
Abstract
Preoperative evaluation of the lung transplant recipient allows for optimal planning of intraoperative ventilation, hemodynamic support, and the need for extracorporeal support. Careful induction of anesthesia is required to avoid acute right ventricular failure and cardiovascular collapse, and transesophageal echocardiography is invaluable in the diagnosis of hemodynamic instability. The increasing perioperative use of extracorporeal membrane oxygenation bestows new challenges on the anesthesiologist, in terms of hemodynamic, anticoagulation, and fluid management. Early postoperative extubation is feasible, and reduction in early complications confers a long-term survival benefit.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Donor organ
- End-stage lung disease
- Extracorporeal support
- Lung transplantation
- Right ventricular failure
-
Preoperative assessment is paramount for planning intraoperative strategies.
-
Careful induction of anesthesia is essential to avoid cardiovascular collapse.
-
Transesophageal echocardiography is an invaluable intraoperative tool.
-
Perioperative extracorporeal membrane oxygenation support is beneficial for patients but provides new challenges for the anesthesiologist.
-
Reduction in early postoperative complications confers a long-term survival benefit.
Introduction
Lung transplantation (LT) is the treatment of choice for some patients with end-stage lung disease or pulmonary vascular disease [1]. The term “lung transplantation” encompasses a group of operations, comprised of lobar transplant, single-lung transplant (SLT), double-lung transplant, bilateral sequential lung transplant (BSLT), and heart-lung transplant (HLT). The first reported human LT was undertaken in 1963 [2], but outcomes were poor until the introduction of ciclosporin (also spelled cyclosporin) and the development of newer surgical techniques in the 1980s. The first reported successful LT was performed in 1983 at Toronto General Hospital [3]. The number of LT has increased significantly over the last 30 years (Fig. 47.1) and outcomes have gradually improved; median survival for LT is now approximately 6 years (Fig. 47.2) [1].

Number of lung transplants reported by year. (From the International Society for Heart and Lung Transplantation, with permission)

Survival for adult lung transplantation. The median survival is the estimated time point at which 50% of all of the recipients have died. The conditional median survival is the estimated time point at which 50% of the recipients who survive to at least 1 year have died. Because the decline in survival is greatest during the first year following transplantation, the conditional survival provides a more realistic expectation of survival time for recipients who survive the early post-transplant period. (From the International Society for Heart and Lung Transplantation, with permission)
Donor Organ Management
The potential donor patient is often cared for in a nontransplant critical care unit [4]. After the diagnosis of brain stem death (BSD), the pathophysiological sequelae must be appropriately managed to effectuate organ preservation [5,6,7,8,9]. This includes intravenous fluid administration and vasoactive drug therapy to achieve a mean arterial pressure (MAP) above 70 mmHg, heart rate 60–120 beats per minutes, and a central venous pressure (CVP) or pulmonary artery wedge pressure (PAWP) between 6 and 10 mmHg [10, 11]. Intravenous fluid restriction and judicious use of diuretics help to reduce fluid accumulation in the lungs. The use of “hormonal” therapy, comprised of thyroxine, methylprednisolone, and vasopressin, has been shown to increase the number of transplantable organs. Ventilatory settings are altered to protect the potential donor lungs. This includes the use of pressure-controlled ventilation with appropriate positive end-expiratory pressure (PEEP) to give tidal volumes of 6–8 mL/kg. Bronchoscopic pulmonary toilet is used to clear retained secretions. Basic critical care therapies, including normothermia, antimicrobial use, nutrition, correction of electrolyte imbalance, and treatment of diabetes insipidus are essential [12,13,14,15].
During procurement, the donor receives systematic heparinization, and the pulmonary artery is flushed with a cold preservation solution. Prostaglandin is infused into the donor pulmonary circulation to inhibit the vasoconstrictive response to the cold pneumoplegia solution and to inhibit platelet aggregation. The donor lungs are ventilated throughout the flush and are inflated to a pressure of 10–20 cmH2O prior to dividing the airways. The harvested allograft is then stored at 4 °C for transfer to the recipient center [16,17,18].
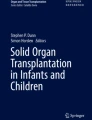
Less than 20% of donors of other solid organs have lungs that are suitable for transplantation. This may be related to the etiology of BSD or secondary to pulmonary aspiration of gastric contents at the time of brain injury [12, 19]. Due to the imbalance between the number of candidates awaiting transplantation and the availability of suitable donor organs, the “standard” criteria for donor lung acceptance have been extended to include “marginal” donors (Table 47.1). The survival of recipients from these “marginal” donors may be decreased to those from standard donors, and a higher incidence of primary graft dysfunction (PGD) has been reported [20,21,22,23]. Several strategies have been developed in an attempt to increase the donor organ pool. This includes the use of patients in Maastricht category III: donation after cardiac death (DCD). Donors are typically patients in a critical care environment, who are expected to die within 60–90 min of withdrawal of active treatment. Ethical considerations mandate the use of two separate teams: one for therapy withdrawal and the second for organ harvesting. Lung preservation interventions are withheld until cardiac death has been certified [10, 24,25,26]. The lungs are unique in their ability to tolerate a warm ischemia time of at least 1 h [27]. Outcomes of recipients from DCD are comparable to those from BSD donors [26, 28]. Ex vivo lung perfusion (EVLP) and reconditioning are techniques that allow assessment and optimization of potential donor lungs outside of the donor. After organ harvesting, the lungs are perfused on an external circuit and ventilated (Fig. 47.3). The lungs can then be optimized and assessed for adequate function prior to transplantation [29,30,31]. Patient outcomes are similar to those with conventional transplants [32, 33]. The role of EVLP is now being extended: assessment of lungs from uncontrolled circulatory death; standard donor organs can be evaluated ex vivo to allow for exclusion of functionally impaired lungs; and the extension of graft perfusion time may facilitate better timing of transplant operations [34,35,36].

Donor lungs inside a sterile plastic dome undergoing ex vivo perfusion. During ventilation via an endotracheal tube in the donor trachea, the lungs are perfused with a crystalloid solution. The yellow cannula is in the main pulmonary artery and the green cannula in the cuff of the donor left atrium
Recipient Candidates
Transplantation is indicated for patients with end-stage lung disease who are failing medical therapy, with the goal to provide a survival benefit. Due to the relative shortage of donor organs, it is necessary to list only patients with realistic beneficial outcomes. Listing for transplantation should occur when life expectancy after transplant exceeds life expectancy without the procedure. Donors and recipients are matched according to blood group and size [37,38,39]. The common underlying pathologies responsible for LT referral include chronic obstructive pulmonary disease (COPD), alpha-1 antitrypsin deficiency (AATD), cystic fibrosis (CF), pulmonary hypertension (PHT), and interstitial lung disease (ILD), incorporating usual interstitial pneumonitis (UIP), fibrosing non-specific interstitial pneumonitis (NSIP), and non-idiopathic interstitial pneumonitis (non-IIP) (Fig. 47.4). Contraindications to LT are listed in Table 47.2.

Indications for lung transplantation. AATD alpha-1 antitrypsin deficiency, CF cystic fibrosis, COPD chronic obstructive pulmonary disease, ILD interstitial lung disease, PHT pulmonary hypertension, Re-Tx re-transplantation. (Based on data form the International Society of Heart and Lung Transplantation <https://www.ishlt.org> accessed May 2017)
Disease-specific indications for referral and listing for transplantation are summarized in Table 47.3 [39]. Patients suffering from emphysematous diseases are assessed using the BODE index, which involves scoring body mass index, airflow obstruction, degree of dyspnea, and exercise capacity on a scale from 0 to 10. A BODE index ≥7 is associated with lower survival than would be expected after transplantation. Three or more severe exacerbations within 1 year are associated with increased mortality, and an episode of acute hypercapnic respiratory failure carries a 43% 1-year mortality [39, 40]. Lung volume reduction surgery may provide an alternative or a bridge-to-transplant in some emphysema patients [41, 42]. Cystic fibrosis patients are prone to colonization with resistant pathogens. Infection with Burkholderia cenocepacia and non-tuberculous Mycobacterium is associated with increased morbidity and mortality and confers a contraindication in some centers [39, 43]. Patients with ILD have the worst prognosis of those referred for LT. The introduction of the lung allocation score (LAS) system, designed to prioritize patients with the highest mortality on the waiting list, has increased the number of ILD candidates receiving transplantation [44, 45]. Significant developments in targeted medical therapy for pulmonary hypertension had led to improvements in management and a postponement in referral for LT listing in this population [39]. Patients with PHT secondary to pulmonary veno-occlusive disease should be referred for LT assessment at the time of diagnosis, as there is no established medical therapy, and the prognosis is poor [46]. The incidence of re-transplantation has increased since the introduction of the LAS system. The same criteria for initial LT listing are used. Whether SLT or BSLT is planned, removal of the failed allograft is recommended to reduce infection risk and ongoing stimulation of the immune system. Patients requiring re-transplant after 2 years of their original procedure have better outcomes than those who are re-transplanted within 30 days [39, 47,48,49]. Previously, patients in a critical condition, supported with mechanical ventilation or extracorporeal life support (ECLS) were deemed unsuitable candidates [50]. However, improvements in technology and expanded experience in the management of ECLS have allowed for such patients to be bridged to transplantation with ECLS, with acceptable outcomes [51,52,53].
Anesthesia for Lung Transplantation
Preoperative Assessment
Due to the nature of LT, the anesthesiologist usually has limited time for preoperative assessment [54]. In some centers the listed candidates are reviewed in an assessment clinic by an anesthesiologist to highlight pertinent anesthetic considerations. Patients are typically debilitated, with poor cardiorespiratory reserve. Latent ischemic heart disease and right ventricular (RV) dysfunction are not uncommon, especially in elderly patients, although the presence of noncritical coronary artery disease does not appear to influence postoperative outcomes [55,56,57,58]. After admission to hospital for surgery, there is limited time to optimize the patient: chest physiotherapy to clear secretions, bronchodilator therapy, and drainage of significant pleural effusions or pneumothoraces. In addition to a standard preoperative evaluation, anesthetic assessment should focus on [59]:
-
Underlying diagnosis: obstructive, restrictive, or suppurative pathology. This facilitates selection of appropriate ventilator settings.
-
Pulmonary artery (PA) pressure: this will dictate the likelihood of undertaking the procedure without the use of ECLS.
-
Ventilation/perfusion (V/Q) scan: the differential perfusion to each lung (in BSLT) will determine which lung initially will better tolerate PA clamping and pneumonectomy.
-
Arterial blood gases (ABGs): baseline pO2/pCO2 helps define acceptable intraoperative limits.
-
Echocardiography: knowledge of RV and left ventricular (LV) function will influence the requirement for ECLS.
Standard premedication involves immunosuppressant drugs, bronchodilator therapy, and supplemental oxygen. The routine use of anxiolytic medication is not recommended, and any sedative agents should be administered with caution, as they can exacerbate hypoxemia and hypercapnia, leading to worsening PHT and RV failure.
Monitoring
Routine monitoring includes electrocardiography (ECG), pulse oximetry, invasive arterial and central venous pressure (CVP) measurements, pulmonary artery catheterization (PAC), temperature measurement, capnography, and inhalational agent monitoring. Minimally invasive cardiac output monitoring has been used extensively in the nontransplant perioperative setting and in nonpulmonary transplantation with mixed conclusions [60,61,62,63]. Mixed venous oximetry has been used successfully intraoperatively, and cerebral oximetry has been shown to improve outcomes in cardiac surgery [64,65,66,67]. The use of depth of anesthesia monitoring may reduce the incidence of awareness, and when used in combination with a closed-loop anesthesia, delivery system provides better titration of drugs, giving the anesthesiologist more time to focus on intraoperative hemodynamic and surgical events [68, 69]. Early detection and prevention of intraoperative hypothermia is important to prevent cardiac dysrhythmias, coagulopathy, and altered drug metabolism and to reduce the risk of postoperative infection [70, 71].
Transesophageal Echocardiography
The value of intraoperative transesophageal echocardiography (TEE) in LT surgery is well established [72,73,74,75]. TEE is more accurate at determining preload and volemic status compared to PAC [76]. It facilitates rapid diagnosis of hemodynamic instability, including evaluation of RV function after PA clamping, LV dysfunction, detection of gaseous emboli, and assessment of surgical anastomotic sites [75, 77,78,79]. Significant stenosis of pulmonary vein anastomoses is more commonly seen on the left (Fig. 47.5) and can result in pulmonary venous congestion and graft failure. However, TEE can overestimate pulmonary vein Doppler peak velocities, and caution is required when interpreting findings [80, 81]. The presence of an interatrial septal defect or patent foramen ovale can lead to a significant right-to-left shunt during periods of increased pulmonary vascular resistance (PVR) or when increased PEEP is employed. Prompt detection by TEE can aid in diagnosing this cause of worsening hypoxemia [82]. With the expansion of intraoperative extracorporeal membrane oxygenation (ECMO) support in LT surgery, TEE is also beneficial in assisting in positioning of cannulae and differentiating between hypovolemia and cannula obstruction when low ECMO flows are encountered (Fig. 47.6) [83, 84].

Transesophageal echocardiography showing turbulence on color flow Doppler imaging (arrow) in a stenotic left pulmonary vein anastomosis. LA left atrium

Transesophageal echocardiography midesophageal (a) and transgastric (b) views showing right ventricular dilatation and flattening of the interventricular septum with leftward shift. LV left ventricle, RV right ventricle
Induction of Anesthesia
Thorough preoxygenation of the patient is prudent. Induction of anesthesia may precipitate cardiovascular collapse due to a combination of factors: systemic vasodilation and negative inotropic effects of anesthetic drugs, reduced venous return due to an increase in intrathoracic pressure secondary to positive pressure ventilation and PEEP, and RV failure caused by an increase in PVR due to hypoventilation and subsequent hypercapnia [85,86,87].
In patients with obstructive lung pathologies, it is important to allow sufficient time for the expiratory phase to occur and to avoid PEEP, in order to reduce the risk of dynamic hyperinflation. Overenthusiastic manual ventilation after induction of anesthesia can lead to severe gas trapping in emphysematous lungs, resulting in reduced venous return and direct cardiac compression: “pulmonary tamponade” [88, 89]. Profound hypotension ensues, and correct management is to disconnect the patient from the breathing circuit to allow sufficient time for expiration of trapped gases [90].
Patients with restrictive lung disease typically require higher ventilatory pressures to deliver an adequate tidal volume and often benefit from the application of increased levels of PEEP. Adoption of a ventilation strategy similar to that used in acute lung injury (ALI) is more appropriate for this group of patients [91, 92].
Recipients with suppurative pathologies may have mixed obstructive/restrictive respiratory defects, so appropriate ventilation should be individualized. Thorough bronchial lavage after intubation of the patient may reduce intraoperative sputum plugging and assist in maintaining adequate ventilation throughout the procedure.
In patients with pulmonary vascular disease, smooth induction of anesthesia is critical to prevent systemic hypotension, PA hypertensive crises, myocardial depression, hypoxemia, and hypercapnia. It may be useful to obtain central venous access before induction of anesthesia for administration of vasopressors. Anesthetic goals include [93]:
-
Avoid acute increases in RV preload: RV dilatation increases RV wall tension, increasing oxygen demand; elevates RV end-diastolic pressure (RVEDP), reducing oxygen delivery; and worsens tricuspid regurgitation (TR), exacerbating volume overload.
-
Maintain RV perfusion: avoid systemic hypotension and increases in RVEDP.
-
Maintain sinus rhythm and positive chronotropy.
-
Augment RV contractility with inotropic support when necessary.
-
Decrease PVR: avoid hypoxemia, hypercapnia, and acidemia.
Ketamine may be a more appropriate induction agent in severe cases, with vasoactive infusions commenced prior to induction. The use of inhaled pulmonary vasodilators and preinduction ECLS has been described [94, 95]. The anesthesiologist should be prepared for emergency institution of cardiopulmonary bypass (CPB) after induction.
Disease-specific intraoperative anesthetic considerations are summarized in Table 47.4.
Following induction, the airway is secured with either a single-lumen or double-lumen tube (DLT). A single-lumen tube in combination with an endobronchial blocker provides an alternative technique to DLT [96, 97]. In BSLT, the blocker will need repositioning under bronchoscopic guidance to allow surgery on the opposite side. A left-sided DLT is preferred to a right-sided DLT, which may interfere with the right-sided bronchial anastomosis. In patients with significant suppurative pathologies (e.g., cystic fibrosis), it is common to initially insert a single-lumen tube in order to facilitate bronchoscopic toilet and suctioning of thick secretions, prior to exchanging for a DLT. Bronchoscopic lavage samples can be sent for microbiological analysis to direct postoperative antimicrobial therapy. Prophylactic antibiotic regimens are institution-related but must provide adequate gram-positive and gram-negative cover. Patients with CF often require alternative antimicrobials, depending on their history of allergies, microbe colonization, and presence of drug-resistant organisms [98, 99].
Maintenance of Anesthesia
Maintenance of anesthesia is achieved with either inhalational or intravenous agents [100, 101]. Nitrous oxide should be avoided as it may increase PVR [102]. SLT can be performed through a standard posterolateral thoracotomy, with the patient in the lateral position, or via an anterior thoracotomy, in the supine position. This latter approach provides easier surgical cannulation access if urgent ECLS is needed. BSLT may be performed either via a midline sternotomy, bilateral thoracotomies, or “clamshell” incision [103].
Initiation of one-lung ventilation (OLV) will initially cause an increase in shunt with worsening hypoxemia until surgical stapling of the PA. During OLV pressure-controlled ventilation may proffer some benefits over volume-controlled ventilation, by reducing peak airway pressures [104, 105]. Patients unable to tolerate OLV will require CPB or ECMO support [106].
Optimal fluid management is paramount during the intraoperative period. Patient hemodynamics are influenced by volemic status and preload optimization is essential. However, the lung allograft is prone to low-pressure pulmonary edema, secondary to re-expansion injury, ischemia-reperfusion microvascular leak, and the absence of lymphatic drainage. A restrictive fluid regimen is recommended, with surgical blood loss replaced by boluses of colloid or blood products as indicated [107, 108].
Management of RV Dysfunction
Surgical clamping of the PA during OLV will reduce shunt and improve oxygenation but will result in an acute increase in PA pressures. In patients with pre-existing PHT, it is prudent for the surgeon to apply temporary PA clamping to determine the effect on PA pressures and RV function [109]. Early diagnosis of RV failure by TEE allows for prompt management and potential avoidance of ECLS [78]. Recipients with severe PHT rarely tolerate PA clamping, and the elective use of ECLS is employed [110].
An acute elevation in PVR causes a combination of detrimental effects, which may ultimately result in RV failure. The increase in RV afterload will initially reduce RV stroke volume, leading to a rise in RVEDV. RV dilatation can worsen the severity of TR, exacerbating volume overload, further raising RVEDV and consequently RVEDP. There is a leftward shift of the interventricular septum, inhibiting LV diastolic filling and decreasing LV stroke volume. The subsequent fall in cardiac output leads to systemic hypotension and, coupled with an increase in RVEDP, a reduction in RV perfusion pressure. RV ischemia follows, with further RV decompensation and failure [93].
The use of selective pulmonary vasodilators, inhaled nitric oxide (iNO), and prostacyclin therapy reduces PVR, improves oxygenation, and can reverse RV failure [111,112,113,114]. Catecholamines and phosphodiesterase inhibitors (PDE-I) will provide positive inotropy and improve RV contractility. PDE-I may reduce PVR but also have the less desirable side effect of systemic vasodilatation and hypotension, often necessitating the addition of vasopressor support to maintain coronary perfusion [115,116,117,118]. Levosimendan restores RV-PA coupling by decreasing PVR and increasing RV contractility but is also associated with systemic vasodilatation [119]. Norepinephrine is the initial vasoconstrictor of choice: it improves ventricular systolic interaction and coronary perfusion and may also improve RV-PA coupling. Vasopressin can be added in cases of refractory hypotension [118].
Extracorporeal Support
There is institutional and surgical variation in preference for utilization of CPB. Elective use of ECLS, either full CPB or ECMO, is indicated in recipients with severe PHT and in HLT [120]. SLT is typically performed “off-pump” via a thoracotomy. When BSLT is performed “off-pump,” the lung receiving less perfusion (from the preoperative V/Q scan) should be replaced first. For BSLT with CPB, the heart remains warm and beating. After implantation of the first allograft, the heart is allowed to eject a little, and the lung is gently ventilated.
In recent years, the use of full CPB has been replaced by other forms of ECLS: veno-venous (VV) and venoarterial (VA) ECMO support [121,122,123]. VA-ECMO, like full CPB, provides both cardiac and respiratory support but requires less heparinization. Central cannulation sites, right atrium (RA) and ascending aorta, are generally preferred, as higher ECMO flows can be achieved, necessitating less anticoagulation. Peripheral cannulation, usually femoral vein (FV) to femoral artery, allows for continued ECLS support into the postoperative period in cases of severe PGD, and the chest can be closed [124, 125]. However, the anesthesiologist must remain vigilant during the intraoperative period, as lower ECMO flows permit more blood flow through the heart and lungs, which may be significantly deoxygenated: ECMO Harlequin syndrome may occur, resulting in cerebral hypoxia with peripheral VA cannulation. Pulse oximetry and arterial pressure monitoring should be placed on the right upper limb to ensure adequate oxygenation, and cerebral oximetry is advantageous [126, 127]. VV-ECMO provides only respiratory support, but the correction of hypoxemia and hypercapnia can markedly enhance RV function, leading to improved hemodynamics. Cannulation is typically peripheral and can be achieved with either a single dual-lumen cannula or by two cannulae [128, 129]. Fluid management is more challenging during ECMO support: ECMO flows are highly dependent on patient venous pressures, so sufficient fluid must be administered to maintain adequate ECMO flows without causing fluid overload and “wet” lungs. The utilization of ECMO support instead of CPB has led to better patient outcomes [130,131,132,133,134]. If postoperative VV-ECMO is probable, it may be useful to avoid using the right internal jugular vein for central access during surgery.
Organ Reperfusion
Reperfusion of the allograft should occur gradually, over a period of 5–10 min, as it may result in significant hypotension due to release of stored pneumoplegia, inflammatory mediators, and gas emboli into the systemic circulation [135]. Simultaneously, gentle alveolar recruitment and ventilation are commenced with limited peak airway pressures, moderate PEEP (5–10 cmH2O), and initially with a fraction of inspired oxygen (FiO2) less than 40% [136,137,138,139]. In BSLT the residual native lung can be ventilated with a high FiO2 to maintain arterial oxygenation, while the new allograft is reperfusing with protective ventilation. After this initial period of reperfusion, the FiO2 to the allograft is increased as necessary, while ventilation to the native lung is stopped to enable surgical explantation. Ischemia-reperfusion injury (IRI) presents as hypoxemia despite increasing FiO2, reduced lung compliance, PHT, and, in severe cases, pulmonary edema. PGD due to IRI is associated with an increased mortality [140]. The administration of iNO is effective in improving oxygenation in cases of IRI, but its routine use to prevent IRI is of less benefit [141,142,143]. Severe PGD can be managed with ECLS, usually VV-ECMO, with acceptable outcomes [144, 145].
Analgesia
In the postoperative period, insufficient pain control hinders spontaneous deep breathing, adequate coughing, and sputum clearance. Analgesic options comprise paracetamol, intravenous opiates, and regional techniques, including epidural and paravertebral analgesia. Opioid-sparing regimens are encouraged to reduce respiratory depression. Epidural insertion can be performed prior to surgery, to facilitate earlier postoperative extubation, or postoperatively, after coagulopathy has been excluded [146, 147]. Paravertebral catheters can be placed by the surgeon at the end of a SLT as an alternative to epidural analgesia [148]. There may be a role for low-dose intravenous ketamine as an adjunct to reduce postoperative opiate requirements [149, 150]. Nonsteroidal anti-inflammatory drugs are avoided due to the increased risk of renal dysfunction in patients receiving calcineurin inhibitors for immunosuppression [151].
Postoperative care
Early extubation in the operating room is feasible, especially after SLT [152, 153]. The advantages include avoidance of positive pressure ventilation, with potential barotrauma, reduced extravascular lung water, decreased PA pressures, lower requirements for vasoactive drugs, and early mobilization with physiotherapy. This is facilitated by the use of short-acting anesthetic agents, epidural analgesia, and the absence of intraoperative complications [153, 154]. For patients returning to the intensive care unit for postoperative ventilation, the DLT is changed to a single-lumen tube, and a nasogastric tube is passed to permit early administration of enteral immunosuppression.
Ventilatory support involves a lung protective strategy and potential differential lung ventilation in patients with SLT for emphysema. Tracheostomy is considered if prolonged ventilation is anticipated [155,156,157,158].
Early complications include PGD, hemorrhage, iatrogenic surgical anastomotic anomalies, infection, cardiac dysrhythmias, renal failure, and venous thromboembolism [159,160,161,162,163,164,165]. Early complications have a negative impact on long-term survival [166]. Prevention of acute rejection is managed with a combination of steroids, calcineurin inhibitors, antiproliferatives, and mammalian target of rapamycin (mTOR) inhibitors. The routine use of induction therapy with monoclonal or polyclonal antibodies is controversial but may confer some survival benefit in BSLT [167]. Late complications include chronic rejection, presenting as bronchiolitis obliterans, infection, renal dysfunction, diabetes mellitus, and malignancy [1, 168].
References
Yusen RD, Edwards LB, Dipchand AI, et al. The registry of the International Society for Heart and Lung Transplantation: thirty-third adult lung and heart-lung transplant report-2016. J Heart Lung Transplant. 2016;35:1170–84.
Hardy JD, Webb WR, Dalton ML Jr. Lung homotransplantations in man: report of the initial case. JAMA. 1963;18:1065–74.
Toronto Lung Transplant Group. Unilateral lung transplantation for pulmonary fibrosis. N Engl J Med. 1986;314:1140–5.
Liao WC, Hwang SL, Ko WJ, et al. Analysis of heart donation for cardiac transplantation at the National Taiwan university Hospital: fifteen-year cases review. Transplant Proc. 2004;36:2365–8.
Cameron EJ, Bellini A, Damian MS, et al. Confirmation of brainstem death. Pract Neurol. 2016;16:129–35.
Smith M. Physiologic changes during brain stem death – lessons for management of the organ donor. J Heart Lung Transplant. 2004;23:S217–22.
Dictus C, Vienenkoetter B, Esmaeilzadeh M, et al. Critical care management of potential organ donors: our current standard. Clin Transpl. 2009;23:2–9.
Faropoulos K, Apostolakis E. Brain death and its influence on the lungs of the donor: how is it prevented? Transplant Proc. 2009;41:4114–9.
Shutter L. Pathophysiology of brain death: what does the brain do and what is lost in brain death? J Crit Care. 2014;29:683–6.
Shemie SD, Ross H, Pagliarello J, et al. Organ donor management in Canada: recommendations of the forum on medical management to optimize donor organ potential. CMAJ. 2006;174:S13–32.
Grissom TE, Richards JE, Herr DL. Critical care management of the potential organ donor. Int Anesthesiol Clin. 2017;55:18–41.
Angel LF, Levine DJ, Restrepo MI, et al. Impact of a lung transplantation donor-management protocol on lung donation and recipient outcomes. Am J Respir Crit Care Med. 2006;174:710–6.
Mascia L, Pasero D, Slutsky AS, et al. Effect of a lung protective strategy for organ donors on eligibility and availability of lungs for transplantation: a randomized controlled trial. JAMA. 2010;304:2620–7.
Novitzky D, Mi Z, Videla LA, et al. Hormone resuscitation therapy for brain-dead donors: is insulin beneficial or detrimental? Clin Transpl. 2016;30:754–9.
Anderson TA, Bekker P, Vagefi PA. Anesthetic considerations in organ procurement surgery: a narrative review. Can J Anaesth. 2015;62:529–39.
Oto T, Griffiths AP, Rosenfeldt F, et al. Early outcomes comparing Perfadex, Euro-Collins and Papworth solutions in lung transplantation. Ann Thorac Surg. 2006;82:1842–8.
Latchana N, Peck JR, Whitson B, et al. Preservation solutions for cardiac and pulmonary donor grafts: a review of the current literature. J Thorac Dis. 2014;6:1143–9.
Van Raemdonck DE, Jannis NC, Rega FR, et al. Extended preservation of ischemic pulmonary graft function by postmortem alveolar expansion. Ann Thorac Surg. 1997;64:801–8.
Orens JB, Boehler A, de Perrot M, et al. A review of lung transplant donor acceptability criteria. J Heart Lung Transplant. 2003;22:1183–200.
Van Raemdonck D, Neyrinck A, Verleden GM, et al. Lung donor selection and management. Proc Am Thorac Soc. 2009;15:28–38.
Bittle GJ, Sanchez PG, Kon ZN, et al. The use of lung donors older than 55 years: a review of the UNOS database. J Heart Lung Transplant. 2013;32:760–8.
Mulligan MJ, Sanchez PG, Evans CF, et al. The use of extended criteria donors decreases one-year survival in high-risk lung recipients: a review of the UNOS database. J Thorac Cardiovasc Surg. 2016;152:891–8.
Botha P, Trivedi D, Weir CJ. Extended donor criteria in lung transplantation: impact on organ allocation. J Thorac Cardiovasc Surg. 2006;131:1154–60.
Van Raemdonck D, Rega FR, Neyrinck A, et al. Non-heart beating donors. Semin Cardiovasc Surg. 2004;16:309–21.
Oto T, Levvey B, McEgan R, et al. A practical approach to clinical lung transplantation from a Maastricht category III donor with cardiac death. J Heart Lung Transplant. 2007;26:196–9.
Wigfield C. Donation after cardiac death for lung transplantation: a review of current clinical practice. Curr Opin Organ Transplant. 2014;19:455–9.
Egan TM. Non-heart-beating donors in thoracic transplantation. J Heart Lung Transplant. 2004;23:3–10.
De Vleeschauwer SI, Wauters S, Dupont LJ, et al. Medium-term outcome after lung transplantation is comparable between brain-dead and cardiac-dead donors. J Heart Lung Transplant. 2011;30:975–81.
Steen S, Ingemansson R, Eriksson L, et al. First human transplantation of a nonacceptable donor lung after reconditioning ex vivo. Ann Thorac Surg. 2007;83:2191–4.
Sanchez PG, Bittle GJ, Burdorf L, et al. State of the art: clinical ex-vivo lung perfusion: rationale, current status, and future directions. J Heart Lung Transplant. 2012;31:339–48.
Van Raemdonck D, Neyrinck A, Cypel M, et al. Ex-vivo lung perfusion. Transplant Int. 2015;28:643–56.
Cypel M, Yeung JC, Machuca T, et al. Experience with the first 50 ex vivo lung perfusions in clinical transplantation. J Thorac Cardiovasc Surg. 2012;144:1200–6.
Wallinder A, Riise GC, Ricksen SE, et al. Transplantation after ex vivo lung perfusion: a midterm follow-up. J Heart Lung Transplant. 2016;35:1303–10.
Valenza F, Citerio G, Palleschi A, et al. Successful transplantation of lungs from an uncontrolled donor after circulatory death preserved in situ by alveolar recruitment maneuvers and assessed by ex vivo lung perfusion. Am J Transplant. 2016;16:1312–8.
Slama A, Schillab L, Barta M, et al. Standard donor lung procurement with normothermic ex vivo lung perfusion: a prospective randomized clinical trial. J Heart Lung Transplant. 2017;36:744–53.
Yeung JC, Krueger T, Yasufuku K, et al. Outcomes after transplantation of lungs preserved for more than 12h: a retrospective study. Lancet Respir Med. 2017;5:119–24.
Orens JB, Estenne M, Arcasoy S, et al. International guidelines for the selection of lung transplant candidates: 2006 update – a consensus report from the Pulmonary Scientific Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2006;25:745–55.
Shah PD, Orens JB. Guidelines for the selection of lung-transplant candidates. Curr Opin Organ Transplant. 2012;17:467–73.
Weill D, Benden C, Corris PA, et al. A consensus document for the selection of lung transplant candidates: 2104 – an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant. 2015;34:1–15.
Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:1005–12.
Van Agteren JE, Carson KV, Tiong LU, et al. Lung volume reduction surgery for diffuse emphysema. Cochrane Database Syst Rev. 2016;(10):CD001001.
Tutic M, Lardinois D, Imfeld S, et al. Lung-volume reduction surgery as an alternative or bridging procedure to lung transplantation. Ann Thorac Surg. 2006;82:208–13.
Morrell MR, Pilewski JM. Lung transplantation for cystic fibrosis. Clin Chest Med. 2016;37:127–38.
Egan TM, Murray S, Bustami RT, et al. Development of the lung allocation system in the United States. Am J Transplant. 2006;6:1212–27.
Egan TM, Edwards LB. Effect of the lung allocation score on lung transplantation in the United States. J Heart Lung Transplant. 2016;35:433–9.
Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology and the European Respiratory Society. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2009;30:2493–537.
Aigner C, Jaksch P, Taghavi S, et al. Pulmonary retransplantation: is it worth the effort? A long-term analysis of 46 cases. J Heart Lung Transplant. 2008;27:60–5.
Schumer EM, Rice JD, Kistler AM, et al. Single versus double lung retransplantation does not affect survival based on previous transplant type. Ann Thorac Surg. 2017;103:236–40.
Aigner C. Retransplantation. Curr Opin Organ Transplant. 2015;20:521–6.
Maurer JR, Frost AE, Estenne M, et al. International guidelines for the selection of lung transplant candidates. Transplantation. 1998;66:951–6.
Chiumello D, Coppola S, Froio S, et al. Extracorporeal life support as abridge to lung transplantation: a systematic review. Crit Care. 2015;19:19.
Rajagopal K, Hoeper MM. State of the art: bridging to lung transplantation using artificial organ support technologies. J Heart Lung Transplant. 2016;35:1385–98.
Lehr CJ, Zaas DW, Cheifetz IM. Ambulatory extracorporeal membrane oxygenation as a bridge to lung transplantation: walking while waiting. Chest. 2015;147:1213–8.
Myles PS. Aspects of anesthesia for lung transplantation. Semin Cardiothorac Vasc Anesth. 1998;2:140–54.
Jones RM, Enfield KB, Mehrad B, et al. Prevalence of obstructive coronary artery disease in patients undergoing lung transplantation: case series and review of the literature. Catheter Cardiovasc Interv. 2014;84:1–6.
Vizza CD, Lynch JP, Ochoa LL, et al. Right and left ventricular dysfunction in patients with severe pulmonary disease. Chest. 1998;113:576–83.
Koprivanac M, Budev MM, Yun JJ, et al. How important is coronary artery disease when considering lung transplant candidates? J Heart Lung Transplant. 2016;35:1453–61.
Choong CK, Meyers BF, Guthrie TJ, et al. Does the presence of preoperative mild or moderate coronary artery disease affect the outcomes of lung transplantation? Ann Thorac Surg. 2006;82:1038–42.
Hoechter DJ, von Dossow V. Lung transplantation: from the procedure to managing patients with lung transplantation. Curr Opin Anesthesiol. 2016;29:8–13.
Funk DJ, Moretti EW, Gan TJ. Minimally invasive cardiac output monitoring in the perioperative setting. Anesth Analg. 2009;108:887–97.
Missant C, Rex S, Wouters PF. Accuracy of cardiac output measurements with pulse contour analysis (PulseCO) and Doppler echocardiography during off-pump coronary artery bypass grafting. Eur J Anaesthesiol. 2008;25:243–8.
Sangkum L, Liu GL, Yu L, et al. Minimally invasive or noninvasive cardiac output measurement: an update. J Anesth. 2016;30:461–80.
Rudnick MR, Marchi LD, Plotkin JS. Hemodynamic monitoring during liver transplantation: a state of the art review. World J Hepatol. 2015;7:1302–11.
Conacher ID, Paes ML. Mixed venous oxygen saturation during lung transplantation. J Cardiothorac Vasc Anesth. 1994;8:671–4.
Shepherd SJ, Pearse RM. Role of central and mixed venous oxygen saturation measurement in perioperative care. Anesthesiology. 2009;111:649–56.
Murkin JM, Adams SJ, Novick RJ, et al. Monitoring brain oxygen saturation during coronary bypass surgery: a randomized, prospective study. Anesth Analg. 2007;104:51–8.
Harilall Y, Adam JK, Biccard BM, et al. The effect of optimising cerebral tissue oxygen saturation on markers of neurological injury during coronary artery bypass graft surgery. Heart Lung Circ. 2014;23:68–74.
Myles PS, Leslie K, McNeil J, et al. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet. 2004;363:1757–63.
De Smet T, Struys MM, Neckebroek MM, et al. The accuracy and clinical feasibility of a new bayesian-based closed-loop control system for propofol administration using the bispectral index as a controlled variable. Anesth Analg. 2008;107:1200–10.
NICE clinical guideline 65: inadvertent perioperative hypothermia. https://www.nice.org.uk/guidance/cg65. Accessed 14 April 2017.
Sessler DI. Perioperative thermoregulation and heat balance. Lancet. 2016;387:2655–64.
Flachskampf FA, Badano L, Daniel WG, et al. Recommendations for transoesophageal echocardiography: update 2010. Eur J Echocardiogr. 2010;11:557–76.
American Society of Anesthesiologists and Society of Cardiovascular Anesthesiologists Task Force on Transesophageal Echocardiography. Practice guidelines for perioperative transesophageal echocardiography. Anesthesiology. 2010;112:1084–96.
Sullivan B, Puskas F, Fernandez-Bustamante A. Transesophageal echocardiography in noncardiac thoracic surgery. Anesthesiol Clin. 2012;30:657–69.
Evans A, Dwarakanath S, Hogue C, et al. Intraoperative echocardiography for patients undergoing lung transplantation. Anesth Analg. 2014;118:725–30.
Della Rocca G, Brondani A, Costa MG. Intraoperative hemodynamic monitoring during organ transplantation: what is new? Curr Opin Organ Transplant. 2009;14:291–6.
Tan TC, Dudzinski DM, Hung J, et al. Peri-operative assessment of right heart function: role of echocardiography. Eur J Clin Investig. 2015;45:755–66.
Ashes C, Roscoe A. Transesophageal echocardiography in thoracic anesthesia: pulmonary hypertension and right ventricular function. Curr Opin Anesthesiol. 2015;28:38–44.
Miyaji K, Nakamura K, Maruo T, et al. Effect of a kink in unilateral pulmonary artery anastomosis on velocities of blood flow through bilateral pulmonary vein anastomoses in living-donor lobar lung transplantation. J Am Soc Echocardiogr. 2004;17:998–9.
Cartwright BL, Jackson A, Cooper J. Intraoperative pulmonary vein examination by transesophageal echocardiography: an anatomic update and review of utility. J Cardiothorac Vasc Anesth. 2013;27:111–20.
Felton ML, Michel-Cherqui M, Sage E, et al. Transesophageal and contact ultrasound echographic assessments of pulmonary vessels in bilateral lung transplantation. Ann Thorac Surg. 2012;93:1094–100.
Shaikh N, Saif AS, Nayeemuddin M, et al. Patent foramen ovale: its significance in anesthesia and intensive care: an illustrated case. Anesth Essays Res. 2012;6:94–7.
Subramaniam K, Esper SA. Role of transesophageal echocardiography in perioperative patient management of lung transplantation surgery. J Perioper Echocardiogr. 2013;1:48–56.
Doufle G, Roscoe A, Billia F, et al. Echocardiography for adult patients supported with extracorporeal membrane oxygenation. Crit Care. 2015;19:326.
Hohn L, Schweizer A, Morel DR, et al. Circulatory failure after anesthesia induction in a patient with severe primary pulmonary hypertension. Anesthesiology. 1999;91:1943–5.
Manthous CA. Avoiding circulatory complications during endotracheal intubation and initiation of positive pressure ventilation. J Emerg Med. 2009;38(5):622–31.
Schisler T, Marquez JM, Hilmi I, et al. Pulmonary hypertensive crisis on induction of anesthesia. Sem Cardiothorac Vasc Anesth. 2017;21:105–13.
Conacher ID. Anaesthesia for the surgery of emphysema. Br J Anaesth. 1997;79:530–8.
Quinlan JJ, Buffington CW. Deliberate hypoventilation in a patient with air trapping during lung transplantation. Anesthesiology. 1993;78:1177–81.
Myles PS, Ryder IG, Weeks AM, et al. Diagnosis and management of dynamic hyperinflation during lung transplantation. J Cardiothorac Vasc Anesth. 1997;11:100–4.
Petrucci N, De Feo C. Lung protective ventilation strategy for the acute respiratory distress syndrome. Cochrane Database Syst Rev. 2013;(2):CD003844.
Papiris SA, Manali ED, Kolilekas L, et al. Clinical review: idiopathic pulmonary fibrosis acute exacerbations − unravelling Ariadne’s thread. Crit Care. 2010;14:246.
Hosseinian L. Pulmonary hypertension and noncardiac surgery: implications for the anesthesiologist. J Cardiothorac Vasc Anesth. 2014;28:1064–74.
Snell GI, Salamonsen RF, Bergin P, et al. Inhaled nitric oxide as a bridge to heart-lung transplantation in a patient with end-stage pulmonary hypertension. Am J Respir Crit Care Med. 1995;151:1263–6.
de Boer WJ, Waterbolk TW, Brugemann J, et al. Extracorporeal membrane oxygenation before induction of anesthesia in critically ill thoracic transplant patients. Ann Thorac Surg. 2001;72:1407–8.
Scheller MS, Kriett JM, Smith CM, et al. Airway management during anesthesia for double-lung transplantation using a single-lumen endotracheal tube with an enclosed bronchial blocker. J Cardiovasc Thorac Anesth. 1992;6:204–7.
Campos JH. Which device should be considered the best for lung isolation: double-lumen endotracheal tube versus bronchial blockers. Curr Opin Anaesthesiol. 2007;20:27–31.
Conway SP, Brownlee KG, Denton M, et al. Antibiotic treatment of multidrug-resistant organisms in cystic fibrosis. Am J Respir Med. 2003;2:321–32.
Haja Mydin H, Corris PA, Nicholson A, et al. Targeted antibiotic prophylaxis for lung transplantation in cystic fibrosis patients colonized with Pseudomonas aeruginosa using multiple combination bactericidal testing. J Transp Secur. 2012;2012:135738.
Pruszkowski O, Dalibon N, Moutafis M, et al. Effects of propofol vs sevoflurane on arterial oxygenation during one-lung ventilation. Br J Anaesth. 2007;98:539–44.
Módolo NS, Módolo MP, Marton MA, et al. Intravenous versus inhalation anaesthesia for one-lung ventilation. Cochrane Database Syst Rev. 2013;(7):CD006313.
Schulte-Sasse U, Hess W, Tarnow J. Pulmonary vascular responses to nitrous oxide in patients with normal and high pulmonary vascular resistance. Anesthesiology. 1982;57:9–13.
Awori Hayanga JW, D’Cunha J. The surgical technique of bilateral sequential lung transplantation. J Thorac Dis. 2014;6:1063–9.
Kim KN, Kim DW, Jeong MA. Comparison of pressure-controlled ventilation with volume-controlled ventilation during one-lung ventilation: a systematic review and meta-analysis. BMC Anesthesiol. 2016;16:72.
Pardos PC, Garutti I, Pineiro P, et al. Effects of ventilatory mode during one-lung ventilation on intraoperative and postoperative arterial oxygenation in thoracic surgery. J Cardiothorac Vasc Anesth. 2009;23:770–4.
Bittner HB, Binner C, Lehmann S, et al. Replacing cardiopulmonary bypass with extracorporeal membrane oxygenation in lung transplantation operations. Eur J Cardiothorac Surg. 2007;31:462–7.
McIlroy DR, Pilcher DV, Snell GI. Does anaesthetic management affect early outcomes after lung transplant? An exploratory analysis. Br J Anaesth. 2009;102:506–14.
Geube MA, Perez-Protto SE, McGrath TL, et al. Increased intraoperative fluid administration is associated with severe primary graft dysfunction after lung transplantation. Anesth Analg. 2016;122:1081–8.
Feltracco P, Serra E, Barbieri F, et al. Anesthetic considerations in lung transplantation for severe pulmonary hypertension. Transplant Proc. 2007;39:1976–80.
Triantafillou AN, Pasque MK, Huddleston CB, et al. Predictors, frequency and indications for cardiopulmonary bypass during lung transplantation in adults. Ann Thorac Surg. 1994;57:1248–51.
Wright BJ. Inhaled pulmonary vasodilators in refractory hypoxemia. Clin Exp Emerg Med. 2015;2:184–7.
Rocca GD, Passariello M, Coccia C, et al. Inhaled nitric oxide administration during one-lung ventilation in patients undergoing thoracic surgery. J Cardiothorac Vasc Anesth. 2001;15:218–23.
Muzaffar S, Shukla N, Angelini GD, et al. Inhaled prostacyclin is safe, effective and affordable in patients with pulmonary hypertension, right-heart dysfunction, and refractory hypoxemia after cardiothoracic surgery. J Thorac Cardiovasc Surg. 2004;128:949–50.
Ventetuolo CE, Klinger JR. Management of acute right ventricular failure in the intensive care unit. Ann Am Thorac Soc. 2014;11:811–22.
Forrest P. Anaesthesia and right ventricular failure. Anaesth Intensive Care. 2009;37:370–85.
Vachiery JL, Huez S, Gillies H, et al. Safety, tolerability and pharmacokinetics of an intravenous bolus of sildenafil in patients with pulmonary arterial hypertension. Br J Pharmacol. 2011;71:289–92.
Price LC, Wort SJ, Finney SJ, et al. Pulmonary vascular and right ventricular dysfunction in adult critical care: current and emerging options for management: a systematic literature review. Crit Care. 2010;14:R169.
Harjola VP, Mebazaa A, Celutkiene J, et al. Contemporary management of acute right ventricular failure: a statement from the Heart Failure Association and the Working Group on Pulmonary Circulation and Right Ventricular Function of the European Society of Cardiology. Eur J Heart Fail. 2016;18:226–41.
Kerbaul F, Gariboldi V, Giorgi R, et al. Effects of levosimendan on acute pulmonary embolism-induced right ventricular failure. Crit Care Med. 2007;35:1948–54.
Nagendran M, Maruthappu M, Sugand K. Should double lung transplant be performed with or without cardiopulmonary bypass? Interact Cardiovasc Thorac Surg. 2011;12:799–804.
Yu WS, Paik HC, Haam SJ, et al. Transition to routine use of venoarterial extracorporeal oxygenation during lung transplantation could improve early outcomes. J Thorac Dis. 2016;8:1712–20.
Ius F, Sommer W, Tudorache I, et al. Five-year experience with intraoperative extracorporeal membrane oxygenation in lung transplantation: indications and midterm results. J Heart Lung Transplant. 2016;35:49–58.
Odell DD, D’Cunha J, Shigemura N, et al. Intraoperative extracorporeal membrane oxygenation as an alternative to cardiopulmonary bypass in lung transplantation. J Heart Lung Transplant. 2013;32:S167–8.
Pavlushkov E, Berman M, Valchanov K. Cannulation techniques for extracorporeal life support. Ann Transl Med. 2017;5:70.
Salman J, Ius F, Sommer W, et al. Mid-term results of bilateral lung transplant with postoperatively extended intraoperative extracorporeal membrane oxygenation for severe pulmonary hypertension. Eur J Cardiothorac Surg. 2017;52:163–70.
Chung M, Shiloh AL, Carlese A. Monitoring of the adult patient on venoarterial extracorporeal membrane oxygenation. ScientificWorldJournal. 2014;2014:393258.
Rupprecht L, Lunz D, Philipp A, et al. Pitfalls in percutaneous ECMO cannulation. Heart Lung Vessel. 2015;7:320–6.
Sidebotham D, Allen SJ, McGeorge A, et al. Venovenous extracorporeal membrane oxygenation in adults: practical aspects of circuits, cannulae, and procedures. J Cardiothorac Vasc Anesth. 2012;26:893–909.
Reis Miranda D, van Thiel R, Brodie D, et al. Right ventricular unloading after initiation of venovenous extracorporeal membrane oxygenation. Am J Respir Crit Care Med. 2015;191:346–8.
Mohite PN, Sabashnikov A, Patil NP, et al. The role of cardiopulmonary bypass in lung transplantation. Clin Transpl. 2016;30:202–9.
Machuca TN, Collaud S, Mercier O, et al. Outcomes of intraoperative extracorporeal membrane oxygenation versus cardiopulmonary bypass for lung transplantation. J Thorac Cardiovasc Surg. 2015;149:1152–7.
Bermudez CA, Shiose A, Esper SA, et al. Outcomes of intraoperative venoarterial extracorporeal membrane oxygenation versus cardiopulmonary bypass during lung transplantation. Ann Thorac Surg. 2014;98:1936–42.
Diamond JM, Lee JC, Kawut SM, et al. Clinical risk factors for primary graft dysfunction after lung transplantation. Am J Respir Crit Care Med. 2013;187:527–34.
Hoechter DJ, Shen YM, Kammerer T, et al. Extracorporeal circulation during lung transplantation procedures: a meta-analysis. ASAIO J. 2017;63:551–61.
Castillo M. Anesthetic management for lung transplantation. Curr Opin Anaesthesiol. 2011;24:32–6.
Shaver CM, Ware LB. Primary graft dysfunction: pathophysiology to guide new preventive therapies. Expert Rev Respir Med. 2017;11:119–28.
Silva CA, Carvalho RS, Cagido VR, et al. Influence of lung mechanical properties and alveolar architecture on the pathogenesis of ischemia-reperfusion injury. Interact Cardiovasc Thorac Surg. 2010;11:46–51.
DeCampos KN, Keshavjee S, Slutsky AS, et al. Alveolar recruitment prevents rapid-reperfusion-induced injury of lung transplants. J Heart Lung Transplant. 1999;18:1096–102.
Singh RR, Laubach VE, Ellman PI, et al. Attenuation of lung reperfusion injury by modified ventilation and reperfusion techniques. J Heart Lung Transplant. 2006;25:1467–73.
Porteous MK, Diamond JM, Christie JD. Primary graft dysfunction: lessons leaned about the first 72h after lung transplantation. Curr Opin Organ Transplant. 2015;20:506–14.
Della Rocca G, Pierconti F, Costa MG, et al. Severe reperfusion lung injury after lung transplantation. Crit Care. 2002;6:240–4.
Tavare AN, Tsakok T. Does prophylactic inhaled nitric oxide reduce morbidity and mortality after lung transplantation? Interact Cardiovasc Thorac Surg. 2011;13:516–20.
Pasero D, Martin EL, Davi A, et al. The effects of inhaled nitric oxide after lung transplantation. Minerva Anestesiol. 2010;76:353–61.
Hsu HH, Ko WJ, Chen JS, et al. Extracorporeal membrane oxygenation in pulmonary crisis and primary graft dysfunction. J Heart Lung Transplant. 2008;27:233–7.
Fischer S, Bohn D, Rycus P, et al. Extracorporeal membrane oxygenation for primary graft dysfunction after lung transplantation: analysis of the Extracorporeal Life Support Organization (ELSO) registry. J Heart Lung Transplant. 2007;26:472–7.
Pottecher J, Falcoz PE, Massard G, et al. Does thoracic epidural analgesia improve outcome after lung transplantation? Interact Cardiovasc Thorac Surg. 2011;12:51–3.
Feltracco P, Barbieri S, Milevoj M, et al. Thoracic epidural analgesia in lung transplantation. Transplant Proc. 2010;42:1265–9.
Yeung JH, Gates S, Naidu BV, et al. Paravertebral block versus thoracic epidural for patients undergoing thoracotomy. Cochrane Database Syst Rev. 2016;(2):CD009121.
Jouguelet-Lacoste J, La Colla L, Schilling D, et al. The use of intravenous infusion or single dose of low-dose ketamine for postoperative analgesia: a review of the current literature. Pain Med. 2015;16:383–403.
Laskowski K, Stirling A, McKay WP, et al. A systematic review of intravenous ketamine for postoperative analgesia. Can J Anaesth. 2011;58:911–23.
Scheffert JL, Raza K. Immunosuppression in lung transplantation. J Thorac Dis. 2014;6:1039–53.
Augoustides JG, Watcha SM, Pochettino A, et al. Early tracheal extubation in adults undergoing single-lung transplantation for chronic obstructive pulmonary disease: pilot evaluation of perioperative outcome. Interact Cardiovasc Thorac Surg. 2008;7:755–8.
Felten ML, Moyer JD, Dreyfus JF, et al. Immediate postoperative extubation in bilateral lung transplantation: predictive factors and outcome. Br J Anaesth. 2016;116:847–54.
Rocca GD, Coccia C, Costa GM, et al. Is very early extubation after lung transplantation feasible? J Cardiothorac Vasc Anesth. 2003;17:29–35.
Thakuria L, Davey R, Romano R, et al. Mechanical ventilation after lung transplantation. J Crit Care. 2016 Feb;31(1):110–8.
Mitchell JB, Shaw AD, Donald S, et al. Differential lung ventilation after single-lung transplantation for emphysema. J Cardiothorac Vasc Anesth. 2002;16:459–62.
Fuehner T, Kuehn C, Welte T, et al. ICU care before and after lung transplantation. Chest. 2016;150:442–50.
Pilarczyk K, Carstens H, Heckmann J, et al. Safety and efficiency of percutaneous dilatational tracheostomy with direct bronchoscopic guidance for thoracic transplant recipients. Respir Care. 2016;61:235–42.
Najafizadeh K, Daneshvar A, Dezfouli AA, et al. Pulmonary artery stenosis shortly after lung transplantation: successful balloon dilation and stent insertion in one case. Ann Transplant. 2009;14:52–5.
Yserbyt J, Dooms C, Vos R, et al. Anastomotic airway complications after lung transplantation: risk factors, treatment modalities and outcome – a single-centre experience. Eur J Cardiothorac Surg. 2016;49:e1–8.
Yun JH, Lee SO, Jo KW, et al. Infections after lung transplantation: time of occurrence, sites, and microbiologic etiologies. Korean J Intern Med. 2015;30:506–14.
Parada MT, Alba A, Sepúlveda C. Early and late infections in lung transplantation patients. Transplant Proc. 2010;42:333–5.
Raghavan D, Gao A. Ahn C, et al Contemporary analysis of incidence of post-operative atrial fibrillation, its predictors, and association with clinical outcomes in lung transplantation. J Heart Lung Transplant. 2015;34:563–70.
Jacques F, El-Hamamsy I, Fortier A, et al. Acute renal failure following lung transplantation: risk factors, mortality and long-term consequences. Eur J Cardiothorac Surg. 2012;41:193–9.
Evans CF, Iacono AT, Sanchez PG, et al. Venous thromboembolic complications of lung transplantation: a contemporary single-institution review. Ann Thorac Surg. 2015;100:2033–9.
Chan EG, Bianco V III, Richards T, et al. The ripple effect of a complication in lung transplantation: evidence for increased long-term survival. J Thorac Cardiovasc Surg. 2016;151:1171–80.
Sweet SC. Induction therapy in lung transplantation. Transpl Int. 2013;26:696–703.
Tabarelli W, Bonatti H, Tabarelli D, et al. Long term complications following 54 consecutive lung transplants. J Thorac Dis. 2016;8:1234–44.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Clinical Case Discussion
Clinical Case Discussion
Case Presentation
A 52-year-old male with mixed interstitial lung disease/COPD presents for right single-lung transplantation via right thoracotomy and left hemidiaphragm plication. He requires supplemental oxygen at 3 lpm at rest and 10 lpm with exertion. He has a 40-pack-year smoking history and quit 5 years ago. His history is notable for five-vessel coronary artery bypass graft 8 years ago and endovascular repair of an abdominal aortic aneurysm 5 years ago. As a teenager, he suffered a traumatic injury to his left neck, resulting in left vocal cord and hemidiaphragm paralysis.
His preoperative medication list includes albuterol, atorvastatin, azithromycin, gabapentin, metoprolol, omeprazole, sertraline, and sildenafil. He has no medication allergies.
The patient’s preoperative workup reveals the following information:
-
Weight: 87 kg, Height: 176 cm, Heart rate: 80 bpm, Blood pressure: 108/70 mmHg Temperature: 37.0 °C, SpO2: 97% on 3 L nasal cannulae
-
ECG: normal sinus rhythm with occasional premature ventricular contractions, left ventricular hypertrophy
-
Hemoglobin: 13.7 g/dL, hematocrit: 42.3%, white blood cell count: 10 x109/L, platelets 229 × 109/L
-
Na+: 138 mmol/L, K+: 4.1 mmol/L, Cl-: 103 mmol/L, CO2: 28 mmol/L, BUN 20 mg/dL, Cr 0.8 mg/dL, Glucose 103 mg/dL, INR 1.0
-
Arterial blood gas on room air: pH 7.37, pCO2 49 mmHg, pO2 59 mmHg, bicarbonate 28 mmol/L, base excess 2 mmol/L
-
FEV1 51% predicted, FVC 59% predicted, FEV1/FVC 86
-
Ventilation/perfusion scan: differential perfusion is 46% to left lung, 54% to right lung
-
Transthoracic echocardiogram: left ventricular ejection fraction 50% with inferior hypokinesis, normal right ventricular systolic function, trivial tricuspid regurgitation
-
Left heart catheterization: significant native vessel coronary artery disease, all grafts patent
-
Right heart catheterization: pulmonary artery (PA) pressure 52/14 mmHg (mean 28), pulmonary vascular resistance 2.4 Wood units, cardiac index 2.6 L/min-m2, pulmonary capillary wedge pressure 9 mmHg
-
Preoperative imaging studies are shown in Figs. 47.7 and 47.8.

Preoperative upright posterior-anterior chest X-ray. Notable findings include left hemidiaphragm elevation, changes consistent with post median sternotomy and CABG, and aortic stent graft within the abdomen

Coronal slice from preoperative computed tomography (CT) scan of the chest. Notable findings are left hemidiaphragm elevation with volume loss in the left hemithorax, right lung hyperinflation, and paraseptal emphysema in the bilateral lung apices
Questions
-
1.
Would you insert a central line and/or pulmonary artery catheter prior to the induction of anesthesia? Does the laterality of central line insertion matter?
-
2.
How would you induce anesthesia in this patient?
-
3.
How would you secure the airway?
-
4.
How would your anesthetic considerations differ if the patient had:
-
(a)
Cystic fibrosis?
-
(b)
COPD?
-
(c)
Primary pulmonary hypertension?
-
(a)
-
5.
Can this transplant be done without cardiopulmonary bypass (CPB) or extracorporeal membrane oxygenation (ECMO)?
Case Continuation
After the induction of anesthesia, intubation with a left-sided double-lumen tube, and insertion of all invasive monitors and a TEE probe, lung isolation is achieved, and one-lung ventilation (OLV) is established. After 30 min of dissection and OLV, the patient remains hemodynamically stable, but the SpO2 has decreased to 85% on 100% inspired oxygen, and the arterial blood gas now reads pH 7.21, pCO2 68 mmHg, pO2 51 mmHg, bicarbonate 22 mmol/L, and base excess −2 mmol/L.
Questions
-
6.
How will you manage OLV?
-
7.
How will you address the hypoxemia that has developed during OLV? What degree of hypoxemia and/or hypercarbia will you tolerate?
Case Continuation
In preparation for explant of the native right lung, the surgeon clamps the right PA. After clamping, the vitals are heart rate 90 bpm, blood pressure 129/74 mmHg, central venous pressure 10 mmHg, PA pressure 46/17 (mean 29) mmHg, and SpO2 99%.
The right lung is explanted. Then the right donor lung is implanted and reperfused, during which time there is severe hemodynamic instability.
Questions
-
8.
How would you expect pulmonary arterial pressures to change with clamping of the left PA?
-
9.
What has caused the hemodynamic instability?
Case Continuation
The donor (right) lung is now ventilated. Soon after, frank pulmonary edema is seen coming from the tracheal (right) lumen of the double-lumen tube.
Questions
-
10.
How would you ventilate the donor lung?
-
11.
Transesophageal echocardiography pulse-wave Doppler evaluation of the right pulmonary veins reveals a peak velocity of 110 cm/s. How would you advise the surgeon?
-
12.
What is the reason for the development of pulmonary edema?
Discussion
-
Question 1: Would you insert a central line and/or pulmonary artery catheter prior to the induction of anesthesia? Does the laterality of central line insertion matter?
This patient does not have significant pulmonary hypertension; thus, the preinduction insertion of a pulmonary artery catheter (PAC) is not required. However, in a patient with significant pulmonary hypertension, the preinduction insertion of a PAC allows for precise hemodynamic management during induction of anesthesia. Central access also offers the advantage of allowing for the use of inotrope infusions (e.g., epinephrine) to support the right ventricle, although this central access is not necessarily required for temporary infusions. Of note, many lung transplant patients will not be able to tolerate preinduction central line/PAC insertion because they may not tolerate Trendelenburg or even supine positioning. Importantly, extreme caution must be taken in administering sedation to lung transplant recipients who often have tenuous respiratory status. The potential exacerbation of baseline hypercapnia or hypoxemia with sedation may precipitate an acute increase in pulmonary vascular resistance and subsequent right ventricular dysfunction/failure with cardiovascular collapse.
If the patient’s pulmonary arterial pressures are approaching or even supra-systemic, it may be prudent to consider preinduction cannulation of the femoral vessels under local anesthesia for either preemptive or emergent institution of ECMO/CPB. Our practice is to typically place the central line and PAC via the left internal jugular vein under ultrasound guidance; this leaves the right internal jugular vein accessible should circulatory support (e.g., ECMO) be required during or after the transplant procedure. In this patient, vascular access in the left neck may be complicated by his previous injury.
-
Question 2: How would you induce anesthesia in this patient?
The induction of anesthesia in lung transplant recipients should focus on extreme attention to hemodynamic stability and management of pulmonary hypertension as well as rapid securement of the airway. With regard to the management of pulmonary hypertension, it is paramount to avoid significant decreases in systemic vascular resistance that will reduce right ventricular perfusion, thus compromising RV function. One must also limit any increase in pulmonary vascular resistance by avoiding hypoxemia, hypercarbia, acidosis, and “light” anesthesia during laryngoscopy and intubation. A preinduction arterial catheter is mandatory for beat-to-beat blood pressure monitoring, and a cardiac-style induction relying primarily on narcotics and benzodiazepines often provides the desired hemodynamic stability. Although rapid securement of the airway is desirable, conventional rapid sequence induction techniques may not be tolerated in patients with RV dysfunction. Despite the potential for adrenocortical suppression, some practitioners select etomidate as part of a rapid sequence induction in combination with succinylcholine. Regardless of the drugs selected for induction, vasoconstrictors and inotropes should be readily available for hemodynamic support and resuscitation. Inotropes without systemic vasodilatory effects are preferred. Careful preoperative assessment of the airway and contingency planning for difficult airway access are prudent, as these patients may not tolerate prolonged periods of apnea. Given the left hemidiaphragm paralysis in this patient, with resultant low lung volumes on the left, this patient may experience more rapid desaturation during induction than might be predicted from his lung disease. Furthermore, this patient is only undergoing single-lung transplantation; therefore, precautions against aspiration, which could compromise the remaining native lung, should be taken.
-
Question 3: How would you secure the airway?
In the vast majority of lung transplant patients, a left-sided double-lumen endotracheal tube (ETT) placed with bronchoscopic guidance is typically used. Patients with a suppurative pathology (e.g., cystic fibrosis) will benefit from initial insertion of a single-lumen ETT to allow for pulmonary toilet via bronchoscopy. This will mostly likely improve oxygenation during one-lung ventilation.
Bronchial blockers to achieve lung isolation are more prone to movement within the airway during manipulation of the hilum and do not allow for effective suctioning, the application of continuous positive airway pressure (CPAP) to the non-ventilated lung, or differential ventilation of the two lungs.
-
Question 4: How would your anesthetic considerations differ if the patient had:
-
(a)
Cystic fibrosis?
-
(b)
COPD?
-
(c)
Primary pulmonary hypertension?
-
(a)
The leading indications for lung transplantation today are pulmonary fibrosis, COPD, and cystic fibrosis. The underlying pathology impacts the surgical procedure as well as the anesthetic considerations. For example, patients with fibrosis often receive single-lung transplants, while patients with cystic fibrosis always require a double-lung transplant.
Induction techniques are similar for all pathologies and reflect consideration of pulmonary artery pressures and underlying right ventricular function, as described above.
Ventilation strategies, on the other hand, should be tailored to the underlying pulmonary pathology. Patients with pulmonary fibrosis have low lung compliance and are at risk for barotrauma associated with mechanical ventilation. Pressure control ventilation may be preferable to volume control ventilation to decrease the airway pressure transmitted to the lungs. Patients with obstructive lung disease, such as COPD or cystic fibrosis, are prone to air trapping and dynamic hyperinflation (see question 6).
Patients such as this one who receive single-lung transplants may have a significant imbalance in pulmonary compliance between the native lung and the transplanted lung, requiring differential lung ventilation via a double-lumen ETT.
-
Question 5: Can this transplant be done without cardiopulmonary bypass (CPB) or extracorporeal membrane oxygenation (ECMO)?
Cardiopulmonary bypass (CPB) offers the advantage of improved hemodynamic stability and systemic oxygenation during lung transplantation. However, CPB has many disadvantages, including bleeding related to full heparinization and coagulopathy, increased use of blood products, increased crystalloid administration, inflammation, and possible damage to other organs. Nonetheless, patients with intractable hypoxemia during one-lung ventilation or RV dysfunction causing hemodynamic compromise may require ECMO or CPB to safely complete the procedure. ECMO is often preferred over CPB because it allows for less heparinization and can be easily extended into the postoperative period if required.
-
Question 6: How will you manage OLV?
Concerns during OLV before transplant include hypoxemia, hypercarbia, dynamic hyperinflation (in cases of obstructive lung disease), and excessively high airway pressures (which may precipitate RV failure). To address dynamic hyperinflation, ventilation should focus on permissive hypercapnia with reduced tidal volume, lower respiratory rate, elimination of positive end-expiratory pressure (PEEP), and adjustments to inspiratory/expiratory (I:E) ratio to favor exhalation. Elevated airway pressures can be ameliorated through reduced tidal volumes, higher respiratory rate, and adjustment of the ventilator I:E ratio.
-
Question 7: How will you address the hypoxemia that has developed during OLV? What degree of hypoxemia and/or hypercarbia will you tolerate?
Hypoxemia during one-lung ventilation (OLV) can be treated with either continuous positive airway pressure (5–10 cmH2O) to the non-ventilated lung to oxygenate the shunt fraction or with PEEP (5–10 cmH2O) to the ventilated lung to minimize atelectasis. Of note, PEEP can potentially reduce venous return to the heart, impair hypoxic pulmonary vasoconstriction, and elevate pulmonary vascular resistance. Definitive treatment of hypoxemia due to shunt during OLV is achieved with surgical clamping of the PA to the non-ventilated lung. Hypoxic pulmonary vasoconstriction may be improved by reducing inhaled volatile anesthetic concentration or utilizing TIVA only and by avoiding IV vasodilators (e.g., nitroglycerin). If intractable hypoxemia occurs despite the above maneuvers and utilization of 100% inspired oxygen, ECMO or CPB may be required.
Management of arterial blood gas values should target the patient’s baseline values prior to induction of anesthesia. While some degree of permissive hypercarbia may be necessary to achieve adequate oxygenation, severe hypercarbia, hypoxemia, or acidosis that produce hemodynamic instability are indications for ECMO or CBP.
-
Question 8: How would you expect pulmonary arterial pressures to change with clamping of the left PA?
It is reasonable to expect a rise in the PA pressure after surgical clamping of either pulmonary artery because the entire cardiac output is now passing through the contralateral lung. This PA pressure increase may be variable depending on the degree of baseline perfusion through the native lung (reference the preoperative ventilation/perfusion lung scan). While a lack of increase in PA pressure with PA clamping may seem reassuring, the anesthesiologist should always be vigilant about the possibility of worsening of RV function.
-
Question 9: What has caused the hemodynamic instability?
Possible causes of hemodynamic instability in this scenario include worsening of RV function, worsening of LV function due to ischemia in this patient with significant coronary disease, and air embolism occurring during reperfusion of the transplanted lung. The best tool for monitoring cardiac function and for diagnosing the cause of intraoperative hemodynamic instability is transesophageal echocardiography (TEE). TEE will be able to differentiate between these scenarios and allow for determination of the cause of hemodynamic instability.
-
Question 10: How would you ventilate the donor lung?
Goals for the management of any newly transplanted lung include the avoidance of atelectasis, hyperoxia, and barotrauma, which can rapidly cause pulmonary edema. During double-lung transplantation, a particularly vulnerable period occurs between the first and second implant when the newly reperfused first lung must tolerate twice the normal blood flow (i.e., the full cardiac output). Single-lung transplants are vulnerable to differences in compliance between the newly implanted lung and the remaining native lung. Institutional perioperative standardized practices for ventilation of the newly transplanted lung are common for goal PEEP (e.g., 8 mmHg), preferred oxygen levels (e.g., room air or the lowest inspired oxygen concentration to maintain SpO2 above 90%), and peak inspiratory pressure (e.g., less than 30 mmHg). At our institution, inhaled nitric oxide (iNO) or inhaled epoprostenol are routinely administered to reduce pulmonary artery pressure and support RV function, although the benefits in lung transplantation are controversial.
-
Question 11: TEE pulse-wave Doppler evaluation of the R pulmonary veins reveals a peak velocity of 110 cm/s. How would you advise the surgeon?
Pre-procedure and post-procedure TEE evaluation provides invaluable information to assist with anesthetic management and to aide in diagnosing surgical complications. Pre-procedure evaluation should focus on RV and LV function, the identification and quantification of any valvular lesions or intracardiac shunts (e.g., PFO), and an assessment of baseline pulmonary vein velocities and pulmonary artery size.
Post-transplant TEE should again evaluate RV and LV function. Most importantly, following reperfusion there should be a careful assessment of the right and left pulmonary arteries and all four pulmonary veins (if possible), including:
-
Assessment of the diameter of pulmonary artery and pulmonary vein anastomoses, if visible
-
Color flow Doppler evaluation of pulmonary artery anastomoses, if visible
-
Color flow Doppler evaluation of pulmonary vein flows and pulsed-wave Doppler determination of pulmonary vein velocities
In general, anastomoses >0.5 cm in diameter and pulmonary vein pulse-wave Doppler peak systolic velocities ≤100 cm/s are acceptable. Although few specific guidelines exist, peak systolic velocities >100–170 cm/s are worrisome for obstruction (kinked or narrow anastomoses) and should prompt discussion with the surgical team before chest closure.
-
Question 12: What is the reason for the development of pulmonary edema?
Reperfusion injury typically presents with poor oxygenation, high PA pressures, and pulmonary edema. It is important to exclude a mechanical cause, such as pulmonary vein or arterial anastomotic stenosis or kinking (best evaluated via TEE, as described above). Otherwise, protective lung ventilation strategies should be employed. Inhaled pulmonary vasodilators can help to reduce the inspired oxygen concentration in patients with high oxygen requirements. Ultimately, significant reperfusion injury or primary graft dysfunction may necessitate the use of ECMO.
Rights and permissions
Copyright information
© 2019 Springer Nature Switzerland AG
About this chapter

Cite this chapter
Roscoe, A., Klinger, R.Y. (2019). Lung Transplantation. In: Slinger, P. (eds) Principles and Practice of Anesthesia for Thoracic Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-00859-8_47
Download citation
DOI: https://doi.org/10.1007/978-3-030-00859-8_47
Published:
Publisher Name: Springer, Cham
Print ISBN: 978-3-030-00858-1
Online ISBN: 978-3-030-00859-8
eBook Packages: MedicineMedicine (R0)