
Abstract
Chemotherapy and radiation treatments for cancer and other conditions can cause permanent infertility. Adult and adolescent males who have reached Tanner III of pubertal development have the option to cryopreserve a semen sample with sperm prior to treatment and use their sample in the future to have biological children using established assisted reproductive technologies. This option is not available to prepubertal boys who are not yet producing mature sperm. However, these boys do have spermatogonial stem cells in their testes that are poised to initiate sperm production at puberty. Centers in the United States and abroad are actively cryopreserving testicular tissue for prepubertal cancer patients, bone marrow transplant patients, and others in anticipation that stem cell therapies will be available for them in the future. This chapter reviews the standard of care options for male patients, as well as experimental techniques, including spermatogonial stem cell transplantation, testicular tissue grafting and xenografting, testicular tissue organ culture, de novo testicular morphogenesis, and pluripotent stem cell-derived gametogenesis.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Stem cells
- Spermatogonial stem cells
- Spermatogenesis
- Cryopreservation
- Sperm banking
- Testicular tissue cryopreservation
- Fertility
- Fertility preservation
- Infertility
- Klinefelter
-
Fertility preservation options for pubertal boys and adult men include sperm banking and testicular sperm extraction (TESE).
-
For prepubertal boys, there are no standard of care options. The only option for prepubertal boys is testicular tissue cryopreservation, which is still considered experimental.
-
Experimental techniques currently in the pipeline for restoring fertility with cryopreserved testicular tissues include spermatogonial stem cell transplantation, de novo testicular morphogenesis, testicular tissue grafting and xenografting, and testicular tissue organ culture.
-
Many centers around the world are actively cryopreserving testicular tissues for prepubertal boys who are at risk for infertility in anticipation that those samples can be use in the future for reproductive purposes.
1 Introduction
Improvements in cancer therapies have resulted in improved 5-year survival rates [68] and an increasing focus on quality of life after cure. Cancer survivors report that parenthood is important to them, and distress over infertility has long-term psychological and relationship implications [152]. Therefore, the American Society for Clinical Oncology [96, 100] and the American Society for Reproductive Medicine [37, 38] recommend that patients be educated about the reproductive risks associated with their therapy as well as options for preserving fertility.
Whole-body radiation , radiation to the hypothalamus, pituitary, or testes, and alkylating and heavy metal chemotherapies are particularly toxic to male fertility [54, 67, 80, 94, 97, 105, 171]. This is an important public health concern because nearly 25,000 males under the age of 44 will be diagnosed with cancer each year in the United States. Epidemiological data [54, 68, 106] indicate that most of these patients will survive their cancer, but many will receive treatments that put them at significant risk for infertility. The Childhood Cancer Survivor Study (CCSS) has shown that male survivors of childhood cancer are half as likely to achieve a pregnancy with their partner compared to their male siblings [54]. When rates of infertility were studied in the CCSS, 46% of cancer survivors compared to 18% of siblings reported experiencing infertility [172].
Patients and families with children facing a cancer diagnosis and planning for treatment may be ill-prepared to discuss, think about, or take action to preserve their future fertility before initiating treatment. Unfortunately, while healthcare professionals acknowledge the need to discuss fertility preservation with their patients, fertility counseling is not consistently implemented [154, 155]. Consequently, many families are inadequately informed of the risk of infertility [154] and the options they have to preserve their child’s fertility [140]. Insufficient training for medical staff to counsel patients on this sensitive topic has been identified as an important factor, along with patient factors such as degree of disease, age, and cultural/religious concerns [48]. Both parents and adolescent cancer patients identify fertility as an important life goal after cancer [87].
Spermatogonial stem cells (SSCs) are at the foundation of spermatogenesis and maintain continuous sperm production throughout the postpubertal life of men [27, 123, 161, 165]. Spermatogenesis is an extraordinarily productive process that generates more than 100 million sperm each day from the testes of adult men [156]. Because spermatogenesis is such a productive system, it can sometimes become an unintended target of cancer therapies that are toxic to rapidly dividing cells. Therapies that deplete the stem cell pool and/or damage the somatic niche can cause temporary or permanent infertility. Infertility in male cancer survivors is due to impaired spermatogenesis, which can be characterized as oligospermia (<15 million sperm/ml of semen) or azoospermia (no sperm in the semen). High-dose alkylating agents (e.g., cyclophosphamide, busulfan, melphalan, chlorambucil), bleomycin, testicular radiation >400 cGy, or genitourinary surgery are associated with the highest risk of developing azoospermia [20, 97, 105, 107, 171, 172]. In contrast to spermatogenesis, the steroidogenic function of the testes appears to be less affected by cancer therapy and the testosterone-producing Leydig cells appear to be fairly resistant to damage by chemotherapy [22].
2 Sperm Banking: The Gold Standard Procedure for Male Fertility Preservation
Boys who have reached Tanner III of pubertal development and adult men have the option to cryopreserve a semen sample containing sperm before initiating treatment, which can be thawed at a later date to achieve pregnancy by intrauterine insemination [3], in vitro fertilization (IVF, [159]), or IVF with intracytoplasmic sperm injection (ICSI, [118]). Unfortunately, only about 24% of adult men freeze a semen sample before initiating their therapy [153]. Some males as young as 12 or 13 years of age are capable of producing a semen sample. Semen is produced via masturbation, but other methods such as vibratory stimulation [151] or electroejaculation [2, 45] have been used. Ideally, patients should provide two to three specimens obtained at 2–3 day intervals. Standard semen analysis would be performed by the andrology laboratory, and results will be available within 1 day to confirm whether the semen specimens contain sperm. Some patients have asked if it is safe to preserve sperm if they have just started chemotherapy. There is insufficient data and no consensus about best practices in this scenario. Please see the following references for discussion [15, 21, 104].
3 Testicular Sperm Extraction (TESE)
For patients who did not preserve a semen sample and have persistent azoospermia after cancer therapy, there is the option to retrieve rare sperm directly from the testis during a surgical procedure called testicular sperm extraction (TESE). This is possible because a few SSCs may survive the gonadotoxic therapy and produce focal areas of spermatogenesis in the seminiferous tubules. Hsiao and colleagues recently described their experience with 73 patients with postchemotherapy azoospermia [70]. They reported that sperm were successfully retrieved from 37% of patients on initial attempt, with an overall success rate of 42.9%. Fertilization rate with the retrieved sperm was 57%; the pregnancy rate was 50%; and the live birth rate was 42%. Success in retrieving sperm was treatment dependent in that study, with the lowest sperm recovery success rates (21%) in patients receiving alkylating chemotherapy [70]. Picton and colleagues surveyed results from a total of five centers (including the Hsiao et al. study) and reported an overall sperm recovery rate of 44% in azoospermic patients undergoing TESE after chemotherapy [124].
There are currently no standard options to treat the infertility of adult patients who did not cryopreserve a semen sample and were not successful with the TESE/ICSI procedure. Adoption and third-party reproduction are family-building options for these patients, but most cancer survivors prefer to have their own biological children [96]. Therefore, sperm banking should be discussed with all pubertal, adolescent, and adult males who are able to produce a semen sample.
4 TESE for Men and Adolescent Boys with Klinefelter Syndrome
TESE is also used effectively for Klinefelter Syndrome (KS) patients who typically have a 46, XXY karyotype and azoospermia, often characterized as a Sertoli cell only phenotype. However, germ cells are sometimes present in the testes of KS patients, which produce focal areas of spermatogenesis in the testes. Success rates for retrieving sperm by TESE from the testes of KS patients are consistently above 50% (50–72%) [14, 88, 114, 130, 147, 183] and are similar to the success rates reported for TESE in azoospermic patients without Klinefelter syndrome. Most importantly, pregnancy rates and live birth rates after ICSI are similar in couples with or without KS, and children fathered by KS patients have a normal karyotype [14, 147, 183]. The infertility phenotype of KS patients is considered progressive, with rapid declines in spermatogenesis during the teenage years [5, 103, 174]. Previous studies in adult KS patients reported that sperm recovery rates were significantly lower after the age of 35 [14, 114, 130]. Therefore, early intervention may be important to preserve the fertility of Klinefelter patients. In fact, some centers have protocols to retrieve sperm by TESE from adolescent boys with KS based on the understanding that the likelihood of retrieving sperm in later years will be reduced [103, 112]. Other groups, however, did not find that performing TESE at a younger age increased the chances of successful sperm retrieval [126, 174], and there is considerable debate about the benefit of early fertility intervention for KS patients [112, 134].
Typically, pubertal development is determined by Tanner staging of pubic hair and genitalia development, testicular size, and hormone levels. In most boys, the median age of onset of spermatogenesis is 13–14 years, correlating to a genital Tanner stage III. However, in patients with KS, the early stages of pubertal development that consist of increase in size of the testes are not reliable since testicular size is often diminished. It is currently unknown when spermatogenesis starts in boys with KS. While it seems to be commonly accepted that there is a progressive depletion of germ cells in the testes of KS patients after the onset of puberty, the evidence to support this notion is equivocal with small patient populations, lack of controls, and no longitudinal data. In addition, the standard therapy for boys with KS is testosterone replacement therapy in order to trigger entry and progression of puberty, secondary sexual characteristics, bone development, and longitudinal growth. However, testosterone supplementation also suppresses spermatogenesis (if present) even further through negative feedback on the hypothalamus-pituitary-gonadal axis. Some argue that any intervention to preserve fertility for KS patients should ideally precede hormone replacement therapy [169], although recent studies have shown that testosterone replacement therapy might not negatively affect spermatogenesis in KS patients [42, 103]. The risks of invasive surgical procedures like TESE for boys should be carefully weighed against the possible benefits for this unique patient population. Systematic, longitudinal studies are needed to characterize spermatogenic decline in KS patients.
5 Gonadal Shielding
Gonadal shielding can be used to protect the testes from scatter radiation using lead shielding. The proper shielding technique should be carefully evaluated on a case-by-case basis depending on total radiation dose, fractionation, and the specific mode of delivery of the external beam therapy [39, 142, 180]. However, when the testicular tissue requires radiation therapy as a part of cancer treatment, shielding cannot be used. At other times, the proximity of the testes to the target of radiation results in scatter radiation to the testes, which can also result in impaired spermatogenesis.
6 Testicular Tissue Banking: An Experimental Procedure for Fertility Preservation
There are currently no standard of care options to preserve the future fertility of prepubertal boys who are not yet producing sperm. This is an important human health concern because, with improved therapies, the event-free survival rate of children with cancer is 85% [69], and these survivors can look forward to a full and productive life after cure. We estimate that each year in the United States, more than 2000 boys will receive gonadotoxic treatments for cancer or other conditions (e.g., myeloablative conditioning prior to bone marrow transplantation) that put them at high risk for infertility [166]. Prepubertal boys are not producing sperm, but they do have spermatogonial stem cells (SSCs) in their testes that are poised to initiate sperm production at the time of puberty [119]. There are several methods in the research pipeline, including SSC transplantation, testicular tissue grafting or xenografting, testicular tissue organ culture, and de novo testicular morphogenesis that might be used to restore spermatogenesis or fertility from cryopreserved SSCs and/or testicular tissue. Induced pluripotent stem cell (iPSC) technologies may also be a fertility option for cancer survivors in the future. These methods are reviewed in this chapter.
Anticipating that new therapies will be available in the future, many centers in the United States and abroad have determined that it is reasonable to preserve testicular tissue for young patients who are at risk for infertility and have no other options to preserve their fertility [50, 53, 81, 116, 124, 139, 141, 178]. Testicular tissue-based fertility preservation methods for children are considered experimental and should be performed with institutional review board (IRB) oversight and approval. Although no pregnancies from cryopreserved testicular tissues have been reported in humans to date, two centers reported that the majority of parents consented to fertility preservation procedures on behalf of their children [49, 176, 178].
7 Considerations for Testicular Tissue Collection, Processing, and Freezing
Testicular tissue for cryopreservation is obtained via needle biopsy, wedge biopsy, or orchiectomy, ideally before the initiation of gonadotoxic treatment (surgery, chemotherapy, radiation). There is insufficient experience or evidence to recommend a particular surgical approach or orchiectomy, and each center will make those decisions based on individual and/or institutional biases about what is in the best interest of the patient in the short term and long term. Needle biopsy may be the least invasive but has an increased risk of unmitigated bleeding and recovers the least amount of tissue for downstream fertility applications. Wedge resection is more invasive than needle biopsy but may allow recovery of more testicular tissue (depending on surgeon preference), and bleeding can be controlled during surgery. Orchiectomy (removal of an entire testis) is the most invasive procedure but allows for the greatest recovery of testicular tissue for downstream fertility applications, and bleeding can be controlled during surgery. Collection of more tissue at the time of surgery should correlate with increased recovery of SSCs and greater flexibility for future fertility applications. However, limited tissue should not be a deterrent to enrollment in a testicular tissue cryopreservation protocol. There are several experimental cell-based and tissue-based options under development with different requirements for the amount of cells/tissue that will be needed.
There are no established “best practices” for processing and freezing testicular tissue or cells. Two labs examined the postthaw recovery of spermatogonia from cryopreserved human testis cell suspensions versus intact pieces of testicular tissue. Yango and colleagues reported that recovery of SSEA4+ (undifferentiated spermatogonia marker) spermatogonia from cryopreserved fetal testicular tissue was similar to cryopreserved testicular cells, but recovery of SSEA4+ cells from cryopreserved adult testicular cells was greater than cryopreserved testicular tissue [182]. Pacchiarotti and coworkers reported that cryopreservation of testicular tissue was comparable in most aspects to cryopreservation of a cell suspension. However, while the viability of total cells from the cryopreserved tissue was higher than the cryopreserved cell suspension, the recovery of SSEA4+ and VASA+ (pan germ cell marker) germ cells from cryopreserved tissue pieces tended to be greater than cryopreserved cell suspensions. These differences were not significant [117].
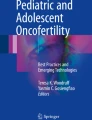
For fertility preservation, most centers are freezing intact pieces of testicular tissue for patients because this preserves the option for both tissue-based and cell-based therapies in the future [11, 50, 53, 81, 115, 124, 164, 178]. Biopsied testicular tissues are typically cut into small pieces (1–9 mm3), suspended in a DMSO-based freezing medium, and frozen at a controlled slow rate using a programmable freezing machine (◘ Fig. 17.1) [50, 81, 82, 116, 124, 164, 177, 178]. Some centers have reported using an ethylene glycol-based freezing medium instead of DMSO [19, 93, 163], and some centers have reported that the viability of vitrified testicular tissue is similar to tissue frozen at a controlled slow rate [13, 26, 127, 138]. This may improve access to testicular tissue freezing technology in centers that do not have programmable freezing machines. The experimental endpoints that have been used to evaluate freezing protocols have been varied and include cell viability, immunocytochemistry for spermatogonial markers, ultrastructural, histological and/or immunohistochemical examination of cultured or grafted tissue, and hormone production. Systematic studies on prepubertal human testicular tissues with evaluation of both cell-based and tissue-based endpoints are needed. It is possible that the optimal freezing condition depends on the intended use of the tissue or cells.

Testicular tissue cryopreservation . Testicular tissues are transported on ice from the operating room to the andrology lab in a sterile specimen container containing medium. (a) The tissue is kept cool and processed in a sterile environment with sterile tools. (b) Most centers cut the testicular tissue into small pieces (1–9 mm3) and deposit these pieces in cryovials with DMSO-based freezing medium. (c) Controlled slow rate freezing using a freezing machine
8 Testicular Cell-Based Methods to Preserve and Restore Male Fertility
Spermatogonial Stem Cell Transplantation
Spermatogonial stem cell transplantation was first described by Ralph Brinster and colleagues in 1994, who demonstrated that SSCs could be isolated and transplanted to regenerate spermatogenesis in infertile recipient mice [17, 18]. SSC transplantation has now been reported in mice, rats, pigs, goats, bulls, sheep, dogs, and monkeys, and donor-derived progeny have been produced by natural breeding in mice, rats, goats, and sheep [16, 60,61,62, 72, 73, 84, 108, 110, 113, 148, 157]. SSCs from donors of all ages, newborn to adult, are competent to regenerate spermatogenesis [137, 157], and SSCs can be cryopreserved and retain spermatogenic function upon thawing and transplantation [28, 29, 60]. Thus, it appears feasible that a testicular tissue biopsy (containing SSCs) could be obtained from a prepubertal boy prior to gonadotoxic therapy, frozen, thawed at a later date, and transplanted back into his testes to regenerate spermatogenesis. If spermatogenesis from transplanted cells is robust, this approach may restore natural fertility, allowing survivors to achieve pregnancy with their partner by natural intercourse and have biological children.
Radford and colleagues already reported cryopreserving testicular cells for 11 adult non-Hodgkin’s lymphoma patients in 1999 and subsequently reported transplanting autologous frozen and thawed testis cells back into the testes of seven survivors [128, 129]. The fertility outcomes for patients in that study have not been reported, and even if the men fathered children, it would not be possible to ascertain whether the sperm arose from transplanted stem cells or surviving endogenous stem cells. This uncertainty will always plague the interpretation of human SSC transplant studies where it is not ethically possible to genetically mark the transplanted cells because the genetic modification would be transmitted to the progeny. Therefore, large epidemiological datasets generated over decades will be required to prove the fertility benefit of SSC transplantation. Nonetheless, this study demonstrates that patients are willing to pursue experimental stem cell-based options even when there is no guarantee of a fertile outcome. There are no published reports of SSC transplantation in humans since Radford’s follow-up report of his non-Hodgkin’s lymphoma patients in 2003 [128].
9 Translating Spermatogonial Stem Cell Transplantation into the Clinic: Challenges and Opportunities
Considering the progress in several animal models and the fact that testicular tissues have already been cryopreserved for hundreds of human patients worldwide [50, 53, 81, 116, 128, 129, 139, 141, 178], it seems reasonable to expect that SSC transplantation and/or other stem cell technologies will impact the fertility clinic in the next decade. However, there are several safety and feasibility issues that must be considered.
Spermatogonial Stem Cell Culture
Based on our experiences at the Fertility Preservation Program in Pittsburgh [116] and published reports [50, 81], it is reasonable to expect that 50–1000 mg of testicular tissue can be obtained by wedge biopsy or needle biopsy from a single testis of a prepubertal boy. This is a small amount of tissue relative to the size of adult human testes that can range from 11 to 26 g in size [167]. It is widely believed that the number of stem cells in biopsies from prepubertal boys will be small and that SSCs will have to be expanded in culture prior to transplant. Conditions for maintaining and expanding rodent SSCs in culture are well established, and SSCs maintained in long-term culture (e.g., several months to 1 year) remain competent to regenerate spermatogenesis and restore fertility [56, 76, 77, 92, 133, 136].
If cultured human SSCs function like cultured rodent SSCs, it should be feasible to expand a few stem cells obtained from the testis biopsy of a prepubertal boy to a number sufficient to produce robust spermatogenesis upon transplantation back into his testes when he is an adult. Several studies have reported culturing human SSCs [1, 4, 9, 23, 24, 44, 51, 55, 58, 89, 98, 99, 102, 109, 111, 125, 139, 141, 158, 175, 184], including two studies in which cultures were established from the testes of prepubertal patients [139, 175]. Human SSC cultures have been evaluated by quantitative PCR or immunocytochemistry for spermatogonial markers or xenotransplantation into mouse testes. Strategies to isolate and culture human spermatogonia have been unique to each study, and to date, no approach has been independently replicated in another laboratory. Also, the field is frustrated by the lack of a functional assay to test the full spermatogenic potential of cultured human cells.
Malignant Contamination
A testicular biopsy obtained from a cancer patient could harbor malignant cells, especially for patients with leukemia. Kim and colleagues [83] reported that 20% of boys with acute lymphocytic anemia had malignant cells in their testicular tissue prior to the initiation of oncologic treatment. Jahnukainen and colleagues [74] reported the transmission of leukemia after transplantation of testis cells from terminally ill leukemic rats into the testes of nonleukemic recipients. The same group further demonstrated that transplantation of as few as 20 leukemic cells was sufficient for disease transmission, leading to terminal leukemia within 3 weeks.
Because infertility is not life threatening and fertility treatments are elective, it is essential that the risk of cancer recurrence after transplant be reduced to zero. Fluorescence-activated cell sorting (FACS) and magnetic-activated cell sorting (MACS) strategies to isolate and enrich therapeutic spermatogonia from testis cell suspension while removing malignant contamination have been explored with mixed results. Fujita and coworkers isolated germ cells from the testes of leukemic mice in the forward scatter high and side scatter low fraction (positive selection), which was then further divided into fractions that were CD45/MHC class I antigens (H-2Kb/H-2Db) double-positive and CD45/MHC class I double-negative cells. All recipient males injected with the CD45+/MHC class I+ cells developed terminal leukemia within 40 days. All mice injected with CD45-/MHC class I− cells survived for 300 days without the onset of leukemia and produced donor-derived offspring [40]. In a subsequent study, the same group reported that seven out of eight human leukemic cell lines expressed the cell surface antigens CD45 and MHC class I [41]. In a rat model of Roser’s T-cell leukemia, Hou and colleagues concluded that single parameter selection using either leukemic (CD4 and MHC Class I) or SSC (Ep-CAM) markers was not sufficient to eliminate malignant contamination [66], but malignant contamination was successfully removed using a combination of leukemia and SSC markers (plus/minus selection) [32, 59]. Using similar positive/negative selection strategies, Hermann and colleagues isolated VASA+ germ cells in the THY-1+/CD45− fraction of leukemia-contaminated prepubertal nonhuman primate testis cells [59], and this fraction did not produce tumors in mice. Dovey and colleagues contaminated human testis cells with MOLT-4 acute lymphoblastic leukemia cells and demonstrated by xenotransplantation that the Ep-CAMlo/HLA-ABC−/CD49e− fraction was enriched 12-fold for transplantable human SSCs and was devoid of malignant contamination [32]. Collectively, these results are encouraging, but caution is still warranted as Geens and colleagues concluded, using EL-4 lymphoma contaminated mouse and human testis cells, that FACS- and MACS-based methods were insufficient to remove malignant contamination [47].
It will not be possible to perform comprehensive in vivo testing on patient samples because this would limit the amount of sample available for fertility therapy. More sensitive PCR-based methods have been described for detection of minimal residual disease (MRD), and this approach has identified malignant contamination in many ovarian tissue samples that were preserved for leukemia patients, even after negative histology and immunocytochemistry examination [30, 135]. However, in one of those studies, Dolmans and colleagues obtained disparate results from histology, qRT-PCR, and xenografting of ovarian tissues from leukemia patients. Quantitative RT-PCR to detect MRD revealed the possibility of malignant contamination in 9 of the 16 samples that was not detected by histological examination. However, when those ovarian tissues were grafted into recipient mice, only five of the nine samples with positive MRD had evidence of leukemic cells 3 months after transplantation [30]. Were the MRD results in the other four cases nefarious or were they accurate and the leukemic cells simply failed to survive freezing, thawing, and grafting? In the absence of a definitive and practical test of malignant contamination, alternatives to autologous transplantation are needed for patients with hematogenous cancers, testis cancers, or cancers that metastasize to the testes.
De Novo Testicular Morphogenesis
Testicular cells (including germ cells, Sertoli cells, peritubular myoid cells, and Leydig cells) have the remarkable ability to reorganize to form normal looking seminiferous tubules when grafted under the skin of recipient mice [8, 33, 43, 64, 86]. Ina Dobrinski and colleagues disaggregated neonatal pig and sheep testis cells, pelleted them by centrifugation, and grafted under the skin of immune-deficient mice. When grafts were recovered between 16 and 41 weeks after transplant, cells had reorganized to form seminiferous tubules with complete spermatogenesis [8, 64]. In a remarkable extension of this approach, Kita and colleagues [86] mixed fetal or neonatal testis cells from mice or rats with GFP+-cultured mouse germline stem cells and growth factor-reduced matrigel (extracellular matrix) and grafted under the skin of immune-deficient mice. Seven to 10 weeks after grafting, seminiferous tubules with complete spermatogenesis originating from both intrinsic germ cells and cultured (GFP+) germ cells were observed. Tubules were dissected and GFP+ round spermatids were recovered and injected into mouse oocytes. The resulting embryos were transferred to recipient females, which gave birth to ten mouse pups, including four with the GFP transgene. In vitro organoid systems have also been developed. In mice and rats, the most promising results have been achieved using 3D scaffolds [6, 95, 160], where postmeiotic cells and spermatozoa developed. In vitro organoid cultures have been less successful with human cells. Maintenance of early and late spermatogonia was reported by several studies [10, 122, 170]; however, only two of the studies observed the presence of postmeiotic markers [122, 170]. These reports used pubertal or adult human tissues that already contain postmeiotic cells, which can make it difficult to determine the origin of the cells expressing the postmeiotic markers. To date, no human sperm has been produced using this model. One day it may be possible to “build a testis,” in vitro or in vivo, on the scaffold of a decellularized human testis [12].
10 Testicular Tissue-Based Methods to Preserve and Restore Male Fertility
Testicular Tissue Grafting and Xenografting
Testicular tissue grafting may provide an alternative approach for generating fertilization competent sperm from small testicular biopsies. In contrast to the SSC transplantation method in which SSCs are removed from their cognate niches and transplanted into recipient seminiferous tubules, grafting involves transplantation of the intact SSC/niche unit in pieces of testicular tissue. Honaramooz and colleagues reported that grafted testicular tissue from newborn mice, rats, pigs, and goats, in which spermatogenesis was not yet established, could mature and produce complete spermatogenesis when xenografted into nude mice [65]. The same group later reported the production of live offspring from sperm obtained from mouse testicular tissue grafts [149]. Fertilization-competent sperm was also produced from xenografts of prepubertal nonhuman primate testicular tissue transplanted into mice [63]. These results suggest that it may be possible to obtain fertilization-competent sperm by xenografting small pieces of testicular tissue from a prepubertal cancer patient under the skin of mice or other animal recipients such as pigs that are already an established source for human food consumption, replacement heart valves [7, 75], and potentially other organs [25]. Xenografting would also circumvent the issue of malignant contamination. However, the xenografting approach raises concerns about xenobiotics because viruses from mice, pigs, and other species can be transmitted to human cells [85, 173]. There is no evidence to date that xenografted human testicular tissue can produce spermatogenesis or sperm in mice [46, 52, 146, 150, 168, 179]. However, there is reason for optimism because Sato and colleagues observed primary spermatocytes 1 year after xenografting testicular tissue from a 3-month-old boy who clearly did not have spermatocytes at the time of transplantation [146]. Xenografting of human testicular tissue to species other than mice has not been tested to our knowledge.
If malignant contamination of the testicular tissue is not a concern, autologous testicular tissue grafting can be considered. Luetjens and colleagues demonstrated that fresh autologous testicular tissue grafts from prepubertal marmosets could produce complete spermatogenesis when transplanted into the scrotum, but not under the skin [101]. Frozen and thawed grafts did not produce complete spermatogenesis in that study, but those grafts were only transplanted under the skin. Therefore, additional experimentation is merited. Testicular tissue grafting will not restore natural fertility, but could generate haploid sperm that can be used to fertilize oocytes by ICSI.
Testicular Tissue Organ Culture
Sato and colleagues reported that intact testicular tissues from newborn mice (2.5–3.5 days old) could be maintained in organ culture and mature to produce spermatogenesis, including the production of fertilization-competent haploid germ cells [144, 145]. Testicular tissues from neonatal mice were minced into pieces (1–3 mm3) and placed in culture at the gas–liquid interface on a slab of agarose that was soaked in medium. Haploid round spermatids and sperm were recovered from the tissue after 3–6 weeks in culture and used to fertilize mouse eggs by ICSI. The resulting embryos were transferred to pseudopregnant females and gave rise to healthy offspring that matured to adulthood and were fertile. If testicular tissue organ culture can be translated to humans, it will provide an alternative to autologous SSC transplantation, autologous grafting, and xenografting in cases where there is concern about malignant contamination of the testicular tissue. The same authors were also successful to produce haploid germ cells in an organ culture of frozen and thawed testicular tissues, which is particularly relevant to the cancer survivor paradigm. However, the fertilization potential of those sperm was not tested [144]. In the initial studies, the testicular tissue deteriorated with time. However, when tissues were maintained in a microfluidics device with continuous media flow to deliver nutrients and remove waste, testicular tissues could be maintained for up to 6 months with continuous production of testosterone and fertilization-competent sperm [91]. To make the microfluidics system more accessible, Komeya and colleagues [90] developed a pumpless microfluidics device that could maintain spermatogenesis in cultured seminiferous tubules for up to 3 months. Testicular tissue organ culture is a promising technology that now needs to be replicated in other laboratories and extended nonhuman primate and human tissues to set the stage for clinical translation.
11 Induced Pluripotent Stem Cell-Based Methods to Preserve and Restore Male Fertility
Several groups have now reported that it is possible to produce germ cells from pluripotent embryonic stem cells (ESCs) or induced pluripotent stem cells (iPSCs) [31, 34, 35, 57, 71, 78, 79, 120, 121, 131, 132, 143, 162, 181]. Hayashi and coworkers reported that it is possible to differentiate ESCs or iPSCs into epiblast-like cells (EpiLCs) that then give rise to primordial germ cell-like cells (PGCLCs) when cultured in the presence of BMP4 [57]. The resulting germ cells were transplanted into the seminiferous tubules of infertile recipient mice where they regenerated spermatogenesis and produced haploid gametes that were used to fertilize mouse oocytes by ICSI. The embryos were transferred to recipient females and gave rise to live offspring. However, some of the offspring developed tumors in the neck area and died prematurely, suggesting that further optimization of the culture and differentiation protocols will be required [57]. Two groups recently reported the differentiation of human pluripotent stem cells into putative hPGCLCs exhibiting gene expression patterns similar to bona fide human PGCs [71, 143]. Of course, functional validation by generation of progeny is not possible in studies with human cells.
An important implication of the iPSC to germ cell differentiation technology, if responsibly developed, is that it will no longer be necessary to preserve fertility before the initiation of gonadotoxic treatments. An adult survivor of a childhood cancer who desires to start his family and discovers that he is infertile can theoretically produce sperm and biological offspring from his own skin, blood, or other somatic cell type. This scenario applies not only to childhood cancer survivors, but all survivors who did not preserve semen or testicular tissue prior to gonadotoxic therapy. Nonhuman primate and human pluripotent stem cells have also been differentiated to the germ lineage, producing putative transplantable germ cells and even rare cells that appear to be haploid [31, 34,35,36, 78, 79, 120, 121, 132, 162, 181]. The challenge with the human studies is that it is not possible to test the spermatogenic potential or fertilization potential of putative germ cells, which are the gold standards in animal studies. Thus, the burden of proof required of human studies is much lower than animal studies. Spermatogenic lineage development and testicular anatomy in nonhuman primates is similar to humans [165], and this may serve as a platform for safety and feasibility studies in which putative germ cells can be tested by transplantation and the resulting gametes can be tested by fertilization [60], embryo transfer and production of live offspring. Perhaps one day, it will be possible to build a human testis in vitro or in vivo on a decellularized human testis scaffold, and this will provide the ultimate platform to test the spermatogenic potential of experimentally derived human germ cells.
12 Conclusions
Many centers worldwide are actively preserving testicular tissue or testicular cells for cancer patients in anticipation that those samples can be used in the future for reproductive purposes. Therefore, it is incumbent on the medical and research communities to responsibly develop the technologies that will allow patients to use their samples to achieve their family-building goals. This is important because cancer survivors report that fertility has a significant impact on their quality of life after cure. It seems reasonable to assume that similar quality of life issues are relevant to men who are infertile due to genetic (e.g., Klinefelter), surgical, age-related, accidental, or other causes. The first, best, and proven approach for fertility preservation in males is to freeze sperm that can be obtained in a semen sample or extracted from the testis. With IVF and IVF with ICSI, only a relatively small number of sperm are required to achieve fertilization and pregnancy. Unfortunately, sperm banking is not an option for all patients, including prepubertal boys who are not yet producing sperm.
There are several testicular cell- and tissue-based technologies in the research pipeline that may have application for patients who cannot preserve sperm. All of the technologies described in this chapter are dependent on stem cells (SSCs or iPSCs) with the potential to generate or regenerate autologous spermatogenesis. Spermatogonial stem cell transplantation, de novo testicular morphogenesis, testicular tissue organ culture, testicular tissue grafting/xenografting, and iPSC-derived germ cells have all produced spermatogenesis with sperm that are competent to fertilize oocytes and give rise to viable offspring in mice. Several of these methods have also been translated to larger animal models, including nonhuman primates, indicating a potential for application in the human fertility clinic.
The greatest challenge in the development of stem cell technologies for treatment of human male infertility is the lack of experimental tools for testing the spermatogenic and fertile potential of human cells. This means that human studies cannot be held to the same standard for burden of proof that is required of animal studies. While it is not realistic or possible to demonstrate the fertilization potential of human stem cell-derived gametes, it may be possible to develop systems to test the spermatogenic potential of human cells, such as de novo testicular morphogenesis or engraftment of a decellularized testis. Progress along these lines will provide powerful tools to ensure responsible development and validation of stem cell technologies before they are translated to the male fertility clinic.
References
Abdul Wahab AY, Md Isa ML, Ramli R. Spermatogonial stem cells protein identification in in vitro culture from non-obstructive azoospermia patient. Malay J Med Sci. 2016;23(3):40–8.
Adank MC, van Dorp W, Smit M, van Casteren NJ, Laven JSE, Pieters R, van den Heuvel-Eibrink MM. Electroejaculation as a method of fertility preservation in boys diagnosed with cancer: a single-center experience and review of the literature. Fertil Steril. 2014;102(1):199–205.e191. https://doi.org/10.1016/j.fertnstert.2014.03.038.
Agarwal A, Allamaneni SR. Artificial insemination. In: Falcone T, Hurd W, editors. Clinical reproductive medicine and surgery. Philadelphia: Elsevier; 2007. p. 539–48.
Akhondi MM, Mohazzab A, Jeddi-Tehrani M, Sadeghi MR, Eidi A, Khodadadi A, Piravar Z. Propagation of human germ stem cells in long-term culture. Iran J Reprod Med. 2013;11(7):551–8.
Aksglaede L, Wikstrom AM, Rajpert-De Meyts E, Dunkel L, Skakkebaek NE, Juul A. Natural history of seminiferous tubule degeneration in Klinefelter syndrome. Hum Reprod Update. 2006;12(1):39–48. https://doi.org/10.1093/humupd/dmi039.
Alves-Lopes JP, Söder O, Stukenborg J-B. Use of a three-layer gradient system of cells for rat testicular organoid generation. Nat Protoc. 2018;13:248. https://doi.org/10.1038/nprot.2017.140.
Andreas M, Wallner S, Ruetzler K, Wiedemann D, Ehrlich M, Heinze G, Binder T, Moritz A, Hiesmayr MJ, Kocher A, Laufer G. Comparable long-term results for porcine and pericardial prostheses after isolated aortic valve replacement. Eur J Cardiothorac Surg. 2014; https://doi.org/10.1093/ejcts/ezu466.
Arregui L, Rathi R, Megee SO, Honaramooz A, Gomendio M, Roldan ER, Dobrinski I. Xenografting of sheep testis tissue and isolated cells as a model for preservation of genetic material from endangered ungulates. Reproduction. 2008;136(1):85–93. https://doi.org/10.1530/REP-07-0433.
Baert Y, Braye A, Struijk RB, van Pelt AM, Goossens E. Cryopreservation of testicular tissue before long-term testicular cell culture does not alter in vitro cell dynamics. Fertil Steril. 2015a;104(5):1252.e1241–4. https://doi.org/10.1016/j.fertnstert.2015.07.1134.
Baert Y, De Kock J, Alves-Lopes JP, Söder O, Stukenborg J-B, Goossens E. Primary human testicular cells self-organize into organoids with testicular properties. Stem Cell Rep. 2017;8(1):30–8. https://doi.org/10.1016/j.stemcr.2016.11.012.
Baert Y, Onofre J, Van Saen D, Goossens E. Cryopreservation of human testicular tissue by isopropyl-controlled slow freezing. In: Alves MG, Oliveira PF, editors. Sertoli cells: methods and protocols. New York: Springer; 2018. p. 287–94. https://doi.org/10.1007/978-1-4939-7698-0_20.
Baert Y, Stukenborg JB, Landreh M, De Kock J, Jornvall H, Soder O, Goossens E. Derivation and characterization of a cytocompatible scaffold from human testis. Human Reprod (Oxford, England). 2015b;30(2):256–67.https://doi.org/10.1093/humrep/deu330.
Baert Y, Van Saen D, Haentjens P, In’t Veld P, Tournaye H, Goossens E. What is the best cryopreservation protocol for human testicular tissue banking? Hum Reprod. 2013; https://doi.org/10.1093/humrep/det100.
Bakircioglu ME, Ulug U, Erden HF, Tosun S, Bayram A, Ciray N, Bahceci M. Klinefelter syndrome: does it confer a bad prognosis in treatment of nonobstructive azoospermia? Fertil Steril. 2011;95(5):1696–9. https://doi.org/10.1016/j.fertnstert.2011.01.005.
Brannigan RE, Sandlow JI. Cryopreservation of sperm after chemotherapy. J Androl. 2008;29(3):e1–2. https://doi.org/10.2164/jandrol.107.004713.
Brinster CJ, Ryu BY, Avarbock MR, Karagenc L, Brinster RL, Orwig KE. Restoration of fertility by germ cell transplantation requires effective recipient preparation. Biol Reprod. 2003;69(2):412–20. https://doi.org/10.1095/biolreprod.103.016519.
Brinster RL, Avarbock MR. Germline transmission of donor haplotype following spermatogonial transplantation. Proc Natl Acad Sci U S A. 1994;91(24):11303–7.
Brinster RL, Zimmermann JW. Spermatogenesis following male germ-cell transplantation. Proc Natl Acad Sci U S A. 1994;91(24):11298–302.
Brook PF, Radford JA, Shalet SM, Joyce AD, Gosden RG. Isolation of germ cells from human testicular tissue for low temperature storage and autotransplantation. Fertil Steril. 2001;75(2):269–74.
Bucci LR, Meistrich ML. Effects of busulfan on murine spermatogenesis: cytotoxicity, sterility, sperm abnormalities, and dominant lethal mutations. Mutat Res. 1987;176(2):259–68.
Carson SA, Gentry WL, Smith AL, Buster JE. Feasibility of semen collection and cryopreservation during chemotherapy. Human Reprod (Oxford, England). 1991;6(7):992–4.
Chemaitilly W, Sklar CA. Endocrine complications in long-term survivors of childhood cancers. Endocr Relat Cancer. 2010;17(3):R141–59. https://doi.org/10.1677/ERC-10-0002.
Chen B, Wang YB, Zhang ZL, Xia WL, Wang HX, Xiang ZQ, Hu K, Han YF, Wang YX, Huang YR, Wang Z. Xeno-free culture of human spermatogonial stem cells supported by human embryonic stem cell-derived fibroblast-like cells. Asian J Androl. 2009;11(5):557–65. https://doi.org/10.1038/aja.2009.21.
Chikhovskaya JV, van Daalen SKM, Korver CM, Repping S, van Pelt AMM. Mesenchymal origin of multipotent human testis-derived stem cells in human testicular cell cultures. MHR: Basic Sci Reprod Med. 2014;20(2):155–67. https://doi.org/10.1093/molehr/gat076.
Cozzi E, White DJ. The generation of transgenic pigs as potential organ donors for humans. Nat Med. 1995;1(9):964–6.
Curaba M, Poels J, van Langendonckt A, Donnez J, Wyns C. Can prepubertal human testicular tissue be cryopreserved by vitrification? Fertil Steril. 2011;95(6):2123.e2129–12. https://doi.org/10.1016/j.fertnstert.2011.01.014.
de Rooij DG, Grootegoed JA. Spermatogonial stem cells. Curr Opin Cell Biol. 1998;10(6):694–701.
Dobrinski I, Avarbock MR, Brinster RL. Transplantation of germ cells from rabbits and dogs into mouse testes. Biol Reprod. 1999;61(5):1331–9.
Dobrinski I, Avarbock MR, Brinster RL. Germ cell transplantation from large domestic animals into mouse testes. Mol Reprod Dev. 2000;57(3):270–9. https://doi.org/10.1002/1098-2795(200011)57:3<270::AID-MRD9>3.0.CO;2-Z.
Dolmans MM, Marinescu C, Saussoy P, Van Langendonckt A, Amorim C, Donnez J. Reimplantation of cryopreserved ovarian tissue from patients with acute lymphoblastic leukemia is potentially unsafe. Blood. 2010;116(16):2908–14. https://doi.org/10.1182/blood-2010-01-265751.
Dominguez AA, Chiang HR, Sukhwani M, Orwig KE, Reijo Pera RA. Human germ cell formation in xenotransplants of induced pluripotent stem cells carrying X chromosome aneuploidies. Sci Rep. 2014;4:6432. https://doi.org/10.1038/srep06432.
Dovey SL, Valli H, Hermann BP, Sukhwani M, Donohue J, Castro CA, Chu T, Sanfilippo JS, Orwig KE. Eliminating malignant contamination from therapeutic human spermatogonial stem cells. J Clin Invest. 2013;123(4):1833–43. https://doi.org/10.1172/JCI65822.
Dufour JM, Rajotte RV, Korbutt GS. Development of an in vivo model to study testicular morphogenesis. J Androl. 2002;23(5):635–44.
Durruthy Durruthy J, Ramathal C, Sukhwani M, Fang F, Cui J, Orwig KE, Reijo Pera RA. Fate of induced pluripotent stem cells following transplantation to murine seminiferous tubules. Hum Mol Genet. 2014;23(12):3071–84. https://doi.org/10.1093/hmg/ddu012.
Easley CA, Phillips BT, McGuire MM, Barringer JM, Valli H, Hermann BP, Simerly CR, Rajkovic A, Miki T, Orwig KE, Schatten GP. Direct differentiation of human pluripotent stem cells into haploid spermatogenic cells. Cell Rep. 2012;2(3):440–6. https://doi.org/10.1016/j.celrep.2012.07.015.
Easley CA, Simerly CR, Schatten G. Stem cell therapeutic possibilities: future therapeutic options for male-factor and female-factor infertility? Reprod BioMed Online. 2013;27(1):75–80. https://doi.org/10.1016/j.rbmo.2013.03.003.
Ethics Committee of the American Society for Reproductive Medicine. Fertility preservation and reproduction in cancer patients. Fertil Steril. 2005;83(6):1622–8.
Practice Committee of American Society for Reproductive Medicine. Fertility preservation in patients undergoing gonadotoxic therapy or gonadectomy: a committee opinion. Fertil Steril. 2013;100(5):1214–23. https://doi.org/10.1016/j.fertnstert.2013.08.012.
Fraass BA, Kinsella TJ, Harrington FS, Glatstein E. Peripheral dose to the testes: the design and clinical use of a practical and effective gonadal shield. Int J Radiat Oncol Biol Phys. 1985;11(3):609–15.
Fujita K, Ohta H, Tsujimura A, Takao T, Miyagawa Y, Takada S, Matsumiya K, Wakayama T, Okuyama A. Transplantation of spermatogonial stem cells isolated from leukemic mice restores fertility without inducing leukemia. J Clin Investig. 2005;115(7):1855–61. https://doi.org/10.1172/Jci124189.
Fujita K, Tsujimura A, Miyagawa Y, Kiuchi H, Matsuoka Y, Takao T, Takada S, Nonomura N, Okuyama A. Isolation of germ cells from leukemia and lymphoma cells in a human in vitro model: potential clinical application for restoring human fertility after anticancer therapy. Cancer Res. 2006;66(23):11166–71. https://doi.org/10.1158/0008-5472.CAN-06-2326.
Garolla A, Selice R, Menegazzo M, Valente U, Zattoni F, Iafrate M, Prayer-Galetti T, Gardiman MP, Ferlin A, Di Nisio A, Foresta C. Novel insights on testicular volume and testosterone replacement therapy in Klinefelter patients undergoing testicular sperm extraction. A retrospective clinical study. Clin Endocrinol. 2018;88:711–8. https://doi.org/10.1111/cen.13572.
Gassei K, Schlatt S, Ehmcke J. De novo morphogenesis of seminiferous tubules from dissociated immature rat testicular cells in xenografts. J Androl. 2006;27(4):611–8. https://doi.org/10.2164/jandrol.05207.
Gat I, Maghen L, Filice M, Wyse B, Zohni K, Jarvi K, Lo KC, Gauthier Fisher A, Librach C. Optimal culture conditions are critical for efficient expansion of human testicular somatic and germ cells in vitro. Fertil Steril. 2017;107(3):595–605.e597. https://doi.org/10.1016/j.fertnstert.2016.12.028.
Gat I, Toren A, Hourvitz A, Raviv G, Band G, Baum M, Lerner-Geva L, Inbar R, Madgar I. Sperm preservation by electroejaculation in adolescent cancer patients. Pediatr Blood Cancer. 2014;61(2):286–90. https://doi.org/10.1002/pbc.24752.
Geens M, De Block G, Goossens E, Frederickx V, Van Steirteghem A, Tournaye H. Spermatogonial survival after grafting human testicular tissue to immunodeficient mice. Hum Reprod. 2006;21(2):390–6. https://doi.org/10.1093/humrep/dei412.
Geens M, Van de Velde H, De Block G, Goossens E, Van Steirteghem A, Tournaye H. The efficiency of magnetic-activated cell sorting and fluorescence-activated cell sorting in the decontamination of testicular cell suspensions in cancer patients. Hum Reprod. 2007;22(3):733–42.
Gilbert E, Adams A, Mehanna H, Harrison B, Hartshorne GM. Who should be offered sperm banking for fertility preservation? A survey of UK oncologists and haematologists. Ann Oncol. 2011;22(5):1209–14. https://doi.org/10.1093/annonc/mdq579.
Ginsberg JP. New advances in fertility preservation for pediatric cancer patients. Curr Opin Pediatr. 2011;23(1):9–13. https://doi.org/10.1097/MOP.0b013e3283420fb6.
Ginsberg JP, Carlson CA, Lin K, Hobbie WL, Wigo E, Wu X, Brinster RL, Kolon TF. An experimental protocol for fertility preservation in prepubertal boys recently diagnosed with cancer: a report of acceptability and safety. Human Reprod (Oxford, England). 2010;25(1):37–41. https://doi.org/10.1093/humrep/dep371.
Goharbakhsh L, Mohazzab A, Salehkhou S, Heidari M, Zarnani AH, Parivar K, Akhondi MM. Isolation and culture of human spermatogonial stem cells derived from testis biopsy. Avicenna J Med Biotechnol. 2013;5(1):54–61.
Goossens E, Geens M, De Block G, Tournaye H. Spermatogonial survival in long-term human prepubertal xenografts. Fertil Steril. 2008;90(5):2019–22. https://doi.org/10.1016/j.fertnstert.2007.09.044.
Goossens E, Van Saen D, Tournaye H. Spermatogonial stem cell preservation and transplantation: from research to clinic. Hum Reprod. 2013;28(4):897–907. https://doi.org/10.1093/humrep/det039.
Green DM, Kawashima T, Stovall M, Leisenring W, Sklar CA, Mertens AC, Donaldson SS, Byrne J, Robison LL. Fertility of male survivors of childhood cancer: a report from the Childhood Cancer Survivor Study. J Clin Oncol. 2010;28(2):332–9. https://doi.org/10.1200/JCO.2009.24.9037.
Guo Y, Liu L, Sun M, Hai Y, Li Z, He Z. Expansion and long-term culture of human spermatogonial stem cells via the activation of SMAD3 and AKT pathways. Exp Biol Med (Maywood). 2015;240(8):1112–22. https://doi.org/10.1177/1535370215590822.
Hamra FK, Chapman KM, Nguyen DM, Williams-Stephens AA, Hammer RE, Garbers DL. Self renewal, expansion, and transfection of rat spermatogonial stem cells in culture. Proc Natl Acad Sci U S A. 2005;102(48):17430–5. https://doi.org/10.1073/pnas.0508780102.
Hayashi K, Ohta H, Kurimoto K, Aramaki S, Saitou M. Reconstitution of the mouse germ cell specification pathway in culture by pluripotent stem cells. Cell. 2011;146(4):519–32. https://doi.org/10.1016/j.cell.2011.06.052.
He Z, Kokkinaki M, Jiang J, Dobrinski I, Dym M. Isolation, characterization, and culture of human spermatogonia. Biol Reprod. 2010;82(2):363–72. https://doi.org/10.1095/biolreprod.109.078550.
Hermann BP, Sukhwani M, Salati J, Sheng Y, Chu T, Orwig KE. Separating spermatogonia from cancer cells in contaminated prepubertal primate testis cell suspensions. Hum Reprod. 2011;26(12):3222–31. https://doi.org/10.1093/humrep/der343.
Hermann BP, Sukhwani M, Winkler F, Pascarella JN, Peters KA, Sheng Y, Valli H, Rodriguez M, Ezzelarab M, Dargo G, Peterson K, Masterson K, Ramsey C, Ward T, Lienesch M, Volk A, Cooper DK, Thomson AW, Kiss JE, Penedo MC, Schatten GP, Mitalipov S, Orwig KE. Spermatogonial stem cell transplantation into rhesus testes regenerates spermatogenesis producing functional sperm. Cell Stem Cell. 2012;11(5):715–26. https://doi.org/10.1016/j.stem.2012.07.017.
Herrid M, Olejnik J, Jackson M, Suchowerska N, Stockwell S, Davey R, Hutton K, Hope S, Hill JR. Irradiation enhances the efficiency of testicular germ cell transplantation in sheep. Biol Reprod. 2009;81(5):898–905. https://doi.org/10.1095/biolreprod.109.078279.
Honaramooz A, Behboodi E, Megee SO, Overton SA, Galantino-Homer H, Echelard Y, Dobrinski I. Fertility and germline transmission of donor haplotype following germ cell transplantation in immunocompetent goats. Biol Reprod. 2003;69(4):1260–4. https://doi.org/10.1095/biolreprod.103.018788.
Honaramooz A, Li MW, Penedo MCT, Meyers S, Dobrinski I. Accelerated maturation of primate testis by xenografting into mice. Biol Reprod. 2004;70(5):1500–3. https://doi.org/10.1095/biolreprod.103.025536.
Honaramooz A, Megee SO, Rathi R, Dobrinski I. Building a testis: formation of functional testis tissue after transplantation of isolated porcine (Sus scrofa) testis cells. Biol Reprod. 2007;76(1):43–7. https://doi.org/10.1095/biolreprod.106.054999.
Honaramooz A, Snedaker A, Boiani M, Scholer H, Dobrinski I, Schlatt S. Sperm from neonatal mammalian testes grafted in mice. Nature. 2002;418(6899):778–81. https://doi.org/10.1038/nature00918.
Hou M, Andersson M, Zheng C, Sundblad A, Soder O, Jahnukainen K. Decontamination of leukemic cells and enrichment of germ cells from testicular samples from rats with Roser’s T-cell leukemia by flow cytometric sorting. Reproduction. 2007;134(6):767–79. https://doi.org/10.1530/REP-07-0240.
Howell SJ, Shalet SM. Spermatogenesis after cancer treatment: damage and recovery. JNCI Monogr. 2005;2005(34):12–7. https://doi.org/10.1093/jncimonographs/lgi003.
Howlader N, Noone AM, Krapcho M, Miller D, Bishop K, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA. SEER cancer statistics review, 1975–2014. Bethesda, MD: National Cancer Institute; 2017.. https://seer.cancer.gov/csr/1975_2014/. Accessed 2/19/2018.
Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Waldron W, Altekruse SF, Kosary CL, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Chen HS, Feuer EJ, Cronin KA, Edwards BK. SEER cancer statistic review 1975–2008. Bethesda, MD: National Cancer Institute; 2010.. http://seer.cancer.gov/csr/1975_2008/.
Hsiao W, Stahl PJ, Osterberg EC, Nejat E, Palermo GD, Rosenwaks Z, Schlegel PN. Successful treatment of postchemotherapy azoospermia with microsurgical testicular sperm extraction: the weill cornell experience. J Clin Oncol. 2011;29(12):1607–11. https://doi.org/10.1200/jco.2010.33.7808.
Irie N, Weinberger L, Tang WW, Kobayashi T, Viukov S, Manor YS, Dietmann S, Hanna JH, Surani MA. SOX17 is a critical specifier of human primordial germ cell fate. Cell. 2015;160(1–2):253–68. https://doi.org/10.1016/j.cell.2014.12.013.
Izadyar F, Den Ouden K, Stout TA, Stout J, Coret J, Lankveld DP, Spoormakers TJ, Colenbrander B, Oldenbroek JK, Van der Ploeg KD, Woelders H, Kal HB, De Rooij DG. Autologous and homologous transplantation of bovine spermatogonial stem cells. Reproduction. 2003;126(6):765–74.
Jahnukainen K, Ehmcke J, Quader MA, Saiful Huq M, Epperly MW, Hergenrother S, Nurmio M, Schlatt S. Testicular recovery after irradiation differs in prepubertal and pubertal non-human primates, and can be enhanced by autologous germ cell transplantation. Human Reprod (Oxford, England). 2011;26(8):1945–54. https://doi.org/10.1093/humrep/der160.
Jahnukainen K, Hou M, Petersen C, Setchell B, Soder O. Intratesticular transplantation of testicular cells from leukemic rats causes transmission of leukemia. Cancer Res. 2001;61(2):706–10.
Jamieson SW, Madani MM. The choice of valve protheses*. J Am Coll Cardiol. 2004;44(2):389–90. https://doi.org/10.1016/j.jacc.2004.04.021.
Kanatsu-Shinohara M, Muneto T, Lee J, Takenaka M, Chuma S, Nakatsuji N, Horiuchi T, Shinohara T. Long-term culture of male germline stem cells from hamster testes. Biol Reprod. 2008;78(4):611–7. https://doi.org/10.1095/biolreprod.107.065615.
Kanatsu-Shinohara M, Ogonuki N, Inoue K, Miki H, Ogura A, Toyokuni S, Shinohara T. Long-term proliferation in culture and germline transmission of mouse male germline stem cells. Biol Reprod. 2003;69(2):612–6. https://doi.org/10.1095/biolreprod.103.017012.
Kee K, Angeles VT, Flores M, Nguyen HN, Reijo Pera RA. Human DAZL, DAZ and BOULE genes modulate primordial germ-cell and haploid gamete formation. Nature. 2009;462(7270):222–5. https://doi.org/10.1038/nature08562.
Kee K, Gonsalves JM, Clark AT, Pera RA. Bone morphogenetic proteins induce germ cell differentiation from human embryonic stem cells. Stem Cells Dev. 2006;15(6):831–7. https://doi.org/10.1089/scd.2006.15.831.
Kenney LB, Cohen LE, Shnorhavorian M, Metzger ML, Lockart B, Hijiya N, Duffey-Lind E, Constine L, Green D, Meacham L. Male reproductive health after childhood, adolescent, and young adult cancers: a report from the Children’s Oncology Group. J Clin Oncol. 2012;30(27):3408–16. https://doi.org/10.1200/jco.2011.38.6938.
Keros V, Hultenby K, Borgstrom B, Fridstrom M, Jahnukainen K, Hovatta O. Methods of cryopreservation of testicular tissue with viable spermatogonia in pre-pubertal boys undergoing gonadotoxic cancer treatment. Human Reprod (Oxford, England). 2007;22(5):1384–95. https://doi.org/10.1093/humrep/del508.
Keros V, Rosenlund B, Hultenby K, Aghajanova L, Levkov L, Hovatta O. Optimizing cryopreservation of human testicular tissue: comparison of protocols with glycerol, propanediol and dimethylsulphoxide as cryoprotectants. Hum Reprod. 2005;20(6):1676–87. https://doi.org/10.1093/humrep/deh797.
Kim TH, Hargreaves HK, Brynes RK, Hawkins HK, Lui VK, Woodard J, Ragab AH. Pretreatment testicular biopsy in childhood acute lymphocytic leukaemia. Lancet. 1981;2(8248):657–8.
Kim Y, Turner D, Nelson J, Dobrinski I, McEntee M, Travis AJ. Production of donor-derived sperm after spermatogonial stem cell transplantation in the dog. Reproduction. 2008;136(6):823–31. https://doi.org/10.1530/REP-08-0226.
Kimsa MC, Strzalka-Mrozik B, Kimsa MW, Gola J, Nicholson P, Lopata K, Mazurek U. Porcine endogenous retroviruses in xenotransplantation – molecular aspects. Viruses. 2014;6(5):2062–83. https://doi.org/10.3390/v6052062.
Kita K, Watanabe T, Ohsaka K, Hayashi H, Kubota Y, Nagashima Y, Aoki I, Taniguchi H, Noce T, Inoue K, Miki H, Ogonuki N, Tanaka H, Ogura A, Ogawa T. Production of functional spermatids from mouse germline stem cells in ectopically reconstituted seminiferous tubules. Biol Reprod. 2007;76(2):211–7. https://doi.org/10.1095/biolreprod.106.056895.
Klosky JL, Simmons JL, Russell KM, Foster RH, Sabbatini GM, Canavera KE, Hodges JR, Schover LR, McDermott MJ. Fertility as a priority among at-risk adolescent males newly diagnosed with cancer and their parents. Support Care Cancer. 2015;23(2):333–41. https://doi.org/10.1007/s00520-014-2366-1.
Koga M, Tsujimura A, Takeyama M, Kiuchi H, Takao T, Miyagawa Y, Takada S, Matsumiya K, Fujioka H, Okamoto Y, Nonomura N, Okuyama A. Clinical comparison of successful and failed microdissection testicular sperm extraction in patients with nonmosaic Klinefelter syndrome. Urology. 2007;70(2):341–5. https://doi.org/10.1016/j.urology.2007.03.056.
Kokkinaki M, Djourabtchi A, Golestaneh N. Long-term culture of human SSEA-4 positive spermatogonial stem cells (SSCs). J Stem Cell Res Ther. 2011;S2:003. https://doi.org/10.4172/2157-7633.S2-003.
Komeya M, Hayashi K, Nakamura H, Yamanaka H, Sanjo H, Kojima K, Sato T, Yao M, Kimura H, Fujii T, Ogawa T. Pumpless microfluidic system driven by hydrostatic pressure induces and maintains mouse spermatogenesis in vitro. Sci Rep. 2017;7(1):15459. https://doi.org/10.1038/s41598-017-15799-3.
Komeya M, Kimura H, Nakamura H, Yokonishi T, Sato T, Kojima K, Hayashi K, Katagiri K, Yamanaka H, Sanjo H, Yao M, Kamimura S, Inoue K, Ogonuki N, Ogura A, Fujii T, Ogawa T. Long-term ex vivo maintenance of testis tissues producing fertile sperm in a microfluidic device. Sci Rep. 2016;6:21472. https://doi.org/10.1038/srep21472.. http://www.nature.com/articles/srep21472 - supplementary-information.
Kubota H, Avarbock MR, Brinster RL. Growth factors essential for self-renewal and expansion of mouse spermatogonial stem cells. Proc Natl Acad Sci U S A. 2004;101(47):16489–94. https://doi.org/10.1073/pnas.0407063101.
Kvist K, Thorup J, Byskov AG, Hoyer PE, Mollgard K, Yding Andersen C. Cryopreservation of intact testicular tissue from boys with cryptorchidism. Human Reprod (Oxford, England). 2006;21(2):484–91. https://doi.org/10.1093/humrep/dei331.
Lambertini M, Del Mastro L, Pescio MC, Andersen CY, Azim HA, Peccatori FA, Costa M, Revelli A, Salvagno F, Gennari A, Ubaldi FM, La Sala GB, De Stefano C, Wallace WH, Partridge AH, Anserini P. Cancer and fertility preservation: international recommendations from an expert meeting. BMC Med. 2016;14(1):1. https://doi.org/10.1186/s12916-015-0545-7.
Lee JH, Kim HJ, Kim H, Lee SJ, Gye MC. In vitro spermatogenesis by three-dimensional culture of rat testicular cells in collagen gel matrix. Biomaterials. 2006a;27(14):2845–53. https://doi.org/10.1016/j.biomaterials.2005.12.028.
Lee SJ, Schover LR, Partridge AH, Patrizio P, Wallace WH, Hagerty K, Beck LN, Brennan LV, Oktay K. American Society of Clinical Oncology recommendations on fertility preservation in cancer patients. J Clin Oncol. 2006b;24(18):2917–31. https://doi.org/10.1200/JCO.2006.06.5888.
Levine J, Canada A, Stern CJ. Fertility preservation in adolescents and young adults with cancer. J Clin Oncol. 2010;28(32):4831–41. https://doi.org/10.1200/JCO.2009.22.8312.
Lim JJ, Sung SY, Kim HJ, Song SH, Hong JY, Yoon TK, Kim JK, Kim KS, Lee DR. Long-term proliferation and characterization of human spermatogonial stem cells obtained from obstructive and non-obstructive azoospermia under exogenous feeder-free culture conditions. Cell Prolif. 2010;43(4):405–17. https://doi.org/10.1111/j.1365-2184.2010.00691.x.
Liu S, Tang Z, Xiong T, Tang W. Isolation and characterization of human spermatogonial stem cells. Reprod Biol Endocrinol: RB&E. 2011;9:141. https://doi.org/10.1186/1477-7827-9-141.
Loren AW, Mangu PB, Beck LN, Brennan L, Magdalinski AJ, Partridge AH, Quinn G, Wallace WH, Oktay K, American Society of Clinical Oncology. Fertility preservation for patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Clin Oncol. 2013;31(19):2500–10. https://doi.org/10.1200/JCO.2013.49.2678.
Luetjens CM, Stukenborg J-B, Nieschlag E, Simoni M, Wistuba J. Complete spermatogenesis in orthotopic but not in ectopic transplants of autologously grafted marmoset testicular tissue. Endocrinology. 2008;149(4):1736–47. https://doi.org/10.1210/en.2007-1325.
Medrano JV, Rombaut C, Simon C, Pellicer A, Goossens E. Human spermatogonial stem cells display limited proliferation in vitro under mouse spermatogonial stem cell culture conditions. Fertil Steril. 2016; https://doi.org/10.1016/j.fertnstert.2016.07.1065.
Mehta A, Paduch DA, Schlegel PN. Successful testicular sperm retrieval in adolescents with Klinefelter syndrome treated with at least 1 year of topical testosterone and aromatase inhibitor. Fertil Steril. 2013;100(4):e27. https://doi.org/10.1016/j.fertnstert.2013.08.001.
Meistrich ML. Potential genetic risks of using semen collected during chemotherapy. Human Reprod (Oxford, England). 1993;8(1):8–10.
Meistrich ML. Male gonadal toxicity. Pediatr Blood Cancer. 2009;53(2):261–6. https://doi.org/10.1002/pbc.22004.
Meistrich ML, Vassilopoulou-Sellin R, Lipshultz LI. Adverse effects of treatment: gonadal dysfunction. In: DeVita VT, Hellman S, Rosenberg SA, editors. Principles and practice of oncology. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2004. p. 2560–74.
Meistrich ML, Wilson G, Brown BW, da Cunha MF, Lipshultz LI. Impact of cyclophosphamide on long-term reduction in sperm count in men treated with combination chemotherapy for Ewing and soft tissue sarcomas. Cancer. 1992;70(11):2703–12.
Mikkola M, Sironen A, Kopp C, Taponen J, Sukura A, Vilkki J, Katila T, Andersson M. Transplantation of normal boar testicular cells resulted in complete focal spermatogenesis in a boar affected by the immotile short-tail sperm defect. Reprod Domest Anim. 2006;41(2):124–8. https://doi.org/10.1111/j.1439-0531.2006.00651.x.
Mirzapour T, Movahedin M, Tengku Ibrahim TA, Koruji M, Haron AW, Nowroozi MR, Rafieian SH. Effects of basic fibroblast growth factor and leukaemia inhibitory factor on proliferation and short-term culture of human spermatogonial stem cells. Andrologia. 2012;44:41–55. https://doi.org/10.1111/j.1439-0272.2010.01135.x.
Nagano M, Brinster CJ, Orwig KE, Ryu BY, Avarbock MR, Brinster RL. Transgenic mice produced by retroviral transduction of male germ-line stem cells. Proc Natl Acad Sci U S A. 2001;98(23):13090–5. https://doi.org/10.1073/pnas.231473498.
Nowroozi MR, Ahmadi H, Rafiian S, Mirzapour T, Movahedin M. In vitro colonization of human spermatogonia stem cells: effect of patient’s clinical characteristics and testicular histologic findings. Urology. 2011;78(5):1075–81. https://doi.org/10.1016/j.urology.2011.06.035.
Oates RD. Sperm retrieval in adolescents with Klinefelter syndrome. Fertil Steril. 2013;100(4):943–4. https://doi.org/10.1016/j.fertnstert.2013.07.003.
Ogawa T, Dobrinski I, Avarbock MR, Brinster RL. Transplantation of male germ line stem cells restores fertility in infertile mice. Nat Med. 2000;6(1):29–34. https://doi.org/10.1038/71496.
Okada H, Goda K, Yamamoto Y, Sofikitis N, Miyagawa I, Mio Y, Koshida M, Horie S. Age as a limiting factor for successful sperm retrieval in patients with nonmosaic Klinefelter’s syndrome. Fertil Steril. 2005;84(6):1662–4. https://doi.org/10.1016/j.fertnstert.2005.05.053.
Onofre J, Baert Y, Faes K, Goossens E. Cryopreservation of testicular tissue or testicular cell suspensions: a pivotal step in fertility preservation. Hum Reprod Update. 2016;22(6):744–61. https://doi.org/10.1093/humupd/dmw029.
Orwig KE, Shaw PH, Sanfilippo JS, Kauma SW, Nayak S, Cannon GM. (http://www.mwrif.org/220) Fertility preservation program of Magee-Womens Hospital in Pittsburgh. http://www.mwrif.org/220
Pacchiarotti J, Ramos T, Howerton K, Greilach S, Zaragoza K, Olmstead M, Izadyar F. Developing a clinical-grade cryopreservation protocol for human testicular tissue and cells. Biomed Res Int. 2013;2013:10. https://doi.org/10.1155/2013/930962.
Palermo G, Joris H, Devroey P, Van Steirteghem AC. Pregnancies after intracytoplasmic injection of single spermatozoon into an oocyte. Lancet. 1992;340(8810):17–8.
Paniagua R, Nistal M. Morphological and histometric study of human spermatogonia from birth to the onset of puberty. J Anat. 1984;139(Pt 3):535–52.
Panula S, Medrano JV, Kee K, Bergstrom R, Nguyen HN, Byers B, Wilson KD, Wu JC, Simon C, Hovatta O, Reijo Pera RA. Human germ cell differentiation from fetal- and adult-derived induced pluripotent stem cells. Hum Mol Genet. 2011;20(4):752–62. https://doi.org/10.1093/hmg/ddq520.
Park TS, Galic Z, Conway AE, Lindgren A, van Handel BJ, Magnusson M, Richter L, Teitell MA, Mikkola HK, Lowry WE, Plath K, Clark AT. Derivation of primordial germ cells from human embryonic and induced pluripotent stem cells is significantly improved by coculture with human fetal gonadal cells. Stem Cells. 2009;27(4):783–95. https://doi.org/10.1002/stem.13.
Pendergraft SS, Sadri-Ardekani H, Atala A, Bishop CE. Three-dimensional testicular organoid: a novel tool for the study of human spermatogenesis and gonadotoxicity in vitro†. Biol Reprod. 2017;96(3):720–32. https://doi.org/10.1095/biolreprod.116.143446.
Phillips BT, Gassei K, Orwig KE. Spermatogonial stem cell regulation and spermatogenesis. Philos Trans R Soc Lond Ser B Biol Sci. 2010;365(1546):1663–78. https://doi.org/10.1098/rstb.2010.0026.
Picton HM, Wyns C, Anderson RA, Goossens E, Jahnukainen K, Kliesch S, Mitchell RT, Pennings G, Rives N, Tournaye H, van Pelt AM, Eichenlaub-Ritter U, Schlatt S. A European perspective on testicular tissue cryopreservation for fertility preservation in prepubertal and adolescent boysdagger. Human Reprod (Oxford, England). 2015;30(11):2463–75. https://doi.org/10.1093/humrep/dev190.
Piravar Z, Jeddi-Tehrani M, Sadeghi MR, Mohazzab A, Eidi A, Akhondi MM. In vitro culture of human testicular stem cells on feeder-free condition. J Reprod Infertility. 2013;14(1):17–22.
Plotton I, Giscard d’Estaing S, Cuzin B, Brosse A, Benchaib M, Lornage J, Ecochard R, Dijoud F, Lejeune H. Preliminary results of a prospective study of testicular sperm extraction in young versus adult patients with nonmosaic 47,XXY Klinefelter syndrome. J Clin Endocrinol Metab. 2015;100(3):961–7. https://doi.org/10.1210/jc.2014-3083.
Poels J, Van Langendonckt A, Many MC, Wese FX, Wyns C. Vitrification preserves proliferation capacity in human spermatogonia. Human Reprod (Oxford, England). 2013;28(3):578–89. https://doi.org/10.1093/humrep/des455.
Radford J. Restoration of fertility after treatment for cancer. Horm Res. 2003;59(Suppl 1):21–3. https://doi.org/10.1159/000067840.
Radford JA, Shalet SM, Lieberman BA. Fertility after treatment for cancer. BMJ. 1999;319(7215):935–6.
Ramasamy R, Ricci JA, Palermo GD, Gosden LV, Rosenwaks Z, Schlegel PN. Successful fertility treatment for Klinefelter’s syndrome. J Urol. 2009;182(3):1108–13. https://doi.org/10.1016/j.juro.2009.05.019.
Ramathal C, Angulo B, Sukhwani M, Cui J, Durruthy-Durruthy J, Fang F, Schanes P, Turek PJ, Orwig KE, Reijo Pera R. DDX3Y gene rescue of a Y chromosome AZFa deletion restores germ cell formation and transcriptional programs. Sci Rep. 2015;5:15041. https://doi.org/10.1038/srep15041.
Ramathal C, Durruthy-Durruthy J, Sukhwani M, Arakaki JE, Turek PJ, Orwig KE, Reijo Pera RA. Fate of iPSCs derived from azoospermic and fertile men following xenotransplantation to murine seminiferous tubules. Cell Rep. 2014;7(4):1284–97. https://doi.org/10.1016/j.celrep.2014.03.067.
Richardson TE, Chapman KM, Tenenhaus Dann C, Hammer RE, Hamra FK. Sterile testis complementation with spermatogonial lines restores fertility to DAZL-deficient rats and maximizes donor germline transmission. PloS One. 2009;4(7):e6308. https://doi.org/10.1371/journal.pone.0006308.
Rives N, Milazzo JP, Perdrix A, Castanet M, Joly-Helas G, Sibert L, Bironneau A, Way A, Mace B. The feasibility of fertility preservation in adolescents with Klinefelter syndrome. Human Reprod (Oxford, England). 2013;28(6):1468–79. https://doi.org/10.1093/humrep/det084.
Rosendahl M, Andersen MT, Ralfkiaer E, Kjeldsen L, Andersen MK, Andersen CY. Evidence of residual disease in cryopreserved ovarian cortex from female patients with leukemia. Fertil Steril. 2010;94(6):2186–90. https://doi.org/10.1016/j.fertnstert.2009.11.032.
Ryu BY, Kubota H, Avarbock MR, Brinster RL. Conservation of spermatogonial stem cell self-renewal signaling between mouse and rat. Proc Natl Acad Sci U S A. 2005;102(40):14302–7. https://doi.org/10.1073/pnas.0506970102.
Ryu BY, Orwig KE, Avarbock MR, Brinster RL. Stem cell and niche development in the postnatal rat testis. Dev Biol. 2003;263(2):253–63.
Sa R, Cremades N, Malheiro I, Sousa M. Cryopreservation of human testicular diploid germ cell suspensions. Andrologia. 2012;44(6):366–72. https://doi.org/10.1111/j.1439-0272.2012.01290.x.
Sadri-Ardekani H, Akhondi MA, van der Veen F, Repping S, van Pelt AM. In vitro propagation of human prepubertal spermatogonial stem cells. JAMA J Am Med Assoc. 2011;305(23):2416–8. https://doi.org/10.1001/jama.2011.791.
Sadri-Ardekani H, Akhondi MM, Vossough P, Maleki H, Sedighnejad S, Kamali K, Ghorbani B, van Wely M, van der Veen F, Repping S. Parental attitudes toward fertility preservation in boys with cancer: context of different risk levels of infertility and success rates of fertility restoration. Fertil Steril. 2013;99(3):796–802. https://doi.org/10.1016/j.fertnstert.2012.11.030.
Sadri-Ardekani H, Mizrak SC, van Daalen SK, Korver CM, Roepers-Gajadien HL, Koruji M, Hovingh S, de Reijke TM, de la Rosette JJ, van der Veen F, de Rooij DG, Repping S, van Pelt AM. Propagation of human spermatogonial stem cells in vitro. JAMA. 2009;302(19):2127–34. https://doi.org/10.1001/jama.2009.1689.
Sanghvi PR, Kaurin DG, McDonald TL, Holland JM. Testicular shielding in low-dose total body irradiation. Bone Marrow Transplant. 2007;39(4):247–8. https://doi.org/10.1038/sj.bmt.1705574.
Sasaki K, Yokobayashi S, Nakamura T, Okamoto I, Yabuta Y, Kurimoto K, Ohta H, Moritoki Y, Iwatani C, Tsuchiya H, Nakamura S, Sekiguchi K, Sakuma T, Yamamoto T, Mori T, Woltjen K, Nakagawa M, Yamamoto T, Takahashi K, Yamanaka S, Saitou M. Robust in vitro induction of human germ cell fate from pluripotent stem cells. Cell Stem Cell. 2015;17(2):178–94. https://doi.org/10.1016/j.stem.2015.06.014.
Sato T, Katagiri K, Gohbara A, Inoue K, Ogonuki N, Ogura A, Kubota Y, Ogawa T. In vitro production of functional sperm in cultured neonatal mouse testes. Nature. 2011;471(7339):504–7. https://doi.org/10.1038/nature09850.
Sato T, Katagiri K, Kubota Y, Ogawa T. In vitro sperm production from mouse spermatogonial stem cell lines using an organ culture method. Nat Protoc. 2013;8(11):2098–104. https://doi.org/10.1038/nprot.2013.138.. http://www.nature.com/nprot/journal/v8/n11/abs/nprot.2013.138.html - supplementary-information.
Sato Y, Nozawa S, Yoshiike M, Arai M, Sasaki C, Iwamoto T. Xenografting of testicular tissue from an infant human donor results in accelerated testicular maturation. Hum Reprod. 2010;25(5):1113–22. https://doi.org/10.1093/humrep/deq001.
Schiff JD, Palermo GD, Veeck LL, Goldstein M, Rosenwaks Z, Schlegel PN. Success of testicular sperm extraction [corrected] and intracytoplasmic sperm injection in men with Klinefelter syndrome. J Clin Endocrinol Metab. 2005;90(11):6263–7. https://doi.org/10.1210/jc.2004-2322.
Schlatt S, Foppiani L, Rolf C, Weinbauer GF, Nieschlag E. Germ cell transplantation into X-irradiated monkey testes. Human Reprod (Oxford, England). 2002;17(1):55–62.
Schlatt S, Honaramooz A, Boiani M, Scholer HR, Dobrinski I. Progeny from sperm obtained after ectopic grafting of neonatal mouse testes. Biol Reprod. 2003;68(6):2331–5. https://doi.org/10.1095/biolreprod.102.014894.
Schlatt S, Honaramooz A, Ehmcke J, Goebell PJ, Rubben H, Dhir R, Dobrinski I, Patrizio P. Limited survival of adult human testicular tissue as ectopic xenograft. Hum Reprod. 2006;21(2):384–9. https://doi.org/10.1093/humrep/dei352.
Schmiegelow ML, Sommer P, Carlsen E, Sønksen JOR, Schmiegelow K, Muller JR. Penile vibratory stimulation and electroejaculation before anticancer therapy in two pubertal boys. J Pediatr Hematol Oncol. 1998;20(5):429–30.
Schover LR. Patient attitudes toward fertility preservation. Pediatr Blood Cancer. 2009;53(2):281–4. https://doi.org/10.1002/pbc.22001.
Schover LR, Brey K, Lichtin A, Lipshultz LI, Jeha S. Knowledge and experience regarding cancer, infertility, and sperm banking in younger male survivors. J Clin Oncol. 2002a;20(7):1880–9. https://doi.org/10.1200/Jco.2002.07.175.
Schover LR, Brey K, Lichtin A, Lipshultz LI, Jeha S. Knowledge and experience regarding cancer, infertility, and sperm banking in younger male survivors. J Clin Oncol. 2002b;20(7):1880–9.
Schover LR, Brey K, Lichtin A, Lipshultz LI, Jeha S. Oncologists’ attitudes and practices regarding banking sperm before cancer treatment. J Clin Oncol. 2002c;20(7):1890–7.
Sharpe RM. Regulation of spermatogenesis. In: Knobil E, Neill JD, editors. The physiology of reproduction. New York: Raven Press, Ltd.; 1994. p. 1363–434.
Shinohara T, Orwig KE, Avarbock MR, Brinster RL. Remodeling of the postnatal mouse testis is accompanied by dramatic changes in stem cell number and niche accessibility. Proc Natl Acad Sci U S A. 2001;98(11):6186–91.
Smith JF, Yango P, Altman E, Choudhry S, Poelzl A, Zamah AM, Rosen M, Klatsky PC, Tran ND. Testicular niche required for human spermatogonial stem cell expansion. Stem Cells Transl Med. 2014;3(9):1043–54. https://doi.org/10.5966/sctm.2014-0045.
Steptoe PC, Edwards RG. Birth after the reimplantation of a human embryo. Lancet. 1978;2(8085):366.
Stukenborg JB, Schlatt S, Simoni M, Yeung CH, Elhija MA, Luetjens CM, Huleihel M, Wistuba J. New horizons for in vitro spermatogenesis? An update on novel three-dimensional culture systems as tools for meiotic and post-meiotic differentiation of testicular germ cells. Mol Hum Reprod. 2009;15(9):521–9. https://doi.org/10.1093/molehr/gap052.
Tegelenbosch RA, de Rooij DG. A quantitative study of spermatogonial multiplication and stem cell renewal in the C3H/101 F1 hybrid mouse. Mutat Res. 1993;290(2):193–200.
Teramura T, Takehara T, Kawata N, Fujinami N, Mitani T, Takenoshita M, Matsumoto K, Saeki K, Iritani A, Sagawa N, Hosoi Y. Primate embryonic stem cells proceed to early gametogenesis in vitro. Cloning Stem Cells. 2007;9(2):144–56. https://doi.org/10.1089/clo.2006.0070.
Unni S, Kasiviswanathan S, D'Souza S, Khavale S, Mukherjee S, Patwardhan S, Bhartiya D. Efficient cryopreservation of testicular tissue: effect of age, sample state, and concentration of cryoprotectant. Fertil Steril. 2012;97(1):200–208 e201. https://doi.org/10.1016/j.fertnstert.2011.10.018.
Valli H, Gassei K, Orwig KE. Stem cell therapies for male infertility: where are we now and where are we going? In: Carrell DT, Schlegel PN, Racowsky C, Gianaroli L, editors. Biennial review of infertility, vol. 4. Cham: Springer International Publishing; 2015a. p. 17–39. https://doi.org/10.1007/978-3-319-17849-3_3.
Valli H, Phillips BT, Gassei K, Nagano MC, Orwig KE. Spermatogonial stem cells and spermatogenesis. In: Plant TM, Zeleznik AJ, editors. Knobil and Neill’s physiology of reproduction, vol. 1. 4th ed. San Diego: Elsevier; 2015b. p. 595–635.
Valli H, Phillips BT, Shetty G, Byrne JA, Clark AT, Meistrich ML, Orwig KE. Germline stem cells: toward the regeneration of spermatogenesis. Fertil Steril. 2014a;101(1):3–13. https://doi.org/10.1016/j.fertnstert.2013.10.052.
Valli H, Sukhwani M, Dovey SL, Peters KA, Donohue J, Castro CA, Chu T, Marshall GR, Orwig KE. Fluorescence- and magnetic-activated cell sorting strategies to isolate and enrich human spermatogonial stem cells. Fertil Steril. 2014b;102(2):566–80. https://doi.org/10.1016/j.fertnstert.2014.04.036.
Van Saen D, Goossens E, Bourgain C, Ferster A, Tournaye H. Meiotic activity in orthotopic xenografts derived from human postpubertal testicular tissue. Hum Reprod. 2011;26(2):282–93. https://doi.org/10.1093/humrep/deq321.
Verit FF, Verit A. Klinefelter syndrome: an argument for early aggressive hormonal and fertility management. Fertil Steril. 2012;98(5):e25; author reply e26. https://doi.org/10.1016/j.fertnstert.2012.08.031.
von Kopylow K, Schulze W, Salzbrunn A, Schaks M, Schäfer E, Roth B, Schlatt S, Spiess A-N. Dynamics, ultrastructure and gene expression of human in vitro organized testis cells from testicular sperm extraction biopsies. MHR: Basic Sci Reprod Med. 2018;24(3):123–34. https://doi.org/10.1093/molehr/gax070.
Wallace WH, Anderson RA, Irvine DS. Fertility preservation for young patients with cancer: who is at risk and what can be offered? Lancet Oncol. 2005;6(4):209–18. https://doi.org/10.1016/S1470-2045(05)70092-9.
Wasilewski-Masker K, Seidel KD, Leisenring W, Mertens AC, Shnorhavorian M, Ritenour CW, Stovall M, Green DM, Sklar CA, Armstrong GT, Robison LL, Meacham LR. Male infertility in long-term survivors of pediatric cancer: a report from the childhood cancer survivor study. J Cancer Surviv. 2014;8(3):437–47. https://doi.org/10.1007/s11764-014-0354-6.
Weiss RA. The discovery of endogenous retroviruses. Retrovirology. 2006;3:67. https://doi.org/10.1186/1742-4690-3-67.
Wikstrom AM, Raivio T, Hadziselimovic F, Wikstrom S, Tuuri T, Dunkel L. Klinefelter syndrome in adolescence: onset of puberty is associated with accelerated germ cell depletion. J Clin Endocrinol Metab. 2004;89(5):2263–70. https://doi.org/10.1210/jc.2003-031725.
Wu X, Schmidt JA, Avarbock MR, Tobias JW, Carlson CA, Kolon TF, Ginsberg JP, Brinster RL. Prepubertal human speratogonia and mouse gonocytes share conserved gene expression of germline stem cell regulatory molecules. Proc Natl Acad Sci U S A. 2009;106(51):21672–7. https://doi.org/10.1073/pnas.0912432106.
Wyns C, Collienne C, Shenfield F, Robert A, Laurent P, Roegiers L, Brichard B. Fertility preservation in the male pediatric population: factors influencing the decision of parents and children. Hum Reprod. 2015; https://doi.org/10.1093/humrep/dev161.
Wyns C, Curaba M, Martinez-Madrid B, Van Langendonckt A, Francois-Xavier W, Donnez J. Spermatogonial survival after cryopreservation and short-term orthotopic immature human cryptorchid testicular tissue grafting to immunodeficient mice. Hum Reprod. 2007;22(6):1603–11. https://doi.org/10.1093/humrep/dem062.
Wyns C, Curaba M, Petit S, Vanabelle B, Laurent P, Wese JF, Donnez J. Management of fertility preservation in prepubertal patients: 5 years’ experience at the Catholic University of Louvain. Human Reprod (Oxford, England). 2011;26(4):737–47. https://doi.org/10.1093/humrep/deq387.
Wyns C, Van Langendonckt A, Wese FX, Donnez J, Curaba M. Long-term spermatogonial survival in cryopreserved and xenografted immature human testicular tissue. Hum Reprod. 2008;23(11):2402–14. https://doi.org/10.1093/humrep/den272.
Yadav P, Kozak K, Tolakanahalli R, Ramasubramanian V, Paliwal BR, Welsh JS, Rong Y. Adaptive planning using megavoltage fan-beam CT for radiation therapy with testicular shielding. Med Dosim. 2012;37(2):157–62. https://doi.org/10.1016/j.meddos.2011.06.005.
Yamauchi K, Hasegawa K, Chuma S, Nakatsuji N, Suemori H. In vitro germ cell differentiation from cynomolgus monkey embryonic stem cells. PloS one. 2009;4(4):e5338. https://doi.org/10.1371/journal.pone.0005338.
Yango P, Altman E, Smith JF, Klatsky PC, Tran ND. Optimizing cryopreservation of human spermatogonial stem cells: comparing the effectiveness of testicular tissue and single cell suspension cryopreservation. Fertil Steril. 2014;102(5):1491–1498 e1491. https://doi.org/10.1016/j.fertnstert.2014.07.1250.
Yarali H, Polat M, Bozdag G, Gunel M, Alpas I, Esinler I, Dogan U, Tiras B. TESE-ICSI in patients with non-mosaic Klinefelter syndrome: a comparative study. Reprod BioMed Online. 2009;18(6):756–60.
Zheng Y, Thomas A, Schmidt CM, Dann CT. Quantitative detection of human spermatogonia for optimization of spermatogonial stem cell culture. Human Reprod (Oxford, England). 2014;29(11):2497–511. https://doi.org/10.1093/humrep/deu232.
Acknowledgments
The authors would like to thank the Scaife Foundation, the Richard King Mellon Foundation, the Magee-Womens Research Institute and Foundation, the Children’s Hospital of Pittsburgh Foundation, and the University of Pittsburgh Departments of Obstetrics, Gynecology and Reproductive Sciences and Urology, which have generously provided funds to support the Fertility Preservation Program in Pittsburgh (► https://fertilitypreservationpittsburgh.org/). It is in this context that we have had the opportunity to meet the infertile patients that fuel our passion for fertility research. The Orwig lab is supported by the Magee-Women’s Research Institute and Foundation, the Eunice Kennedy Shriver National Institute of Child Health and Human Development grants HD075795 and HD076412, the US-Israel Binational Science Foundation, and gift funds from Montana State University, Sylvia Bernassoli, and Julie and Michael McMullen.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Review Questions and Answers
Review Questions and Answers
-
Q1.
What are the standard of care fertility preservation options for pubertal boys and adult males?
-
A1.
Sperm banking is the gold standard for male fertility preservation. If no sperm is present in the ejaculate, testicular sperm extraction (TESE) could be considered.
-
Q2.
Which fertility preservation options are available for prepubertal boys?
-
A2.
Currently, there are no standard of care options available. The only option for prepubertal boys is testicular tissue freezing, which is still considered experimental.
-
Q3.
How is testicular tissue obtained from prepubertal patients?
-
A3.
Either through needle biopsy, wedge biopsy, or orchiectomy
-
Q4.
What are the possible future options for using stored testicular tissue?
-
A4.
Methods to restore fertility using cryopreserved testicular tissue in the future include spermatogonial stem cell transplantation, de novo testicular morphogenesis, testicular tissue grafting and xenografting, and testicular tissue organ culture.
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gassei, K. et al. (2019). Male Fertility Preservation: Current Options and Advances in Research. In: Woodruff, T., Shah, D., Vitek, W. (eds) Textbook of Oncofertility Research and Practice. Springer, Cham. https://doi.org/10.1007/978-3-030-02868-8_17
Download citation
DOI: https://doi.org/10.1007/978-3-030-02868-8_17
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-02867-1
Online ISBN: 978-3-030-02868-8
eBook Packages: MedicineMedicine (R0)