
Abstract
Young adults with long-term health conditions (LTHCs) are increasing due to improvements in care, therapy regimens and medical technology. In the UK, transition to adult services occurs at a stage when they are also learning self-management skills. For some, transfer from paediatric to adult care providers may result in a loss of psychosocial support. Higher mortality rates and lower access to healthcare are common in young adults aged between 18 and 25 years of age compared to adolescents (10–17 years) and those who are in the 26 to 30 year age group. Failure to provide attention to the complex balancing act between medication demands, hospital appointments, work and social activities, nutrition and key tasks of development (Walker-Harding et al. 2017) means young adults face significant challenges in the move to independent living.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Young adults with long-term health conditions (LTHCs) are increasing due to improvements in care, therapy regimens and medical technology. In the UK, transition to adult services occurs at a stage when they are also learning self-management skills. For some, transfer from paediatric to adult care providers may result in a loss of psychosocial support. Higher mortality rates and lower access to healthcare are common in young adults aged between 18 and 25 years of age compared to adolescents (10–17 years) and those who are in the 26 to 30 year age group. Failure to provide attention to the complex balancing act between medication demands, hospital appointments, work and social activities, nutrition and key tasks of development (Walker-Harding et al. 2017) means young adults face significant challenges in the move to independent living.
This chapter describes The Transforming Transition Programme (TTP), a UK nurse-led initiative to improve transition for young people with haemophilia. The development of the programme involved a review of current practices, collective agreement as to the outcomes that would be measured, and delivering and evaluating a patient-led development programme. The TTP demonstrated the developmental need for negotiation and change management skills in haemophilia nurses. The programme highlighted the importance of addressing the knowledge and skills necessary for self-management and living well with haemophilia to support the smooth transition between paediatric and adult services.
As a result of the programme, a ‘Transition Toolkit’ was created, offering nurses a number of resources that can be used with young people and to assist them with the evaluation of the transition process within their centre/network.
11.1 Introduction
Young adults with long-term health conditions (LTHCs) are increasing due to improvements in care, therapy regimens and medical technology (Nelson et al. 2012; Stoll et al. 2010). For young people with haemophilia in the UK, transition to adult services occurs at a stage when they are also learning self-management skills. For some transfer from paediatric to adult care providers may also result in a loss of psychosocial support (Pembroke and Dodgson 2018). A chronological boundary is often used to define the move between children’s and adult services based on the UK National Service Framework for children, young people and maternity services transition services which suggests paediatric services should retain responsibility for young people until their 16th birthday, if not till 18 years (Department of Health 2006).
In 1999, Scal et al. noted that the majority of transitional care models are hospital based, within disease specific specialist teams (Scal et al. 1999). Nearly two decades later little has changed. Sawyer and Aroni (2005: 406) state developmentally appropriate healthcare (DAH) is the ‘key principle underpinning the practice of adolescent medicine’ and argue the key component of ‘healthcare transition’ must be overarching framework of DAH where professionals understand and respond to biopsychosocial and developmental needs of young people providing individualised healthcare, health education and health promotion.
Adolescence is a unique and critical period of development. Specific intervention and prevention strategies may decrease threats to health and alter trajectories into emerging adulthood. During this developmental phase, young people move towards achieving goals, life responsibilities and independence. The neurobiology of the adolescent brain underpins the importance of peer acceptance and openness to social stimulation as well as risk-taking and reward-seeking behaviours that let young people try out different experiences, and develop self-determination and identity (Blakemore 2012). Self-care can be influenced by experimentation, attitudes and beliefs about the impact of illness on future choices where young people act in ways that appear to reflect a desire to wish their condition ‘away’ in their search for ‘normality’ (Dovey-Pearce and Christie 2013).
Higher mortality rates and lower access to healthcare are common in young adults, between 18 and 25 years of age compared to adolescents, 10–17 years and those who are in the 26–30 year age group. Failure to provide attention to the complex balancing act between medication demands, hospital appointments, work and social activities, nutrition and key tasks of development (Walker-Harding et al. 2017) means young adults face significant challenges in the move to independent living.
A focus on ‘organisational transfer’ alone results in the developmental needs of emerging young adults being overlooked (Rosen et al. 2003, Crowley et al. 2011). All adolescents should know well in advance that the location of their care will change and preparation for this should be embedded within a framework of quality adolescent healthcare.
A recent 5-year study of health service provision and healthcare outcomes for young people aged 14–18 with LTHCs (Colver et al. 2013; Merrick et al. 2015; Kmietowicz 2017) focused on three aspects of service provision:
-
Promoting young peoples’ confidence in their ability to manage their health and wellbeing,
-
Supporting appropriate parental involvement (i.e. meeting the needs of both the parent and young people (YP)),
-
Facilitating a meeting with the adult team before transfer between services.
Haemophilia services in the UK are provided in paediatric and combined (paediatric and adult) treatment centres; there is no national guidance about how or when transition planning should be implemented. This lack of guidance has resulted in disjointed services with varying outcomes, which miss some of the basic principles of adolescent transition:
-
Developmentally appropriate care
-
Enhance patient autonomy
-
Collaboration between healthcare providers
-
Instruction on skills of negotiation
-
Gradation of responsibility to the adolescent
-
Provision of community resources
-
Designated professional with responsibility for transition
-
A portable summary of healthcare needs
-
Current transition plan documented
The lack of evidence based transition guidance within haemophilia in the UK, and a recognition amongst haemophilia nurses that this could lead to disruption in care, with some reports of poor adherence to treatment with undesirable outcomes, led to a discussion of how to improve care and standards. A group of UK haemophilia nurses formed a working party to benchmark transition through a three-year action-research project called the Transforming Transition Programme.
11.2 Transforming Transition Programme
11.2.1 Aims and Purpose
The Transforming Transition Programme (TTP) was a UK nurse-led initiative to improve transition for young people with haemophilia. The development of this programme involved a review of current practices, collective agreement as to the outcomes that would be measured, and delivering and evaluating a patient-led development programme (see Table 11.1). The aim of the programme was to improve transition by securing changes in working practices that enabled nurses to facilitate improved transition outcomes, and enhance self-management by people with haemophilia.
11.2.2 Haemophilia Care in the UK
Haemophilia is a rare disorder, mostly affecting boys, which is characterised by internal bleeding predominantly into the weight bearing joints leading to early joint damage, known as haemophilic arthropathy and disability. Haemophilia is a genetic condition which is caused by a reduction or absence of one of the two main clotting factors, factor VIII in haemophilia A or factor IX in haemophilia B. The severity of haemophilia depends upon the amount of factor that is missing in the blood and varies from a mild bleeding phenotype to one which causes spontaneous life threatening bleeding. Treatment of bleeding historically occurred only after a bleed; however, contemporary treatment uses prophylactic injections of coagulation factor, given intravenously every 2–3 days to raise the factor levels and reduce bleed risk (Richards et al. 2010).
Haemophilia care, in the UK, is delivered through a network of ‘comprehensive care centres’, which are usually sited in specialist hospitals in the larger cities and ‘haemophilia centres’ in district general hospitals. Children with haemophilia may be seen in paediatric only or paediatric/adult combined centres with varying transition and transfer processes provided. Some patients will see the same clinical team in another environment; and for others, there will be a geographical move between hospitals. Progressing from child to adolescent care is a critical time for young people as this is also the stage during which they become responsible for their own self-management (Khair et al. 2013).
11.2.3 Need for the Project
While transition is routinely discussed in haemophilia review clinics, anecdotal reports from individuals with haemophilia suggest that the transition process is often poorly planned, leaving them feeling lost and unsupported by the healthcare professionals, who until this point have been core members of their support network (Breakey et al. 2010). Rarely are the views of young people or their families sought about the process or outcome of their transition process (Pembroke and Dodgson 2018).
In 2010, Breakey et al. stated that ‘there were no published validated transition programmes to specifically deal with the needs of patients with haemophilia’. They described the complexities of transition in haemophilia where there may be several affected children of differing ages in a family leading to disjointed family care, and where outcome measures and tools are lacking for clinicians/researchers to evaluate transition practice. Assessment of transition is further complicated as the number of adult haemophilia care centres is greater than paediatric centres; therefore, transition from one paediatric care provider to several adult services may be required.
Transition should be an individualised age and developmentally appropriate process, through which each young person is empowered to self-manage with support from their families and multidisciplinary team (MDT). It is widely recognised that young people who are not engaged in self-management become lost in the transfer to adult care, and frequently are not or have become non-adherent to therapy. For those with bleeding disorders, this can have a life-long impact on joint health and quality of life (Young 2012). Within the haemophilia MDT, specialist nurses often take the lead in facilitating transition but in many haemophilia centres, nurses do not have the authority to make referrals resulting in ‘medical transfer’ between services. The TTP was established to benchmark and improve this.
Given the lack of UK transition services available for young adults with haemophilia, a steering group consisting of haemophilia nurses from across the UK convened to develop and deliver the TTP along with representatives of young people with haemophilia. They identified transition barriers as well as examples of good transition practice. TTP was funded through a competitively sought research grant based on a transition initiative from the Burdett Fund for Nursing, which was awarded in 2015. TTP ran as a three-year action research programme wherein the research was initiated as a reflective process aiming to solve the problem of transition through developing a community of practice (Dodgson et al. 2018).
Action research was first described by Lewin in 1946 as a methodology to research conditions and effects of social action ‘that uses “a spiral of steps”, each of which is composed of a circle of planning, action and fact-finding about the result of the action’. Social action brings about social change which benefits individuals, communities or societies and is undertaken by individuals or groups of people working together for the good of others and not for profit.
Action research involves actively participating in a change situation, often via an existing organisation such as the Haemophilia Nurses Association, while simultaneously conducting research to improve strategy, practice and knowledge. As designers and stakeholders, researchers work with others to propose a new action or process to help their community improve its work practices (Bradbury Huang 2010).
Ethical approval for the study was not required as this was deemed a benchmarking project and the participants were NHS staff. An audit of the perspectives of recently transitioned young adults was sought via telephone interviews, which were conducted by three young adults with haemophilia. Twenty young adults with haemophilia aged 18–21 who had recently transitioned from paediatric to adult care were interviewed to seek their opinions about transition processes and if these differed based on diagnosis, gender or geographical location (Pembroke and Dodgson 2018). This discussion was facilitated by the national patient organisation (The Haemophilia Society) to get maximum geographical exposure. Two of the patient co-researchers, who are also ‘Youth Ambassadors’ for the Haemophilia Society, a role established to support the particular needs of young people, also participated in the TTP as members of the steering committee.
11.2.4 Findings
The patient transition interviews were analysed using thematic analysis and revealed positive and potentially negative aspects of transition experience (Pembroke and Dodgson 2018). Much of negativity is related to communication between paediatric and adult teams which was complicated by families of several children/YP being at different stages of a ‘transition pathway’ because of different chronological ages (see Table 11.2). Findings clearly indicated that consistency, planning and communication were extremely important factors that contributed towards a good transition experience for people with haemophilia.
Through continued collaborative working with haemophilia nurses at TTP workshops over the 3-year programme, a defined list of outcome measures for transition in haemophilia care was identified and tested. As the programme progressed three key themes emerged:
-
Identification, development and testing of outcome measures based upon the acquisition of knowledge and skills during transition period that would be needed to increase the chances of successful transfer to adult services.
-
Collaborative approaches among nurses that fostered the sharing of changes implemented in working practices within their centres, their experiences with developing and reviewing local action plans, and to co-produce practice development resources.
-
Supporting the development of Transforming Transitions participants’ skills to lead change within their centres to implement transition programs, and as members of a nurse leadership community to facilitate the provision of transition services in partnership with the Haemophilia Nurse Association.
Input from steering group members, the workshops participants and those involved with local practice development by haemophilia nurses led the production of practice resources for clinicians to use with young people, families and carers. These resources were designed to support young people with haemophilia (and their families/carers) in developing their knowledge and understanding of haemophilia and self-management skills including understanding pharmacokinetics and dosing strategies. These self-management competencies were deemed necessary to enhance the experiences leading up to and beyond the point of transfer to adult services.
At the first action research workshop (see Table 11.1), the need to differentiate the point of transfer to adult services from the overall process of transition became clear, particularly with regard to the development of useable outcome tools. This approach was already implicit in some haemophilia centres; the TTP provided an opportunity for this distinction to be made explicit, to be shared to co-create a national transition programme. This led to the identification and description of an overarching statement that haemophilia centre teams worked towards and that the action research methodology supported:
‘Transfer to adult services is significantly enhanced when people with haemophilia are able to self-infuse/self-treat and have been supported by their clinical team to understand and manage their condition at a developmentally appropriate age/stage’.
This overarching aim aligned with the patient activation strand of the Five-Year Forward View for the NHS (2014), sets out a central ambition for the NHS to become better at helping people with long-term conditions to manage their own health: ‘staying healthy, making informed choices of treatment, managing conditions and avoiding complications’.
For people with haemophilia, the Five-Year Forward View is key to preventing long-term consequences, such as joint damage that impacts on an individual’s quality of life, requirements for treatment and need for support from health and social care. This overarching outcome is underpinned by the indicators described in the NICE guidance on transition from children’s to adults’ services [NG43] published in 2016 (see Table 11.3). The NICE indicators (person centred planning, leadership, education and training, consent and confidentiality, documentation, service planning and delivery, safety/safeguarding, assessment) were used as objectives for the TTP (Dodgson et al. 2018).
A key challenge identified in year one of the action research programme was an apparent reluctance among some nurses to question transition practice within their own haemophilia centres. Much of the development work to support young people and their families in being prepared for transfer to adult services is provided by nurses. Strengthening their voice in the multidisciplinary team through development of the necessary skills and promoting enhanced confidence to implement change in transition practice within their centres was seen as a key measure for year two of the action-research project.
In parallel, the development of future leaders of haemophilia nursing was identified by the Haemophilia Nurse Association (HNA), which agreed to co-fund a clinical leadership programme aimed at participants in the TTP. The ASPIRE course was developed by members of the Transforming Transition steering group and focused on leading clinical practice, theoretical and practical perspectives on leadership, with an emphasis on leading real world change within haemophilia centres.
11.2.5 Case Study: Leading Change in Practice
One haemophilia nurse used actions identified during TTP and the ASPIRE course to develop a new transition program. As a result, the centre has introduced a transition clinic, initially for patients with severe haemophilia, which has improved both the patient experience and the centre’s documentation of patients’ knowledge and skills and transition plans.
One key objective of this centre’s transition plan was to ‘normalise’ the opportunity for boys from the age of 11 to discuss issues with their clinical team without their parents in the consultation room after appropriate ‘rules of confidentiality’ had been agreed by YP, their parents and healthcare professionals (e.g. safeguarding issues would have to be revealed). This was achieved by discussing the proposed changes to transition practice with the young people and their families and carers.
Since the initiation of the transition plan, a number of young people have since chosen to speak with members of their clinical team without a parent or carer present, and have welcomed the opportunity to do so. The implementation of this centre’s transition plan has altered nursing practice. Now, nurses assess haemophilia knowledge and self-management skills using individualised education and training to support seamless transition for these young people.
Another outcome of the TTP involved the ASPIRE course participants who collectively developed a shared vision for ‘ensuring excellent care is everyday practice’, a motto that they continue to use in their centres. This vision has two distinct elements:
-
The continuing shift to a culture of comprehensive care with nurse-led services was a shared goal.
-
The TTP exemplifies the contribution of nurse leadership and sharing practice in changing the ways that centres work with patients and their families/carers.
Following the ASPIRE programme, the participating nurses used their newly acquired leadership skills to begin exploring, trialling and pioneering new approaches to transition in haemophilia care in their centres.
11.2.6 Outcomes
One of the key issues identified during the TTP was the variation in transition working practices among haemophilia centres and within combined centres from paediatric to adult care. For many participants, the introduction of transition clinics and improved documentation resulted from the Transforming Transition workshops where they were able to share ideas, experiences and practices with colleagues in other parts of the UK. This resulted in the development of local/regional action plans, with practical tools, sharing of progress and the development of the next steps for implementation being discussed and implemented during the programme. These included four key aspects, which are described below:
-
1.
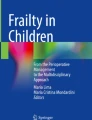
During the 2016 annual UK HNA conference nurses were asked to comment on a timeline of living with haemophilia—the time at which they thought children were able to start self-infusion, the time at which they were competent at this and the time at which transition should be part of the care pathway. There was a great range of views offered with paediatric centres appearing to be more proactive in starting the transition/self-care process at an earlier age. An online survey to gather a greater range of views using a sequence of graphics was developed, centred on ‘Ben’, a developmentally typical child with severe haemophilia, and his family. Respondents were asked to indicate at what age, based on their own experience and practice, they thought ‘Ben’ should achieve each of a series of haemophilia-specific milestones. The responses were then interrogated for consensus (>80% agreement), and means and standard deviations were calculated (see Fig. 11.1).
This exercise demonstrated considerable variations in practice, which were debated. It was agreed that determining a specific age for each stage would be complex, requiring further research to better understand the consequences of differences in practice on health, and that this was outside the scope of the TTP. However, the age ranges for the different stages remain a useful tool in reviewing centre-based practice, and to address and document skills attainment as well as to identify those adolescents and young adults who fall outside the expected range of self-care.
-
2.
Documentation is one of the indicators for effective transition practice indicated in the NICE guidance (National Institute for Health and Care Excellence 2014). Historically, combined haemophilia centres wherein providers treat both children and adults have not seen the necessity for formal transition documentation, while those based in stand-alone paediatric and adult centres have used traditional transfer methods, such as a referral letter. Some centres have used a shared approach between paediatric and adult care placing the young person at the centre of transition using the ‘Ready Steady Go—Hello’ (RSG-H) materials. These have been shown to be effective with other long-term conditions and to empower young people in the lead-up to and transfer to adult services (Nagra et al. 2015). Designed for use with people from the age of 11 years and above, it covers:
-
Knowledge of condition (education/future)
-
Self-advocacy—speaking up for yourself (psychosocial issues)
-
Health and lifestyle (transition process)
Participating haemophilia centres that were already using, or who become ‘early implementers’ of Ready Steady Go—Hello during the TTP found it valuable. Haemophilia nurses developed supplementary questions for the application of the tool in the context of haemophilia (e.g. if the young person was able to self-infuse). It was agreed that this represented a much better use of resources than adapting the tool as a whole.
-
-
3.
Children with haemophilia learn to infuse their own coagulation factors, intravenously (‘self-infusion’) at a relatively early age; whilst not an obvious transition processes in itself, this is a key part of the self-management skills that are a prerequisite to transferring to adult care. Young people with haemophilia are able to comprehend complex treatment decisions and make treatment plans that offer them maximum protection with minimal interference in their day-to-day activities (Khair et al. 2012a) enabling them to participate fully with peers in sporting activities and improve their quality of life (Khair et al. 2012b).
Young (2012) describes transition in haemophilia as a process involving both medical and psychological issues, which start from birth and continue well into adulthood with the ‘most challenging’ period being the teen years (ages 13–18). He describes this period as being a time of non-adherence (to treatment) and rebellion, with young people having a desire to be seen as ‘normal’ and like un-affected siblings and peers. This developmental stage provides haemophilia nurses with a new challenge in supporting young people with haemophilia cope with the difficult physiological transition in attempting to come to terms with both the medical and psychological challenges that they are experiencing. Community care and support including the General Practitioner is paramount at this stage, when the nurse is able to help the young person to move from the specialist-driven haemophilia services to using local services which support adolescent health issues such as contraception and mental health concerns (Segar et al. 2013).
The milestones associated with living with haemophilia described above and shown in Fig. 11.1 show that UK haemophilia nurse consensus on self-treatment/management was achieved during the TTP; this has resulted in changes in nursing practice to encourage earlier self-care in affected boys. To illustrate, a haemophilia centre worked with their younger children (aged 5–7 years) to develop an application to learn about haemophilia in a fun way (‘Haemic’ available at the app store). The staff in this haemophilia centre now use this app in haemophilia clinics, asking the boys to play with it whilst waiting to be seen. During the clinical consultation, the children are then asked about their use of the app, their understanding of haemophilia (genetics, inheritance) and treatment—how and when to treat bleeds, what dose to use and so forth. Early evaluation of this project (data not yet published) has demonstrated an increased knowledge and engagement of young people with their own haemophilia care with the use of this application.
Another centre worked with 8–12 year olds to make educational videos about their perspectives with day-to-day issues of living with haemophilia, by telling real stories in a comedic way. These boys revealed a lack of awareness of self-infusion techniques and a lack of understanding about how treatment works (pharmacokinetics) and how and when to dose. They made further animated videos for peer-to-peer learning/support, which are now available to download from www.haemnet.com/infusion
-
4.
At the start of the programme, the initial challenge of engaging with young people to gain their insights and experiences of transition was addressed through collaboration with the UK Haemophilia Society. The Haemophilia Society Youth Ambassadors interviewed other patients in the community, obtaining valuable and honest results that informed the development plans created by centres during the programme.



Age/development stage and self-management skills towards transition, UK haemophilia nurse consensus
Two of the Youth Ambassadors subsequently became members of the core group of the TTP, representing the patients’ voice. Their continued involvement and input throughout the programme helped shape changes to transition care for those with haemophilia nationally. They did this during the workshops by directly challenging healthcare professionals’ views of living with haemophilia, haemophilia care and transition practices. The interaction of people with the lived experience of haemophilia and transition (good and bad) at the workshops greatly benefited the nurses who saw the impact of transition from beyond a hospital perspective.
One centre proposed developing a better understanding of their transition pathway and welcomed the opportunity to work with young people in doing so. A one-day, regional workshop was organised with young people who were invited to the workshop to discuss the impact of transition on them and their families. These insights reconfirmed the findings from the interviews with young people and the insights shared by those who attended the transition programme. The group agreed that the transition process was successful yet reactive and these programs could benefit from a more proactive approach. The participants agreed that earlier education on the importance of treatment and future options would help to make the transition process smoother.
Transition for those with genetic disease is complicated for parents when there are affected children/young people of different ages. The young people in the transition projects in the TTP revealed the complexity of having younger/older brothers with haemophilia and the impact on the family of having to attend two haemophilia centres to receive the same care (when using both paediatric (for younger) and adult centres (for older siblings)) (Pembroke and Dodgson 2018). This is a well-recognised issue; transition programmes should involve parents as well as young adults. Suris et al. (2017) suggest that parental readiness influences young peoples’ period of readiness for transition. They stated that transitional care must also meet the needs of parents. Given that young people are still dependent on their parents, often for a significant time after transition to adult care, healthcare providers need to work with parents to support the transition to self-care, transfer to adult care and transition to adulthood (Nguyen et al. 2016).
Part of the parental concern may be that they have a 16 (or more) year relationship with the healthcare providers at the paediatric centre and that they have been shielded from adult care and adult hospital environments. This may have inadvertently inhibited the development of transition skills such as being able to self-infuse, or taking on self-management tasks for young people (Al-Yateem and Docherty 2015). After all, young people manage transition in their everyday lives as they change schools and perhaps move out of the house. It is perhaps a failure of healthcare providers who like to hold on to young people within their own centres/hospitals perhaps believing that it is easier for a mother to attend one hospital when she has several boys with haemophilia across an age-range, rather than addressing the needs of each individual child. This is particularly evident in long-term condition management (Aldiss et al. 2017). ‘Holding on’ can be detrimental to the health outcomes in young people, particularly if no disease-specific measures and outcomes are measured during and after transition (Coyne et al. 2017). Ideally, transition of young people with haemophilia can occur at an age/development appropriate stage, whilst retaining other younger family members within paediatric care; this can result in better support, particularly for parents, as they develop relationships with new teams or haemophilia centres.
11.2.7 What Would You Do Differently in the Next Project?
The TTP was aspirational in its vision to transform national practice. Retrospectively several lessons have been learned with this experience. Pragmatically it would have been better to focus initially on a regional project rather than a national one from the start. This shift would have enabled us to work more closely with a smaller number of centres, to support the nurses involved more closely and to tailor the programme to individual centres needs.
We have not been able to design a single tool that can be used nationally; therefore, we have not been able to evaluate change pertaining to the empowerment of nurses involved with the implementation of this new model of care or the impact of the new models of transition on young people. Nationally, we have seen evidence of several changes in practice which continue to improve local transition care. We still need to roll out these improvements to benefit young people in other haemophilia centres, particularly smaller centres where there may not be a specialist nurse.
There is a range of new treatments for people with haemophilia from sub-cutaneous therapies to gene therapy on the horizon, which will change self-care and outcomes for young people and their family members. The impact of these innovations on day-to-day hospital delivered care, the need for repeat hospital visits and the role of nurses in supporting care beyond traditional hospital boundaries leaves us with an opportunity to re-evaluate transition. We would like to develop a standard protocol, which could be adapted to local practice and could be evaluated as an outcome measure in the national haemophilia peer review process. We continue to work on this.
11.3 Conclusion
The TTP demonstrated the developmental need for negotiation and change management skills in haemophilia nurses. We learned that nurses need to be empowered and supported to lead the implementation of transition practice within haemophilia centres. Working with young people as peers in the co-creation of the programme made significant contributions to the overall programmatic goals. This experience highlighted the importance of addressing the knowledge and skills necessary for self-management and living well with haemophilia to support the smooth transition between paediatric and adult services.
The TTP programme provided a platform to support the development of future nurse leaders in the effort to develop and implement transition programs in haemophilia centres in the UK. Through the TTP, training was provided to nurses that equipped them with the skills and confidence to enable changes with the transition process within their centres and to provide assistance and support to colleagues and peers working in other UK centres across the UK to acquire the knowledge and skills needed to provide transition services. As a result of the programme, a ‘Transition Toolkit’ was created, offering nurses a number of resources that can be used with young people and to assist them with the evaluation of the transition process within their centre/network.
11.4 Advantages and Challenges
11.4.1 Advantages
A key advantage of the TTP was the involvement of haemophilia nurses from across the UK along with young people representatives in the development of the initiative and involvement in the three-year action research process. This meant that those with the responsibility for delivering and those receiving the input remained at the forefront of the process, namely changing the age of initiation of early self-management and discussion about transition to adult care almost from the point of diagnosis.
An important advantage was the differentiation of the point of transfer to adult services from the overall process of transition, particularly with regard to the development of useable outcome tools. The development of outcome measures was therefore generated from hearing the experiences of the young people and their families rather than being driven by the healthcare professional professionals. The TTP provided an opportunity for the distinction between point of transfer and process to be made explicit and to be shared with young people and families in order to co-create a national transition programme and a shared statement of intent.
A consequence of the aspirational nature of the programme was the development of future leaders of haemophilia nursing. The development of the clinical leadership programme of the Transforming Transition initiative was initiated. This leadership program focused on leading clinical practice, theoretical and practical perspectives on leadership, with an emphasis on leading real world change within haemophilia centres.
By focusing on national perspectives, the TTP identified the variation in transition working practices among haemophilia centres and combined centres of both paediatric to adult care. This meant that participants were able to share ideas, experience and practice with colleagues in other parts of the UK. This collegial collaboration resulted in the development of local/regional action plans, with sharing practical tools, progress and next steps for implementation discussed and implemented during the programme. UK haemophilia nurse consensus on self-treatment/management was achieved during the programme. This consensus effort resulted in changes in nursing practice to encourage earlier initiation of self-care in affected boys as well as the development of innovative and developmentally appropriate resources.
The continued involvement and input throughout the programme of young people with the lived experience of haemophilia helped shaped changes to transition care and assisted nurses understand the impact of transition (positives and negatives) beyond the hospital perspective. A key learning point of the members was an agreement that earlier education on the importance of treatment and future options would help to make the transition process smoother.
As new treatments for people with haemophilia are developed self-care and outcomes for young people and their family members will have an impact on day-to-day hospital delivered care, avoidable hospitalisations and the role of nurses in supporting care beyond traditional hospital boundaries. The TTP has created an opportunity to re-evaluate transition and the momentum to developing a standard protocol, which could be adapted to local practice and therefore could be evaluated as an outcome measure for national and ultimately international haemophilia care centres. Nationally, we have seen evidence of several changes in practice, which continue to improve local transition care but there still is the need to roll out these improvements to benefit young people in other haemophilia centres.
11.4.2 Challenges
A significant challenge to the development of a coherent approach to the transition for UK children with haemophilia is that they may be seen in either paediatric only or paediatric/adult combined centres that provide varying transition and transfer processes. For some, they will see the same clinical team in another environment and for others there will be a geographical move between hospitals. Under these circumstances, the transition process is often poorly planned, leaving young people and families feeling lost and unsupported by the healthcare professionals, who until this point have been core members of their support network. Paediatric healthcare providers in long-term condition management often hold on to young people within their own centres/hospitals.
Given that young people are still dependent on their parents to varying degrees, often for a significant time after transition to adult care, healthcare providers need to work with parents to support transition to self-care, transition to adult care and transition to adulthood (Nguyen et al. 2016). Young people in the transition projects in the TTP revealed the complexity of having younger/older brothers with haemophilia and the impact of their siblings’ having to attend two haemophilia centres to receive the same care when using both paediatric and adult centres.
A key challenge identified in year one of the action research programme was the apparent reluctance among some nurses to question the transition practice within their own haemophilia centres. In many haemophilia centres, nurses do not have the authority to make referrals resulting in ‘medical transfer’ between services, although much of the development work to support young people and their families for the transfer to adult services is provided by nurses. Key measures for year two of the action-research project were strengthening nurses’ voices on the multidisciplinary team through development of the necessary skills to provide transition services and promoting enhanced confidence to implement change in transition practice within their centres. In all LTHCs transition is understood as a process involving both medical and psychological issues, which begins at birth and continues well into adulthood with the ‘most challenging’ period being the teen years (ages 13–18) (Young 2012). The teen years are exemplified by being a time of non-adherence (to treatment) and rebellion with a desire to not be seen as different from their un-affected siblings and peers (Palareti et al. 2015). This provides haemophilia nurses with a new role in supporting young people in coming to terms with both the medical, physiological and psychological challenges that they are experiencing.
As there are no national guidelines supporting self-management or transition for young adults with haemophilia in the UK as considerable variations in transition practice exist. Determining a specific chronological age for each stage would be complex, requiring further research to better understand the consequences of differences in practice on health, which was outside the remit of the transition project. Focussing on the national rather than a regional perspective made it difficult to work closely with the large number of centres involved in the TTP and limited the amount of support for the nurses who were involved in TTP. As the project did not design evaluation tools that could be used nationally to measure change with the extent to which nurses were empowered or the impact of new models of transition on young people.
11.5 Programme Replication
The TTP was the first initiative to investigate transition practices within haemophilia care in the UK. There are issues pertaining to the treatment settings involving children and adults with haemophilia as treatment for both groups may be provided in different hospitals or different clinics within the same hospital and clinical team. Some haemophilia centres work as networks, involving patient movement within the services to access specialist services such as dentistry, gynaecology and psychology support. The majority of young people described their physical transition process in terms of changing schools—something that they knew was inevitable at some point. The major ‘issue’ they reported was centred on communication between the paediatric and adult haemophilia teams (Pembroke and Dodgson 2018).
Programme replication is effective when associated with another program that has reported demonstratable improvements with outcomes. We would recommend smaller action research sets, with peer support and engagement with others who already have had experience in implementing transition programmes. This could be haemophilia specific or shared learning from other long-term conditions. This replication could be delivered as service evaluation or quality improvement projects to enable a better understanding of local issues and change management.
Future programmes should include young people and their families in the planning, delivery and evaluation. There is about to be a national transition study in France (Ressegueir et al. 2018), which will be assessing transition from both a qualitative and quantitative view—this may give us a format to follow in future UK studies. So far only their methodology is published; it will be interesting to see the results. This project and the TTP focused on young people with severe haemophilia—those who have the most bleeding and treatment and who are most likely to be able to self-infuse and self-manage care. This is supported in the literature where discussion of transition focuses primarily on the most severe bleeding disorders (Pembroke and Dodgson 2018). Young people with milder conditions usually transfer to adult care with minimal self-care education and transition support processes; this is particularly the case with young females treated in paediatric centres who require gynaecology advice at the menarche—they usually ‘just’ transfer to adult services without any preparation (Pembroke and Dodgson 2018). Maybe this is where we should focus future attention, as these young people may become lost in adult care due to the infrequency of bleeding and review, whilst those with severe haemophilia are unlikely to be lost due to the severity of their condition and their ongoing need for treatment. Young women, the sisters of boys with haemophilia who are lost, risk inappropriate antenatal and obstetric care when delivering the next generation of boys with haemophilia—we need to ensure that this issue is addressed with future research and support.
11.6 Key Advice
-
Training in adolescent health/development should be mandatory for HCP working with young people.
-
Young people need to be supported to discuss their health in the context of their daily life and should be offered individual consultation time separate from parent(s)/carer(s).
-
During the first consultation, parameters of confidentiality should be discussed.
-
Parent(s)/carer(s) should be involved in supporting young people throughout transition.
-
HCP should facilitate communication between the young person, parent(s)/carer(s) and professionals to co-create the consultation agenda.
-
All aspects of young people’s healthcare and their biopsychosocial development must be considered in the development of transition programmes.
11.7 Useful Resources
-
‘Making Healthcare Work for Young People’: A Toolkit to support delivery of developmentally appropriate healthcare in the NHS
-
Department of Health (2011): Self-review tool for quality criteria for young people friendly health services. Available at: https://www.gov.uk/government/publications/self-review-tool-for-quality-criteria-for-young-people-friendly-health-services
-
https://www.northumbria.nhs.uk/sites/default/files/nhs-making-healthcare-work-web.pdf
-
Transforming Transition Toolkit resources:
-
‘Hemic’ Haemophilia related educational game app available at www.apple.com/uk/ios/app.store
-
Self-infusion hints and tips web-based resource (https://www.youtube.com/watch?v=720ZedqAr6s)
-
Understanding pharmacokinetic and dosing animation https://www.youtube.com/watch?v=720ZedqAr6s
-
Living well with haemophilia: from diagnosis to adulthood https://youtu.be/1Kes2VXAOuo
-
Transition to adult services: Ben’s story https://youtu.be/CEM5ASv4Zvs
-
References
Aldiss S, Cass H, Ellis J, Gibson F. ‘We sometimes hold on to ours’ – professionals’ views on factors that both delay and facilitate transition. Frontiers in Paediatrics. 2017;4:125. https://doi.org/10.3389/fped.2016.00125.
Al-Yateem N, Docherty C. Transition: a concept of significance to nursing and health care professionals. J Nurs Educ Pract. 2015;5(5):35–40.
Blakemore SJ. Imaging brain development: the adolescent brain. NeuroImage. 2012;61(2):397–406.
Bradbury Huang H. What is good action research?: why the resurgent interest? Action Res. 2010;8:93. https://doi.org/10.1177/1476750310362435.
Breakey V, Blanchette V, Bolton-Maggs P. Towards comprehensive care in transition for young people with haemophilia. Haemophilia. 2010;16:848–57.
Colver AF, Merrick H, Deverill M, Le Couteur A, Parr J, Pearce MS, Rapley T, Vale L, Watson R, McConachie H. Study protocol: longitudinal study of the transition of young people with complex health needs from child to adult health services. BMC Public Health. 2013;13(1):675.
Coyne B, Hallowell S, Thompson M. Measurable outcomes after transition from pediatric to adult providers in youth with chronic illness. J Adolesc Health. 2017;60:3–16.
Crowley R, Wolfe I, Lock K, McKee M. Improving the transition between paediatric and adult healthcare: a systematic review. Arch Dis Child. 2011;96:548–53.
Department of Health. Transition: getting it right for young people. Improving the transition of young people with long term conditions from children’s to adult health services; 2006. http://webarchive.nationalarchives.gov.uk/20130124072700/ http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_4132149.pdf
Dodgson S, Holland M, Pembroke L, Khair K. Transforming transition: enhancing practice in haemophilia. J Haem Pract. 2018;5(1):111. https://doi.org/10.17225/jhp00120.
Dovey-Pearce G, Christie D. Transition in diabetes: young people move on – we should too. Paediatr Child Health. 2013;23(4):174–9.
Five-year Forward view for the NHS. 2014. www.england.nhs.uk/publication/nhs-five-year-forward-view
Khair K, Gibson F, Meerabeau L. The benefits of prophylaxis: views of adolescents with severe haemophilia. Haemophilia. May. 2012a;18(3):e286–9.
Khair K, Littley A, Will A, von Mackensen S. The impact of sport on children with haemophilia. Haemophilia. 2012b;18(6):898–905.
Khair K, Gibson F, Meerabeau L. Self-management and skills acquisition in boys with haemophilia. Health Expect. 2013;18(May 27):1105. https://doi.org/10.1111/hex.12083.
Kmietowicz Z. Five minutes with... Allan Colver. BMJ. 2017;359. https://www.bmj.com/content/359/bmj.j4903
Lewin K. Action research and minority problems. J Soc Issues. 1946;2(4):34–46.
Merrick H, McConachie H, Le Couteur A, Mann K, Parr JR, Pearce MS, Colver A. Characteristics of young people with long term conditions close to transfer to adult health services. BMC Health Serv Res. 2015;15(1):435.
Nagra A, McGinnity PM, Davis N, Salmon AP. Implementing transition: Ready Steady Go. Arch Dis Child Educ Pract Ed. 2015;100(6):313–20. https://doi.org/10.1136/archdischild-2014-307423.
National Institute for Health and Care Excellence. Transition from children's to adult services for young people using health or social care services. Guideline. Scope. 2014;. www.nice.org.uk/guidance/gid-scwave0714/resources/transition-from-childrens-to-adult-services-final-scope3
Nelson KE, Hexem KR, Feudtner C. Inpatient hospital care of children with trisomy 13 and trisomy 18 in the United States. Pediatrics. 2012;129(5):869–76.
Nguyen T, Henderson D, Stewatr D, Hlyva O, Punthakee Z, Gortre JW. You never transition alone! Exploring the experiences of youth with chronic health conditions, parents and healthcare providers on self-management. Child. 2016;42(4):464–72.
Palareti L, Poti S, Cassis F, Emiliani F, Matino D, Iorio A. Shared topics on the experience of people with haemophilia living in the UK and the USA and the influence of individual and contextual variables: results from the HERO qualitative study. Int J Qual Stud Health Well-being. 2015;10:10. https://doi.org/10.3402/qhw.v10.28915.
Pembroke L, Dodgson S. Young people’s experience of transition from paediatric to adult haemophilia care in the UK. J Haem Pract. 2018;5(1):122. https://doi.org/10.17225/jhp00127.
Ressegueir N, Rosso-Delsemme N, Baltran Anzola A, Baumstarck K, Milien V, Ardillon L, Bayart S, Berger C, Bertrand M-Arbitron-Andreani C, Borel-Derlon A, Castet S, Chamouni P, Claeyssens Donadel S, De Raucourt E, Desprez D, Falaise C, Frotscher B, Gay V, Goudemand J, Gruel Y, Guillet B, Harroche A, Hassoun A, Huguenin Y, Thierry Lambert, Lebreton A, Lienhart A, Martin M, Meunier S, Monpoux F, Mourey G, Negrier C, Nguyen P, Nyombe P, Oudot C, Pan-Petesch B, Polack B, Rafowicz A, Rauch A, Rivaud D, Schneider P, Spiegel A, Stoven C, Tardy B, Trossaërt M, Valentin J-B, Vanderbecken S, Volot F, Voyer-Ebrard A, Wibaut B, Leroy T, Sannie T, Chambost H, Auquier P. Determinants of adherence and consequences of the transition from adolescence to adulthood among young people with severe haemophilia (TRANSHEMO): study protocol for a multicentric French national observational cross-sectional study. BMJ Open 2018; 8: e022409. doi: https://doi.org/10.1136/bmjopen-2018-022409.
Richards M, Willaims M, Chalmers E, Liesner R, Collins P, Vidler V, Hanley J. A United Kingdom Haemophilia Centre doctors’ organization guideline approved by the British Committee for Standards in Haematology: guideline on the use of prophylactic factor VIII concentrate in children and adults with severe haemophilia a. B J Haem. 2010;149:498–507.
Rosen DS, Blum RW, Britto M, Sawyer SM, Siegel DM. Transition to adult health care for adolescents and young adults with chronic conditions: position paper of the Society for Adolescent Medicine. J Adolesc Health. 2003;33(4):309–11.
Sawyer SM, Aroni RA. Self-management in adolescents with chronic illness. What does it mean and how can it be achieved. Med J Aust. 2005;183(8):405.
Scal P, Evans T, Blozis S, Okinow N, Blum R. Trends in transition from pediatric to adult health care services for young adults with chronic conditions. J Adolesc Health. 1999;24(4):259–64.
Segar J, Rogers A, Salisbury C, Thomas C. Roles and identities in transition: boundaries of work and inter-professional relationships at the interface between telehealth and primary care. Health Soc Care Commun. 2013;21(6):606–13. https://doi.org/10.1111/hsc.12047.
Stoll BJ, Hansen NI, Bell EF, Shankaran S, Laptook AR, Walsh MC, Hale EC, Newman NS, Schibler K, Carlo WA, Kennedy KA. Neonatal outcomes of extremely preterm infants from the NICHD neonatal research network. Pediatrics, Pediatrics. 2010;126(3):443–56. https://doi.org/10.1542/peds.2009-2959.
Suris JC, Labre JP, Hofer M, Hauschild M, Barrebse-Dias Y, Berchold A, Akre C. Transition for paediatric to adult care: what makes it easier for parents? Child. 2017;43(1):152–5.
Walker-Harding LR, Christie D, Joffe A, Lau JS, Neinstein L. Young adult health and well-being: a position statement of the society for adolescent health and medicine. J Adolesc Health. 2017;60(6):758–9. https://doi.org/10.1016/j.jadohealth.2017.03.021.
Young G. From boy to man: recommendations for the transition process in haemophilia. Haemophilia. 2012;18(s5):27–32.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Khair, K., Pembroke, L., Christie, D. (2020). Nurse-Led Effort in Developing, Implementing and Evaluating Healthcare Transition and Promoting Developmentally Appropriate Healthcare for Young People with Haemophilia. In: Betz, C., Coyne, I. (eds) Transition from Pediatric to Adult Healthcare Services for Adolescents and Young Adults with Long-term Conditions. Springer, Cham. https://doi.org/10.1007/978-3-030-23384-6_11
Download citation
DOI: https://doi.org/10.1007/978-3-030-23384-6_11
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-23386-0
Online ISBN: 978-3-030-23384-6
eBook Packages: MedicineMedicine (R0)