
Abstract
In the emergency setting, accurate clinical assessment in combination with appropriate imaging is key to the identification of patients with or at risk of neurological deficit. This chapter aims to familiarise students with the role of imaging for patients with spinal trauma . The primary concern with any spinal injury is not the vertebral column but the closely related neurological elements: the spinal cord, nerve roots and cauda equina. It is important that students understand the basic concepts of imaging in the context of the clinical examination . After completion of this tutorial students should be able to describe the key imaging features of typical patterns of spinal injury.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
Aims and Guidance for Tutors
In the emergency setting, accurate clinical assessment in combination with appropriate imaging is key to the identification of patients with or at risk of neurological deficit. This chapter aims to familiarise students with the role of imaging for patients with spinal trauma . The primary concern with any spinal injury is not the vertebral column but the closely related neurological elements: the spinal cord, nerve roots and cauda equina. It is important that students understand the basic concepts of imaging in the context of the clinical examination . After completion of this tutorial students should be able to describe the key imaging features of typical patterns of spinal injury.
Introduction
-
Road traffic accidents (40%) and falls (35%) are the leading causes of spinal injury.
-
The greater the mechanism force (e.g. higher velocity) typically the greater the associated injury
-
Cervical spine is most commonly affected followed by thoracic spine and lumbar spine
-
In any suspected spinal injury immobilisation is key so as not to worsen any existing or potential neurological deficit
-
The mechanisms of injury include flexion, extension, flexion with rotation, and compression.
-
The AOSpine classification system is an internationally accepted imaging classification system based on recognised spinal injury patterns.
-
Common types of spinal fractures are:
-
Compression
-
Burst
-
Seat-belt associated e.g. Chance fracture
-
Fracture -dislocation
-
Radiological Modalities Utilised
Radiography
-
Mainstay of spinal imaging. AP and lateral radiographs of the region of the spinal area affected.
-
Initial investigation of choice in most cases. Radiography is widely available and can be performed rapidly and without moving the patient from their trolley if needed.
-
When imaging the cervical spine it is essential to include dedicated imaging of the odontoid peg in the cervical spine and the cervicothoracic junction (C7–T1).
-
Radiography allows assessment of:
-
Vertebral alignment.
-
Vertebral body height and cortical margins for fractures .
-
-
It is important to be cognizant of the limitations of radiography for the imaging of spinal trauma : Radiography will in many cases fail to establish the full extent of spinal injury. In addition, radiography has a lower sensitivity for fracture detection when compared to CT .
-
In many trauma units, CT cervical spine has replaced radiography as the initial imaging investigation for high risk patients presenting after high velocity cervical spine injury.
-
CT spine or as part of body CT scan
-
Often performed as part of a work-up for other associated injuries (intra-abdominal/intra-thoracic).
-
Can be performed to further assess an abnormality identified on plain radiographs or as initial investigation if there is high clinical suspicion.
-
CT allows detailed anatomic identification of fractures and whether fractures are stable/unstable and whether there is cord compression
-
Helpful for pre-operative planning if surgical fixation is being considered.
MRI spine
-
In comparison with CT , there are several practical reasons that MRI is less suited for use in the emergency setting:
-
Longer imaging time required.
-
Sensitivity to patient motion.
-
Possible incompatibilities with indwelling medical devices or foreign bodies.
-
-
For these reasons, MRI is usually performed after CT .
-
MRI is far superior to CT for the identification of neurological injuries of the spinal cord such as contusions, oedema and haematoma. MRI can also identify soft tissue abnormalities such as ligamentous injury and intervertebral disc disruption.
Radiologist’s tips : limitations of radiographs
-
For the majority of patients with relatively low mechanisms of injury plain radiography should be sufficient
-
However in the presence of a high velocity injuries, have a low threshold for further imaging
-
CT can better delineate the bony structures of the vertebral column
-
MRI can better delineate the spinal cord and soft tissues around the vertebral column
-
Often a patient will require CT and MRI imaging when there is a fracture with neurological deficit to determine extent of injuries and plan fixation.
Indications for Imaging
-
The need for imaging is dictated by clinical assessment.
-
Patients who have sustained trauma with associated tenderness should have plain films of that portion of the spine.
-
If a high velocity mechanism e.g. motor vehicle accident then CT imaging should be performed, usually as part of a trauma body CT scan to look for associated injuries.
-
When a neurological deficit is present then an MRI should be performed as part of the imaging work-up.
Review of Relevant Radiological Anatomy: Spinal Radiography

Technically satisfactory AP (a), lateral (b) and open-mouth (c) views of the cervical spine. There are 7 cervical vertebrae: C1–C7. The AP and lateral radiographs demonstrate vertebral bodies, disc spaces, facet joints and spinous processes. Note on the lateral projection the normal shadow of the prevertebral soft tissues (arrow)—these can become swollen after cervical spine trauma. Recognition of prevertebral soft tissue thickening can help the Radiologist identify cases of significant cervical spine injury. Also appreciable on the lateral projection is the normal curvature of the cervical spine (cervical lordosis). c The open-mouth view demonstrates the odontoid process of C2 (also called the axis) and lateral masses of C1 (also called the atlas). The solid line between the odontoid process and lateral masses on either side should be equidistant and the dotted lines along the lateral margins of C1 and C2 should be smooth and continuous. Abnormalities of either of these lines suggests high cervical spine injury

Lateral radiograph of the cervical spine on which longitudinal lines are depicted. Anterior vertebral line—along the anterior margins of the vertebral bodies. Posterior vertebral line—along the posterior margins of the vertebral bodies, this delineates the anterior margin of the spinal canal. Spinolaminar line—along the junctions of the laminae and spinous processes of the vertebrae, this delineates the posterior margin of the spinal canal. Posterior spinous line—along the posterior margins of the spinous processes. Disruption of any of these lines suggests spinal injury and close examination for associated fractures should be performed

AP (a) and lateral (b) radiographs of the thoracic spine. There are 12 thoracic vertebrae (T1–T12), which articulate with 12 pairs of ribs

AP (a) and lateral (b) radiographs of the lumbar spine. There are 5 lumbar vertebrae (L1–L5). Partially imaged upper sacrum is included
Radiologist’s tips: Spinal injury on plain films
-
Assess the integrity of the spinal lines.
-
This will identify and displacement or associated soft tissue abnormality
-
-
Trace the outline of each vertebra to identify:
-
Compression fractures: wedging of the vertebral body anteriorly
-
Burst fractures: discontinuity of the cortex of the vertebra anteriorly or posteriorly
-
-
Check for uniformity of the disc spaces, this will help identify flexion/extension injuries
Fracture Types
Compression
-
Typically result in wedge fractures due to hyperflexion injuries from axial loading.
-
Most commonly affecting the anterior aspect of the vertebral body in the lumbar and thoracic spine (Fig. 4).
-
Risk factors include osteoporosis and can occur after minimal trauma (Fig. 5).
Fig. 5 
Lateral radiograph of the thoracic spine of an elderly patient that demonstrates anterior wedging of T9 with approximately 50% loss of height anteriorly. There is a resultant exaggerated thoracic kyphosis

Burst
-
These are a type of compression fracture related to high-energy axial loading spinal trauma (for example—a fall from a height in a standing position).
-
The posterior vertebral body cortex is disrupted with retropulsion into the spinal canal. If the spinal cord is compressed this can result in neurological deficits below the level (Fig. 6).
Fig. 6 
a Lateral radiograph of the lumbar spine demonstrates some compression of L3 (arrow). There is also disruption of the posterior spinal line with retropulsion of a bone fragment into the spinal canal. b Sagittal CT through the lumbar spine demonstrates the burst-type fracture which extents through the anterior, superior and posterior cortices. A fragment arising posterosuperiorly is retropulsed into the spinal canal (dashed arrow), this likely causes some compression of the cauda equina nerve roots, which are not visible on CT . The posterior elements are intact

Seat belt associated e.g. chance fracture
-
Flexion-distraction type injuries of the spine that extend to involve the anterior and posterior elements, which may be ligamentous.
-
These are unstable injuries and have a high association with intra-abdominal injuries especially in the retroperitoneum of the pancreas and duodenum (Fig. 7).
Fig. 7 
a Sagittal CT of the thoracolumbar junction demonstrates a fracture through the L1 vertebral body, with extension of the fracture line posteriorly through the posterior elements of L1 (arrow). b Sagittal T2 weighted MRI demonstrates high signal with L1 vertebra (curved arrow), this is marrow oedema due to the fracture . Posteriorly injury of the spinous process of T12 and in the interspinous ligaments is evident by the increased signal (dashed arrow)

Flexion teardrop
-
These result from severe axial loading with associated flexion. Most commonly occurring in the mid/lower cervical spine.
-
Important to recognise as they indicate extensive underlying ligamentous injury and spinal instability. Associated spinal cord injury is common, especially anterior cervical cord syndrome and quadriplegia.
-
The key finding is fracture of the anteroinferior lip of vertebral body and posterior displacement of the vertebral body often with widening of interspinous distance at that level, indicating ligamentous injury (Fig. 8).
Fig. 8 
Cervical spine imaging for a patient involved in a road traffic accident. a Lateral radiograph of the cervical spine with the patient immobilised in spinal blocks (partially visualised rectangular outline). A displaced fracture fragment is seen arising anteroinferiorly from C5 (arrow). In this case all of the longitudinal spinal lines have been disrupted—the C5 vertebral body has slipped posteriorly relative to the C6 vertebral body (this is called “retrolisthesis”). b Sagittal CT better depicts the fracture . Note also the presence of an endotracheal tube due to impaired respiratory function (arrow). c Sagittal T2 MRI again demonstrated the fracture also with disruption of the anterior longitudinal ligament and elevation of the posterior longitudinal ligament. The retrolisthesis of C5 has resulted in severe spinal canal stenosis and compression of the cervical cord. There is diffuse high signal within the cord from C4 to C6 consistent with oedema (arrow)

Extension teardrop
-
This injury occurs due to forced extension of the neck with resulting avulsion of the anteroinferior corner of the vertebral body, this disrupts the anterior longitudinal ligament.
-
There is no vertebral body displacement. Generally not considered as severe as a flexion teardrop fracture (Fig. 9).
Fig. 9 
a Sagittal CT demonstrating a small fracture fragment at the anterinferior margin of C6 (arrow) with some widening of the disc space at this level. b Sagittal T2 weighted MRI again demonstrates the fracture fragment, with increased signal within the C6–C7 disc and disruption of the anterior longitudinal ligament (arrow)

C-Spine Specific Fractures
There are several important fractures unique to the cervical spine. If neurological compromise results then symptoms affect both the upper and lower limbs .
Jefferson fracture
-
This is a burst fracture of C1 (atlas), typically as a result of a significant axial load to the head that transmits through the occipital condyles resulting in fracture of the ring of C1 (Fig. 10).
Fig. 10 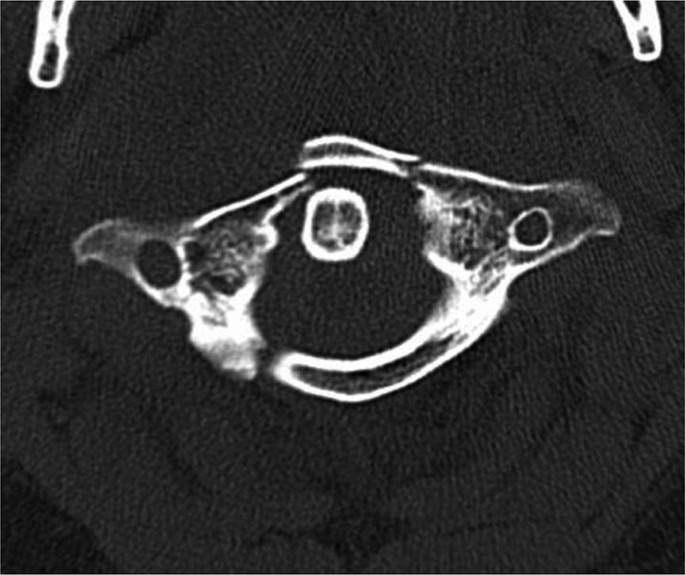
Axial CT through C1 demonstrates two fracture lines within the anterior arch of C1 and a third fracture line through the posterior arch on the right

Hangman fracture
-
This results from hyperextension and distraction of the C2 vertebra (axis) with resultant bilateral fractures through the pars interarticularis of C2.
Odontoid process (peg) fracture
-
Fracture involving the vertical protuberance of C2 often as a result of sudden neck flexion or extension. Elderly patients with osteoporosis are particularly at risk for sustaining this fracture . These fractures are at risk of nonunion and may require stabilisation with surgical fixation (Fig. 11).
Fig. 11 
a Lateral cervical spine radiograph demonstrating a minimally displaced fracture through the odontoid process (arrow) which is confirmed on CT (b)

Clay-shoveler fracture
-
Fracture through the spinous processes of a lower cervical vertebra, usually C7 often with displacement.
-
This fracture was originally described in workers shovelling clay—when throwing the clay of the shovel, on occasion the clay would stick to the shovel resulting in a flexion injury to the neck and a “clay-shoveler fracture “ (Fig. 12).
Fig. 12 
Lateral radiograph of the cervical spine that demonstrates a mildly displaced fracture of the spinous process of C7 (arrow). Note the loss of normal cervical spine curvature—this can be an indirect sign of cervical spine trauma

Traumatic Listhesis
-
Can occur either with or without associated fracture .
-
In the absence of fractures then facet joint dislocation must occur:
-
Subluxed: partial uncovering of facet joint.
-
Perched: complete uncovering of facet joint.
-
Locked: occurs when the inferior articular process jumps over the superior articular process of the vertebra below and becomes locked in the position.
-
Cord compression
-
Neurological dysfunction: The neurological level is at the most lowest segment with normal motor and sensory function
-
Complete:
-
Flaccid paralysis with total loss of sensory and motor functions below that level. Autonomic dysfunction can also be present: perianal and “saddle” paraesthesia, bowel and/or bladder dysfunction
-
-
Incomplete (mixed loss):
-
Anterior cord syndrome: Due to compression fracture of vertebral body or anterior dislocation. Anterior spinal artery compression. Loss of power, reduced pain and temperature below the lesion.
-
Posterior cord syndrome: Hyperextension injuries, Posterior vertebral body fracture , Loss of proprioception and vibration sense, Severe ataxia.
-
Central cord syndrome: Older age with degenerative cervical disc disease results from hyperextension with minor trauma. The cord is compressed by osteophytes from vertebral body against thick ligamentum flavum. Damages the central cervical tract. UMN lesion to legs (spastic). LMN to arms (flaccid paralysis).
-
Brown sequard’s syndrome: Hemisection of the cord, usually as a result of stab injury and lateral mass fractures . The uninjured side has good power but absent pinprick and temperature. This is because the spinothalamic tracts cross to opposite side of the cord three segments below.
-
Suggested Reading
-
Parizel PM, van der Zijden T, Gaudino S et-al. Trauma of the spine and spinal cord: imaging strategies. Eur Spine J. 2010;19 Suppl 1(S1):S8–17.
-
Munera F, Rivas LA, Nunez DB et al. Imaging evaluation of adult spinal injuries: emphasis on multidetector CT in cervical spine trauma. Radiology. 2012;263(3):645–60. https://doi.org/10.1148/radiol.12110526.
-
Kim KS, Chen HH, Russell EJ et-al. Flexion teardrop fracture of the cervical spine: radiographic characteristics. Am J Roentgenol. 1989;152(2):319–26. https://doi.org/10.2214/ajr.152.2.319.
-
Looby S, Flanders A. Spine trauma. Radiol Clin North Am. 2011;49:129–63.
-
Gamanagatti S, Rathinam D, Rangarajan K, Kumar A, Farooque K, Sharma V. Imaging evaluation of traumatic thoracolumbar spine injuries: radiological review. World J Radiol. 2015;7(9):253–65.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
O’Neill, D., Given, M. (2020). Tutorial 3: Spinal Trauma. In: Redmond, C., Lee, M. (eds) Tutorials in Diagnostic Radiology for Medical Students. Springer, Cham. https://doi.org/10.1007/978-3-030-31893-2_3
Download citation
DOI: https://doi.org/10.1007/978-3-030-31893-2_3
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31892-5
Online ISBN: 978-3-030-31893-2
eBook Packages: MedicineMedicine (R0)