
Abstract
Complex combined injuries to the femora represent a small subset of femur injuries yet warrant the treating surgeon’s utmost attention. This chapter aims to heighten the orthopedic surgeon’s awareness of these combined patterns to improve operative outcomes and minimize complications. Intracapsular and extracapsular femur injuries combined with femoral shaft injuries occur in combination less than 10%, with the majority being intracapsular/shaft combination. Classically, surgeons in training are taught to look for these subtle injuries, but diagnosis is still missed frequently. Misdiagnosis/failure to recognize these patterns leads to higher complication rates noted versus univocal femur injuries. Systematically, this chapter aims to create a “surgical walk-through.” By highlighting preoperative planning/patient evaluation, creation of a “stable operative platform,” surgical approaches, and reduction techniques, both open and closed, the chapter provides a road map for successful treatment of patients with bifocal femoral injury. Ultimately, the authors provide their specific tips, tricks, and pitfalls to addressing these relatively unusual but difficult injuries to treat.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Combined injuries of the ipsilateral femoral shaft and proximal femur are uncommon and they present significant surgical challenges for the treating physician. Estimates of combined proximal femur and shaft injuries (bifocal femoral injury) and typically high-energy vertical femoral neck fractures have historically been reported as high as 9% [1,2,3,4]. Most of our data regarding bifocal femoral injuries are related to intracapsular injuries. However, extracapsular injuries also occur, albeit at a reduced incidence, in combination with femoral shaft injuries and are equally challenging to treat. Extracapsular injuries commonly are transverse intertrochanteric femur fractures [5]. The diaphyseal component is often mid-shaft, transverse, or comminuted and often an open injury [2]. Recognizing these patterns is of the utmost significance as the risk for complications was noted to be higher than for isolated fractures of the femur [4, 6].
The vast majority of the injuries are high energy and most commonly due to motor vehicle collisions [1,2,3,4,5,6]. Careful observation of the proximal segment is of utmost importance as historical data has shown a large percentage of injuries are non-displaced/minimally displaced (up to 59%) and often are missed. Some literature has shown delayed diagnosis rate of upward of 31% [1, 4, 7]. A strict diagnostic approach, careful preoperative evaluation, and optimum implant selection for surgical stabilization of these combined injuries is advocated to minimize treatment delay (due to other distracting pathology in the trauma patient) and minimize complications [8, 9].
Anatomic Location
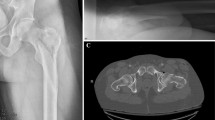
Evaluation of injury films is an essential component to define these injuries and to allow for preoperative planning. For planning purposes we look at two distinct groups of fracture patterns: intracapsular proximal femur fractures with associated diaphyseal femur fractures versus extracapsular proximal femur fractures with associated diaphyseal femur fractures. The intracapsular group consists of femoral neck fractures of varying morphology. The extracapsular group includes basicervical and intertrochanteric femur fractures. Of note again the combination of intracapsular injuries with diaphyseal injuries occurs more frequently than extracapsular injuries in combination.
Preoperative Planning
The aim of our preoperative evaluation is to provide a “surgical walk-through” to fluidly execute the operative plan while creating a “stable surgical platform.” Preoperative planning for femoral shaft fractures associated intracapsular or extracapsular proximal femur fractures requires critical analysis to address all components of the injury. Problem lists for these injuries include competing areas for fixation, poor vascularity, overall bone quality, fracture patterns (load accepting), and pre-injury alignment (open reduction required). Common practice is for the orthopedic surgeon to focus on proximal fracture reduction and fixation (femoral neck/intertrochanteric) prior to addressing more distal fractures (femoral shaft component). The argument is often made that complications like nonunion, malunion, and avascular necrosis of the proximal segment are more difficult sequelae to address relative to diaphyseal complications [6, 9, 10]. Another reason is the high percentage of non-displaced proximal injuries could displace during surgical fixation of the diaphyseal component [1, 4, 5]. Proximal femur fractures can be addressed with a variety of implants but careful consideration of available “real estate” for fixation is needed when combining implants to treat these injuries with the femoral shaft component. Extracapsular/shaft fracture patterns may also be amendable to single implant fixation once anatomic reduction of the proximal component and distal component is achieved.
Recent reviews of literature to evaluate implant choice for fixation of bifocal femoral injuries showed that no consensus exists to scientifically support any one method of fixation [10]. Intracapsular/diaphyseal bifocal femurs in our practice are commonly treated with a formal open reduction and internal fixation. Our approach to stabilize the femoral neck is usually with a 2.0 mm mini-fragment plate contoured to the anterior or medial aspect of the femoral neck and secured with 2.4 mm screws. We add additional fixation with large (6.5 or 7.3 mm) cannulated screw fixation as needed [11,12,13,14]. Occasionally, utilization of the 2.0 mm mini-fragment plates will be utilized with a sliding hip screw. Recent data suggests increased biomechanical strength with locking plate augmentation and overall increased load to failure in utilization of cannulated screws for vertical femoral neck fractures [15]. The diaphyseal femur fracture is then often addressed using standard retrograde intramedullary technique [16].
Extracapsular/diaphyseal bifocal femurs in our practice are commonly addressed with sliding hip screw plus/minus de-rotational screw and retrograde intramedullary nailing [16,17,18,19,20,21]. Single-implant constructs can be utilized to address this injury, but reports have shown an increased incidence of malalignment utilizing one implant [4, 19,20,21].
It is essential to understand the need for direct reduction (in most cases) for femoral neck injuries due to tenuous blood supply and the risk of nonunion. Furthermore, femoral neck union depends on a stable anatomic reduction [1, 11,12,13,14]. Indirection reduction techniques are commonly employed when addressing intertrochanteric and femoral shaft components to minimize biologic insult and promote fracture union. These techniques and their utility will be further elucidated later in the chapter.
Operative Setup
When setting the operative suite for fixation of these bifocal femur fractures, our preference is to use a fully radiolucent table with off the table traction draped into the surgical field (Fig. 18.1). While the fracture table can also be utilized for these fracture patterns, more often in combined extracapsular/shaft injuries, it is not our preference as it can be cumbersome in polytrauma patient positioning, decreases control of the limb, leaves the proximal segment unsupported, and requires a perineal post which presents its own complications. The patient is then positioned on the radiolucent fracture table in the supine position. The patient is then bumped into a floppy lateral position utilizing a rolled blanket to bolster the ipsilateral shoulder torso and hip. Patient is positioned with the shoulders centered on the table and affected hip pulled all the way to the edge of the table (Fig. 18.2). The body is then in a comma position or (C shape) allowing easier access to antegrade starting points as indicated. Skeletal traction either distal femoral or proximal tibial is applied with 1.6 mm K-wire and tension bow with weight (usually £20–25) hanging from rope off the end of the table. A radiolucent triangle or foam ramp is used to assist in positioning of the leg to facilitate easier imaging. All of the above position tips are utilized to create a “stable surgical platform” for the surgeon (Fig. 18.3).

Attachment for radiolucent diving board for our typical off the table traction setup

(a) Placement of patient at the edge of table for access to starting point. (b) Positioning on bolster to roll operative (right) side with arm over position

Placement of tibial skeletal traction off bed with radiolucent triangle to create stable surgical platform
The C-arm is placed on the contralateral side from the affected extremity and the surgeon stands on the side of the ipsilateral hip. C-arm viewing monitor is placed at the foot of the bed for the easy view of the surgeon. The surgical assistant will also stand at the foot of the bed with the mayo stand (Fig. 18.4).

Standard operating room setup. Note position of fluoroscopy, viewer, surgical assistant, and back table
Prior to sterile preparation and drape, it is advocated to obtain comparison images of the contralateral extremity to assist in reduction with length and proximal femur version (rotation). A radiolucent ruler may be employed to measure length or the contralateral limb. Rotational profile can be obtained by performing a perfect lateral of the knee with superimposed femoral condyles and then moving the C-arm proximally and progressing from lateral position rotating C-arm up to obtain a perfect lateral of the proximal femur. The degree difference noted on the C-arm rotation is the version of the femoral neck [22] (Fig. 18.5).

Femoral version image showing fluoroscopic image of “true” lateral of femoral neck and shaft and “true” lateral distal femur
In addition to operative position, it is essential to discuss with anesthesia prior to the case starting about the need for muscle paralysis to aid the surgeon during reduction. General anesthesia with pharmacologic muscle paralysis or spinal anesthesia is recommended during this surgical intervention.
Closed Reduction Maneuvers
In almost every combined femoral case, several closed reduction maneuvers are employed in order to further facilitate and obtain a stable surgical platform. A radiolucent triangle, often small or medium, is placed underneath the ipsilateral knee in order to minimize deforming muscular forces, in particular hip and knee flexors. Strategically placed rolled towels or bumps placed can be utilized to reduce proximal and distal segments, preventing posterior sag. Radiolucent foam ramps may be used as a substitute to the triangles and also work well in combination with rolled towels/bumps to reduce individual segments. Skeletal traction placed either in the distal femur or in the proximal tibia aids further in the help offset the deforming muscular forces and aids the surgeon in maintenance of reduction in combination with muscular paralysis to prevent shortening (Fig. 18.3). Alternatively, technique articles also discuss the use of a femoral distractor as an alternative to the fracture table or off the table traction [23]. In addition manual reduction techniques to manipulate flexion/extension, abduction/adduction, and external/internal rotation aid may result in acceptable reduction on fluoroscopic views prior to proceeding to open reduction techniques.
Reduction Instruments
When preoperative planning for fixation of bifocal femoral fractures, it is essential to have instrumentation specific to the individual injuries in order to facilitate anatomic reduction and fixation. Based on the location of each injury, our preferred instrumentation to aid in reduction of each injury is organized by anatomic location.
Instrumentation specific to femoral neck fractures includes 3/4.0 mm Schanz pins, 2.0 mm K-wires (threaded is better), large and small Weber reduction clamps, modified left and right Weber reduction clamps (Fig. 18.6), and 2.0/2.4 mm mini-fragment plates (Fig. 18.7). When addressing intertrochanteric femur fractures, operative setup should include 2.0 mm K-wires, 5.0 mm Schanz pins, large Weber reduction forceps, ball-spike pusher, bone hook, and collinear clamp (Figs. 18.8 and 18.9). Finally instrumentation specific to the femoral shaft component should include 2.0 mm K-wires, tension bow, 5.0 Schanz pins, large Weber reduction forceps, ball-spike pusher, bone hook, right-angle hemostat, femoral distractor, large external fixator instrumentation, 2.7/3.5 mm locking plates, and the collinear clamp (Figs. 18.9 and 18.10). The specific utility, placement, and pitfalls of these instruments will be discussed later in the chapter.

Reduction forceps (from left to right): (1) large Weber forceps. (2) Modified right Weber forceps. (3) Modified left Weber forceps

2.0/2.4 mini-fragment plates. Note the number of screw holes per unit length increases with 2.0 mm plate

(From right to left) ball-spike pusher, short carbon fiber ex-fix bar with pin to bar clamps, 5.0 mm Schanz pins and 3.2 mm drill bit, T-handles for Schanz pin insertion and manipulation

Long right-angle clamp

Collinear clamp with bone hook attachment
Surgical Approach
The surgical approach to the femoral neck can be obtained utilizing the anterolateral (Watson-Jones) approach or the direct anterior (Smith-Peterson) approach. The anterolateral approach exploits the interval between tensor fascia lata and gluteus medius, both innervated by the superior gluteal nerve (Fig. 18.11). The anterolateral approach allows both applications of implant as well as visualization for reduction maneuvers. The visualization of the femoral neck injury is more difficult than the direct anterior approach as the soft tissue envelope typically proves more limiting. Care must be taken if capsulotomy is performed at base of the neck for visualization as this poses risk to the vascular supply. Femoral neurovascular bundle is at risk if a retractor is placed to medially near the psoas tendon. Furthermore, a postoperative abductor lurch is a known complication of this approach.

(a) Deep exposure of the anterior hip with retractors placed anterior, medial and lateral around anterior hip capsule, (b) Deep retraction of the split posterior gluteus medius, (c) Deep exposure with partial reflection of the posterior gluteus medius tendon. Anterior lateral approach. J Korean Hip Soc. 2011 Jun;23(2):95–102. Korean. Published online June 30, 2011. https://doi.org/10.5371/jkhs.2011.23.2.95
The direct anterior approach superficial dissection is between the sartorius (femoral nerve) and the tensor fascia lata (Fig. 18.12). Deep dissection develops the interval between rectus femoris (femoral nerve) and gluteus medius. Of note, the use of triangle or bone foam flexing the hip increases visualization by relaxing surrounding musculature. Remember that retractor placement can result in a deforming force on the posterior femoral neck accentuating deformity (retroversion). During the approach dissection is essential to identify and protect lateral femoral cutaneous nerve as injury can result in a painful neuroma. For this reason, we recommend moving the skin incision 2 to 3 fingerbreadths lateral to the first muscle interval. During the deeper dissection, the surgeon must also identify the ascending branch of the lateral femoral circumflex artery as this may cause excessive bleeding if not controlled. The direct anterior approach provides excellent visualization of the femoral neck fracture allowing assessment of comminution/displacement as well as placement of reduction forceps or supplemental fixation (Fig. 18.13). The anterior approach is commonly used in association with a lateral approach for implant placement. Our preference is the use of the combined anterior and then a smaller lateral approach in the young patient with a combined intracapsular proximal femur injury and femoral shaft injury as we feel this injury necessitates anatomic open reduction of the femoral neck. Geriatric patients may have an attempt at closed reduction of proximal injury and if deemed acceptable may not require a formal open approach.

(a) Superficial exposure of the anterior approach to the hip with sartoris anterior and tensor posterior, (b) Retraction of the gluteus medius posterior esposing superior lateral caspule. Direct anterior approach. J Korean Hip Soc. 2011 Jun;23(2):95–102. Korean. Published online June 30, 2011. https://doi.org/10.5371/jkhs.2011.23.2.95

Provisional plate fixation of femoral neck with K-wire
When approaching basicervical and intertrochanteric femur fracture component, the direct lateral approach to the hip provides excellent access. Superficially, the tensor fascia lata is split. The direct lateral approach splits the gluteus medius proximally (if necessary) and vastus lateralis (femoral nerve) distally. Extension proximally is limited by the gluteus split and the superior gluteal nerve about 5 cm above the greater trochanter. Distal dissection of the vastus lateralis typically involves making a small L-shaped release of anterior proximal lateralis insertion and carefully splitting the fibers of the lateralis to minimize soft tissue insult. Again our preference for this injury, extracapsular proximal femur with associated femoral shaft fracture, is the more extensive open lateral approach in the young patient as we feel this injury necessitates anatomic open reduction. Geriatric patients, in our hands, may have closed reduction of proximal injury that is deemed acceptable and may not require formal open approach.
Access to the femoral shaft can be obtained through the same direct lateral approach as above when plating or directly reduction is needed. The tensor fascia is split in-line and then the fibers of the vastus lateralis can be elevated off the intermuscular septum. Care must be taken during dissection to identify and ligate the perforating vessels while elevating the vastus lateralis. Although, in the majority of cases, we use percutaneous methods or indirect methods to achieve reduction of the diaphyseal component, the direct lateral approach proves useful when minimally invasive methods fail to provide acceptable reduction. Careful dissection and understanding the anatomy of this approach is essential to minimize soft tissue insult.
When retrograde intramedullary nailing is the treatment of choice, a transpatellar ligament splitting approach through the anterior knee is utilized. While some may advocate a medial parapatellar approach, this is not our approach of choice. For antegrade approaches a lateral approach several centimeters proximal to the greater trochanter is utilized. Sharp dissection is carried down through the fascia and then access to the piriformis fossa or trochanteric entry points can be accessed depending on implant choice.
Open Reduction
When addressing femoral neck injuries, the anteroinferior neck typically provides the best cortical read and the posterior aspect of the neck typically presents with varying amounts of comminution. Utilization of 3/4.0 mm Schanz pins at the head/neck junction as well as in the proximal femoral segment allows for joystick movement of the segments to help manipulate angulation, rotation, and translation (Fig. 18.14). Alternatively threaded K-wires may also be placed in the femoral head again to utilize joystick control over the head. In order to assure neck length as well as maintenance of reduction in the face of comminution, an anterior inferior 2.0/2.4 mm mini-fragment plate can be applied to the neck (Figs. 18.13 and 18.15). Large Weber spin down clamps can be positioned to compress across fracture planes. In addition these clamps may be modified straightening one tine. Straightening of one tine facilitates ease of placement of tines into 2.5 mm drill holes, which can be positioned for optimal open reduction (Fig. 18.6). Placing the clamp anteriorly will allow compression of the anterior usually intact cortical surface of the femoral neck. It may however induce some excessive anteversion so attention to the femoral neck version is recommended.

Utilization of Schanz pins, right-angle clamp, and ball-spike pusher to achieve acceptable reduction of extracapsular component

Femoral neck with mini-frag plate, K-wire, clamp, and perc screw
In our hands, reductions of extracapsular injuries are largely done with percutaneous techniques. Again utilization of 5.0 mm Schanz pins in the proximal and distal segment femur allows for joystick movement of the segments to help manipulate angulation, rotation, and translation (Fig. 18.16). Percutaneous stab incisions may be made under fluoroscopic guidance to insert ball-spike pusher in both the coronal and sagittal planes. Percutaneous clamps, including large Weber reduction forceps and the collinear clamp, may also be placed to reduce the fracture prior to fixation (Fig. 18.17b, c). Care is taken to orient clamps under fluoroscopic guidance to achieve reduction across fractures planes as well as with implant placement in mind. Bone hooks or long right-angle clamps can also be used to pull fragments and reduce the fracture prior to fixation (Fig. 18.14). Open reduction may be necessary based on fracture displacement as well as your patient’s body habitus. Utilizing a lateral approach allows visualization as well as the ability to palpate fracture lines and assess quality of reduction.

Percutaneous reduction of femoral shaft with unicortical schanz pins used as joysticks

(a) Percutaneous clamps for comminuted femoral shaft. (b) Clamp on the femoral neck holding reduction prior to pinning. (c) Collinear clamp for subtrochanteric fracture
The diaphyseal component of the injury is often addressed by percutaneous and/or indirect reduction techniques. Unicortical Schanz pins 5.0 mm can be utilized via percutaneous stab incisions to hold and maintain provisional reduction. Pins may be held by an experienced assistant, application of pin to bar clamps, and external fixation of carbon fiber bar or femoral distractor (Fig. 18.18). The use of external fixator/femoral distractor frees the assistant as well as more reliably maintains length rotation and alignment helping to create a stable surgical platform. Pins again require strategic placement to avoid consuming real estate for fixation. Once again, percutaneous stab incisions may be made under fluoroscopic guidance to insert a ball-spike pusher, bone hooks, large right-angle clamps, large Weber reduction forceps,, and collinear clamp to aid in fracture reduction prior to fixation (Figs. 18.14–18.17). Remember to orient clamps under fluoroscopic guidance to achieve reduction across fracture planes as well as with implant placement in mind. Open reduction is often utilized in the case of an open diaphyseal injury or when percutaneous methods have failed. A direct lateral approach can be utilized and exposure of the fracture site allows exposure for direct reduction and provisional fixation utilization of well-placed lag screws or unicortical locking plate fixation with 2.7 or 3.5 mm implant (Fig. 18.19). Definitive fixation with a nail or larger plate can then be placed to maintain the reduction (Fig. 18.20).

Anterior ex-fix for provisional alignment segmental femur distal

Mini-frag plate holding provisional fixation distal femur. Schanz pain holding varus/valgus. Finger reduction tool for wire passage prior to nailing

Treatment of triple segmental femur injury in 30-year-old female
Implant Insertion
In the treatment of these injuries, cannulated screw fixation needs to be positioned against femoral neck cortex particularly against the posterior and inferior cortex. Cannulated crews should be positioned above the lesser trochanter to minimize a stress riser but also allow access for intramedullary implants. Careful scrutiny of tip to apex distance in sliding hip screw or cephalomedullary constructs is needed to ensure distances of 20 mm or less to minimize implant failure. Radiographic views of both “true” AP and lateral views of the hip are essential to evaluate final implant fixation in the proximal segment. Utilization of preoperative measurements of femoral neck version and femur length should be checked upon final implant insertion to minimize discrepancy as previously described. Evaluation of the lateral knee is essential for evaluation of retrograde intramedullary nail placement to ensure nail depth above Blumensaat’s line.
Tips/Tricks/Pitfalls
In order to successfully manage these difficult bifocal femoral injuries, one must be able to perform “open” reductions when necessary. With these injuries, closed reduction (indirect) techniques will often not be successful and the surgeon will have to move to an open reduction to obtain adequate alignment. However, for a multitude of reasons, the surgeon often accepts inadequate closed reductions. The resistance to moving to an open reduction to obtain the necessary reduction must be overcome. Accepting less than anatomic reduction in a young patient with a femoral neck fracture is essentially accepting failure. The surgeon treating this injury must be comfortable, capable, and proficient with performing open approaches around the hip and lateral femur in order to expect good outcomes.
Having said that, using percutaneous techniques to obtain the acceptable reduction should be exhausted before moving to open reduction. The percutaneous techniques become easier and the surgeon becomes more fascicle using them with time and experience. Understanding the deforming forces is critical and alleviating them with traction, bumps, leg supports, etc. can create the nearly acceptable reduction and a stable operative platform. Once the “macro” reduction has been obtained, the “micro” reduction (anatomic) can often be obtained fairly easily using the percutaneous reduction techniques. As with all surgical endeavors, the learning curve for use of percutaneous devices to facilitate a closed reduction of a bifocal femoral fracture is real but certainly worth learning. Preserving the biology by avoiding the need for an open reduction can be the difference between union and nonunion. Remembering the axiom of preserving the biology is paramount to successful outcomes in managing this complex injury.
Specific tips I have for managing the intracapsular fracture associated with the femoral shaft fracture are that open reduction is usually the rule rather than the exception. The opposite is true for the femoral shaft component of this injury. After performing the anterior approach to the hip, I like to use the 3/4 mm Schanz pins as joysticks to manipulate the femoral neck fracture fragments. Once I can reduce the fracture with the joysticks, I often place a modified Weber (point to point) clamp anterior and superior to hold and compress the fracture. At this point, I often place a 2.0 mm medial femoral neck plate. Placement of a small plate can add significant stability before placing lateral based hardware (cannulated screws or sliding hip screw). Additionally, the medial femoral neck plate will resist the torque placed on the head by the cannulated and/or the sliding hip screws.
If Weber clamp placement is unsuccessful, a small unicortical plate anterior can be placed to hold the reduction before adding lateral fixation. However, the anterior plate must be contoured to avoid retroverting the head fragment. Additionally, the hardware can take up important real estate and potentially block lateral fixation. Unicortical fixation is my preferred method using at least one locking screw on each side of the fracture.
Once the proximal intracapsular reduction is obtained, the diaphyseal femur fracture is managed with a retrograde nail using percutaneous reduction techniques.
Specific tips regarding reduction and management of the extracapsular proximal femur fracture and femoral shaft injury are focused again on obtaining and maintaining the proximal femur reduction. For this injury, I exhaust all percutaneous techniques before moving to open reduction. The proximal fragment is often flexed and adducted by the pull of the psoas and the abductors. Placing a ball-spike pusher anterior laterally can often correct both vectors simultaneously. I usually place a 2.5 mm drill hole for the tip of the ball spike to rest in before pushing on this fragment. Once I have the fragments reduced, provisional K-wires (usually 2.8 or greater) can be placed to hold the reduction. Occasionally, the fracture plane will accept either a collinear clamp or a Weber clamp that will hold the reduction prior to placing definitive fixation. In my hands, if I can effect an anatomic reduction of the proximal femur, I would lean toward one fixation device to hold the proximal and shaft fracture, usually a cephalomedullary nail. I prefer to use a two-screw cephalomedullary nail in the younger patient but move to a single screw or blade for the elderly patient.
Plate fixation of the proximal femur is acceptable, but it needs to be a fixed angle so I would lean toward a blade plate or a sliding hip screw. If a standard lateral proximal femur plate is chosen, one must remember they all have poor biomechanics with high failure rates of the plate around the subtrochanteric region. So if the shaft fracture is close to the subtrochanteric region, indirect reduction is paramount as direct exposure will likely prolong healing and put the plate at risk of early failure. Again, if the proximal injury is secured with a short fixed ankle device like a sliding hip screw, the shaft component of this bifocal injury can be treated with a retrograde nail or by just elongating the plate laterally in a percutaneous submuscular fashion.
The reduction with Schanz pins placed anteriorly is usually successful and will allow nail or plate passage without two much difficulty. The use of skeletal traction off the table will be needed as well as a radiolucent triangle with bumps to help with alignment of the shaft for passage of a nail while holding the reduction. If a long side plate is chosen, percutaneous placement of the distal screws is my preferred method of fixation here.
Summary
Management of bifocal femoral fractures is challenging. Prioritizing the proximal intracapsular injury is mandatory (especially in the younger patient) for good outcomes. The surgeon must be knowledgeable and facile with open reduction techniques of the proximal femur and move to them when closed reduction techniques are unable to produce acceptable alignment. The diaphyseal component of the injury requires the surgeon to continue to be vigilant with length rotation and alignment but can often be managed by closed indirect reduction means with a nail or long plate. The authors have attached some of the cases we have treated to union successfully using these aforementioned techniques (Figs. 18.21, 18.22, 18.23, 18.24, 18.25, 18.26, and 18.27).

Complex triple segmental femur. Non-displaced vertical femoral neck, comminuted diaphyseal and supracondylar/intercondylar distal femur fractures

Proximal nail with supplemental screw fixation of neck and subtrochanteric fracture

Provisional fixation SC/IC distal portion of segmental femur fracture

(a, b) Final fixation of segmental femur with nail, lag screw, and neutralization plate

(a, b) Bifocal EC/shaft treated with single implant

Quadruple segmental femur fracture

Quadruple segmental femur fracture comminuted intertrochanteric femur, diaphyseal femur, supracondylar and intercondylar distal femur fracture
References
Wolinsky PR, Johnson KD. Ipsilateral femoral neck and shaft fractures. Clin Orthop Relat Res. 1995;318:81–90.
Alho A. Concurrent ipsilateral fractures of the hip and femoral shaft: a meta-analysis of 659 cases. Acta Orthop Scand. 1996;67(1):19–28.
Bennett FS, Zinar DM, Kilgus DJ. Ipsilateral hip and femoral shaft fractures. Clin Orthop Relat Res. 1993;296:168–77.
Barei DP, Schildhauer TA, Nork SE. Noncontiguous fractures of the femoral neck, femoral shaft, and distal femur. J Trauma. 2003;55:80–6.
Barquet A, et al. Epidemiology and diagnosis of ipsilateral femoral neck and shaft fractures: a systematic review of 1761 cases in 1758 patients (1990–2015). Trauma Cases Rev. 2015;1:3.
Watson JT, Moed BR. Ipsilateral femoral neck and shaft fractures: complications and their treatment. Clin Orthop Relat Res. 2002;399:78–86.
Swiontkowski MF, Hansen ST Jr, Kellam J. Ipsilateral fractures of the femoral neck and shaft. A treatment protocol. J Bone Joint Surg Am. 1984;66(2):260–8.
Tornetta P III, Kain MS, Creevy WR. Diagnosis of femoral neck fractures in patients with a femoral shaft fracture. Improvement with a standard protocol. J Bone Joint Surg Am. 2007;89(1):39–43.
Hak DJ, et al. Ipsilateral femoral neck and shaft fractures: current diagnostic and treatment strategies. Orthopedics. 2015;38(4):247–51.
Boulton CL, Pollak AN. Special topic: ipsilateral femoral neck and shaft fractures—does evidence give us the answer? Injury. 2015;46(3):478–83.
Panteli M, Rodham P, Giannoudis PV. Biomechanical rationale for implant choices in femoral neck fracture fixation in the non-elderly. Injury. 2015;46(3):445–52.
Thein R, et al. Osteosynthesis of unstable intracapsular femoral neck fracture by dynamic locking plate or screw fixation: early results. J Orthop Trauma. 2014;28(2):70–6.
Bedi A, Karunakar MA, Caron T, Sanders RW, Haidukewych GJ. Accuracy of reduction of ipsilateral femoral neck and shaft fractures: an analysis of various internal fixation strategies. J Orthop Trauma. 2009;23(4):249–53.
Oh CW, Oh JK, Park BC, et al. Retrograde nailing with subsequent screw fixation for ipsilateral femoral shaft and neck fractures. Arch Orthop Trauma Surg. 2006;126(7):448–53.
Kunapuli SC, et al. Biomechanical analysis of augmented plate fixation for the treatment of vertical shear femoral neck fractures. J Orthop Trauma. 2015;29(3):144–50.
Ricci WM, et al. Retrograde versus antegrade nailing of femoral shaft fractures. J Orthop Trauma. 2001;15(3):161–9.
Ostrum RF, et al. Ipsilateral proximal femur and shaft fractures treated with hip screws and a reamed retrograde intramedullary nail. Clin Orthop Relat Res. 2014;472(9):2751–8.
McConnell A, et al. The biomechanics of ipsilateral intertrochanteric and femoral shaft fractures: a comparison of 5 fracture fixation techniques. J Orthop Trauma. 2008;22(8):517–24.
Hung S-H, et al. Surgical treatment for ipsilateral fractures of the hip and femoral shaft. Injury. 2004;35(2):165–9.
Jain P, Maini L, Mishra P, Upadhyay A, Agarwal A. Cephalomedullary interlocked nail for ipsilateral hip and femoral shaft fractures. Injury. 2004;35(10):1031–8.
Bali K, et al. Cephalomedullary fixation for femoral neck/intertrochanteric and ipsilateral shaft fractures: surgical tips and pitfalls. Chin J Traumatol. 2013;16(1):40–5.
Adil A, Calder M, Hanson C, Norris B. How accurate is intra-operative fluoroscopy in gauging femoral anteversion? In: Mid-America Orthopaedic Association 35th annual meeting to be held April 19–23, 2017, at the Omni Amelia Island Plantation at Amelia Island, FL.
McFerran MA, Johnson KD. Intramedullary nailing of acute femoral shaft fractures without a fracture table: technique of using a femoral distractor. J Orthop Trauma. 1992;6(3):271–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Nollin, Z., Norris, B. (2020). Complex Bifocal Femoral Fractures. In: Giannoudis, P. (eds) Fracture Reduction and Fixation Techniques. Springer, Cham. https://doi.org/10.1007/978-3-030-24608-2_18
Download citation
DOI: https://doi.org/10.1007/978-3-030-24608-2_18
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-24607-5
Online ISBN: 978-3-030-24608-2
eBook Packages: MedicineMedicine (R0)