
Abstract
Catecholaminergic polymorphic ventricular tachycardia (CPVT) is a highly malignant inherited arrhythmia syndrome, characterized by bidirectional or polymorphic ventricular tachycardia (VT) and ventricular fibrillation (VF) during physical or emotional stress in structurally normal hearts. This disease is illustrative of the progress that has been made in the field of cardiogenetics in the last decennia.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
- Ventricular Tachycardia
- Sarcoplasmic Reticulum
- Polymorphic Ventricular Tachycardia
- Ventricular Ectopy
- Catecholaminergic Polymorphic Ventricular Tachycardia
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
1 Introduction
Catecholaminergic polymorphic ventricular tachycardia (CPVT) is a highly malignant inherited arrhythmia syndrome, characterized by bidirectional or polymorphic ventricular tachycardia (VT) and ventricular fibrillation (VF) during physical or emotional stress in structurally normal hearts.1 This disease is illustrative of the progress that has been made in the field of cardiogenetics in the last decennia. The first case reports on CPVT date from the 1960s and 1970s, among others a case of a 6-year-old girl with bidirectional tachycardia triggered by exercise.2 An important series describing the phenotype of 21 children with CPVT was published in 1995,1 and the underlying molecular genetic basis was discovered in 2001.3 – 5 In recent years significant progress has been made in the treatment of this potentially lethal condition.6 – 9
2 Etiology
2.1 Molecular Background
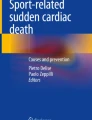
CPVT is caused by modifications in the normal cardiac calcium homeostasis (Fig. 12.1).10 – 13 In the normal heart, a small quantity of calcium enters the cell via voltage-dependent L-type calcium channels during the plateau phase of the action potential. This triggers calcium release from the sarcoplasmic reticulum (SR) into the cytosol through the cardiac ryanodine type 2 receptor (RyR2) channel, which is located in the membrane of the SR. This entire process is termed calcium-induced calcium release (CICR). As a consequence, the cytosolic calcium concentration increases significantly, which causes activation of the actin-myosin filaments with subsequent myocyte shortening and systole. Stimulation of the sympathetic nervous system is associated with activation of intracellular cyclic AMP, which results in phosphorylation of RyR2 through protein kinase A (PKA) and activation of CICR.14

Regulation of the RyR2 channel function in cardiac myocytes.T T-tubule; L L-type of Ca2+ channel; E, NE epinephrine, norepinephrine; hAR beta-adrenergic receptor; cAMP cyclic AMP; PKA protein kinase A; FKBP12.6 calstabin2; TRD triadin 1; JCN junctin; CASQ2 calsequestrin 2; SR sarcoplastic reticulum; SERCA2a sarcoplastic reticulum Ca2 + -ATPase; NCX Na+/Ca + exchanger (Adapted from 14. With permission)
During diastole, most of the reuptake of cytosolic calcium into the SR is performed via SR calcium adenosine triphosphatase (SERCA).11 In addition, calcium is removed from the cell by sodium/calcium exchanger (NCX).
2.2 Pathophysiology
Genetic defects in the genes encoding RyR2 and cardiac calsequestrin (CASQ2) underlie CPVT.3,5 To date, over 70 mutations have been identified in the RyR2 gene, which causes an autosomal dominant CPVT phenotype and is termed CPVT type 1. The rare CPVT type 2 phenotype is caused by mutations in the gene encoding CASQ2 and shows an autosomal recessive inheritance pattern. A third and highly malignant type of CPVT maps to a yet unknown gene that resides on chromosome 7p14–p22 and also segregates as an autosomal recessive trait.15
Both RyR2 and CASQ2 are calcium regulatory proteins.12 Out of the three isoforms of ryanodine receptor (RyR1 to RyR3), RyR2 is considered to be the cardiac isoform.11 RyR2 is one of the largest cardiac ion channel proteins, comprising 4,967 amino acids and the gene encoding RyR2 is located on chromosome 1 (1q42–q43).16 CASQ2 is a 399 amino acid protein and is located in the cardiac SR as well and modulates the activity of the RyR2 channels.11 When the calcium concentration in the SR is low, CASQ2 inhibits RyR2 activity and this inhibition is relieved when the calcium concentration increases.17 The gene encoding CASQ2 also resides on chromosome 1 (1p11–p13.3).5
Mutations in the genes encoding RyR2 or CASQ2 modify their function, which results in calcium leakage from the SR into the cytosol.18,19 This intracellular calcium overload results in activation of NCX. NCX exchanges one calcium ion for three sodium ions, which produces a transient inward current (ITi). ITi generates delayed afterdepolarizations (DADs), which can lead to triggered activity in myocytes and ventricular arrhythmias, in particular under conditions of β-adrenergic stimulation.20 – 22
3 Clinical Aspects
3.1 Epidemiology
There are relatively few epidemiological data on CPVT. The prevalence in the general population is unknown, but is estimated to be approximately 1 in 10 000.13
However, this rare disease seems to be much more common in young victims of sudden unexplained death (SUD), that is, sudden death victims with no significant anatomical abnormalities at autopsy, or in which no autopsy is performed. This was, for example, shown by Tester et al., who performed nontargeted screening of the cardiac ion channel genes in 49 SUD victims aged 1–43 years.23 In seven patients (14%), a putative causal mutation was detected in the RyR2 gene. In similar subsequent series, Creighton et al. identified three RyR2 mutations (21%) in 14 exercise-triggered SUD victims aged 1–43 years,24 and Nishio et al. found three RyR2 mutations (18%) out of 17 cases of SUD at the age of 12–42 years.25
Another clue of the significant contribution of CPVT to SUD in the young was derived from studies by Tan et al. and Hofman et al.26,27 In these series, the yield of cardiological and genetic examination in surviving relatives of the SUD victims was assessed. In the series by Tan et al., comprising 43 SUD victims aged 1–40 years, CPVT was diagnosed in five cases (12%).26 Hofman et al. included 25 pediatric SUD victims (partly overlapping with the series decribed by Tan et al.) and found CPVT in the relatives of two of them (8%).27 In contrast, in two comparable series by Behr et al., comprising 32 and 57 SUD victims aged 4–64 years in which autopsy was negative in all cases, CPVT was diagnosed in none of the families.28,29
In sudden infant death syndrome (SIDS), which is defined as the sudden death of an infant under 1 year of age that remains unexplained after thorough investigation including autopsy, CPVT might also play a role. Tester et al. demonstrated that 1–2% of SIDS may be due to CPVT.30
3.2 Clinical Diagnosis
The first key element in diagnosing CPVT is the patient’s clinical history.1,31 CPVT patients experience complaints, which are typically induced by exercise or emotional stress, in particular dizziness or syncope. Most symptomatic patients are young children. The first syncope usually occurs at the age of 7–9 years and not before the age of 3.1 Sometimes these children know exactly which activities induce their complaints, and most often they try to avoid these triggers. Family history frequently contains syncope or sudden death in young relatives related to similar triggers.
Many of the patients who in the end are diagnosed with CPVT, have been misdiagnosed previously, predominantly with epilepsy. This is probably because syncope in CPVT can resemble epilepsy. It can include a hypertonic phase, convulsive movements, and loss of urine or feces.
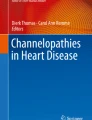
The second key element, the typical bidirectional or polymorphic VT, is sometimes registered with Holter monitoring during syncope. However, most often VT is provoked and registered during exercise testing. The typical exercise test in an untreated CPVT patient is as follows. Ventricular premature beats (VPBs) appear during sinustachycardia, first isolated and monomorphic. The number of VPBs increases with sinus rate, for example, to bigeminy. Finally, the VPBs form rarely monomorphic and mostly polymorphic salvos. These rapid, irregular, and polymorphic VTs may persist when exercise is continued. When the exercise test is ceased, ventricular ectopy frequently disappears immediately. The typical bidirectional VT, which is infrequently observed, refers to ventricular complexes with beat-to-beat alternating right and left QRS axis (Fig. 12.2). Sinus rate at the start of ventricular ectopy is often well reproducible within a patient. The onset focus of ventricular ectopy has been observed to be located frequently in the right ventricular outflow tract.7


Exercise test recordings in a female CPVT patient. (a) The resting ECG shows sinusbradycardia with no ventricular ectopy or other abnormalities. (b) At a sinus rate of 80/min the first ventricular ectopy appears, that is, VPBs in bigeminy (indicated with an asterisk). (c) During maximum exercise the last four VPBs of a bidirectional NSVT are shown on the left. After one regular sinus beat a NSVT of 15 beats starts. In the extremity leads the NSVT is bidirectional and at the switch to the precordial leads it becomes polymorphic. At the right, after one regular sinus beat a NSVT initiates again. VPB ventricular premature beat; NSVT nonsustained ventricular tachycardia
Supraventricular arrhythmias, mainly atrial ectopic beats, nonsustained supraventricular tachycardia, and short runs of atrial fibrillation, can also appear in CPVT patients during exercise.31
When exercise test is not possible or not preferred, adrenaline (0.1–0.3 μg/kg/min) or isoproterenol infusion can be used for simulation.1 ,17, 32 These tests can also be considered in a patient with a normal resting ECG and a negative exercise test in whom syncope or aborted cardiac arrest (ACA) occurred during exertion or emotion.17 Programmed electrical stimulation has not been proven valuable to induce VT in CPVT.1
Resting ECG has inconsistently been described to show several abnormalities, in particular bradycardia and prominent U-waves.1,31,33 Physical examination, echocardiography, and other cardiological examinations are typically normal in CPVT patients.
4 Genetic Diagnosis
The yield of genotyping in CPVT depends on the certainty of the clinical diagnosis.34,35 In patients with a conclusive diagnosis, that is, documented exercise or emotion-induced bidirectional or polymorphic VT, in the absence of structural cardiac disease, a RyR2 mutation is found in 50–70%.34 – 36 CPVT patients with a RyR2 mutation are more often male, and syncope occurs at significantly younger age as compared to nongenotyped patients.36 The yield of RyR2 genotyping is 38% in patients with exertion-induced syncope and exercise test-induced ventricular ectopy, but no bidirectional or polymorphic VT,35 and 5% in patients with exercise or emotion-induced syncope without documented bidirectional or polymorphic VT, 34 both a possible diagnosis of CPVT. Notably, in 45 cases with exercise-induced syncope, corrected QT interval values <480 ms, and no mutations in the 12 long QT syndrome (LQTS)-associated genes, RyR2 missense mutations were found in 31%.35 Mutations in RyR2 are clustered in certain regions.35 This facilitates a tiered genotyping strategy, which was recently proposed and seems attractive and more cost-effective because of the large size of this gene.35 The RyR2 genotyping strategy starts with screening the 16 exons known to host three of more unique CPVT-associated mutations, which (in case of negative results) can be followed by screening the 13 exons with two mutations reported and 16 exons with one mutation reported. Finally, when no mutation is detected yet, the normal pseudo-comprehensive RyR2 scan can be performed.
Identifying a putative pathogenic mutation is important, because it provides the opportunity to genotype relatives of the index patient. The phenotype is similar in genotype-positive and nongenotyped CPVT patients, thus the identification of a mutation does not influence treatment or risk stratification in the index patient.
When relatives of an index patient appear to be carrier of the same mutation, sometimes complaints and exercise-induced VT can be completely absent. In one series of 43 RyR2 mutation carriers, 35% was completely asymptomatic.37 However, these silent mutation carriers are at risk of cardiac events as well.37,38
4.1 Differential Diagnosis
When a patient presents with exercise or emotional stress-induced syncope or ACA, LQTS, particularly type 1, is another possible diagnosis. In most cases, resting 12-lead ECG can immediately differentiate between LQTS and CPVT. In CPVT, usually no abnormalities are seen, whereas LQTS can be revealed most often by a prolonged QTc interval and/or an abnormal T wave morphology. When resting ECG is normal; exercise testing can help to discriminate between LQTS and CPVT. Ventricular ectopy is rarely observed in LQTS and ventricular ectopy beyond a single intermittent VPB is much more common in CPVT.39 In a cohort of 381 patients who were referred because of a suspicion of LQTS, VPBs in bigeminy had a sensitivity of 81%, specificity of 96%, positive predictive value of 45%, and negative predictive value of 99% for CPVT.39
When bidirectional VT is observed during exercise, Andersen–Tawil syndrome (LQTS type 7) should also be considered.13 This condition is caused by loss of function mutations in the KCNJ2 gene, and is usually associated with extracardiac manifestations, that is, periodic paralysis and facial dysmorphisms.
RyR2 mutations have been reported in few families with arrhythmogenic right ventricular dysplasia/cardiomyopathy as well.40 However, as in CPVT no structural cardiac abnormalities are present, the differences between these two phenotypes are usually very clear.
4.2 Therapy and Prognosis
4.2.1 Lifestyle Modifications
CPVT patients are advised not to perform any (competitive) sports, especially when VT is observed during exercise testing. In pediatric CPVT patients, the parents are recommended to observe their children while playing and swimming. Although cardiac events during swimming are more typical for LQTS type 1, they also occur in CPVT patients.41
4.2.2 β-Blocker Therapy
As the trigger for arrhythmias in CPVT is an adrenergic state, β-blocker therapy is the cornerstone of therapy. β-blockers have been empirically used with success for the treatment of CPVT for decades, but not until in 2009 Hayashi et al. provided statistical evidence that β-blockers protect for cardiac events and fatal or near fatal events.38 In this series of 101 CPVT patients, 20 patients were not treated with β-blockers by their physician, most frequently because cardiac symptoms and stress-induced VT were absent. The 8-year cardiac event rate, which was defined as stress-induced syncope, ACA (including appropriate implantable cardioverter-defibrillator (ICD) discharge) or SCD, was 27% in the patients treated with β-blockers, as compared to 58% in the untreated patients. In 11% of the patients treated with β-blockers a fatal or near-fatal event (SCD or ACA) occurred during 8 year of follow-up, in comparison to a 25% fatal or near-fatal event rate in the untreated patients. In multivariate analysis, the absence of β-blocker treatment was an independent predictor for any cardiac event (hazard ratio (HR), 5.48; 95% CI, 1.80–16.68; P = 0.003) and fatal or near-fatal events (HR, 5.54; 95% CI, 1.17–26.15; P = 0.03).
An other important finding in this study was that the event rates within patients with a syncopal history before diagnosis and patients with no history of syncope do not differ.38 Moreover, cardiac events also occurred in silent mutation carriers. This signifies that every CPVT patient and/or RyR2 or CASQ2 mutation carrier should be treated aggressively, regardless of any prior syncopal events or documented ventricular arrhythmias.
Furthermore, a younger age at the time of the diagnosis independently predicted cardiac events, both in the entire series (HR, 0.54 per decade; 95% CI, 0.33–0.89, P = 0.02), and in the subgroup treated with β-blockers (HR, 0.31 per decade, 95% CI, 0.14–0.69, P = 0.004).38 Children are most often treated with a β-blocker dosage based on bodyweight, but these results suggest that this might be inadequate.
Although the authors state that in their series, the cardiac events in patients on β-blocker therapy might be due to an insufficient dosage or noncompliance,38 there have been more observations of suboptimal treatment with the maximum tolerable dosage of β-blockers in some patients. For example, in a series by Sumitomo et al., seven of the 29 CPVT patients died suddenly during a follow-up of 6.8 years, including four patients on β-blocker therapy.7 and Priori et al. even reported sustained VT or VF in 18 out of 39 (46%) on β-blocker therapy during 40–52 months of follow-up.36
The effectiveness of the different β-blockers in CPVT have never been compared with one another. In most case series nadolol is used.1 A dosage of >1.5 mg/kg is advisable.38 Atenolol, bisoprolol, metoprolol, propanolol, and sotalol are also used. β-blockers with intrinsic sympathomimetic activity are not recommended. Whatever β-blocker prescribed, the optimal dosage to suppress VT should be titrated by performing exercise tests on a regular base.
4.2.3 Other Pharmacologic Therapy
As β-blocker therapy is not sufficient in all CPVT patients, calcium channel blocker therapy has been suggested as an adjuvant.6,42 Rosso et al. showed that oral verapamil (2–3 mg per kg bodyweight per day in children, and 240 mg per day in adults) in addition to β-blocker therapy decreased VT during exercise test in five CPVT patients when compared to monotherapy with β-blockers.6 Swan et al. reported similar findings in six CPVT patients who were on β-blocker therapy and underwent an exercise test after intravenous infusion of verapamil (0.2 mg per kg bodyweight).42
Watanabe et al. recently provided evidence for a beneficial effect of flecainide in two highly symptomatic CPVT patients despite conventional drug therapy.9 In a CPVT mouse model, flecainide proved to inhibit RyR2-mediated calcium release into the cytoplasm, which prevented ventricular arrhythmias. Subsequently, this mechanism-based approach suppressed VT in two patients, who had remained highly symptomatic despite β-blocker and calcium channel blocker therapy. These promising results will need to be confirmed in a larger series of conventional therapy-resistant CPVT patients.
Other pharmacologic agents, such as amiodarone and magnesium, have been tested in CPVT patients, but lacked efficacy.1,7 In the acute setting, adenosine and propanolol have been reported in case reports to terminate VT in CPVT patients.43,44
4.2.4 Nonpharmacologic Therapy
Surgical left cardiac sympathetic denervation (LCSD) has been proven to be a highly effective therapy in CPVT patients whose symptoms are not controlled by pharmacologic therapy.8,45 – 47 During this procedure, the lower part of the stellate ganglion and the second and third thoracic ganglia are ablated. As a result, the release of norepinephrine in the heart is highly diminished, which has an antiarrhythmic effect. A few cases with excellent results after this procedure have been published,8 including one case with 10 year follow-up,45 and several patients in whom video-assisted thoracoscopic surgery was used.46,47
4.3 Follow-up
The basis of follow-up of CPVT patients is performance of exercise testing and Holter monitoring on a regular basis. With these examinations, the efficacy of treatment can be monitored and, if necessary, adjustments can be made. It is important to emphasize that in a part of CPVT patients VPBs remain present during exercise testing despite optimal therapy. In clinical practice this is considered safe and acceptable, though its prognostic relevance is actually unknown. However, the presence of couplets or more successive VPBs should not be accepted, as these are significantly associated with future cardiac events (sensitivity, 0.62; specificity, 0.67; P = 0.03).38
4.4 Risk Stratification/Indication for ICD
The 2006 ACC/AHA/ESC Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention for Sudden Cardiac Death give a class I recommendation for implantation of an ICD in addition to β-blocker therapy for CPVT patients who are survivors of ACA.48 A class IIa recommendation is given for ICD implantation in CPVT patients with syncope and/or documented sustained VT despite β-blocker therapy.
However, as the malignancy of this disease has been well recognized, in the recent years ICD implantation has been performed more liberal than the guidelines recommend. This is an unfortunate development, because ICD implantation has some serious disadvantages in the setting of this specific condition and can even be harmful. Both appropriate and inappropriate shocks cause pain and fear, which raises the release of catecholamines and can result in VT, electrical storm or VF. This mechanism was illustrated in two case reports on death of a CPVT patient with an ICD.49,50 In one case, a young male CPVT patient received inappropriate ICD therapy as a result of paroxysmal atrial fibrillation, which triggered the fatal ventricular arrhythmias.49 In the second case, a young woman with incessant rapid polymorphic VT could not be saved despite appropriate ICD therapy.50 Hence, lessons to be learned from these cases are that one should be very reluctant to implant an ICD in CPVT patients. Indeed, ICDs can be proarrhythmic in this setting.
4.5 Cardiogenetics Aspects
The odds of positive genotyping are highest in patients with a conclusive diagnosis of CPVT.14,34 Bai et al. found a RyR2 mutation in 62% of 81 patients with a conclusive diagnosis of CPVT, which resulted in an estimated cost of US $5263 per one positive RyR2 genotyping. In patients with exercise or emotion-induced syncope without documented bidirectional or polymorphic VT, ACA survivors, and relatives of SCD victims the yield of genotyping was much lower, resulting in considerably higher costs. Thus, it is highly recommendable to reserve genotyping for index patients with a certain diagnosis of CPVT. When no mutation is found in RyR2, CASQ2 genotyping can be considered. Apart from families with consanguinity, this is also recommended in cases with a clear CPVT phenotype, as heterozygous carriership of CASQ2 mutations can cause CPVT.51
When a particular CPVT genotype is detected, first-degree relatives should be tested to identify those relatives at risk of cardiac events. This provides the unique opportunity to take preventive measure in mutation carriers, as the first manifestation of CPVT can be cardiac arrest. In contrast to many other inherited diseases, genotyping in CPVT is strongly recommended in children from the age of 4 years, because the disease can manifest itself at young age. In case no mutation is detected in the index patient, thorough clinical evaluation of first-degree relatives is recommended.
5 Summary
CPVT is a rare, but very lethal primary arrhythmia syndrome, most often caused by gain-of-function mutations in the gene encoding RyR2, which result in an intracellular calcium overload. Increased adrenergic stimulation induces the classic bidirectional or polymorphic ventricular VT or even ventricular fibrillation. The typical pediatric patients often experience syncopes during stress and have structurally normal hearts. The primary treatment consists of cessation of physical exertion and β-blocker therapy, with regular follow-up including exercise, testing, and Holter monitoring. This treatment should be offered to all CPVT patients, that is, clinically diagnosed patients with or without syncope and silent mutation carriers. In case of insufficient suppression of ventricular arrhythmias, addition of a calcium channel blocker or perhaps flecainide are alternative options. LCSD can be performed in the most severe cases. Implantation of an ICD should be avoided as much as possible because of its potential proarrhythmic effect in this specific condition. In all first-degree relatives above the age of 4 of an index patient, cardiological and genetic evaluation is recommended to provide the opportunity of taking preventive measures in the affected individuals.
References
Leenhardt A, Lucet V, Denjoy I, Grau F, Ngoc DD, Coumel P. Catecholaminergic polymorphic ventricular tachycardia in children. A 7-year follow-up of 21 patients. Circulation. 1995;91:151-159.
Reid DS, Tynan M, Braidwood L, Fitzgerald GR. Bidirectional tachycardia in a child. A study using His bundle electrography. Br Heart J. 1975;37:339-344.
Priori SG, Napolitano C, Tiso N, et al. Mutations in the cardiac ryanodine receptor gene (hRyR2) underlie catecholaminergic polymorphic ventricular tachycardia. Circulation. 2001;103:196-200.
Laitinen PJ, Swan H, Kontula K. Molecular genetics of exercise-induced polymorphic ventricular tachycardia: identification of three novel cardiac ryanodine receptor mutations and two common calsequestrin 2 amino-acid polymorphisms. Eur J Hum Genet. 2003;11:888-891.
Lahat H, Pras E, Olender T, et al. A missense mutation in a highly conserved region of CASQ2 is associated with autosomal recessive catecholamine-induced polymorphic ventricular tachycardia in Bedouin families from Israel. Am J Hum Genet. 2001;69:1378-1384.
Rosso R, Kalman JM, Rogowski O, et al. Calcium channel blockers and beta-blockers versus beta-blockers alone for preventing exercise-induced arrhythmias in catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2007;4:1149-1154.
Sumitomo N, Harada K, Nagashima M, et al. Catecholaminergic polymorphic ventricular tachycardia: electrocardiographic characteristics and optimal therapeutic strategies to prevent sudden death. Heart. 2003;89:66-70.
Wilde AA, Bhuiyan ZA, Crotti L, et al. Left cardiac sympathetic denervation for catecholaminergic polymorphic ventricular tachycardia. N Engl J Med. 2008;358:2024-2029.
Watanabe H, Chopra N, Laver D, et al. Flecainide prevents catecholaminergic polymorphic ventricular tachycardia in mice and humans. Nat Med. 2009;15:380-383.
Liu N, Priori SG. Disruption of calcium homeostasis and arrhythmogenesis induced by mutations in the cardiac ryanodine receptor and calsequestrin. Cardiovasc Res. 2008;77:293-301.
Katz G, Arad M, Eldar M. Catecholaminergic polymorphic ventricular tachycardia from bedside to bench and beyond. Curr Probl Cardiol. 2009;34:9-43.
Gyorke S. Molecular basis of catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2009;6:123-129.
Liu N, Ruan Y, Priori SG. Catecholaminergic polymorphic ventricular tachycardia. Prog Cardiovasc Dis. 2008;51:23-30.
Kontula K, Laitinen PJ, Lehtonen A, Toivonen L, Viitasalo M, Swan H. Catecholaminergic polymorphic ventricular tachycardia: recent mechanistic insights. Cardiovasc Res. 2005;67:379-387.
Bhuiyan ZA, Hamdan MA, Shamsi ET, et al. A novel early onset lethal form of catecholaminergic polymorphic ventricular tachycardia maps to chromosome 7p14-p22. J Cardiovasc Electrophysiol. 2007;18:1060-1066.
Swan H, Piippo K, Viitasalo M, et al. Arrhythmic disorder mapped to chromosome 1q42-q43 causes malignant polymorphic ventricular tachycardia in structurally normal hearts. J Am Coll Cardiol. 1999;34:2035-2042.
Cerrone M, Napolitano C, Priori SG. Catecholaminergic polymorphic ventricular tachycardia: A paradigm to understand mechanisms of arrhythmias associated to impaired Ca(2+) regulation. Heart Rhythm. 2009;6:1652-1659.
Jiang D, Xiao B, Yang D, et al. RyR2 mutations linked to ventricular tachycardia and sudden death reduce the threshold for store-overload-induced Ca2+ release (SOICR). Proc Natl Acad Sci U S A. 2004;101:13062-13067.
di Barletta MR, Viatchenko-Karpinski S, Nori A, et al. Clinical phenotype and functional characterization of CASQ2 mutations associated with catecholaminergic polymorphic ventricular tachycardia. Circulation. 2006;114:1012-1019.
Schlotthauer K, Bers DM. Sarcoplasmic reticulum Ca(2+) release causes myocyte depolarization. Underlying mechanism and threshold for triggered action potentials. Circ Res. 2000;87:774-780.
Cerrone M, Noujaim SF, Tolkacheva EG, et al. Arrhythmogenic mechanisms in a mouse model of catecholaminergic polymorphic ventricular tachycardia. Circ Res. 2007;101:1039-1048.
Knollmann BC, Chopra N, Hlaing T, et al. Casq2 deletion causes sarcoplasmic reticulum volume increase, premature Ca2+ release, and catecholaminergic polymorphic ventricular tachycardia. J Clin Invest. 2006;116:2510-2520.
Tester DJ, Spoon DB, Valdivia HH, Makielski JC, Ackerman MJ. Targeted mutational analysis of the RyR2-encoded cardiac ryanodine receptor in sudden unexplained death: a molecular autopsy of 49 medical examiner/coroner’s cases. Mayo Clin Proc. 2004;79:1380-1384.
Creighton W, Virmani R, Kutys R, Burke A. Identification of novel missense mutations of cardiac ryanodine receptor gene in exercise-induced sudden death at autopsy. J Mol Diagn. 2006;8:62-67.
Nishio H, Suzuki K. Postmortem molecular analysis for fatal arrhythmogenic disease in sudden unexplained death. Leg Med (Tokyo) 2009.
Tan HL, Hofman N, van Langen IM, van der Wal AC, Wilde AA. Sudden unexplained death: heritability and diagnostic yield of cardiological and genetic examination in surviving relatives. Circulation. 2005;112:207-213.
Hofman N, Tan HL, Clur SA, Alders M, van Langen I, Wilde AA. Contribution of inherited heart disease to sudden cardiac death in childhood. Pediatrics. 2007;120:e967-e973.
Behr E, Wood DA, Wright M, et al. Cardiological assessment of first-degree relatives in sudden arrhythmic death syndrome. Lancet. 2003;362:1457-1459.
Behr ER, Dalageorgou C, Christiansen M, et al. Sudden arrhythmic death syndrome: familial evaluation identifies inheritable heart disease in the majority of families. Eur Heart J. 2008;29:1670-1680.
Tester DJ, Dura M, Carturan E, et al. A mechanism for sudden infant death syndrome (SIDS): stress-induced leak via ryanodine receptors. Heart Rhythm. 2007;4:733-739.
Napolitano C, Priori SG. Diagnosis and treatment of catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2007;4:675-678.
Krahn AD, Gollob M, Yee R, et al. Diagnosis of unexplained cardiac arrest: role of adrenaline and procainamide infusion. Circulation. 2005;112:2228-2234.
Postma AV, Denjoy I, Kamblock J, et al. Catecholaminergic polymorphic ventricular tachycardia: RYR2 mutations, bradycardia, and follow up of the patients. J Med Genet. 2005;42:863-870.
Bai R, Napolitano C, Bloise R, Monteforte N, Priori SG. Yield of genetic screening in inherited cardiac channelopathies: how to prioritize access to genetic testing. Circ Arrhythmia Electrophysiol. 2009;2:6-15.
Medeiros-Domingo A, Bhuiyan ZA, Tester DJ, et al. The RYR2-encoded ryanodine receptor/calcium release channel in patients diagnosed previously with either catecholaminergic polymorphic ventricular tachycardia or genotype negative, exercise-induced long QT syndrome: a comprehensive open reading frame mutational analysis. J Am Coll Cardiol. 2009;54:2065-2074.
Priori SG, Napolitano C, Memmi M, et al. Clinical and molecular characterization of patients with catecholaminergic polymorphic ventricular tachycardia. Circulation. 2002;106:69-74.
Bauce B, Rampazzo A, Basso C, et al. Screening for ryanodine receptor type 2 mutations in families with effort-induced polymorphic ventricular arrhythmias and sudden death: early diagnosis of asymptomatic carriers. J Am Coll Cardiol. 2002;40:341-349.
Hayashi M, Denjoy I, Extramiana F, et al. Incidence and risk factors of arrhythmic events in catecholaminergic polymorphic ventricular tachycardia. Circulation. 2009;119:2426-2434.
Horner JM, Ackerman MJ. Ventricular ectopy during treadmill exercise stress testing in the evaluation of long QT syndrome. Heart Rhythm. 2008;5:1690-1694.
Tiso N, Stephan DA, Nava A, et al. Identification of mutations in the cardiac ryanodine receptor gene in families affected with arrhythmogenic right ventricular cardiomyopathy type 2 (ARVD2). Hum Mol Genet. 2001;10:189-194.
Choi G, Kopplin LJ, Tester DJ, Will ML, Haglund CM, Ackerman MJ. Spectrum and frequency of cardiac channel defects in swimming-triggered arrhythmia syndromes. Circulation. 2004;110:2119-2124.
Swan H, Laitinen P, Kontula K, Toivonen L. Calcium channel antagonism reduces exercise-induced ventricular arrhythmias in catecholaminergic polymorphic ventricular tachycardia patients with RyR2 mutations. J Cardiovasc Electrophysiol. 2005;16:162-166.
De Rosa G, Delogu AB, Piastra M, Chiaretti A, Bloise R, Priori SG. Catecholaminergic polymorphic ventricular tachycardia: successful emergency treatment with intravenous propranolol. Pediatr Emerg Care. 2004;20:175-177.
Sumitomo N, Sakurada H, Mugishima H, Hiraoka M. Adenosine triphosphate terminates bidirectional ventricular tachycardia in a patient with catecholaminergic polymorphic ventricular tachycardia. Heart Rhythm. 2008;5:496-497.
Makanjee B, Gollob MH, Klein GJ, Krahn AD. Ten-year follow-up of cardiac sympathectomy in a young woman with catecholaminergic polymorphic ventricular tachycardia and an implantable cardioverter defibrillator. J Cardiovasc Electrophysiol. 2009;20(10):1167-1169.
Collura CA, Johnson JN, Moir C, Ackerman MJ. Left cardiac sympathetic denervation for the treatment of long QT syndrome and catecholaminergic polymorphic ventricular tachycardia using video-assisted thoracic surgery. Heart Rhythm. 2009;6:752-759.
Atallah J, Fynn-Thompson F, Cecchin F, DiBardino DJ, Walsh EP, Berul CI. Video-assisted thoracoscopic cardiac denervation: a potential novel therapeutic option for children with intractable ventricular arrhythmias. Ann Thorac Surg. 2008;86:1620-1625.
Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: a report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (writing committee to develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006;114:e385-e484.
Pizzale S, Gollob MH, Gow R, Birnie DH. Sudden death in a young man with catecholaminergic polymorphic ventricular tachycardia and paroxysmal atrial fibrillation. J Cardiovasc Electrophysiol. 2008;19:1319-1321.
Mohamed U, Gollob MH, Gow RM, Krahn AD. Sudden cardiac death despite an implantable cardioverter-defibrillator in a young female with catecholaminergic ventricular tachycardia. Heart Rhythm. 2006;3:1486-1489.
Postma AV, Denjoy I, Hoorntje TM, et al. Absence of calsequestrin 2 causes severe forms of catecholaminergic polymorphic ventricular tachycardia. Circ Res. 2002;91:e21-e26.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2011 Springer-Verlag London Limited
About this chapter
Cite this chapter
van der Werf, C., Wilde, A.A.M. (2011). Catecholaminergic Polymorphic Ventricular Tachycardia. In: Baars, H., Doevendans, P., van der Smagt, J. (eds) Clinical Cardiogenetics. Springer, London. https://doi.org/10.1007/978-1-84996-471-5_12
Download citation
DOI: https://doi.org/10.1007/978-1-84996-471-5_12
Published:
Publisher Name: Springer, London
Print ISBN: 978-1-84996-470-8
Online ISBN: 978-1-84996-471-5
eBook Packages: MedicineMedicine (R0)