
Abstract
Female cancer survivors are at risk for decreased fertility and early menopause usually due to the impact of therapy on oocytes and ovaries. The ability to assess ovarian reserve or the number of oocytes in the ovaries may significantly improve care by elucidating which therapies and patients are at a higher risk of ovarian failure, as well as which patients would benefit most from fertility preservation therapies. Current markers of ovarian reserve were developed and have been well studied in infertile populations; thus, their utility in children and adolescents who undergo cancer therapy remains unknown. This chapter will discuss currently used markers of fertility and ovarian reserve and their implications in girls with cancer.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
- Ovarian reserve
- Premature ovarian insufficiency
- Infertility
- Antral follicle count
- Anti-Mullerian hormone
-
Ovarian reserve testing is a surrogate marker of fertility potential developed and evaluated in women undergoing ovarian stimulation.
-
Anti-Mullerian Hormone (AMH) is promising as an ovarian reserve marker in girls receiving cancer therapy, but many questions remain unanswered.
-
AMH levels can be impacted by many clinical parameters including current hormonal contraception, GnRH agonist therapy, and cancer therapy.
1 Background
Female cancer survivors are known to be at risk for decreased fertility and early menopause. Fertility is defined as the ability to produce young [1,2,3]. Conversely, infertility is defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse [4]. Having pregnancies thus would be the best measure of fertility. Using pregnancies as a measure of fertility, however, limits one to wait until a childhood cancer survivor has grown into an adult and has attempted to get pregnant. Even among adults, not all adult women attempt to get pregnant. Thus, surrogate measures of fertility are necessary to assess the effect of chemotherapy/radiation/surgery on fertility.
Most cancer survivors experience infertility due to direct effects of treatment on the ovary or testes. The initial number of follicles in humans is established in utero at 5 months gestation with approximately ten million primordial follicles. This number of follicles (or ovarian reserve) diminishes in utero and after birth to nearly 500,000 at menarche and continues to decline thereafter until these fall below a certain threshold and menopause appears [5]. Ovarian reserve is the concept that views reproductive potential as a function of the number and quality of oocytes. Radiation and other gonadotoxic agents are thought to affect the number of follicles by possibly accelerating this process of attrition [2, 6,7,8]. The effect of treatment on an individual patient’s ovarian reserve depends on many factors including the age at the time of gonadotoxic treatment, the type and dose of therapy, genetic factors, previous illnesses, and prior infertility. It is important to note that even before menopause (or the cessation of menses) is noted, the number and/or quality of the follicles may preclude pregnancy [9]. Infertility may be caused by decreased ovarian reserve or sperm production, but other causes such as tubal, uterine, and cervical factors may influence fertility. Thus, surrogate measures of ovarian or testicular reserve do not fully measure fertility potential.
2 Assessing Ovarian Reserve
There are several markers that have been used to assess ovarian reserve (OR) . It should be noted, however, that most of the research regarding these markers has been performed in healthy ovarian aging and women seeking treatment for infertility, and debate still remains regarding the ability of these markers to predict oocyte quality, quantity, and fecundity in healthy women. Furthermore, it is important to note that these tests are “screening” tests that would be helpful only if they predict ovarian reserve prior to menopause or ovarian insufficiency [6]. Thus, these markers may not be good measures of fertility for young women treated with gonadotoxic agents [10].
2.1 Menstrual Cycles
In 2006, the American College of Obstetrics and Gynecology (ACOG) and the American Academy of Pediatrics (AAP) issued a Committee Opinion stating that the menstrual cycle is a vital sign, thus stressing the importance of menses [11]. The average age of menarche in the western world declined rapidly in the last two centuries but has been stable since the 1950s in the developed world. Normal menstrual cycles in young females include a median age of menarche of 12 years, mean cycle interval of 32 days with a range of 21–45 days, and flow length of 7 days. Primary amenorrhea is defined as the absence of menses by age 15, and secondary amenorrhea has been defined as the absence of cycles for more than 6 months [11]. Early menopause has been defined as cessation of menses prior to age 40, and the average age of menopause in the United States is 51. Adult female survivors of childhood cancers have been noted to have earlier age of menopause and a higher rate or premature menopause than the general population [3].
The presence or absence of menses has traditionally been used as the primary measure of fertility and ovarian function in cancer survivors, but it should be noted that there are many common causes of amenorrhea including pregnancy, polycystic ovary syndrome, structural issues (scarring of the uterus), and disturbances of the central gonadotropin-releasing hormone pulse generator. These disturbances are often referred to as hypogonadotropic hypogonadism and may be caused by significant weight loss, strenuous exercise, substantial changes in sleeping or eating habits, as well as severe stressors [11]. For example, a young cancer survivor may have absence of menses due to hypothalamic disturbances caused by the stress of treatment or ovarian insufficiency due to gonadotoxic agents. In addition, women may continue to have regular menses even in the presence of diminished ovarian reserve (such as occurs in the perimenopause). Thus, the presence of menses is a poor predictor of ovarian reserve, and other markers should be used to assess OR.
2.2 Antral Follicle Counts and Ovarian Volume
Antral follicle counts and ovarian volume have traditionally been measured using transvaginal ultrasound in adult women. Both of these undergo an age-related decline and are good predictors of the number of eggs that can be retrieved with ovarian stimulation in women undergoing in vitro fertilization. Antral follicle count (AFC) is the number of small follicles (2–9 mm) that are observed in both ovaries during the early follicular phase of the cycle [6]. AFC is noted to have good inter-cycle and inter-observer reliability and thus is considered promising as a screening test for ovarian reserve. Again tests revealing low AFC (three to six total antral follicles) correlate with poor response to ovarian stimulation but do not reliably predict failure to conceive [6]. Ovarian volume in general correlates with a number of follicles but has been noted in some studies to have poor inter-cycle reliability [6]. Though inter-observer variability can be minimized with the use of three-dimensional sonography, this test is poor at predicting diminished ovarian reserve [6]. In children, AFC and ovarian volume can be performed transabdominally but requires a radiologist skilled in this technique and has not been well studied in this age group. Thus, antral follicle counts may help in predicting decreased ovarian reserve but deserves further study in cancer populations and children.
2.3 Endocrine Hormones
Biochemical tests for ovarian reserve in adult women include basal measurements such as follicle-stimulating hormone (FSH), estradiol, inhibin B, and anti-Mullerian hormone as well as stimulated tests such as the clomiphene citrate challenge test [6]. The latter cannot be performed in children, but the former should be further studied.
2.4 Follicle-Stimulating Hormone (FSH), Inhibin B, and Estradiol
FSH is secreted by the pituitary in order to stimulate follicular growth and varies throughout the menstrual cycle. When ovarian reserve is decreased, FSH begins to rise earlier in the cycle and lead to earlier follicular growth and increase in estradiol concentrations. As follicles further decrease in number, the FSH continues to rise and estradiol levels fall. Inhibin B is secreted by preantral follicles, and as follicles decrease, so does inhibin B, which in turn lowers central nervous system feedback and thus further increases FSH [12,13,14].
Serum FSH assays have significant inter- and intra-cycle variability; the absolute values differ depending on which one is used, and the sensitivity in identifying poor responders to ovarian stimulation in women varies widely [6]. In addition, children have low FSH due to hypothalamic suppression. It should be noted that in spite of these limitations, consistently high levels of FSH are predictive of diminished ovarian reserve, and repeated levels above 40 IU/L are diagnostic for premature ovarian insufficiency or menopause [6]. Estradiol assays also have poor intra- and inter-cycle variability, and basal levels do not differ between women with and without diminished ovarian reserve [6]. Furthermore, in prepubertal children, estradiol levels are also low due to hypothalamic suppression. Inhibin B has also been noted to not be a reliable measure of ovarian reserve. Thus, the use of FSH, inhibin B, and estradiol levels in assessing fertility potential of cancer patients is limited by variation with the menstrual cycles, poor sensitivity, and the low to undetectable levels in prepubertal children. Furthermore, combined ovarian reserve test models have not been shown to be superior to single tests in predicting ovarian reserve [6].
2.5 Anti-Mullerian Hormone (AMH)
AMH is a hormone produced by the granulosa cells, which acts as a follicular gatekeeper and is independent of FSH or gonadotropin. This marker is an indirect marker of antral follicle counts and thus ovarian reserve [15]. In childhood and adolescence, there is a complex rise in AMH level, which likely reflects the different stages of follicle development. It then peaks in a woman’s early 20s before declining to menopause, correlating positively with nongrowing follicle recruitment [16].
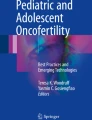
Interest in the use of AMH as a measure of ovarian reserve to measure the gonadotoxic effect of chemotherapy/radiotherapy is growing, especially for children in whom FSH and inhibin B are not useful. When compared with other ovarian reserve markers, AMH levels reflect changes in ovarian function earlier, there is less significant fluctuation of AMH during the menstrual cycle, and it is highly predictive for the timing of menopause [17,18,19], suggesting that it may be the most useful marker for monitoring the decline of reproductive capacity. Moreover, serum AMH levels are detectable in healthy females from birth to menopause [16, 20], making it suitable as a marker even in prepubertal girls (◘ Fig. 12.1).

A validated model of serum AMH from conception to menopause [16]
It should be noted that though studies of AMH screening reveal an association with poor results with in vitro fertilization (IVF), levels are not necessarily predictive [6]. Low AMH cut points are associated with sensitivities in general IVF populations of 40–97% with specificities of 78–92%, and low levels of AMH are specific for poor ovarian response but not pregnancy [6]. Furthermore, there are limited data correlating AMH and natural fertility at different stages of reproductive life and especially in children and adolescents. AMH assays continue to evolve, with intra- and inter-assay variability and sample stability and storage issues [21]. Furthermore, several clinical factors may influence AMH levels: systemic illness, endometriosis, chemotherapy, current smoking, low vitamin D levels, and certain genetic factors such as BRCA1 carrier and FMR1 mutation may decrease AMH, and white race, polycystic ovary syndrome, and granulosa cell tumor may increase AMH [21]. It is also important to note that AMH decreases during cancer therapy and may recover thereafter [22, 23]. In a case series of 16 postpubertal adolescents, more than half of patients had recovery of AMH levels by 18–24 months including several with undetectable AMH immediately after therapy [23]. A review of 192 women beginning 5 years after therapy, however, did not note an accelerated decline in AMH thereafter when compared to controls [24].
Therefore, though AMH appears to be a promising tool, more long-term data is needed to ascertain the use of AMH to evaluate fertility preservation strategies as well as predict long-term ovarian function after cancer therapy.
2.6 Current Data on AMH in Children Receiving Cancer Therapy
In women treated with mechlorethamine, vincristine, procarbazine, and prednisone (MOPP) chemotherapy for Hodgkin lymphoma during childhood, AMH was noted to be lower compared with healthy women and women treated without MOPP [25]. In a larger series of 185 childhood cancer survivors, although the cohort’s median AMH concentration was no different from controls, the AMH levels were lower than the tenth percentile of normal values in 27% of the survivors. Survivors treated with three or more procarbazine-containing chemotherapy cycles and those treated with abdominal or total body irradiation had significantly lower AMH levels than controls [26]. Recent studies have revealed low AMH in more than half of childhood cancer survivors with the lowest levels in those treated with radiation and bone marrow transplant and those treated for Hodgkin’s lymphoma but effects noted even in those receiving low-risk therapies [27, 28]. As stated before, in adult women and adolescents with cancer, AMH declines during treatment followed by recovery in some patients, with the rate of recovery determined by the pretreatment AMH level [23, 29].
2.7 Ovarian Reserve Testing as a Predictor of Menstrual Pattern and Fertility
Ovarian reserve testing to predict the risk of acute ovarian failure and early menopause and future fertility in females prior to cancer therapy would allow us to better target patients for ovarian preservation procedures [30]. In adults, one small series in breast cancer survivors demonstrated that inhibin B and AMH prior to therapy were significantly lower in the women who went on to develop amenorrhea after treatment [31]. Similarly, in 46 adolescent and young adult women with a new cancer diagnosis requiring chemotherapy, pretreatment AMH levels were associated with the rate of recovery of AMH after treatment. Participants with a pretreatment AMH level >2 ng/mL had a faster rate of recovery of AMH after chemotherapy compared to participants with pretreatment AMH levels </= 2 ng/mL [29]. More recently, studies in breast cancer patients have provided some prognostic tools to predict the likelihood and timing of return of ovarian function after chemotherapy [21].
In addition, the ability of ovarian reserve testing to predict time to menopause and ovarian insufficiency on survivors who are menstruating would be very useful in order for them to plan post-treatment fertility preservation and other therapies [30]. In a prospective study of breast cancer survivors who were still menstruating, the patients who had cessation of menses 2 years later were more likely to have lower AMH and higher FSH at study entry [30].
Most research regarding ovarian reserve testing and prediction of ovarian function after chemotherapy have been performed in breast cancer, and thus, research in other types of cancer therapies is needed. Furthermore, to date, there is no data regarding the ability of ovarian reserve testing to predict the risk of premature menopause in prepubertal girls before therapy or in survivors of childhood cancer.
2.8 Effect of Female Hormones on Ovarian Reserve Testing
Many young women who receive cancer therapy are placed on birth control pills to regulate menses or estrogen replacement therapy when ovarian insufficiency is suspected. It is important to understand the effect of this treatment on ovarian reserve testing. A study evaluating ovarian reserve testing in 887 healthy women, 18–46 years old, found that AMH, antral follicle counts, and ovarian volume were all significantly decreased in oral contraception users when compared to nonusers [32]. In a small study comparing young cancer survivors on birth control pills with control women on the pills during the 3rd week of pills (while taking active pills), there were no differences noted in FSH, inhibin B, estradiol, or AMH, but the AFC was lower in the cancer survivors [33]. Furthermore, AMH levels may change with GnRH agonist administration, which is often used during cancer treatment to suppress menses or for possible ovarian protection [34].
Several studies have evaluated ovarian reserve testing during the placebo or pill-free week comparing survivors with spontaneous menses and those on birth control pills. Results from these studies are contradictory, use small samples, and compare populations exposed to cancer therapy to each other and not healthy age-matched controls [25, 35]. In addition, there are no studies which evaluate whether ovarian reserve testing in women on female hormones is predictive of menstrual function or fertility.
3 Conclusions
Ovarian reserve testing has been extensively studied in healthy women who seek infertility treatment but not in young girls receiving cancer therapy. This population would benefit significantly from rigorous data regarding ovarian reserve testing, which may predict their risk of early menopause and assess the risk and benefits of fertility preservation options. Research in this population is limited by the fact that the numbers of girls at individual institutions are low as well as the fact that the outcome of interest (the ability to achieve successful pregnancy) may be far in the future [33]. Future multicenter studies with collaborative efforts of reproductive specialists, oncologists, and patient advocates will need to be performed.
References
Byrne J, et al. Early menopause in long-term survivors of cancer during adolescence. Am J Obstet Gynecol. 1992;166(3):788–93.
Green DM, et al. Ovarian failure and reproductive outcomes after childhood cancer treatment: results from the Childhood Cancer Survivor Study. J Clin Oncol. 2009;27(14):2374–81.
Thomas-Teinturier C, et al. Age at menopause and its influencing factors in a cohort of survivors of childhood cancer: earlier but rarely premature. Hum Reprod. 2013;28(2):488–95.
Zegers-Hochschild F, et al. International Committee for Monitoring Assisted Reproductive Technology (ICMART) and the World Health Organization (WHO) revised glossary of ART terminology, 2009. Fertil Steril. 2009;92(5):1520–4.
Faddy MJ, Gosden RG. A model conforming the decline in follicle numbers to the age of menopause in women. Hum Reprod. 1996;11(7):1484–6.
Practice committee of the american society for reproductive medicine. Testing and interpreting measures of ovarian reserve: a committee opinion. Fertil Steril. 2015;103(3):e9–17.
Goodwin PJ, et al. Risk of menopause during the first year after breast cancer diagnosis. J Clin Oncol. 1999;17(8):2365–70.
Bines J, Oleske DM, Cobleigh MA. Ovarian function in premenopausal women treated with adjuvant chemotherapy for breast cancer. J Clin Oncol. 1996;14(5):1718–29.
Koyama H, et al. Cyclophosphamide-induced ovarian failure and its therapeutic significance in patients with breast cancer. Cancer. 1977;39(4):1403–9.
Domingues TS, Rocha AM, Serafini PC. Tests for ovarian reserve: reliability and utility. Curr Opin Obstet Gynecol. 2010;22(4):271–6.
ACOG Committee Opinion No. 349. November 2006: menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Obstet Gynecol. 2006;108(5):1323–8.
Burger HG. The endocrinology of the menopause. Maturitas. 1996;23(2):129–36.
Richardson SJ, Senikas V, Nelson JF. Follicular depletion during the menopausal transition: evidence for accelerated loss and ultimate exhaustion. J Clin Endocrinol Metab. 1987;65(6):1231–7.
Burger HG, et al. The endocrinology of the menopausal transition: a cross-sectional study of a population-based sample. J Clin Endocrinol Metab. 1995;80(12):3537–45.
La Marca A, et al. Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART). Hum Reprod Update. 2010;16(2):113–30.
Kelsey TW, et al. A validated model of serum anti-Mullerian hormone from conception to menopause. PLoS One. 2011;6(7):e22024.
Tsepelidis S, et al. Stable serum levels of anti-Mullerian hormone during the menstrual cycle: a prospective study in normo-ovulatory women. Hum Reprod. 2007;22(7):1837–40.
van Rooij IA, et al. Serum antimullerian hormone levels best reflect the reproductive decline with age in normal women with proven fertility: a longitudinal study. Fertil Steril. 2005;83(4):979–87.
Broer SL, et al. Anti-mullerian hormone predicts menopause: a long-term follow-up study in normoovulatory women. J Clin Endocrinol Metab. 2011;96(8):2532–9.
Hagen CP, et al. Serum levels of anti-Mullerian hormone as a marker of ovarian function in 926 healthy females from birth to adulthood and in 172 Turner syndrome patients. J Clin Endocrinol Metab. 2010;95(11):5003–10.
Tal R, Seifer DB. Ovarian reserve testing: a user’s guide. Am J Obstet Gynecol. 2017;217(2):129–40.
Miyoshi Y, Yasuda K, Tachibana M, Yoshida H, Miyashita E, Miyamura T, Hashii Y, Hashimoto K, Kimura T, Ozono K. Longitudinal observation of serum anti-Müllerian hormone in three girls after cancer treatment. Clin Pediatr Endocrinol. 2016;25(4):119–26.
Gupta AA, Lee Chong A, Deveault C, Traubici J, Maloney AM, Knight S, Lorenzo A, Allen L. Anti-Müllerian hormone in female adolescent cancer patients before, during, and after completion of therapy: a pilot feasibility study. J Pediatr Adolesc Gynecol. 2016;29(6):599–603.
van der Kooi AL, van den Heuvel-Eibrink MM, van Noortwijk A, Neggers SJ, Pluijm SM, van Dulmen-den Broeder E, van Dorp W, Laven JS. Longitudinal follow-up in female childhood cancer survivors: no signs of accelerated ovarian function loss. Hum Reprod. 2017;32(1):193–200.
van Beek RD, et al. Anti-Mullerian hormone is a sensitive serum marker for gonadal function in women treated for Hodgkin’s lymphoma during childhood. J Clin Endocrinol Metab. 2007;92(10):3869–74.
Lie Fong S, et al. Assessment of ovarian reserve in adult childhood cancer survivors using anti-Mullerian hormone. Hum Reprod. 2009;24(4):982–90.
Krawczuk-Rybak M, Leszczynska E, Poznanska M, Zelazowska-Rutkowska B, Wysocka J. Anti-müllerian hormone as a sensitive marker of ovarian function in young cancer survivors. Int J Endocrinol. 2013;2013:125080.
Elchuri SV, Patterson BC, Brown M, Bedient C, Record E, Wasilewski-Masker K, Mertens AC, Meacham LR. Low anti-Müllerian hormone in pediatric cancer survivors in the early years after gonadotoxic therapy. J Pediatr Adolesc Gynecol. 2016;29(4):393–9.
Dillon KE, et al. Pretreatment antimullerian hormone levels determine rate of posttherapy ovarian reserve recovery: acute changes in ovarian reserve during and after chemotherapy. Fertil Steril. 2013;99(2):477–83.
Su HI. Measuring ovarian function in young cancer survivors. Minerva Endocrinol. 2010;35(4):259–70.
Anders C, et al. A pilot study of predictive markers of chemotherapy-related amenorrhea among premenopausal women with early stage breast cancer. Cancer Investig. 2008;26(3):286–95.
Birch Petersen K, et al. Ovarian reserve assessment in users of oral contraception seeking fertility advice on their reproductive lifespan. Hum Reprod. 2015;30(10):2364–75.
Bath LE, et al. Depletion of ovarian reserve in young women after treatment for cancer in childhood: detection by anti-Mullerian hormone, inhibin B and ovarian ultrasound. Hum Reprod. 2003;18(11):2368–74.
Broer SL, Broekmans FJ, Laven JS, Fauser BC. Anti-Müllerian hormone: ovarian reserve testing and its potential clinical implications. Hum Reprod Update. 2014;20(5):688–701.
Larsen EC, et al. Reduced ovarian function in long-term survivors of radiation- and chemotherapy-treated childhood cancer. J Clin Endocrinol Metab. 2003;88(11):5307–14.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Review Questions and Answers
Review Questions and Answers
-
Q1.
Ovarian reserve testing refers to testing to evaluate the number of follicles remaining in the ovaries. True or False?
-
A1.
True
-
Q2.
Menstrual history is an excellent way to assess ovarian reserve. True or False?
-
A2.
False
-
Q3.
Of the following markers of ovarian reserve , which is the most promising for children and adolescents?
-
(a)
FSH
-
(b)
Inhibin-B
-
(c)
Antral Follicle Count (AFC)
-
(d)
AMH
-
(e)
Menses
-
(a)
-
A3.
(d)
-
Q4.
AMH results are impacted as stated below except:
-
(a)
Current chemotherapy is associated with decreased AMH
-
(b)
Birth control pills are associated with increased AMH
-
(c)
Low vitamin D is associated with decreased AMH
-
(d)
Polycystic ovary syndrome (PCOS) is associated with increased AMH
-
(e)
White race is associated with increased AMH
-
(a)
-
A4.
(b)
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Gosiengfiao, Y., Gomez-Lobo, V. (2019). Assessing Ovarian Reserve. In: Woodruff, T., Shah, D., Vitek, W. (eds) Textbook of Oncofertility Research and Practice. Springer, Cham. https://doi.org/10.1007/978-3-030-02868-8_12
Download citation
DOI: https://doi.org/10.1007/978-3-030-02868-8_12
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-02867-1
Online ISBN: 978-3-030-02868-8
eBook Packages: MedicineMedicine (R0)