
Abstract
Rabies has shaped humanity for centuries and continues to be one of the few pathogens that have a near 100% case fatality rate following the onset of clinical disease. Rabies virus, as with all related viruses within the Lyssavirus genus, is spread via the mechanistic action of the bite of an infected animal. Lyssaviruses are strongly neurotropic and as such most often require the dermal barrier to be breached to enable access to and infection of the nervous system. The domestic dog represents the principal reservoir of rabies virus globally and 99% of human cases involve the bite of an infected dog. Lyssaviruses are predominantly shed through saliva and so although a bite appears to be the most efficient mechanism of transmission rare alternative routes, including organ transplantation, have been reported. Despite the near 100% case fatality rate, post-exposure intervention can prevent the development of clinical disease and resulting fatality. Vaccines against rabies have been available, in various forms, for over 100 years and alongside the observation that passive immunisation with rabies immunoglobulin can completely prevent disease when administered pre-clinically the disease is entirely preventable. However, in endemic regions the cost and availability of post-exposure vaccines and immunoglobulins often precludes their use and rabies develops with the concomitant high fatality reported in endemic countries. The need for efficacious and yet cheaper pan-lyssavirus vaccines and biologicals to both prevent and treat rabies remains an important issue for future development. Furthermore, a lack of adequate reporting systems means that rabies is grossly underreported and that the burden of disease may be considerably higher. This chapter considers the basis of rabies classification, epidemiology and pathogenesis is reviewed highlighting areas for potential improvement in our understanding of this important group of viruses.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Introduction
Rabies is an ancient zoonotic disease caused by viruses of the order Mononegavirales, family Rhabdoviridae, and genus Lyssavirus [1]. Rabies, or hydrophobia as it has been historically described through the profound fear of water observed in some clinical cases, is most commonly transmitted following the bite of an aggressive animal, most often a rabid dog. Rabies has shaped humanity for centuries with the first descriptions of rabies disease being recorded in the fourth century BC [2]. With a case fatality rate approaching 100% the disease, rabies, has shaped human history and remains one of the most globally feared pathogens. Whilst all members of the Lyssavirus genus are capable of causing rabies, only the prototype lyssavirus, rabies virus (RABV), is truly an important pathogen of humans and animals with an estimated 60,000 human fatalities being caused by rabies each year. The majority of human deaths occur across Africa and Asia where the virus is enzootic. Despite this death toll, both animal and human rabies are entirely preventable. In the 1800s, Louis Pasteur developed the first rabies vaccination during a time widely considered to be the dawn of vaccination. In the 100 years since the development of the first human vaccines, rabies vaccines have remained largely unchanged, with only the development of alternatives to the nerve tissue-derived vaccines through the establishment of vaccines prepared in cell culture, thereby altering the safety of the product available [3]. From these vaccines, the 0.5 IU/ml threshold, which was considered indicative for a protective virus neutralising antibody (VNA) response was established for human protection [4]. Despite the insensitivity of existing neutralisation tests to define a lower limit for VNA titres that could be considered as a protective level, this cut-off of 0.5 IU/ml has been universally accepted as a standard parameter that is representative of protective immunity against rabies virus [5]. Of course, the discovery of a further 15 proposed lyssaviruses dictates that a thorough assessment of neutralisation titre is required across the genus [6]. For the vaccination of dogs, several vaccine preparations are available although parenteral vaccination, though often logistically challenging, remains the most readily adopted mechanism of vaccination. Certainly, where responsible dog ownership is practised, parenteral vaccination and assessment of serological titre is undertaken [7]. In endemic areas, where free-roaming dogs are often abundant, options including oral vaccination have been proposed [8,9,10,11] although adoption of dog licencing and responsible ownership to reduce free-roaming populations is the only viable future option for rabies control in these areas [12].
Classification and Epidemiology of the Lyssaviruses
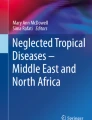
The prototype virus of the Lyssavirus genus is RABV. However, although RABV is the most notable cause of human fatalities from rabies, other lyssaviruses have been described that are capable of causing rabies and that have contributed to the human and animal death toll from these viruses. In total, there are 16 proposed members of the Lyssavirus genus with the majority of the lyssavirus species having been detected in bats [13]. Although the death toll associated with infection with lyssaviruses other than rabies is negligible, in RABV endemic regions the diagnostic tools required to type lyssaviruses species are generally lacking and as such the exact epidemiology of lyssaviruses is unclear [1]. Furthermore, whilst the existing rabies vaccines are able to stimulate a VNA response that protects against RABV, protection afforded against the other lyssaviruses is undefined and for specific lyssavirus species, it is acknowledged that current human vaccines are completely ineffective in preventing clinical disease and death [14, 15]. From an antigenic standpoint, this has led to the grouping of lyssaviruses into phylogroups, reflecting the data of vaccine protection within the Lyssavirus genus. All phylogroup I viruses are considered to be neutralised by the VNA response generated following rabies vaccination. For viruses in phylogroups II and III, either minimal or no protection is conferred by rabies vaccination. The taxonomic classification according to phylogenetic analysis of the nucleoprotein (N-gene) and detailing division of viral species into phylogroups is detailed in Fig. 1.

Global members of the Lyssavirus genus
Whilst RABV, and the often horrific manifestations of the disease it causes, has shaped many elements of humanity [16], the remaining lyssaviruses are comparatively recent in their description [13]. Whilst the basic properties of the RABV life cycle and clinical disease are well defined, empirical data is still required to further our understanding of the lyssaviruses. Epidemiologically, RABV is present globally with all mammals being considered susceptible, although the development of clinical disease may depend on the infecting dose, the viral species involved and the host exposed [1]. The domestic dog, often free-roaming in areas where the virus is endemic [17], is the principal reservoir of the virus and almost all transmission events to humans involve the bite of an infected dog [5]. Other mechanisms of human infection have been reported that can deviate from the standard bite related exposure including rare events of organ transplantation [18] and interactions with bats where cryptic infection can occur through unknown exposures [19]. From an epidemiological standpoint, one confounding feature of lyssavirus epidemiology is the distribution of the different lyssavirus species globally. Rabies virus has been detected globally in terrestrial carnivores although infection of bats seems limited to bats in the Americas where cycles of infection exist in insectivorous, frugivorous and hematophagous bats [20]. In the Old World, whilst terrestrial carnivores maintain RABV, it has never been detected in bats there [21]. In contrast, the remaining 15 species of lyssaviruses have only been discovered in the Old World, with bat infection predominating. Such genetically divergent lyssaviruses include European bat lyssaviruses types 1 and 2, Bokeloh bat lyssavirus and Lleida bat lyssavirus within Europe; Aravan bat lyssavirus, Khujand bat lyssavirus, Irkut bat lyssavirus, Gannoruwa bat lyssavirus and West Caucasian bat lyssavirus across Asia; Duvenhage bat lyssavirus, Shimoni bat lyssavirus, Ikoma lyssavirus, Mokola lyssavirus and Lagos bat lyssavirus across Africa; and Australian bat lyssavirus in Australasia. Interestingly, these lyssavirus species have never been detected in the Americas [22]. Other features of lyssavirus epidemiology, however, remain a paradox, particularly whether the origins of the ‘cosmopolitan’ strain of RABV and subsequent worldwide spread of this strain exist in the Old or New World.
Basic Viral Life Cycle
Lyssaviruses constitute a group of non-segmented negative-strand RNA viruses with small genomes of 11–12 kilobases encoding only five genes in the following conserved gene order: the nucleoprotein (N), phosphoprotein (P), matrix protein (M), glycoprotein (G) and Large polymerase protein (L). Conservation at the nucleotide level across the lyssavirus genome is high with maximum divergence of 60% being seen across the genome. Gene lengths and intergenic regions are also generally well conserved and the basic replication strategy of all non-segmented negative-strand viruses following a common theme as outlined below. Genome RNAs exist as fully encapsidated RNA molecules, protected from the harsh cytoplasmic milieu by the N-protein encapsidation. The negative-strand RNA genomes serve as the template for messenger RNAs that are generated by a transcriptase complex that includes the N, P and L proteins in association with the RNA. The complex of RNA, encapsidated in N and in association with P and L represents the minimal replicative unit for these viruses—the ribonucleoprotein complex (RNP). Viral transcription of mRNA species leads to the generation of viral proteins with mRNAs being translated on host cell ribosomes. An accumulation of viral proteins within the cell contributes to a switch from transcriptive to replicative activity whereby the polymerase generates full-length positive-sense genome strands of RNA that are co-transcriptionally encapsidated. These replicative intermediates then act as templates for the production of nascent genome negative-sense RNA that is encapsidated and released from the cell as nascent infectious virions.
Transmission and Pathogenesis
Lyssaviruses are most efficiently transmitted through exposure to virus-laden saliva that must cross the dermal barrier to infect although transmission can also occur through contact with mucous membranes. Once the virus has entered the host, it enters peripheral nerves and transports to neurons in the central nervous system (CNS) via retrograde axonal transport. Once in the CNS, the virus replicates, causing the development of clinical disease as it spreads through the brain. Behavioural changes are the result of this replication with two main outcomes of disease: furious and paralytic rabies. Whilst the late-stage disease in either outcome may differ, early stages of infection may be similar to paraesthesia and/or pruritus being evident at the bite site. Further, incoordination, fever, and inhibitory spasms may be seen before the disease progresses to an aggressive or paralytic conclusion [23]. Cause of death is generally considered to be heart failure although replication within the brain can cause multi-organ system failure. For rabies, pathogenesis has been well defined in humans and animals although no symptoms are considered pathognomonic for rabies and as such only laboratory confirmation can prove a lyssavirus as the causative agent. In areas where diagnostic capabilities are unable to confirm the presence of a lyssavirus strain, infection may be considered to be caused by other infectious agents [24] or medical conditions [25]. For the remaining lyssaviruses, pathogenesis is poorly defined with only a small number of human cases being associated with infection [13]. Of those, the infection with European and Australian bat lyssaviruses has most extensively documented as they have occurred in countries with adequate health care and diagnostic capabilities to enable assessment of the infected individuals throughout the course of disease [26]. As seen with rabies, a progressive encephalitis was observed that resulted in death [27,28,29]. Following such high profile cases in humans in rabies-free areas, several recommendations were made regarding interactions with bats including a recommendation for pre-immunisation and use of personal protective equipment when handling any bats [30]. Where human infection has not been reported, and the association of a lyssavirus species is restricted to bat species, the epidemiology of these lyssaviruses is poorly defined. Certainly, numerous lyssaviruses exist as only single isolates and as such, there is limited information regarding their evolution and global distribution. Based on the genetic heterogeneity within the Old World lyssavirus species, it has been speculated that the evolutionary origins of lyssaviruses originated in the Paleo-Arctic regions [31], a hypothesis in direct contrast to the ‘out of Africa’ postulated previously [32]. This new hypothesis has led to the suggestion that the New World RABV evolved from a recent common ancestor in the Old World, probably in a sympatric bat host, before host switching from chiropteran into mammalian species. It is clear that the continued discovery of novel, phenotypically and genetically divergent lyssaviruses from different regions of the world prevents meaningful assessment of lyssavirus evolution, especially in instances where the number of isolates detected remains low.
Rabies Diagnosis
In endemic regions, the diagnosis of rabies is challenging due to a general lack of diagnostic capabilities and cultural practises that resist the submission of diagnostic material at post-mortem. The optimal sample for rabies diagnosis is brain material that can only be taken at post-mortem although options for ante-mortem testing, including saliva swabs and nuchal skin biopsies have shown utility [33]. For human rabies diagnosis, the requirement for brain sampling is problematic as post-mortem of the deceased is often culturally unacceptable in endemic regions and as such a definitive diagnosis is rarely made [34]. As previously described, this can lead to the misdiagnosis of rabies [24]. To this end, a high priority in the fight to eliminate rabies is the development of diagnostic infrastructure at both animal and human health centres such that endemic regions have the capability to accurately diagnose the infection at both ante- and post-mortem using internationally validated diagnostic tools. The technological evolution of molecular techniques and next-generation sequencing has revolutionized the ability to diagnose infectious organisms although such technology is often lacking in resource-limited areas [35]. Future efforts should focus on enabling diagnosticians within endemic regions through the provision of tools and training to be able to accurately diagnose lyssavirus infections. At its simplest, local diagnosis can be confirmed at national or international reference laboratories [35].
Global Efforts to Eliminate Dog-Mediated Rabies
In a vital first step in the planned elimination of dog-mediated rabies, the World Health Organisation (WHO) and World Organisation for Animal Health (OIE) have mandated that human and animal rabies should be considered notifiable diseases. As a first stage, a system for diagnosis and surveillance should be initiated to ensure accurate reporting and notification of animal and human rabies cases [35]. However, despite this important definition, endemic areas often lack the laboratory infrastructure to enable timely reporting of cases. To this end, governments in endemic areas should follow a step-wise approach towards dog rabies elimination that links achievable goals on a structured pathway to disease elimination [12].
The WHO, OIE and the Food and Agriculture Organisation (FAO) have advocated the elimination of dog-mediated human rabies by 2030. This aim forms part of the Millennium Development Goals to reduce poverty and preventable childhood deaths from infectious diseases in resource-limited regions of the world and, although it is considered a neglected tropical disease, the burden on human life and cost of post-exposure prophylactic resources places rabies as a high priority [36]. The FAO in collaboration with the OIE and WHO has further developed a Progressive Control Pathway towards rabies elimination, in which the final stage is maintaining freedom from rabies in both human and animal populations [37]. As the vast majority of human cases of rabies arise following the bite from an infected dog, this aim, if successful, will all but eradicate terrestrial rabies, as wildlife reservoirs of the disease are thought to contribute to a fraction of human cases. However, improved rabies surveillance in the light of elimination of dog-mediated rabies might demonstrate that certain sylvatic reservoirs are of greater importance than others and that other lyssaviruses also pose a serious threat to human and animal health. The successful elimination of rabies from domestic species across Western Europe and North America has demonstrated the impact of elimination of the disease. However, the continued presence of sylvatic rabies in North America has highlighted that improvements to vaccination strategies for wildlife rabies are required to eliminate this remaining threat. It is unclear how much this situation will be seen across endemic areas in Africa and Asia, where free-roaming dog populations act as the principal reservoir and wildlife cases are rarely reported. However, it is likely that similar factors will affect rabies elimination strategies in the longer term. Whilst the elimination of terrestrial rabies is an achievable goal with the concomitant reduction of human rabies cases worldwide, options to eliminate lyssaviruses in bat populations remain challenging. Consequently, the true eradication of lyssaviruses from all mammalian reservoirs, with comparison to the eradication of Smallpox and Rinderpest, is thought to be unachievable at present.
Clearly, the factors associated with the elimination of rabies include complex obstacles that require attention. The elimination of RABV from domestic dogs will drive a considerable reduction in human disease, but relies on the development of both human and veterinary infrastructure that will support a consistent and sustained programme of elimination [38]. To achieve the global elimination of dog-mediated rabies, it is estimated that investment of over US$6.3 billion is required [39]. Frustratingly, cultural and behavioural shifts in the management of dog populations would readily remove this obstacle to elimination. Seventy percent vaccine coverage has been defined as the cut-off for which vaccination can disrupt the transmission chain of the virus in free-roaming dog communities [40,41,42], and as such responsible dog ownership and vaccination is a simple mechanism that would enable the prevention of human rabies [43]. Where extensive free-roaming dog populations circulate, the oral vaccination of free-roaming dog populations has been proposed as a complementary measure to parenteral vaccination, but the delivery of vaccines in this way, in a manner that negates the risk of human consumption is challenging, as is any post-vaccinal assessment of immune responses [44]. Whilst the elimination of sylvatic rabies from Western Europe has demonstrated the utility of oral vaccination programmes, the challenges in achieving sufficient mastication of the vaccine in dogs to enable adequate exposure and seroconversion remains a surmountable obstacle [45]. In an era where dog-mediated rabies has been eliminated, the full impact of other lyssaviruses may be further defined and as such options for optimised, cross-reactive pan-lyssavirus vaccines that are affordable for use in economically restricted countries may need to be developed [6] although they are unlikely to be of interest unless a substantial threat from other lyssaviruses in causing human rabies cases is demonstrated [38].
References
Fooks AR, Banyard AC, Horton DL, Johnson N, McElhinney LM, Jackson AC. Current status of rabies and prospects for elimination. Lancet. 2014;384(9951):1389–99.
Neville J. Rabies in the ancient world. In: King AA, Fooks AR, Aubert M, editors. Historical perspective of rabies in Europe and the Mediterranean Basin. Paris: OIE; 2004. p. 1–12.
Hicks DJ, Fooks AR, Johnson N. Developments in rabies vaccines. Clin Exp Immunol. 2012;169(3):199–204.
Moore SM, Hanlon CA. Rabies-specific antibodies: measuring surrogates of protection against a fatal disease. PLoS Negl Trop Dis. 2010;4(3):e595.
WHO. WHO expert consultation on rabies. 2013. p. 1–139.
Evans JS, Horton DL, Easton AJ, Fooks AR, Banyard AC. Rabies virus vaccines: is there a need for a pan-lyssavirus vaccine? Vaccine. 2012;30(52):7447–54.
Goddard AD, Donaldson NM, Horton DL, Kosmider R, Kelly LA, Sayers AR, Breed AC, Freuling CM, Muller T, Shaw SE, Hallgren G, Fooks AR, Snary EL. A quantitative release assessment for the noncommercial movement of companion animals: risk of rabies reintroduction to the United kingdom. Risk Anal. 2012;32(10):1769–83.
Campbell JB. Oral rabies immunization of wildlife and dogs: challenges to the Americas. Curr Top Microbiol Immunol. 1994;187:245–66.
Cliquet F, Guiot AL, Munier M, Bailly J, Rupprecht CE, Barrat J. Safety and efficacy of the oral rabies vaccine SAG2 in raccoon dogs. Vaccine. 2006;24(20):4386–92.
Cliquet F, Gurbuxani JP, Pradhan HK, Pattnaik B, Patil SS, Regnault A, Begouen H, Guiot AL, Sood R, Mahl P, Singh R, Meslin FX, Picard E, Aubert MF, Barrat J. The safety and efficacy of the oral rabies vaccine SAG2 in Indian free-roaming dogs. Vaccine. 2007;25(17):3409–18.
Corn JL, Mendez JR, Catalan EE. Evaluation of baits for delivery of oral rabies vaccine to dogs in Guatemala. Am J Trop Med Hyg. 2003;69(2):155–8.
Fahrion AS, Taylor LH, Torres G, Müller T, Dürr S, Knopf L, de Balogh K, Nel LH, Gordoncillo MJ, Abela-Ridder B. The road to dog rabies control and elimination-what keeps us from moving faster? Front Public Health. 2017;5(103):1–8.
Banyard AC, Fooks AR. The impact of nove lyssavirus discovery. Microbiol Australia. 2017;38(1):18–21.
Badrane H, Bahloul C, Perrin P, Tordo N. Evidence of two Lyssavirus phylogroups with distinct pathogenicity and immunogenicity. J Virol. 2001;75(7):3268–76.
Hanlon CA, Kuzmin IV, Blanton JD, Weldon WC, Manangan JS, Rupprecht CE. Efficacy of rabies biologics against new lyssaviruses from Eurasia. Virus Res. 2005;111(1):44–54.
Baer GM. Rabies—an historical perspective. Infect Agents Dis. 1994;3(4):168–80.
Bagcchi S. India fights rabies. Lancet Infect Dis. 2015;15(2):156–7.
Wallace RM, Stanek D, Griese S, Krulak D, Vora NM, Pacha L, Kan V, Said M, Williams C, Burgess TH, Clausen SS, Austin C, Gabel J, Lehman M, Finelli LN, Selvaggi G, Joyce P, Gordin F, Benator D, Bettano A, Cersovsky S, Blackmore C, Jones SV, Buchanan BD, Fernandez AI, Dinelli D, Agnes K, Clark A, Gill J, Irmler M, Blythe D, Mitchell K, Whitman TJ, Zapor MJ, Zorich S, Witkop C, Jenkins P, Mora P, Droller D, Turner S, Dunn L, Williams P, Richards C, Ewing G, Chapman K, Corbitt C, Girimont T, Franka R, Recuenco S, Blanton JD, Feldman KA. A large-scale, rapid public health response to rabies in an organ recipient and the previously undiagnosed organ donor. Zoonoses Public Health. 2014;61(8):560–70.
Messenger SL, Smith JS, Rupprecht CE. Emerging epidemiology of bat-associated cryptic cases of rabies in humans in the United States. Clin Infect Dis. 2002;35(6):738–47.
Banyard AC, Hayman DTS, Freuling CF, Mueller T, Fooks AR, Johnson N. Bat rabies. In: Jackson AC, editor. Rabies: scientific basis of the disease and its management. 3rd ed. Oxford: Elsevier Academic Press; 2013.
Badrane H, Tordo N. Host switching in Lyssavirus history from the Chiroptera to the Carnivora orders. J Virol. 2001;75(17):8096–104.
Banyard AC, Evans JS, Luo TR, Fooks AR. Lyssaviruses and bats: emergence and zoonotic threat. Viruses. 2014;6(8):2974–90.
Hemachudha T, Ugolini G, Wacharapluesadee S, Sungkarat W, Shuangshoti S, Laothamatas J. Human rabies: neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013;12(5):498–513.
Mallewa M, Fooks AR, Banda D, Chikungwa P, Mankhambo L, Molyneux E, Molyneux ME, Solomon T. Rabies encephalitis in malaria-endemic area, Malawi, Africa. Emerg Infect Dis. 2007;13(1):136–9.
Sheikh KA, Ramos-Alvarez M, Jackson AC, Li CY, Asbury AK, Griffin JW. Overlap of pathology in paralytic rabies and axonal Guillain-Barre syndrome. Ann Neurol. 2005;57(5):768–72.
Fooks AR, McElhinney LM, Pounder DJ, Finnegan CJ, Mansfield K, Johnson N, Brookes SM, Parsons G, White K, McIntyre PG, Nathwani D. Case report: isolation of a European bat lyssavirus type 2a from a fatal human case of rabies encephalitis. J Med Virol. 2003;71(2):281–9.
Francis JR, Nourse C, Vaska VL, Calvert S, Northill JA, McCall B, Mattke AC. Australian Bat Lyssavirus in a child: the first reported case. Pediatrics. 2014;133(4):e1063–7.
Fraser GC, Hooper PT, Lunt RA, Gould AR, Gleeson LJ, Hyatt AD, Russell GM, Kattenbelt JA. Encephalitis caused by a Lyssavirus in fruit bats in Australia. Emerg Infect Dis. 1996;2(4):327–31.
Lumio J, Hillbom M, Roine R, Ketonen L, Haltia M, Valle M, Neuvonen E, Lahdevirta J. Human rabies of bat origin in Europe. Lancet. 1986;1(8477):378.
Banyard AC, Hartley M, Fooks AR. Reassessing the risk from rabies: a continuing threat to the UK? Virus Res. 2010;152(1–2):79–84.
Nel LH, Rupprecht CE. Emergence of lyssaviruses in the Old World: the case of Africa. Curr Top Microbiol Immunol. 2007;315:161–93.
Hayman DT, Fooks AR, Marston DA, Garcia RJ. The global phylogeography of lyssaviruses—challenging the ‘Out of Africa’ hypothesis. PLoS Negl Trop Dis. 2016;10(12):e0005266.
Dacheux L, Reynes JM, Buchy P, Sivuth O, Diop BM, Rousset D, Rathat C, Jolly N, Dufourcq JB, Nareth C, Diop S, Iehle C, Rajerison R, Sadorge C, Bourhy H. A reliable diagnosis of human rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008;47(11):1410–7.
Banyard AC, Horton D, Freuling C, Müller T, Fooks AR. Control and prevention of canine rabies: the need for building laboratory based surveillance capacity. Antiviral Res. 2013;98(3):357–64.
Banyard AC, Horton DL, Freuling C, Muller T, Fooks AR. Control and prevention of canine rabies: the need for building laboratory-based surveillance capacity. Antiviral Res. 2013;98(3):357–64.
Abela-Ridder B, Knopf L, Martin S, Taylor L, Torres G, De Balogh K. The beginning of the end of rabies? Lancet Glob Health. 2016;4(11):e780–1.
Coetzer A, Kidane AH, Bekele M, Hundera AD, Pieracci EG, Shiferaw ML, Wallace R, Nel LH. The SARE tool for rabies control: current experience in Ethiopia. Antiviral Res. 2016;135:74–80.
Rupprecht C, Kuzmin I, Meslin F. Lyssaviruses and rabies: current conundrums, concerns, contradictions and controversies. F1000Res. 2017;6:184
Wallace RM, Undurraga EA, Blanton JD, Cleaton J, Franka R. Elimination of dog-mediated human rabies deaths by 2030: needs assessment and alternatives for progress based on dog vaccination. Front Vet Sci. 2017;4:9
Coleman PG, Dye C. Immunization coverage required to prevent outbreaks of dog rabies. Vaccine. 1996;14(3):185–6.
Hampson K, Dushoff J, Cleaveland S, Haydon DT, Kaare M, Packer C, Dobson A. Transmission dynamics and prospects for the elimination of canine rabies. PLoS Biol. 2009;7(3):e53.
Leung T, Davis SA. Rabies vaccination targets for free-roaming dog populations. Front Vet Sci. 2017;4:52
Lavan RP, King A, Sutton DJ, Tunceli K. Rationale and support for a One Health program for canine vaccination as the most cost-effective means of controlling zoonotic rabies in endemic settings. Vaccine. 2017;35(13):1668–74.
WHO. Guidance for research on oral rabies vaccines and field application of oral vaccination of dogs against rabies. In: Meslin F, editor. Oral vaccination of dogs against rabies. Geneva: WHO; 2007.
Muller T, Batza HJ, Beckert A, Bunzenthal C, Cox JH, Freuling CM, Fooks AR, Frost J, Geue L, Hoeflechner A, Marston D, Neubert A, Neubert L, Revilla-Fernandez S, Vanek E, Vos A, Wodak E, Zimmer K, Mettenleiter TC. Analysis of vaccine-virus-associated rabies cases in red foxes (Vulpes vulpes) after oral rabies vaccination campaigns in Germany and Austria. Arch Virol. 2009;154(7):1081–91.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Banyard, A.C., Fooks, A.R. (2020). Rabies Life Cycle, Transmission and Pathogenesis. In: Ertl, H. (eds) Rabies and Rabies Vaccines. Springer, Cham. https://doi.org/10.1007/978-3-030-21084-7_1
Download citation
DOI: https://doi.org/10.1007/978-3-030-21084-7_1
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-21083-0
Online ISBN: 978-3-030-21084-7
eBook Packages: Biomedical and Life SciencesBiomedical and Life Sciences (R0)