodulatory agent PG545 (pixatimod) in subjects with advanced solid tumours. British Journal of Cancer, 118, 1035–1041.
Galli, M., Chatterjee, M., Grasso, M., Specchia, G., Magen, H., Einsele, H., et al. (2018). Phase I study of the heparanase inhibitor roneparstat: An innovative approach for ultiple myeloma therapy. Haematologica, 103, e469–ee72.
O’Reilly, E. M., Roach, J., Miller, P., Yu, K. H., Tjan, C., Rosano, M., et al. (2017). Safety, pharmacokinetics, pharmacodynamics, and antitumor activity of necuparanib combined with nab-paclitaxel and gemcitabine in patients with metastatic pPancreatic cancer: Phase I results. The Oncologist, 22, 1429–e139.
Liu, C. J., Lee, P. H., Lin, D. Y., Wu, C. C., Jeng, L. B., Lin, P. W., et al. (2009). Heparanase inhibitor PI-88 as adjuvant therapy for hepatocellular carcinoma after curative resection: A randomized phase II trial for safety and optimal dosage. Journal of Hepatology, 50, 958–968.
Vreys, V., & David, G. (2007). Mammalian heparanase: What is the message? Journal of Cellular and Molecular Medicine, 11, 427–452.
Rickles, F. R. (2006). If heparanase is the answer, what is the question? Journal of Thrombosis and Haemostasis, 4, 557–559.
Ilan, N., Elkin, M., & Vlodavsky, I. (2006). Regulation, function and clinical significance of heparanase in cancer metastasis and angiogenesis. The International Journal of Biochemistry & Cell Biology, 38, 2018–2039.
Rivara, S., Milazzo, F. M., & Giannini, G. (2016). Heparanase: A rainbow pharmacological target associated to multiple pathologies including rare diseases. Future Medicinal Chemistry, 8, 647–680.
Vlodavsky, I., Beckhove, P., Lerner, I., Pisano, C., Meirovitz, A., Ilan, N., et al. (2012). Significance of heparanase in cancer and inflammation. Cancer Microenvironment, 5, 115–132.
Gohji, K., Okamoto, M., Kitazawa, S., Toyoshima, M., Dong, J., Katsuoka, Y., et al. (2001). Heparanase protein and gene expression in bladder cancer. The Journal of Urology, 166, 1286–1290.
Tang, W., Nakamura, Y., Tsujimoto, M., Sato, M., Wang, X., Kurozumi, K., et al. (2002). Heparanase: A key enzyme in invasion and metastasis of gastric carcinoma. Modern Pathology, 15, 593–598.
Ohkawa, T., Naomoto, Y., Takaoka, M., Nobuhisa, T., Noma, K., Motoki, T., et al. (2004). Localization of heparanase in esophageal cancer cells: Respective roles in prognosis and differentiation. Laboratory Investigation, 84, 1289–1304.
Beckhove, P., Helmke, B. M., Ziouta, Y., Bucur, M., Dorner, W., Mogler, C., et al. (2005). Heparanase expression at the invasion front of human head and neck cancers and correlation with poor prognosis. Clinical Cancer Research, 11, 2899–2906.
Takaoka, M., Naomoto, Y., Ohkawa, T., Uetsuka, H., Shirakawa, Y., Uno, F., et al. (2003). Heparanase expression correlates with invasion and poor prognosis in gastric cancers. Laboratory Investigation, 83, 613–622.
Rohloff, J., Zinke, J., Schoppmeyer, K., Tannapfel, A., Witzigmann, H., Mossner, J., et al. (2002). Heparanase expression is a prognostic indicator for postoperative survival in pancreatic adenocarcinoma. British Journal of Cancer, 86, 1270–1275.
Sato, T., Yamaguchi, A., Goi, T., Hirono, Y., Takeuchi, K., Katayama, K., et al. (2004). Heparanase expression in human colorectal cancer and its relationship to tumor angiogenesis, hematogenous metastasis, and prognosis. Journal of Surgical Oncology, 87, 174–181.
Kelly, T., Miao, H.-Q., Yang, Y., Navarro, E., Kussie, P., Huang, Y., et al. (2003). High heparanase activity in multiple myeloma is associated with elevated microvessel density. Cancer Research, 63, 8749–8756.
Barash, U., Lapidot, M., Zohar, Y., Loomis, C., Moreira, A., Feld, S., et al. (2018). Involvement of Heparanase in the pathogenesis of mesothelioma: Basic aspects and clinical applications. Journal of the National Cancer Institute, 110, 1102–1114.
Cheng, C., Lu, X., Wang, G., Zheng, L., Shu, X., Zhu, S., et al. (2010). Expression of SATB1 and heparanase in gastric cancer and its relationship to clinicopathologic features. Acta Pathologica, Microbiologica, et Immunologica Scandinavica., 118, 855–863.
Hu, B., Wang, Q., Shi, Y., Lu, S., Qu, H., Wang, L., et al. (2017). Significance of heparanase in metastatic lymph nodes of cervical squamous cell cancer. Oncology Lett., 13, 3219–3224.
Kundu, S., Xiong, A., Spyrou, A., Wicher, G., Marinescu, V. D., Edqvist, P. D., et al. (2016). Heparanase promotes glioma progression and is inversely correlated with patient survival. Molecular Cancer Research, 14, 1243–1253.
Leiser, Y., Abu-El-Naaj, I., Sabo, E., Akrish, S., Ilan, N., Ben-Izhak, O., et al. (2011). Prognostic value of heparanase expression and cellular localization in oral cancer. Head & Neck, 33, 871–877.
Sun, X., Zhang, G., Nian, J., Yu, M., Chen, S., Zhang, Y., et al. (2017). Elevated heparanase expression is associated with poor prognosis in breast cancer: A study based on systematic review and TCGA data. Oncotarget, 27, 43521–43535.
Vornicova O, Boyango I, Feld S, Naroditsky I, Kazarin O, Zohar Y, et al. The prognostic significance of heparanase expression in metastatic melanoma. Oncotarget. 2016;15;7(46):74678–74685.
Vornicova, O., Naroditsky, I., Boyango, I., Shachar, S. S., Mashiach, T., Ilan, N., et al. (2018). Prognostic significance of heparanase expression in primary and metastatic breast carcinoma. Oncotarget, 9, 6238–6244.
Wang, X., Wen, W., Wu, H., Chen, Y., Ren, G., & Guo, W. (2013). Heparanase expression correlates with poor survival in oral mucosal melanoma. Medical Oncology, 30, 633.
Wu, X., Yu, J., Gao, G., Wang, X., Liu, Y., Zhu, S., et al. (2015). Salivary Heparanase level is a potential biomarker to diagnose and Prognose the malignant salivary gland tumor. PLoS One, 10, e0143009.
Xia, F., Xu, J. C., Zhang, P., Zhang, Y. Y., Zhang, Q. W., Chao, Z. H., et al. (2014). Glucose-regulated protein 78 and heparanase expression in oral squamous cell carcinoma: Correlations and prognostic significance. World Journal of Surgical Oncology, 12, 121.
Arvatz, G., Shafat, I., Levy-Adam, F., Ilan, N., & Vlodavsky, I. (2011). The heparanase system and tumor metastasis: Is heparanase the seed and soil? Cancer Metastasis Reviews, 30, 253–268.
Barash, U., Zohar, Y., Wildbaum, G., Beider, K., Nagler, A., Karin, N., et al. (2014). Heparanase enhances myeloma progression via CXCL10 downregulation. Leukemia, 28, 2178–2187.
Boyango, I., Barash, U., Naroditsky, I., Li, J. P., Hammond, E., Ilan, N., et al. (2014). Heparanase cooperates with Ras to drive breast and skin tumorigenesis. Cancer Research, 74, 4504–4514.
Ramani, V. C., Zhan, F., He, J., Barbieri, P., Noseda, A., Tricot, G., et al. (2016). Targeting heparanase overcomes chemoresistance and diminishes relapse in myeloma. Oncotarget, 7, 1598–1607.
Shteingauz, A., Boyango, I., Naroditsky, I., Hammond, E., Gruber, M., Doweck, I., et al. (2015). Heparanase enhances tumor growth and chemoresistance by promoting autophagy. Cancer Research, 75, 3946–3957.
Weissmann, M., Arvatz, G., Horowitz, N., Feld, S., Naroditsky, I., Zhang, Y., et al. (2016). Heparanase-neutralizing antibodies attenuate lymphoma tumor growth and metastasis. Proceedings of the National Academy of Sciences of the United States of America, 113, 704–709.
Gutter-Kapon, L., Alishekevitz, D., Shaked, Y., Li, J. P., Aronheim, A., Ilan, N., et al. (2016). Heparanase is required for activation and function of macrophages. Proceedings of the National Academy of Sciences of the United States of America, 113, E7808–E7E17.
Arvatz, G., Barash, U., Nativ, O., Ilan, N., & Vlodavsky, I. (2011). Post-transcriptional regulation of heparanase gene expression by a 3’ AU-rich element. The FASEB Journal, 24, 4969–4976.
Ostrovsky, O., Korostishevsky, M., Shafat, I., Mayorov, M., Ilan, N., Vlodavsky, I., et al. (2009). Inverse correlation between HPSE gene single nucleotide polymorphisms and heparanase expression: Possibility of multiple levels of heparanase regulation. Journal of Leukocyte Biology, 86, 445–455.
Ostrovsky, O., Shimoni, A., Baryakh, P., Morgulis, Y., Mayorov, M., Beider, K., et al. (2014). Modification of heparanase gene expression in response to conditioning and LPS treatment: Strong correlation to rs4693608 SNP. Journal of Leukocyte Biology, 95, 677–688.
Ostrovsky, O., Grushchenko-Polaq, A. H., Beider, K., Mayorov, M., Canaani, J., Shimoni, A., et al. (2018). Identification of strong intron enhancer in the heparanase gene: Effect of functional rs4693608 variant on HPSE enhancer activity in hematological and solid malignancies. Oncogene, 7, 51.
Jiang, P., Kumar, A., Parrillo, J. E., Dempsey, L. A., Platt, J. L., Prinz, R. A., et al. (2002). Cloning and characterization of the human heparanase-1 (HPR1) gene promoter: Role of GA-binding protein and Sp1 in regulating HPR1 basal promoter activity. The Journal of Biological Chemistry, 277, 8989–8998.
Lu, W. C., Liu, Y. N., Kang, B. B., & Chen, J. H. (2003). Trans-activation of heparanase promoter by ETS transcription factors. Oncogene, 22, 919–923.
O’Connor, L., Gilmour, J., & Bonifer, C. (2016). The role of the ubiquitously expressed transcription factor Sp1 in tissue-specific transcriptional regulation and in disease. The Yale Journal of Biology and Medicine, 89, 513–525.
de Mestre, A. M., Khachigian, L. M., Santiago, F. S., Staykova, M. A., & Hulett, M. D. (2003). Regulation of inducible heparanase gene transcription in activated T cells by early growth response 1. The Journal of Biological Chemistry, 278, 50377–50385.
de Mestre, A. M., Rao, S., Hornby, J. R., Soe-Htwe, T., Khachigian, L. M., & Hulett, M. D. (2005). Early growth response gene 1 (EGR1) regulates Heparanase gene transcription in tumor cells. The Journal of Biological Chemistry, 280, 35136–35147.
de Mestre, A. M., Soe-Htwe, T., Sutcliffe, E. L., Rao, S., Pagler, E. B., Hornby, J. R., et al. (2007). Regulation of mouse Heparanase gene expression in T lymphocytes and tumor cells. Immunology and Cell Biology, 85, 205–214.
de Mestre, A. M., Staykova, M. A., Hornby, J. R., Willenborg, D. O., & Hulett, M. D. (2007). Expression of the heparan sulfate-degrading enzyme heparanase is induced in infiltrating CD4+ T cells in experimental autoimmune encephalomyelitis and regulated at the level of transcription by early growth response gene 1. Journal of Leukocyte Biology, 82, 1289–1300.
Meirovitz, A., Hermano, E., Lerner, I., Zcharia, E., Pisano, C., Peretz, T., et al. (2011). Role of heparanase in radiation-enhanced invasiveness of pancreatic carcinoma. Cancer Research, 71, 2772–2780.
Shteper, P. J., Zcharia, E., Ashhab, Y., Peretz, T., Vlodavsky, I., & Ben-Yehuda, D. (2003). Role of promoter methylation in regulation of the mammalian heparanase gene. Oncogene, 22, 7737–7749.
Ogishima, T., Shiina, H., Breault, J. E., Tabatabai, L., Bassett, W. W., Enokida, H., et al. (2005). Increased heparanase expression is caused by promoter hypomethylation and up-regulation of transcriptional factor early growth response-1 in human prostate cancer. Clinical Cancer Research, 11, 1028–1036.
Ogishima, T., Shiina, H., Breault, J. E., Terashima, M., Honda, S., Enokida, H., et al. (2005). Promoter CpG hypomethylation and transcription factor EGR1 hyperactivate heparanase expression in bladder cancer. Oncogene, 24, 6765–6772.
Bakheet, T., Frevel, M., Williams, B. R., Greer, W., & Khabar, K. S. (2001). ARED: Human AU-rich element-containing mRNA database reveals an unexpectedly diverse functional repertoire of encoded proteins. Nucleic Acids Research, 29, 246–254.
Barreau, C., Paillard, L., & Osborne, H. B. (2005). AU-rich elements and associated factors: Are there unifying principles? Nucleic Acids Research, 33, 7138–7150.
Chen, C. Y., & Shyu, A. B. (1995). AU-rich elements: Characterization and importance in mRNA degradation. Trends in Biochemical Sciences, 20, 465–470.
Eberhardt, W., Doller, A., Akool el, S., & Pfeilschifter, J. (2007). Modulation of mRNA stability as a novel therapeutic approach. Pharmacology & Therapeutics, 114, 56–73.
Cohen, I., Pappo, O., Elkin, M., San, T., Bar-Shavit, R., Hazan, R., et al. (2006). Heparanase promotes growth, angiogenesis and survival of primary breast tumors. International Journal of Cancer, 118, 1609–1617.
Elkin, M., Cohen, I., Zcharia, E., Orgel, A., Guatta-Rangini, Z., Peretz, T., et al. (2003). Regulation of heparanase gene expression by estrogen in breast cancer. Cancer Research, 63, 8821–8826.
Cohen, I., Maly, B., Simon, I., Meirovitz, A., Pikarsky, E., Zcharia, E., et al. (2007). Tamoxifen induces heparanase expression in estrogen receptor-positive breast cancer. Clinical Cancer Research, 13, 4069–4077.
Baraz, L., Haupt, Y., Elkin, M., Peretz, T., & Vlodavsky, I. (2006). Tumor suppressor p53 regulates heparanase gene expression. Oncogene, 25, 3939–3947.
Rao, G., Liu, D., Xing, M., Tauler, J., Prinz, R. A., & Xu, X. (2010). Induction of heparanase-1 expression by mutant B-Raf kinase: Role of GA binding protein in heparanase-1 promoter activation. Neoplasia, 12, 946–956.
Ibrahim, S. A., Hassan, H., & Gotte, M. (2014). MicroRNA regulation of proteoglycan function in cancer. The FEBS Journal, 281, 5009–5022.
Tang, D., Zhang, Q., Zhao, S., Wang, J., Lu, K., Song, Y., et al. (2013). The expression and clinical significance of microRNA-1258 and heparanase in human breast cancer. Clinical Biochemistry, 46, 926–932.
Zhang, L., Sullivan, P. S., Goodman, J. C., Gunaratne, P. H., & Marchetti, D. (2011). MicroRNA-1258 suppresses breast cancer brain metastasis by targeting heparanase. Cancer Research, 71, 645–654.
Qu, H., Zheng, L., Pu, J., Mei, H., Xiang, X., Zhao, X., et al. (2015). miRNA-558 promotes tumorigenesis and aggressiveness of neuroblastoma cells through activating the transcription of heparanase. Human Molecular Genetics, 24, 2539–2551.
El-Assal, O. N., Yamanoi, A., Ono, T., Kohno, H., & Nagasue, N. (2001). The clinicopathological significance of heparanase and basic fibroblast growth factor expressions in hepatocellular carcinoma. Clinical Cancer Research, 7, 1299–1305.
Maxhimer, J. B., Quiros, R. M., Stewart, R., Dowlatshahi, K., Gattuso, P., Fan, M., et al. (2002). Heparanase-1 expression is associated with the metastatic potential of breast cancer. Surgery, 132, 326–333.
Doweck, I., Kaplan-Cohen, V., Naroditsky, I., Sabo, E., Ilan, N., & Vlodavsky, I. (2006). Heparanase localization and expression by head and neck cancer: Correlation with tumor progression and patient survival. Neoplasia, 8, 1055–1061.
Nagler, R., Ben-Izhak, O., Cohen-Kaplan, V., Shafat, I., Vlodavsky, I., Akrish, S., et al. (2007). Heparanase up-regulation in tongue cancer: Tissue and saliva analysis. Cancer, 110, 2732–2739.
Shafat, I., Ben-Arush, M. W., Issakov, J., Meller, I., Naroditsky, I., Tortoreto, M., et al. (2011). Pre-clinical and clinical significance of heparanase in Ewing’s sarcoma. Journal of Cellular and Molecular Medicine, 15, 1857–1864.
Vlodavsky, I., Gross-Cohen, M., Weissmann, M., Ilan, N., & Sanderson, R. D. (2018). Opposing functions of Heparanase-1 and Heparanase-2 in Cancer progression. Trends in Biochemical Sciences, 43, 18–31.
Vlodavsky, I., Singh, P., Boyango, I., Gutter-Kapon, L., Elkin, M., Sanderson, R. D., et al. (2016). Heparanase: From basic research to therapeutic applications in cancer and inflammation. Drug Res Updates., 29, 54–75.
Barash, U., Arvatz, G., Farfara, R., Naroditsky, I., Doweck, I., Feld, S., et al. (2012). Clinical significance of heparanase splice variant (t5) in renal cell carcinoma: Evaluation by a novel t5-specific monoclonal antibody. PLoS One, 7, e51494.
Barash, U., Cohen-Kaplan, V., Arvatz, G., Gingis-Velitski, S., Levy-Adam, F., Nativ, O., et al. (2010). A novel human heparanase splice variant, T5, endowed with protumorigenic characteristics. The FASEB Journal, 24, 1239–1248.
Fux, L., Feibish, N., Cohen-Kaplan, V., Gingis-Velitski, S., Feld, S., Geffen, C., et al. (2009). Structure-function approach identifies a COOH-terminal domain that mediates heparanase signaling. Cancer Research, 69, 1758–1767.
Fux, L., Ilan, N., Sanderson, R. D., & Vlodavsky, I. (2009). Heparanase: Busy at the cell surface. Trends in Biochemical Sciences, 34, 511–519.
Billings, P. C., & Pacifici, M. (2015). Interactions of signaling proteins, growth factors and other proteins with heparan sulfate: Mechanisms and mysteries. Connective Tissue Research, 56, 272–280.
Lindahl U, Couchman J, Kimata K, Esko JD. Proteoglycans and Sulfated Glycosaminoglycans. In: rd, Varki A, Cummings RD, et al., editors. Essentials of Glycobiology. Cold Spring Harbor (NY)2015. p. 207–221.
Barash, U., Cohen-Kaplan, V., Dowek, I., Sanderson, R. D., Ilan, N., & Vlodavsky, I. (2010). Proteoglycans in health and disease: New concepts for heparanase function in tumor progression and metastasis. The FEBS Journal, 277, 3890–3903.
Elkin, M., Ilan, N., Ishai-Michaeli, R., Friedmann, Y., Papo, O., Pecker, I., et al. (2001). Heparanase as mediator of angiogenesis: Mode of action. The FASEB Journal, 15, 1661–1663.
Zhang, D., Wan, A., Chiu, A. P., Wang, Y., Wang, F., Neumaier, K., et al. (2013). Hyperglycemia-induced secretion of endothelial heparanase stimulates a vascular endothelial growth factor autocrine network in cardiomyocytes that promotes recruitment of lipoprotein lipase. Arteriosclerosis, Thrombosis, and Vascular Biology, 33, 2830–2838.
Sela, S., Natanson-Yaron, S., Zcharia, E., Vlodavsky, I., Yagel, S., & Keshet, E. (2011). Local retention versus systemic release of soluble VEGF receptor-1 are mediated by heparin-binding and regulated by heparanase. Circulation Research, 108, 1063–1070.
Zetser, A., Bashenko, Y., Edovitsky, E., Levy-Adam, F., Vlodavsky, I., & Ilan, N. (2006). Heparanase induces vascular endothelial growth factor expression: Correlation with p38 phosphorylation levels and Src activation. Cancer Research, 66, 1455–1463.
Hu, J., Wang, J., Leng, X., Hu, Y., Shen, H., & Song, X. (2017). Heparanase mediates vascular endothelial growth factor gene transcription in high-glucose human retinal microvascular endothelial cells. Molecular Vision, 23, 579–587.
Li, J., Meng, X., Hu, J., Zhang, Y., Dang, Y., Wei, L., et al. (2017). Heparanase promotes radiation resistance of cervical cancer by upregulating hypoxia inducible factor 1. American Journal of Cancer Research, 7, 234–244.
Cohen-Kaplan, V., Naroditsky, I., Zetser, A., Ilan, N., Vlodavsky, I., & Doweck, I. (2008). Heparanase induces VEGF C and facilitates tumor lymphangiogenesis. International Journal of Cancer, 123, 2566–2573.
Lv, B., Zhang, B., Hu, X. Y., & Zeng, Q. D. (2016). Heparanase regulates in vitro VEGF-C expression and its clinical significance to pancreatic ductal cell adenocarcinoma. Oncology Letters, 11, 1327–1334.
Blich, M., Golan, A., Arvatz, G., Sebbag, A., Shafat, I., Sabo, E., et al. (2013). Macrophage activation by heparanase is mediated by TLR-2 and TLR-4 and associates with plaque progression. Arteriosclerosis Thrombosis and Vascular Biology, 33, e56–e65.
Goodall, K. J., Poon, I. K., Phipps, S., & Hulett, M. D. (2014). Soluble heparan sulfate fragments generated by heparanase trigger the release of pro-inflammatory cytokines through TLR-4. PLoS One, 9, e109596.
Nadir, Y., Brenner, B., Zetser, A., Ilan, N., Shafat, I., Zcharia, E., et al. (2006). Heparanase induces tissue factor expression in vascular endothelial and cancer cells. Journal of Thrombosis and Haemostasis, 4, 2443–2451.
Ramani, V. C., Yang, Y., Ren, Y., Nan, L., & Sanderson, R. D. (2011). Heparanase plays a dual role in driving hepatocyte growth factor (HGF) signaling by enhancing HGF expression and activity. The Journal of Biological Chemistry, 286, 6490–6499.
Parish, C. R., Freeman, C., Ziolkowski, A. F., He, Y. Q., Sutcliffe, E. L., Zafar, A., et al. (2013). Unexpected new roles for heparanase in type 1 diabetes and immune gene regulation. Matrix Biology, 32, 228–233.
Purushothaman, A., Chen, L., Yang, Y., & Sanderson, R. D. (2008). Heparanase stimulation of protease expression implicates it as a master regulator of the aggressive tumor phenotype in myeloma. The Journal of Biological Chemistry, 283, 32628–32636.
Yang, Y., Ren, Y., Ramani, V. C., Nan, L., Suva, L. J., & Sanderson, R. D. (2010). Heparanase enhances local and systemic osteolysis in multiple myeloma by upregulating the expression and secretion of RANKL. Cancer Research, 70, 8329–8338.
Zetser, A., Levy-Adam, F., Kaplan, V., Gingis-Velitski, S., Bashenko, Y., Schubert, S., et al. (2004). Processing and activation of latent heparanase occurs in lysosomes. Journal of Cell Science, 117, 2249–2258.
Levy-Adam, F., Abboud-Jarrous, G., Guerrini, M., Beccati, D., Vlodavsky, I., & Ilan, N. (2005). Identification and characterization of heparin/heparan sulfate binding domains of the endoglycosidase heparanase. The Journal of Biological Chemistry, 280, 20457–20466.
Levy-Adam, F., Feld, S., Suss-Toby, E., Vlodavsky, I., & Ilan, N. (2008). Heparanase facilitates cell adhesion and spreading by clustering of cell surface heparan sulfate proteoglycans. PLoS One, 3, e2319.
Bass, M. D., Roach, K. A., Morgan, M. R., Mostafavi-Pour, Z., Schoen, T., Muramatsu, T., et al. (2007). Syndecan-4-dependent Rac1 regulation determines directional migration in response to the extracellular matrix. The Journal of Cell Biology, 177, 527–538.
Tkachenko, E., Elfenbein, A., Tirziu, D., & Simons, M. (2006). Syndecan-4 clustering induces cell migration in a PDZ-dependent manner. Circulation Research, 98, 1398–1404.
Tkachenko, E., Rhodes, J. M., & Simons, M. (2005). Syndecans: New kids on the signaling block. Circulation Research, 96, 488–500.
Woods, A., & Couchman, J. R. (2001). Syndecan-4 and focal adhesion function. Current Opinion in Cell Biology, 13, 578–583.
Gingis-Velitski, S., Zetser, A., Flugelman, M. Y., Vlodavsky, I., & Ilan, N. (2004). Heparanase induces endothelial cell migration via protein kinase B/Akt activation. The Journal of Biological Chemistry, 279, 23536–23541.
Doviner, V., Maly, B., Kaplan, V., Gingis-Velitski, S., Ilan, N., Vlodavsky, I., et al. (2006). Spatial and temporal heparanase expression in colon mucosa throughout the adenoma-carcinoma sequence. Modern Pathology, 19, 878–888.
Zetser, A., Bashenko, Y., Miao, H.-Q., Vlodavsky, I., & Ilan, N. (2003). Heparanase affects adhesive and tumorigenic potential of human glioma cells. Cancer Research, 63, 7733–7741.
Ben-Zaken, O., Gingis-Velitski, S., Vlodavsky, I., & Ilan, N. (2007). Heparanase induces Akt phosphorylation via a lipid raft receptor. Biochemical and Biophysical Research Communications, 361, 829–834.
Spyrou, A., Kundu, S., Haseeb, L., Yu, D., Olofsson, T., Dredge, K., et al. (2017). Inhibition of heparanase in pediatric brain tumor cells attenuates their proliferation, invasive capacity, and in vivo tumor growth. Molecular Cancer Therapeutics, 16, 1705–1716.
Cassinelli, G., Dal Bo, L., Favini, E., Cominetti, D., Pozzi, S., Tortoreto, M., et al. (2018). Supersulfated low-molecular weight heparin synergizes with IGF1R/IR inhibitor to suppress synovial sarcoma growth and metastases. Cancer Letters, 415, 187–197.
Cohen-Kaplan, V., Doweck, I., Naroditsky, I., Vlodavsky, I., & Ilan, N. (2008). Heparanase augments epidermal growth factor receptor phosphorylation: Correlation with head and neck tumor progression. Cancer Research, 68, 10077–10085.
Cohen-Kaplan, V., Jrbashyan, J., Yanir, Y., Naroditsky, I., Ben-Izhak, O., Ilan, N., et al. (2012). Heparanase induces signal transducer and activator of transcription (STAT) protein phosphorylation: Preclinical and clinical significance in head and neck cancer. The Journal of Biological Chemistry, 287, 6668–6678.
Goldberg, R., Sonnenblick, A., Hermano, E., Hamburger, T., Meirovitz, A., Peretz, T., et al. (2017). Heparanase augments insulin receptor signaling in breast carcinoma. Oncotarget, 8, 19403–19412.
Hob, S. G., Grundmann, M., Benkel, T., Gockel, L., Schwarz, S., Kostenis, E., et al. (2018). Pro-angiogenic effects of latent heparanase and thrombin receptor-mediated pathways-do they share a common ground in melanoma cells? Thrombosis and Haemostasis, 118, 1803–1814.
Haskell, M. D., Slack, J. K., Parsons, J. T., & Parsons, S. J. (2001). C-Src tyrosine phosphorylation of epidermal growth factor receptor, P190 RhoGAP, and focal adhesion kinase regulates diverse cellular processes. Chemical Reviews, 101, 2425–2440.
Nardella, C., Lahm, A., Pallaoro, M., Brunetti, M., Vannini, A., & Steinkuhler, C. (2004). Mechanism of activation of human heparanase investigated by protein engineering. Biochemistry, 43, 1862–1873.
Hulett, M. D., Hornby, J. R., Ohms, S. J., Zuegg, J., Freeman, C., Gready, J. E., et al. (2000). Identification of active-site residues of the pro-metastatic endoglycosidase heparanase. Biochemistry, 39, 15659–15667.
Lai, N. S., Simizu, S., Morisaki, D., Muroi, M., & Osada, H. (2008). Requirement of the conserved, hydrophobic C-terminus region for the activation of heparanase. Experimental Cell Research, 314, 2834–2845.
Simizu, S., Suzuki, T., Muroi, M., Lai, N. S., Takagi, S., Dohmae, N., et al. (2007). Involvement of disulfide bond formation in the activation of heparanase. Cancer Research, 67, 7841–7849.
Ben-Zaken, O., Shafat, I., Gingis-Velitski, S., Bangio, H., Kelson, I. K., Alergand, T., et al. (2008). Low and high affinity receptors mediate cellular uptake of heparanase. International Journal of Biochemistry & Cell Biology, 40, 530–542.
Wood, R. J., & Hulett, M. D. (2008). Cell surface-expressed cation-independent mannose 6-phosphate receptor (CD222) binds enzymatically active heparanase independently of mannose 6-phosphate to promote extracellular matrix degradation. The Journal of Biological Chemistry, 283, 4165–4176.
Gingis-Velitski, S., Zetser, A., Kaplan, V., Ben-Zaken, O., Cohen, E., Levy-Adam, F., et al. (2004). Heparanase uptake is mediated by cell membrane heparan sulfate proteoglycans. The Journal of Biological Chemistry, 279, 44084–44092.
Nadav, L., Eldor, A., Yacoby-Zeevi, O., Zamir, E., Pecker, I., Ilan, N., et al. (2002). Activation, processing and trafficking of extracellular heparanase by primary human fibroblasts. Journal of Cell Science, 115, 2179–2187.
Ramani, V. C., Vlodavsky, I., Ng, M., Zhang, Y., Barbieri, P., Noseda, A., et al. (2016). Chemotherapy induces expression and release of heparanase leading to changes associated with an aggressive tumor phenotype. Matrix Biology, 55, 22–34.
Wang, F., Jia, J., Lal, N., Zhang, D., Chiu, A. P., Wan, A., et al. (2016). High glucose facilitated endothelial heparanase transfer to the cardiomyocyte modifies its cell death signature. Cardiovascular Research, 112, 656–668.
Vreys, V., Delande, N., Zhang, Z., Coomans, C., Roebroek, A., Durr, J., et al. (2005). Cellular uptake of mammalian heparanase precursor involves low density lipoprotein receptor-related proteins, mannose 6-phosphate receptors, and heparan sulfate proteoglycans. The Journal of Biological Chemistry, 280, 33141–33148.
Goldshmidt, O., Nadav, L., Aingorn, H., Irit, C., Feinstein, N., Ilan, N., et al. (2002). Human heparanase is localized within lysosomes in a stable form. Experimental Cell Research, 281, 50–62.
Abboud-Jarrous, G., Atzmon, R., Peretz, T., Palermo, C., Gadea, B. B., Joyce, J. A., et al. (2008). Cathepsin L is responsible for processing and activation of proheparanase through multiple cleavages of a linker segment. The Journal of Biological Chemistry, 283, 18167–18176.
Abboud-Jarrous, G., Rangini-Guetta, Z., Aingorn, H., Atzmon, R., Elgavish, S., Peretz, T., et al. (2005). Site-directed mutagenesis, proteolytic cleavage, and activation of human proheparanase. The Journal of Biological Chemistry, 280, 13568–13575.
Cohen, E., Atzmon, R., Vlodavsky, I., & Ilan, N. (2005). Heparanase processing by lysosomal/endosomal protein preparation. FEBS Letters, 579, 2334–2338.
Levy-Adam, F., Feld, S., Cohen-Kaplan, V., Shteingauz, A., Gross, M., Arvatz, G., et al. (2010). Heparanase 2 interacts with heparan sulfate with high affinity and inhibits heparanase activity. The Journal of Biological Chemistry, 285, 28010–28019.
Fuki, I. V., Kuhn, K. M., Lomazov, I. R., Rothman, V. L., Tuszynski, G. P., Iozzo, R. V., et al. (1997). The syndecan family of proteoglycans. Novel receptors mediating internalization of atherogenic lipoproteins in vitro. The Journal of Clinical Investigation, 100, 1611–1622.
Stanford, K. I., Bishop, J. R., Foley, E. M., Gonzales, J. C., Niesman, I. R., Witztum, J. L., et al. (2009). Syndecan-1 is the primary heparan sulfate proteoglycan mediating hepatic clearance of triglyceride-rich lipoproteins in mice. The Journal of Clinical Investigation, 119, 3236–3245.
Fears, C. Y., & Woods, A. (2006). The role of syndecans in disease and wound healing. Matrix Biology, 25, 443–456.
Beauvais, D. M., & Rapraeger, A. C. (2004). Syndecans in tumor cell adhesion and signaling. Reproductive Biology and Endocrinology, 2, 3.
Shteingauz, A., Ilan, N., & Vlodavsky, I. (2014). Processing of heparanase is mediated by syndecan-1 cytoplasmic domain and involves syntenin and alpha-actinin. Cellular and Molecular Life Sciences, 71, 4457–4470.
Baietti, M. F., Zhang, Z., Mortier, E., Melchior, A., Degeest, G., Geeraerts, A., et al. (2012). Syndecan-syntenin-ALIX regulates the biogenesis of exosomes. Nature Cell Biology, 14, 677–685.
Roucourt, B., Meeussen, S., Bao, J., Zimmermann, P., & David, G. (2015). Heparanase activates the syndecan-syntenin-ALIX exosome pathway. Cell Research, 25, 412–428.
Thompson, C. A., Purushothaman, A., Ramani, V. C., Vlodavsky, I., & Sanderson, R. D. (2013). Heparanase regulates secretion, composition, and function of tumor cell-derived exosomes. The Journal of Biological Chemistry, 288, 10093–10099.
Chen, G., Wang, D., Vikramadithyan, R., Yagyu, H., Saxena, U., Pillarisetti, S., et al. (2004). Inflammatory cytokines and fatty acids regulate endothelial cell heparanase expression. Biochemistry, 43, 4971–4977.
Lerner, I., Hermano, E., Zcharia, E., Rodkin, D., Bulvik, R., Doviner, V., et al. (2011). Heparanase powers a chronic inflammatory circuit that promotes colitis-associated tumorigenesis in mice. The Journal of Clinical Investigation, 121, 1709–1721.
Shafat, I., Vlodavsky, I., & Ilan, N. (2006). Characterization of mechanisms involved in secretion of active heparanase. The Journal of Biological Chemistry, 281, 23804–23811.
Carroll, B., & Dunlop, E. A. (2017). The lysosome: A crucial hub for AMPK and mTORC1 signalling. The Biochemical Journal, 474, 1453–1466.
Davidson, S. M., & Vander Heiden, M. G. (2017). Critical functions of the lysosome in Cancer biology. Annual Review of Pharmacology and Toxicology, 57, 481–507.
Hamalisto, S., & Jaattela, M. (2016). Lysosomes in cancer-living on the edge (of the cell). Current Opinion in Cell Biology, 39, 69–76.
Lamming, D. W., & Bar-Peled, L. (2019). Lysosome: The metabolic signaling hub. Traffic, 20, 27–38.
Egeberg, M., Kjeken, R., Kolset, S. O., Berg, T., & Prydz, K. (2001). Internalization and stepwise degradation of heparan sulfate proteoglycans in rat hepatocytes. Biochimica et Biophysica Acta, 1541, 135–149.
Rosenfeldt, M. T., & Ryan, K. M. (2011). The multiple roles of autophagy in cancer. Carcinogenesis, 32, 955–963.
White, E. (2012). Deconvoluting the context-dependent role for autophagy in cancer. Nature Reviews. Cancer, 12, 401–410.
Ilan, N., Shteingauz, A., & Vlodavsky, I. (2015). Function from within: Autophagy induction by HPSE/heparanase-new possibilities for intervention. Autophagy, 11, 2387–2389.
Dunlop, E. A., & Tee, A. R. (2014). mTOR and autophagy: A dynamic relationship governed by nutrients and energy. Seminars in Cell & Developmental Biology.
Korolchuk, V. I., Saiki, S., Lichtenberg, M., Siddiqi, F. H., Roberts, E. A., Imarisio, S., et al. (2011). Lysosomal positioning coordinates cellular nutrient responses. Nature Cell Biology, 13, 453–460.
Das, C. K., Mandal, M., & Kogel, D. (2018). Pro-survival autophagy and cancer cell resistance to therapy. Cancer and Metastasis Reviews.
Larrue, C., Saland, E., Boutzen, H., Vergez, F., David, M., Joffre, C., et al. (2016). Proteasome inhibitors induce FLT3-ITD degradation through autophagy in AML cells. Blood, 127, 882–892.
Levy, J. M., & Thorburn, A. (2011). Targeting autophagy during cancer therapy to improve clinical outcomes. Pharmacology & Therapeutics, 131, 130–141.
Wu, W. K., Coffelt, S. B., Cho, C. H., Wang, X. J., Lee, C. W., Chan, F. K., et al. (2012). The autophagic paradox in cancer therapy. Oncogene, 31, 939–953.
Chude, C. I., & Amaravadi, R. K. (2017). Targeting autophagy in Cancer: Update on clinical trials and novel inhibitors. International Journal of Molecular Sciences, 18.
Bar-Ner, M., Eldor, A., Wasserman, L., Matzner, Y., Cohen, I. R., Fuks, Z., et al. (1987). Inhibition of heparanase-mediated degradation of extracellular matrix heparan sulfate by non-anticoagulant heparin species. Blood, 70, 551–557.
Nakajima, M., Irimura, T., Di Ferrante, N., & Nicolson, G. L. (1984). Metastatic melanoma cell heparanase. Characterization of heparan sulfate degradation fragments produced by B16 melanoma endoglucuronidase. The Journal of Biological Chemistry, 259, 2283–2290.
Casu, B., Vlodavsky, I., & Sanderson, R. D. (2008). Non-anticoagulant heparins and inhibition of cancer. Pathophysiology of Haemostasis and Thrombosis, 36, 195–203.
Dredge, K., Hammond, E., Davis, K., Li, C. P., Liu, L., Johnstone, K., et al. (2010). The PG500 series: Novel heparan sulfate mimetics as potent angiogenesis and heparanase inhibitors for cancer therapy. Investigational New Drugs, 28, 276–283.
Miao, H. Q., Liu, H., Navarro, E., Kussie, P., & Zhu, Z. (2006). Development of heparanase inhibitors for anti-cancer therapy. Current Medicinal Chemistry, 13, 2101–2111.
Jia, L., & Ma, S. (2016). Recent advances in the discovery of heparanase inhibitors as anti-cancer agents. European Journal of Medicinal Chemistry, 121, 209–220.
McKenzie, E., Tyson, K., Stamps, A., Smith, P., Turner, P., Barry, R., et al. (2000). Cloning and expression profiling of Hpa2, a novel mammalian heparanase family member. Biochemical and Biophysical Research Communications, 276, 1170–1177.
Nadir, Y., Brenner, B., Gingis-Velitski, S., Levy-Adam, F., Ilan, N., Zcharia, E., et al. (2008). Heparanase induces tissue factor pathway inhibitor expression and extracellular accumulation in endothelial and tumor cells. Thrombosis and Haemostasis, 99, 133–141.
Gross-Cohen, M., Feld, S., Doweck, I., Neufeld, G., Hasson, P., Arvatz, G., et al. (2016). Heparanase 2 attenuates head and neck tumor vascularity and growth. Cancer Research, 76, 2791–2801.
Fong, S., Debs, R. J., & Desprez, P. Y. (2004). Id genes and proteins as promising targets in cancer therapy. Trends in Molecular Medicine, 10, 387–392.
Gross-Cohen, M., Feld, S., Naroditsky, I., Nativ, O., Ilan, N., & Vlodavsky, I. (2016). Heparanase 2 expression inversely correlates with bladder carcinoma grade and stage. Oncotarget, 7, 22556–22565.
Masola, V., Zaza, G., Granata, S., Gambaro, G., Onisto, M., & Lupo, A. (2013). Everolimus-induced epithelial to mesenchymal transition in immortalized human renal proximal tubular epithelial cells: Key role of heparanase. Journal of Translational Medicine, 11, 292.
Bernard, D., Mehul, B., Delattre, C., Simonetti, L., Thomas-Collignon, A., & Schmidt, R. (2001). Purification and characterization of the endoglycosidase heparanase 1 from human plantar stratum corneum: A key enzyme in epidermal physiology? The Journal of Investigative Dermatology, 117, 1266–1273.
Saxton, R. A., & Sabatini, D. M. (2017). mTOR Signaling in growth, metabolism, and disease. Cell, 168, 960–976.
Boyango, I., Barash, U., Fux, L., Naroditsky, I., Ilan, N., & Vlodavsky, I. (2018). Targeting heparanase to the mammary epithelium enhances mammary gland development and promotes tumor growth and metastasis. Matrix Biology, 65, 91–103.
Hong, X., Jiang, F., Kalkanis, S. N., Zhang, Z. G., Zhang, X., Zheng, X., et al. (2008). Increased chemotactic migration and growth in heparanase-overexpressing human U251n glioma cells. Journal of Experimental & Clinical Cancer Research, 27, 23.
Riaz, A., Ilan, N., Vlodavsky, I., Li, J. P., & Johansson, S. (2013). Characterization of heparanase-induced phosphatidylinositol 3-kinase-AKT activation and its integrin dependence. The Journal of Biological Chemistry, 288, 12366–12375.
Rubinfeld, H., Cohen-Kaplan, V., Nass, D., Ilan, N., Meisel, S., Cohen, Z. R., et al. (2011). Heparanase is highly expressed and regulates proliferation in GH-secreting pituitary tumor cells. Endocrinology, 152, 4562–4570.
Weissmann, M., Bhattacharya, U., Feld, S., Hammond, E., Ilan, N., & Vlodavsky, I. (2019). The heparanase inhibitor PG545 is a potent anti-lymphoma drug: Mode of action. Matrix Biology, 77, 58–72.
Conflict of Interest
The authors have no potential conflict of interest to declare.
Funding
These studies were generously supported by research grants awarded by the Israel Science Foundation (grant 601/14, 2572/16); the United States-Israel Binational Science Foundation (BSF); the Israel Cancer Research Fund (ICRF); and the National Institutes of Health (CA211752). I. Vlodavsky is a Research Professor of the ICRF.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Ilan, N. et al. (2020). Heparanase-The Message Comes in Different Flavors. In: Vlodavsky, I., Sanderson, R., Ilan, N. (eds) Heparanase. Advances in Experimental Medicine and Biology, vol 1221. Springer, Cham. https://doi.org/10.1007/978-3-030-34521-1_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-34521-1_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-34520-4
Online ISBN: 978-3-030-34521-1
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)