
Abstract
The abdominal radiograph is rapidly acquired low-cost exam, which provides information on a large number of structures. In current practice, the abdominal radiograph is often performed as a screening test, with positive findings prompting progression to a CT scan. Alternatively repeat abdominal radiographs are often used to follow up conditions such bowel dilatation or urinary stone disease, avoiding the need for repeated CT scans. Radiograph allows distinction between five radiographic densities; gas, fat, fluid/soft tissue, bone/calcium and metal. Further differentiation between tissue subtypes is typically not possible. An overview of the normal radiographic appearance of bowel is presented, along with common and important pathologies. The radiographic appearances of the major intra-abdominal organs is described. This chapter aims to present the reader with a structured approach to interpreting an abdominal radiograph.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Aims and Guidance for Tutors
The abdominal radiograph is an examination performed for a variety of indications. It encompasses many organs and spaces and a structured approach to interpreting the abdominal radiograph is essential to detect pathology. It is important that students comprehend the contemporary role of the abdominal radiograph. Its use has largely been replaced by CT for the radiological assessment of the acute abdomen. However in several settings the abdominal radiograph can provide important diagnostic information. Even where specific radiographic findings are present such as free intra-abdominal air or bowel obstruction which previously represented absolute indications for laparotomy in current practice a subsequent CT is often performed to assess the exact location and severity of pathology guiding treatment decisions. This chapter aims to present the student with a structured approach to interpreting an abdominal radiograph
Introduction
-
The abdominal radiograph provides information on five radiographic densities; from least dense (darkest) to most dense (brightest) these are gas, fat, fluid/soft tissue, bone/calcium and metal. Further differentiation between tissue subtypes is typically not possible due to inherent limitations in radiograph contrast resolution (Fig. 1).
Fig. 1 
A satisfactory abdominal radiograph. The radiograph includes the diaphragm superiorly, lateral abdominal walls laterally, and the inferior pubic rami inferiorly. In addition, patient orientation (supine) is demarcated by the downward arrow, and the side of the radiograph is marked (R indicating right)
-
Gas is typically confined to the gastrointestinal tract. With instrumentation, gas can be seen in other organs. Air outside of the GI tract or instrumented organ is typically pathological.
-
Fat is a normal constituent of the abdominal wall (forming the properitoneal fat plane), encases the retroperitoneal organs, and also occurs within the peritoneal cavity in the form of mesentery and omentum.
-
Fluid and soft tissue (such as organ tissue and muscle) are typically of similar density (reflecting the high percentage of water in the cellular contents of organs). The difference between fluid and various solid abdominal organs is typically too small to be reliably perceived on radiography.
-
Bone, vascular calcification and mineral calculi are formed from the deposition of minerals such as calcium, phosphate and magnesium. The much higher density of these minerals, as compared with the other tissue types on abdominal radiographs, makes them readily assessable on radiography.
-
Metallic foreign bodies may be visualised in the form of surgical clips, staples, or devices, and can provide clues as to the surgical history.

Abdominal Radiography Technical Principles and Anatomy
-
Abdominal radiographs can be performed in a variety of ways. Patient positioning can alter the appearance on a radiograph, particularly the way gas and fluid behave. Position should thus be specified on the radiograph for the reporting radiologist. For example, a supine radiograph is less sensitive than an erect radiograph in assessing for free air, but both can look identical unless the image is labelled appropriately.
-
The x-ray tube generates an x-ray beam with exposure factors optimised to maximise differentiation between soft tissues (generally the structures of interest), whilst ensuring adequate beam penetration.
-
The dose from an abdominal radiograph is approximately 1.3 mSV, which is much greater than that of a chest radiograph, and approximately one quarter of the dose of a full abdominopelvic CT (Fig. 2).
Fig. 2 
Graphic representation of standard acquisition of abdominal radiograph. The x-ray tube (positioned over the patient) directs x rays toward the detector plate (positioned under the patient)
-
The following structures should be included on an abdominal radiograph:
-
The diaphragm superiorly
-
The lateral abdominal walls laterally
-
The inferior pubic rami inferiorly
-

Anatomy
Although not exhaustive, an outline of the following structures may be visible on abdominal radiography. Larger organs may be visible under normal conditions (indicated below with *), whereas smaller organs may only be apparent under pathological conditions such as enlargement or calcification. A knowledge of expected location and normal appearance will aid in detecting pathology (Figs. 3 and 4).

Relative radiographic position of the liver (L), gallbladder (GB) and urinary bladder (UB) are outlined, with coronal contrast-enhanced CT for reference

More posteriorly within the abdomen, the relative radiographic position of the liver (L), spleen (S), left kidney (LK) and right kidney (RK) are outlined, with coronal contrast-enhanced CT for reference
-
Solid organs:
-
Liver*
-
Spleen*
-
Kidneys*
-
Pancreas
-
Adrenal glands
-
Uterus and ovaries
-
Prostate
-
-
Hollow organs:
-
Gastrointestinal tract*
-
Renal collecting system, ureters and urinary bladder
-
Gall bladder, biliary tree
-
-
Other:
-
Cavities (peritoneal, retroperitoneal)
-
Subcutaneous tissues (such as the properitoneal fat plane)
-
Lung bases
-
Bones
-
Hardware
-
Indications
-
While CT has replaced abdominal radiography for most indications, there are some persisting indications for abdominal radiography.
-
Abdominal radiographs are a rapid and easily performed test for suspected acute pathologies such as perforation, obstruction, or urinary stone disease.
-
Abdominal radiographs can be used to follow established diagnoses such as obstruction or toxic megacolon. The radiograph assesses for improvement or worsening over serial studies, without requiring a full repeat CT each time.
-
Abdominal radiographs allow for the assessment of medical hardware (such as tubes, stents, electrical stimulation devices), to ensure no dislodgement or breakage.
-
Contraindications
-
There are no absolute contraindications to abdominal radiography. Due to reasonably high radiation dose, judicious use in young patients is advised. In possible or confirmed pregnancy, alternative modalities which do not involve radiation such as ultrasound or MRI should be considered.
Obstruction
Small Bowel Obstruction
-
Small bowel obstruction occurs when there is an impedance to transit along the length of the small bowel (Fig. 5). This is the most common level of gastrointestinal obstruction. Common causes are adhesions, herniae, malignancy and strictures from inflammatory bowel disease or radiation. Objects causing obstruction (such as gallstones or ingested foreign bodies) frequently become impacted within the terminal ilium, the narrowest point of the enteric tract.
Fig. 5 
Dilated loops of small bowel are identified within the central abdomen. On this erect radiograph, air-fluid levels are present within the dilated small bowel loops

Clinical features:
-
Vomiting (as the gastrointestinal tract continuously secretes many litres of digestive fluids each day, which can only decompress proximally when obstructed distally).
-
Abdominal distention.
-
Abdominal pain.
-
Increased bowel sounds.
-
Reduction in passage of stool or flatus per rectum.
Key imaging appearances:
-
Dilated loops of small bowel (measuring >3 cm in diameter) throughout the abdomen. Small bowel loops are characterised by regular, fine folds (called valvulae coniventes) which fully encircle the bowel and differentiate them from large bowel. Small bowel loops are also smaller and tend to be located centrally within the abdomen, forming a ladder-like configuration when obstructed.
-
Dilated small bowel loops are generally only seen when (at least some of) the bowel loops contain air, which provide contrast with the background fluid/soft-tissue density of the abdomen. Fluid-filled loops of small bowel are generally occult on radiographs, although well seen on CT.
-
Dilated stomach can be present, however both vomiting or the placement of a gastric decompression tube can result in an empty stomach.
-
Differential air-fluid levels, in which there are different heights of air-fluid interfaces in the same loop of bowel, may also aid in determining the presence of a mechanical obstruction.
-
The cause of the obstruction may be visible on the radiograph, such as an inguinal hernia, a radiopaque gallstone or foreign body.
-
Complications of obstruction (such as perforation, pneumatosis, etc.) may also be visible and should be closely searched for once small bowel obstruction has been diagnosed.
Large Bowel Obstruction
-
Large bowel obstruction occurs when there is a blockage located anywhere between the caecum and the anus (Fig. 6). This is less common than small bowel obstruction. Causes include malignancy (classically from a stricturing colorectal cancer), volvulus and inflammatory strictures (such as from inflammatory bowel disease or chronic sigmoid diverticular disease).
Fig. 6 
The large bowel is dilated down to the level of the sigmoid colon, where there is a non-dilated segment is seen (arrowheads), distal to which the remaining sigmoid colon and rectum are decompressed. Mildly dilated loops of small bowel within the central abdomen are also noted. Subsequent CT confirmed an obstructing sigmoid tumour

Clinical features:
-
Constipation or obstipation.
-
Abdominal distention.
-
Abdominal pain.
-
Large bowel obstruction can cause upstream dilatation of the small bowel (particularly in patients with an incompetent ileocaecal valve which permits the obstructed large bowel to decompress proximally). Thus, symptoms of large and small bowel obstruction often overlap.
Key imaging appearances:
-
Large bowel is characterised by a wider diameter than small bowel, with folds (called haustra) which do not fully encircle the bowel. In addition, large bowel tends to be located at the peripheral margins of the abdominal cavity.
-
Dilatation of the cecum beyond 9 cm, or the remaining large bowel beyond 6 cm is worrisome for obstruction.
-
As dilatation occurs upstream from the level of the obstruction, the location of the dilated large bowel may hint at the level of obstruction.
-
As with small bowel obstruction, the cause of large bowel obstruction and its complications may be visible on the abdominal radiograph, and should be carefully searched for.
-
When large bowel dilatation occurs in the absence of a clear cause, it is known as pseudo-obstruction (Ogilvie syndrome) (Fig. 7).
Fig. 7 
Abdominal radiograph performed for abdominal distention in a nursing home resident. Dilated loops of large bowel are present. CT failed to identify a specific cause for obstruction, favouring a diagnosis of pseudo-obstruction

Common Radiographically Characterisable Causes of Bowel Obstruction
Herniation:
-
The presence of a bowel loop (either small or large) outside of the expected location of the abdominal cavity with co-existing bowel obstruction suggests an obstructing hernia. Gas within a loop of bowel inferior to the inguinal ligament may suggests an inguinal or femoral hernia, collectively the commonest obstructing hernias.
Volvulus:
-
The large bowel may twist on its mesentery, which can pinch off a loop of large bowel. This commonly occurs at the sigmoid (which can elongate and become mobile in the elderly, predisposing it to volvulus). This is also seen within the caecum, which can be hypermobile in predisposed individuals.
-
The loop may untwist itself, or intervention may be required in the form of intubation (such as with a rectal tube) or surgery.
-
The abdominal radiograph will typically demonstrate a dilated loop of large bowel, said to resemble a coffee bean, although this is often questionable. A dilated loop arising from the right lower quadrant favours a caecal volvulus, while a dilated loop arising from the left lower quadrant favours a sigmoid volvulus.
Perforation:
-
Perforation of the gastrointestinal tract can lead to spillage of contents into the peritoneal cavity (if intraperitoneal) or retroperitoneum (if retroperitoneal), depending on the part of the bowel that perforates.
-
In addition to air, spilled contents typically include fluid when arising from the stomach or small bowel, or feculent material from the colon.
-
The presence of intra-abdominal air that does not conform to the shape of the gastrointestinal lumen suggests perforation (Fig. 8).
Fig. 8 
An abdominal radiograph demonstrates air under the right hemi-diaphragm, consistent with pneumoperitoneum. A positive Rigler sign is also noted, with both sides of the bowel wall exquisitely outlined by air (both intraluminal and extramural). Dilation of both the small and large bowel is also noted
-
As air is the least dense constituent of all abdominal components, it will rise. Erect radiographs can be used to detect even small amounts of air rising up under the diaphragm. A curvilinear lucent line beneath the undersurface of the diaphragm on erect abdominal or chest radiograph may be seen.

Colitis/Toxic Megacolon:
-
Colitis is broad term describing diseases in which the colon is inflamed, and can be secondary to a variety of causes such as infection, inflammatory bowel disease, ischaemia and medications.
-
On radiographs, this may be seen as thickening of the colon wall. The normally thin colon wall becomes thicker, and the normally thin haustral folds progress from fine lines to thicker indentations (likened to the width of the thumb, and thus referred to as “thumbprinting”) (Fig. 9).
Fig. 9 
The transverse colon is dilated in a patient with ulcerative colitis and toxic megacolon. The normally-thin haustral folds are now thickened, giving the appearance of thumbprints projecting from the bowel wall

Gallstone Ileus:
-
Air within the gallbladder suggests either gas forming bacteria within the gallbladder, or a communication between the gallbladder and bowel (in the absence of intervention).
-
In chronic cholecystitis, fistulation between the gallbladder and the bowel can occur. Large gallstones, which would normally be prevented from passing into the GI tract by the narrow width of the cystic duct, can therefore pass through fistulae into bowel, causing obstruction (or gallstone ileus) (Fig. 10).
Fig. 10 
A calcified gallstone is identified within the left central abdomen (arrow). Dilated loops of small bowel are present. Linear air-filled tubular structures within the right upper quadrant consistent with pneumobilia (arrowheads). This is consistent with Rigler’s triad (gallstone ileus). A nasogastric tube has been inserted for gastric decompression
-
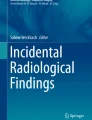
The characteristic combination of small bowel obstruction, an ectopic gallstone, and air in the biliary tree (due to fistulation between the gallbladder and bowel) is known as Rigler’s triad, and is detectable on abdominal radiography (Fig. 11).
Fig. 11 
Abdominal radiograph demonstrates a staghorn calculus within the left renal collecting system. No calculi are seen within the right kidney


Genitourinary Tract
-
Non-contrast is considerably more sensitive for the detection of urinary tract calculi.
-
Urinary calculi can be composed of a variety of material. Stones containing calcium (oxalate stones, struvite stones) are typically well seen on abdominal radiographs. Calculi composed of uric acid, cystine, indinavir or matrix stones can be invisible on abdominal radiograph.
-
Calculi can occur at any level within the urinary tract, including the kidneys, ureters, bladder and urethra (Fig. 11).
-
As with other hollow organs, air can be introduced into the urinary tract by instrumentation, by gas forming bacteria, or by infarction of the wall. Clinical correlation is instructive in such cases.
Mimics of urinary tract calculi:
-
Phleboliths:
-
Calcification within veins is a common occurrence, particularly within the pelvis.
-
These calcifications (referred to as phleboliths) are typically well-circumscribed and round, with a lucent centre. They are often symmetrical and bilateral.
-
-
Stool in air-filled bowel:
-
Stool within bowel overlying the genitourinary tract can obscure urinary calculi disease. Additional views in various phases of respiration can be used in an effort to shift overlying bowel.
-
-
Excreted contrast from recent IV contrast administration:
-
Renal excretion of iodinated contrast can appear dense within the urinary tract, and can mimic calculi. Typically this is bilateral and symmetrical, and there is a history of recent intravascular contrast administration.
-
Retroperitoneum
-
Under normal circumstances, the retroperitoneum contains organs and structures separated by fat.
-
Where a retroperitoneal structure perforates, it may leak contents into the retroperitoneum. This may be seen with perforation of duodenum, ascending or descending colon, pancreas, biliary tree or urinary tract. Leaked content (such as air in the case of bowel perforation) tracks along tissue planes and may outline retroperitoneal structures such as the psoas muscles (Fig. 12).
Fig. 12 
Abdominal radiograph performed in a patient with a remote history of cholecystectomy, presenting with acute upper abdominal pain. The right kidney and right psoas demonstrate a lucent outline, when compared with the left side. This is consistent with a right-sided pneumoretroperitoneum (secondary to a perforated duodenal ulcer)

Displacement of Structures
-
The abdominal organs can enlarge secondary to a number of causes.
-
Enlargement may be detectable by displacement of surrounding structures away from their expected location.
-
Splenic enlargement (splenomegaly) enlarges from the left upper quadrant inferiorly and medially, and may displace bowel inferomedially (Fig. 13). This may be seen secondary to portal hypertension or any haemoglobinopathy.
Fig. 13 
Abdominal radiograph demonstrates a soft-tissue density structure extending from the left upper quadrant and displacing the colon inferomedially, consistent with splenomegaly
-
Liver enlargement (hepatomegaly) enlarges from the right upper quadrant inferiorly, and may displace bowel inferiorly and medially. This is commonly seen due to primary liver disease or metastases.
-
A pelvic mass or distended bladder displaces bowel superiorly and peripherally.
-
Large volume ascites will tend to centralise bowel loops as well as obscure liver and splenic margins.

Medical Hardware and Foreign Bodies
-
A variety of medical devices are commonly encountered within the abdomen:
-
Peritoneal Dialysis Catheter
-
Endovascular Stents
-
Biliary Stents
-
Ureteric Stents, urethral catheters
-
Bowel Stents
-
Feeding Tubes (NG, gastrostomy, etc.)
-
Nerve Root Stimulators
-
Surgical Implements or Gauze
-
Femoral lines
-
IUD
-
Radiologist’s tips
-
When describing a medical device, first determine what is the nature of the device.
-
Ensure that the device is intact, by assessing for any breakage or discontinuity along the line of a device.
-
Ensure the device is within the expected position. Devices may migrate with time, particularly devices with the peristalsing gastrointestinal or urinary tract.
-
Finally, assess if the device could be retained or lost to follow-up. Retained gauze, forgotten ureteric stents or IVC filters represent a significant cause of morbidity.
Vascular Calcification
-
Blood vessels are of a similar density to fluid and soft-tissue, and are thus not directly visualised on abdominal radiographs.
-
Calcific atherosclerotic disease may sufficiently calcify a vessel to allow radiographic assessment however.
-
In addition to signifying increased systemic risk of cardiovascular disease, calcified vessel diameters can be assessed to permit the diagnosis of aneurysms.
Radiologist’s tips:
A checklist to ensure all structures have been assessed is helpful in ensuring a thorough interpretation.
-
Begin by clarifying patient gender, age, radiograph orientation and position.
-
Air—Assess bowel gas pattern. Air should only be present within bowel loops, and any air outside of bowel merits close scrutiny. Unexpectedly-well demarcated tissue planes outlining structures such as the psoas muscles can be a sign of surrounding air.
-
Fat—Assessment of fat planes may be helpful to localise pathology.
-
Fluid/Soft Tissue Density—Loss of normally-seen tissue planes can indicate interposed fluid/soft-tissue, as can be seen with ascites. Displacement of structures away from their expected location can indicate mass effect, such as with organomegaly.
-
Calcifications—All calcifications should all be explainable. Calcification of the costal cartilages, phleboliths, prostate and vascular calcification are all commonly encountered and of little acute clinical significance. Calcification over the genitourinary tract or gallbladder however may indicate stone disease.
-
Surgical hardware/medical devices—Where surgical hardware or medical devices are present, their position and integrity should be assessed.
Suggested Reading
-
James B, Kelly B. The abdominal radiograph. Ulster Med J. 2013;82 (3): 179.
-
Jaffe T, Thompson WM. Large-bowel obstruction in the adult: classic radiographic and CT findings, aetiology, and mimics. Radiology. 2015;275(3):651–63.
-
Wasnik AP, Maturen KE, Kaza RK, Al-Hawary MM, Francis IR. Primary and secondary disease of the peritoneum and mesentery: review of anatomy and imaging features. Abdom Imaging. 2015;40(3):626–42.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Murray, T.E., Pang, E.H.T. (2020). Tutorial 10: The Abdominal Radiograph. In: Redmond, C., Lee, M. (eds) Tutorials in Diagnostic Radiology for Medical Students. Springer, Cham. https://doi.org/10.1007/978-3-030-31893-2_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-31893-2_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31892-5
Online ISBN: 978-3-030-31893-2
eBook Packages: MedicineMedicine (R0)