
Abstract
Trauma is an important cause of death and disability in the United States. Unintentional injury is the leading cause of death among people 1–44 years of age. In 2009, over 177,000 people died as the result of unintentional injury and as a result, 2.5 million potential years of life were lost. Historically, injury was thought to be purely accidental due to uncontrollable and unalterable events, essentially random chance. This began to change in the mid-twentieth century as researchers began to study injury in an effort to understand, define, and prevent these events. The first of these steps was the recognition of injury as a biomechanical event due to the interaction of a person (or victim) with an energy source in certain environments (e.g., an automobile). Several small advances ultimately led to the description of injury as a multiphase event, which can be readily studied by application of an injury matrix. As society has become more complex, injury prevention has evolved from simply studying the biomechanical forces of injury to creating prevention strategies through education, enforcement, and engineering.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Introduction
Unintentional injury is the leading cause of death among people 1–44 years of age [1, 2]. Furthermore, in this age group, injuries are the leading cause of physician contact resulting in more than 2.8 million hospitalizations and almost 30 million patient evaluations [3]. This burden is especially true in the youngest demographic, individuals between the ages of 1–34 [1]. The leading causes of death in this age group are motor vehicle collision followed by homicide. The economic cost of injuries is impressive as well. In 2005, an estimated $406 billion dollars in cost from medical- and work-related loss were absorbed due to evaluation, hospitalization, and deaths related to injury [2]. While trauma and emergency services personnel evaluate most of these patients, the urologist plays a role in the evaluation and management of patients with genitourinary injuries. In the United States, abdominal organ injuries resulted in 6.3 % of total injuries, whereas pelvic injuries resulted in 4.5 % [4]. Based on current US population data, approximately 15,000 persons would sustain renal injuries requiring hospital evaluation annually. Urethral and bladder injuries occur in approximately 10–15 % of pelvic fractures and the incidence of pelvic fracture in 2007 was greater than 67,000. Thus, an additional 6,000–10,000 urological injuries occur as a result of pelvic injury. Injuries to the genitourinary system are rarely life threatening, but the potential morbidity is quite high and results in significant changes in quality of life. Despite the fact that traumatic injury to the urinary system is a minor component of traumatic injuries, it is a prevalent disease. Recent literature suggests that the US trauma management system is strained and injury prevention activities do not constitute a significant portion of patient care, especially in these at risk individuals [5]. Historically, unintentional injuries were felt to be accidents or “acts of God” and therefore not preventable due to the seeming random pattern with which they occur. Only in the twentieth century did injury prevention and research develop a critical mass of strategies, programs, policies, and practices to become a recognized field of study [6]. The study of injury prevention seeks to understand the characteristics of injury through surveillance, research, and identification of risk factors. Targeting of these risk factors through well-developed and scientifically based prevention efforts determines which are effective and worth pursuing and which are ineffective and should be changed or discontinued. For the purposes of this chapter, all injury and prevention strategies will be limited to unintentional injuries rather than intentional (e.g., suicide and poisoning).
Impact of Trauma
Trauma continues to be an important source of disease and disability in the United States. In 2009, over 177,000 people died as the result of unintentional injury and 2.5 million potential years of life were lost [1]. Based on the CDC National Center for Health Statistics in 2008, unintentional injury was the fifth leading cause of death (Table 2.1) [1, 7]. Unintentional injury is one of the top five causes of mortality in all age groups until the seventh decade of life (Table 2.2) [7]. It is the leading cause of death until age 44. Of unintentional injuries, motor vehicle collision or traffic-related fatality is the leading cause of death resulting in 38,000 deaths [8]. The third leading cause of death is unintentional falls and this results in 24,000 deaths annually [1]. In 2009, 29.6 million people sustained injury and the injury rate per 100,000 persons is 9,661. By age 15, unintentional injury related to motor vehicle collision is the third or fourth leading cause of nonfatal injury and overall resulted in 2.64 million emergency department evaluations in 2009. On a daily basis in the United States, tens of thousands of people (adults and children) are injured severely enough to seek medical care (Table 2.3). Of those, about 200 will develop long-term disability due to injury and 400 will die [9, 10]. On a global basis, 1.6 million people die from injuries each year and the incidence continues to increase [11, 12]. The ramifications of trauma go beyond injury or statistics of evaluation and death. Injury results in significant societal and personal monetary costs as well as personal disability. Injury, both intentional and unintentional, causes changes to the lives of affected individuals and their families. In addition to physical disability, they must adapt to changes in independence, decreased work ability, chronic fatigue, and interpersonal relationship changes from traumatic stress or brain injury. The lifetime cost of medical- and work-related unintentional injury in 2005 was 99 billion dollars [1].
Injury Defined
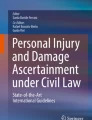
If injury is defined as a biomechanical event, the simplest definition is harm inflicted on a person due to the release and transfer of physical energy from an object. The release of a large amount of energy and its projection to the human body overwhelms the resistance mechanism. This energy transfer results in injuries when people, unstable environments, and hazards or objects converge. These three components, people, environment, and objects, are normally in balance with equal distribution and result in equilibrium of energy. When this distribution becomes unbalanced, there is a transfer of energy to a person and excessive energy transfer can result in injury. If this equilibrium is considered in terms of human performance, the balance of energy is expressed as performance and task demand [13]. Performance is defined as how well a task is completed. Task demand is defined as the effort required to complete an action. Depending on the complexity of the task, individuals are at greater or lesser risk for injury depending on their ability to equalize performance and task demand. These variables fluctuate over time and injuries occur when the performance does not meet task demand (substandard performance) or task demand exceeds performance ability. Performance and task demand can be analyzed graphically and the curves plotted. At each point the curves intersect, that intersection is referred to as an event (Fig. 2.1). Energy is unbalanced at these points and if this unbalanced energy is transferred from the object or environment to an individual, injury can result.

Graphic depiction of performance and task demand (adapted from Martinez [13])
In the modern world physical energy comes in many forms including thermal, mechanical, electrical, nuclear, or chemical each of which is transferred to the human body in different ways [14]. Energy transfer is often a rapid process and due to its physical principals the results are predictable. Unfortunately, energy transfer and the resultant injury often have both immediate consequences and long-term sequelae [15]. The study of injury prevention seeks to evaluate and characterize this dual nature of injury, the immediate effects and chronic outcomes. This is especially important as injury is a unique disease that disproportionately affects a younger population and is not only a leading cause of death, but a cause of disability as well.
Injury Prevention: Historical Chronology
A fundamental change in the understanding of injury began when investigators first studied injury as a process or disease rather than a series of unrelated events. The scientific study of injury prevention began in the 1930s. Prior to this, victims of injury were thought to have suffered a random accident or were responsible for the injury due to carelessness or bad luck. However, this changed in the early twentieth century when researchers began to look at injury systematically. The first person to study injury as a cause and effect process was Hugh De Haven. De Haven was a physiologist who studied the kinetic forces related to crash or fall. In 1942, he published a study evaluating survival in falls from heights and found that if the transfer of energy could be changed or altered, the severity of the injury could be lessened [16]. He noted that the human body had a certain tolerance or resistance to transfer of mechanical energy. His theory that separation of the mechanical energy from the body lessened injury was the initial step in the study of injury prevention. With greater forces, the body sustains a greater injury; however, the body can sustain a certain amount of imparted energy without significant injury. The next major step in the science of injury prevention came from John Gordon who described injury in the epidemiologic terms of host (victim), agent (energy), and vector (environment) [17]. His description was important because it was the first time injury was viewed as a disease process and demonstrated how injury could be studied like other epidemiologic problems, namely infectious disease. The person most responsible for the discipline of injury prevention, however, was William Haddon. Haddon was the first director of the National Highway Traffic Safety Administration and in this capacity, his primary focus was road, traffic, and vehicular safety [18]. He approached injury systematically and studied injury as a biomechanical event due to the transfer of energy. He recognized, like De Haven, that if an individual can be separated from the energy transfer in the injury event, i.e., motor vehicle collision, then the damage inflicted can be diminished or eliminated. Haddon recognized that injury is the result of energy transfer and the effect of the uncontrolled energy is predictable based on physical laws. If energy is considered the vector and is predictable in its action, then the disease (injury) can be studied systematically. He went on to expand the epidemiological theory of Gordon and noted that each epidemiologic factor (host, agent, and environment) is affected by three constant and reproducible phases of injury: pre-event, event, and post-event [18]. By combining the epidemiologic factors of disease with the sequence of events in trauma and injury (pre-event, event, and post-event) Haddon’s matrix is created (Table 2.4). Haddon’s matrix is important as it gives a framework for analysis and study of injury. In addition to the matrix, Haddon’s other major contribution to injury prevention is his strategies for injury prevention. These ten strategies were the result of his observation that by separating injury into three phases of injury, several measures can be taken at each point to prevent injury. The basis of these strategies is to separate the agent or energy from the host.
Haddon’s original ten strategies for injury prevention [18, 19]:
-
1.
Pre-event
-
(a)
Prevent creation of the hazard.
-
(b)
Reduce the amount of the hazard.
-
(c)
Prevent the release of the hazard that already exists.
-
(a)
-
2.
Event phase
-
(a)
Modify the rate of the release of the hazard from its source.
-
(b)
Separate, in time or space, the hazard being released from that which is to be protected.
-
(c)
Separate, by mechanical barrier, the hazard from that which is to be protected.
-
(d)
Modify the basic quality of the hazard to reduce the energy released.
-
(e)
Make what is to be protected more resistant to damage from the hazard.
-
(a)
-
3.
Post-event phase
-
(a)
Detect and counter the damage already done by the environmental hazard.
-
(b)
Stabilize, repair, and rehabilitate the damaged object.
-
(a)
Haddon’s ten strategies for injury prevention and the subsequent matrix are the basis for most injury prevention programs and ongoing prevention studies.
Injury Prevention Strategies and Analysis
Despite the fact that the source of injury is a fast acting force, injury occurs over a continuum. Injury is studied by breaking this process into the three phases proposed by Haddon. In the pre-event phase, energy has not yet been released or transferred to cause injury and strategies applied at this point are often referred to as primary prevention. At this point in the injury continuum, the strategies seek to prevent injury from occurring by changing susceptibility or inhibiting exposure. Examples of primary prevention include driver’s education classes or sobriety checkpoints. During the event phase, the energy is transferred to the host and strategies at this point are referred to as secondary prevention. These factors tend to attempt to reduce energy transfer to the host either by early detection or early treatment. Examples of secondary prevention include seat belts and automobile air bags. The final phase, post-event, energy has been transferred and strategies here are referred to as tertiary prevention. Factors applied here seek to minimize injury and the focus is on restoring function of the individual or limiting the resultant disability. Examples of tertiary prevention include emergency medical services, designated trauma centers, and specialized rehabilitation centers.
In Haddon’s matrix each component of the epidemiologic triangle (host, agent–vector, and environment) has application for each of the phases of injury. Thus, the host (human) can be impacted in each of the phases: pre-event—impaired capabilities, event—injury tolerance of the body, post-event—degree of injury sustained [18]. Haddon’s ten general strategies for injury prevention provide an outline for the logical and systematic evaluation of injury events. This framework can be termed an options analysis [13]. In this context, a problem is approached by evaluating each strategy as it applies to the problem and generating the most likely preventative actions at each phase of the injury event. A unique aspect of the options analysis is that it does not require an in-depth understanding of the factors responsible for the injury as the analysis is directed at preventative strategies not elimination of the problem. The end result of the application of an option analysis is countermeasures to injury or preventative strategies. Prior to implementation, each prevention strategy or countermeasure must be evaluated in terms of cost, practicality, and effectiveness. In using Haddon’s outline for development of injury prevention strategies, the real world application is that each point is not always applicable to each problem. However, the outline allows for thoughtful analysis of a problem and in this process several actionable strategies to the problem emerge.
Approaches to Injury Prevention
Identification of practical strategies for injury prevention is only half of the work; the other half is the implementation of these identified measures. The methods of implementation fall into one of three categories, known as the three “E’s”: education, enforcement, and engineering [20]. These three categories can be divided into two types of intervention: active and passive. Active interventions necessitate a change in the behavior of the individual and require performance of an act such fastening a seatbelt. Passive interventions do not require any action by the host (person) and typically these preventative measures are built into the design of the agent (vehicle). The host will receive protection simply by use of the object or vehicle (agent) in the environment.
Education: Education is the easiest strategy to implement and the most common method used in injury prevention. The idea behind education is that once the host or person is given information, knowledge, or training they will process and store this information and use it to reduce their risk of injury. Education is an active intervention that seeks to change behaviors and protect the host in this fashion. However, the person must be able to understand, process and apply the knowledge to gain benefit. The most effective education programs have ongoing evaluation for changes in behavior and outcome. This has not always been the case and without analysis and appropriate implementation, education programs are less successful or even completely ineffective [21]. Furthermore, to ensure long-term success, education strategies must have a plan for long-term effectiveness otherwise the initial effort loses impact. Despite this, education is a simple, powerful tool that can disseminate information effectively to large populations. Additionally, in today’s society, social media and marketing can inform large segments of society and effectively change social attitudes, ultimately creating popular support for injury prevention strategies.
Enforcement: The second active intervention in the three “E’s” is enforcement. These are legal and administrative directives enacted to effect injury prevention strategies. The legal aspect of enforcement includes both legislative efforts to create laws and government enforcement of the laws. These are often more effective than education because implementation is mandated rather than suggested. However, the legal and administrative directives come with many limitations and restrictions [22].
To begin with, the population at large must recognize and agree that the problem merits legislation and passage of a law. In American society, people favor legislation if they perceive that it will protect them or prevent someone from injuring them, but oppose something that limits their rights including the ability to harm or injure oneself. For example, the public favors laws restricting drunk driving but does not approve of mandatory safety belts or use of motorcycle helmets [13]. Typically, Americans support laws that affect other people and oppose laws that affect them personally. The major challenges to legislation and legal directives are cost and loss of personal freedom [23]. One hurdle with respect to cost is convincing individuals that despite the direct cost they may incur due to legislation, the treatment and rehabilitation of preventable injuries is an expense shared by the larger population in the form of taxes and public healthcare support. When considering loss of personal freedom, three factors reduce the effectiveness of laws and legislation: exemptions, enforcement, and punishment [24]. Exemption detracts from the law by creating ambiguous enforcement rules or altering the intent of the law. Seat belt laws exemplify this as many states do not allow for primary enforcement of these laws but rather citation if a driver is stopped for other reasons [25]. In this scenario, primary enforcement of seat belt laws is exempted. Laws that are enforced based on age are an example as well. Compliance with laws and directives has a direct correlation to enforcement and punishment. If the population does not believe that enforcement is likely then there is no incentive to comply with the law. The easiest laws to enforce are laws that are easy to for law enforcement observe, i.e., speed limits and helmet laws. Speed limits are easy to enforce as the top speed is posted and laser or radar speed detectors are used to directly measure a vehicle’s speed. Punishment for violation of laws improves compliance with laws as well. If violation of a law does not result in punishment, fewer individuals will comply with the law because there is no fear in punishment. An important legal phenomenon, however, is that more severe punishment lessens the punishment or conviction rate because a severe punishment necessitates greater strength of evidence due to the severity of the penalty [13].
Engineering: The final E is engineering. Engineering strategies are considered passive actions. Passive actions do not require any participation on the part of the host. A unique aspect of engineering is that it is a strategy that is effective in the event phase of an injury, i.e., airbags in an automobile. Since no active participation is required from the individual, engineering is thought to be the most effective injury prevention strategy. However, despite the fact that this is a passive intervention, engineering faces opposition not unlike legislation: complaints of loss of personal freedom and benefits which do not outweigh the costs [26]. American society continues to evaluate injury prevention and other social efforts with the viewpoint that safety should be a design element that does not limit the performance of things we use. However, it is apparent that advances in engineering make many potential hazards, especially motor vehicles, safer [14]. In addition to the event phase, engineering can impact the post-event phase as well. Automobiles are designed to reduce fires at impact, sensors in automobiles can alert medical care, and trauma systems can remotely monitor the injured person (host) in transit. Again, these benefits of engineering are passive interventions that do not require participation of the host [18].
Evaluation of Injury Prevention Programs
Injury prevention programs are only as successful as the results of their interventions. These programs should be evaluated at two points: process and outcome. Process evaluation is an ongoing step to provide and obtain feedback for the intervention. If the outcomes from an injury prevention program are not equivalent to those envisioned during the design of the program, the end result cannot be ensured. Outcome, ultimately, is the most important measure of any injury prevention program. The goal of a program is to reduce or impact the incidence or severity of specific injuries. Often it is necessary to measure the outcome in stages and to look for changes in behavior, which ultimately will affect the incidence of the injury. An example is the increase in number of helmets worn by motorcycle riders after passage of helmet laws or legislation [27]. While there is not an immediate change in brain or spinal injury following these actions, if the observed number of helmets worn increases, then the assumption can be made that ultimately, brain and spinal injury due to motorcycle collisions will decrease. Additionally, outcome can be measured with a series of questions: Have attitudes changed? Has behavior changed? Is there a correlation between favorable outcome and behavior change? [13]. Ultimately, if the first two questions result in positive answers but the last question, outcomes, is unchanged then the program is not successful. The programs which have all three questions answered affirmatively usually require fewer, ideally one or two, major but simple changes in behavior.
Priority Areas for Genitourinary Injury Prevention
Urologists have many opportunities to impact the field of injury prevention through investigation, research, and public education merging our knowledge of the genitourinary system with the three “E’s.” The primary “E” for urologists is education. The American Urological Association has created a model in the male health check list [28]. The male health checklist is divided into two sections, urology specific and related health categories and these are subdivided into four age groups. With this framework, urology-specific and related health injury risks can be created and stratified by age. Organ- and age-specific injury databases will assist with identification of potential injury causes and preventative measures can be developed from these data. The second “E,” enforcement, is the most underutilized “E.” Two applicable scenarios for prevention are sports-related and military combat-related genitourinary injury. Presently, there is very little policy or rule with regard to genitourinary injury and its prevention through enforcement or penalty. The only sport, either professional or amateur, to require genitourinary protective equipment is Little League baseball [29]. Their rules require players to wear athletic supporters but not necessarily a protective cup-type device. The recent military literature has considerable documentation showing the decrease in genitourinary injury with the use of body armor [30–32]. In the current conflicts in Iraq and Afghanistan, more soldiers are injured by improvised explosive devices than missile or other blast injury [33]. Recently, explosion resistant undergarment had been created using flexible armor plates and Kevlar woven into the fabric. Troops are now deployed with both body armor and external genital armor/protective garments. No official policy exists requiring soldiers to wear either armor or protective garments despite this evidence. The primary limitation in both civilian and military realms is inspection. Any external protection is easy to inspect, however, identification of undergarment protection is time-consuming and fraught with privacy issues. The third “E,” engineering, is an emerging area in which we as urologists are becoming involved. Blunt injury is the most common form of genitourinary system injury and the leading cause is motor vehicle collision. As the field of injury prevention matures, centers of excellence, such as the Harborview Injury Prevention and Research Center, are emerging and contributing to this “E.” Two recent publications have evaluated both sources of injury in the passenger compartment of an automobile as well as the effectiveness of passive protective devices, i.e., airbags [34]. In evaluating sources of injury, the steering wheel, central console, and seatbelt buckles are the key causes of renal injury in frontal and side impact collisions [35]. With this knowledge, engineers and designers can modify the passenger compartment layout and passive safety equipment accordingly. Furthermore, airbags may both be a protective device or source of injury based on vehicle speed. Changing the airbag deployment sensors and calculating for vehicle speed can improve the protective effect and reduce the injury component of these safety devices. Injury prevention has great importance in the era of healthcare reform and cost containment. Focusing on more minor injuries will impact a larger segment of the population as a greater number of persons sustain minor injuries annually and require medical evaluation while severe injuries, although more morbid are less common. The urologist is in a position of educator and simple tools such as an injury checklist and prevention strategies are the easiest to implement. Continued legislative focus, such as the American Urological Association task force on Urotrauma, can bring about reasonable changes in military enforcement and improved engineering. Finally, continued efforts to identify injury sources and partner with industry are one way urologic injury prevention improves through engineering.
Conclusion
Injury prevention programs and interventions are beneficial at the individual and societal level. However, injury prevention requires a multidisciplinary team work and often the assistance of nonmedical or first responder persons. Injury prevention has developed into a discipline combining elements of medical care, epidemiology, and biomechanical sciences. All of these aspects are critical both to the evaluation and strategy of injury care but also the implementation and advertisement of the program. Haddon’s well established matrix and ten prevention strategies (based on the pre-event, event, and post-event phase of injury) provide the framework for the conception for all of these activities. Physicians play a critical role in this process as well as they are well positioned both as injury data collectors, care givers following injury events and educators to patients and the public for prevention strategies. By properly embracing this leadership role, physicians contribute to safer communities through reduction of injury at the local, state, and national level.
References
NCIPC: Web-based Injury Statistics Query and Reporting System (WISQARS). http://www.cdc.gov/injury/wisqars/index.html. Accessed 20 June 2011.
Finkelstein E, Corso PS, Miller TR. The incidence and economic burden of injuries in the United States. Oxford: Oxford University Press; 2006.
National Center for Health Statistics (U.S.). Division of Health Care Statistics: National hospital discharge survey: 2007 summary. In: National health statistics reports. Hyattsville, Md.: Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics; 2010.
National Trauma Data Bank Annual Report; Clarke DE, Fantus RJ (Eds), Chicago: American College of Surgeons; 2007.
McDonald EM et al. Injury prevention activities in U.S. trauma centres: are we doing enough? Injury. 2007;38:538–47.
National Committee for Injury Prevention and Control (U.S.). Injury prevention: meeting the challenge. New York: Oxford University Press; 1989.
Miniño AM, Murphy SL, Xu J, Kochanek KD. Deaths: final data for 2008. Natl Vital Stat Rep. 2011;59(10):1–22.
National Highway Traffic Safety Administration. Traffic safety facts: crashes. 2009 data. Washington, DC: NHTSA; 2011.
Barss P. Injury prevention: an international perspective: epidemiology, surveillance, and policy. Oxford: Oxford University Press; 1998.
Bonnie RJ et al. Reducing the burden of injury: advancing prevention and treatment. Washington, DC: National Academy Press; 1999.
Krug EG et al. World report on violence and health. Geneva: World Health Organization; 2002.
Mock C et al. Advancing injury prevention and trauma care in North America and globally. Surg Clin North Am. 2007;87:1–19.
Martinez R. Injury control: a primer for physicians. Ann Emerg Med. 1990;19:72–7.
Baker SP. The injury fact book. 2nd ed. New York: Oxford University Press; 1992.
Branas C. Injury prevention. In: Flint LM, editor. Trauma: contemporary principles and therapy. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2008. p. 99–103.
De Haven H. Mechanical analysis of survival of falls from heights of fifty to one hundred and feet. War Med. 1942;2:586–96.
Gordon JE. The epidemiology of accidents. Am J Public Health Nations Health. 1949;39:504–15.
Haddon Jr W. Advances in the epidemiology of injuries as a basis for public policy. Public Health Rep. 1980;95:411–21.
Haddon Jr W. Energy damage and the 10 countermeasure strategies. Inj Prev. 1995;1:40–4.
Maier RV. Injury prevention. In: Feliciano DV, Mattox KL, Moore EE, editors. Trauma. 6th ed. New York: McGraw-Hill; 2008. p. 41–56.
What works and what doesn’t work to improve highway safety. In: Status report. Insurance Institute for Highway Safety; 2001;36(5):1–7.
Waller J. Prevention of premature death and disability due to injury. In: Maxcy KF et al., editors. Public health and preventive Medicine. Stamford, CT: Appleton & Lange; 1998.
Baker SP. On lobbies, liberty, and the public good. Am J Public Health. 1980;70:573–5.
Robertson LS. Injuries—causes, control strategies, and public policy. Lexington, MA: Lexington Books; 1983.
Nelson GD, Moffit PB. Safety belt promotion: theory and practice. Accid Anal Prev. 1988;20:27–38.
Baker SP, Teret SP. Freedom and protection: a balancing of interests. Am J Public Health. 1981;71:295–7.
Williams AFG, Burchman PF. Motorcycle helmet use in relation to legal requirements. Accid Anal Prev. 1979;11:271–3.
AUA men’s health check list. http://www.auanet.org/content/media/COM-1552_MensHealthChecklistNoCrops.pdf. Accessed 19 Oct 2012.
Equipment check list. http://www.littleleague.org/Assets/forms_pubs/asap/EquipmentChecklist.pdf. Accessed 19 Oct 2012.
Paquette EL. Genitourinary trauma at a combat support hospital during Operation Iraqi Freedom: the impact of body armor. J Urol. 2007;177:2196–9.
Waxman S. Lower urinary tract injuries in Operation Iraqi Freedom (OIF) and Operation Enduring Freedom (OEF). Mil Med. 2012;177:621–3.
Serkin F, Soderdahl D, Hernandez J, et al. Combat urologic trauma in US military overseas contingency operations. J Trauma. 2010;69:S175–8.
Owens BD, Kragh Jr JF, Wenke JC, et al. Combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom. J Trauma. 2008;64:295–9.
Smith III TG, Wessells H, Mack CD, et al. Examination of the impact of airbags on renal injury using a national database. J Am Coll Surg. 2010;211:355–60.
Kuan JK, Kaufman R, Wright JL, et al. Renal injury mechanisms of motor vehicle collisions: analysis of the crash injury research and engineering network data set. J Urol. 2007;178:935–40.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Smith, T.G. (2013). Injury Prevention. In: Wessells, H. (eds) Urological Emergencies. Current Clinical Urology. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-62703-423-4_2
Download citation
DOI: https://doi.org/10.1007/978-1-62703-423-4_2
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-62703-422-7
Online ISBN: 978-1-62703-423-4
eBook Packages: MedicineMedicine (R0)