
Abstract
The significance of the Global Burden of Disease (GBD) studies for recognition of headache as a major public-health concern cannot be overrated.
GBD aims to provide a scientific basis for prioritizations of health investments, decoupling these decisions from professional and commercial interests. It measures disease burden in time units: as years of life lost (YLLs) to a disease (through early mortality), as years of life lived with disability (YLDs), and as the sum of these, expressed as disability-adjusted life years (DALYs). YLDs are estimated as the number of years lived with a disorder (or with a health state attributable to it) multiplied by a disability weight (DW) for that disorder (or health state). YLDs are highly relevant to headache disorders whereas YLLs are not.
Through extensive mathematical modelling, GBD can make use of a wide range of data, allowing estimation of disease prevalence and burden for each gender and all age groups, for all major world regions, nations and, sometimes, areas within countries, for the years from 1990 until 2017 (so far).
GBD is now updated annually. In GBD2016, migraine affected more than one billion people globally, caused 45 million YLDs and was the second most disabling condition worldwide. Among young adults (under 50 years of age), it was the most disabling. Tension-type headache affected 1.9 billion people but, owing to its much lower DW, was estimated to cause only seven million YLDs.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Headache
- Global burden of disease (GBD)
- Years lived with disability (YLD)
- Years of life lost (YLL)
- Disability-adjusted life years (DALY)
- Institute for Health Metrics and Evaluation (IHME)
1 Introduction
In some sense, it is true that migraine appeared on the global health map in 2001, when the World Health Organization (WHO) published its World Health Report of the Global Burden of Disease 2000 study (GBD2000) [1]. Before that, some doctors, in particular headache specialists, some people affected by headache and their organizations were aware of the impact of headache disorders on personal health and well-being. To some degree, they were aware also of their economic impact at individual and societal levels. However, perception of headache as a major public-health concern was mostly lacking, even in these circles. The influence of GBD, from GBD2000 and through its later iterations, has been far-reaching, and not least for the headaches. If the current neglect of headache disorders abates in years to come, the contributory importance of GBD must be recognized.
The aim of this chapter is to provide an overview of the GBD project from its commencement, with a particular focus on headache. We explain the methodology relevant to headache used in GBD2016 and present the main results from this study (for which we have earlier published a thorough analysis [2]). We mention a few methodological changes that were made with regard to headache in GBD2017. Finally, we point to some challenges that should be addressed in future GBD iterations.
2 History of the GBD Studies with a Focus on Headache
2.1 GBD1990
This first GBD project, commissioned by the World Bank in 1991 and undertaken collaboratively by the Bank and WHO, was the background for the Bank’s report, Investment in Health [3]. It was intended to be used by governments and non-governmental organizations (NGOs) to prioritize efforts in healthcare provision and research. Three goals, still highly relevant, were central to the project [4]:
-
1.
To decouple epidemiological assessment of the magnitude of health problems from advocacy of particular health policies or interventions by interest groups
-
2.
To include, in international health-policy debates, information on non-fatal health outcomes along with information on mortality
-
3.
To undertake the quantification of health problems in time-based units that could also be used in economic appraisal
Goals 2 and 3 were fulfilled by establishing a new measure, disability-adjusted life years (DALYs), which are the sum of years of life lost (YLLs) through early mortality and years lived with disability (YLDs). YLL calculations for a disease are based on a set standard life expectancy at the age of each early death, itself derived from a life table combining the lowest observed age-specific mortality rates in any population greater than five million. YLDs are estimated as the number of years lived with a disorder (or with a health state attributable to it) multiplied by a disability weight (DW) for that disorder (or health state).
YLDs are highly relevant to headache disorders, whereas YLLs are not (headache disorders are not considered to be underlying causes of death), but neither migraine nor any other headache disorder were part of GBD1990.
2.2 GBD2000
This follow-up to GBD1990 was undertaken by WHO. It included data on a larger number of conditions, while providing burden estimates for all 21 WHO health regions.
Unlike its predecessor, GBD2000 recognized the importance of mental and neurological disorders and included migraine within these [1]. It used a rather intricate but relatively unsophisticated disease model to estimate overall disability attributable to migraine [5, 6]. Consultations with experts determined the distribution, in the population, of different attack severities (mild, moderate, severe) and their frequencies, and made assumptions about disease duration (between 15 and 45 years) and attack duration (24 h untreated and 6 h treated). A disability weight (DW) based on some previous estimates, on a scale from 0 to 1, was assigned to each attack severity (mild: 0.05; moderate: 0.16; severe: 0.7), and to the periods between attacks, for those with relatively frequent attacks (more than one per week), a DW of 0.03 was assigned. For the different world regions, GBD2000 assumed different proportions of treated and untreated attacks. Combining these DWs proportionately, an overall average DW of 0.03 was assigned to each person with untreated migraine and a DW of 0.007 to each person with treated migraine.
As in later iterations, prevalence estimates were based on population-based studies applying the then-current classification of the International Headache Society (IHS); for GBD2000, this was ICHD-I [7]. Studies included were mostly from Western Europe and North America, with a few from South America, East Asia and the Middle East and one from Africa [5]. Based on these epidemiological data, age-standardized prevalences (i.e. adjusted for age distributions in the different world regions) varied considerably: for women from 17% in parts of Europe to 3% in parts of Africa, and for men from 5.5% to 1%, with world prevalences of 7.9% for women and 2.8% for men [5]. In the whole world, men experienced 0.7 YLDs per 1000 person-years and women 1.8 YLDs per 1000 person-years. In the World Health Report 2001 [1, 5], migraine accounted for 1.4% of all YLDs, which placed it among the top 20 (19th) disabling disorders worldwide. In women of all ages, it accounted for 2.0% of YLDs, putting it in 12th place. Even with no mortality (0 YLLs), migraine was the 19th highest cause of DALYs in young women (15–44 years).
GBD2000 was updated each year until 2004, when migraine fell out of the list of the 20 most disabling disorders, possibly owing to slight adjustments to some of the DWs.
All in all, the burden calculation for migraine in GBD2000 was complicated, not very transparent and based on several questionable assumptions. Nevertheless, the significance of GBD2000 for headache was considerable. It was later stated that
“With the publication of data on burden of migraine in WHR 2001, WHO recognises headache disorders as a high-priority public health problem and as such they deserve higher attention…” [6].
2.3 GBD2010, GBD2013 and GBD2015
GBD2010 was a major revision, with regard not only to its breadth and scope (many more conditions and risk factors) but also to its innovative methods and use of a wide variety of data sources. The project was described as a “systematic, scientific effort to quantify the magnitude of health loss due to diseases, injuries, and risk factors by age, sex, and geography for specific points in time” [8].
GBD was now led by the newly established (2007) Institute for Health Metrics and Evaluation (IHME) at the University of Washington, Seattle, USA, with funding from the Bill and Melinda Gates Foundation. The study had become a truly global endeavour, representing the work of several high-ranking institutions (Harvard University, Imperial College London, Johns Hopkins University, University of Queensland, University of Tokyo and WHO), and altogether included 486 scientists from 302 institutions in 50 countries [9].
In GBD2010, the methodology was substantially revised. While earlier GBD iterations had been based on disease incidence, which is very relevant for prevention but for which there are limited data for many disorders, GBD2000 estimates were instead based on prevalence measures. For these, there were far more data, particularly for the chronic and episodic disorders. Extensive mathematical disease models were introduced to enable use of all available data (rather than selecting a single “most appropriate” source for a particular geographical location) and to provide estimates for all countries and all age and gender groups at different time points. Instead of expert opinions as the basis for determining DWs, these were now to be derived from “lay descriptions” of all health states in a so-called pairwise comparisons method, with, eventually, over 60,000 people participating in nine country surveys and an open internet survey. Descriptions of two hypothetical persons with different, randomly selected health states were presented to respondents, who were asked to indicate which person in their view was the healthier of the two. The rationale behind the method was the intuition that conditions perceived as relatively similar in their effect on health would create more disagreement (i.e. closer to 50/50 responses), while conditions very different in their effect would create less (e.g. 90/10 responses). By comparing all responses, conditions could be ranked from most to least effect on health. Still no exact DW could be assigned: this was achieved by another set of pairwise comparisons, this time of population health programmes. Respondents were asked to compare the health benefits of 30 different life-saving or disease-prevention programmes: for example, one that prevented 1000 rapid deaths and another that prevented a number of cases, varying between 2000 and 10,000, of a non-fatal disease. In this way, health conditions were placed on a 0–1 scale, where 0 was perfect health and 1 was disability deemed equivalent to death.
For headache disorders, now including both migraine and TTH, the method of YLD estimation had in some ways become much less intricate. In contrast to GBD2000, where three levels of migraine attack severity were described and each assigned a DW, in GBD2010 and subsequently, only one (ictal) health state was defined for migraine and one for TTH. This was sensible, because there were limited data on the population distributions of different attack severities. To achieve this, the lay descriptions of the health states attempted to capture, for each disorder, the “mean” headache attack. Thus, in GBD2010, the DW for migraine (ictal state) was 0.434 [10]: during an attack, health loss was equated to 43.4% of death. The corresponding DW for TTH was 0.040 [10].
Data sources for headache from GBD2010 onwards were, mostly, published population-based studies of prevalence identified by regular PubMed searches (using the terms headache epidemiology, headache prevalence, migraine epidemiology and migraine prevalence) and through scrutiny of reference lists in published papers. Some data were also solicited from the GBD network of collaborators, allowing, for example, the inclusion of data from not-yet-published LTB studies. Studies subsequent to the publication of ICHD-I in 1988 [7] were considered, with some earlier studies after appropriate adjustments of the data.
A weakness of GBD2000 was that the large majority of headache studies were from Western Europe and North America; at that time, there were few data from large and populous areas of the world (South East Asia, Eastern Europe, large parts of Africa and mainland China). Some of the few studies existing from outside Europe and North America encompassed many different disorders and gave unrealistically low prevalence estimates (e.g. a study from Saudi Arabia reported a lifetime prevalence of headache overall of only 8% [11]). Prevalence data for GBD2010 were taken from a 2007 review of all published prevalence and burden studies [12], which used explicit quality criteria for acceptance of studies [13]. The result was inclusion of many more studies than those available for GBD2000, but still evidence was lacking from important countries and several regions. Therefore, Lifting The Burden (LTB) [14] supplied supplementary data from new population-based studies performed in Russia [15], China [16, 17] and India [18].
GBD2010 was thus able to report on TTH as well as migraine, while GBD2013 and GBD2015, each including further headache epidemiological studies, added estimates for MOH.
3 GBD2016 and GBD2017
3.1 Methods
A full description and analysis of the methods and results of GBD2016 in relation to headache have been published [2]; the following relates mostly to GBD2016, with GBD2017 mentioned only where the methods differ.
In GBD2016, the number of collaborators increased to more than 2500, from 133 countries [19]. GBD2016 used a hierarchical list of 328 diseases and injuries with four levels of increasing diagnostic detail (“granularity”), in which migraine and TTH were on level 3, under neurological disorders (level 2) and non-communicable diseases (level 1). GBD2017 introduced a new category of “headache disorders” at level 3, displacing migraine and TTH to level 4. At level 5 of the hierarchy, GBD2016 listed 2989 sequelae: the direct consequences of disease or injuries, each mapped to a parsimonious set of 235 health states. GBD2016 considered MOH a sequela of either migraine or TTH rather than a separate entity, and the burden attributed to MOH was added to the burden estimates for each of these disorders according to the proportions believed to arise from them (migraine: 73%; TTH: 27%) [20, 21].
YLDs in GBD reflect the number of years lived with a disorder, adjusted for the attributable health loss expressed in the DW assigned to it. For most diseases, YLDs for a certain year are calculated as prevalence times DW. For episodic disorders such as headaches, the DW pertains only to the symptomatic (ictal) state, and YLD calculations are based on estimates of time in this state.
GBD2016 (and GBD2017) used variations of the DWs, which were first introduced in GBD2013 as participation expanded in the surveys whereby they were quantified (see above). Thus, the DW for migraine (symptomatic state) was increased very slightly to 0.441, and the DW for TTH was diminished very slightly to 0.037. The DW for MOH, included for the first time in GBD2013, was 0.223 [22]. Table 9.1 shows these and the DWs of some other disorders for comparison.
GBD2016 analyzed data from 195 countries and territories grouped into 21 geographical regions and seven super-regions based on geographical proximity and epidemiological similarity of countries [19]. Countries were also scored according to a sociodemographic index (SDI), a composite measure of income, education and fertility meant to capture, roughly, their level of “development” over time [19].
Data sources in GBD2016 included United States (US) medical claims data, for the years 2000, 2010 and 2012. GBD2017 omitted these because of the large adjustments needed to make them comparable with data from population-based studies.
Migraine data were extracted from 135 studies in GBD2016, covering 16 of the 21 GBD world regions; TTH data came from 76 studies in 16 regions; MOH data came from 37 studies in seven regions [19]. For migraine, 13 studies provided data on frequency and duration of attacks, collectively indicating that people with migraine spend, on average, 8.5% of their time in the symptomatic state. For TTH, seven studies indicated 4.7% of time in this state. Frequency and duration were generally categorized, and it was presumed that the mean of the upper and lower limits fairly represented each category. For MOH, only one study provided data [15], indicating that people with MOH have headache on a mean of 23.1 days per month.
3.1.1 Comprehensiveness
GBD studies employ extensive mathematical modelling in order to make them comprehensive: that is, to provide estimates of incidence, prevalence, mortality and remission rate for all included disease states in all countries, in all age groups and both genders, and at different time points. The so-called compartmental disease model provides the relationships between these variables, and can be used to estimate those missing (e.g. there are very few data on incidence for headache disorders). For all headaches, mortality is set at zero, as is occurrence below 5 years of age.
For most disorders, including the headaches, data are scarce or lacking for many countries, regions and age groups, the methods used to estimate prevalence (and incidence) have been heterogenous, and available data are of varying quality (because, for example, of varying case definitions, age categories and representativeness of population samples (see Chaps. 6 and 7)). To enable comprehensiveness in spite of these problems, GBD has developed a so-called Bayesian meta-regression method called DisMod-MR. This mathematically models disease variables such as prevalence and incidence by combining the methods of meta-analysis (using weighted averages of many data points) with estimates of associations (“regressions”) between, for example, prevalence of a disorder and covariates. For headache, these covariates are the fixed effects of gender and of methodological characteristics of studies (“study level covariates” (see below)) and the random effects of geography (region, country). Bayesian means that the method uses priors (initial estimates), derived from other countries, to make final estimates for a certain gender-age group for a country where data are missing.
3.1.2 Adjustment
As to study level covariates, these are taken from the published guidelines on performance and quality evaluation of studies on headache prevalence, burden and cost [13]. From GBD2015 onwards, all headache epidemiological studies have been scored according to a modified version (dichotomized variables) of these criteria, considering representativeness of the population, quality of sampling, headache recall period, participation proportion, survey method, validation of diagnostic instrument and the way in which ICHD criteria were applied. In Dismod-MR, these variables are evaluated as potential covariates for adjustment of data.
In the migraine epidemiological studies in GBD2016, only two of these factors appeared to play a role: low participation proportion and poor survey method. The US claims data apparently underestimated prevalence grossly, by almost 90%, yet their age pattern was consistent with that of US surveys and they were used after adjustment because they provided detailed estimates by state in the USA. For TTH, adjustments were required for survey method, low participation proportion, poor sampling method, poor application of ICHD criteria and lack of validation of the diagnostic instrument. Claims data underestimated TTH prevalence by approximately 85%. For MOH, adjustments were required for poor application of ICHD criteria and low participation proportion.
3.1.3 Borrowing Strength Over Space and Time
By these means, a best guess can be made even where no data exist. Where there are no data for an age group, gender or a time point, estimates are made from those adjacent. For countries with data, final estimates are still, to some degree, informed by those from the whole world, super-region and region, making them less vulnerable to bias and random effects. In GBD terminology, estimates “borrow strength over space and time”.
Each new GBD cycle will include not only new data from the preceding year(s) but also newly available old data concerning past years. Since DisMod is continuously upgraded and refined, new covariates, and values for them, are introduced, and diagnostic entities may be changed. Hence, new estimations affect the whole time series, implying that, for example, migraine estimates for 1990 may not be the same in GBD2010 as in GBD2016 or GBD2017.
3.1.4 Comorbidity Correction
Since many people suffer from the consequences of two or more conditions, especially with aging, simply adding DWs can result in a combined DW greater than 1, which does not have meaning. To avoid overestimation of the burden, both on the individual and at societal level, comorbidity correction for YLDs is the final step.
Comorbidities are considered to be independent of each other: that is, they co-occur by chance, according to their respective prevalences. (Dependent comorbidity is recognized when two disorders tend to co-occur more often than would be expected by chance. Dependent comorbidities are incompletely known, computationally very challenging and probably do not make a large difference to estimates when corrections are made for age.)
In GBD, comorbidity corrections are performed for each gender, age, time and location group. The following example concerns only two comorbid conditions, but the model can include more. In a person with two disorders A and B, with different DWs (DWA and DWB), the total (“cumulative”) DW is calculated by the formula DWA+B = [1 ‑ (1 ‑ DWA)∗(1 ‑ DWB)]. This can intuitively be understood as follows: when a person already with disorder A develops disorder B, the DW of the second disorder is calculated on the basis not of full health but of the health remaining after DWA has been deducted. So, in the example, if DWA = 0.5 and DWB = 0.4, the cumulative DWA+B = 0.7.
The cumulative DW combines the DWs of two (or more) disorders, but, often, interest is only in the resultant DW of one disorder after comorbidities have been taken into account. This is determined by first calculating the attributable DWs with respect to the disorder of interest, and then taking the population averages of attributable DWs in all individuals in the population. This yields comorbidity-corrected YLDs for the disorder in the population. To continue the example, consider a population of 1000 in which disorder A (the disorder of interest) has a prevalence of 10% (100 people affected) and disorder B 5% (50 people affected); furthermore, comorbidity here is solely due to chance. Among the 100 with disorder A, five will also have disorder B. To the 95 without, DWA = 0.5 is applied. Among the five, the disability attributable to A is 0.3, represented by DWattrib = 0.5∗0.6, where 0.6 is the health remaining after deduction of DWB. In the population of 1000, the comorbidity-corrected DW among the 100 people with A is only 0.49, calculated as [(95∗0.5) + (5∗0.3)]/100.
3.2 Headache Estimates in GBD2016
Results have been extracted from relevant parts of the GBD2016 capstone paper on prevalences and YLDs for all diseases [19] and from the publication of headache results [2].
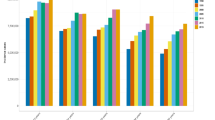
GDB2016 reported almost three billion people affected by headache disorders: 1.90 billion (95% uncertainty interval (UI): 1.71–2.10 bn) had TTH and 1.04 billion (1.00–1.09 bn) had migraine. Globally, TTH was the third most prevalent disorder (after dental caries and latent tuberculosis infection) and migraine eighth [19]. Global age-standardized prevalences were 26.1% (95% UI: 23.6–29.0) for TTH (30.8% [28.0–34.0] in women and 21.4% [19.2–23.9] in men) and 14.4% (13.8–15.0) for migraine (18.9% [18.1–19.7] in women and 9.8% [9.4–10.2] in men). Age-standardized prevalences of both TTH and migraine varied considerably through the different GBD regions and were almost twice as high in Western Europe and Australasia as in Eastern sub-Saharan Africa (Fig. 9.1). The numbers in the different regions (Fig. 9.2) demonstrate that approximately 40% of all people with migraine (430 million) or TTH (770 million) in the world were living in South Asia or East Asia.

Age-standardized prevalences (per 100,000 population) in males (left) and females (right), ranked by total, in the different GBD regions (in alphabetical order: Andean Latin America, Australasia, Caribbean, Central Asia, Central Europe, Central Latin America, Central sub-Saharan Africa, East Asia, Eastern Europe, Eastern sub-Saharan Africa, High Income Asia Pacific, High Income North America, Middle East and North Africa, Oceania, South Asia, Southeast Asia, Southern Latin America, Southern sub-Saharan Africa, Tropical Latin America, Western Europe, Western sub-Saharan Africa) (from [19])

Migraine was responsible for 45.1 (29.0–62.8) million YLDs globally in 2016, and TTH for 7.2 (4.6–10.5) million. Global age-standardized YLD rates (YLDs/100,000 population) were, for migraine, 599.0 (386.0–833.3) (777.6 [500.4–1083.6] in women, 422.3 [274.3–586.7] in men) and, for TTH, 95.9 (61.5–140.0) (114.6 [73.6–162.4] in women, 77.4 [49.6–113.2] in men). Figure 9.3 shows the percentages of all YLDs caused by each disorder analyzed at cause-level 3, highlighting migraine (5.4% of all YLDs) and TTH (0.9%). At level 4, the most specific (granular) cause level, migraine was the second cause of disability (after back pain) in 1990, 2006 and 2016 [19] and, in GBD2016, the first cause of disability in people under 50 years [23]. In terms of percentage of all YLDs, migraine was first in two regions, second in nine, third in five, fourth in two, fifth in two and sixth in one. Globally, TTH was 28th in 1990, 2006 and 2016 [19]. Absolute number of YLDs for migraine increased by 32.3% between 1990 and 2006 and by 14.3% between 2006 and 2016, but the mean changes in age-standardized YLD rates were small (−0.4% and +1.1%, respectively). For TTH, there were also marked increases in absolute rates over the two periods (32.7% and 15.4%, respectively), but not in age-standardized rates (−0.7% and +0.4%). Migraine, along with low back pain, ranked among the top 10 causes of YLDs (age-standardized) in all 195 countries [19].

Headache on the global disease map. Graphical presentation of the relative proportions (age-standardized) of YLDs for all disorders (level 3) in 2016, in both genders and all world regions (blue area: non-communicable diseases; green area: injuries; red area: nutritional, mother-child and communicable diseases (from IHME interactive website: https://vizhub.healthdata.org/gbd-compare/). We have emphasized migraine (red outline) and tension-type headache (yellow outline), and indicated percentage YLDs of the global total
Figure 9.4 relates YLD rates to age for migraine and TTH. Both disorders were most burdensome at ages 35–45 years, whereafter the burdens of both, but particularly of migraine, tapered to less than a third of the peak value by age 85. However, the figure shows that headache, and in particular migraine, represented a substantial burden in young and elderly people.

Global YLD rates (YLDs per 100,000 population) for migraine (light green) and tension-type headache (dark green) for both genders by age (from IHME interactive website (https://vizhub.healthdata.org/gbd-compare/))
Figure 9.5 shows there was no obvious relation between the burdens (DALY rates) of migraine and TTH and SDI in the different groups of countries.

YLD rates (YLDs per 100,000 population) in the five regions defined by sociodemographic index (SDI) for migraine (light green) and TTH (dark green) in men (left) and women (right) (from IHME interactive website (https://vizhub.healthdata.org/gbd-compare/))
With regard to DALYs, these are the same as YLDs for migraine and TTH, since no mortality is attributed to headache. Globally, in both genders and all ages, migraine caused 1.9% (1.3–2.5) of all DALYs, 2.7% (1.8–3.6) of those in women and 1.2% (0.8–1.7) of those in men. The corresponding numbers for TTH were 0.3% (0.2–0.4) for both genders, 0.4% (0.3–0.5) in women and 0.2% (0.2–0.3) in men. Table 9.2 shows the proportion of all YLDs and DALYs for the neurological conditions, stroke and some pain conditions. This shows that migraine is second after low back pain with regard to YLDs and third after low back pain and stroke with regard to DALYs. Among the purely neurological disorders, it is by far the most burdensome.
4 Comments
The GBD studies have recently been described as “a systematic scientific effort to quantify the comparative magnitude of health loss from diseases, injuries and risks by age sex, and population over time” [24]. GBD makes use of a wide variety of data sources on diseases and risk factors, thereby enhancing the value of all the single studies, enabling corrections for comorbidities, associations and known sources of error. There are several limitations to the estimates on headaches that must be taken into consideration and amended, but they nevertheless give a clear message to the world about the importance of headache for global public health.
4.1 The Importance of the GBD Headache Estimates
GBD has shown that headache disorders, and in particular migraine, are among the principal causes of disability all over the world, particularly in women. In 2016, migraine and TTH affected nearly three billion people globally, causing 7% of all YLDs and 2% of all DALYs in spite of no mortality. Migraine was the second cause of disability, and particularly burdensome during the most productive years of life, while its impact was not negligible among children and adolescents, or among the middle-aged and elderly. Migraine is by far the most important cause of morbidity among the purely neurological disorders (except for stroke when measured in DALYs). Among the painful disorders, migraine is the second most burdensome globally, after low back pain (a mixture of disorders).
The increases in headache YLDs over the years are most probably due to growth and aging of the world’s population, since YLD rates (per 100,000) have remained stable. On DALY rankings, the headaches are higher in 2016 than in 1990 because of a decrease in the relative importance of fatal disorders during these years.
GBD also documents that headache is not a western disorder, confined to the rich part of the world. In contrast, some of the highest prevalences are found in some low- and middle-income countries. It has previously been shown that many countries are undergoing a double set of transitions: a demographic transition from high to low mortality and fertility, accompanied by an epidemiological transition from high to low rates of communicable diseases, maternal diseases and childhood mortality, with an increase in relative importance of non-communicable diseases. Both transitions are strongly linked to changes in the SDI. However, headaches seem little affected by these transitions, as there is no obvious relation between SDI level and headache YLD rates. Therefore, it can be predicted that the relative importance of headache for public health will increase as the importance of fatal diseases decrease. Of course, in many poor countries, people suffer the double burden of both communicable and non-communicable diseases: one does not lessen the other.
Finally, GBD shows that the large majority of people with migraine in the world live in countries where medications of proven efficacy are either unavailable or unaffordable for the majority, and where there is little medical attention given to headache. This gives a strong call for improving health care for headache, and embedding it within existing healthcare systems (see Chaps. 13, 14, and 15). The call sounds everywhere: not only in the richest countries. Studies in several developing countries have demonstrated large national productivity losses due to headache: 1.3% in China [17], 1.6% in Ethiopia [25], 1.9% in Zambia [26], 3% in India [27] and 5.6% in Nepal [28]. If only part of this lost productivity can be recovered through better treatment, investments in improved health services will be highly cost-effective (see Chap. 15).
4.2 Limitations in GBD Methods and Headache Burden Estimates
Lack of data is still a limitation. Although a number of headache epidemiological studies in the last decade have included large and populous regions of the world, such as Russia, China, India and parts of Africa, where no data existed before, it remains the case that the majority of studies are from a few high-income regions, and there are still five regions wholly undocumented for migraine. No data exist for the large populations of Indonesia, Vietnam, Bangladesh, Egypt, South Africa and the Democratic Republic of Congo. In sub-Saharan Africa, only five countries have any data on headache. For TTH and MOH, the data are even more scarce. In addition, there are very few population-based studies that provide good estimates of average headache duration and frequency, which are necessary for calculation of time spent in the symptomatic state. Further, there is a need to update results in many places, to gather more reliable data and, perhaps, to monitor secular trends in headache epidemiology.
In GBD, DisMod-MR makes it possible to adjust results of studies according to methodological norms for how to perform and evaluate studies. An important aspect not taken into account in this model is the distinction between definite and probable diagnoses of migraine and TTH. Definite diagnoses fulfil all main diagnostic ICHD criteria, whereas probable diagnoses fail to fulfil one of these. The latter, as noted, are relatively common in epidemiological studies because data gathering is unavoidably less searching and thorough than in clinical settings. Studies that have reported both definite and probable migraine have found similar prevalences of each (see Chap. 7).
Importantly, probable diagnoses do not represent separate nosological entities (see Chap. 6). In clinical settings, they are useful for patients in whom there is diagnostic uncertainty pending confirmation (or refutation) later. This is not the case in epidemiological studies, and, unless probable diagnoses are included within either migraine or TTH, large numbers of people with headache—perhaps half—will not be counted. However, until now, the vast majority of studies of migraine have reported only definite migraine or are silent on the issue.
Studies investigating who received probable migraine diagnoses in epidemiological studies have found the great majority failed on attack duration, reporting attacks of less than 4 h (e.g. [29,30,31]). Otherwise, the characteristics of definite and probable migraine are similar, and the latter is associated with considerable disability and suffering. GBD needs to develop methods to include probable migraine, addressing its omission from most historical data; otherwise, much disability will be unaccounted for. While GBD2017 began the process, the methods need further refinement. Similar arguments can be made for probable TTH, although the missed YLDs are far fewer because of the much lower DW of TTH.
Another problem is the handling of the chronic headache disorders: those characterized by headache on 15 or more days per month for more than 3 months. Many of these will fall into the categories of chronic migraine, chronic TTH or MOH, but these diagnoses generally cannot be made with any certainty in epidemiological studies, which are mostly based on structured questionnaires administered by lay interviewers or self-administered (see Chaps. 6 and 7). Probable MOH may be identified where headache on 15 or more days per month is associated with medication overuse (see Chap. 7), but otherwise these undoubtedly disabling headaches are not captured by the diagnoses used in GBD. It is not clear how this problem might be solved: future epidemiological studies cannot easily improve the recognition of chronic migraine and chronic TTH.
Despite efforts to adjust for methodological differences between studies, some of the variation between countries may be due to measurement error. Efforts to standardize the methods for studies on prevalence and burden of headache, and adherence to the published guidelines ([13]; also, Chaps. 6 and 7), will, hopefully, make future comparisons more reliable of headache-attributed burden across geographical borders and over time periods.
The fact that SDI, when applied across countries and cultures, is not reflected in differences in headache prevalence does not eliminate the possibility that socioeconomic factors are important within a country or region. A socioeconomic gradient, to the effect that low socioeconomic status is linked to higher headache prevalence, has been shown in high-, middle- and low-income countries [15, 32,33,34].
In conclusion, there are still major limitations in GBD headache burden estimations, but they are, by far, the most precise and comprehensive that we have.
4.3 The Challenge for Future GBD Headache Studies
GBD estimates will now be updated annually. They will include more data from countries where none existed, and reflect a continuing development of the methods of imputation of data for countries with little direct evidence.
This requires continued work also in headache. For the headache research community, it must be a priority regularly to feed data of high quality to the project. Whatever is the motivation to do headache epidemiological studies in the future, these studies should be conducted so as to be relevant and informative to GBD. This means use of standardized methodology, study instruments and reporting (see Chaps. 6 and 7). In particular, prevalences should be estimated for each age group by gender, and for definite and probable diagnoses of migraine and TTH. As important are good data on average frequency and duration of headache episodes for each diagnosis, to allow calculations of time spent with headache. Better diagnostic precision for the chronic headache disorders would allow them to be classified as migraine, TTH, MOH or, in a few cases, none of these, but this is a counsel of perfection.
5 Concluding Remarks
When GBD2010 was published, Steiner and co-workers drew attention to the project in the headache science community by authoring an editorial called “Migraine—the seventh disabler”. This was published simultaneously in all three main scientific headache journals [35,36,37], after consultations with the three editors-in-chief, who thereby, presciently, endorsed the importance of GBD for their readers. In these papers, the following statement is found concerning the GBD reports: “Few reports are likely to have more profound meaning for people with headache, or carry greater promise for a better future, than the seven papers … that were presented [in GBD2010]”.
With GBD2016, we can now talk of migraine as the second disabler, and first in people under 50 [23]. With the increased relative importance of non-communicable diseases, the importance of headache for global public health is not likely to diminish in the future.
References
World Health Organization. The World Health Report 2001. Chapter 2. Burden of mental and behavioural disorders; 2001, pp 19–45. http://www.who.int/whr/2001/en/index.html.
Stovner LJ, Nichols E, Steiner TJ, Abd-Allah F, Abdelalim A, Al-Raddadi RM, Ansha MG, Barac A, Bensenor IM, Doan LP, Edessa D, Endres M, Foreman KJ, Gankpe FG, Gururaj G, Goulart AC, Gupta R, Hankey GJ, Hay SI, Hegazy MI, Hilawe EH, Kasaeian A, Kassa DH, Khalil I, Khang Y-H, Khubchandani J, Kim YJ, Kokubo Y, Mohammed MA, Moradi-Lakeh M, Nguyen HLT, Nirayo YL, Qorbani M, Ranta A, Roba KT, Safiri S, Santos IS, Satpathy M, Sawhney M, Shiferaw MS, Shiue I, Smith M, Szoeke CEI, Truong NT, Venketasubramanian N, Weldegwergs KG, Westerman R, Wijeratne T, Xuan Tran B, Yonemoto N, Feigin VL, Vos T, Murray CJL. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17:954–76.
Murray CJ, Lopez AD, Jamison DT. The global burden of disease in 1990: summary results, sensitivity analysis and future directions. Bull World Health Organ. 1994;72:495–509.
Mather C, Bernard CS, Iburg KM, Inoue M, Fat DM, Shibuya K, Stein CM, Tomijima T, Xu H. Global burden of disease in 2002: data sources, methods and results. Global Programme on Evidence for Health Policy discussion paper no 54. Geneva: World Health Organization; 2004. https://www.who.int/healthinfo/paper54.pdf.
Leonardi M, Mathers C. Global burden of migraine in the Year 2000: summary of methods and data sources; 2000. http://www.who.int/healthinfo/statistics/bod_migraine.pdf.
Leonardi M, Steiner TJ, Scher AT, Lipton RB. The global burden of migraine: measuring disability in headache disorders with WHO’s Classification of Functioning, Disability and Health (ICF). J Headache Pain. 2005;6:429–40.
Headache Classification Committee of the International Headache Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalalgia. 1988;8(Suppl 7):1–96.
Murray CJ, Ezzati M, Flaxman AD, Lim S, Lozano R, Michaud C, Naghavi M, Salomon JA, Shibuya K, Vos T, Wikler D, Lopez AD. GBD 2010: design, definitions, and metrics. Lancet. 2012;380:2063–6.
Horton R. GBD 2010: understanding disease, injury, and risk. Lancet. 2012;380:2053–4.
Salomon JA, Vos T, Hogan DR, Gagnon M, Naghavi M, Mokdad A, Begum N, Shah R, Karyana M, Kosen S, Farje MR, Moncada G, Dutta A, Sazawal S, Dyer A, Seiler J, Aboyans V, Baker L, Baxter A, Benjamin EJ, Bhalla K, Bin Abdulhak A, Blyth F, Bourne R, Braithwaite T, Brooks P, Brugha TS, Bryan-Hancock C, Buchbinder R, Burney P, Calabria B, Chen H, Chugh SS, Cooley R, Criqui MH, et al. Common values in assessing health outcomes from disease and injury: disability weights measurement study for the Global Burden of Disease Study 2010. Lancet. 2012;380:2129–43.
Abduljabbar M, Ogunniyi A, Al Balla S, Alballaa S, Al-Dalaan A. Prevalence of primary headache syndrome in adults in the Qassim region of Saudi Arabia. Headache. 1996;36:385–8.
Stovner LJ, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher A, Steiner T, Zwart JA. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27:193–210.
Stovner LJ, Al Jumah M, Birbeck GL, Gururaj G, Jensen R, Katsarava Z, Queiroz LP, Scher AI, Tekle-Haimanot R, Wang SJ, Steiner TJ. The methodology of population surveys of headache prevalence, burden and cost: principles and recommendations from the Global Campaign against Headache. J Headache Pain. 2014;15:5.
Steiner TJ. Lifting The Burden: the global campaign against headache. Lancet Neurol. 2004;3:204–5.
Ayzenberg I, Katsarava Z, Sborowski A, Chernysh M, Osipova V, Tabeeva G, Yakhno N, Steiner TJ. The prevalence of primary headache disorders in Russia: a countrywide survey. Cephalalgia. 2012;32:373–81.
Yu S, Liu R, Zhao G, Yang X, Qiao X, Feng J, Fang Y, Cao X, He M, Steiner T. The prevalence and burden of primary headaches in China: a population-based door-to-door survey. Headache. 2012;52:582–91.
Yu S, He M, Liu R, Feng J, Qiao X, Yang X, Cao X, Zhao G, Fang Y, Steiner TJ. Headache yesterday in China: a new approach to estimating the burden of headache, applied in a general-population survey in China. Cephalalgia. 2013;33:1211–7.
Rao GN, Kulkarni GB, Gururaj G, Rajesh K, Subbakrishna DK, Steiner TJ, Stovner LJ. The burden of headache disorders in India: methodology and questionnaire validation for a community-based survey in Karnataka state. J Headache Pain. 2012;13:543–50.
Vos T, Abajobir AA, Abate KH, Abbafati C, Abbas KM, Abd-Allah F, Abdulkader RS, Abdulle AM, Abebo TA, Abera SF, Aboyans V, Abu-Raddad LJ, Ackerman IN, Adamu AA, Adetokunboh O, Afarideh M, Afshin A, Agarwal SK, Aggarwal R, Agrawal A, Agrawal S, Ahmadieh H, Ahmed MB, Aichour MTE, Aichour AN, Aichour I, Aiyar S, Akinyemi RO, Akseer N, Al Lami FH, Alahdab F, Al-Aly Z, Alam K, Alam N, Alam T, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390:1211–59.
Jonsson P, Hedenrud T, Linde M. Epidemiology of medication overuse headache in the general Swedish population. Cephalalgia. 2011;31:1015–22.
Katsarava Z, Muessig M, Dzagnidze A, Fritsche G, Diener HC, Limmroth V. Medication overuse headache: rates and predictors for relapse in a 4-year prospective study. Cephalalgia. 2005;25:12–5.
Salomon JA, Haagsma JA, Davis A, de Noordhout CM, Polinder S, Havelaar AH, Cassini A, Devleesschauwer B, Kretzschmar M, Speybroeck N, Murray CJ, Vos T. Disability weights for the Global Burden of Disease 2013 study. Lancet Glob Health. 2015;3:e712–23.
Steiner TJ, Stovner LJ, Vos T, Jensen R, Katsarava Z. Migraine is first cause of disability in under 50s: will health politicians now take notice? J Headache Pain. 2018;19:17.
Murray CJL, Lopez AD. Measuring global health: motivation and evolution of the Global Burden of Disease Study. Lancet. 2017;390:1460–4.
Zebenigus M, Tekle-Haimanot R, Worku DK, Thomas H, Steiner TJ. The burden of headache disorders in Ethiopia: national estimates from a population-based door-to-door survey. J Headache Pain. 2017;18:58.
Mbewe E, Zairemthiama P, Paul R, Birbeck GL, Steiner TJ. The burden of primary headache disorders in Zambia: national estimates from a population-based door-to-door survey. J Headache Pain. 2015;16:36.
Steiner TJ, Rao GN, Kulkarni GB, Gururaj G, Stovner LJ. Headache yesterday in Karnataka state, India: prevalence, impact and cost. J Headache Pain. 2016;17:74.
Manandhar K, Risal A, Linde M, Steiner TJ. The burden of headache disorders in Nepal: estimates from a population-based survey. J Headache Pain. 2015;17:3.
Kim BK, Chung YK, Kim JM, Lee KS, Chu MK. Prevalence, clinical characteristics and disability of migraine and probable migraine: a nationwide population-based survey in Korea. Cephalalgia. 2013;33:1106–16.
Lanteri-Minet M, Valade D, Geraud G, Chautard MH, Lucas C. Migraine and probable migraine—results of FRAMIG 3, a French nationwide survey carried out according to the 2004 IHS classification. Cephalalgia. 2005;25:1146–58.
Arruda MA, Guidetti V, Galli F, Albuquerque RC, Bigal ME. Primary headaches in childhood—a population-based study. Cephalalgia. 2010;30:1056–64.
Hagen K, Vatten L, Stovner LJ, Zwart JA, Krokstad S, Bovim G. Low socio-economic status is associated with increased risk of frequent headache: a prospective study of 22718 adults in Norway. Cephalalgia. 2002;22:672–9.
Lipton RB, Bigal ME. The epidemiology of migraine. Am J Med. 2005;118(Suppl 1):3S–10S.
Gururaj G, Kulkarni GB, Rao GN, Subbakrishna DK, Stovner LJ, Steiner TJ. Prevalence and sociodemographic correlates of primary headache disorders: results of a population-based survey from Bangalore, India. Indian J Public Health. 2014;58:241–8.
Steiner TJ, Stovner LJ, Birbeck GL. Migraine: the seventh disabler. Cephalalgia. 2013;33:289–90.
Steiner TJ, Stovner LJ, Birbeck GL. Migraine: the seventh disabler. J Headache Pain. 2013;14:1.
Steiner TJ, Stovner LJ, Birbeck GL. Migraine: the seventh disabler. Headache. 2013;53:227–9.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Stovner, L.J., Nichols, E., Steiner, T.J., Vos, T. (2019). Headache in the Global Burden of Disease (GBD) Studies. In: Steiner, T., Stovner, L. (eds) Societal Impact of Headache. Headache. Springer, Cham. https://doi.org/10.1007/978-3-030-24728-7_9
Download citation
DOI: https://doi.org/10.1007/978-3-030-24728-7_9
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-24726-3
Online ISBN: 978-3-030-24728-7
eBook Packages: MedicineMedicine (R0)