
Abstract
The acute presentation of rectal and anal cancer can be varied and difficult to manage. Accurate diagnosis and staging are crucial first steps in management of each malignancy. Indications for acute intervention include obstruction, hemorrhage, and perforation. If the patient has failed initial attempts at conservative or endoscopic management, surgical options should be considered. Operative considerations include low anterior resection, abdominoperineal resection, and damage control operations consisting of washout, drainage, and diversion depending on the appropriate clinical situation.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Rectal Cancer
Clinical Presentation
Colorectal cancer is the third most common cancer diagnosed and the third most common cause of cancer death in the United States. Per the American Cancer Society, approximately 43,030 new cases of rectal cancer will be diagnosed in 2018 [1]. Of those, approximately 20% of colorectal cancer will present acutely as a surgical emergency [2]. Of critical importance in the treatment algorithm for rectal cancer is the site of pathology. High rectal cancer, defined as rectal cancer from 10–15 cm from the anal verge and above the peritoneal reflection, should be managed differently than a mid- to low rectal cancer that presents acutely. Like all cancers, tissue diagnosis is important to establish a treatment plan.
Initial Management
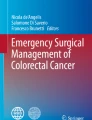
The initial step for identification is physical exam and lower endoscopy. Digital rectal exam is of utmost importance in identifying the location of the lesion in the rectum (anterior versus posterior), the distance from the anal verge, and the tumor’s location in relation to the anal sphincters (see Fig. 7.1). Rigid proctoscopy is a useful adjunct for visual identification of a lesion as well as affords the ability to sample any concerning masses. A rigid proctoscope can be easily performed in the office or the emergency department with adequate lighting, lubricant, and if needed a pre-procedural enema. Ideally a full colonoscopy should be performed when the patient is stable to identify location of the tumor and to rule out synchronous tumors. Approximately 3–5% of rectal cancers present with synchronous tumors that would alter the surgical approach [3]. Locoregional staging should be performed with magnetic resonance imaging of the pelvis (MR pelvis) or endorectal ultrasound to establish T staging and nodal involvement. Endorectal ultrasound often requires specialized expertise and is subject to operator technique; therefore MR pelvis is preferred at the authors’ institution. After locoregional staging, evaluation with CT chest/abdomen/pelvis is obtained to evaluate for the presence of metastatic disease. Approximately 20–25% of rectal cancers present with evidence of metastatic disease (see Table 7.1).

Rectum and anus anatomy, coronal view
Stage II–III disease, if possible, should be referred for neoadjuvant chemoradiation. Following neoadjuvant therapy, referral back to a colorectal surgeon for resection is recommended. However, rectal cancer that acutely presents with bleeding causing hemodynamic instability, obstruction, perforation, or peritonitis is an indication for urgent operative intervention.
Management of acutely presenting rectal cancer should always begin with resuscitation. The main modalities of resuscitation often initiated in the emergency room are IV fluid administration, broad-spectrum antibiotics for sepsis, blood product transfusion as needed for anemia or coagulopathy, and identification of the cause of acute presentation. Lower endoscopy is an invaluable tool for the diagnosis and acute management of rectal cancer. The use of endoscopic management for bleeding and obstruction is presented in another chapter (See Chap. 11, Endolumenal Therapies for Bleeding and Obstructing Colorectal Malignancy).
Surgical Management
After diagnosis, localization, and staging of the offending pathology, surgical management should be individualized to patients who can tolerate an operation that adheres to oncologic principles. Patients presenting with an acute clinical obstruction with evidence of resectability on imaging are candidates for creation of a diverting ostomy as a bridge to neoadjuvant therapy prior to definitive resection [4]. However, surgeons should be aware that there can be a significant delay to neoadjuvant therapy and the subsequent definitive resection following creation of a decompressive ostomy compared to starting neoadjuvant therapy right away [5]. As such, surgeons should reserve a diverting ostomy only for those who are clinically obstructed (see Fig. 7.2).

CT images of obstructing high rectal tumor. (a) CT obstructing high rectal tumor with proximal colonic dilation, sagittal view. (b) CT obstructing high rectal tumor, axial view. The patient underwent endoscopic stenting but would eventually succumb to her metastatic disease [24]
If diversion is used, then referral to a colorectal surgeon should be considered for definitive resection. Additionally, evaluation by a tumor board should also be considered for timing and appropriateness of neoadjuvant therapy. If during the acute setting of obstruction, bleeding, or perforation, resection and anastomosis is considered, the surgeon must remember the oncologic principles. During definitive resection, the surgical principles required for radical transabdominal resection of rectal cancer include complete resection of the tumor and a high-quality total mesorectal excision (TME) with preservation of the autonomic pelvic nerve plexuses and clear circumferential radial margin (CRM) [6]. The use of a defunctioning stoma for anastomotic protection should be considered in any anastomosis performed under tension, in the setting of hemodynamic instability, or gross contamination from a perforation. It should be strongly considered in cases of a low pelvic anastomosis and after neoadjuvant chemoradiation. Laparoscopic resection of rectal tumors is safe with noninferior oncologic outcomes including quality of TME, improved postoperative SSI, and length of stay [7, 8]. The operating surgeon should perform whichever operation he/she feels comfortable performing to achieve the best clinical outcomes.
For tumors of the upper rectum (10–15 cm from the anal verge), a low anterior resection with mesorectal excision extending 5 cm below the distal edge of the tumor is the operation of choice [9]. For an intra-abdominal perforation or chronic obstruction of a high rectal tumor, LAR with primary anastomosis and diverting loop ileostomy or if necessary a Hartmann’s procedure should again be considered depending on the physiologic status of the patient.
For tumors of the middle rectum, a low anterior resection with total mesorectal excision is also indicated [10]. A clear distal bowel margin of at least 1 cm is required. A diverting stoma should again be considered in these cases.
For early-stage tumors of the lower rectum (T1, N0 or T2-3, N0) with a distance of >1 cm from the external anal sphincter, a LAR with TME and intersphincteric distal dissection with hand sewn coloanal anastomosis and diverting ileostomy can be considered [11]. However, for a tumor with the above characteristics and a coloanal anastomosis that would result in poor functional outcomes (i.e., a patient with existing fecal incontinence), an abdominoperineal resection is recommended.
For patients presenting with sepsis due to mid to low rectal tumors with proximal colonic perforation, with or without sphincter involvement, attempts at non-oncologic resectional management of the primary tumor can be considered in a damage control setting. Again, this would be control of the perforation with resection and an ostomy and mucous fistula. This damage control option can be considered in patients unable to tolerate a full resection or in an attempt to bridge to neoadjuvant chemoradiation for an attempt at sphincter preservation. For local sepsis from perforation of the rectal tumor in the pelvis, diverting ostomy with transrectal, transanal, or transperineal drainage should be considered. However, it should be noted again that all surgical options delay the timing to initiation of neoadjuvant therapy.
In cases of perforation of a high or mid rectal cancer, abdominal resection should be pursued to prevent worsening sepsis [12]. After initial resuscitation with IV fluids and antibiotics, a Hartmann’s procedure with resection of the tumor, mesorectum, and end colostomy and tagging of the distal rectal stump may be performed. Drain placement is recommended. Only in extremely rare selected patients with perforation and sepsis should a resection and primary anastomosis be considered. Drainage and proximal diversion with loop ileostomy would be strongly advised to protect and mitigate the consequences of an anastomotic leak if an anastomosis is performed.
The two types of diversionary stomas commonly employed are the loop ileostomy and loop colostomy. There is no clear answer to which is superior in terms of morbidity following resection. Ileostomies are associated with significantly less prolapse, septic complications, and reoperation rates compared to colostomies (see Fig. 7.3). However, colostomies have lower rates of dehydration, acute kidney injury, and resultant renal failure. Therefore, it is recommended that a loop ileostomy should be preferred and colostomy reserved for those who are at risk of dehydration [13]. Closure of the stoma can be performed 6–8 weeks following completion of any adjuvant therapy (see Table 7.2).

Loop ileostomy creation
Special Circumstances
Perforation while undergoing neoadjuvant therapy
Given the age of most patients diagnosed with rectal cancer, there are a number of special circumstances to be discussed. Patients with previously diagnosed locally advanced rectal cancer often are undergoing or have previously undergone chemoradiation in anticipation of upcoming operative resection. Occasionally these patients will present with contained or free perforations. Given the vasculitis following pelvic radiation, anastomoses in this setting are extremely tenuous and should be protected with proximal intestinal diversion. If the patient has completed or is near completion of neoadjuvant therapy and is not septic, an attempt at primary anastomosis with proximal diversion is reasonable depending on the conditions in the pelvis. If the patient presents acutely septic, resection and proximal diversion with an end colostomy should be considered.
The Anticoagulated Patient
A second scenario is the anticoagulated patient who presents with melena or hematochezia due to a rectal tumor. Often these patients are treated under current protocols of lower gastrointestinal bleeding which consists of temporarily holding and reversing anticoagulation medication. In the rare patient that anticoagulation cannot be stopped (i.e., recent cardiac stent placement on dual antiplatelet therapy), an exam under anesthesia with attempt to locally control bleeding can be considered. Use of local hemostatic adjuncts can be an invaluable tool to assist in bleeding control with surgical electricity use, manual compression, and hemostatic products such as Surgicel (mechanical oxidized cellulose hemostat), Combat Gauze (hemostatic procoagulant Kaolin-based dressing), Floseal (liquid bovine thrombin-fibrinogen adhesive), or Tisseel (liquid fibrinogen-thrombin adhesive) [14]. These products can be used locally without concern for systemic absorption. For patients who are not candidates for resection who present with excessive lower GI bleeding, consideration for angiogram and internal iliac branch embolization should be considered.
Abscess Formation
Another complex situation is the patient who presents with chronic or acute abscesses or pelvic sepsis due to perforation. All attempts at source control should be made with drainage, diversion, and resection in an attempt to bridge the patient to neoadjuvant chemotherapy +/− radiation for local control. These infections will undoubtedly delay the initiation of rectal cancer therapy and should be managed aggressively. Initial attempts at management with antibiotics and noninvasive drain placement via interventional radiology or endoscopically should be considered as first-line options. Operative washouts, if necessary, should be performed with a liberal use of surgical drain placement making it rare for a patient to require multiple operative washouts. This again would help to prevent further delays to neoadjuvant therapy.
Anal Cancer
Clinical Presentation
Anal cancer represents a small percentage of cancers of the GI tract. Per the American Cancer Society from 2018, the estimated incidence of anal cancer in the United States is 8580 new cases with resultant estimated deaths of approximately 1160 [15]. Risk factors associated with anal cancer include the presence of precancerous anal lesions such as high-grade anal intraepithelial neoplasms (AIN), chronic immunosuppression, HIV, and smoking. Knowledge of the anatomy of the anal canal assists in diagnosis and management of the various types of anal neoplasms. The surgical anal canal can be divided into two unequal areas by the dentate line: an upper zone lined with columnar epithelium supplied by the superior rectal artery and a lower zone lined with squamous epithelium supplied by the inferior rectal artery. The short segment area between the two is termed the anal transition zone. Neoplasms of the anal canal include squamous cell cancer, anal adenocarcinoma, neuroendocrine tumors, and anal melanoma (see Fig. 7.4).

Anal canal anatomy, coronal view
Anal cancers usually present with bleeding (45%) or palpation/sensation of a perianal mass (30%); however up to one third may be asymptomatic. Other complaints include discomfort while sitting, change in bowel habits, discharge, fecal incontinence (from sphincter infiltration), anal abscess, fissures, fistula, or very rarely obstruction. Diagnosis should be confirmed by visual inspection using an anoscope and pathologic biopsy when suspected. If neoplasm is confirmed, staging is performed with a digital rectal exam and a CT chest/abdomen/pelvis or combination PET/CT depending on local availability and expertise [16, 17].
Initial Management
Initial management of an acute presentation of anal cancer should include resuscitation and accurate diagnosis. Often with large masses, clinical evidence of neoplasm may be visually obvious, but multiple biopsy specimens should be obtained to confirm histologic diagnosis. Resuscitation with IV fluids for hypovolemia or dehydration should always be performed, especially when the patient presents with obstruction and sequestration of fluid. Rarely a patient will present with symptomatic anemia and should be transfused to a minimal hemoglobin safe for anesthesia (usually up to 7 g/dL at the author’s institution) or cessation of symptoms. Workup for and full reversal of any existing anticoagulation should also be initiated prior to any intervention. It is uncommon for anal cancer to cause an acute drop in hemoglobin, and given the usual age at presentation, concomitant diagnoses for alternate causes of anemia should be in the differential diagnosis and evaluated. A complete history including any previous colonoscopies should be elicited from the patient during initial workup [18].
Indications for Surgical Management
Emergent presentation requiring urgent surgical management of anal cancer is rare. Indications for surgical management include patients who present acutely with bleeding, obstruction, or those with a symptomatic anal mass without diagnosis. The surgical approach differs depending on the clinical presentation. For a slowly bleeding anal cancer without hemodynamic instability, prompt initiation of external beam radiation via radiation oncology is recommended, often with concurrent chemotherapy. For bleeding causing hemodynamic instability, various surgical approaches are available as damage control.
Surgical Approach
Perineal Approach
A perineal approach with the patient in high lithotomy or prone jackknife position affords the surgeon adequate positioning for full evaluation of the anal canal (see Fig. 7.5). For the acutely bleeding mass without other endoluminal sources, a prompt exam under anesthesia and anorectal exam should be performed. Attempts to incompletely resect the bleeding mass can be performed with the goal of bleeding cessation rather than a complete R0 resection. Strict avoidance of any injury to the rectum should be maintained to avoid further complicating the situation. Use of previously listed local hemostatic adjuncts can be an invaluable tool to assist in bleeding control. Complications of acute perineal debulking include the potential for abscess and fistula formation as well as a nonhealing wound which could delay definitive chemoradiation therapy for the patient.

Illustrations of prone jackknife and high lithotomy positioning
Tumors outside the anal canal that present acutely with lifestyle limiting pain may be amenable to debulking if below the dentate line (see Fig. 7.6). Wide local excision with at least 1 cm margin should be performed and can alleviate the patient’s acute symptoms. However, long-term oncologic benefit will depend on disease-free resection margins and adjunctive therapy with chemotherapy and radiation [19]. Though initial improvement in pain can be achieved, complications of abscess and fistula are common. A similar delay to definitive therapy and a deforming and unacceptable scar can result.

Anal tumors can also present with perianal abscess or fistulas. If the patient has an abscess, aggressive management with incision and drainage and postoperative antibiotics should be employed, bridging to eventual standard management with chemoradiation [20]. If suspicion of cancer exists without a tissue diagnosis, then a concurrent biopsy should be performed for histologic diagnosis. For supralevator abscesses associated with superior extension of an anal cancer, transabdominal or transgluteal drainage should be considered in addition to transrectal drainage. Antibiotics should cover skin flora as well as enteric bacteria (see Fig. 7.7).

Anal cancer with associated abscess and Penrose drain placement. (Anandam [26])
Abdominal Approach
In addition to a perineal approach, an abdominal approach may be indicated in acute anal cancer presentations that present with obstruction or fecal incontinence. Fecal incontinence is due to infiltration of the external sphincters by the tumor. The diversion is done to better control the fecal stream.
Diversion
Creation of a diverting loop ileostomy and loop colostomy are common treatment options to divert the intestinal stream and prevent perforation. Either can be performed laparoscopically or via an open technique to relieve an impending complete obstruction. A loop colostomy allows for proximal diversion and distal decompression via the efferent limb and can be performed at any part of the colon that will reach the abdominal wall without tension. The more distal the colostomy creation site, the more water can be absorbed, and solid stool will be extruded mimicking the natural function of the colon. Though an end colostomy may be appropriate in some circumstances, caution should be used when creating an end colostomy in the setting of a distal anal obstructing tumor for fear of creating a closed loop rectal obstruction. Diverting end colostomies, however, are more prone to prolapse as well as more difficult in terms of eventual closure through a peristomal incision should that be warranted in the future.
Though technically easier to create, a diverting loop ileostomy can be associated with peristomal dermatitis, pouching difficulties, dehydration, electrolyte disturbances, and even acute kidney injury due to high output. Similar to an end colostomy, caution should be warranted in the creation of an end ileostomy in a patient with a distal obstruction and a patent ileocecal valve. A meta-analysis of randomized controlled trials comparing diverting loop ileostomies and colostomies shows no difference between the two groups in terms of stoma complications or in time to ostomy closure [21].
Abdominoperineal Approach
For recurrent or persistent anal canal cancer following definitive chemoradiation therapy, consideration for an abdominoperineal resection should be discussed as salvage therapy [22]. Here again, consideration should be given for referral to a colorectal surgeon if the acute surgeon is not comfortable or familiar with this procedure. Consideration should be given to an APR if the patient has developed a recurrence following chemoradiation, is unable to tolerate initial definitive chemoradiation therapy, has developed intolerable fecal incontinence or lifestyle limiting anal pain, or has persistent disease months after chemoradiation [23]. In the acute setting of bleeding or obstruction, a damage control operation should be considered prior to definitive resection and permanent stoma. Following damage control procedures and bridging to definitive therapy, evaluation of the patient for a larger resection such as an abdominoperineal resection can be performed.
Conclusions
Acute presentations for anal and rectal cancers are fortunately not common, but they certainly may be seen by any general surgeon taking call. For rectal diseases, it is important to recognize the location of the disease in the rectum because this will dictate the type of surgery that is required. If the patient can be stabilized and neoadjuvant therapy can be initiated, this may relieve the symptoms allowing the opportunity for a more definitive cure afterward. If they cannot and a surgical decompression or hemorrhage control is needed, this will likely delay the start of chemoradiation therapy. For anal cancers, acute presentations can be controlled with local resection versus a diverting ostomy with/without hemorrhage control and drainage of associated abscesses if needed. Most anal cancers can be treated with chemoradiation therapy only. Surgery is reserved for those who fail chemoradiation therapy, who cannot tolerate chemoradiation therapy, or who have a complication while undergoing chemoradiation therapy. Patients at risk of dehydration and kidney disease should be considered for a colostomy as opposed to an ileostomy.
References
Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER cancer statistics review, 1975–2013. Bethesda: National Cancer Institute. http://seer.cancer.gov/csr/1975_2013/, based on November 2015 SEER data submission, posted to the SEER web site, April 2016.
Cuffy M, et al. Colorectal cancer presenting as surgical emergencies. Surg Oncol. 2004;13(2–3):149–57.
Van Leersum NJ, et al. Synchronous colorectal carcinoma. Dis Colon Rectum. 2014;57(4):460–6. https://doi.org/10.1097/dcr.0000000000000068.
Anderson BJ, Hill EG, Sweeney RE, Wahlquist AE, Marshall DT, Staveley O’Carroll KF, Cole DJ, Camp ER. The impact of surgical diversion before neoadjuvant therapy for rectal cancer. Am Surg. 2015;81(5):444–9.
Patel JA, Fleshman JW, Hunt SR, Safar B, Birnbaum EH, Lin AY, Mutch MG. Is an elective diverting colostomy warranted in patients with an endoscopically obstructing rectal cancer before neoadjuvant chemotherapy? Dis Colon Rectum. 2012;55(3):249–55.
Heald R, Ryall R. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;327(8496):1479–82.
Guillou PJ, Quirke P, Thorpe H, et al. Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial): multicentre, randomised controlled trial. Lancet. 2005;365:1718–26.
Trastulli S, Cirocchi R, Listorti C, et al. Laparoscopic vs open resection for rectal cancer:a meta-analysis of randomized clinical trials. Color Dis. 2012;14:e277–96.
Monson JR, Weiser MR. Practice parameters for the management of rectal cancer (Revised). Dis Colon Rectum. 2013;48(3):535–50. https://doi.org/10.1007/s10350-004-0937-9.
Scott N, Jackson P, Al-Jaberi T, Dixon MF, Quirke P, Finan PJ. Total mesorectal excision and local recurrence: a study of tumour spread in the mesorectum distal to rectal cancer. Br J Surg. 1995;82:1031–3.
Kuvshinoff B, Maghfoor I, Miedema B, et al. Distal margin requirements after preoperative chemoradiotherapy for distal rectal carcinomas: are < or = 1 cm distal margins sufficient? Ann Surg Oncol. 2001;8:163–9. 77.
Slanetz CA Jr. The effect of inadvertent intraoperative perforation on survival and recurrence in colorectal cancer. Dis Colon Rectum. 1984;27:792–7.
Rondelli F, Reboldi P, Rulli A, et al. Loop ileostomy versus loop colostomy for fecal diversion after colorectal or coloanal anastomosis:a meta-analysis. Int J Color Dis. 2009;24:479–88.
Chiara O, et al. A systematic review on the use of topical hemostats in trauma and emergency surgery. BMC Surg. 2018;18(1):68.
American Cancer Society. Cancer facts & figures 2018. Atlanta: American Cancer Society; 2018.
Otto SD, Lee L, Buhr HJ, Frericks B, Höcht S, Kroesen AJ. Staging anal cancer: prospective comparison of transanal endoscopic ultrasound and magnetic resonance imaging. Gastrointest Surg. 2009;13:1292–8.
Krengli M, Milia ME, Turri L, et al. FDG-PET/CT imaging for staging and target volume delineation in conformal radiotherapy of anal carcinoma. Radiat Oncol. 2010;5:10.
Wasvary HJ, Barkel DC, Klein SN. Is total colonic evaluation for anal cancer necessary? Am Surg. 2000;66:592–4.
Gordon PH, et al. Current status: perianal and anal canal neoplasms. Dis Colon Rectum. 1990;33:799–808.
Gaertner WB, Hagerman GF, Finne CO, Alavi K, Jessurun J, Rothenberger DA, Madoff RD. Fistula-associated anal adenocarcinoma: good results with aggressive therapy. Dis Colon Rectum. 2008;51(7):1061–7.
Guenaga KF, et al. Ileostomy or colostomy for temporary decompression of colorectal anastomosis. Cochrane Database Syst Rev. 2007;(1):CD004647.
Renehan AG, Saunders MP, Schofield PF, O’Dwyer ST. Patterns of local disease failure and outcome after salvage surgery in patients with anal cancer. Br J Surg. 2005;92:605–14.
Mariani P, Ghanneme A, De la Rochefordière A, Girodet J, Falcou MC, Salmon RJ. Abdominoperineal resection for anal cancer. Dis Colon Rectum. 2008;51:1495–501.
Anandam J. CT image of obstructing high rectal tumor. [Photograph]. Dallas: University of Texas Southwestern; 2018.
Anandam J. Fungating anal cancer. [Photograph]. Dallas: University of Texas Southwestern; 2018.
Anandam J. Anal cancer with associated abscess. [Photograph]. Dallas: University of Texas Southwestern; 2018.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Anandam, J., Abdelsayed, J. (2019). Abdominal and Perineal Operative Considerations for Acute Presentations of Anal and Rectal Malignancies. In: Lim, R. (eds) Multidisciplinary Approaches to Common Surgical Problems. Springer, Cham. https://doi.org/10.1007/978-3-030-12823-4_7
Download citation
DOI: https://doi.org/10.1007/978-3-030-12823-4_7
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-12822-7
Online ISBN: 978-3-030-12823-4
eBook Packages: MedicineMedicine (R0)