
Abstract
Early rehabilitation efforts are a key component of acute burn management. Burn caregivers should be aware of the short- and long-term impact of wound maturation and scarring and the consequences for functional recovery and quality of life, as well as techniques for preventing and treating burn-associated impairments.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
1 Overview
1.1 Burn Rehabilitation
The overarching goals of burn rehabilitation are the restoration of function, independence, and quality of life following burn injury. Reaching this goal requires a detailed understanding of the impact of burn injury and the application of early interventions to prevent and treat complications that would impact recovery. In addition, burn rehabilitation providers must also be mindful of longer term complications associated with scar maturation as well as psychological and social consequences that may arise at later stages of recovery as survivors attempt to return to pre-morbid activities. In many cases, the impact of these late-stage factors can be mitigated by early interventions, planning, and patient education on the part of rehabilitation staff.
1.2 Defining Burn Therapy
Resources are available to guide rehabilitation providers towards the knowledge base, skills, and experience that are associated with burn injury recovery. The Burn Rehabilitation Therapist Competency Tool (BRTCT) project has worked to define the key areas of competence and best practice and exists to assist burn centers in developing center-specific standards for orientation and professional development of burn therapists [1, 2]. In many cases, these skill sets are largely outside of the routine training of occupational therapists, physiotherapists, and speech-language pathologists, and it can be argued that a burn rehabilitation therapist can evolve from a number of backgrounds with sufficient experience and education.
Burn treatment and rehabilitation require the dedicated effort of the entire interdisciplinary team. The core team consists of physicians, nurses, respiratory therapists, occupational therapists, physiotherapists, social workers, pharmacists, dieticians, speech-language pathologists, psychologists, child-life therapists as well as the patient and their families. It is important for everyone to work together to help the patient maximize their recovery. Many rehabilitation efforts must be coordinated with nursing, such as patient positioning, splinting, and encouraging functional use of the involved extremities. For example, range of motion (ROM) interventions can be done in conjunction with dressing changes to maximize windows if increased analgesia and sedation.
1.3 Patient Assessment and Goals
For any significant burn injury, early assessments should incorporate a functional history that includes an understanding of the patient’s baseline activities and any pre-existing medical conditions that altered function, their social background and responsibilities, and patient-specific goals and concerns. Ongoing treatment should consider these goals and background as the plan of care is determined, and should be mindful of the potential psychological impact and quality of life. Concomitant injuries may also be present, particularly for instances of trauma.
Specific to the burn injury itself, multiple factors should be considered. Characteristics such as burn size (total body surface area), depth of injury, inhalational injury, and pre-existing medical conditions can predict hospital length of stay, surgical needs, and associated general immobility from hospitalization [3,4,5]. Typically, superficial and superficial partial burn injuries will heal spontaneously and do not have the same concerns associated with deeper injuries. However, pain and edema often still require management to aid in short-term functional recovery. Most of the consequences detailed within this chapter are specific to deep partial and full thickness burn injuries in which the body’s capacity to heal spontaneously is compromised, skin grafting is frequently necessary, and more profound scarring and metabolic changes are triggered [6]. The location of burn injury must also be considered—particularly for areas of high function such as the hands and face and skin approximating bony joints. Finally, the source of burn injury can play a role in anticipated rehabilitation needs, particularly in the case of electrical injuries.
1.4 The Impact of Burn Rehabilitation
The impairments of burn injury have features that distinguish them from many other diagnoses with functional consequences. First, the base impairments such as edema, contracture, and hypertrophy can frequently be reduced or eliminated with consistent treatment. As a result, the goals of care are often directed at reducing the impairment (e.g., lack of full hand closure) rather than focusing on long-term adaptations or modified techniques to reduce disability. Second, burn injury impairments are recurrent for a period of months, requiring sustained treatment efforts to avoid ongoing development of scarring complications [7, 8]. As a result, patient and therapy efforts—whether through formal treatment, home exercises, or therapeutic activity—must often continue for long periods of time to prevent development of disability. If successful, many burn survivors have the capacity to return to most if not all pre-morbid activities [9, 10].
Therapy should begin at the time of hospital admission and typically will be ongoing until discharge unless medically contraindicated by specific conditions or concerns regarding early skin graft fragility. Early mobility training including transfer training and progressive ambulation has been found to improve functional outcomes such as ROM and hospital length of stay over more passive approaches focusing on positioning and splinting [11], however, approaches need to be customized case-by-case depending on the specific patient and burn injury. Many patients can discharge from the hospital once wound care can be managed in an outpatient setting if the patient is able to mobilize safely, carry out key aspects of self-care, and perform the required home therapy exercises independently [12]. Consideration should also be made for factors such as the size, location, and functional impact of the wounds, psychological health, social support, transportation to key services, and anticipated compliance with home exercise programs.
Patients with more severe injuries and/or those heavily impacting function may benefit from admission to a dedicated inpatient rehabilitation unit. Inpatient rehabilitation has been found to improve length of stay, ROM, function, and balance specific to burn recovery [13,14,15,16].
1.5 Quality of Life and Long-Term Recovery
A full review of the impact of burn injury long-term on quality of life, psychological factors, and body image is outside the scope of this chapter. However, when treating patients in an acute setting it is important to consider longer term outcomes. While quality of life is impacted by major burn injury, most survivors can return to a high level of health satisfaction even when injuries are present catastrophic [9, 10]. Many patients with burn injury will be able to return to work [10, 17,18,19]. A number of factors may influence their success such as the size, severity, and locations of injury (such as the hands), psychosocial factors, and job-specific factors. As a result of these issues, approximately a quarter of major burn survivors will not return to employment in long-term recovery and many return to alternate employment than their original career [20].
In the immediate period following discharge, it is important to note that at least one longitudinal study has found an association between mental health emergencies and the post-burn period, and mental health support should be considered in all cases of major burn injury [21]. Adjustment and coping with body image changes should also be considered as patients’ transition through stages of care.
2 Functional Complications of Burn Injury
2.1 Contracture
Contracture is defined as a loss of ROM or malalignment of anatomical structures such as joints due to the development of scar tissue and the loss of normal soft tissue length and extensibility. By convention, contracture in burn injury is referred to by the direction of resistance; for example, an elbow flexion contracture impairs elbow extension [22].
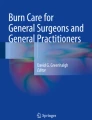
Contracture is a common complication of burn injury and is associated with normal processes of healing, wound contracture, and scarring leading to a loss of normal skin elasticity [7]. A 38.7% incidence of shoulder, elbow, hip, and knee contractures has been reported among survivors of major burn injury at the time of acute care discharge [23]. Relative incidence was related to factors such as length of stay, skin grafting, and the size of burn injury, while the severity of contracture was associated with graft size, amputation, and the presence of inhalational injury [23]. In burn recovery, ROM is measured primarily through goniometry though additional tools have been validated for thumb opposition and compound finger flexion that facilitate tracking the movement of smaller joints less amenable to goniometry use (Fig. 28.1) [24,25,26].

Compound finger flexion using distance between the fingertip and palmar crease as a measurement of finger ROM at the metacarpophalangeal and interphalangeal joints. Source: Ellis and Bruton, 2002 [25]
One highly useful concept in understanding the potential impact of scar contracture is that of cutaneous functional units (CFUs) [27]. Under normal circumstances, uninjured skin allows for joint motion through a process of elongation and recoil. Intuitively, skin directly overlying a bony joint undergoes this process of stretching during motion; however, the research of Richard et al. has skin is recruited from a wide field surrounding the joint. For example, in the majority of individuals, full shoulder abduction is associated with skin movement and stretching to the level of the umbilicus in the majority of individuals (Fig. 28.2). The serial recruitment of this available pool of normal soft tissue segments—or CFUs —allows for full joint motion without skin trauma and is critical to normal function.

Cutaneous functional units . Skin markings are spaced at 2 in. increments on the anterior torso. The image to the left is a double exposure photograph demonstrating the movement of markings indicating skin recruitment during shoulder abduction. The image on the right identifies the size of the soft tissue recruitment in normal individuals; the majority of the individuals tested (14 of 20) recruited soft tissue to at least the umbilicus. Source: Richard et al., 2009 [27]
Following burn injury, this pliable skin is replaced with scar tissue with reduced elasticity. Not surprisingly, the volume of CFUs affected by burn injury has shown value in predicting the development of burn scar contracture in survivors [28]. As a result, burn rehabilitation providers should be mindful of not only the impact of local injury to a joint, but the compound effect of scarring to the pool of soft tissue surrounding the joint in a wider area involved in full joint motion. The risks of developing specific issues must also be considered, such as webbing between digits, microstomia (loss of opening volume of the mouth), ectropion (inversion of the eye lid), and lagophthalmos (incomplete eyelid closure) [6, 29].
Frequently, the methods employed for patients at varying stages of recovery need to evolve over time from the onset of injury. In early stages , techniques must accommodate bulky dressings, acute pain, ongoing medical interventions such as central lines, and patients with impaired level of consciousness and deconditioning. In later stages, these factors lessen, however, as patients regain independence contracture prevention methods may become more difficult to tolerate and may compete with functional use of limbs, but can be replaced with more active and functional techniques of restoring and maintaining ROM.
2.1.1 Mobilization
Early mobilization is key to limit the impact of bed rest, reduce adverse events, and to begin the process of functional recovery and contracture prevention. Specific to the post-grafting period, mobilization must balance concerns for early graft loss with the areas above. In many cases, surgeons will require a period of immobilization prior to resuming activity. Early post-operative mobilization has been proposed, but medical literature to guide specific decision-making are limited [30, 31]. Recent practice guidelines have been proposed from the burn rehabilitation community regarding early ambulation for patients with smaller grafts (less than 300 cm2) which are not overlying joints and that can be effectively braced and have pressure dressings applied and can serve as a starting point for team decisions regarding early post-operative therapy [30].
2.1.2 Positioning
Patient positioning can be an important tool in the prevention of contracture during the acute phase of care. The body area affected by the burn should be positioned opposite the direction of potential burn scar contracture. Positioning must also consider the expected “position of comfort” in a setting of trauma and pain—most often the fetal position—as well as the impact of immobility and bed rest. Practice guidelines exist to serve as an effective starting point for considering positioning though individual scenarios and injury patterns should be considered in all cases for specific prescriptions of care [32] (Fig. 28.3).

Clinical practice guidelines for joint positioning following burn injury. Source: Serghiou et al., 2016 [32]
2.1.3 Splinting
Splinting is frequently used to provide prolonged low-load stretching, particularly during periods of early graft fragility, reduced level of consciousness, but also with focused application in later care. A large range of splints have been employed in burn recovery to prevent and treat losses in ROM through prolonged, passive stretching, though scientific data supporting use of specific splint designs is limited, as are outcomes studies evaluating specific approaches and prescriptions of use [33,34,35,36]. While there are theoretical concerns regarding the influence of prolonged stretch on the development of contracture during wound healing, recent analyses have found substantially decreased odds ratios of developing contracture through splint usage as a therapy tool [37, 38].
2.1.4 Stretching and Scar Massage
Mechanical stretching and massage of scar tissue to improve extensibility are also traditional approaches to burn-associated contracture. Like other interventions, specific medical literature to guide technique and outcomes are limited but suggest benefit for burn recovery [39, 40]. Stretching has the theoretical advantages of being focused on specific areas of ROM losses, progressive throughout a treatment to continually advance ROM gains, and can be integrated into functional or recreational activities over time. Scar massage is typically deferred for a few weeks following skin grafting to prevent early graft shearing or superficial injury, but a number of techniques exist as potential tools once skin resilience has improved.
2.1.5 Functional Impact of Contracture
The specific functional impairment from contracture remains a complex issue. At face value, the basic relationship is simple—as ROM decreases, impairment is expected to increase. However, injuries of some locations on the body (e.g., hands) have much larger functional implications than a simple size and depth of burn for another location (e.g., torso). Predicting the impact of specific contractures is also challenged by the potential for multi-joint ROM losses leading to compound movement issues [41]. Finally, the functional needs of individual patients and baseline ROM may also vary.
2.2 Edema
Inflammation and wound healing lead to formation of edema particularly in the acute phase of care. Functionally, this can hinder mobility and cause pain particularly in dependent areas and can factor into contracture [42]. Elevation of dependent limbs above the heart can reduce edema and can be initiated early post-injury, and edema in the head and face can be managed by elevating the head of the bed. Compressive dressings and splinting can reduce edema while preventing contracture and become increasingly important for the lower extremities as patients mobilize [43]. Edema can be particularly limiting in the setting of hand injuries, and early graded pressure approaches can improve pain and ROM. In later stages, compression gloves can be employed. Active muscle contraction and functional use of the hand should be encouraged to promote edema mobilization.
2.3 Scar Hypertrophy
Scar formation is common following burn injury and is associated with many factors ranging from depth of injury, complications, age, and genetic background [44]. In many cases, scarring becomes hypertrophic, with progressive increases in scar height and thickness, altered pigmentation, erythema, and reduced pliability. During the acute phase of care, hypertrophic scarring is typically not present given the timeframe of development, however, acute care rehabilitation team members should be aware of the fundamentals of burn scar hypertrophy and its management.
Multiple measurement tools are available though serial measurements may be challenging due to the slow rate of change and the need to establish reproducible locations for measurement particularly in the setting of larger burn injuries [44, 45]. The Vancouver Scar Scale is one of the most studied in the setting of burn (Fig. 28.4) [46, 47].

The modified Vancouver scar scale . Source: Nedelec et al., 2008 [47]
The two primary means of treatment are custom pressure garments and silicone gels and sheets. Pressure garments influence the collagen remodeling phase of wound healing. While the exact mechanism of action is unknown, it may be related to impact on local hydration, circulation, or inflammation [48]. Recent reviews of the available medical literature have found that pressure therapy is effective for scar height and erythema, less clearly associated with improvements in scar pliability and joint range of motion, and less likely to impact pigmentation or scar maturation [8]. Pressure garments should be custom fitted, employed as soon as wound healing allows application without adverse effect on dressings or injury from shearing, and worn 23 h per day for 12 months or until scar is mature [8].
Silicone is hypothesized to mitigate hypertrophy through mechanisms such as occlusion and hydration of the skin [49]. Recent practice guidelines for the use of silicone gels and sheets have noted the following: silicone should be applied in cases likely to form hypertrophy scars once the wound has re-epithelialized, the benefit is likely only for immature scars, and silicone gels may have reduced adverse reactions compared to gel sheets [50].
3 Skin Physiology Following Burn Injury
The skin is the largest organ in the human body, and it plays a range of physiological roles including the sense of touch, temperature regulation, and moisturization of the skin. The majority of these functions occur through dermis-derived structures that are compromised with deep tissue injury and which typically remain impaired despite split thickness or sheet grafting. Long-term physiological skin changes from deep dermal injury should be considered in early recovery and patient education.
The loss of distal nerve endings in the dermis leads to an increased threshold for detecting light touch, cold, and heat and a subsequent loss of perceived skin sensation and these changes typically persist long term [51, 52]. Temperature regulation occurs through the skin both through vascular shunting of blood via vasodilation and constriction as well as sweating and piloerection. Following skin grafting, these processes remain impaired with consequent decreased heat and cold tolerance relative to the size of skin injured [51, 53] though heat acclimation exercises may improve heat tolerance over time [54]. This is of particular importance given the benefits of strength training and aerobic conditioning in burn recovery [55].
Superficially, the loss of sebaceous glands and oil production may seem trivial, but problems with pruritis, dry skin, and need for artificial lubrication through lotion remain some of the most common long-term complaints following major burn injury [52]. Beyond the need for early education, alterations in skin oil may need to be considered for activities and employment that are accompanied by exposure to chemical irritants, dry heat, or cleaning materials.
4 Burn-Specific Complications
4.1 Peripheral Nerve Injury
The incidence of peripheral nerve injury in burn injury ranges widely in the medical literature depending on the inclusion criteria regarding the severity of burn injury [56, 57]. In those categorized as major burn injury, research has found an incidence of 11% and associations with larger burns, more days on mechanical ventilation, increased surgical requirements, and longer periods of hospitalization [56].
Focal peripheral nerve injury typically occurs in the region of the burn injury, but can also arise as a consequence of critical illness, pressure from positioning or dressings, edema, or compartment syndrome. Focal injury incidence typically follows that of entrapment neuropathies, with the median, ulnar, and peroneal nerves most often at-risk and the upper extremity a more common site than the lower [56,57,58].
4.2 Heterotopic Ossification
Heterotopic ossification is the formation of pathological, ectopic bone in soft tissue and it is associated with a wide range of conditions ranging from spinal cord injury and traumatic brain injury to bony fractures and joint replacement surgeries. In the setting of burn, it is a rare complication associated with larger total body surface area of injury, and most often occurring adjacent to the elbow joint [59]. While rare, the rehabilitation implications of heterotopic ossification can be severe, with patients experiencing increased pain, loss of ROM, and nerve entrapment particularly involving the ulnar nerve. These changes may often be first noted during therapy interventions. Described medical interventions for prevention and treatment have included non-steroidal anti-inflammatory drugs, bisphosphonates, and radiation, and many patients require surgical resection of heterotopic ossification once the process has matured and the risk of recurrence has diminished months after onset.
Specific to rehabilitation, management of heterotopic ossification is ill defined. Early studies and scientific theories raised concerns that early, aggressive mobilization may be associated with the development and progression of heterotopic ossification [60]. However, in many cases the absence of early mobilization in the at-risk population would be expected to lead to soft tissue contracture and, once present, heterotopic ossification can cause severe upper extremity disability present for prolonged periods before patients can become candidates for surgery. Given these competing demands, there may be a role for ongoing mobilization despite concerns with heterotopic ossification, but the timing, intensity, and safety parameters of doing so remain unclear [60,61,62].
4.3 Electrical
Electrical injuries can cause all of the complications and therapy concerns discussed in this chapter, but due to the potential for deep tissue injury from electrical current travelling through the body can cause a wide range of additional pathology with functional implications. Electrical injury is associated with fourfold increased risk of peripheral nerve injury, spinal cord injury and dysfunction, increased rates of limb amputation, ophthalmological complications including cataract formation, and a wide range of neurological and psychological manifestations [56, 63,64,65,66,67,68].
Complicating these issues is the fact that in many cases development of complications can continue to progress for weeks or months following injury. This may be due to the varied nature of the injury itself, with trauma occurring not only from thermal energy, but also due to vascular injury and pathological changes at a cellular or subcellular level [69], such as lasting cell membrane damage and protein denaturation. In addition—and likely also due to the unusual nature of damage from electrical injury—routine medical testing may fail to identify focal pathology [70]. As a result, rehabilitation providers should have a low index of suspicion for electrical injury-associated complications both at onset and over time, and consider the wide range of potential areas of tissue injury when reviewing patient complaints.
5 Summary
Early rehabilitation efforts are a key component of acute burn management. Burn caregivers should be aware of the short- and long-term impact of wound maturation and scarring and the consequences for functional recovery and quality of life, as well as techniques for preventing and treating burn-associated impairments. Successful programs should consider an evolution of recovery from the intensive care unit to the community and incorporate support and planning for sustained prevention of complications and long-term activity goals.
Summary Box
Early rehabilitation efforts are a key component of acute burn management. Care providers must consider both short- and long-term implications of wound healing and scar maturation as well as specific complications of burn that carry functional and quality of life implications. This chapter provides an overview of acute care therapy and rehabilitation including topics such as:
-
Patient assessment and goals
-
The impact of burn rehabilitation
-
Quality of life and long-term recovery
-
Functional complications of burn injury: contracture, edema, and scar hypertrophy
-
Skin physiology following burn injury
-
Burn-specific complications: peripheral nerve injury, heterotopic ossification, electrical injury
References
Parry I, Esselman PC. Rehabilitation Committee of the American Burn A. Clinical competencies for burn rehabilitation therapists. J Burn Care Res. 2011;32:458–67.
Parry I, Forbes L, Lorello D, Benavides L, Calvert C, Hsu SC, et al. Burn rehabilitation therapists competency tool-version 2: an expansion to include long-term rehabilitation and outpatient care. J Burn Care Res. 2017;38(1):e261–e8.
Tredget EE, Shankowsky HA, Taerum TV, Moysa GL, Alton JD. The role of inhalation injury in burn trauma. A Canadian experience. Ann Surg. 1990;212(6):720–7.
Burton KR, Sharma VK, Harrop R, Lindsay R. A population-based study of the epidemiology of acute adult burn injuries in the Calgary Health Region and factors associated with mortality and hospital length of stay from 1995 to 2004. Burns. 2009;35(4):572–9.
Thombs BD, Singh VA, Halonen J, Diallo A, Milner SM. The effects of preexisting medical comorbidities on mortality and length of hospital stay in acute burn injury: evidence from a national sample of 31,338 adult patients. Ann Surg. 2007;245(4):629–34.
Esselman PC, Thombs BD, Magyar-Russell G, Fauerbach JA. Burn rehabilitation: state of the science. Am J Phys Med Rehabil. 2006;85:383–413.
Nedelec B, Ghahary A, Scott PG, Tredget EE. Control of wound contraction. Basic and clinical features. Hand Clin. 2000;16:289–302.
Sharp PA, Pan B, Yakuboff KP, Rothchild D. Development of a best evidence statement for the use of pressure therapy for management of hypertrophic scarring. J Burn Care Res. 2016;37(4):255–64.
Anzarut A, Chen M, Shankowsky H, Tredget EE. Quality-of-life and outcome predictors following massive burn injury. Plast Reconstr Surg. 2005;116(3):791–7.
Holavanahalli RK, Helm PA, Kowalske KJ. Long-term outcomes in patients surviving large burns: the musculoskeletal system. J Burn Care Res. 2016;37(4):243–54.
Deng H, Chen J, Li F, Li-Tsang CW, Liu Q, Ma X, et al. Effects of mobility training on severe burn patients in the BICU: a retrospective cohort study. Burns. 2016;42(7):1404–12.
Choo B, Umraw N, Gomez M, Cartotto R, Fish JS. The utility of the functional independence measure (FIM) in discharge planning for burn patients. Burns. 2006;32(1):20–3.
Schneider JC, Qu HD, Lowry J, Walker J, Vitale E, Zona M. Efficacy of inpatient burn rehabilitation: a prospective pilot study examining range of motion, hand function and balance. Burns. 2012;38:164–71.
Sliwa JA, Heinemann A, Semik P. Inpatient rehabilitation following burn injury: patient demographics and functional outcomes. Arch Phys Med Rehabil. 2005;86:1920–3.
Spires MC, Bowden ML, Ahrns KS, Wahl WL. Impact of an inpatient rehabilitation facility on functional outcome and length of stay of burn survivors. J Burn Care Rehabil. 2005;26:532–8.
DeSanti L, Lincoln L, Egan F, Demling R. Development of a burn rehabilitation unit: impact on burn center length of stay and functional outcome. J Burn Care Rehabil. 1998;19:414–9.
Schneider JC, Bassi S, Ryan CM. Barriers impacting employment after burn injury. J Burn Care Res. 2009;30:294–300.
Schneider JC, Bassi S, Ryan CM. Employment outcomes after burn injury: a comparison of those burned at work and those burned outside of work. J Burn Care Res. 2011;32:294–301.
Quinn T, Wasiak J, Cleland H. An examination of factors that affect return to work following burns: a systematic review of the literature. Burns. 2010;36(7):1021–6.
Mason ST, Esselman P, Fraser R, Schomer K, Truitt A, Johnson K. Return to work after burn injury: a systematic review. J Burn Care Res. 2012;33(1):101–9.
Mason SA, Nathens AB, Byrne JP, Ellis J, Fowler RA, Gonzalez A, et al. Association between burn injury and mental illness among burn survivors: a population-based, self-matched, longitudinal cohort study. J Am Coll Surg. 2017;225(4):516–24.
Richard R, Baryza MJ, Carr JA, Dewey WS, Dougherty ME, Forbes-Duchart L, et al. Burn rehabilitation and research: proceedings of a consensus summit. J Burn Care Res. 2009;30:543–73.
Goverman J, Mathews K, Goldstein R, Holavanahalli R, Kowalske K, Esselman P, et al. Adult contractures in burn injury: a burn model system National Database Study. J Burn Care Res. 2016;42:1067.
Edgar D, Finlay V, Wu A, Wood F. Goniometry and linear assessments to monitor movement outcomes: are they reliable tools in burn survivors? Burns. 2009;35:58–62.
Ellis B, Bruton A. A study to compare the reliability of composite finger flexion with goniometry for measurement of range of motion in the hand. Clin Rehabil. 2002;16:562–70.
Parry I, Walker K, Niszczak J, Palmieri T, Greenhalgh D. Methods and tools used for the measurement of burn scar contracture. J Burn Care Res. 2010;31(6):888–903.
Richard RL, Lester ME, Miller SF, Bailey JK, Hedman TL, Dewey WS, et al. Identification of cutaneous functional units related to burn scar contracture development. J Burn Care Res. 2009;30:625–31.
Parry I, Sen S, Sattler-Petrocchi K, Greenhalgh D, Palmieri T. Cutaneous functional units predict shoulder range of motion recovery in children receiving rehabilitation. J Burn Care Res. 2017;38(2):106–11.
Esselman PC. Burn rehabilitation: an overview. [Review] Arch Phys Med Rehabil. 2007;88:S3–6.
Nedelec B, Serghiou MA, Niszczak J, McMahon M, Healey T. Practice guidelines for early ambulation of burn survivors after lower extremity grafts. J Burn Care Res. 2012;33(3):319–29.
Lorello DJ, Peck M, Albrecht M, Richey KJ, Pressman MA. Results of a prospective randomized controlled trial of early ambulation for patients with lower extremity autografts. J Burn Care Res. 2014;35(5):431–6.
Serghiou MA, Niszczak J, Parry I, Richard R. Clinical practice recommendations for positioning of the burn patient. Burns. 2016;42(2):267–75.
Richard R, Staley M, Miller S, Warden G. To splint or not to splint—past philosophy and present practice: part I. [Review] J Burn Care Rehabil. 1996;17:444–53.
Richard R, Staley M, Miller S, Warden G. To splint or not to splint: past philosophy and current practice—part II. J Burn Care Rehabil. 1997;18:64–71.
Richard R, Staley M, Miller S, Warden G. To splint or not to splint—past philosophy and present practice: part III. J Burn Care Rehabil. 1997;18:251–5.
Richard R, Ward RS. Splinting strategies and controversies. [Review] J Burn Care Rehabil. 2005;26:392–6.
Schouten HJ, Nieuwenhuis MK, van Zuijlen PP. A review on static splinting therapy to prevent burn scar contracture: do clinical and experimental data warrant its clinical application?. [Review] Burns. 2012;38:19–25.
Richard R, Dewey S, Parry I, Jones J. Letter to the editor. Burns. 2013;39(3):539–41.
Zhang Y-T, Li-Tsang CWP, Au RKC. A systematic review on the effect of mechanical stretch on hypertrophic scars after burn injuries. Hong Kong J Occup Ther. 2017;29(Suppl. C):1–9.
Godleski M, Oeffling A, Bruflat AK, Craig E, Weitzenkamp D, Lindberg G. Treating burn-associated joint contracture: results of an inpatient rehabilitation stretching protocol. J Burn Care Res. 2013;34(4):420–6.
Korp K, Richard R, Hawkins D, Renz E, Blackbourne LH. Refining “functional” in burn recovery outcomes. J Burn Care Res. 2011;32:S160.
Barillo D, Paulsen SM. Management of burns to the hand. Wounds. 2003;15(1):4–9.
Staley MJ, Richard RL. Use of pressure to treat hypertrophic burn scars. Adv Wound Care. 1997;10(3):44–6.
Dunkin CS, Pleat JM, Gillespie PH, Tyler MP, Roberts AH, McGrouther DA. Scarring occurs at a critical depth of skin injury: precise measurement in a graduated dermal scratch in human volunteers. Plast Reconstr Surg. 2007;119(6):1722–32; discussion 33–4.
Tyack Z, Simons M, Spinks A, Wasiak J. A systematic review of the quality of burn scar rating scales for clinical and research use. Burns. 2012;38(1):6–18.
Nedelec B, Shankowsky HA, Tredget EE. Rating the resolving hypertrophic scar: comparison of the Vancouver Scar Scale and scar volume. J Burn Care Rehabil. 2000;21(3):205–12.
Nedelec B, Correa JA, Rachelska G, Armour A, LaSalle L. Quantitative measurement of hypertrophic scar: intrarater reliability, sensitivity, and specificity. J Burn Care Res. 2008;29(3):489–500.
Bloemen MC, van der Veer WM, Ulrich MM, van Zuijlen PP, Niessen FB, Middelkoop E. Prevention and curative management of hypertrophic scar formation. Burns. 2009;35(4):463–75.
Mustoe TA. Evolution of silicone therapy and mechanism of action in scar management. Aesthet Plast Surg. 2008;32(1):82–92.
Nedelec B, Carter A, Forbes L, Hsu SC, McMahon M, Parry I, et al. Practice guidelines for the application of nonsilicone or silicone gels and gel sheets after burn injury. J Burn Care Res. 2015;36(3):345–74.
Nedelec B, Quanzhi H, Ismahen S, Choiniere M, Beauregard G, Dykes RW. Sensory perception and neuroanatomical structures in normal and grafted skin of burn survivors. Burns. 2005;31:817–30.
Holavanahalli RK, Helm PA, Kowalske KJ. Long-term outcomes in patients surviving large burns: the skin. J Burn Care Res. 2010;31:631–9.
Davis SL, Shibasaki M, Low DA, Cui J, Keller DM, Wingo JE, et al. Sustained impairments in cutaneous vasodilation and sweating in grafted skin following long-term recovery. J Burn Care Res. 2009;30(4):675–85.
Schlader ZJ, Ganio MS, Pearson J, Lucas RA, Gagnon D, Rivas E, et al. Heat acclimation improves heat exercise tolerance and heat dissipation in individuals with extensive skin grafts. J Appl Physiol (1985). 2015;119(1):69–76.
Nedelec B, Parry I, Acharya H, Benavides L, Bills S, Bucher JL, et al. Practice guidelines for cardiovascular fitness and strengthening exercise prescription after burn injury. J Burn Care Res. 2016;37(6):e539–e58.
Kowalske K, Holavanahalli R, Helm P. Neuropathy after burn injury. J Burn Care Rehabil. 2001;22(5):353–7; discussion 2.
Khedr EM, Khedr T, el-Oteify MA, Hassan HA. Peripheral neuropathy in burn patients. Burns. 1997;23:579–83.
Gabriel V, Kowalske KJ, Holavanahalli RK. Assessment of recovery from burn-related neuropathy by electrodiagnostic testing. J Burn Care Res. 2009;30(4):668–74.
Evans EB. Heterotopic bone formation in thermal burns. Clin Orthop Relat Res. 1991;263:94–101.
Casavant AM, Hastings H 2nd. Heterotopic ossification about the elbow: a therapist’s guide to evaluation and management. [Review] J Hand Ther. 2006;19:255–66.
Rachel K, Nichola F, Dale E, Denis V, Elad O, Josef H, et al. The development and impact of heterotopic ossification in burns: a review of four decades of research. Scars Burn Heal. 2017;3:2059513117695659.
Coons D, Godleski M. Range of motion exercises in the setting of burn-associated heterotopic ossification at the elbow: case series and discussion. Burns. 2013;39(4):e34–8.
Ko SH, Chun W, Kim HC. Delayed spinal cord injury following electrical burns: a 7-year experience. Burns. 2004;30(7):691–5.
Lammertse DP. Neurorehabilitation of spinal cord injuries following lightning and electrical trauma. NeuroRehabilitation. 2005;20(1):9–14.
Tarim A, Ezer A. Electrical burn is still a major risk factor for amputations. Burns. 2013;39(2):354–7.
Handschin AE, Vetter S, Jung FJ, Guggenheim M, Künzi W, Giovanoli P. A case-matched controlled study on high-voltage electrical injuries vs thermal burns. J Burn Care Res. 2009;30(3):400–7.
Hsueh YY, Chen CL, Pan SC. Analysis of factors influencing limb amputation in high-voltage electrically injured patients. Burns. 2011;37(4):673–7.
Singerman J, Gomez M, Fish JS. Long-term sequelae of low-voltage electrical injury. J Burn Care Res. 2008;29(5):773–7.
Lee RC. Injury by electrical forces: pathophysiology, manifestations, and therapy. Curr Probl Surg. 1997;34(9):677–764.
Fish JS, Theman K, Gomez M. Diagnosis of long-term sequelae after low-voltage electrical injury. J Burn Care Res. 2012;33(2):199–205.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2020 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Godleski, M., Umraw, N.C. (2020). Rehabilitation Management During the Acute Phase. In: Jeschke, M., Kamolz, LP., Sjöberg, F., Wolf, S. (eds) Handbook of Burns Volume 1. Springer, Cham. https://doi.org/10.1007/978-3-030-18940-2_28
Download citation
DOI: https://doi.org/10.1007/978-3-030-18940-2_28
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-18939-6
Online ISBN: 978-3-030-18940-2
eBook Packages: MedicineMedicine (R0)