
Abstract
Hamstring function is influenced by a number of neural, architectural and morphological factors, and the adaptability of these characteristics has important implications for optimizing performance and reducing injury risk. High rates of maximal or near-maximal hamstring force development are required to generate peak horizontal velocities during running, and this is largely determined by the extent to which these muscles can be voluntarily activated. Greater eccentric hamstring strength also correlates with better acceleration capacity and likely improves the ability to decelerate the lower limb during the presumably injurious terminal swing phase of high-speed running. The intra- and intermuscular coordination of the hamstrings appears to influence both hamstring muscle fatiguability and the risk of muscle strain injury. Muscle volume and architectural features such as fascicle length and pennation angle also influence hamstring function, and these vary considerably between hamstring muscles, between individuals and with training status. The adaptability of these features has been explored to a significant extent in recent times, and careful exercise selection allows selective targeting of individual hamstring muscles or muscle segments and this appears to influence the pattern of chronic adaptations such as muscle hypertrophy. Short fascicles within the often-injured long head of biceps femoris may predispose athletes to strain injury but these appear to respond in a contraction-mode-specific manner; lengthening after eccentric training and shortening after concentric training of 4 or more weeks. Conventional training with eccentric and concentric phases in each repetition can also lengthen fascicles, possibly in an excursion (muscle length)-dependent manner. A large biceps femoris muscle to proximal aponeurosis width ratio has been proposed as a potential risk factor for hamstring strain injury, although this is only supported by biomechanical modelling at the time of writing. High levels of anterior pelvic tilt and lateral trunk flexion during sprint running may also predispose athletes to hamstring strain injury, although the quantity of evidence for this is small at the moment. At present, the optimal methods for altering coordination and running technique are not known.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

5.1 Neural Factors Relating to Hamstring Muscle Function, Performance and Injury
5.1.1 Leg Muscle Strength, Rate of Force Development (RFD) and Sprint Performance
In human athletic activities, maximal acceleration and sprint capacity are strongly determined by maximal strength and the rate of force development (RFD) of the lower limb muscles. In terms of lower limb muscle strength, strong inverse relationships (r = −0.94 to −0.61) have been observed between 1-RM squat strength and the time to cover 5, 10 and 20 m sprint distances performed from a standing start [1,2,3]. These observations indicate that a large proportion (r2 = 37–88%) of the inter-individual variance in acceleration/sprint capacity is governed by differences in leg extensor strength.
Independently of maximal leg muscle strength, the ability to generate force rapidly also exerts a governing influence on human sprint performance. For example, static squat RFD normalised to maximal force (maximum voluntary contraction [MVC]) correlated strongly to 5 m sprint time (r = −0.62) when examined in British elite rugby players [4]. Further, athletes with a superior acceleration capacity (5 m sprint time <1 s) were characterised by a 40–60% higher leg extensor RFD in the very early phase of rising muscle force (0–100 ms) compared to players with less explosive acceleration capacity (5 m sprint time ≥1 s). Notably, maximal isometric squat force was not associated with sprint performance (−0.04 < r < 0.25), suggesting that lower limb RFD serves an independent role for human acceleration/sprint ability.
Recent reports have examined the effect of hamstring RFD on sprint and acceleration capacity. For example, Ishøi and colleagues [5] demonstrated that in elite youth football players (16–17 years), isometric hamstring RFD during the early phase of rising muscle force (0–100 ms) was inversely related with 5 m (r = −0.45), 15 m (r = −0.47) and 30 m (r = −0.41) sprint times. Similar relationships have been observed on isolated RFD assessment for the quadriceps and hamstring muscles. Examining Danish elite team handball players (n = 12, DHF Premier League) using isokinetic dynamometry, isometric quadriceps RFD (normalised to body mass) measured in the early contraction phase (0–100 ms) was found to be closely associated (r = −0.71 to −0.78) with the time to cover 5 m and 10 m sprints using a standing start (Aagaard et al., unpublished data). Notably, an equally strong association was noted between isometric hamstring RFD and 10 m sprint times (r = −0.82) (Fig. 5.1). Collectively, these data suggest that hamstring RFD represents an important factor in human sprint and acceleration performance.

Unpublished observations demonstrating the relationship between isometric knee flexor rate of force development (RFD), as assessed on an isokinetic dynamometer (a), and 10 m sprint times in n = 10 Danish elite team handball players (b) (Aagaard and colleagues, unpublished data)
5.1.2 Eccentric Hamstring Strength and Sprint Performance
Sprint speed is governed by two distinct factors: stride length and stride frequency. Theoretically, higher levels of eccentric hamstring strength may improve the rate at which the forward swinging shank can be decelerated during the terminal swing phase of sprinting, which would likely contribute to better sprint performance via greater stride frequency. In addition, high eccentric hamstring muscle force production during the transition from eccentric to concentric contraction, just prior to initial foot contact (start of stance phase) (Fig. 5.2), would be expected to transfer into an enlarged hip extensor moment during the late propulsive stance phase. In support of this notion, maximal eccentric hamstring strength measured in the Nordic hamstring exercise (NHE) was positively related (r = 0.52) to short-distance (20 m) sprint acceleration performance in highly trained youth soccer players (n = 119) [6]. Further, 10 weeks of NHE training in amateur football players (age 17–26 years) stimulated a significant improvement in maximal eccentric hamstring strength which paralleled gains in sprint acceleration performance [7]. Additional reports exist of improved sprint capacity in response to 7–10 weeks of training with the eccentric NHE [8], an eccentrically biased flywheel leg curl [9], or a combination of free weight hamstring exercises [10]. However, sprint acceleration performance appears to be most consistently improved as reflected by faster short-distance sprint times (5, 10, 15 m) [7, 8, 10], whereas gains in longer-distance sprint capacity (30 m) are less frequently observed [9]. In conclusion, training-induced improvements in maximal eccentric hamstring muscle strength can result in enhanced acceleration capacity and maximal sprint speed, and these effects appear to occur independent of training status.

Surface electromyographical (sEMG) activity and muscle lengths of the medial (semimembranosus and semitendinosus (SM and ST) and lateral (biceps femoris long head BFLH) hamstrings throughout various phases of the gait cycle. RF rectus femoris, m metres
5.1.3 Neuromuscular Hamstring Activity, Sprint Performance and Risk of Muscle Strain Injury
The hamstring muscles are highly active during human sprinting, characterised by periods of peak electromyographical (EMG) activity during terminal swing, followed by a second bout of peak EMG activity in the midstance phase [11, 12] (Fig. 5.2). The specific pattern of hamstring activation bears significant importance for overground sprint performance. Recently, Morin and co-workers [13] used multivariate regression analysis to combine measurements of maximal isolated eccentric hamstring strength obtained by isokinetic dynamometry and lateral hamstring (BF) EMG activity recorded during the terminal-swing phase of maximal sprinting, respectively. Together, these measures explained a substantial portion (r2 = 0.49) of the horizontal ground reaction force (FH) produced during the sprints, which represents the main governing factor for maximal sprint acceleration performance. Interestingly, maximal eccentric hamstring strength alone was not associated with FH, underlining that the magnitude and timing of neural drive to active hamstring muscle fibres during the sprint stride plays an important role for a successful sprint performance.
Maximal eccentric muscle force production is influenced by spinally modulated sources of neural inhibition that limit efferent neural drive to the contracting motor units, despite maximal volitional effort (for review, see [14]). This inhibition in voluntary activation capacity can be downregulated by means of physical training, most effectively in the form of heavy-resistance strength training [14,15,16]. Experimental evidence of suppressed motor neuron activity during eccentric muscle actions has been reported for the knee extensors, ankle plantar flexors [14] and the hamstrings [17]. As a consequence, we might expect that increases in eccentric hamstring strength are likely to be highly beneficial not only for sprint acceleration performance (as discussed above), but also for the prevention of muscle strain injury.
In addition to the aforementioned performance benefits, high levels of eccentric hamstring strength may have implications for mitigating the risk of strain injury. Inspection of the in situ force-length relationship for skeletal muscle reveals a pronounced mismatch at elongated muscle lengths between the magnitude of active force production from muscle fibres and the passive stretch forces arising from elongation of the parallel-elastic muscle structures, in steep favour of the latter (Fig. 5.3). This observation predicts that muscle strain injury (1) will predominantly occur during active lengthening at elongated muscle lengths (as contractile force production ≪ passive force production) and (2) will mainly manifest as cellular signs of myotendinous/aponeurosis junction failure. Interestingly, these theoretically derived conditions are well matched by real-life observations [18]. Consequently, reduced eccentric strength expression due to the presence of neural inhibition may well elevate the risk of hamstring strain injury (HSI) [19] due to an increased mismatch between active and passive force-generating structures. Conversely, increasing maximal eccentric hamstring muscle strength as a result of training-induced gains in neural drive (resulting from reduced spinal motor neuron inhibition, as discussed above) reduces the mismatch between active and passive tissue force generation, which would be expected to contribute to a reduced risk of HSI. Evidence for the role of hamstring strength and strength-endurance as a risk factor for subsequent hamstring muscle strain injury is discussed below.

The length-tension relationship for skeletal muscle, illustrating the contribution of active (i.e. contractile) and passive (i.e. series and parallel elastic) components to total tension
5.1.4 Hamstring Strength, Endurance and Injury Risk
Eccentric knee flexor weakness is arguably the most commonly cited risk factor for HSI [20,21,22]. However, as discussed in Chap. 4, the results from prospective investigations are mixed and a recent meta-analysis of isokinetic studies concluded that eccentric knee flexor strength is only weakly associated with hamstring injury [21]. In the largest of these studies, involving 190 hamstring strains in 614 elite Qatari footballers, lower levels of eccentric knee flexor strength significantly increased the risk of future hamstring injury (odds ratio = 1.37; 95% CI = 1.01–1.85) [23]. However, the strength difference between subsequently injured and uninjured players was extremely small (9.1 Nm; effect size <0.2), which indicates that it would be impossible to distinguish between these individuals clinically. Elite Australian rules football [24] and professional soccer players [25] with lower levels of eccentric knee flexor strength (<279 N and <337 N, respectively) during the NHE have been shown to be significantly more likely to suffer hamstring injuries in the following season than stronger players, although contradictory results from studies of similar design [26] and with larger samples [27] have been reported. In the studies to have found an association between eccentric strength and injury rates, interactions were observed between eccentric strength, age and previous hamstring injury, whereby higher levels of strength appeared to counter the risk of injury associated with being older or having a history of hamstring injury [24, 25]. These findings suggest the possibility that eccentric strength may be a more important consideration in athletes who simultaneously present with other predisposing risk factors. However, low to moderate specificities and sensitivities for conventional isokinetic or Nordic knee flexor strength tests suggest that there is very limited value in trying to predict who will sustain hamstring injuries [21, 23, 24, 26]. It is possible that tests of knee flexor strength are simply not specific enough to running and that more specific strength tests may better reflect injury risk.
The effects of fatigue may also limit the value of strength screening because tests are typically performed in a fresh and relatively rested state and this does not reflect the potential impact of repeated sprinting [28,29,30,31] or kicking [32]. Eccentric knee flexor strength falls significantly more than concentric strength after a range of running protocols that include repeated high-speed efforts [28,29,30], and there is some evidence that this is correlated with a decline in surface EMG (sEMG) from the BF long head (BFLH) but not medial hamstrings [31]. Repeated drop-punt kicking also causes preferentially eccentric weakness, and while this occurs alongside reductions in both BFLH and medial hamstring surface EMG, the decline in eccentric strength is correlated only with sEMG changes in the more frequently injured BFLH [32]. While not conclusive evidence, the contraction-mode-specific decline in strength and surface EMG is consistent with the possibility of a deficit in muscle activation which, during the stretching of isolated animal muscles, decreases the amount of energy absorbed prior to specimen failure [33]. Testing eccentric strength, or perhaps some aspects of sprinting performance such as horizontal ground reaction force [34], before, during and after repeated sprint sessions may therefore prove to be of greater value than assessments performed in a rested state.
Hip extensor endurance may be a risk factor for HSI. For example, Freckleton and colleagues [35] reported that amateur and semi-elite Australian rules footballers who sustained a right limb hamstring injury during follow-up performed significantly fewer single leg bridges on that side than players who did not sustain an injury. However, the same was not true for left leg injuries [35]. Schuermans and colleagues [36] have also provided prospective evidence, suggesting that poor knee flexor endurance is associated with higher risk of HSI.
As discussed in detail below (cf. Intra and intermuscular coordination), an altered timing profile in peak hamstring muscle activity and lower amounts of gluteal and trunk muscle activity during the airborne phases of sprinting suggest that imbalances in muscle synergist activation and ‘load sharing’ may also play a role in subsequent strain injury. These observations underline that neuromuscular factors related to muscle activation and coordination may contribute to the aetiology of muscle strain disorders, independently of muscle strength, endurance and RFD. Importantly, such neural factors most likely will be modifiable with training, which suggests a need to develop and implement specific training exercises that will result in a motor reprogramming into less hazardous muscle activation patterns (discussed in the following subsection). Only few reports exist on the effect of hamstring muscle exercise on the specific activation pattern for this muscle group. One study demonstrated that 6 weeks of training with the NHE stimulated increased surface EMG activity of both the semitendinosus (ST) and BF during the performance of the exercise [37]. However, more work is required to validate the transfer effect of specific exercise training on the pattern of hamstring muscle activity during sports activities that involve a high risk of HSI (e.g. sprinting).
5.2 Intra- and Intermuscular Coordination
While the BFLH is the most commonly injured hamstring during high-speed running, it has been proposed that injury risk is not only related to neuromuscular characteristics of this muscle but also to the coordination and the relative contribution of the other hamstrings (intramuscular coordination) [36, 38] and lumbopelvic muscles (intermuscular coordination) [39,40,41].
5.2.1 Intramuscular Coordination of the Hamstrings
Intramuscular hamstring coordination refers to the spatial and temporal patterns of hamstring muscle activation during planned movement. Schuermans and colleagues [38] were the first to propose that altered intramuscular coordination (i.e. between the lateral and medial hamstrings) might contribute to hamstring muscle injury by changing the distribution of load within these muscles. In this study [38], amateur male soccer players completed leg curl exercise until task failure (when they could no longer maintain the required cadence) with 5-kg weights attached to their ankles. Functional magnetic resonance imaging (MRI) assessments of hamstring metabolic activity (from T2 relaxation times) were performed immediately before and after exercise. Participants with a previous history of hamstring injury displayed lower metabolic activity from the ST which was partially compensated for by higher activity from the BF (both heads combined). A prospective follow-up study [36] of 44 male amateur soccer players demonstrated that this greater reliance upon the BF was associated with an increased susceptibility to primary HSI in the following 1.5 seasons. Subsequently injured players also reached task failure in the leg curl test significantly earlier than those who remained injury-free. Schuermans and colleagues [36] suggested that a relatively high reliance on BF was associated with reduced endurance, and this is at least partly supported by more recent sEMG findings, which showed that a disproportionate reliance upon any of the hamstring muscles was related to poor endurance when 20% of maximal knee flexor force was held until task failure [42]. These findings suggest that intramuscular coordination makes a significant contribution to hamstring fatigue [36, 38, 42] and injury risk [36], presumably via its influence on ‘load sharing’ between the hamstring muscles. The prospective observation [36] also suggests that the imbalanced load sharing observed in prolonged isolated knee flexion exercise may also be evident in high-speed running, although this has yet to be observed.
While we currently do not know how to alter the relative reliance upon different hamstring muscles, these findings suggest that to adequately protect athletes from running-related hamstring injury, training should not focus solely on stimulating the BF, but that just as much attention should be given to conditioning its agonists and possibly specifically targeting the ST [36, 38]. Interestingly, the NHE preferentially activates the ST [43], and this observation might partly explain why this simple eccentric hamstring exercise has proven successful in primary and secondary HSI prevention [44, 45].
5.2.2 Intermuscular Coordination: More Than Just a ‘One-Muscle Job’
To effectively contribute to the development of horizontal ground reaction forces in running, the hamstrings need to be coordinated with both synergists at the hip and knee and stabilisers at these and adjacent joints. Recently, Schuermans and colleagues investigated lower limb and lumbopelvic kinematics [40] and muscle activity patterns [39] by performing three-dimensional (3D) motion capture and sEMG measurements between the 15th and 25th metre of 40-m straight line sprints (Fig. 5.4). Sprint techniques were examined in a cohort of 29 male football players using statistical parametric mapping, which allowed investigation of kinematics across the entire gait cycle rather than looking at more discrete time intervals just before or at touch down. Four players who went on to sustain hamstring strains exhibited greater anterior tilt of the trunk and pelvis and higher levels of lateral trunk flexion than 25 players without injury [40] (Fig. 5.4). Of 51 players who performed preseason sprinting with sEMG analysis, 15 went on to sustain a hamstring injury in the subsequent 18 months (1.5 seasons) [39]. Those who suffered hamstring injury exhibited lower levels of normalised gluteus maximus (GM) activity in forward swing and lower levels of trunk muscle activity (obliques and erector spinae muscles combined) in back swing than players who remained injury-free (Fig. 5.4). These between-group differences reached their maximums near the end of the front swing for GM activation and at the end of the backswing for the trunk muscles. The results are supportive of prior biomechanical modelling [46] which suggested that the coordination of lumbopelvic muscles plays an important role in protecting the hamstrings during high-speed running. Chumanov and colleagues [46] suggested that small deviations in the level of lumbopelvic muscle activation would alter the strains experienced by the BFLH in the late forward swing phase of gait, with excessive hip flexor activity and insufficient hip extensor activity both having potential to increase BFLH strain and the risk of injury.

Top: 3D kinematic and sEMG analysis of maximal overground sprint. Middle: Players who subsequently sustained hamstring injury displayed lower gluteus maximus (GM) EMG in forward swing and lower trunk muscle EMG during back swing (airborne) phases of high-speed running than those without injury. Bottom: Soccer players who subsequently sustained hamstring injury during follow-up (FU) demonstrated more anterior pelvic tilt (b) and thoraco-pelvic lateral flexion (d) than players who did not sustain injury (a and c). (Reproduced from Schuermans et al. [39, 40], with permission)
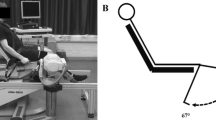
Schuermans and colleagues [41] also conducted a prospective study to examine whether the timing of sEMG onset of the lateral and medial hamstring, GM and erector spinae muscles during prone hip extension had any association with hamstring injury susceptibility (Fig. 5.5). Fifty-one amateur male soccer players performed three prone hip extensions on verbal command and were then followed for injury across 1.5 seasons, during which 15 players sustained hamstring injuries. No significant differences were observed in erector spinae or GM sEMG onsets between subsequently injured and uninjured players. However, subsequently injured players did display a significantly greater delay in hamstring sEMG onset than those with no subsequent injury. No differences were found in sEMG amplitude or contraction intensity of any of the investigated muscles. These findings suggest that the temporal coordination of the hamstrings along with the GM and erector spinae muscles may play a role in safe hamstring functioning and primary injury prevention. Previous hamstring injury history had no influence on the timing of sEMG onset [41]. If a similar delayed onset of hamstring activity were to occur during sprinting, it may contribute to altered loading, potentially increasing the strain that these muscles experience during the terminal-swing phase of gait.

Prone hip extension test with sEMG measurement of posterior chain muscle recruitment
5.3 Structural Factors Relating to Hamstring Muscle Function, Performance and Injury
At the simplest level, muscles are collections of sarcomeres which are laid in series and in parallel with each other so as to span the distance between the aponeuroses and tendons from which they originate and insert. The number of in-parallel sarcomeres determines the physiological cross-sectional area (PCSA) and, to a significant extent, the muscle’s force-generating capacity [47]. The number of in-series sarcomeres influences contractility (the extent to which a muscle can shorten), the theoretical maximum rate at which it can shorten (if completely unloaded) and, to some extent, its force generation while shortening [47]. This latter effect comes about because in muscle shortening at a given rate, sarcomere shortening rates are lower (and force accordingly higher), when there are more contractile elements in series.
The orientation of muscle fascicles and their constituent fibres relative to the long axes of the muscle and the aponeuroses (the pennation angle) also has a significant impact on muscle performance because this dictates the relative distribution of sarcomeres in series and in parallel. As a consequence, a strap-like muscle with a close to zero pennation angle will generate less isometric force but exhibit a greater contractility and a faster maximum rate of shortening than a pennate muscle of equal volume. These two muscles will also have equal peak power outputs, because this measure is proportional to muscle volume, but the strap-like muscle will generate its peak power at higher rates of shortening [47]. The ‘gearing’ of pennate muscles also has an impact because fascicle angle and length changes both contribute to tendon excursion, and this allows fibres to contract more slowly and undergo smaller length changes than the whole muscle-tendon unit (MTU) [48]. Slower fibre shortening enhances force generation in accordance with the force-velocity curve and shortening across a smaller range potentially allows for the muscle to remain close to its optimal length.
As discussed in Chap. 1, the morphological and architectural characteristics of the human hamstrings have received significant research attention. Early studies relied predominantly upon cadavers for assessments of muscle volume, fascicle lengths, pennation angles and estimates of PCSAs [49,50,51], and these parameters are now also being determined via scanning technologies such as MRI and ultrasound (US) [52,53,54,55]. Studies of healthy ‘active’ humans [56] and sprint-trained track and field athletes [53] have revealed significantly larger hamstring muscle volumes and PCSAs than those reported for cadaveric samples which almost invariably come from the sedentary elderly [49]. Table 5.1 shows results from a selection of studies that examined hamstring muscle volumes in young adults [42, 52, 53, 56]. Avrillon and colleagues [42] also assessed hamstring fascicle lengths and pennation angles (at multiple positions along each muscle) via panoramic B-mode US and then estimated PCSA for BFLH and biceps femoris short head (BFSH) and semimembranosus (SM) muscles from the equation:
Here the ST muscle was deemed to be fusiform (pennation angle was taken as zero) and its PCSA was determined by its volume divided by its length [42]. Handsfield and colleagues [56] employed MRI measures of muscle volumes and combined these with the architectural features from cadaver studies. These PCSA measurements (Table 5.1) suggest that the maximum force-generating capacity is ranked SM > BFLH > BFSH > ST [42, 56].
Direct comparisons between the results of different studies must be made with caution because of methodological differences and the use of mixed sex cohorts with varying proportions of male and female participants. Nevertheless, Table 5.1 shows a general trend for hamstring muscles to be larger in athletes. It is also worth noting that the relative sizes of the hamstring muscles vary significantly between cadavers [49] and athletes [52, 53]. For example, Ward and colleagues [49] reported that the ST mass was ~74% of that of the SM in cadavers and this is consistent with the relative volumes of these two muscles in healthy adults (~76%) [56]. In sprint and jump athletes, however, the ST and SM have almost identical volumes (ST is 97% of SM volume) [53].
Handsfield and colleagues [53] have compared lower limb muscle volumes in sprinters and jumpers (hereafter referred to as ‘sprint-trained’ athletes) to those of sedentary young adults [56]. Volumes were determined via MRI and corrected for body size by being expressed relative to the product of height and mass. The greatest degree of relative hypertrophy of all lower limb muscles was observed for the ST, which was 54% larger (relative to body size) in sprint-trained athletes. By contrast, the BFLH and BFSH were both 26% larger, SM 20% larger, GM 31% larger and adductor magnus (AM) 26% larger in the athletes. Hip flexor muscles, the tensor fascia latae, rectus femoris and sartorius were also particularly hypertrophied in athletes, with relative volumes 42%, 40% and 37% larger than non-athletes, respectively. At the other end of the spectrum, some muscles like the gluteus medius (+8%), lateral (+7%) and medial gastrocnemius (+4%) displayed little ‘relative’ hypertrophy according to volume differences [53]. However, some of these muscle bellies may have been shorter in sprint-trained athletes and could potentially have been relatively large in terms of PCSA. For example, sprint-trained athletes have been reported to have thicker lateral gastrocnemius muscles than sedentary adults [57, 58]. While a degree of muscle size difference may have pre-dated sport involvement and potentially helped to ‘select’ certain individuals as speed athletes, these data also suggest the possibility that high-speed running and the associated strength and conditioning programmes place significantly greater ‘overload’ on some muscles than others.
Hamstring muscle morphology also varies considerably between individuals with similar training status and this is often overlooked because we typically see means and standard deviations presented in the literature. So, while SM is fairly consistently reported as the largest of the hamstrings by volume (Table 5.1), Bourne and colleagues observed that it was the largest in only 16 of 30 young adult men who were engaged in recreational sport, while ST and BFLH were the largest by volume in 10 and 4 men, respectively [52]. Furthermore, the BFLH was small as 23% and as large as 35% of the total hamstring volume in the two athletes with the smallest and largest BFLH proportions. Similarly, ST volume ranged from 24% to 39% of the total hamstring volume and similar variability was observed for anatomical cross-sectional areas (ACSAs). These findings suggest considerable inter-individual variability in the hamstring muscles with the greatest potential power outputs and force generation capacities. As yet it is unknown whether this variability has any impact on running performance or the risk of HSI.
The joint torque created by a given skeletal muscle is the product of its force and the length of its moment arm, and sagittal plane hamstring moment arms at the knee vary between hamstrings and with knee angle. For example, the ST moment arm (5.7 ± 0.7 cm) is larger than that of the SM (4.8 ± 0.5 cm) and BF muscles (4.6 ± 0.4 cm) when the knee is flexed by 45° [42]. This partially compensates for the ST’s relatively small PCSA, but in untrained adults, this muscle is still estimated to have 53% and 56% as much torque-generating potential in isometric contractions as the SM and BF muscles, respectively [42]. ST and BF moment arms shorten appreciably as the knee extends between angles of 90° and 0° of flexion, while the SM moment arm remains relatively constant in this range [59]. Consideration of muscle PCSAs [56] and moment arms suggests that the hamstrings are the major providers of knee flexor torque, although a considerable contribution is potentially made by the gastrocnemius which has a large PCSA but relatively small moment arms [60].
Hamstring sagittal plane moment arms at the hip are larger for the ST (5.6 cm) and BF (5.4 cm) than the SM (4.6 cm) [61], and these change across the hip’s range of motion, reaching their peaks between ~30° and 50° of flexion [62]. By contrast, the moment arm of the GM declines, while that of the AM increases considerably between the hip angles of 0° and 90° of flexion. These changes suggest a highly variable contribution to total hip extension torque from the GM and AM across the range of motion (ROM) while the hamstrings’ contribution is likely more constant. Furthermore, the estimated PCSAs of the combined hamstrings (~81 cm2) is substantially larger than that of the GM (~47 cm2) and AM (~46 cm2) [56] suggesting that the hamstrings are particularly strong hip extensors. Nevertheless, given the significant potential for non-hamstring muscles to generate torque, neither knee flexor nor hip extensor strength tests can be considered as assessments of hamstring strength alone.
5.3.1 Muscle Architecture and Function
Vastus lateralis and gastrocnemius fascicles, expressed in absolute terms or relative to limb lengths, are longer in track and field sprinters than in sedentary adults and generally longer in sedentary adults than in endurance-trained runners [57]. Furthermore, fascicle lengths in these muscles are significantly correlated with 100-m sprint performance in male athletes whose best times ranged from 10.0 to ~11.7 s [58] and in female athletes with best times between ~11.0 and 13.4 s [63]. In these studies, sprint-trained athletes exhibited smaller vastus lateralis pennation angles than distance runners, although little difference existed between these groups’ gastrocnemius pennation angles [58, 63]. As the data is retrospective, it is unwise to attribute fascicle length differences to training programme design. Nevertheless, it is likely that longer fascicles are well suited to high-velocity and high-power activities. Furthermore, shorter fascicles are well suited to endurance activities because of the efficiency of having fewer energy-consuming sarcomeres in series. At the time of writing, we are not aware of studies that have compared hamstring fascicle lengths or pennation angles in different athletic groups or attempted to correlate these lengths with sprint performance.
5.3.2 Hamstring Fascicle Lengths, Pennation Angles and Injury Risk
Fascicle lengths and pennation angles vary considerably between the hamstring muscles [42] and, as discussed in Chap. 1, even along the lengths of individual muscles. Fascicles are longest in the ST and shortest in the SM, while pennation angles are highest in the SM and lowest in the ST, although some differences exist between studies (see Table 5.1). These observations suggest that the ST should be able to generate significant forces across a large ROM and when they are shortening rapidly. By contrast, the SM is thought to be best suited to force and power generation at shorter lengths and at slower speeds.
A single prospective study of 152 elite Australian soccer players has demonstrated that those with shorter BFLH fascicles (<10.56 cm) were ~four-fold more likely to sustain a future HSI than those with longer fascicles [25]. Furthermore, the probability of injury was reduced by 21% for every 1-cm increase in fascicle length, while pennation angle and muscle thickness had no association with injury rates. In this study, interactions were also observed between fascicle length, age and prior hamstring injury, whereby longer BF fascicles countered the risk of injury associated with being older or having a history of this injury (Fig. 5.6) [25]. Other studies have reported shorter BF fascicles in limbs with a history of injury to this muscle [64]. Furthermore, the fascicles of previously injured BF muscles have been reported to lengthen less in response to the demands of preseason Australian rules football training than those in uninjured muscles [65]. It has been proposed that short fascicles, with fewer in-series sarcomeres, are more susceptible to damage as a consequence of sarcomere overextension during active lengthening [66].

Top: The interaction between BFLH fascicle length and history of HSI and the probability of future HSI. Bottom: The interaction between BFLH fascicle length and age and the probability of future HSI. Error bars represent 95% confidence intervals. (Replicated from Timmins et al. [25], with permission)
There is a pressing need to more conclusively establish fascicle length as a risk factor for HSI, and the inconsistency of risk factor studies [21, 67] should be considered when designing a training programme with increasing fascicle lengths in mind. It should also be acknowledged that there are limitations to the methods that have most often been employed to estimate skeletal muscle fascicle lengths in vivo [68]. Firstly, two-dimensional US cannot determine the lengths of all fascicles in a complex three-dimensional structure. Secondly, estimates of fascicle length (generally in the region of 9–13 cm) have typically been made on the basis of extrapolating fascicle and aponeurosis structures visualised within the ~4- to 4.6-cm wide fields of view (FOV) with straight lines outside the FOV. In reality, fascicles and aponeuroses are often curved and this may lead to considerable errors in the estimates of fascicle lengths and muscle fibre pennation angles [68].
5.3.3 Altering Muscle Architecture: The Roles of Contraction Mode and Muscle Excursion
There is mounting evidence that eccentric knee flexor training results in lengthening of the BFLH fascicles [52, 55, 69,70,71,72,73,74,75,76], although this adaptation has not always been observed [54, 73]. For example, Lovell and colleagues [73] reported fascicle lengthening when the NHE was performed before but not after soccer training. Increases in fascicle lengths have also been found after both high- and low-volume hamstring training [74] (see Table 5.2). There is also emerging evidence for fascicle lengthening in the ST after NHE training [70] and in the SM after combined NHE and eccentric stiff-leg deadlift training [77].
The findings that knee flexion tasks do not selectively activate the BFLH but nevertheless evoke significant (~10–24%) increases in estimated fascicle lengths [52] might suggest that high levels of activation are not necessary for stimulating architectural changes in the hamstrings. However, absolute levels of BF EMG activity are high in the Nordic exercise [43], and there is also evidence that when low-volume NHE training (eight repetitions per week) is conducted, higher intensities (obtained by holding 5- to 30-kg weights on the chest) are more effective at inducing fascicle length change [75].
Hip extension training using a 45° Roman chair and conventional loading (concentric and eccentric loads were identical) has been shown to lengthen BFLH fascicles in recreationally active men [52]. This is the only training study of which we are aware to have examined the effect of a purely hip extension intervention on BFLH muscle architecture. The effects of the commonly employed Romanian or stiff-leg deadlifts are as yet undetermined.
It is worth noting that despite theories to the contrary [78], the moderate hamstring muscle lengths experienced during the eccentric NHE are not a barrier to fascicle lengthening. In fact, when directly compared, the NHE and the 45° hip extension were shown to stimulate statistically indistinguishable increases in BFLH fascicle lengths, although the mean changes favoured the NHE (21% vs. 13%) [52]. Furthermore, concentric training at long [55] and moderate [76] muscle lengths has been reported to reduce BFLH fascicle lengths so it appears that contraction mode exerts a powerful effect on architectural adaptations. Nevertheless, muscle excursion is also likely to influence fascicle length changes and the one study to have examined long- versus short-length eccentric training reported a statistically insignificant trend for greater fascicle lengthening after long-length training [71].
At the time of writing, we are not aware of any published studies that have examined the impact of sprint training on hamstring fascicle lengths. Nevertheless, increases in vastus lateralis and rectus femoris fascicle lengths have been reported after 5 weeks of sprinting and bounding training in recreationally active individuals [79], so there is nothing infeasible about fascicle length changes in response to high-speed running programmes.
The BFLH fascicle length increases induced by eccentric hamstring training occur very rapidly (within 2 weeks of training with an isokinetic dynamometer) and are lost within 1–4 weeks once training is stopped [55, 74, 75]. The shortening induced by concentric training is also noted within 2–4 weeks but the changes appear to be smaller and more persistent than those seen after eccentric training. For example, Timmins and colleagues [55] observed that the fascicle shortening during 6 weeks of a concentric isokinetic intervention persisted at least for 4 weeks after the cessation of training. The rapidity of some of these changes has prompted doubt as to whether or not the estimates of fascicle length are valid, primarily because some believe that 2 weeks is too short a time for meaningful architectural adaptations to occur within humans. We should also consider the possibility that fascicle lengthening may not be the mechanism that mediates the protective effect of eccentric interventions. Changes in the composition of connective tissue, as discussed below, or other adaptations are possible. However, a muscle’s resistance to the damage caused by eccentric exercise is significantly improved by a single exposure to a small number (6–30) of strong eccentric actions [80]. So, muscle resistance to microtrauma can change drastically with a small number of exercise sessions and this is central to the rationale for eccentric exercise in hamstring injury prevention [81,82,83,84]. However, the repeated bout effect is also known to last for weeks and months [80] while fascicle length changes are reversed more rapidly than this.
Regardless of whether fascicle lengths account for the protective effects of eccentric training, we should consider the contrasting effects of purely eccentric and purely concentric exercise on the susceptibility of muscles to exercise-induced damage. Concentric training has been shown to increase the susceptibility of human [85] and animal muscles [83, 84] to eccentrically induced damage and this may translate to a greater risk of strain injury but will almost certainly influence muscle soreness. As a consequence, the balance between eccentric and concentric stimuli should be carefully considered when designing a training programme.
Two studies have reported that BFLH pennation angles declined with eccentric and increased with concentric training, one involving training on an isokinetic dynamometer [55] and the other involving either the NHE or concentric leg curl [76]. Studies employing the NHE have generally reported small to moderate reductions in BFLH [70, 73,74,75] and ST pennation angles [70]. However, no significant pennation angle changes were observed by Seymore and colleagues [54], who also reported no change in fascicle lengths after NHE. Lovell and colleagues [73] observed a decrease in pennation angle when the NHE was employed before but not after soccer training and the reduction in pennation angles occurred along with an increase in fascicle length. In fact, across most hamstring architecture studies, there is a trend for pennation angles to decrease as fascicle lengths increase [70, 73,74,75]. One eccentric leg curl study reported no changes in pennation angle despite very large increases in fascicle length increases [72]; however, this study differed from all others mentioned here in that the US assessments of BFLH were taken at the distal end of the muscle.
5.3.4 Muscle-Tendon Junction Morphology
The muscle-tendon junction (MTJ) represents the interface between muscle and tendon and is mechanically the weakest part of the MTU [86]. The majority of running-induced hamstring strains affect the proximal MTJ of the BFLH [87], which is also the site of greatest localised tissue strains during active lengthening [88]. Recent work has suggested that the morphology and composition of the proximal MTJ may be associated with its increased propensity for damage.
5.3.5 Aponeurosis Geometry
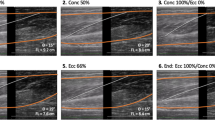
A narrow proximal BF aponeurosis and a large muscle to aponeurosis width ratio have been proposed as potential risk factors for future HSI [89]. Biomechanical modelling [88, 90] has demonstrated that the geometry of this structure strongly influences the location and magnitude of strain within the BF. For example, an 80% reduction in the width of the proximal BF aponeurosis increases strain within the commonly injured proximal MTJ by 60% [88]. Recent work has also identified substantial interindividual variability in the size of the proximal BF aponeurosis and the muscle to aponeurosis width ratio [89, 90] (Fig. 5.7), although no prospective study has explored whether these factors are associated with hamstring injury risk.

BF aponeurosis width measurements showing a wide and narrow aponeurosis. (Reproduced from Fiorentino et al. [90])
If the aponeurosis to muscle width ratio is established as a risk factor in the future, interventions which increase the size of the proximal aponeurosis while having minimal effects on BF size may be valuable for mitigating the risk of running-induced HSI. However, no study to date has assessed training-induced adaptations to BF aponeurosis. Observations from other muscle groups suggest that aponeurosis surface area may increase as a consequence of skeletal muscle hypertrophy, although in the short term at least, muscle dimensions increase significantly more and this may increase muscle fibre strains rather than reduce them. For example, 12 weeks of unilateral knee extensions evoked a 1.9 ± 3.8% increase in the width of the vastus lateralis distal aponeurosis and a 10.7 ± 7.6% increase in its ACSA [91]. However, weightlifters have been reported to display 32% larger vastus lateralis aponeuroses than untrained individuals [92] and this raises the possibility that long-term training may have relatively larger and potentially positive effects.
If aponeurosis to muscle width ratio is established as a risk factor for hamstring injury, subsequent work might then examine the impacts of altering this ratio to differing extents with exercises that target the BFLH to different extents. In this context, it may be worth considering that training with the NHE has relatively small effects on BF muscle volume compared to the hip extension exercise [20].
The collagen composition of the MTJ and its adjoining fibres may be an important factor influencing its susceptibility to damage. Although prospective studies are lacking, a recent training intervention involving individuals scheduled for anterior cruciate ligament surgery demonstrated that 4 weeks of hamstring strength training involving the NHE, leg curls and hip extensions altered collagen expression in the endomysium of muscle fibres at the distal MTJ of the ST and gracilis [93]. Specifically, the intervention appeared to increase the amount of collagen XIV, a protein that may be important in strengthening the extracellular matrix of the MTJ [93]. These results may provide at least one additional mechanism by which strength training interventions protect against HSI.
5.4 Conclusion
Hamstring function is determined by the interaction of a number of neuromuscular characteristics. The ability to generate force rapidly, particularly during active lengthening, is important for optimal hamstring performance and this is influenced to a significant extent by the capacity to fully voluntarily activate these muscles. Structural features such as muscle volume, PCSA, fascicle lengths and pennation angles are also important determinants of hamstring function, and these vary considerably between the heads of this muscle group and between individuals. While more proof is required, short BFLH fascicles may also increase the risk of strain injuries and there is evidence that fascicle length can be altered relatively rapidly with strength training. The complex coordination of hamstring muscles and their synergists also has a role in determining performance, including the endurance capacity of the knee flexors. There is also emerging evidence that dysfunction in intra- and intermuscular coordination plays a role in hamstring injury causation.
At present, there is ample evidence that muscle morphology and architecture can be altered, at least in uninjured individuals, with well-planned exercise programmes. However, there is currently little understanding of how best to improve the various aspects of lumbopelvic coordination so as to best protect the hamstrings from injury.
References
Wisloff U, Castagna C, Helgerud J, Jones R, Hoff J. Strong correlation of maximal squat strength with sprint performance and vertical jump height in elite soccer players. Br J Sports Med. 2004;38(3):285–8.
Comfort P, Bullock N, Pearson SJ. A comparison of maximal squat strength and 5-, 10-, and 20-meter sprint times, in athletes and recreationally trained men. J Strength Cond Res. 2012;26(4):937–40.
McBride JM, Blow D, Kirby TJ, Haines TL, Dayne AM, Triplett NT. Relationship between maximal squat strength and five, ten, and forty yard sprint times. J Strength Cond Res. 2009;23(6):1633–6.
Tillin NA, Pain MT, Folland J. Explosive force production during isometric squats correlates with athletic performance in rugby union players. J Sports Sci. 2013;31(1):66–76.
Ishoi L, Aagaard P, Nielsen MF, Thornton KB, Krommes KK, Holmich P, et al. The influence of hamstring muscle peak torque and rate of torque development for sprinting performance in football players: a cross-sectional study. Int J Sports Physiol Perform. 2018;14:665–73.
Markovic G, Sarabon N, Boban F, Zoric I, Jelcic M, Sos K, et al. Nordic hamstring strength of highly trained youth football players and its relation to sprint performance. J Strength Cond Res. 2018. https://doi.org/10.1519/JSC.0000000000002800.
Ishoi L, Holmich P, Aagaard P, Thorborg K, Bandholm T, Serner A. Effects of the nordic hamstring exercise on sprint capacity in male football players: a randomized controlled trial. J Sports Sci. 2018;36(14):1663–72.
Krommes K, Petersen J, Nielsen MB, Aagaard P, Holmich P, Thorborg K. Sprint and jump performance in elite male soccer players following a 10-week nordic hamstring exercise protocol: a randomised pilot study. BMC Res Notes. 2017;10(1):669.
Askling C, Karlsson J, Thorstensson A. Hamstring injury occurrence in elite soccer players after preseason strength training with eccentric overload. Scand J Med Sci Sports. 2003;13(4):244–50.
Mendiguchia J, Martinez-Ruiz E, Morin JB, Samozino P, Edouard P, Alcaraz PE, et al. Effects of hamstring-emphasized neuromuscular training on strength and sprinting mechanics in football players. Scand J Med Sci Sports. 2015;25(6):e621–9.
Swanson SC, Caldwell GE. An integrated biomechanical analysis of high speed incline and level treadmill running. Med Sci Sports Exerc. 2000;32(6):1146–55.
Simonsen EB, Thomsen L, Klausen K. Activity of mono- and biarticular leg muscles during sprint running. Eur J Appl Physiol Occup Physiol. 1985;54(5):524–32.
Morin JB, Gimenez P, Edouard P, Arnal P, Jimenez-Reyes P, Samozino P, et al. Sprint acceleration mechanics: the major role of hamstrings in horizontal force production. Front Physiol. 2015;6:404.
Aagaard P. Spinal and supraspinal control of motor function during maximal eccentric muscle contraction: effects of resistance training. J Sport Health Sci. 2018;7(3):282–93.
Aagaard P, Simonsen EB, Andersen JL, Magnusson SP, Halkjaer-Kristensen J, Dyhre-Poulsen P. Neural inhibition during maximal eccentric and concentric quadriceps contraction: effects of resistance training. J Appl Physiol. 2000;89(6):2249–57.
Andersen LL, Andersen JL, Magnusson SP, Aagaard P. Neuromuscular adaptations to detraining following resistance training in previously untrained subjects. Eur J Appl Physiol. 2005;93(5–6):511–8.
Opar DA, Williams MD, Timmins RG, Dear NM, Shield AJ. Knee flexor strength and bicep femoris electromyographical activity is lower in previously strained hamstrings. J Electromyogr Kinesiol. 2013;23(3):696–703.
Opar DA, Williams MD, Shield AJ. Hamstring strain injuries: factors that lead to injury and re-injury. Sports Med. 2012;42(3):209–26.
Fyfe JJ, Opar DA, Williams MD, Shield AJ. The role of neuromuscular inhibition in hamstring strain injury recurrence. J Electromyogr Kinesiol. 2013;23(3):523–30.
Bourne MN, Timmins RG, Opar DA, Pizzari T, Ruddy RD, Sims C, et al. An evidence-based framework for strengthening exercises to prevent hamstring injury. Sports Med. 2018;48(2):251–67.
Green B, Bourne MN, Pizzari T. Isokinetic strength assessment offers limited predictive validity for detecting risk of future hamstring strain in sport: a systematic review and meta-analysis. Br J Sports Med. 2018;52(5):329–36.
Shield AJ, Bourne MN. Hamstring injury prevention practices in elite sport: evidence for eccentric strength vs. lumbo-pelvic training. Sports Med. 2018;48(3):513–24.
van Dyk N, Bahr R, Whiteley R, Tol JL, Kumar BD, Hamilton B, et al. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. 2016;44(7):1789–95.
Opar DA, Williams MD, Timmins RG, Hickey J, Duhig SJ, Shield AJ. Eccentric hamstring strength and hamstring injury risk in australian footballers. Med Sci Sports Exerc. 2014;47(4):857–65.
Timmins R, Bourne M, Shield A, Williams M, Lorenzon C, Opar D. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. 2016;50(24):1524–35.
Bourne M, Opar DA, Williams M, Shield A. Eccentric knee-flexor strength and hamstring injury risk in rugby union: a prospective study. Am J Sports Med. 2015;43(11):2663–70.
van Dyk N, Bahr R, Burnett AF, Whiteley R, Bakken A, Mosler A, et al. A comprehensive strength testing protocol offers no clinical value in predicting risk of hamstring injury: a prospective cohort study of 413 professional football players. Br J Sport Med. 2017;51(23):1695.
Greig M. The influence of soccer-specific fatigue on peak isokinetic torque production of the knee flexors and extensors. Am J Sport Med. 2008;36(7):1403–9.
Small K, McNaughton L, Greig M, Lovell R. The effects of multidirectional soccer-specific fatigue on markers of hamstring injury risk. J Sci Med Sport. 2010;13(1):120–5.
Small K, McNaughton LR, Greig M, Lohkamp M, Lovell R. Soccer fatigue, sprinting and hamstring injury risk. Int J Sports Med. 2009;30:573–8.
Timmins RG, Opar DA, Williams MD, Schache AG, Dear NM, Shield AJ. Reduced biceps femoris myoelectrical activity influences eccentric knee flexor weakness after repeat sprint running. Scand J Med Sci Sports. 2014;24(4):e299–305.
Duhig SJ, Williams MD, Minett GM, Opar D, Shield AJ. Drop punt kicking induces eccentric knee flexor weakness associated with reductions in hamstring electromyographic activity. J Sci Med Sport. 2017;20(6):595–9.
Garrett W, Safran M, Seaber AV, Glisson RR, Ribbeck B. Biomechanical comparison of stimulated and nonstimulated skeletal muscle pulled to failure. Am J Sport Med. 1987;15(6):448–54.
Lord C, Ma'ayah F, Blazevich AJ. Change in knee flexor torque after fatiguing exercise identifies previous hamstring injury in football players. Scand J Med Sci Sports. 2018;28(3):1235–43.
Freckleton G, Cook J, Pizzari T. The predictive validity of a single leg bridge test for hamstring injuries in Australian Rules Football Players. Br J Sports Med. 2014;48(8):713–7.
Schuermans J, Van Tiggelen D, Danneels L, Witvrouw E. Susceptibility to hamstring injuries in soccer: a prospective study using muscle functional magnetic resonance imaging. Am J Sports Med. 2016;44(5):1276–85.
Delahunt E, McGroarty M, De Vito G, Ditroilo M. Nordic hamstring exercise training alters knee joint kinematics and hamstring activation patterns in young men. Eur J Appl Physiol. 2016;116(4):663–72.
Schuermans J, Van Tiggelen D, Danneels L, Witvrouw E. Biceps femoris and semitendinosus-teammates or competitors? New insights into hamstring injury mechanisms in male football players: a muscle functional MRI study. Br J Sports Med. 2014;48(22):1599–606.
Schuermans J, Danneels L, Van Tiggelen D, Palmans T, Witvrouw E. Proximal neuromuscular control protects against hamstring injuries in male soccer players: a prospective study with electromyography time-series analysis during maximal sprinting. Am J Sports Med. 2017;45(6):1315–25.
Schuermans J, Van Tiggelen D, Palmans T, Danneels L, Witvrouw E. Deviating running kinematics and hamstring injury susceptibility in male soccer players: cause or consequence? Gait Posture. 2017;57:270–7.
Schuermans J, Van Tiggelen D, Witvrouw E. Prone hip extension muscle recruitment is associated with hamstring injury risk in amateur soccer. Int J Sports Med. 2017;38(9):696–706.
Avrillon S, Guilhem G, Barthelemy A, Hug F. Coordination of hamstrings is individual-specific and is related to motor performance. J Appl Physiol (1985). 2018;125:1069–79.
Bourne MN, Opar DA, Al Najjar A, Shield AJ. Impact of exercise selection on hamstring muscle activation. Br J Sports Med. 2017;51(13):1021–8.
Petersen J, Thorborg K, Nielsen MB, Budtz-Jørgensen E, Hölmich P. Preventive effect of eccentric training on acute hamstring injuries in men’s soccer a cluster-randomized controlled trial. Am J Sports Med. 2011;39(11):2296–303.
van der Horst N, Smits DW, Petersen J, Goedhart EA, Backx FJ. The preventive effect of the nordic hamstring exercise on hamstring injuries in amateur soccer players: a randomized controlled trial. Am J Sports Med. 2015;43(6):1316–23.
Chumanov ES, Heiderscheit BC, Thelen DG. The effect of speed and influence of individual muscles on hamstring mechanics during the swing phase of sprinting. J Biomech. 2007;40(16):3555–62.
Lieber RL, Friden J. Functional and clinical significance of skeletal muscle architecture. Muscle Nerve. 2000;23(11):1647–66.
Blazevich AJ, Sharp NC. Understanding muscle architectural adaptation: macro- and micro-level research. Cells Tissues Organs. 2005;181(1):1–10.
Ward SR, Eng CM, Smallwood LH, Lieber RL. Are current measurements of lower extremity muscle architecture accurate? Clin Orthop Relat Res. 2009;467(4):1074–82.
Woodley SJ, Mercer SR. Hamstring muscles: architecture and innervation. Cells Tissues Organs. 2005;179(3):125–41.
Wickiewicz TL, Roy RR, Powell PL, Edgerton VR. Muscle architecture of the human lower limb. Clin Orthop Relat Res. 1983;179:275-83.
Bourne MN, Timmins RG, Williams MD, Opar DA, Al Najjar A, Kerr GK, Shield AJ. Impact of the nordic hamstring and hip extension exercises on hamstring architecture and morphology: implications for injury prevention. Br J Sports Med. 2017;51(5):469–77.
Handsfield GG, Knaus KR, Fiorentino NM, Meyer CH, Hart JM, Blemker SS. Adding muscle where you need it: non-uniform hypertrophy patterns in elite sprinters. Scand J Med Sci Sports. 2017;27(10):1050–60.
Seymore KD, Domire ZJ, DeVita P, Rider PM, Kulas AS. The effect of nordic hamstring strength training on muscle architecture, stiffness, and strength. Eur J Appl Physiol. 2017;117(5):943–53.
Timmins RG, Ruddy JD, Presland J, Maniar N, Shield AJ, Williams MD, et al. Architectural changes of the biceps femoris after concentric or eccentric training. Med Sci Sports Exerc. 2016;48(3):499–508.
Handsfield GG, Meyer CH, Hart JM, Abel MF, Blemker SS. Relationships of 35 lower limb muscles to height and body mass quantified using MRI. J Biomech. 2014;47(3):631–8.
Abe T, Kumagai K, Brechue WF. Fascicle length of leg muscles is greater in sprinters than distance runners. Med Sci Sports Exerc. 2000;32(6):1125–9.
Kumagai K, Abe T, Brechue WF, Ryushi T, Takano S, Mizuno M. Sprint performance is related to muscle fascicle length in male 100-m sprinters. J Appl Physiol (1985). 2000;88(3):811–6.
Herzog W, Read L. Lines of action and moment arms of the major force-carrying structures crossing the human knee joint. J Anat. 1993;182(Pt 2):213.
Spoor CW, van Leeuwen JL, Meskers CG, Titulaer AF, Huson A. Estimation of instantaneous moment arms of lower-leg muscles. J Biomech. 1990;23(12):1247–59.
Dostal WF, Soderberg GL, Andrews JG. Actions of hip muscles. Phys Ther. 1986;66(3):351–61.
Nemeth G, Ohlsen H. In vivo moment arm lengths for hip extensor muscles at different angles of hip flexion. J Biomech. 1985;18(2):129–40.
Abe T, Fukashiro S, Harada Y, Kawamoto K. Relationship between sprint performance and muscle fascicle length in female sprinters. J Physiol Anthropol Appl Hum Sci. 2001;20(2):141–7.
Timmins RG. Biceps femoris long head muscle architecture a reliability and retrospective injury study. Med Sci Sports Exerc. 2015;47(5):905–13.
Timmins RG, Bourne MN, Hickey JT, Maniar N, Tofari PJ, Williams MD, et al. Effect of prior injury on changes to biceps femoris architecture across an australian football league season. Med Sci Sports Exerc. 2017;49(10):2102–9.
Morgan DL. New insights into the behavior of muscle during active lengthening. Biophys J. 1990;57(2):209–21.
Freckleton G, Pizzari T. Risk factors for hamstring muscle strain injury in sport: a systematic review and meta-analysis. Br J Sports Med. 2013;47(6):351–8.
Pimenta R, Blazevich AJ, Freitas SR. Biceps femoris long-head architecture assessed using different sonographic techniques. Med Sci Sports Exerc. 2018;50(12):2584–94.
Ribeiro-Alvares JB, Marques VB, Vaz MA, Baroni BM. Four weeks of Nordic hamstring exercise reduce muscle injury risk factors in young adults. J Strength Cond Res. 2018;32:1254–62.
Alonso-Fernandez D, Docampo-Blanco P, Martinez-Fernandez J. Changes in muscle architecture of biceps femoris induced by eccentric strength training with nordic hamstring exercise. Scand J Med Sci Sports. 2018;28(1):88–94.
Guex K, Degache F, Morisod C, Sailly M, Millet GP. Hamstring architectural and functional adaptations following long vs. short muscle length eccentric training. Front Physiol. 2016;7:340.
Potier TG, Alexander CM, Seynnes OR. Effects of eccentric strength training on biceps femoris muscle architecture and knee joint range of movement. Eur J Appl Physiol. 2009;105(6):939–44.
Lovell R, Knox M, Weston M, Siegler JC, Brennan S, Marshall PWM. Hamstring injury prevention in soccer: before or after training? Scand J Med Sci Sports. 2018;28(2):658–66.
Presland JD, Timmins RG, Bourne MN, Williams MD, Opar DA. The effect of nordic hamstring exercise training volume on biceps femoris long head architectural adaptation. Scand J Med Sci Sports. 2018;28(7):1775–83.
Pollard CW, Opar DA, Williams MD, Bourne MN, Timmins RG. Razor hamstring curl and nordic hamstring exercise architectural adaptations: impact of exercise selection and intensity. Scand J Med Sci Sports. 2019;29(5):706–15.
Duhig SJ, Bourne MN, Buhmann RL, Williams MD, Minett GM, Roberts LA, et al. Effect of concentric and eccentric hamstring training on sprint recovery, strength and muscle architecture in inexperienced athletes. J Sci Med Sport. 2019;22(7):769–74.
Lacome M, Avrillon S, Cholley Y, Simpson B, Guilhem G, Buchheit M. Hamstring eccentric strengthening program: does training volume matter? Int J Sport Physiol. 2019;2019:1–27.
Guex K, Millet GP. Conceptual framework for strengthening exercises to prevent hamstring strains. Sports Med. 2013;43(12):1207–15.
Blazevich AJ, Gill ND, Bronks R, Newton RU. Training-specific muscle architecture adaptation after 5-wk training in athletes. Med Sci Sports Exerc. 2003;35(12):2013–22.
Chen TC, Nosaka K, Sacco P. Intensity of eccentric exercise, shift of optimum angle, and the magnitude of repeated-bout effect. J Appl Physiol (1985). 2007;102(3):992–9.
Brockett C, Morgan D, Proske U. Human hamstring muscles adapt to eccentric exercise by changing optimum length. Med Sci Sports Exerc. 2001;33(5):783–90.
Brockett CL, Morgan DL, Proske U. Predicting hamstring strain injury in elite athletes. Med Sci Sports Exerc. 2004;36(3):379–87.
Lynn R, Morgan D. Decline running produces more sarcomeres in rat vastus intermedius muscle fibers than does incline running. J Appl Physiol. 1994;77(3):1439–44.
Lynn R, Talbot J, Morgan D. Differences in rat skeletal muscles after incline and decline running. J Appl Physiol. 1998;85(1):98.
Gleeson N, Eston R, Marginson V, McHugh M. Effects of prior concentric training on eccentric exercise induced muscle damage. Br J Sports Med. 2003;37(2):119–25; discussion 25.
Tidball JG. Myotendinous junction injury in relation to junction structure and molecular composition. Exerc Sport Sci Rev. 1991;19:419–45.
Koulouris G, Connell DA, Brukner P, Schneider-Kolsky M. Magnetic resonance imaging parameters for assessing risk of recurrent hamstring injuries in elite athletes. Am J Sport Med. 2007;35(9):1500–6.
Rehorn MR, Blemker SS. The effects of aponeurosis geometry on strain injury susceptibility explored with a 3D muscle model. J Biomech. 2010;43(13):2574–81.
Evangelidis PE, Massey GJ, Pain MT, Folland JP. Biceps femoris aponeurosis size: a potential risk factor for strain injury? Med Sci Sports Exerc. 2015;47(7):1383–9.
Fiorentino NM, Epstein FH, Blemker SS. Activation and aponeurosis morphology affect in vivo muscle tissue strains near the myotendinous junction. J Biomech. 2012;45(4):647–52.
Wakahara T, Ema R, Miyamoto N, Kawakami Y. Increase in vastus lateralis aponeurosis width induced by resistance training: implications for a hypertrophic model of pennate muscle. Eur J Appl Physiol. 2015;115(2):309–16.
Abe T, Kumagai K, Bemben MG. Muscle aponeurosis area is greater in hypertrophied than in normal muscle. J Gen Intern Med. 2012;27:399.
Jakobsen JR, Mackey AL, Knudsen AB, Koch M, Kjaer M, Krogsgaard MR. Composition and adaptation of human myotendinous junction and neighboring muscle fibers to heavy resistance training. Scand J Med Sci Sports. 2017;27(12):1547–59.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Bourne, M., Schuermans, J., Witvrouw, E., Aagaard, P., Shield, A. (2020). Neuromuscular Factors Related to Hamstring Muscle Function, Performance and Injury. In: Thorborg, K., Opar, D., Shield, A. (eds) Prevention and Rehabilitation of Hamstring Injuries. Springer, Cham. https://doi.org/10.1007/978-3-030-31638-9_5
Download citation
DOI: https://doi.org/10.1007/978-3-030-31638-9_5
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-31637-2
Online ISBN: 978-3-030-31638-9
eBook Packages: MedicineMedicine (R0)