
Abstract
This chapter is an overview of neuropsychiatric and mental health research and consequences of the Chernobyl catastrophe in children and adolescents. These effects derive from both biological effects of radiation exposure and psychosocial effects of trauma and displacement. With respect to radiological factors, several scenarios of radiation exposure related to children and adolescents will be discussed: (1) exposure in utero, (2) exposure in childhood and adolescence, and (3) particular overexposure of the thyroid to radiation and the subsequent incidence of thyroid cancer. Prenatal exposure has had more objective studies than other exposure types, but findings remain controversial. Among some of the children, the existing data testify to subtle signs of intellectual impairment that are reflected, for example, in a larger than the usual gap between verbal and nonverbal IQ indices. We then discuss the psychosocial effects of trauma and the research that shows children from contaminated territories have many signs of mental health problems, including anxiety, psychosomatic disturbances, and autonomic dysfunction (dysautonomia). After consideration of the mental health needs of children and adolescents following the radiation emergency of the Chernobyl catastrophe, we discuss possible strategies for improving the mental healthcare and psychiatric rehabilitation for these individuals.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Prenatal irradiation
- Brain damage
- Chernobyl catastrophe
- Ionizing radiation
- Children
- Adolescents
- Mental health
1 Introduction
The Chernobyl catastrophe, also referred to as the Chernobyl disaster and/or accident, occurred on April 26, 1986, at the Chernobyl Nuclear Power Plant (NPP) Unit IV near Pripyat city, which was then part of the Ukrainian Soviet Socialist Republic of the Soviet Union (USSR). The Chernobyl catastrophe dominated the energy accident category, as the most disastrous nuclear power plant accident in history, both in terms of cost and casualties. It was classified as a level 7 event (the maximum level) on the International Nuclear Event Scale. More than 300 MCi (Megacuries) or 11·1018 decays per second (or Becquerels, Bq) of radioactive materials were released from the reactor core, causing the contamination of 50,500 km2 area of Ukraine, where over 2.4 million people lived in 2218 settlements (Serdiuk et al. 2011). Among the 134 cases of acute radiation sickness, 28 died within the first 4 months of the accident (UNSCEAR 2000).
In addition to the central part of Ukraine, the southeastern regions of Belarus and some regions of European Russia underwent the highest level of contamination. These territories were inhabited by 17.5 million people, including 2.5 million children under the age of 7 years. Over 600,000 people took part in the 1986–1989 cleanup work (“liquidators”). By the end of 1986, a total of 116,000 inhabitants were evacuated from 188 settlements (Serdiuk et al. 2011).
Thus, the Chernobyl catastrophe was not only the largest nuclear accident in the world but also a catastrophic event which was, unfortunately, followed by a series of other highly stressful situations for the same population, including the collapse of the USSR, which happened 5 years after the disaster.
According to the report, Thirty Years of Chernobyl: Lessons and Prospects (Zablotska 2016) based on Parliamentary hearings and approved by the Cabinet of Ministers of the Ukraine, 2293 settlements located in the territories of 77 districts of 12 distinct regions were radioactively contaminated. As of January 1, 2016, there are 1,961,904 citizens in Ukraine who have been classified as victims of the Chernobyl catastrophe, including 418,777 children and 108,530 disabled adults.
Epidemiological studies at first reported increased long-term risks of physical diseases in those exposed as children and adolescents. Soon afterward, the short- and long-term consequences for mental health issues started to attract increased attention. In fact, mental health effects appear to be the most significant public health consequence of the accident in the three most contaminated countries: Ukraine, Belarus, and the Russian Federation (Zablotska 2016). In 2006, the health committee of the UN Chernobyl Forum recognized the mental health consequences as the largest public health issue and social burden of the Chernobyl catastrophe. The committee outlined the main problems: (1) stress-related disorders, (2) effects on the developing brain, (3) organic brain damage in the Chernobyl catastrophe cleanup workers (liquidators), and (4) suicides (Bennett et al. 2006).
In spite of the fact that adverse long-term psychological, psychiatric, and neuropsychiatric consequences of the Chernobyl catastrophe are generally recognized, their etiology and mechanisms are still controversial (Bennett et al. 2006; Loganovsky 2009; Bromet et al. 2011a; Bromet 2012). The main controversy pertains to the differential impact of ionizing radiation versus the psychosocial stressors of the ongoing trauma on neuropsychological functioning, as well as the nature of their interaction. Focusing on the radiological factor, four scenarios of radiation exposure related to children and adolescents have been examined: (1) exposure in utero, (2) exposure in childhood and adolescence, (3) congenital malformations of the nervous system in descendants of inhabitants of radioactively contaminated territories (liquidators and evacuees), and (4) particular overexposure of the thyroid to radiation and the resulting incidence of thyroid cancer.
To this day, the majority of pertinent studies have been focused on the mental health, neuropsychiatric issues, and neurocognitive deficits among prenatally exposed individuals. Prenatally exposed persons have thus been the most wellstudied group so far. Since they were registered in a timely fashion, they have maintained low rates of study attrition. On the other hand, fewer investigations were related to mental health and neuropsychiatric disorders among the so-called Chernobyl children—those exposed in childhood and adolescence—or Chernobyl grandchildren, descendants of survivors. Moreover, as we will discuss below, due to the difficulties inherent in this research, the existing data for all these exposure types has been contradictory, and estimates of the prevalence of disorders have been hampered by challenges in longitudinally following these cohorts.
2 Prenatal Radiation Exposure
The developing brain is extremely sensitive to negative physical, chemical, and even psychosocial influences especially during the so-called vulnerable periods, when critical neurodevelopment processes like proliferation, migration, differentiation, synaptogenesis, dendritic arborization, pruning, myelination, and apoptosis are occurring (Rice and Barone Jr. 2000; Weinstock 2008). Within the set of hazardous environmental factors that may lead to neurotoxic effects, radioactive irradiation is one of the most toxic and can result in structural brain changes, behavioral difficulties, and cognitive dysfunctions (Rice and Barone Jr. 2000). This is well established in animal studies and confirmed by observations in humans, though the human studies are often challenged due to the complexities of establishing causal links with certainty.
An important example involves persons exposed in utero to the atomic bombings of Hiroshima and Nagasaki, especially during the 8th–15th and 16th–25th weeks of gestation. In these individuals, severe intellectual disability was shown to occur including reduced intelligence quotient (IQ) scores, poor school performance, microcephaly, and seizures (ICRP 1986; Valentin 2003). The occurrence of intellectual disability was observed with intrauterine exposure during the 8th–15th weeks of gestation at doses of 0.06–0.31 Gy (Gray [Gy] is a unit of absorbed radiation dose equal to absorption of 1 J of radiation energy per kilogram of ordinary non-biological matter) and during the 16th–25th weeks of gestation with an exposure dose of 0.28–0.87 Gy (Otake 1996). There also seemed to be an increased incidence of schizophrenia in those prenatally irradiated in the bombing of Nagasaki. However, as we discuss below, the role of ionizing radiation in causing an increase incidence of schizophrenia remains controversial (Imamura et al. 1999).
The Sievert (Sv), another unit for measuring radiation doses, is related to the Gray but accounts for the special nature of the interaction of biological tissue with radiation. It is defined as the deposit of 1 J of radiation energy per kilogram of biological tissue. In cases of external uniform gamma-irradiation (as in Chernobyl), the Sv is practically the same as the Gy.
A 1 Sv dose of irradiation, during the 8th–15th weeks of gestation, is believed to result in an IQ decrease of approximately 30 points. Effects below 100 mSv have not been found, but each additional 100 mSv above 100 mSv of prenatal exposure leads to a decrease of approximately 3 IQ points. However, during 16th–25th weeks, there is a lesser effect (European Commission 1998; ICRP 2000).
Therefore, three proven human neuroembryological effects of irradiation are (1) cognitive deficits that result in a dose-related intellectual decline and, in extreme cases, can lead to severe intellectual disability; (2) microcephaly; and (3) seizures. The IQ decrease depends on the development phase of the brain at the time of the irradiation. Other potential neuroembryological effects (e.g., schizophrenia) have been identified but may require further research to definitively identify their causal relation with prenatal ionizing radiation.
2.1 Research on In Utero Exposure to Ionizing Radiation
In spite of the principle that the developing brain in utero is extremely sensitive to exposure to any exogenous hazards including low doses of ionizing radiation, the extent of the effects of the prenatal exposure during the Chernobyl catastrophe on brain damage and its subsequent mental health consequences remain an area of scientific controversy. As we mentioned above, it is sometimes difficult to establish a direct causal link between radiation exposure and brain structure or subsequent behavior in human subjects. Moreover, the mental health effects of the ongoing psychosocial and traumatic exposures from a mass disaster like Chernobyl can make it difficult to separate the direct effects of radiation from the effects of the post-disaster psychosocial stressors. Later in the chapter, we discuss the psychosocial impacts. Here, we will discuss selected examples of the literature that support or question the radio-neuroembryological effects of the Chernobyl catastrophe. We present these selected studies in Table 10.1. The heading “Neuropsychiatric outcome” in that table denotes any identified neuropsychological dysfunction, while “Radiation effect” denotes evidence for the identification of the specific role of radiation in this damage. In Table 10.1 the conditional effect strength is as follows: “-” NO effect, “+/-” doubtful effect, “+” low effect, “++” moderate effect, and “+++” strong effect. Assessment of effect strength was conducted by the authors of this chapter.
The World Health Organization (WHO) in 1992–1995 implemented a pilot project Brain Damage in Utero within the International Program on the Health Effects of the Chernobyl Accident (IPHECA) (entry 1 in Table 10.1). Analysis of the results in Belarus, the Russian Federation, and Ukraine indicated that (1) the prevalence of mild intellectual disability in children exposed in utero was higher than in the control groups; (2) there was a trend in the incidence of emotional and behavioral disorders in children exposed in utero; and (3) there was an increased prevalence of possible neuropsychiatric disorders in parents of prenatally exposed babies (Souchkevitch and Tsyb 1996). However, these results were not definitively established, and the possible relationship between neuropsychiatric effects and doses of prenatal radiation exposure remained unclear.
In a French-German initiative to explore the consequences of the Chernobyl catastrophe (French-German Initiative for Chernobyl, FGI) (2 in Table 10.1), children who were prenatally exposed were assessed at the age of 10–12 years, and they showed the following abnormalities: decreased verbal IQ; high frequency of low-amplitude and epileptiform patterns on electroencephalogram (EEG), with left-hemispheric lateralization of dysfunction; increase of delta and beta power and decrease of alpha and theta power on EEG; increase in the frequency of mental disorders; autonomic dysfunction; disorders of psychological development; as well as emotional and behavioral disorders. Cerebral dysfunction appeared to be etiologically heterogeneous. In addition, radiation-induced dysfunction of the pituitary-thyroid system was found at a threshold dose of 0.3 Gy to the thyroid gland in utero (Nyagu et al. 1998, 2000, 2002, 2004) (2 in Table 10.1). These results were partly confirmed by Stepanova et al. (1992) (4 in Table 10.1), who reported neurodevelopmental disturbances in about half of those who were exposed in utero but did not demonstrate direct radiation causality.
The studies of prenatally exposed children conducted in Kiev (Ukraine) by Nyagu et al. (1992, 1998, 2000, 2002, 2004) (3 in Table 10.1) and by Loganovskaja and Loganovsky (1999, 2000), Loganovskaja (2005) and Loganovsky et al. (2008, 2011, 2013, 2014) (5 in Table 10.1), as well as those done in Sweden (Almond et al. 2009) (6 in Table 10.1), Finland (Huizink et al. 2007) (7 in Table 10.1), and Norway (Heiervang et al. 2010a) (8 in Table 10.1), identified neuropsychiatric impairments associated with in utero radiation exposure that could indicate the presence of prenatal neurodevelopmental disorders. Moreover, Hatch et al. (2017) (9 in Table 10.1) found smaller head sizes at birth in the cohort of prenatally exposed Ukrainian newborns as a result of the Chernobyl catastrophe. We will discuss some of these findings in greater detail.
In the Swedish cohort (Almond et al. 2009) (6 in Table 10.1), individuals who were exposed in utero during the Chernobyl catastrophe were found to have impaired academic achievement in comparison to the population at large, based on the most complete database of 562,637 people born between 1983 and 1988 in Sweden. Among this group, the highest impairment was found in those exposed between the eighth and 25th weeks of gestation and born in regions with the highest amount of fallout. These results suggest that prenatal exposure causes cognitive impairment at exposure levels that were previously considered safe.
In the Finland (Huizink et al. 2008) (7 in Table 10.1) research, persons irradiated at the second trimester of pregnancy experienced a 2.32-fold higher risk (95% confidence interval, 1.13; 4.72) of depressive symptoms and major depressive disorder according to the DSM-III-R criteria (odds ratio [OR] 2.48; 95% confidence interval, 1.06; 5.7), as well as attention deficit hyperactivity disorder. No association between prenatal impact of the Chernobyl catastrophe and an anxious or an oppositional defiant disorder was revealed. The potential effect of prenatal stress associated with the Chernobyl catastrophe was also surveyed in Finland. Serum cortisol levels in both boys and girls, and testosterone levels in girls were substantially higher for those maternally exposed to Chernobyl in the second trimester of pregnancy, compared to the reference group of nonexposed adolescents. The prenatal impact to the abnormal cortisol level was 3%, whereas contribution of testosterone reached up to 18%. Additionally, there were no differences between the effects at the first or third trimester of pregnancy. The prenatal maternal status therefore can be reflected on the prenatal programming of physiological systems responsible for cortisol and testosterone maintenance (Huizink et al. 2008) (7 in Table 10.1).
There were also observed associations of radiation exposure, from radioiodine, with decreased head and chest circumference (according to the medical records at birth) that are consistent with those observed in the Japanese in utero-exposed atomic bomb survivors (Hatch et al. 2017) (9 in Table 10.1).
In a study in Belarus, children exposed in utero showed higher rates of mental and neuropsychiatric disorders, due to the increased frequency of impedance of mental development against the background of residual brain damage associated with prenatal exposure and dependent on the gestational week at the time of the disaster (Ermolina et al. 1994, 1996) (10 in Table 10.1). A study of the prenatally exposed immigrants from the former USSR to Israel showed scores for hyperactivity and attention deficit hyperactivity disorder that were significantly elevated compared to controls (Bar et al. 2004) (11 in Table 10.1).
On the other hand, in a Ukrainian-American prospective study, 300 persons who were exposed in utero to 15 months after Chernobyl presented no elevated incidence of neurobehavioral or cognitive disorders compared to their 300 nonexposed classmates (Bromet et al. 2011b) (12 in Table 10.1).
Similarly, some expert in the report of the United Nations Scientific Committee on the Effects of Atomic Radiation UNSCEAR (UNSCEAR 2000) came to the conclusion that the decisive role in the origin of borderline intellectual functioning and emotional disorders in children prenatally irradiated in Belarus belongs to unfavorable sociopsychological and sociocultural factors rather than the result of radiation on the developing brain (UNSCEAR 2000) (13 in Table 10.1). We will discuss those sociocultural factors in a later section.
Further research is necessary to assess these disparate results, which may be due to different measurement methods, different locations with different levels of exposure, different timings of the studies, and different research approaches.
2.2 Radioactive Iodine, Thyroid, and IQ
In prospective studies conducted in Ukraine, discrepant scores on IQ (due to the lowering of verbal IQ compared to performance IQ) were found, and they appeared to be a radio-neuroembryological effect of prenatal exposure as a result of the accident at Chernobyl. In their first studies, the authors hypothesized that the damage was in the usually dominant left cerebral hemisphere, especially its cortical-limbic structures (Loganovskaja and Loganovsky 1999). Later work confirmed the disrupted development of the left (dominant) brain hemisphere after prenatal exposure. There were statistically lower general and verbal IQs and a pronounced intellectual discrepancy between verbal and performance IQs in children with prenatal radiation exposure after the Chernobyl catastrophe, compared to the Kiev control group (Loganovskaja 2005; Loganovsky et al. 2008; Loganovsky 2012; Loganovsky and Loganovskaja 2013) (5 in Table 10.1).
Radioactive iodine is one of the isotopes present at the Chernobyl catastrophe, and it can be incorporated into the human body through inhalation and ingestion, where it preferentially accumulates in the thyroid. It thus becomes a concentrated and inner source of radiation. Therefore, the authors examined the relation between the IQ disharmony mentioned above and the thyroid radiation dose in utero of those children (871.3 ± 330.2 mSv; range, 421.3–1281.1 mSv r = 0.7; p = 0.05). Weeks 8–15 and 16–25 are the most critical periods of cerebrogenesis and correspond to the radio-cerebral effects under a purely external exposure, as observed after the atomic bombings at Hiroshima and Nagasaki. However, after the Chernobyl catastrophe, given the fact that thyroid size during the most critical period of cerebrogenesis (i.e., gestation weeks 8–15) is small and thyroid metabolism is at a minimal, there were relatively low fetal radiation doses from the thyroid at that gestational stage. Thus, there were likely no alterations in developmental processes such as neuronal migration. However, at the next critical period of cerebrogenesis (i.e., gestation weeks 16–25), activation of cellular differentiation and intensification of synaptogenesis occur, cerebral cytoarchitectonics takes shape, the main limbic structures develop, and cerebral asymmetry and hemispheric dominance emerge. The growth of thyroid mass and thyroid metabolism now leads to an increase in the in utero thyroid concentration of radioactive iodine and an increase in dose of embryo/fetal radiation, including to the brain. It has therefore been hypothesized that radiosensitivity of a developing brain during this period leads to abnormalities of neuroembryological events and can explain discrepant scores on IQ. Though the developing brain’s radiosensitivity is lower during later periods of gestation (i.e., weeks 26+), the thyroid and fetal prenatal radiation exposures also increase. Thus, it is possible that discrepant scores on IQ could result from thyroid radiation exposures during later parts of gestation (Loganovskaja and Loganovsky 2000; Loganovskaja 2004; Loganovska and Nechayev 2004; Loganovska 2005; Loganovsky et al. 2008).
2.3 Schizophrenia and Radiation Exposure
These results should be considered within the frame of a hypothesis of schizophrenia as a neurodevelopmental disorder associated with radiation exposure (Loganovsky 2009; Loganovsky et al. 2008). A series of publications in radio-neuroembryological support the hypothesis of a possible association of prenatal radiation exposure and excessive schizophrenia risk later in life. Based on morpho-functional changes in the brains of primates, and some behavioral consequences following exposure in utero, radiation-induced schizophrenia has been proposed (Korr et al. 2001; Gelowitz et al. 2002; Schindler et al. 2002; Schmitz et al. 2005; Selemon et al. 2005, 2009; Friedman and Selemon 2010; Selemon and Friedman 2013). This hypothesis has received clinical and epidemiological support from the increased schizophrenia risk after prenatal diagnostic X-ray in the Jerusalem cohort (Gross et al. 2018) and in other studies (Loganovsky and Loganovskaja 2000; Loganovsky et al. 2005, 2008; Loganovskaja and Loganovsky 1999).
The human brain is anatomically, neurochemically, and functionally asymmetric (Flor-Henry 1983). Disrupted development of lateralization and brain asymmetry is an important cause of mental disorders, in particular schizophrenia (Shirakawa et al. 2001). Flor-Henry (1969b) showed that schizophrenia-like reactions are associated with left temporal lobe epilepsy, while right temporal lobe epilepsy was related to affective psychoses (1969a). Also, the left frontotemporal EEG abnormalities following exposure to ionizing radiation in the Chernobyl catastrophe in cleanup workers were associated with schizophrenia-like symptoms. Lastly, an excess of schizophrenia in the Chernobyl exclusion zone was reported.
We also proposed the neural diathesis-stress hypothesis of schizophrenia, in which genetic predisposition to this disorder can be triggered by environmental stressors, such as ionizing radiation (Loganovsky et al. 2005). The diathesis-stress hypothesis is in accord with the role of left-hemispheric frontotemporal dysfunction in schizotypal features. Taken together these observations support the concept of ionizing radiation being a potential risk factor for schizophrenia spectrum disorders (Loganovsky and Loganovskaja 2000; Loganovsky et al. 2005). However, this expected higher risk for schizophrenia has not yet been widely confirmed.
The deleterious effects of the Chernobyl catastrophe have been well established across Europe and as far north as Scandinavia. Results of Norwegian research are especially relevant for an unbiased understanding of the consequences of prenatal brain exposure after the Chernobyl catastrophe, especially in the context of schizophrenia risk. The prenatally irradiated adolescents in Norway have decreased indices of verbal operational memory, verbal learning and memory, information processing speed, and executive function vs. nonexposed cohorts. These deficits may relate to schizophrenia risk. In any case, it must be emphasized that study results from these Norwegian authors provided new and substantial support to the authors’ data on a selective damage to the dominant hemisphere after prenatal radiation exposure due to the Chernobyl catastrophe (Heiervang et al. 2010b, 2011) (8 in Table 10.1). These previously unrecognized neuropsychiatric effects can be related to the relatively short-term effect of radioactive fallout levels which previously had been considered safe (Nowakowski and Hayes 2008).
2.4 Effects of Prenatal Radiation Exposure: Future Research
As indicated by the discussion above, various aspects of the genesis of the neuropsychiatric consequences of Chernobyl have proven extremely controversial. However, the cerebral effects of low doses of ionizing radiation, especially in regard to cerebrovascular disease and cognitive impairment, remain the focus of ongoing research worldwide (Bazyka et al. 2013a, b, 2014, 2015; Loganovsky 2012; Loganovsky and Zdanevich 2013). An increasing pool of data supports the conclusion about high radiosensitivity of the developing central nervous system (CNS). There are several possible mechanisms for these radio-cerebral effects: disrupted neurogenesis in the hippocampus, changes in the gene expression profile, neuro-inflammatory response, neuro-signaling alterations, apoptotic cell death, cell death and injury mediated by secondary damage, “glial-vascular union,” etc. At the same time, the cortical-limbic system seems to be a main target for the radiation-based brain damage where hippocampal neurogenesis dysfunction is crucial (Loganovsky 2009, 2012; Marazziti et al. 2012, 2015, 2016; Picano et al. 2012).
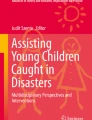
The existing research certainly warrants that all individuals who were prenatally irradiated or exposed within the first year of life after the Chernobyl catastrophe should be carefully monitored. In fact, such a lifetime monitoring of potential neuropsychiatric effects in prenatally irradiated and exposed persons from the age of 0–1 year is continuing in the National Research Center for Radiation Medicine of National Academy of Medical Sciences of Ukraine (NRCRM) in Kiev. At age 23–25, exposed persons still have significantly more neuropsychiatric disorders (see Fig. 10.1), especially paroxysmal disorders including epilepsy and epileptic syndromes, autonomic dysfunction and headache syndromes, dorsalgia, and neurotic and somatoform disorders. There is certainly a potential risk for the neurodevelopmental effects of exposure in utero to result in paroxysmal disorders (including epilepsy), organic mental disorders, demyelinating diseases of the nervous system, and schizophrenia spectrum disorders. The specific neurocognitive deficits, like decrement in verbal IQ, left temporal lobe epilepsy, and left frontotemporal cerebral lesions, point toward developmental disorders of the dominant (left) brain hemisphere. Moreover, in-utero-exposed persons were found to have a more severe and increased rate of depression (Loganovsky et al. 2011, 2013). Ongoing research of both the Chernobyl catastrophe and the aftermath of the Fukushima Daiichi Nuclear Power Plant Accident will help elucidate these issues further.

Frequency of neuropsychiatric disorders in prenatally and at 0–1 year exposed and nonexposed (at age of 23–25 years) (Loganovsky et al. 2013)
3 Chernobyl-Induced Thyroid Cancer and Neuropsychiatry
A dramatic excess of radiation-induced thyroid cancer after the Chernobyl catastrophe has been discovered (Bennett et al. 2006). In addition to oncological and endocrine aspects, thyroid cancer also affects neuropsychiatric problems. This connection is related to the following factors: (1) association of cancer pathology with mental disorders, (2) inadequate levels of thyroid hormone for normal development of the central nervous system, and (3) treatment for thyroid cancer can affect the brain and body. Thus, the comorbidity between thyroid cancer and psychiatric problems is significant from the medical, social, and psychological perspective in the population affected by Chernobyl, given their increased risk for both types of malady (Loganovsky et al. 2005).
A higher prevalence of mental disorders in children with thyroid cancer has been shown (38.4% vs. 22.5% in control group, p < 0.01), and neurotic disorders were particularly high (32.5% vs. 15.7% in control). Neurasthenia was assessed as the main mental disorder (14.3%), while post-traumatic stress disorder (PTSD) was diagnosed only in 3%. The rate of neurasthenia was 2.5 times higher in females than in males, and PTSD was found to be 4 times higher in females (Bazylchik 1998).
Children who have undergone surgery for oncological pathology of the thyroid gland have an increased frequency of adjustment disorder and post-traumatic stress disorder (PTSD), as well as disorders of activity and attention. Among children with persistent postoperative thyroid disorders, there is a significant decrease in the average group IQ and an increased trend in the frequency of disorders of activity and attention. Children with thyroid cancer show a decline in social and psychological adjustment in addition to the increased incidence of mental and behavioral disorders (Igumnov and Drozdovich 1998).
Patients with thyroid cancer have been characterized by deterioration of the quality of life in physical, psychological, emotional, and social spheres, as well as in their responses to stress. Corrective measures should be directed toward the psychological aspects associated with the need for lifelong replacement therapy and specialized observations (Grigoryeva and Igumnov 2009).
In summary, as clearly demonstrated among those who were children or adolescents at the time of the Chernobyl catastrophe, the increased rate of thyroid cancer is the most critical issue when considering the effects of radiation on the health of children. Therefore, in the early days after a nuclear accident, the primary concern should be to protect children from exposure to radioactive iodine through inhalation and ingestion, as this radioactive iodine preferentially accumulates in the thyroid. In the longer term, another concern is exposure to radionuclides with long half-lives, including 137Cs (Cesium) and 134Cs, with half-lives of 30 and 2 years, respectively. Research on the health effects of low-level radiation should be prioritized so that accurate information on these effects can be disseminated to both prevent unnecessary public fear when the risk is low and alert the public when the risks are high (Fushiki 2013). Moreover, lifelong neuropsychiatric monitoring for all patients with thyroid cancer is required, in conjunction with implementation of effective health and social measures to protect their mental health.
4 Psychosocial Factors in Mental Health of “Chernobyl Children”
The impact of radiation emergencies and other technological disasters on the mental health of children and adolescents and the role of radiation risk perception (fear of oncological diseases) have not been sufficiently explored. Clearly it is not only the irradiation that plays a role in the mental health outcomes of persons affected by the Chernobyl catastrophe.
The first psychosocial investigation of people’s reactions to the Chernobyl catastrophe was conducted in July–September 1986, which focused on psychological distress such as ongoing fear and risk perception related to nuclear facilities rather than on psychiatric disorders. Participants were pregnant women, parents of newborn children, farmers, adolescents, and childless men in various areas of Sweden, who differed in the degree of exposure they had received. In the most affected areas, the accident doubled the number of people who had negative attitudes toward nuclear power. For most groups, there was a fear of radiation risks, but in the more highly exposed areas, there was more concern. Farmers, in particular, emerged as strongly opposed to nuclear power and concerned about its risks. Women were more worried about the risks and had more negative attitudes to nuclear power than men, while adolescents appeared to be the least affected by the accident in terms of these attitudes (Sjöberg and Drottz 1987).
The first official estimates of psychological distress in the Chernobyl catastrophe survivors were extrapolated from previous radiation accidents, including the accident on March 28, 1979, at the Three Mile Island Nuclear Generating Station (a civilian nuclear power plant, near Middletown, PA, USA). Former USSR officials sought to downplay the psychological distress and fear of the population by using terms such as “radiophobia” (Il’in 1988) to imply that these fears were intrinsically pathologic. The authors reject the use of the epithet “radiophobia,” as it plays down the real danger and psychological consequences of the event itself. It also minimizes the egregiousness of the willful dissemination of inaccurate and contradictory information proliferated by Soviet officials in the aftermath of Chernobyl. The International Atomic Energy Agency (IAEA) International Chernobyl Project (1992) experts have emphasized that if the stress factor is a real danger, then it would be dishonest to say or to pretend that feelings of disquietude appearing in a response to that danger are something abnormal.
The term “radiophobia” in Western Europe and the USA only applies to an irrational fear of an event considered to be absolutely safe. Therefore, labeling the safety concerns of the wider population as “radiophobia” is inappropriate and potentially pejorative. The term “radioanxiety” was proposed as more accurate characterization of psychological reactions to radiation danger (Arkhangelskaya and Zykova 2001), but that term may have the similar problematic connotations.
In reality, anxiety plays an important role in both the perception and reality of mental health consequences after a disaster. According to Litcher et al. (2000), mothers of evacuated children reported memory problems in their children four times more frequently than controls, but results of neuropsychological testing did not show these differences. This was understood to be a result of mothers’ excess fear about the well-being of their children leading to overreporting problems.
In a similar study that looked at help-seeking behaviors, 600 child-mother dyads (300 evacuees and 300 classmate controls) were initially assessed in 1997, when the children were 11 years old, and followed up in 2005–2006, when they were 19 years old. A population control group (304 mothers and 327 children) was added in 2005–2006. At both times, poor health perceptions were associated with subjects seeking and obtaining a medical examination. From 2005 to 2006, this clinic attendance was also associated with the young adults’ risk perceptions, depression or generalized anxiety disorder, lower standard of living, and female gender (Guey et al. 2008).
A related study examined 265 adolescent evacuees, 261 classmate controls, and 327 population-based controls 19 years after the accident, looking at a number of outcomes as follows: risk perceptions, 12-month DSM-IV major depression (MDD), generalized anxiety disorder (GAD), and current symptomatology. Significantly more evacuees (48.7%) than controls (33.4–40.0%) reported at least one negative perception of Chernobyl; 18.1% of evacuees versus 10.0–12.8% of controls reported two to four negative perceptions. By contrast, 75.7% of evacuee mothers versus 34.8–37.6% of controls endorsed two to four negative perceptions. In the unadjusted analyses, adolescents’ perceptions were associated with both MDD/GAD in the previous 12 months and with more current symptomatology. However, after adjusting for possibly confounding risk factors, perceptions were associated only with symptomatology (p < 0.01). Among the possibly confounding risk factors, gender, self-esteem, life events, and peer support were significantly associated with MDD/GAD. These measures, along with the quality of parental communication, fathers’ belligerence when intoxicated, and maternal MDD/GAD, were significantly associated with the presence of symptoms. Thus, more evacuee teens reported negative risk perceptions than controls, and these perceptions were modestly associated with mental health outcomes. Nevertheless, the strongest risk factors for mental health outcomes were the same as those in parts of the world without a disaster history (Bromet et al. 2011a).
Another study conducted in 1997 found that at age 11, school grades and neuropsychological performance were similar in 300 children evacuated to Kiev as infants or in utero compared with 300 classmate controls. Yet, more evacuee mothers believed that their children had memory problems. In 2005–2006, researchers conducted an 8-year follow-up of the evacuees (n = 265) and classmate controls (n = 261) assessed in Kiev in 1997. Evacuees and classmates performed similarly and, in the normal range, on all tests, and no differential temporal changes were found. The rates of university attendance and self-reported memory problems were also similar. Nevertheless, the evacuee mothers were almost three times as likely to report that their children had memory problems compared with controls. The authors came to the conclusion that Chernobyl did not influence the cognitive functioning of exposed infants, although more evacuee mothers still believed that their offspring had memory problems. These lingering worries reflected a wider picture of persistent health concerns as a consequence of the accident (Taormina et al. 2008).
In Belarus, authors of several studies have come to the conclusion that unfavorable sociopsychological and sociocultural factors play a decisive role in the origin of borderline intellectual functioning and emotional disorders in Chernobyl children (Igumnov 1996; Kolominsky et al. 1999; Igumnov and Drozdovitch 2000, 2002, 2004). Although the average IQ of the most profoundly exposed participants (with doses to the thyroid in utero >1 Gy) was lower compared to other exposed children (Igumnov and Drozdovitch 2000), the low educational level of parents, the breaks in microsocial contacts, and the difficulties of adaptation, which appeared in the wake of evacuation and relocation from the contaminated areas, were considered the main risk factors.
4.1 Mental Health in “Chernobyl Children/Adolescents”: Evacuees
After the Chernobyl catastrophe, a number of children found themselves in ongoing traumatic situations. These included evacuation, loss of contact with parents, an unexpected change in their living situation, health problems, etc. A number of children had difficulty adjusting to the resettlements and were homesick. About 40% of child evacuees depending on age experienced homesickness. Many schoolchildren clearly remembered the places they used to live, events connected with their resettlement, and settling in a new place. These factors impeded formation of new behavioral models, contributed to tension and uncertainty, and may have caused fixation on the child’s problem and inability to cope. In 1987, almost all (97%) adolescents who were evacuated from the Chernobyl exclusion zone reported being afraid of possible negative health consequences (mostly of cancer). For many of them (72%), worries about dying were also reported. In 1994, a study of the psycho-emotional discrepancies between evacuees and unexposed adolescents living in Kiev was conducted, and an association between autonomic dysfunction and emotional stress was observed (Bebeshko and Korol 1995; Korol et al. 1998).
Psychophysiological functioning of exposed children was characterized by cognitive impairment, fatigue, and emotional lability (Bondar et al. 1995). From 1993 to 1997, the psychoneurological disorders occupied the third place in general pathology, while disorder of autonomic regulation had the highest position among mental health issues (37–38%) (Boroday and Usatenko 1998).
An excess of borderline neuropsychiatric disorders was found in 56.2% of children/adolescents who had been evacuated from Pripyat, while in the general population, the estimated level of such disorders was 21.2% (p < 0.01). Within this category, they diagnosed vegetative dystonia (33.7%), asthenic syndrome (15.6%), and neuroses and neurotic reactions (13.2%) (Arbuzova et al. 1992).
In 2000–2001, anxiety was noted in 40.6% of child evacuees, among whom 15.9% had a high score on the General Health Questionnaire-12 (GHQ-12). Depression was found in 36.4% of the children. Children with anxiety or depression had autonomic dysregulation and neurotic disorders more frequently than those without. The findings revealed a correlation between somatic concerns and mental health symptoms in survivors who were exposed during childhood (Shibata et al. 2003). There were also consistent reports of heightened emotional (28.4%) and psychosomatic (30.8%) disorders (Chunihin 2003).
Bromet et al. (2000) assessed the aftermath of the 1986 Chernobyl disaster in children evacuated to Kiev from the contaminated zone surrounding the nuclear power facility. In 1997, they evaluated 300 10- to 12-year-old children in Kiev who were in utero or infants at the time of the disaster and who had resided near Chernobyl (evacuees) against 300 sex-matched homeroom classmates who had never lived in a radiation-contaminated area. Response rates were 92% (evacuees) and 85% (classmates). Data were obtained from children, mothers, and teachers using standard measures of well-being and risk factors for childhood psychopathology. The children also received physical examinations and basic blood tests. The evacuees and classmates perceived their mental health similarly except for Chernobyl-related anxiety symptoms and perceived scholastic competence. No differences were found on the IOWA Conners Teacher Rating Scale. Although the physical examination and blood test results were normal, the evacuee mothers rated their children’s well-being as significantly worse, especially with respect to somatic symptoms on the Children’s Somatization Inventory and Child Behavior Checklist. The most important risk factors for these ratings were maternal somatization and Chernobyl-related stress. Given the multiple stressful experiences to which evacuee families were exposed to, the small differences in the children’s self-reports suggested that there were protective factors in the lives of these children. The trauma experienced by the mothers was reflected in their perceptions of their children’s well-being, particularly somatic symptoms, but in this case the anxiety was not transmitted to the children themselves (Bromet et al. 2000).
Studies show that the rates of depression and post-traumatic stress disorder (PTSD) in Bromet et al.’s (2000) sample remained elevated two decades later. Very young children and those in utero who lived near the plant when it exploded or in severely contaminated areas have been the subject of considerable research, but the findings are inconsistent. Recent studies conducted in Kiev and Scandinavia point to specific neuropsychological and psychological impairments associated with radiation exposure, whereas other studies found no significant cognitive or mental health effects in exposed persons later in life. Mothers of young children exposed to the disaster remain a high-risk group for these conditions, primarily due to lingering worries about the adverse health effects on their families. Thus, long-term mental health consequences continue to be a concern (Bromet et al. 2011b).
The “Chernobyl children” in Israel demonstrated separation anxiety disorder at a rate of 45.9%, though this disorder appeared during the first week after their arrival in Israel when they were separated from their parents and placed in an unusual cultural and language environment. The authors also demonstrated symptoms of radiation anxiety which were mainly diagnosed in teenage girls. These symptoms increased during the Persian Gulf War. Among other psychopathological symptoms, nocturnal enuresis, dysthymia, attention deficit hyperactivity disorder (ADHD), and suffering were observed. The data indicated a high risk for development of radiation anxiety in schoolchildren that could be exacerbated by separation anxiety disorder (Katz et al. 1995).
4.2 Mental Health in “Chernobyl Children/Adolescents”: Non-evacuees
Chronic frustration of children living in contaminated territories was another distinct issue. These children were not resettled; though they remained in their houses, and retained many of their friends and their schools, their environment had become “hostile.” Children remaining in contaminated areas were constantly facing danger to their health and safety caused by all the elements of the environment (water, air, soil, etc.). Contact with nature and with agricultural activities became rather dangerous. The situation was made worse by uncertainty about the future (i.e., potential health problems occurring or worsening). Thus, in order to provide effective psychosocial support to these children and adolescents, it was necessary to monitor their activities and their social and psychological conditions in both contaminated territories and areas of resettlement (Garnets and Panok 1998).
Among the children living in radioactively contaminated areas of the Russian Federation in 1–3 years after the Chernobyl catastrophe, an increase in etiologically unclear asthenic-vegetative disorders was found. They were observed mainly among the children who had mild residual organic cerebral deficiency. However, the authors did not exclude the impact of psychogenic factors (Sukhotina et al. 1993).
In the early 1990s, according to the data of the State Register of Ukraine (Chernobyl survivors), only 59.3% of the “Chernobyl children/adolescents” (age 0–14 years) could be considered healthy. Mental health disorders occupied the ninth place in morbidity, and, among these, nocturnal enuresis was found in 62.2% cases. Delays in psychomotor development were found as well in 27.8% of all mental disorder cases at that time (Ledoschuk et al. 1992).
Autonomic nervous system disorders were reported in 67% of exposed “Chernobyl children/adolescents” and neuroses and neurosis-like disorders in 10.8%, while in unexposed adolescents, such disorders were present only in 5–7% (Galina and Levinsky 1992). Moreover, emotional disorders were found in two-thirds of them: frustration (>40%), personality disorders (20%), and neurotic and related disorders (10%) (Svistunov et al. 1992).
Clinical-epidemiological studies showed that in radioactively contaminated areas, only 18.5% of “Chernobyl children/adolescents” could be considered “mentally healthy” compared with 49.7% in the general childhood population. In the majority of affected persons (64–78%), there were borderline neuropsychiatric disorders according to ICD-9, framed as “310: Specific nonpsychotic mental disorders due to brain damage” (Podkorytov et al. 1992). In a follow-up study, mental health deviations were found in 75% of exposed children and adolescents. These were mostly cerebro-asthenic and neurosis-like disorders, as well as borderline intellectual disability (Podkorytov 1995). From a 1990–1996 prospective study, compensated neuropsychiatric disturbances and speech problems were revealed in the majority (65–85%) of childhood survivors born in 1986 in radioactively contaminated areas (Podkorytov et al. 1998).
In adolescents from radioactively contaminated areas of Belarus, an emergence of schizoid and asthenic character traits was found (Bazylchik et al. 1992). Additional symptoms of stress, frustration, tension, anxiety, affective lability, irritability, and apathy, as well as disorders of memory, thinking, and motivation attenuation, were shown (Vishnevskaja 1992).
The Chernobyl Childhood Illness Program (CCIP) was a humanitarian assistance effort funded by the US Congress. Its purpose was to assist the Ukrainian government to identify and treat adolescents who developed mental and physical problems following their exposure as young children to the Chernobyl catastrophe. Thirteen years after the Chernobyl catastrophe, the CCIP examined 116,655 Ukrainian adolescents for thyroid diseases. Of these, 115,191 were also screened for depression, suicidal ideation, and other psychological problems. The adolescents lived in five of Ukraine’s seven most contaminated provinces. They were up to 6 years of age or in utero when exposed to nuclear fallout or were born up to 45 months after Chernobyl. According to the results of the Children’s Depression Inventory (CDI), probable depression was diagnosed in 15,399 adolescents (13.2%), suicidal ideation in 813 (5.3%), and attempted suicide in 354 (2.3%). Underlying components of the participants’ depression were negative mood, interpersonal difficulties, negative self-esteem, ineffectiveness, and anhedonia. Depression was greater in females. Those with thyroid and psychological problems were referred for treatment. The adolescents screened by the CCIP represented the largest Ukrainian cohort exposed to the Chernobyl catastrophe as children who were evaluated for both thyroid tumors and depression. The group had an increased prevalence of thyroid cancer, thyroid nonmalignant tumors, depression, and suicidal ideation. The CCIP demonstrated that psychological problems among Chernobyl-exposed adolescents began earlier in life than previously reported. They also experienced socioeconomic problems due to their relocation from radiation-affected areas and the Soviet Union’s inadequate responses to their health needs. The CCIP’s findings underscored the requirement that governments prepare plans to deal promptly with the diagnosis and treatment of nuclear accident victims’ medical and psychological problems (Contis and Foley Jr. 2015).
Following the Chernobyl catastrophe, several areas of Central Norway were heavily affected by far field radioactive fallout. In a study of the psychological well-being of 53 adolescents who were exposed to Chernobyl radiation as fetuses in Norway, adolescents and their mothers reported their perceptions of current psychological health, as measured by the Youth Self-Report and Child Behavior Checklist. In spite of previous reports of subtle cognitive deficits in these exposed adolescents, there were few self-reported problems and fewer problems reported by the mothers. This contrasts with findings on children from the former Soviet Union exposed in utero, in which self-reports by mothers expressed concern for adolescents’ cognitive functioning and psychological well-being. The authors suggest that protective factors in Norway, in addition to perceived physical and psychological distance from the disaster, made the mothers less vulnerable to Chernobyl-related anxiety, thus preventing a negative effect on the psychological health of both mother and child (Heiervang et al. 2011).
Radiation accidents, radiological terrorist attacks, and other forms of nuclear conflict are substantially different from natural disasters, and wars that don’t involve the use of nuclear material. The long-lasting and uncertain effects of radiation contamination induce additional anxieties within the community over and above that of other mass disasters. To a greater extent than other disasters, the clinical features of exposure to radiological events include major aspects of PTSD—“immersion” in the experience, “avoidance,” “hyperexcitability,” and “social functioning deficits” (Rumyantseva et al. 2007; Rumyantseva and Stepanov 2008). Survivors of radiological events who suffer from PTSD have more general psychiatric symptomatology, state and trait anxiety, and depression. The individual perception and assessment of ongoing radioactive hazards play a determining role in the development of PTSD (Tarabrina et al. 1996). Anxiety about the future (the risk of cancer and other diseases, congenital malformations in descendants etc.), long-term radioactive contamination, evacuation and resettlement, as well as incomplete governmental regulations regarding social benefits to the victims all contribute significantly to the development of these psychopathological responses (Loganovsky 2012; Loganovsky et al. 2014).
5 Neuropsychiatric/Psychosocial Management and Rehabilitation
Below we offer suggestions for approaches to neuropsychiatric/psychosocial management and rehabilitation for children and adolescents after radiation emergencies based on our experience of more than 30 years.
The significant incidence and heterogeneity of mental disorders among the children exposed to ionizing radiation after radiation emergencies necessitate a complex application of differential approaches toward management and rehabilitation. First, it should be noted that there are predictable psychosocial problems that substantially hamper, or render ineffective, certain therapeutic interventions in children and adolescents exposed to radiation emergencies. Those psychosocial problems are inaccurate estimates of health issues in children and their parents especially regarding the impact of radiation, negative effects of prolonged hospital stays, children’s avoidance of school and social activities, assuming the victim role rather than that of a survivor, learned helplessness, and difficulty obtaining social benefits and health insurance. Understanding and identifying these issues as they manifest in each individual case, together with focused treatment for the affected child/adolescent and the therapeutic involvement of their family members, make the mental health prognosis much better.
The psychological factors surrounding the Chernobyl catastrophe included the sudden trauma of evacuation, long-term effects of being a refugee, disruption of social networks, physical illness, separation and its effects on families, effects of children’s perception on their development, and threat of long-term, unending consequences. In addition, the breakdown of the Soviet Union, the consequent collapse of health services, and the increasing poverty and malnutrition also played a role in the lives of the many affected by Chernobyl. These complexities made it necessary to develop new individual and social treatment methods in UNESCO Community Centers. This led to positive results, such as the development of individual and group self-help programs, the advancement of the professions of counseling and social work, and the improvement of programs for community development (Barnett 2007).
An excess of neuropsychiatric and mental health disorders should be expected moving forward among persons exposed to radiation in utero, exposed in childhood/adolescents, and in descendants of those exposed to radiation. Taking into account the prevalence and persistence of these mental health disorders, further research on the optimal educational, psychosocial, and healthcare interventions are required.
5.1 The Main Principle of Management: Do Not Separate the Family
Research/implementation essentials of psychological/psychiatric care for children/adolescent survivors of radiation emergencies include the following:
-
1.
Neuropsychiatric approach
-
2.
Biopsychosocial paradigm
-
3.
Effective prophylaxis
-
4.
Social readaptation and rehabilitation
Organizational principles of the psychological/psychiatric aid for children/adolescent survivors of radiation emergencies include the following:
-
1.
Preparedness and planning
-
2.
Effective management based on a flexible and coordinated structural-functional organization
-
3.
Adequate procurement
-
4.
Timely, thorough, and proactive
-
5.
Availability to all population groups
-
6.
Continuous interaction and cooperation with radiological and dosimetric (biophysical) services
-
7.
Evidence-based, individualized, and correlation to the particular radiation emergency
-
8.
Effective interaction and cooperation with local authorities and government agencies
-
9.
Availability of an emergency reception center
-
10.
Cooperation with mass media regarding constructive presentation of information
-
11.
Avoiding panic, manipulation of survivors, and other socially negative consequences of a radiation emergency (preventing mass fear and its consequences)
-
12.
Teaching and supervision of related/allied personnel
-
13.
Providing the maximum effective psychological/psychiatric aid
Principal approaches toward mental health disorders in children/adolescent survivors of radiation emergencies include the following:
-
1.
Communication of understandable, serviceable, and impartial information regarding the radiation emergency in a timely and ongoing fashion
-
2.
Training and preparedness for these situations
-
3.
Governmental preparedness
-
4.
Rational interventions
-
5.
Psychological support
-
6.
Emphasizing the social and economic benefits of the label “survivor” rather than the “victim”
-
7.
Constructive, professional, and realistically optimistic approach by the mass media
-
8.
Psycho-prophylaxis, psycho-rehabilitation, and management
-
9.
Social readaptation
Approaches to optimization of treatment, prevention, and rehabilitation arrangements for children/adolescent survivors of radiation emergencies include the following:
-
1.
Integration of biological and psychosocial interventions
-
2.
Multidimensional approach, taking into account a variety of activities and different fields of rehabilitation (psychological, social, family, etc.)
-
3.
Appeal to the individual personality and formation of treatment partnerships, i.e., a child/adolescent involved in the treatment process as an active participant and involved in physical rehabilitation as well as social reintegration
-
4.
Stepped care principle (continuity/portability of interventions in healthcare institutions, day treatment facilities as well as overnight ones, and rest/recreation clinics)
General requirements for the complex management of children and adolescents suffering mental disorders are as follows:
-
1.
Specificity and the management methods are to be adequate to the given mental disorder
-
2.
Adequacy for the patient’s age and development
-
3.
Variability and adjustability to insure practical implementation
-
4.
Effectiveness, based on empirical survey feedback (sequential estimates)
Initial and maintenance treatments are to be multimodal, with due consideration of etiologic heterogeneity of mental disorders:
The therapeutic process should be under the supervision of a child and adolescent psychiatrist who include other healthcare professionals, if necessary (pediatrician, pediatric neurologist, social skills teacher, and psychologist). The following structural elements should be included within a therapeutic process:
-
1.
Sociopsychological and psychotherapeutic interventions, which include education of key persons (parents, child, school personnel), support groups for parents, training for parents, family psychotherapy, and interventions at school
-
2.
Pharmacological therapy for the major disorder and comorbidities
-
3.
Complementary (non-pharmacological) methods and tools, i.e., exercise therapy, physiotherapy, and folk medicine approaches
-
4.
Development of the individual rehabilitation plan
Taking into account the substantial number of prenatally exposed children suffering organic mental disorders and psychological developmental abnormalities (often in combination), the following recommendations are appropriate to stimulate healthy development:
-
1.
Cognitive sphere. Trainings are recommended as a continuation of diagnostic procedures for the enhancement of attention, concentration, memory, thinking, behavior, learning process, and the ability to solve problems.
-
2.
Emotional sphere. Antidepressants are often recommended, given affective lability and comorbid depressive disorders. Behavioral therapy is indicated in case of phobias and other obsessions.
-
3.
Social behavior. Social training programs should be focused on helping the patient to predict social problems and the consequences of their own behaviors. Pharmacological treatment is indicated under certain circumstances for aggressive behavior.
-
4.
Impulse control. Psychotherapeutic programs are recommended to develop reflection/self-consciousness as a control mechanism between an impulse to act and its execution (“think first, then do”). Pharmacological therapy is a supplementary tool here in special circumstances.
-
5.
Autonomic symptoms. Utilize combination of pharmacological and behavioral therapy.
-
6.
Neurological deficit. Utilize exercise therapy, physiotherapy, neuro-metabolic pharmacotherapy, and anticonvulsive therapy in case of epileptic attacks.
Within development psychological disorders, the management should include:
-
1.
Consulting the children, their parents, and teachers regarding their particular disabilities (e.g., specific reading disorder)
-
2.
Special trainings for teaching remedial skills
-
3.
Psychotherapeutic arrangements to support compensatory capacities and (if necessary) management of concomitant mental disorders
-
4.
Awareness regarding potential suicidal behavior, risk assessment, and resilience promotion
The psychotherapeutic aims and tools for the somatoform disorders are as follows:
-
1.
Create a confidential relationship.
-
2.
Develop therapeutic motivation. Discuss the long-term aims and short-term aims of therapy with parents, identify unrealistic goals, and focus on what is possible within the therapy.
-
3.
Develop a psychosomatic understanding of the disease. Explain the interrelationship between physical, mental, and social processes.
-
4.
Reduce the somatic medical treatments to the permissible minimum. Limit the administration of medications to a minimum, avoid unnecessary medical intervention, and agree on a specific schedule for doctor visits.
-
5.
Reduce avoidance behaviors. Encourage physical activity and participation in sports, and remove the avoidance behaviors regarding school and social activities. Prompt the patient to take on age-appropriate responsibility.
-
6.
Help patient have an accurate internal picture of their disease. Correct self-defeating attitudes toward the present disorders and their medico-social consequences.
-
7.
Improve quality of life. Stimulate social contacts, optimize leisure activities, and encourage hobbies, interests, and communication.
Application of the aforementioned principles in treating affected children will promote the optimization of their social adaptation and personal development.
6 Conclusion
The Chernobyl catastrophe is a historical example of a disastrous traumatic event with a mixture of stressful factors—those related to psychosocial stress (evacuation, relocation, loss of property, and drastic alterations to life plans), those related to perceived stress (anxiety regarding health effects of the irradiation, especially regarding babies and children, anxiety due to shortage of accurate information, fear and helplessness in the face of a disaster, embitterment, and anger), and those related to physical effects of the radioactive contamination (specific radionuclides inhaled or ingested or other exposures, concentration in certain organs, effects on the developing brain, etc.). All of these stressors act simultaneously, overlap, and interact with each other. Unborn fetuses, babies, and very young children are presumably the mostly affected by the physical factors, while older children and adolescents, who are more aware of the levels of anxiety around them and the severity of the situation, are more vulnerable to psychosocial and perception factors.
Existing data on the mental health consequences of the Chernobyl catastrophe are based on a variety of studies which were conducted in different countries, often using different standards and incomplete information (timing, level of exposure, incorporated radionuclides, etc.). Nevertheless, efforts by national and international teams helped to establish the main domains in which these consequences may be traced and objectively characterized. They include cognitive, emotional, behavioral, and vegetative (mostly psychosomatic) disturbances, which have seriously impaired the quality of life in exposed youth. There is a need for follow-up studies and prolonged monitoring of exposed youngsters as well as future generations.
The Chernobyl catastrophe provides valuable experience for promoting reasonable measures that may help prevent mental health problems in exposed populations in similar situations. The Fukushima disaster provided another occasion to test the relevance of our hard-fought experience. Unfortunately, in the age of nuclear power, it appears that there will be more disasters to come and more occasions to take what we have learned and apply it in efficacious ways to mitigate the damage that future victims could suffer.
There is an urgent need for international efforts to collect and disseminate this information worldwide for the sake of protecting the mental health of the next generation.
References
Almond D, Edlund L, Palme M. Chernobyl’s subclinical legacy: prenatal exposure to radioactive fallout and school outcomes in Sweden. Q J Econ. 2009;124(4):1729–72.
Arbuzova V, Kukuruza A, Zhdanova I. Early diagnosis of mental and social maladjustment in children and adolescents who were evacuated from the town of Pripyat. Paper presented at the social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences, Kiev. 1992.
Arkhangelskaya H, Zykova I. The monitoring of radiation anxiety. Int J Radiat Med. 2001;3(1–2):8.
Bar JN, Reisfeld D, Tirosh E, Silman Z, Rennert G. Neurobehavioral and cognitive performances of children exposed to low-dose radiation in the Chernobyl accident: the Israeli Chernobyl Health Effects Study. Am J Epidemiol. 2004;160(5):453–9.
Barnett L. Psychosocial effects of the Chernobyl nuclear disaster. Med Confl Surviv. 2007;23(1):46–57.
Bazyka D, Ilyenko I, Loganovsky K, Lyashenko L. Cognitive deficit at the late period after low dose radiation exposure influences gene expression and cell differentiation. Paper presented at the La theorie de replicon: 50 ans deja. Institut Pasteur, Paris. 2013a.
Bazyka D, Loganovsky K, Ilyenko IN, Chumak SA, Marazziti D, Maznichenko OL, et al. Cellular immunity and telomere length correlate with cognitive dysfunction in clean-up workers of the Chernobyl accident. Clin Neuropsychiatry. 2013b;106:280–1.
Bazyka D, Ilyenko I, Loganovsky K, Benotmane M, Chumak S. TERF1 and TERF2 downregulate telomere length in cognitive deficit at the late period after low-dose exposure. Probl Radiat Med Radiobiol. 2014;19:170–85.
Bazyka D, Loganovsky K, Ilyenko I, Chumak S, Bomko M. Gene expression, telomere and cognitive deficit analysis as a function of Chornobyl radiation dose and age: from in utero to adulthood. Probl Radiat Med Radiobiol. 2015;20:283–310.
Bazylchik S. Mental disorders in children with cancer of thyroid gland. In: Nyagu A, Souchkevitch G, editors. Long-term health consequences of the Chernobyl disaster, 1–6 June 1998. Kiev: Chernobylinterinform; 1998.
Bazylchik S, Kazak E, Terekhova Z. Features of character accentuations in adolescents living in areas contaminated with radionuclides. In Social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences, 28–30 Sept 1992. Kiev. 1992.
Bebeshko V, Korol N. Psychological status and main health status parameters in adolescents evacuated from town Pripyat. In International conference on the mental health consequences of the Chernobyl disaster: current state and future prospects, 24–28 May 1995. Kiev. 1995.
Bennett B, Repacholi M, Carr Z. Health effects of the Chernobyl accident and special health care programmes. In: Bennett B, Repacholi M, Carr Z, editors. Report of the UN Chernobyl Forum Expert Group “Health”. Geneva: World Health Organization; 2006.
Bondar A, Nedelko V, Polka N. Psychophysiological functions peculiarities in children of different age resident on controlled territories. In International conference on the mental health consequences of the Chernobyl disaster: current state and future prospects, 24–28 May 1995. Kiev. 1995.
Boroday G, Usatenko ZV. Indices of pathological affection among children included in to clinical and epidemiological register. In: Nyagu A, Souchkevitch G, editors. Long-term health consequences of the Chernobyl disaster, 1–6 June 1998. Kiev: Chernobylinterinform; 1998.
Bromet EJ. Mental health consequences of the Chernobyl disaster. J Radiol Prot. 2012;32(1):N71.
Bromet EJ, Goldgaber D, Carlson G, Panina N, Golovakha E, Gluzman SF, et al. Children’s well-being 11 years after the Chornobyl catastrophe. Arch Gen Psychiatry. 2000;57(6):563–71.
Bromet EJ, Guey LT, Taormina DP, Carlson GA, Havenaar JM, Kotov R, et al. Growing up in the shadow of Chornobyl: adolescents’ risk perceptions and mental health. Soc Psychiatry Psychiatr Epidemiol. 2011a;46(5):393–402.
Bromet EJ, Havenaar JM, Guey L. A 25 year retrospective review of the psychological consequences of the Chernobyl accident. Clin Oncol. 2011b;23(4):297–305.
Chunihin YA. Mental health in Chernobyl children. Int J Radiat Med. 2003;5(3):27–8.
Contis G, Foley TP Jr. Depression, suicide ideation, and thyroid tumors among Ukrainian adolescents exposed as children to Chernobyl radiation. J Clin Med Res. 2015;7(5):332–8.
Ermolina L, Sukhotina N, Sosyukalo O, Kashnikova A, Tatarova I. Effects of low radiation doses on neuropsychic heath in children (methodological approaches and preliminary data). Report #1. Soc Clin Psychiatry. 1994;4(1):37–43.
Ermolina L, Sukhotina N, Sosyukalo O, Kashnikova A, Tatarova I. Effects of low radiation doses on neuropsychic heath in children (radio-ontogenic issue of the problem). Report #2. Soc Clin Psychiatry. 1996;6(3):5–13.
European Commission. Radiation protection 100: guidance for protection of unborn children and infants irradiated due to parental medical exposures. Brussels: European Commission; 1998.
Flor-Henry P. Psychosis and temporal lobe epilepsy; a controlled investigation. Epilepsia. 1969a;10(3):363–95.
Flor-Henry P. Schizophrenic-like reactions and affective psychoses associated with temporal lobe epilepsy: etiological factors. Am J Psychiatry. 1969b;126(3):400–4.
Flor-Henry P. Cerebral basis of psychopathology. Littleton: J. Wright; 1983.
Friedman HR, Selemon LD. Fetal irradiation interferes with adult cognition in the nonhuman primate. Biol Psychiatry. 2010;68(1):108–11.
Fushiki S. Radiation hazards in children–lessons from Chernobyl, Three Mile Island and Fukushima. Brain Dev. 2013;35(3):220–7.
Galina I, Levinsky M. Mental state of adolescents with autonomic dysfunction from areas with high radiation background. In Social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences, 28–30 Sept 1992. Kiev. 1992.
Garnets O, Panok V. Peculiarities of psycho-traumatic situation of children suffered from Chernobyl catastrophe. In: Nyagu A, Souchkevitch G, editors. Long-term health consequences of the Chernobyl disaster, 1–6 June 1998. Kiev: Chernobylinterinform; 1998.
Gelowitz DL, Rakic P, Goldman-Rakic PS, Selemon LD. Craniofacial dysmorphogenesis in fetally irradiated nonhuman primates: implications for the neurodevelopmental hypothesis of schizophrenia. Biol Psychiatry. 2002;52(7):716–20.
Grigoryeva I, Igumnov S. Medical and psychological assistance, and internal picture of the disease features in patients with thyroid cancer. Medico-biological and Socio-psychological Problems of Security in Emergency Situations. 2009;(5):27–32.
Guey LT, Bromet EJ, Gluzman SF, Zakhozha V, Paniotto V. Determinants of participation in a longitudinal two-stage study of the health consequences of the Chornobyl nuclear power plant accident. BMC Med Res Methodol. 2008;8(1):27.
Gross R, Hamid H, Harlap S, Malaspina D. Prenatal X-ray exposure may increase risk of schizophrenia: results from the Jerusalem perinatal cohort schizophrenia study. Int J Mental Health. 2018;47(3):236–40. https://doi.org/10.1080/00207411.2017.1308293
Hatch M, Little MP, Brenner AV, Cahoon EK, Tereshchenko V, Chaikovska L, et al. Neonatal outcomes following exposure in utero to fallout from Chernobyl. Eur J Epidemiol. 2017;32(12):1075–88.
Heiervang KS, Mednick S, Sundet K, Rund BR. Effect of low dose ionizing radiation exposure in utero on cognitive function in adolescence. Scand J Psychol. 2010a;51(3):210–5.
Heiervang KS, Mednick S, Sundet K, Rund BR. The Chernobyl accident and cognitive functioning: a study of Norwegian adolescents exposed in utero. Dev Neuropsychol. 2010b;35(6):643–55.
Heiervang KS, Mednick S, Sundet K, Rund BR. The psychological well-being of Norwegian adolescents exposed in utero to radiation from the Chernobyl accident. Child Adolesc Psychiatry Ment Health. 2011;5(1):12.
Huizink A, Dick DM, Sihvola E, Pulkkinen L, Rose RJ, Kaprio J. Chernobyl exposure as stressor during pregnancy and behaviour in adolescent offspring. Acta Psychiatr Scand. 2007;116(6):438–46.
Huizink A, Bartels M, Rose R, Pulkkinen L, Eriksson C, Kaprio J. Chernobyl exposure as stressor during pregnancy and hormone levels in adolescent offspring. J Epidemiol Community Health. 2008;62(4):e5.
IAEAC. The international Chernobyl project: technical report. I.A.E. Agency. 1992.
ICRP. Developmental effects of irradiation on the brain of the embryo and fetus: a report of a Task Group of Committee 1 of the International Commission on Radiological Protection. In: Annals of the ICRP. Oxford: Pergamon Press; 1986.
ICRP Publication 84. Pregnancy and medical radiation. Ann ICRP. 2000;30(1):1–43.
Igumnov S. Psychological development of children exposed to radiation in prenatal period as a result of Chernobyl disaster. Acta Med Nagasaki. 1996;41(3–4):20–5.
Igumnov S, Drozdovich V. Clinical and dosimetric analysis of the peculiarities of intellectual development, emotional and behavioral disorders in children with oncological pathology of thyroid gland. Ukr Med J. 1998;2(4):36–40.
Igumnov S, Drozdovich V. Cerebral bioelectrical activity in children prenatally exposed to ionizing radiation after the Chernobyl NPP accident (prospective study). Med Radiol Radiat Prot. 2002;5:33–42.
Igumnov S, Drozdovitch V. The intellectual development, mental and behavioural disorders in children from Belarus exposed in utero following the Chernobyl accident. Eur Psychiatry. 2000;15(4):244–53.
Igumnov S, Drozdovitch V. Antenatal exposure following the Chernobyl accident: neuropsychiatric aspects. Int J Radiat Med. 2004;6(1–4):108.
Il’in L. The Chernobyl experience in the context of contemporary radiation protection problems. In: All-Union conference, USSR Ministry of Health, All-Union Scientific Centre of Radiation Medicine, USSR Academy of Medical Sciences 11–13 May 1988. Vienna: IAEA; 1988. p. 47–64. IAEA–TECDOC–516.
Imamura Y, Nakane Y, Ohta Y, Kondo H. Lifetime prevalence of schizophrenia among individuals prenatally exposed to atomic bomb radiation in Nagasaki City. Acta Psychiatr Scand. 1999;100(5):344–9.
Katz M, Khobler H, Lerner Y. “Radiophobia” and separation anxiety disorder in children from examination of immigrant children in Israel. In International conference on the mental health consequences of the Chernobyl disaster: current state and future prospects, 24–28 May 1995. Kiev. 1995.
Kolominsky Y, Igumnov S, Drozdovitch V. The psychological development of children from Belarus exposed in the prenatal period to radiation from the Chernobyl atomic power plant. J Child Psychol Psychiatry. 1999;40(2):299–305.
Korol N, Shibata Y, Nakane Y. Psychosomatic health status of children exposed to the Chernobyl accident. Acta Med Nagasaki. 1998;43(3–4):57–61.
Korr HTR, Benders J, Dafotakis M, Grolms N, Schmitz C. Neuron loss during early adulthood following prenatal low-dose X-irradiation in the mouse brain. Int J Radiat Biol. 2001;77(5):567–80.
Ledoschuk B, Treskunova T, Khomenko N. Mental and physical health of children from Ivankov district registered in the State registry of Ukraine. In Social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences, 28–30 Sept 1992. Kiev. 1992.
Litcher L, Bromet EJ, Carlson G, Squires N, Goldgaber D, Panina N, et al. School and neuropsychological performance of evacuated children in Kyiv 11 years after the Chornobyl disaster. J Child Psychol Psychiatry. 2000;41(3):291–9.
Loganovska T, Nechayev S. Psychophysiological effects in prenatally irradiated children and adolescents after the Chornobyl NPP accident. Med Universe. 2004;4(1):130–7.
Loganovskaja T. Psychophysiological pattern of acute prenatal exposure to ionizing radiation as a result of the Chernobyl accident. Int J Psychophysiol. 2004;54(1–2):95–6.
Loganovskaja T. Mental disorders in children exposed to prenatal irradiation as a result of the Chernobyl accident. The dissertation for the academic degree of a candidate of medical sciences (PhD). 2005.
Loganovskaja T, Loganovsky K. EEG, cognitive and psychopathological abnormalities in children irradiated in utero. Int J Psychophysiol. 1999;34(3):213–24.
Loganovskaja T, Loganovsky K. Visual vertex potential and psychopathology of children irradiated in utero. Int J Psychophysiol. 2000;35:69.
Loganovsky K. Do low doses of ionizing radiation affect the human brain? Data Sci J. 2009;8:BR13–35.
Loganovsky K. Brain damage following exposure to low doses of ionizing radiation as a result of the Chernobyl accident. Clin Neuropsychiatry. 2012;9(5):203–5.
Loganovsky K, Loganovskaja T. Schizophrenia spectrum disorders in persons exposed to ionizing radiation as a result of the Chernobyl accident. Schizophr Bull. 2000;26(4):751–73.
Loganovsky K, Loganovskaja T. Cortical-limbic neurogenesis asymmetry as possible cerebral basis of brain laterality following exposure to ionizing radiation. J Treat Eval. 2013;10:3–4.
Loganovsky K, Zdanevich N. Cerebral basis of posttraumatic stress disorder following the Chernobyl disaster. CNS Spectr. 2013;18(02):95–102.
Loganovsky K, Volovik SV, Manton KG, Bazyka D, Flor-Henry P. Whether ionizing radiation is a risk factor for schizophrenia spectrum disorders? World J Biol Psychiatry. 2005;6(4):212–30.
Loganovsky K, Loganovskaja T, Nechayev SY, Antipchuk YY, Bomko MA. Disrupted development of the dominant hemisphere following prenatal irradiation. J Neuropsychiatry Clin Neurosci. 2008;20(3):274–91.
Loganovsky K, Bazyka D, Loganovskaja T. Potential neurodevelopmental effects of exposure in utero. In The effects of low and very low doses of ionizing radiation on human health and biotopes, 5–7 Dec 2011. Kiev. 2011.
Loganovsky K, Bazyka D, Loganovskaja T. Neuropsychiatric monitoring improving in persons exposed in prenatal period and at the age of 0–1 years as a result of radiation emergencies. Kiev: N.A.O.M.S.O.U. Ministry of Public Health, Ukrainian Scientific Center of Medical Information and Patent-Licensed Work; 2013.
Loganovsky K, Bazyka D, Loganovskaja T, Ilyenko I, Golyarnik N, Antypchuk K. Method of retrospective differentiated designation of the human brain irradiation, which occurred in the early stages of developmental period. Patent for Inventions of Ukraine No. 106419. 26.08.2014 2014.
Marazziti D, Baroni S, Catena-Dell’osso M, Schiavi E, Ceresoli D, Conversano C, et al. Cognitive, psychological and psychiatric effects of ionizing radiation exposure. Curr Med Chem. 2012;19(12):1864–9.
Marazziti D, Tomaiuolo F, Dell’Osso L, Demi V, Campana S, Piccaluga E, et al. Neuropsychological testing in interventional cardiology staff after long-term exposure to ionizing radiation. J Int Neuropsychol Soc. 2015;21(9):670.
Marazziti D, Piccinni A, Mucci F, Baroni S, Loganovsky K, Loganovskaja T. Ionizing radiation: brain effects and related neuropsychiatric manifestations. Probl Radiat Med Radiobiol. 2016;21:64.
Nowakowski RS, Hayes NL. Radiation, retardation and the developing brain: time is the crucial variable. Acta Paediatr. 2008;97(5):527–31.
Nyagu A, Cheban A, Salamatov V, Limanskaja G, Yashchenko A, Zvonareva G, et al. Psychosomatic health of children exposed in utero after the Chernobyl NPP accident. In: Social–psychological and psycho–neurological aspects of Chernobyl NPP accident consequences: Proceedings of Community States Scientific Conference with International Participation. Kiev, September, 28–30; 1992. p. 265–70.
Nyagu A, Loganovsky K, Loganovskaja T. Psychophysiologic after effects of prenatal irradiation. Int J Psychophysiol. 1998;30(3):303–11.
Nyagu A, Loganovskaya T, Loganovsky K. Neuropsychiatric health of the prenatally irradiated children as a result of the Chernobyl disaster. Ukr Med J. 2000;2(16):105–12.
Nyagu A, Loganovsky K, Loganovskaja T, Repin VS, Nechaev SY. Intelligence and brain damage in children acutely irradiated in utero as a result of the Chernobyl accident. KURRI KR. 2002;79:202–30.
Nyagu A, Loganovsky K, Repin V, Bomko M, Pott-Born R. Effects of prenatal brain irradiation as a result of the Chernobyl accident. Int J Radiat Med. 2004;6(1–4):91.
Otake M. Threshold for radiation-related severe mental retardation in prenatally exposed A-bomb survivors: a re-analysis. Int J Radiat Biol. 1996;70(6):755–63.
Picano E, Vano E, Domenici L, Bottai M, Thierry-Chef I. Cancer and non-cancer brain and eye effects of chronic low-dose ionizing radiation exposure. BMC Cancer. 2012;12(1):157.
Podkorytov V. Mental health status dynamic in children resident in radionuclides contaminated regions of Ukraine. In International conference on the mental health consequences of the Chernobyl disaster: current state and future prospects, 24–28 May 1995. Kiev. 1995.
Podkorytov V, Filyk V, Malyshko M. Psychovegetative status peculiarities of children living in areas of strict control, in connection with the accident at the Chernobyl NNP. In: Proceedings of International Conference “Social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences”, Kiev, 28–30 September; 1992.
Podkorytov V, Shestopalova L, Myshanova M, et al. Neuro-mental health status in children from various regions of Ukraine after the Chernobyl disaster. In: Nyagu A, Souchkevitch G, editors. Long-term health consequences of the Chernobyl disaster, 1–6 June 1998. Kiev: Chernobylinterinform; 1998.
Rice D, Barone S Jr. Critical periods of vulnerability for the developing nervous system: evidence from humans and animal models. Environ Health Perspect. 2000;108(Suppl 3):511.
Rumyantseva G, Stepanov A. Post-traumatic stress disorder in different types of stress (clinical features and treatment). Neurosci Behav Physiol. 2008;38(1):55–61.
Rumyantseva G, Levina T, Chinkina O, et al. Peculiarities of psychological-psychiatric after-effects of radiation accidents. Hum Ecol. 2007;9:42–7.
Schindler MK, Wang L, Selemon LD, Goldman-Rakic PS, Rakic P, Csernansky JG. Abnormalities of thalamic volume and shape detected in fetally irradiated rhesus monkeys with high dimensional brain mapping. Biol Psychiatry. 2002;51(10):827–37.
Schmitz C, Born M, Dolezel P, Rutten B, de Saint-Georges L, Hof P, et al. Prenatal protracted irradiation at very low dose rate induces severe neuronal loss in rat hippocampus and cerebellum. Neuroscience. 2005;130(4):935–48.
Selemon LD, Friedman HR. Motor stereotypies and cognitive perseveration in non-human primates exposed to early gestational irradiation. Neuroscience. 2013;248:213–24.
Selemon LD, Wang L, Nebel MB, Csernansky JG, Goldman-Rakic PS, Rakic P. Direct and indirect effects of fetal irradiation on cortical gray and white matter volume in the macaque. Biol Psychiatry. 2005;57(1):83–90.
Selemon LD, Begović A, Rakic P. Selective reduction of neuron number and volume of the mediodorsal nucleus of the thalamus in macaques following irradiation at early gestational ages. J Comp Neurol. 2009;515(4):454–64.
Serdiuk A, Bebeshko V, Bazyka D, Yamashita S. Health effects of the Chornobyl accident: a quarter of century aftermath. Kiev: DIA; 2011.
Shibata Y, Korol N, Honda S, et al. Correlation between somatic and mental conditions in people exposed to the Chernobyl accident in their childhood. Int J Rad Med Special Issue. 2003;5(3):106–7.
Shirakawa O, Kitamura N, Lin X-H, Hashimoto T, Maeda K. Abnormal neurochemical asymmetry in the temporal lobe of schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry. 2001;25(4):867–77.
Sjöberg L, Drottz B-M. Psychological reactions to cancer risks after the Chernobyl accident. Med Oncol Tumor Pharmacother. 1987;4(3–4):259–71.
Souchkevitch G, Tsyb A. Health consequences of the Chernobyl accident: results of the IPHECA pilot projects and related national programmes: scientific report. Geneva: World Heath Organization. International Programme on the Health Effects of the Chernobyl Accident (IPHECA); 1996.
Stepanova Y, Kondrashova V, Kolpakov Y, Pasechnic L, Kolesnikov Y. Psycho–vegetative status in children irradiated in prenatal period as the result of ChNPP accident. In: Social–psychological and psycho–neurological aspects of Chernobyl NPP accident consequences: Proceedings of Community States Scientific Conference with International Participation. Kiev, September, 28-30, 1992, Kiev; 1993. p. 230.
Stepanova E. Health condition of children irradiated in utero. In: International Conference One decade after Chernobyl: Book of extended synopses. Vienna: IAEA; 1996. p. 379–80.
Sukhotina NK, Kashnikova AA, Preĭs VB, Tatarova IN, Terekhina TV. An epidemiological method for studying the effect of elevated background radiation on the neuropsychic health of children. Zh Nevrol Psikhiatr Im S S Korsakova. 1993;93(3):64–8.
Svistunov T, Viskonvatov Y, Chebykin A, et al. Emotional state of children living in the zone of influence of the Chernobyl disaster. In Social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences, 28–30 Sept 1992. Kiev. 1992.
Taormina D, Rozenblatt S, Guey L, Gluzman S, Carlson G, Havenaar J, et al. The Chornobyl accident and cognitive functioning: a follow-up study of infant evacuees at age 19 years. Psychol Med. 2008;38(04):489–97.
Tarabrina N, Lazebnaya E, Zelenova M, Lasko N. Chernobyl clean-up workers’ perception of radiation threat. Radiat Prot Dosim. 1996;68(3–4):251–5.
UNSCEAR. Exposures and effects of the Chernobyl accident’s radiation. The United Nations Scientific Committee on the Effects of Atomic Radiation Report to the General Assembly, with Scientific Annexes. United Nations Publications Sources and Effects of Ionizing Radiation, vol II: Effects. 2000.
Valentin J. Biological effects after prenatal irradiation (embryo and fetus): ICRP Publication 90 approved by the commission in October 2002. Amsterdam: Elsevier (Pergamon); 2003.
Vishnevskaja V. On changes in mental health of children living in areas contaminated with radionuclides. In Social, psychological and psychoneurological aspects of Chernobyl NPP accident consequences, 28–30 Sept 1992. Kiev. 1992.
Weinstock M. The long-term behavioural consequences of prenatal stress. Neurosci Biobehav Rev. 2008;32(6):1073–86.
Zablotska LB. 30 years after the Chernobyl nuclear accident: time for reflection and re-evaluation of current disaster preparedness plans. J Urban Health. 2016;93(3):407–13.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Loganovsky, K.N., Loganovskaya, T.K. (2019). Responses to Children’s Mental Health Needs Following the Chernobyl Disaster. In: Hoven, C., Amsel, L., Tyano, S. (eds) An International Perspective on Disasters and Children's Mental Health. Integrating Psychiatry and Primary Care. Springer, Cham. https://doi.org/10.1007/978-3-030-15872-9_10
Download citation
DOI: https://doi.org/10.1007/978-3-030-15872-9_10
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-15871-2
Online ISBN: 978-3-030-15872-9
eBook Packages: MedicineMedicine (R0)