
Abstract
Activation and pacemapping in the pulmonary artery (PA) should be considered if the PVC morphology suggests the RVOT as the site of origin. Partial success or unsuccessful ablation for PVC, which appear to be originating from RVOT, could be secondary to its origin from PA instead of RVOT. Mapping can be safely performed in the PA under ICE visualization.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
1 Case Summary
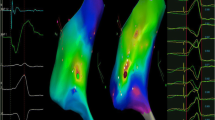
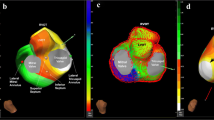
A 61-year-old man was referred for catheter ablation of symptomatic premature ventricular complexes (PVCs). Physical examination and echocardiography did not show any evidence of structural heart disease. An ambulatory monitor showed 42,000 PVCs/24 h. He underwent an attempted catheter ablation procedure to ablate his PVCs at an outside hospital; however, the procedure was aborted because no PVCs were seen. He was started on flecainide and metoprolol but remained highly symptomatic with breakthrough PVCs. He then came for PVC ablation at our facility, at which time abundant PVCs were present. The PVC QRS duration was 165 ms, with left bundle branch block, inferior axis and minimal variability of coupling interval from the prior normal QRS (38 ms) (Fig. 6.1). Activation and pace-mapping were performed in right ventricle (RV), RV outflow tract (RVOT) and pulmonary artery (PA) with assistance of intracardiac echocardiography (ICE). Earliest activation (35 ms prior to PVC QRS onset) was seen at a site above the pulmonic valve within the PA (Fig. 6.2; Video 6.1). A 95% pace-match was observed at this site (Fig. 6.3). Sites just below the pulmonic valve were 22 ms pre-QRS with 85–92% pacematching (Fig. 6.4). Pressure from the ablation catheter at the site where electrograms were 35 ms pre-QRS resulted in sudden transient suppression of PVCs (Fig. 6.5). RF application at the site resulted in complete elimination of PVCs. Can successful PVC ablation be achieved from just below the pulmonic valve?

Twelve lead electrocardiogram showing left bundle inferior axis PVC in a bigeminy pattern

In pulmonary artery the site of earliest activation had electrograms preceding PVC QRS by 35 ms.

Pace mapping at the site of earliest activation in PA had 95% pace match (PVC QRS superimposed in red over paced QRS)

Site just below pulmonary valve at septal RVOT had electrograms preceding PVC QRS by 22 ms

Pressure from ablation catheter at the site of earliest activation in pulmonary artery resulted in complete suppression of PVCs
2 Case Discussion
PVCs and ventricular tachycardia originating in the PA have been reported [1, 2]. It is believed that ectopic impulses form in the PA and conduct down a muscle sleeve to exit into the RVOT. Therefore ablation at site of impulse formation in the PA or its exit point across the pulmonic valve can result in elimination of PVCs. However, if the PA muscle sleeve splits before exiting into the RVOT, ablation in the RVOT could result in a change in QRS morphology but not complete PVC elimination [3,4,5]. Therefore, activation and pacemapping in the PA should be considered if the PVC morphology suggests the RVOT as the site of origin. Mapping can be safely performed in the PA under ICE visualization. The muscle sleeves in the PA appear to be very superficial and therefore we suggest careful mapping to avoid catheter pressure suppression.
References
Timmermans C, Rodriguez LM, Crijns HJ, Moorman AF, Wellens HJ. Idiopathic left bundle-branch block-shaped ventricular tachycardia may originate above the pulmonary valve. Circulation. 2003;108(16):1960–7.
Timmermans C, Rodriguez LM, Medeiros A, Crijns HJ, Wellens HJ. Radiofrequency catheter ablation of idiopathic ventricular tachycardia originating in the main stem of the pulmonary artery. J Cardiovasc Electrophysiol. 2002;13(3):281–4.
Chen YJ, Chen SA, Tai CT, Chiang CE, Lee SH, Wen ZC, et al. Radiofrequency ablation of idiopathic left ventricular tachycardia with changing ECG morphology. Pacing Clin Electrophysiol. 1998;21(8):1668–71.
Chinushi M, Aizawa Y, Takahashi K, Kouji O, Kitazawa H, Washizuka T, et al. Morphological variation of nonreentrant idiopathic ventricular tachycardia originating from the right ventricular outflow tract and effect of radiofrequency lesion. Pacing Clin Electrophysiol. 1997;20(2 Pt 1):325–36.
Tada H, Hiratsuji T, Naito S, Kurosaki K, Ueda M, Ito S, et al. Prevalence and characteristics of idiopathic outflow tract tachycardia with QRS alteration following catheter ablation requiring additional radiofrequency ablation at a different point in the outflow tract. Pacing Clin Electrophysiol. 2004;27(9):1240–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
1 Electronic Supplementary Material
Visualization of ablation catheter inside the pulmonary artery on intracardiac echocardiography (MP4 6310 kb)
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Jain, R., Miller, J.M., Barmeda, M. (2020). Premature Ventricular Complexes from Pulmonary Artery. In: Natale, A., Wang, P., Al-Ahmad, A., Estes, N. (eds) Cardiac Electrophysiology. Springer, Cham. https://doi.org/10.1007/978-3-030-28533-3_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-28533-3_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-28531-9
Online ISBN: 978-3-030-28533-3
eBook Packages: MedicineMedicine (R0)