
Abstract
Sixty-two eyes of 37 cataract patients underwent implantation of the AcrySof ReSTOR SN6AD1.
Distance and near visual acuities, contrast sensitivity, defocus curve, and ocular optical performance were reported.
A significant improvement after surgery in distance and near visual acuities was observed (p < 0.05). Contrast sensitivity outcomes are within the normal range for the same age sample for all spatial frequencies. Defocus curve for AcrySof ReSTOR SN6AD1 provides two peaks of maximum vision, at 0D and −2.5D defocus levels.
The AcrySof ReSTOR SN6AD1 IOL models provide excellent visual outcomes for distance and near vision. Contrast sensitivity values are within the normal limits.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Introduction
Diffractive multifocal intraocular lenses (IOLs) follow the Huygens-Fresnel principle . These IOLs generate interference patterns using multiple diffractive rings to create two primary focal points. [1] A side effect produced by this type of multifocal IOL is a reduction in contrast sensitivity compared to monofocal IOLs. To avoid this effect, the apodized diffractive multifocal IOLs were designed. For apodized designs [1], the step height of the diffractive elements is reduced from the center to the periphery. However, it should be noted that dysphotopsia, including halos and glare, is still observed with apodized multifocal IOLs.
The spherical AcrySof ReSTOR SN60D3 IOL incorporated an apodized hybrid diffractive–refractive structure to create an IOL with two focal points. This model was replaced by an aspheric model with a near addition of 4.00 diopters (D), the AcrySof ReSTOR SN6AD3 IOL. At present, two aspheric successors of this multifocal IOL are available: the AcrySof ReSTOR SN6AD1 IOL with a near add of 3.00D and the AcrySof ReSTOR SV25T0 with near add of 2.50D. Aspheric IOLs provide negative spherical aberration [2] to improve contrast sensitivity [3], whereas spherical IOLs add to rather than counterbalance the positive spherical aberration of the cornea.
The 3.00D model was designed to provide better intermediate vision without compromising near or distance visual acuity. De Vries et al. [4] have demonstrated that the AcrySof ReSTOR SN6AD1 IOL gave better results than the AcrySof ReSTOR SN6AD3 IOL in intermediate vision without compromising near and distance visual acuity and contrast sensitivity.
2 Surgical Technique
This multifocal intraocular lens does not require any specific surgical maneuver. The implantation is performed, following cataract removal, through a 2.2 mm incision. In our cases, we perform the cataract surgery by Microincision cataract surgery (MICS). Then, the 2.2 mm incision is placed at the corneoscleral limbus at the steeper corneal meridian. The AcrySof ReSTOR IOL model was implanted using the Monarch III injector (Alcon). The IOL is then injected using the corneal tunnel incision technique to avoid any further incision distortion or enlargement.
3 AcrySof ReSTOR SN6AD1 IOL
The AcrySof ReSTOR SN6AD1 IOL (3.0D addition in the lens plane) is designed to provide quality near to distance vision by combining apodized diffractive and refractive technologies. The center of the IOL surface consists of an apodized diffractive optic (3.6 mm diameter) that focuses light for near through distance. The refractive region of the IOL bends light as it passes through the lens to a focal point on the retina. This outer ring of the lens surrounds the apodized diffractive region and is dedicated to focusing light for distance vision.
3.1 Clinical Experience
3.1.1 Patients
A total of 62 eyes of 37 cataract patients with ages ranging between 48 and 86 were included in the study. All patients underwent cataract surgery with implantation of the apodized diffractive IOL AcrySof ReSTOR SN6AD1 (Alcon). Patients analyzed were patients with incipient or moderate cataract referring a significant reduction of the visual quality and no other ocular comorbidity that might influence the visual outcome.
3.1.2 Preoperative and Postoperative Examinations
Preoperatively all patients had a full ophthalmologic examination including the evaluation of the refractive status, the distance and near visual acuities, slit lamp examination, tonometry, and funduscopy. Distance visual acuity was evaluated with Snellen charts (4 m) and the near (40 cm) with Radner Reading Charts. Besides these clinical tests, other specific examinations were performed, such as corneal topography (CSO, Costruzione Strumenti Oftalmici) and biometry (IOL Master, Zeiss).
Postoperative examinations at 1 and 3 months were identical to the preoperative protocol, with the additional measurements at 1 and 3 months of the contrast sensitivity in photopic (85 cd/m2) and scotopic (3 cd/m2) conditions, the defocus curve and corneal, internal, and ocular aberrometry. The aberrometry was measured with the KR-1 W aberrometer.
3.2 Results
3.2.1 Visual and Refractive Outcomes
Table 19.1 summarizes the preoperative and postoperative visual outcomes of the eyes analyzed. At 1 month after surgery, a statistically significant improvement was observed in the uncorrected distance visual acuity (UDVA), in corrected distance visual acuity (CDVA), and uncorrected near visual acuity (UNVA) (all p ≤ 0.03). No statistical significant differences were detected in corrected near visual acuity (CNVA) after surgery (p = 0.18).
Regarding manifest refraction, a significant decrease was found in the sphere and spherical equivalent 1 month after surgery (p = 0.01). In contrast, no significant changes in the manifest cylinder was detected (p = 0.46) (Table 19.1). As expected, a significant improvement in distance visual outcomes and in UNVA was achieved after IOL implantation. This was consistent with previous findings reported by other studies using the same IOL [4,5,6,7,8,9,10,11,12,13,14], confirming the expectations on the safety of cataract surgery with the evaluated MIOL (Fig. 19.1)

A general view of the AcrySof ReSTOR SN6AD1
3.2.2 Contrast Sensitivity Outcomes
Figure 19.2 shows the mean postoperative contrast sensitivity function in logarithmic scale measured under photopic and scotopic conditions 3 months after surgery. As shown, photopic and low mesopic contrast sensitivity was within the photopic and low mesopic normal limits for the sample age for all spatial frequencies. Several studies compared contrast sensitivity with other multifocal IOLs and reported similar values of contrast sensitivity than the AcrySof ReSTOR SN6AD1 [15,16,17].

Mean photopic and low mesopic contrast sensitivity of the AcrySof ReSTOR SN6AD1 Photopic and low mesopic contrast sensitivity are within the normal limits for all spatial frequencies. Green line, photopic contrast sensitivity; purple line, scotopic contrast sensitivity; black discontinuous lines, normal values of photopic contrast sensitivity for the same age sample; gray discontinuous lines, normal values of low mesopic contrast sensitivity for the same age sample
3.2.3 Defocus Curve
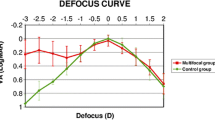
Figure 19.3 shows the mean defocus curve of the patients analyzed. As shown, this multifocal IOL was able to provide two peaks of maximum vision, one at distance (around 0D defocus level) and one at near (around −2.5D defocus level). Between these two peaks, an acceptable intermediate vision was maintained. Alfonso et al. [5] compared the intermediate vision between the AcrySof ReSTOR SN6AD1 and the AcrySof ReSTOR SN6AD3 and found better results with the +3.0D model. A previous study that compared the defocus curve obtained of the AcrySof ReSTOR SN6AD1 with trifocal IOLs showed similar values for the defocus levels corresponding to intermediate vision than the FineVision and lower than the AT Lisa tri 839MP [16].

Mean defocus curve of the AcrySof ReSTOR SN6AD1 multifocal IOL
3.2.4 Optical Quality Outcomes
Figure 19.4 shows the optical quality outcomes through the mean corneal, internal, and ocular wavefront aberration values 3 months postoperatively. As shown, no larger values of these aberrometric parameters were observed after implantation of the AcrySof ReSTOR SN6AD1 multifocal IOL. Toto et al. [14] demonstrated that the ReSTOR +3 model induced less spherical aberration than the ReSTOR +4.

Mean postoperative aberrometry measured by means of the KR-1 W aberrometer after implantation of the AcrySof ReSTOR SN6AD1. Blue bars, corneal aberrations; orange bars, internal aberrations; green bars, ocular aberrations
3.2.5 Quality of Life Outcomes
Previous publications that analyzed the quality of life, spectacle independence, and quality of vision reported high rates for these issues after implantation of AcrySof ReSTOR SN6AD1. These studies compared the outcomes obtained with this IOL model with other multifocal diffractive bifocal and trifocal IOLs and not differences between them were reported.
4 Conclusions
The AcrySof ReSTOR SN6AD1 IOL is able to successfully restore the distance and near visual function after cataract surgery with an optimal intermediate vision. This model of multifocal IOL provides good photopic and low mesopic contrast sensitivity within the normal values. Patients after implantation of this IOL model are satisfied with the quality of vision and spectacle independence obtained.
Advantages
-
Restore the distance and near visual function effectively after cataract surgery.
-
Patients are satisfied with the quality of vision and spectacle independence obtained.
Disadvantages
-
The AcrySof ReSTOR SN6AD1 is less effective for intermediate vision than other trifocal IOLs.
-
Low mesopic contrast sensitivity is negatively affected.
-
Halos are frequently reported by the implanted patients.
Compliance with Ethical Requirements
Ana B. Plaza-Puche and Jorge L. Alió declare that they have no conflict of interest. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients for being included in the study. No animal studies were carried out by the authors for this chapter.
References
Pallikaris I, Plainis S, Charman W. Presbyopia: origins, effects, and treatment Neil. Ed Slack Incorporated. ISBN: 9781617110269.
Sandoval HP, Fernández de Castro LE, Vroman DT, Solomon KD. Comparison of visual outcomes, photopic contrast sensitivity, wavefront analysis, and patient satisfaction following cataract extraction and IOL implantation: aspheric vs spherical acrylic lenses. Eye (Lond). 2008;22:1469–75.
Mencucci R, Menchini U, Volpe R, Vannoni M, Molesini G. Intraocular lenses with surface aspherization: interferometric study. J Cataract Refract Surg. 2007;33:1624–30.
De Vries NE, Webers CA, Montés-Micó R, Ferrer-Blasco T, Nuijts RM. Visual outcomes after cataract surgery with implantation of a +3.00 D or +4.00 D aspheric diffractive multifocal intraocular lens: comparative study. J Cataract Refract Surg. 2010;36:1316–22.
Alfonso JF, Fernández-Vega L, Puchades C, Montés-Micó R. Intermediate visual function with different multifocal intraocular lens models. J Cataract Refract Surg. 2010;36:733–9.
Santhiago MR, Wilson SE, Netto MV, et al. Modulation transfer function and optical quality after bilateral implantation of a +3.00 D versus a +4.00 D multifocal intraocular lens. J Cataract Refract Surg. 2012;38:215–20.
Maxwell WA, Cionni RJ, Lehmann RP, Modi SS. Functional outcomes after bilateral implantation of apodized diffractive aspheric acrylic intraocular lenses with a +3.0 or +4.0 diopter addition power; randomized multicenter clinical study. J Cataract Refract Surg. 2009;35:2054–61.
Alfonso JF, Fernandez-Vega L, Amhaz H, Montes-Mico R, Valcarcel B, Ferrer-Blasco T. Visual function after implantation of an aspheric bifocal intraocular lens. J Cataract Refract Surg. 2009;35:885–92.
Kohnen T, Nuijts R, Levy P, Haefliger E, Alfonso JF. Visual function after bilateral implantation of apodized diffractive aspheric multifocal intraocular lenses with a +3.0 D addition. J Cataract Refract Surg. 2009;35:2062–9.
Hayashi K, Manabe S-I, Hayashi H. Visual acuity from far to near and contrast sensitivity in eyes with a diffractive multifocal intraocular lens with a low addition power. J Cataract Refract Surg. 2009;35:2070–6.
Santhiago MR, Netto MV, Espindola RF, Mazurek MG, Gomes BAF, Parede TRR, Harooni H, Kara-Junior N. Reading performance after bilateral implantation of multifocal intraocular lenses with +3.00 or +4.00 diopter addition. J Cataract Refract Surg. 2010;36:1874–9.
Lane SS, Javitt JC, Nethery DA, Waycaster C. Improvements in patient-reported outcomes and visual acuity after bilateral implantation of multifocal intraocular lenses with +3.0 diopter addition: multicenter clinical trial. J Cataract Refract Surg. 2010;36:1887–96.
Kaymak H, Breyer D, Alió JL, Cochener B. Visual performance with bifocal and trifocal diffractive intraocular lenses: a prospective three-armed randomized multicenter clinical trial. J Refract Surg. 2017;33:655–62.
Toto L, Carpineto P, Falconio G, Agnifili L, Di Nicola M, Mastropasqua A, Mastropasqua L. Comparative study of Acrysof ReSTOR multifocal intraocular lenses +4.00 D and +3.00 D: visual performance and wavefront error. Clin Exp Optom. 2013;96:295–302.
Alió JL, Kaymak H, Breyer D, Cochener B, Plaza-Puche AB. Quality of life related variables measured for three multifocal diffractive intraocular lenses: a prospective randomised clinical trial. Clin Exp Ophthalmol. 2018;46:380–8.
Plaza-Puche AB, Alio JL, Sala E, Mojzis P. Impact of low mesopic contrast sensitivity outcomes in different types of modern multifocal intraocular lenses. Eur J Ophthalmol. 2016;26:612–7.
Mastropasqua R, Pedrotti E, Passilongo M, Parisi G, Marchesoni I, Marchini G. Long-term visual function and patient satisfaction after bilateral implantation and combination of two similar multifocal IOLs. J Refract Surg. 2015;31:308–14. Erratum in: J Refract Surg. 2015;31:522.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Plaza-Puche, A.B., Alió, J.L. (2019). Multifocal Intraocular Lenses: AcrySof ReSTOR SN6AD1 Lens. In: Alió, J., Pikkel, J. (eds) Multifocal Intraocular Lenses. Essentials in Ophthalmology. Springer, Cham. https://doi.org/10.1007/978-3-030-21282-7_19
Download citation
DOI: https://doi.org/10.1007/978-3-030-21282-7_19
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-21281-0
Online ISBN: 978-3-030-21282-7
eBook Packages: MedicineMedicine (R0)