
Abstract
Molecular imaging such as positron emission tomography (PET) has been widely used in clinical oncology. Currently, F18-labeled fluorodeoxyglucose (18F-FDG.) PET/CT is accounted for the majority of all molecular imaging procedures. Accurate and reliable imaging studies are needed to proper stage cancer patients for treatment plans and to provide imaging parameters and biomarkers for optimal assessment of therapeutic response. Immunotherapy and targeted therapies have become the standard of practice for oncology treatments. Molecular imaging such as PET is likely to play an even greater role in the treatment selection and monitoring treatment response. Success of FDG PET is also recognized with certain limitations. Special attention has been devoted to the development of new tracers for better evaluation of tumor burden and immunotherapy response. In this chapter, we will outline the clinical utility of FDG PET (PET/CT) and provide a brief discussion of new radiotracers for renal cell carcinoma (RCC).
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Molecular imaging such as positron emission tomography (PET) has been widely used in clinical oncology. Currently, F18-labeled fluorodeoxyglucose (18F-FDG) PET/CT is accounted for the majority of all molecular imaging procedures. Accurate and reliable imaging studies are needed to proper stage cancer patients for treatment plans and to provide imaging parameters and biomarkers for optimal assessment of therapeutic response. Immunotherapy and targeted therapies have become the standard of practice for oncology treatments. Molecular imaging such as PET is likely to play an even greater role in the treatment selection and monitoring treatment response. Success of FDG PET is also recognized with certain limitations. Special attention has been devoted to the development of new tracers for better evaluation of tumor burden and immunotherapy response. In this chapter, we will outline the clinical utility of FDG PET (PET/CT) and provide a brief discussion of new radiotracers for renal cell carcinoma (RCC).
Renal cell carcinoma (RCC) accounts for about 3% of all adult cancers and 85% to 90% of all primary renal tumors. It is the seventh most common cancer in men and the ninth most common in women. The incidence of RCC is rising over time, partially attributable to the success of modern imaging technologies. Choudhary and colleagues estimated 50–60% of RCCs are found incidentally when diagnostic imaging is performed for an unrelated indication [1]. Characterization of a small renal mass can be done through tissue biopsy, which is invasive with known procedural complications, potential sampling errors, and concern of track metastasis. It is not commonly performed due to inaccuracy and ineffectiveness in clinical management. Non-invasive imaging modalities are useful in diagnosing, staging, and monitoring therapy response. To date, the role of FDG PET in the initial detection and diagnosis of RCC is still limited, controversial, and discordant. It is not recommended by NCCN guidelines. However, FDG PET seems to show some promise for the detection of distant metastases and local recurrence, and may be complementary to other cross-sectional imaging techniques. Semi-quantitative FDG PET/CT imaging may be helpful to predict tumor differentiation and prognosis. Immunotherapy with checkpoint inhibition has revolutionized the treatment of many cancers. Standard criteria for response assessment of immunotherapy are limited due to delayed response and initial pseudoprogression occurring in some patients. Few data are available using FDG PET/CT for the assessment of immunotherapy response for mRCC. Alternative targeted therapies for mRCC such as tyrosine kinase inhibitors (TKIs) are aimed at specific biologic molecules or processes to modify response or signal transduction. These drugs act as a cytostatic and inhibit growth rather than induce tumor regression. Conventional imaging techniques such as CT and MRI are size based and are not optimal in evaluating early changes after therapy. Molecular imaging has become more important in evaluating response for these cytostatic agents. The change in FDG uptake on PET scans before and after therapy is a strong indicator of biological response to TKIs.
In this chapter, we will examine the current application of FDG PET (PET/CT) for detecting primary RCC, locoregional metastasis evaluation, and distant metastasis assessment including liver, lung, and bone. We will also discuss the prognostic value of FDG PET/CT and the utility of FDG PET/CT for monitoring therapeutic response for mRCC.
Primary Renal Cell Carcinoma Diagnosis
Kidney cancer used to be considered a single disease many years ago. It is now known that renal cell carcinoma has different histological patterns and variable clinical courses that appear to respond differently to therapy [2]. The Heidelberg classification identifies five distinct malignant subtypes: clear cell, papillary, chromophobe, collecting duct, and RCC unclassified. Benign tumors have been subclassified into metanephric adenoma and adenofibroma, papillary renal cell adenoma, and renal oncocytoma [3]. Approximately 54% of renal masses are more aggressive clear cell carcinoma [2].
The initial diagnosis of a renal mass is usually made with ultrasound, CT, or MRI. Most cases are discovered incidentally during procedures for other indications [4]. CT is currently the imaging modality of choice to stage and detect metastasis in patients with RCC. These are essential for prognostic evaluation and surgical planning. Surgical resection by either partial or radical nephrectomy remains the standard of care for the localized disease.
FDG PET provides unique information about molecular pathways of disease. It has gained increasing acceptance for the diagnosis of cancer. Early studies using FDG PET reported a broad range of accuracy for detecting primary RCC. Ramdave et al. [5] studied 17 patients with known or suspected primary tumors and found true positive in 15, one true negative, and one false negative. The accuracy of FDG PET and CT was identical (94%). Similar results were also reported by Goldberg et al. [6]. Two other studies [7, 8] with larger sample of 53 and 66 patients showed different results. Aide et al. [7] reported a sensitivity, specificity, and accuracy of 47%, 80%, and 51%, respectively. Kang et al. [8] reported a sensitivity of 60% and a specificity of 100% for PET versus 91.7% sensitivity and 100% specificity for CT. Kang and colleagues concluded that the role of FDG PET in the detection of primary RCC is limited by low sensitivity. But the superior specificity of the PET may have a complementary role in equivocal cases on conventional imaging [8]. Several factors may explain the large ranges of variation of sensitivity. First, due to the heterogeneity of RCC, some have low FDG uptake due to low glucose transporter-1 expression [9]. In a study with 44 primary clear cell RCC, SUVmax (maximum standardized uptake value) ranges from 2.5 to 18.4, with average SUVmax 6.8 [10]. Second, the kidneys and collecting system are the route for radiotracer FDG excretion; this makes the diagnosis of small parenchymal mass difficult, even with hydration and diuretics [11]. Third, due to the limited resolution and the lack of anatomic (CT) correlation of old generation non-hybrid PET-only scanners, small lesions are very difficult to detect. The main disadvantage of FDG PET for RCC is the relatively high false-negative results. Another drawback of the FDG PET is the lower spatial resolution of PET images when compared to a CT scanner. There is known false-positive uptake in infection and inflammation for PET as well. It is worth noting that most articles published regarding RCC were based on PET-only scanners, which may lower the sensitivity and specificity by about 5–10%. The newer generation of hybrid PET/CT scanners with improved resolution has markedly improved the localization of lesions and diagnostic accuracy compared to either CT or PET stand-alone applications. A more recent study with FDG PET/CT by Kayani et al. detected 41/43 of primary RCC with the smallest tumor measuring less than 2.5 cm [10].
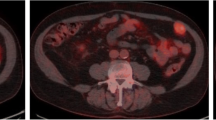
There is limited data regarding the ability to predict the histological diagnosis based on anatomic imaging findings [12]. Clear cell RCC is the most common type of renal malignancy. It can be hypodense, isodense, or hyperdense on pre-contrast CT studies. Post-contrast CT usually enhances significantly and can be heterogeneous due to necrosis [13]. No correlation of FDG uptake has been found between benign and malignant renal tumors. Most of the clear cell RCC demonstrate increased FDG uptake above the background renal parenchyma activity (Fig. 6.1). SUVmax (maximum standardized uptake value) has been reported ranging from 2.5 to 18.4 with an average of 6.5 [10].

Clear cell renal carcinoma. (a) Non-contrast CT shows a 5-cm right renal mass. (b) FDG PET demonstrates heterogeneous increased uptake in right renal mass. SUVmax 5.7. (c) Fused PET/CT image
Oncocytoma is considered a benign tumor. On unenhanced CT, it usually appears isodense or hypodense to the renal parenchyma and shows enhancement on post-IV contrast CT images. On PET, oncocytoma normally shows no appreciable FDG uptake as previously reported [14]. However, a case report described intense uptake in a renal oncocytoma [15]. A typical appearance of oncocytoma is shown in Fig. 6.2.

Oncocytoma. (a) CT with IV contrast shows a well-defined 5-cm mass with mild heterogeneous enhancement. (b) FDG PET shows mild increased uptake. SUVmax 2.9. (c) Fused PET/CT image
Angiomyolipoma is the most common benign tumor of the kidney. These lesions characteristically contain variable amounts of abnormal blood vessels, adipose tissue, and smooth muscle elements. The majority of angiomyolipomas can be accurately diagnosed on unenhanced CT as the lesions contain macroscopic fat (Fig. 6.3). There is limited literature on the role of FDG PET in the diagnosis of angiomyolipoma. Kochhar et al. [14] showed a renal angiomyolipoma without significant FDG uptake similar to our case in Fig. 6.3.

Angiomyolipoma of the kidney. (a) FDG PET shows focal mild uptake equal to or less than background renal parenchymal activity. SUVmax 1.9. (b) A well-marginated tumor with fatty attenuation seen on CT scan (arrow), highly suggestive of angiomyolipoma. (c) Fused PET/CT image
Locoregional Metastasis
Approximately 18% of patients with RCC have metastasis at the time of diagnosis [16]. CT and MRI are currently the study of choice to provide important information about tumor extension, vascular invasion, and regional metastasis. MRI has a special role to assess thrombus extension. Lymphadenopathy remains a major challenge for cross-sectional imaging. Current cross-sectional imaging criteria for suspicious lymph nodes include a short-axis diameter of 1 cm or more and loss of kidney shape and fatty hilum. Yet, some of the enlarged lymph nodes were related to hyperplastic and inflammatory change. FDG PET provides an alternative to contrast-enhanced CT by showing the metabolic activity of the disease. In RCC, both CT and PET data for local extension and regional nodal metastases are limited at the current time and believed to be similar [17].
FDG PET helps detect small metastatic nodes (Fig. 6.4). Kang et al. [8] reported 75% sensitivity and 100% specificity for retroperitoneal lymph node metastases and/or local recurrence by PET while abdominal CT showed 92.6% sensitivity and 98.1% specificity. Aide et al. [7] reported two patients with local nodal metastasis. FDG PET detected one of them; with IV contrast, CT correctly identified both. Kocher et al. [18] compared the results of FDG PET with histology in patients with suspected RCC. They found true regional lymph node metastasis in three patients and true negative in seven. Ramdave et al. [5] reported two cases of locoregional lymph node metastasis detected on FDG PET but not on CT.

Papillary renal cell carcinoma with local small nodal metastasis and tumor invading renal vein and IVC. (a) Staging FDG PET/CT demonstrates a large left renal mass and a 10-mm left para-aortic node (arrow) on non-contrast CT. (b) There is a markedly dilated left renal vein and IVC (arrows). (c) Fused FDG PET/CT images demonstrate heterogeneous uptake in the left renal mass, SUVmax 11, and corresponding uptake in a10-mm left para-aortic lymph node (arrow), suggesting metastatic disease. (d) There is intense FDG uptake in left renal vein and IVC (arrows), consistent with tumor extension
Although some publications have suggested that only tumor and infected thrombi show increased FDG uptake, a few reports showed that bland thrombus may have this appearance as well, a finding consistent with the acute inflammatory phase of aseptic deep venous thrombosis [19]. It seems that FDG PET is not useful in recognizing the cause of the thrombus because FDG uptake relies on the degree of reactive inflammation, which is variable and does not correlate with bland or tumor thrombus. However, there is generally accepted consensus that tumor thrombi have higher uptake than bland thrombus. A case with tumor thrombosis is shown in Fig. 6.4.
The incidence of local recurrence ranges from 1.8% to 27% after nephrectomy [20]. CT interpretation of the renal bed is difficult because of migration of the adjacent normal organs into the renal fossa, postoperative scar, and artifacts from surgical clips. In addition, patients may develop renal failure after nephrectomy which makes IV contrast injection relatively contraindicated. The metabolic activity of tumor is not altered by these factors. Therefore, FDG PET may be superior for evaluation of renal bed recurrence (Fig. 6.5). Ramdave et al. [5] showed that in the eight patients referred for this condition, PET was able to clearly differentiate tumor recurrence from fibrosis or necrosis. The diagnostic accuracy of FDG PET was calculated to be 100%. In comparison, the diagnostic accuracy of CT was 88%.

Chromophobe renal cell cancer with local recurrence. (a) Re-staging FDG PET/CT demonstrates a left retroperitoneal soft-tissue mass on non-contrast CT, question of post-surgical change vs local recurrence. (b) FDG PET demonstrates focally increased uptake, SUVmax 2.5, consistent with recurrent disease. (c) Fused FDG PET/CT image
Distant Metastasis
FDG PET/CT is very useful in evaluating distant metastases , partially attributable to the length (routine skull base to mid thigh) of the scan. It has shown promising results with RCC, with sensitivity range from 60% to 100% and the specificity close to 100% for the majority of cases [7, 17, 21,22,23,24,25]. Majhail et al. reported two cases of unsuspected distant metastasis detected by FDG PET not seen by CT in 17 patients evaluated for primary RCC [21]. In another study [26], FDG PET detected 77/112 of the metastatic lesions. Of those, 32 lesions had not been detected by any other anatomic imaging. The results of CT and FDG PET for detecting distant metastases from RCC were comparable, with sensitivities of 70% and 69%, respectively. Safaei et al. [27] reported a study of 20 patients with 25 lesions biopsied. FDG PET accurately identified 21/25 metastases and demonstrated a sensitivity of 87% and a specificity of 100%. Park et al. [17] evaluated FDG PET/CT for the postoperative surveillance of advanced RCC and found that it has 89.5% sensitivity, 83.3% specificity, 77.3% PPV, 92.6% NPV, and 85.7% accuracy in detecting local recurrent and distant metastasis. A study by Aide et al. [7] showed no metastases detected by CT that were missed by FDG PET. In fact, FDG PET was able to detect additional metastatic sites, leading to better accuracy compared with CT.
Liver Metastasis
Liver is the third most common site of metastasis for RCC after lung and bone and accounts for 15–20% of metastasis in RCC [28, 29]. Liver metastasis is associated with poor prognosis [30]. CT is the mainstay of imaging in the detection of intra-abdominal metastases. On CT, liver metastases can appear as ill-defined low attenuation lesions that may show peripheral enhancement or appear as hypervascular masses with or without central necrosis [31]. On a non-IV CT contrast FDG PET/CT scan, lesions on the CT component can be subtle. In general, there is high target to background ratio of uptake seen on FDG PET, which makes it easier to detect (Fig. 6.6). Study by Kang et al. [8] showed FDG PET has a sensitivity of 61.5% and a specificity of 100% for liver metastases. In contrast, CT has a sensitivity of 76.9% and a specificity of 94.1%. FDG PET detected 2/13 metastases that were negative on CT. In the study by Park et al. [17], FDG PET/CT has a sensitivity of 100% for liver metastasis.

Clear cell renal cancer with liver metastases . (a) CT shows a large right renal mass and subtle liver lesions (arrows). (b) FDG PET shows intense heterogeneous uptake in the right renal mass and clearly multiple foci of liver uptake (arrows). (c) Fused FDG PET/CT
Lung Metastasis
Lung is the most common site of mRCC and accounts for 50–60% of metastasis [28, 29]. Patients with lung-only metastases have a better survival rate than patients with other sites of metastases [30]. Pulmonary metastases usually appear as well-defined round or ovoid nodules on both chest radiography and CT. They can be solitary or multiple and typically range in size from 0.5 to 2 cm in diameter. They are one of the well-known causes of “cannonball” metastases [31]. CT with IV contrast is the current study of choice to evaluate lung metastases with high sensitivity. However, CT has limitation due to its low specificity to differentiate benign from malignant nodules. FDG PET assesses the metabolic process of the lesions and is useful in evaluating malignant potential. A large study of 585 patients by Bryant and colleagues showed the higher the SUV, the more likelihood of malignancy [32]. Fortes et al. [33] evaluated 83 patients with metastatic pulmonary nodules from different primaries and found that FDG PET is positive in only 67.5% of them. Nodule size and grade affect the sensitivity of FDG PET. For nodules ranging from 1 mm to 5 mm, the sensitivity of FDG PET was 23.5% (4/17); however, for nodules greater than 25 mm in diameter, the sensitivity of FDG PET was 88.5% (23/26).
With FDG PET, Majhail et al. [21] reported a sensitivity of 63.2% and 100% PPV in detecting pulmonary metastasis from RCC. The mean size of lung metastases in patients with true-positive FDG PET was 2.0 cm (95% CI, 1.3 to 2.7 cm) compared with 0.8 cm (95% CI, 0.5 to 1.2 cm) in patients with false-negative FDG PET.
A dual modality hybrid PET/CT scanner takes advantage of the high sensitivity from CT and the greater specificity of FDG PET which results in increasing accuracy as compared to either modality alone. Small pulmonary metastasis from RCC even without significant metabolic activity can be seen by CT (Fig. 6.7). A pulmonary nodule with corresponding FDG uptake is highly suspicious for metastasis in a patient with history of RCC (Fig. 6.8). Due to overlapping FDG uptake between inflammatory cells and cancer cells, false-positive metastasis is not uncommonly seen on FDG PET/CT (Fig. 6.9).

Clear cell renal cancer with lung metastasis . (a) CT component of FDG PET/CT scan shows a 2-cm solitary right lower lobe pulmonary nodule. (b) FDG PET demonstrates intense uptake. SUVmax 6.4. (c) Fused FDG PET/CT

Metabolic negative lung metastases from clear cell renal cancer. FDG PET/CT in a 63-year-old female with clear cell renal cancer and biopsy-proven pulmonary metastases. (a) Multiple lung nodules, largest measuring 10 mm (arrow) on CT. (b) No significant FDG uptake corresponding to these small nodules on PET. (c) Fused FDG PET/CT

False-positive lung metastasis from clear cell renal carcinoma. (a) CT component shows a large lung nodule, measuring 2.7×1.7 cm (arrow). (b) FDG PET demonstrates increased uptake corresponding to the large nodule, SUVmax 2.7. (c) Fused FDG PET/CT. Biopsy of this nodule shows inflammation and necrotic tissue
Bone Metastasis
Osseous metastasis accounts for 30–40% of distance metastasis in RCC [34]. Bone metastases classically appear as large expansile lytic lesions on plain radiography, most commonly in the axial skeleton [31]. Contrast-enhanced CT shows bone destruction with or without the presence of an enhancing soft-tissue mass. Bone scan is not routinely performed for RCC patients due to the mainly lytic nature of the bone metastasis, which is commonly negative in conventional bone scan. The general consensus is to order a bone scan only for patients with symptomatic bone pain and elevated serum alkaline phosphatase [27, 35].
FDG PET has been reported to be very accurate to stage bone metastasis in breast and lung cancers [36, 37]. FDG PET may offer improved specificity over bone scintigraphy in the detection of bone metastases (Fig. 6.10). Another advantage of PET over bone scan is the evaluation of both bone and soft tissue in one setting. Solitary bone metastasis from RCC is not uncommon, and a subtle bone lesion is not easily seen on CT scan (Fig. 6.11). Wu et al. [38] showed that for detecting bone metastasis, FDG PET had both sensitivity and accuracy of 100% compared with 77.5% and 59.6%, respectively, for bone scintigraphy. Kang et al. [8] showed that positive predictive value and negative predictive value for bone metastases were 99% and 93.2%, respectively, and indicate that FDG PET is the most sensitive test for imaging bone metastasis of RCC.

Multiple bone metastases from clear cell renal carcinoma. (a, b) Re-staging scan demonstrates destructive and lytic bone lesions on CT component (arrows). (c, d) PET/CT fused images demonstrate moderate increased uptake corresponding to these bone lesions

Solitary bone metastasis from clear cell renal carcinoma. (a) Re-staging FDG PET/CT in a 63-year-old male with clear cell renal carcinoma. PET demonstrates a focal moderate uptake in the right humerus. (b) On the corresponding CT, there is an easy to miss lesion with subtle cortex thinning. (c) Fused image clearly demonstrates abnormal uptake in the bone and marrow. (d) Follow-up plain film shows lytic lesion in the right humerus
Recently a study has demonstrated that NaF-18 PET is more accurate than 99mTc-diphosphonate SPECT for identifying both malignant and benign lesions of the skeleton [39]. Combining the NaF-18 PET with CT using a PET/CT scanner can improve the specificity and overall accuracy of detecting skeletal metastasis.
Surveillance
Chae et al. found that after resection of RCC, the mean time of tumor recurrence was 17 months, and 83% of recurrence occurred within 2 years [29]. Thus, they recommend follow-up imaging should be performed intensively the first 2 years after surgery. Most guidelines use anatomical and conventional imaging to monitor relapse and recurrence. FDG PET has been shown to identify relapse and/or recurrence more readily than conventional imaging with higher sensitivity and specificity [17]. One advantage of FDG PET/CT imaging is that IV contrast is not essential to perform the study, thus avoiding potential renal damage, which is very important for the renal preservation of RCC patients. Nakatani and coworkers [40] reviewed 28 scans in 23 patients who had undergone FDG PET scans after surgery. They correlated the FDG PET findings with other imaging and histology or by clinical follow-up at least 6 months and reported overall sensitivity, specificity, and diagnostic accuracy of 81%, 71%, and 79%, respectively. FDG PET correctly detected local recurrence and metastases in all cases in the peritoneum, bone, muscle, and adrenal gland. Their experience suggested FDG PET would be useful for postoperative surveillance in patients with RCC.
Prognostic Values of FDG PET for RCC
A prognostic model has been developed by Motzer et al. [41]. Patients were categorized into favorable, intermediate, or poor prognostic groups based on five risk factors: Karnofsky performance status, elevated lactate dehydrogenase (> 1.5 times the upper limit of normal), low hemoglobin (less than normal), high corrected calcium, and absence of prior nephrectomy. Patients with no risk factors (favorable risk) had a median survival of 20 months; with one to two risk factors (intermediate risk), 10 months; and with three or more risk factors (poor risk), 4 months. Furthermore, Motzer et al. [42] performed a retrospective study to identify prognostic factors for survival in previously treated patients with advanced RCC. They found risk factors for shorter survival were low Karnofsky performance status, low hemoglobin level, and high corrected serum calcium. The median time to death in patients with zero risk factors was 22 months. The median survival in patients with one of these prognostic factors was 11.9 months. Patients with two or three risk factors had a median survival of 5.4 months.
Studies have shown the metabolic tumor burden (MTB) and/or metabolic tumor volume (MTV) on FDG PET/CT is an independent prognostic factor in lung, head and neck, and esophageal cancers [43,44,45]. Other studies showed that SUVmax (maximum standardized uptake value) of FDG predicts prognosis in various cancers [46,47,48]. The role of FDG uptake such as SUVmax or MTB as a prognostic factor has not been fully established in RCC, but it is generally accepted that a more aggressive tumor has a higher SUV. One study showed that RCC patients with SUVmax equal or above 8.8 demonstrated poor prognosis [49]. Kayani et al. [10] showed a SUVmax of 7.1 was the most significant level to predict overall survival. In another study, Revheim et al. [50] found that patients with relatively low FDG uptake before treatment (defined as a SUVmax <5) had significantly longer progression-free survival than those with relatively high initial 18F-FDG uptake (SUVmax >5). Patients with low FDG uptake in their metastatic lesions are favorable for longer survival (Fig. 6.12). These findings suggest that SUVmax should be considered as a criterion to incorporate in future prognostic models.

Low FDG uptake in metastatic mRCC lesions demonstrates long-term survival. This 75-year-old male was diagnosed with clear cell renal carcinoma in 2001 and developed a left lower lobe nodule (a). FDG PET/CT showed minimal uptake. He underwent wedge resection of this nodule which was later confirmed as metastatic renal cell carcinoma. Subsequently, the patient developed multiple new low FDG avid metastases. He survived more than 10 years after the initial diagnosis of mRCC. The most recent FDG PET/CT showed a lytic bone lesion in the left scapula with mild FDG uptake (b)
Monitoring Therapeutic Response
Immunotherapy has become a cornerstone treatment for mRCC. Based on the CheckMate-214 trial [51], the European Association of Urology has recommended the combination of two immune checkpoint inhibitors ipilimumab and nivolumab as the first-line therapy for mRCC [52]. Conventional standard criteria for response assessment are not suitable to immunotherapy based on the fact that early pseudoprogression of existing lesions and small new lesions can occur in these late responders [53]. Therefore, immune-related response criteria were proposed by Wolchok et al. [53]. It is hypothesized that the initial pseudoprogression in some patients treated with immunotherapy is due to inflammatory cell infiltrates. Given that both cancer and immune infiltrates can be FDG avid, it is a challenge for FDG PET/CT to differentiate cancer progression with pseudoprogression. Several studies have been conducted to explore the role of non-FDG radiotracers, the “immuno-PET” for the evaluation of immunotherapy [54, 55]. Nevertheless, a negative FDG PET/CT after immunotherapy indicates good response to therapy (Fig. 6.13).

Monitoring of immunotherapy response by FDG PET/CT. A 75-year-old male presented with a large left renal clear cell carcinoma with extensive metastasis to bilateral adrenal, right lung, right pleura, and bone with negative PD-1 expression (a). He was treated with combined checkpoint inhibitors (Nivo + Ipi). After 4 cycles of therapy, restaging FDG PET/CT showed dramatic response to therapy (b). Follow-up scan demonstrated continued treatment response of metastatic disease. Worsening of uptake in the primary left renal lesion may represent pseudoprogression (c)
Alternative therapies are also used for the treatment of mRCC. These include TKIs such as sorafenib and sunitinib, inhibitors of mammalian target of rapamycin (mTOR) such as temsirolimus and everolimus, and other biologic agents such as bevacizumab. Currently, TKIs are still agents of choice for favorable-risk patients with mRCC [52]. These agents block cell signaling through various mechanisms and demonstrate better outcomes in patients with advanced clear cell RCC compared with standard therapies [19, 56].
Most and near all of these new agents can induce stabilization of RCC. A decrease in primary tumor diameter >30% while on targeted therapy is rare [57]. Since these therapies induce tumor necrosis with little tumor shrinkage, an unchanged residual mass does not necessary imply poor therapeutic responses. This makes anatomic imaging less suitable for monitoring treatment response for mRCC. In addition, differentiation between vital tumor and fibrosis or necrosis is difficult using anatomic imaging. Thus, molecular imaging such as FDG PET can be an attractive alternative to morphological imaging for this purpose. The new RECIST 1.1 now adds functional imaging in the response assessment [58, 59]. Data is now available on the monitoring of the therapeutic response of mRCC using FDG PET and FDG PET/CT [60,61,62]. A recent study [50] demonstrated that in patients with metastatic RCC, a high baseline FDG uptake indicates aggressive disease, and patients with a partial metabolic response or stable metabolic disease after two courses of sunitinib had improved prognosis as compared with those with progressive metabolic disease. They concluded that the inclusion of the PET results seems to improve the clinical counseling of patients with advanced disease.
Early metabolic response monitoring is possible with molecular imaging since the signal change at the cellular level takes quite some time to translate into size change (Fig. 6.14). Interestingly, in a multicenter phase II study, Kayani et al. [10] found that after 4 weeks of sunitinib, metabolic response occurred in 24/42 (57%) patients, but this did not correlate with progression-free survival (PFS) or overall survival (OS). After 16 weeks of treatment, disease progression on FDG PET/CT occurred in 28% of patients which correlated with a decreased OS and PFS.

Good response to therapy. FDG PET/CT in a 61-year-old male with bilateral renal cell cancer and liver metastasis. Top row: (a) Pre-therapy staging scan shows large focus of abnormal uptake in the right hepatic lobe (arrow). SUVmax 6.5. (b) Subtle hypodense lesion noted on non-contrast CT. (c) Fused PET/CT image. Bottom row: (d) 6 months after sorafenib treatment, there is marked improvement of uptake in liver metastasis. (e) Large lesion in the liver is now easily seen on CT with contrast. (f) Fused PET/CT image. Patient’s disease is stable with sorafenib treatment 4 years after initial diagnosis
FDG PET might be useful to identify nonresponding patients early in the treatment phase of TKIs (Fig. 6.15). This can guide a personalized treatment plan and avoid unnecessary therapy; the potential benefits to patients, the medical community, and the economy could be enormous.

Progression of metastatic disease. FDG PET/CT scans in a 70-year-old male with metastatic clear cell renal cancer. (a) Pre-therapy FDG PET/CT scan shows disease in peri-spinal soft tissue and left thigh (arrows). There is post-surgical/radiation uptake in right humeral metastasis. (b) Post-therapy with sunitinib, FDG PET/CT scan shows interval increased in size and intensity of FDG uptake in peri-spinal mass and left thigh soft-tissue mass (arrows). There are multiple new pulmonary and mediastinal metastases, indicating progression of the disease
Influence on Management
It is very important to know whether FDG PET scan has an impact on patient management in terms of clinical decision making. Studies have shown that FDG PET altered the management of patients with mRCC. In one study [5], FDG PET was completed in 25 patients with known or suspected primary RCC and/or metastasis, and the results were compared to those that received conventional imaging techniques. Normally all patients would go to surgery post-conventional imaging, but PET scan altered the treatment plan for 6 (35%); 3 could be treated with partial nephrectomy rather than radical surgery, and 3 avoided surgery owing to confirmation of benign pathology or detection of unsuspected metastasis leading to systemic therapy. Similar results were reported by others as well [7, 8, 27, 35].
National Oncologic PET Registry (NOPR) conducted a large study to evaluate the impact of FDG PET on Medicare cancer patients. The results of the NOPR were published in several high impact journals through a peer review process [63,64,65]. The first paper was published in the Journal of Clinical Oncology in May 2008 with over 22,000 studies analyzed [63]. This large, prospective, nationally representative registry of elderly cancer patients found that physicians often change their intended management on the basis of PET scan results across the full spectrum of its potential uses. In this article, there were 1600 cases of kidney and other urinary tract cancer patients, which account for 7% of total cases. Overall, physicians changed their intended management in 36.5% (95% CI, 35.9 to 37.2) of cases after FDG PET scan.
Another article was published in the Journal of Nuclear Medicine by the same group at the end of 2008 with similar findings and more details [65]: including 895 cases for initial staging of RCC, with a 41.1% change in management; 979 cases for RCC restaging, with a 34.4% change in management; and 1003 cases for monitoring response, with a 32.4% change in management. Given the evidence-based large population study results, FDG PET was approved by CMS for virtually all cancer types as the initial treatment strategy in mid-2009.
Novel Tracers and Future
124I-cG250 for Clear Cell RCC
Preoperative identification of tumor type could have important implications for the treatment choice for RCC. Carbonic anhydrase IX (CA IX), a membrane protein over-expressed in clear cell RCC, was found in 94% of clear cell carcinomas, and decreased CA IX levels are independently associated with poor survival in advanced RCC [66]. G250, a monoclonal antibody to carbonic anhydrase IX (CA IX), has extreme high affinity binding to clear cell RCC with tumor uptake approaching 0.5% of injected dose per gram of tumor tissue [67]. G250 was originally labeled with 131I [68]. Later on, positron emitters such as 89Zr [69] and 124I were labeled to cG250 [70]. A chimeric form of the antibody (cG250) has been generated with a less immunogenic response. A study using 124I-cG250 to target clear cell RCC showed great results from the phase 1 trial. Divgi and his group [70] demonstrated that 124I-cG250 PET could accurately distinguish clear cell RCC histology from other renal lesions with a sensitivity of 94% and a specificity of 100%, indicating the potential clinical utility of this tracer in the non-invasive molecular evaluation and subtyping of RCC. A renal tumor with a positive 124I-cG250 scan is found to be almost 100% a clear cell type (Fig. 6.16), while a negative scan is suggestive of non-clear cell type with 90% accuracy (Figs. 6.17 and 6.18). A false-negative scan has been seen in tumor with extended necrosis and a small size (less than 1 cm). In addition, metastatic lesion(s) can also be seen on the scan with high confidence (Fig. 6.19).

Bilateral clear cell renal carcinoma. 124I-cG250 PET/CT in a 65-year-old male with bilateral renal masses. (a) Triphasic CT shows a 5-cm enhancing lesion in the right kidney and a 2-cm enhancing lesion in the left kidney (arrows). (b) 124I-cG250 PET shows intense uptake in both renal lesions, indicating clear cell renal carcinoma. (c) Fused PET/CT image

Papillary renal cell carcinoma. 124I-cG250 PET/CT scan in a 49-year-old female with right kidney mass. (a) Triphasic CT scan demonstrates a non-enhancing lesion in right lower pole (arrow), HU 41. (b) No significant 124I-cG250 uptake corresponding to this renal mass, suggesting non-clear cell renal tumor

Left renal oncocytoma. 124I-cG250 PET/CT scan in a 59-year-old male with a left renal mass. (a) Triphasic CT shows a 2-cm enhancing lesion (arrow), HU 120. (b) 124I-cG250 fused PET shows no significant corresponding uptake in the lesion, ruling out clear cell carcinoma

Bone metastasis from clear cell renal cancer detected by 124I-cG250. 124I-cG250 PET/CT scan in a 65-year-old male with bilateral clear cell renal carcinoma. (a) PET shows a focal abnormal uptake (arrow). (b) There is a small corresponding lytic bone lesion in T1 vertebral body on CT (arrow). (c) Fused PET/CT image
Based on this phase 1 result, a comprehensive and multicenter comparative study for pre-surgical detection of clear cell RCC using 124I radiolabeled cG250 antibody was performed and completed in late 2009, and the results of the trial were published in JCO in early 2013 [71]. 124I-cG250 may improve the decision making for RCC treatment. For example, due to high possibility of clear cell RCC identification, patients with positive scans might need more aggressive therapy. Patients with negative scans may be candidates for active surveillance. The detection of metastasis may alter the treatment management plan from surgery to systematic medical therapy. More research is needed to fully evaluate the potential of this tracer in the future.
Other Novel Tracers
There are many targets and/or disease control points for new tracer development. The ideal tracer should target a specific disease process to provide patients with optimal care. The common targets or disease control points include metabolism, proliferation, hypoxia, angiogenesis, and apoptosis. Metabolism has been extensively studied by FDG PET with adequate data, and is well incorporated into the daily practice of clinical oncology.
18F-labeled thymidine (FLT), an analog of the nucleic acid thymidine, is a tracer that evaluates cellular proliferation. In a recent study, 18F-FLT was used to characterize and quantify changes in RCC tumor proliferation during sunitinib exposure and temporary withdrawal [72]. Data regarding the clinical use of 18F-FLT in RCC is still limited.
Hypoxia is another phenomenon commonly studied with novel PET tracers and PET imaging. 18F-FMISO appears to be the most commonly used tracer for imaging hypoxia. In a study, 18F-FMISO was performed in 17 patients with presumed RCC and showed only minimal increased uptake in RCC compared to normal renal tissue [73]. The mean SUV for RCC was 1.3, while that in the normal contralateral kidney was 1.1. A more recent study [74] with 53 patients evaluated the relationship between initial hypoxia-induced metastasis and after 1 month of sunitinib treatment using FMISO-PET scans. They concluded that sunitinib reduced hypoxia in hypoxic metastases but did not induce significant hypoxia in non-hypoxic lesions.
18F-labeled choline has been used for PET imaging of other tumors [75,76,77,78] such as lung and prostate. Middendorp and coworkers [79] published their initial experience with 18F-fluoroethylcholine PET/CT in staging and monitoring therapy response of advanced renal cell carcinoma. 18F-fluoroethylcholine PET/CT detected 56% of mRCC lesions on the baseline scan. Further study, ideally in comparison with FDG PET, should be investigated.
Acetate is another compound of interest. 11C-acetate has shown increased uptake in primary RCC and metastasis [80] as well. But another study showed low uptake [81]. 11C-acetate has been used for early prediction of sunitinib response in metastatic RCC with some success [80]. The use of this agent is limited due to the short half-life of 11C (20 minutes) requiring the need for an on-site cyclotron or one very near to the imaging facility to produce. Recently available 18F-labeled acetate makes the delivery and commercialization of this tracer possible.
Conclusion
FDG PET offers limited advantage over conventional imaging in initial diagnosis of primary RCC. FDG PET is complementary to anatomic imaging in detecting locoregional and distant RCC metastasis. FDG PET/CT has the advantage of detecting small nodal metastasis and locoregional recurrent disease after nephrectomy. FDG PET/CT is the most accurate method used to study for bone metastasis from RCC.
Monitoring immunotherapy response of metastatic RCC by FDG PET/CT requires further studies to validate. FDG PET/CT has proven its usefulness in monitoring targeted therapies. These targeted therapeutic agents inhibit tumor growth rather than kill the tumor cells. This limits the use of conventional imaging modalities that are based solely on tumor size criteria. The information provided by molecular imaging such as maximum standardized uptake value (SUVmax) has shown to be an independent prognostic factor for RCC. SUVmax should be considered to be incorporated into future prognostic models.
There are limitations for FDG PET/CT as a diagnostic tool for RCC. New tracers focusing on disease processes such as hypoxia, angiogenesis, and apoptosis might be of value in RCC as well. Immuno-PET may help better assess the immunotherapy response. If we could find a specific tracer for each disease process, we might improve our patient care significantly and provide true individualized therapy for our patients.
References
Choudhary S, Sudarshan S, Choyke PL, Prasad SR. Renal cell carcinoma: recent advances in genetics and imaging. Semin Ultrasound CT MR. 2009;30(4):315–25.
Linehan WM, Walther MM, Zbar B. The genetic basis of cancer of the kidney. J Urol. 2003;170(6 Pt 1):2163–72.
Kovacs G, Akhtar M, Beckwith BJ, Burgert P, Cooper CS, Delahunt B, Eble JN, Fleming S, Ljungberg B, Medeiros J, et al. The Heidelberg classification of renal cell tumours. J Pathol. 1997;183:131–3.
Vasudevan A, Davies RJ, Shannon BA, Cohen RJ. Incidental renal tumours: the frequency of benign lesions and the role of preoperative core biopsy. BJU Int. 2006;97(5):946–9.
Ramdave S, Thomas GW, Berlangieri SU, Bolton DM, Davis I, Danguy HT, et al. Clinical role of F-18 fluorodeoxyglucose positron emission tomography for detection and management of renal cell carcinoma. J Urol. 2001;166(3):825–30.
Goldberg MA, Mayo-Smith WW, Papanicolaou N, Fischman AJ, Lee MJ. FDG PET characterization of renal masses: preliminary experience. Clin Radiol. 1997;52(7):510–5.
Aide N, Cappele O, Bottet P, Bensadoun H, Regeasse A, Comoz F, et al. Efficiency of [(18)F]FDG PET in characterising renal cancer and detecting distant metastases: a comparison with CT. Eur J Nucl Med Mol Imaging. 2003;30(9):1236–45.
Kang DE, White RL Jr, Zuger JH, Sasser HC, Teigland CM. Clinical use of fluorodeoxyglucose F 18 positron emission tomography for detection of renal cell carcinoma. J Urol. 2004;171(5):1806–9.
Lidgren A, Bergh A, Grankvist K, Rasmuson T, Ljungberg B. Glucose transporter-1 expression in renal cell carcinoma and its correlation with hypoxia inducible factor-1 alpha. BJU Int. 2008;101(4):480–4.
Kayani I, Avril N, Bomanji J, Chowdhury S, Rockall A, Sahdev A, Nathan P, Wilson P, Shamash J, Sharpe K, Lim L, Dickson J, Ell P, Reynolds A, Powles T. Clin Cancer Res. 2011;17(18):6021–8. Epub 2011 Jul 8.
Bouchelouche K, Oehr P. Recent developments in urologic oncology: positron emission tomography molecular imaging. Curr Opin Oncol. 2008;20(3):321–6.
Krajewski KM, Giardino AA, Zukotynski K, Van den Abbeele AD, Pedrosa I. Imaging in renal cell carcinoma. Hematol Oncol Clin North Am. 2011;25(4):687–715.
Zhang J, Lefkowitz RA, Ishill NM, Wang L, Moskowitz CS, Russo P, Eisenberg H, Hricak H. Solid renal cortical tumors: differentiation with CT. Radiology. 2007;244(2):494–504.
Kochhar R, Brown RK, Wong CO, Dunnick NR, Frey KA, Manoharan P. Role of FDG PET/CT in imaging of renal lesions. J Med Imaging Radiat Oncol. 2010;54(4):347–57.
Blake MA, McKernan M, Setty B, Fischman AJ, Mueller PR. Renal oncocytoma displaying intense activity on 18F-FDG PET. AJR Am J Roentgenol. 2006;186(1):269–70.
Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62(1):10–29.
Park JW, Jo MK, Lee HM. Significance of 18F-fluorodeoxyglucose positron-emission tomography/computed tomography for the postoperative surveillance of advanced renal cell carcinoma. BJU Int. 2009;103(5):615–9.
Kocher F, Grimmel S, Hautmann R, et al. Preoperative lymph node staging in patients with kidney and urinary bladder neoplasm. J Nucl Med Suppl. 1994;35:223.
Khosa F, Otero HJ, Prevedello LM, Rybicki FJ, Di Salvo DN. Imaging presentation of venous thrombosis in patients with cancer. AJR Am J Roentgenol. 2010;194(4):1099–108. Review.
Itano NB, Blute ML, Spotts B, Zincke H. Outcome of isolated renal cell carcinoma fossa recurrence after nephrectomy. J Urol. 2000;164:322–5.
Majhail NS, Urbain JL, Albani JM, Kanvinde MH, Rice TW, Novick AC, et al. F-18 fluorodeoxyglucose positron emission tomography in the evaluation of distant metastases from renal cell carcinoma. J Clin Oncol. 2003;21(21):3995–4000.
Schoder H, Larson SM. Positron emission tomography for prostate, bladder, and renal cancer. Semin Nucl Med. 2004;34(4):274–92.
Mueller-Lisse UG, Mueller-Lisse UL, Meindl T, Coppenrath E, Degenhart C, Graser A, et al. Staging of renal cell carcinoma. Eur Radiol. 2007;17(9):2268–77.
Hyodo T, Sugawara Y, Tsuda T, Yanagihara Y, Aoki K, Tanji N, et al. Widespread metastases from sarcomatoid renal cell carcinoma detected by (18)F-FDG positron emission tomography/computed tomography. Jpn J Radiol. 2009;27(2):111–4.
Kumar R, Shamim SA, Shandal V, Sharma P, Gadodia A, Malhotra A. FDG PET/CT in detection of adrenal metastasis in patients with renal cell carcinoma. Clin Nucl Med. 2011;36(7):513–7.
Brouwers AH, Dorr U, Lang O, et al. 131I-cG250 monoclonal antibody immunoscintigraphy versus [18F] FDG-PET imaging in patients with metastatic renal cell carcinoma: a comparative study. Nucl Med Commun. 2002;23:229–36.
Safaei A, Figlin R, Hoh CK, Silverman DH, Seltzer M, Phelps ME, et al. The usefulness of F-18 deoxyglucose whole-body positron emission tomography (PET) for re-staging of renal cell cancer. Clin Nephrol. 2002;57(1):56–62.
Eggener SE, Yossepowitch O, Pettus JA, Snyder ME, Motzer RJ, Russo P. Renal cell carcinoma recurrence after nephrectomy for localized disease: predicting survival from time of recurrence. J Clin Oncol. 2006;24:3101–6.
Chae EJ, Kim JK, Kim SH, Bae SJ, Cho KS. Renal cell carcinoma: analysis of postoperative recurrence patterns. Radiology. 2005;234:189–96.
Flanigan RC, Salmon SE, Blumenstein BA, et al. Nephrectomy followed by interferon alfa-2b compared with interferon alfa-2b alone for metastatic renal-cell cancer. N Engl J Med. 2001;345:1655–9.
Griffin N, Gore ME, Sohaib SA. Imaging in metastatic renal cell carcinoma. AJR Am J Roentgenol. 2007;189(2):360–70.
Bryant AS, Cerfolio RJ. The maximum standardized uptake values on integrated FDG-PET/CT is useful in differentiating benign from malignant pulmonary nodules. Ann Thorac Surg. 2006;82(3):1016–20.
Fortes DL, Allen MS, Lowe VJ, Shen KH, Wigle DA, Cassivi SD, et al. The sensitivity of 18F-fluorodeoxyglucose positron emission tomography in the evaluation of metastatic pulmonary nodules. Eur J Cardiothorac Surg. 2008;34(6):1223–7.
Kollender Y, Bickels J, Price WM, et al. Metastatic renal cell carcinoma of bone: indications and technique of surgical intervention. J Urol. 2000;164:1505–8.
Dilhuydy MS, Durieux A, Pariente A, de Clermont H, Pasticier G, Monteil J, et al. PET scans for decision-making in metastatic renal cell carcinoma: a single-institution evaluation. Oncology. 2006;70(5):339–44.
Cook GJ, Houston S, Rubens R, Maisey MN, Fogelman I. Detection of bone metastases in breast cancer by 18FDG PET: differing metabolic activity in osteoblastic and osteolytic lesion. J Clin Oncol. 1998;16:3375–9.
Bury T, Barreto A, Daenen F, Barthelemy N, Ghaye B, Rigo P. Fluorine-18 deoxyglucose positron emission tomography for the detection of bone metastases in patients with non-small cell lung cancer. Eur J Nucl Med. 1998;25:1244–7.
Wu HC, Yen RF, Shen YY, Kao CH, Lin CC, Lee CC. Comparing whole-body 18F-2-deoxyglucose positron emission tomography and technetium-99m methylene diphosphate bone scan to detect bone metastases in patients with renal cell carcinomas: a preliminary report. J Cancer Res Clin Oncol. 2002;128:503–6.
Grant FD, Fahey FH, Packard AB, Davis RT, Alavi A, Treves ST. Skeletal PET with 18F-fluoride: applying new technology to an old tracer. J Nucl Med. 2008;49(1):68–78.
Nakatani K, Nakamoto Y, Saga T, Higashi T, Togashi K. The potential clinical value of FDG-PET for recurrent renal cell carcinoma. Eur J Radiol. 2011;79(1):29–35.
Motzer RJ, Mazumdar M, Bacik J, Berg W, Amsterdam A, Ferrara J. Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. J Clin Oncol. 1999;17:2530–40.
Motzer RJ, Bacik J, Schwartz LH, Reuter V, Russo P, Marion S, et al. Prognostic factors for survival in previously treated patients with metastatic renal cell carcinoma. J Clin Oncol. 2004;22(3):454–63.
Zhu D, Ma T, Niu Z, Zheng J, Han A, Zhao S, et al. Prognostic significance of metabolic parameters measured by (18)F-fluorodeoxyglucose positron emission tomography/computed tomography in patients with small cell lung cancer. Lung Cancer. 2011;73:332–7.
Seol YM, Kwon BR, Song MK, Choi YJ, Shin HJ, Chung JS, et al. Measurement of tumor volume by PET to evaluate prognosis in patients with head and neck cancer treated by chemo-radiation therapy. Acta Oncol. 2010;49:201–8.
Hyun SH, Choi JY, Shim YM, Kim K, Lee SJ, Cho YS, et al. Prognostic value of metabolic tumor volume measured by 18F-fluorodeoxyglucose positron emission tomography in patients with esophageal carcinoma. Ann Surg Oncol. 2010;17:115–22.
Allal AS, Slosman DO, Kebdani T, Allaoua M, Lehmann W, Dulguerov P. Prediction of outcome in head-and-neck cancer patients using the standardized uptake value of 2-[18F]fluoro-2-deoxy-D-glucose. Int J Radiat Oncol Biol Phys. 2004;59:1295–3000.
Downey RJ, Akhurst T, Gonen M, Vincent A, Bains MS, Larson S, Rusch V. Preoperative F-18 fluorodeoxyglucose-positron emission tomography maximal standardized uptake value predicts survival after lung cancer resection. J Clin Oncol. 2004;22:3255–60.
Lee YY, Choi CH, Kim CJ, Kang H, Kim TJ, Lee JW, Lee JH, Bae DS, Kim BG. The prognostic significance of the SUVmax (maximum standardized uptake value for F-18 fluorodeoxyglucose) of the cervical tumor in PET imaging for early cervical cancer: preliminary results. Gynecol Oncol. 2009;115:65–8.
Namura K, Minamimoto R, Yao M, Makiyama K, Murakami T, Sano F, Hayashi N, Tateishi U, et al. Impact of maximum standardized uptake value (SUVmax) evaluated by 18-Fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography (18F-FDG-PET/CT) on survival for patients with advanced renal cell carcinoma: a preliminary report. BMC Cancer. 2010;10:667.
Revheim ME, Winge-Main AK, Hagen G, Fjeld JG, Fossa SD, Lilleby W. Combined positron emission tomography/computed tomography in sunitinib therapy assessment of patients with metastatic renal cell carcinoma. Clin Oncol (R Coll Radiol). 2011;23(5):339–43.
Escudier B, Tannir NM, McDermott DF, et al. CheckMate 214: efficacy 316 and safety of nivolumab plus ipilimumab vs sunitinib for treatment-naïve 317 advanced or metastatic renal cell carcinoma, including 318 IMDC risk and PD-L1 expression subgroups. Ann of Oncol. 2017;28(Suppl. 5):v605–49. LBA5, ESMO 319 2017.
Powles T, Albiges L, Staehler M, Bensalah K, Dabestani S, Giles RH, Hofmann F, Hora M, Kuczyk MA, Lam TB, Marconi L, Merseburger AS, Fernández-Pello S, Tahbaz R, Volpe A, Ljungberg B, Bex A. Updated European Association of Urology guidelines: recommendations for the treatment of first-line metastatic clear cell renal cancer. European Urol. 2018;73:311–5.
Wolchok JD, Hoos A, O'Day S, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009;15:7412–20.
Higashikawa K, Yagi K, Watanabe K, Kamino S, Ueda M, Hiromura M, Enomoto S. 64Cu-DOTA-anti-CTLA-4 mAb enabled PET visualization of CTLA-4 on the T-cell infiltrating tumor tissues. PLoS One. 2014;9:e109866.
Maute RL, Gordon SR, Mayer AT, McCracken MN, Natarajan A, Ring NG, Kimura R, Tsai JM, Manglik A, Kruse AC, et al. Engineering high-affinity PD-1 variants for optimized immunotherapy and immuno-PET imaging. Proc Natl Acad Sci U S A. 2015;112:E6506–14.
Murdoch D, Sager J. Will targeted therapy hold its promise? An evidence-based review. Curr Opin Oncol. 2008;20(1):104–11.
Abel EJ, Culp SH, Tannir NM, Matin SF, Tamboli P, Jonasch E, et al. Primary tumor response to targeted agents in patients with metastatic renal cell carcinoma. Eur Urol. 2011;59(1):10–5.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Schwartz LH, Bogaerts J, Ford R, Shankar L, Therasse P, Gwyther S, et al. Evaluation of lymph nodes with RECIST 1.1. Eur J Cancer. 2009;45(2):261–7.
Jennens RR, Rosenthal MA, Lindeman GJ, Michael M. Complete radiological and metabolic response of metastatic renal cell carcinoma to SU5416 (semaxanib) in a patient with probable von Hippel-Lindau syndrome. Urol Oncol. 2004;22(3):193–6.
Lyrdal D, Boijsen M, Suurkula M, Lundstam S, Stierner U. Evaluation of sorafenib treatment in metastatic renal cell carcinoma with 2-fluoro-2-deoxyglucose positron emission tomography and computed tomography. Nucl Med Commun. 2009;30(7):519–24.
Vercellino L, Bousquet G, Baillet G, Barre E, Mathieu O, Just PA, et al. 18F-FDG PET/CT imaging for an early assessment of response to sunitinib in metastatic renal carcinoma: preliminary study. Cancer Biother Radiopharm. 2009;24(1):137–44.
Hillner BE, Siegel BA, Liu D, Shields AF, Gareen IF, Hanna L, et al. Impact of positron emission tomography/computed tomography and positron emission tomography (PET) alone on expected management of patients with cancer: initial results from the National Oncologic PET registry. J Clin Oncol. 2008;26(13):2155–61.
Hillner BE, Siegel BA, Shields AF, Duan F, Gareen IF, Hanna L, et al. Impact of dedicated brain PET on intended patient management in participants of the national oncologic PET registry. Mol Imaging Biol. 2011;13(1):161–5.
Hillner BE, Siegel BA, Shields AF, Liu D, Gareen IF, Hunt E, et al. Relationship between cancer type and impact of PET and PET/CT on intended management: findings of the national oncologic PET registry. J Nucl Med. 2008;49(12):1928–35.
Bui MH, Seligson D, Han KR, et al. Carbonic anhydrase IX is an independent predictor of survival in advanced renal clear cell carcinoma: implications for prognosis and therapy. Clin Cancer Res. 2003;9:802–11.
Steffens MG, Boerman OC, Oosterwijk-Wakka JC, et al. Targeting of renal cell carcinoma with iodine-131-labeled chimeric monoclonal antibody G250. J Clin Oncol. 1997;15:1529–37.
Brouwers AH, Dorr U, Lang O, Boerman OC, Oyen WJ, Steffens MG, et al. 131 I-cG250 monoclonal antibody immunoscintigraphy versus [18 F]FDG-PET imaging in patients with metastatic renal cell carcinoma: a comparative study. Nucl Med Commun. 2002;23(3):229–36.
Brouwers A, Verel I, Van Eerd J, Visser G, Steffens M, Oosterwijk E, et al. PET radioimmunoscintigraphy of renal cell cancer using 89Zr-labeled cG250 monoclonal antibody in nude rats. Cancer Biother Radiopharm. 2004;19(2):155–63.
Divgi CR, Pandit-Taskar N, Jungbluth AA, Reuter VE, Gonen M, Ruan S, et al. Preoperative characterisation of clear-cell renal carcinoma using iodine-124-labelled antibody chimeric G250 (124I-cG250) and PET in patients with renal masses: a phase I trial. Lancet Oncol. 2007;8(4):304–10.
Divgi CR, Uzzo RG, Gatsonis C, Bartz R, Treutner S, Yu JQ, Chen D, Carrasquillo JA, Larson S, Bevan P, Russo P. Positron emission tomography/computed tomography identification of clear cell renal cell carcinoma: results from the REDECT trial. J Clin Oncol. 2013;31(2):187–94.
Liu G, Jeraj R, Vanderhoek M, Perlman S, Kolesar J, Harrison M, et al. Pharmacodynamic study using FLT PET/CT in patients with renal cell cancer and other solid malignancies treated with sunitinib malate. Clin Cancer Res. 2011;17(24):7634–44.
Lawrentschuk N, Poon AM, Foo SS, Putra LG, Murone C, Davis ID, et al. Assessing regional hypoxia in human renal tumours using 18F-fluoromisonidazole positron emission tomography. BJU Int. 2005;96(4):540–6.
Hugonnet F, Fournier L, Medioni J, Smadja C, Hindie E, Huchet V, et al. Metastatic renal cell carcinoma: relationship between initial metastasis hypoxia, change after 1 month's sunitinib, and therapeutic response: an 18F-fluoromisonidazole PET/CT study. J Nucl Med. 2011;52(7):1048–55.
Bansal A, Shuyan W, Hara T, Harris RA, Degrado TR. Biodisposition and metabolism of [(18)F]fluorocholine in 9L glioma cells and 9L glioma-bearing fisher rats. Eur J Nucl Med Mol Imaging. 2008;35(6):1192–203.
DeGrado TR, Coleman RE, Wang S, Baldwin SW, Orr MD, Robertson CN, et al. Synthesis and evaluation of 18F-labeled choline as an oncologic tracer for positron emission tomography: initial findings in prostate cancer. Cancer Res. 2001;61(1):110–7.
Pieterman RM, Que TH, Elsinga PH, Pruim J, van Putten JW, Willemsen AT, et al. Comparison of (11)C-choline and (18)F-FDG PET in primary diagnosis and staging of patients with thoracic cancer. J Nucl Med. 2002;43(2):167–72.
Schillaci O, Calabria F, Tavolozza M, Ciccio C, Carlani M, Caracciolo CR, et al. 18F-choline PET/CT physiological distribution and pitfalls in image interpretation: experience in 80 patients with prostate cancer. Nucl Med Commun. 2010;31(1):39–45.
Middendorp M, Maute L, Sauter B, Vogl TJ, Grunwald F. Initial experience with 18F-fluoroethylcholine PET/CT in staging and monitoring therapy response of advanced renal cell carcinoma. Ann Nucl Med. 2010;24(6):441–6.
Maleddu A, Pantaleo MA, Castellucci P, Astorino M, Nanni C, Nannini M, et al. 11C-acetate PET for early prediction of sunitinib response in metastatic renal cell carcinoma. Tumori. 2009;95(3):382–4.
Kotzerke J, Linne C, Meinhardt M, Steinbach J, Wirth M, Baretton G, et al. [1-(11)C]acetate uptake is not increased in renal cell carcinoma. Eur J Nucl Med Mol Imaging. 2007 Jun;34(6):884–8.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Yu, J.Q., Dou, Y. (2020). Molecular Imaging for Renal Cell Carcinoma. In: Libertino, J., Gee, J. (eds) Renal Cancer. Springer, Cham. https://doi.org/10.1007/978-3-030-24378-4_6
Download citation
DOI: https://doi.org/10.1007/978-3-030-24378-4_6
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-24377-7
Online ISBN: 978-3-030-24378-4
eBook Packages: MedicineMedicine (R0)