
Key Points
-
Available studies on body fat distribution and menopause suggest that menopause is associated with an acceleration in the accumulation of abdominal adipose tissue, and most likely, intra-abdominal fat.
-
This trend toward central obesity favors increased cardiovascular, cancer, and metabolic risks, and may partially mediate the increased morbidity and mortality after menopause.
-
Compared with other races and ethnic groups, Asians such as Chinese, Japanese, and Singaporeans were reported to be with lower BMI but with higher percent body fat and more abdominal fat at any given level of BMI.
-
Chinese women undergoing menopausal transition and postmenopausal women were associated with decreased lean mass, and increased percent body fat, trunk fat mass, and trunk–leg fat mass ratio comparing with women remained premenopausal.
-
Limited evidence identified the effect of menopause on fat distribution among Chinese women; however, more research was needed to confirm the findings with longitudinal design, larger sample size, and more advanced measuring technologies.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Obesity is a medical condition in which excess body mass has accumulated to the extent that it may cause an adverse effect on health, leading to reduced life expectancy and/or increased health problems including cardiovascular disease, type 2 diabetes, cancer, osteoarthritis and so on [1]. Changes in body composition, including the amount and distribution of body fat, are important predictors of cardiovascular risk. In particular, abdominal fat accumulation is associated with increased risks for cardiovascular diseases [1, 2]. Menopause is commonly defined as the absence of menses for 12 consecutive months. Endocrine changes resulting from menopause not only lead to cessation of reproduction and accompanying symptoms in women, but also dramatically impact health in postmenopausal life. Recent studies have found that change of body composition may mediate the relationship between menopause and adverse health outcomes. The findings about effects of menopause on body composition have been inconsistent due to different study design and characteristics of target populations: some studies have observed a progressive increase in fat mass, decrease in lean mass, and a shift to a more central body fat distribution caused by menopause, but others have not, especially after controlling the effects of aging [3–5]. This chapter discusses the effects of menopause on body composition and potential behind mechanisms with particularly Chinese aspects.
Menopause and Body Composition
Two patterns of body fat distribution have been usually observed, the accumulation of fat in the central region (android or apple shape) and the accumulation of fat in the gluteo-femoral region (gynoid or pear shape). The accumulation of fat in the central region (intra-abdominal) has been linked to increased risk of cardiovascular diseases independent of overall obesity. Despite conflicting results, menopause was believed to associate with weight gain, increased fat mass and abdominal fat, and a shift to a more central, android body fat distribution.
Menopause, Body Weight and Total Body Fat
Women tended to gain weight with aging, and many women reported their weight gain started around the time of their menopause [6]. A number of studies on Caucasian middle-aged women reported an annual weight gain of about 0.5 kg or more, however there did not appear to be an independent effect of menopause on the weight gain [7, 8]. Wing et al. studied 485 US women who were initially premenopausal and followed them for 3 years during which 61 were postmenopausal, 94 were perimenopausal, and 279 were still premenopausal. However, they found the weight gain was similar in the women who remained premenopausal and those who had a natural menopause [8]. In a comparison of premenopausal and postmenopausal Caucasian women matched for age, premenopausal women actually had a higher mean body weight [5, 9]. These evidence suggest that weight gain in midlife among women per se is more consistent with a pattern of chronologic aging, and not uniquely due to the menopausal transition.
Nevertheless, body weight consists of many compartments and components, and thus weight change alone is not an adequate indicator to the underlying changes in body composition that occur during menopause [6]. Wang and colleagues found that total lean mass decreased during the menopausal transition among Danish women [4], which indicated that increases in fat mass may occur with menopause despite a lack of change or even a reduction in body weight. Toth et al. claimed that total body mass was 28 % higher and percentage fat was 17 % higher in postmenopausal than in premenopausal US women, and a similar pattern of differences in total adiposity was noted in subsamples of premenopausal and postmenopausal women matched by age [10]. A longitudinal analysis of 6-year changes in body composition among African-American and Caucasian women showed menopause was associated with substantial weight gain, significant increases in fat mass, and loss of skeletal muscle mass. The pattern of change in weight is linear, suggesting only an age effect, whereas the changes in fat mass and skeletal muscle mass were more with curvilinear pattern over time, suggesting a menopause effect [11, 12].
Menopause and Central Fat Distribution
In addition to body weight and total fat, more literature suggested that it was not just the amount of fat but also its distribution that determined the risk associated with obesity [13]. Excess abdominal fat is as great a risk factor for disease as excess body fat per se [1]. Although some studies using anthropometric measurements of abdominal fat distribution most often failed to detect an effect of the menopause transition after adjust for age [14, 15], both cross-sectional [16] and longitudinal studies [9, 17] have shown a menopause-related increase in central adiposity among Caucasians, independent of the effect of age and total body adiposity. By comparing postmenopausal with age-matched controls premenopausal US women, Poehlman et al. found that the transition to menopause was associated with an increase in the waist-to-hip ratio (WHR) and total body fat [17]. Using data from the Study of Women’s Health Across the Nation (SWAN) among African-American and Caucasian women, Sowers et al. found that waist circumference (WC) continued to increase over time but the rate of increase slowed approximately 1 year after the final menstrual period, which indicated that both chronological aging and ovarian aging contribute to substantial changes in WC [12]. However, in subsequent SWAN longitudinal analyses with longer follow-up and including Japanese and Chinese women, change in waist seemed to be linear in relation to the final menstrual period [5].
The dual energy X-ray absorptiometry (DXA) provides more details information on whole-body and regional estimates of fat mass, even though this technique does not differentiate subcutaneous from intra-abdominal adipose tissue compartments [18]. Several studies have reported a shift toward abdominal fat distribution among African-Americans and Caucasians at menopause based on DXA data [12, 19–21]. Dawson-Hughes and Harris studies body composition changes across a 1-year period in 125 postmenopausal US women and found an increase in trunk fat measured by DXA. However, as there was no premenopausal comparison group in this study, it is not clear whether this change was due to menopause per se or aging [22, 23]. Gambaccianni and colleagues examined DXA measured trunk fat in a sample of premenopausal, perimenopausal, and postmenopausal Caucasian women, and found both perimenopausal and postmenopausal women had higher total and central body fat compared to premenopausal women. The effect of the menopause was further confirmed in a subgroup of women matched for age and body mass index (BMI) [24].
Menopause and Ectopic Fat
Ectopic fat is defined as excess adipose tissue in locations not classically associated with adipose tissue storage, such as visceral, heart, liver, and bone marrow [2]. Ectopic fat is an important predictor of metabolic (in particular insulin resistance) and cardiovascular disease, carrying more risk than general fat accumulation [25]. For instance, intra-abdominal visceral fat is most highly associated with increased health risks, and some studies indicate that visceral obesity may be a better predictor of morbidity and mortality related to cardiovascular diseases and type 2 diabetes than general obesity [26].
Computed tomography (CT) is current gold standard technique which can quantify both subcutaneous and intra-abdominal adipose tissue depots [27]. Toth and colleagues found that postmenopausal African-American and Caucasian women had a 49 % greater intra-abdominal and a 22 % greater abdominal subcutaneous fat area compared to premenopausal women. The menopause-related difference in intra-abdominal fat persisted after statistical adjustment for age and total body fat mass, whereas no difference in abdominal subcutaneous fat was noted [10]. Enzi et al. have reported that postmenopausal Italian women have a decreased subcutaneous-to-visceral fat ratio measured by CT scan comparing to age-matched premenopausal women [28]. Similar findings were reported by Lovejoy et al. in a longitudinal study in which they found that all African-American and Caucasian women gained subcutaneous fat over time but only those who became postmenopausal had a significant increase in visceral adipose tissue [3]. However, studies using the magnetic resonance imaging (MRI) reported no significant effect for menopause on abdominal fat accumulation. Schreiner et al. concluded that menopause did not accelerate intra-abdominal fat accumulation, though a very small sample of postmenopausal US women was examined in this study [29].
Recent findings suggested an association between bone marrow fat and bone loss, and osteoporosis has been proposed as the “obesity of bone” [30]. However, little literature was available for the change of bone marrow fat during menopause, and whether this change is associated with menopause-induced osteoporosis. Using proton (1H) magnetic resonance spectroscopy (MRS), Griffith found that in females vertebral marrow fat content rose sharply between 55 and 65 years of age while in males vertebral marrow fat content rose more slowly throughout life with no sharp rise in above range of age [31]. This increased deposition in marrow fat concurs with recognized changes in extraosseous fat distribution in postmenopausal females, which suggested that the bone marrow fat deposition may be menopause-related. More studies are needed before any conclusion can be made.
In summary, there are discrepancies in previous cross-sectional studies which may be related to the methodology used for the measurement of body fat distribution. Studies using anthropometric measures (WC or WHR) more likely failed to detect the difference independent of age and total fat. DXA and CT led to the conclusion that the menopause accelerated the selective deposition of intra-abdominal fat. Available longitudinal studies supported an increase in central fat accumulation occurring with menopause.
Mechanism Behind Menopause and Body Composition
The sex hormones have been suggested to play a critical role in menopause-related changes in body fat and fat distribution. Menopause is of occurrence with decline of estrogen levels. A number of studies reported that menopause-induced hormonal changes may be associated with abdominal fat distribution. Haffer et al. found that in postmenopausal Mexican-American and non-Hispanic white women overall adiposity and an unfavorable body fat distribution are associated with decreased sex hormone binding globulin (SHBG) concentration [32]. Observational studies and clinical trials have showed the effect of hormone replacement therapy (HRT) on fat distribution [33, 34]. The HRT using among postmenopausal women was associated with prevention, attenuation, or delay of abdominal fat accumulation related to menopause [35]. Therefore, changes in fat distribution during menopausal transition may be related to the dynamics of hormone such as estrogens and SHBG.
The physiologic basis for the shifting fat distribution after menopause appears to be a decreased lipoprotein lipase activity in femoral adipocytes and a loss of the high lipolytic responsiveness of abdominal and mammary adipocytes that is observed in premenopausal women [36]. Thus, unlike premenopausal women, postmenopausal women do not preferentially deposit fat in the periphery but are equally likely to deposit fat in adipose depots in the trunk. Lindberg et al. have also shown that treatment with estrogen in postmenopausal women restores the lipoprotein lipase activity of the femoral adipocytes [37].
In contrast to the stable patterns of daily food intake observed in males of many species, in females of many species caloric intake are cyclic and correlate with phases of the menstrual or estrous cycle [23]. When estrogen is elevated and progesterone is low, female show a significant decrease in caloric intake. Furthermore, it has been reported in female rodent models, physiologic levels of estrogen within the estrus phase was inversely related to food intake [23, 38]. Given the data linking changes in estrogen levels to alterations in food intake across the menstrual cycle, it might be expected that the decrease in estrogen at menopause may cause changes in eating behavior. Unfortunately, few studies have investigated the effect of menopause on food intake. A recent study found a decrease of energy intake after the onset of menopause compared with 3–4 years before the onset, but a slightly increase were found 2 years after the menopause [3].
In addition to affecting total energy intake, cyclic fluctuations in reproductive hormones also affect preference for macronutrients, such as fat and carbohydrate. In female rodents, low levels of estradiol during the luteal phases of the cycle are associated with increased preference and intake of fat [39]. In a recent longitudinal study, after adjustment for changes in total energy intake, protein, carbohydrate seem to decline overtime and were relatively higher in the years preceding onset of menopause than those after menopause. In contrast, fat intakes were higher 2 years after menopause onset compared with menopause onset and tended to increase over time [3].
Current literature indicated that natural menopause may be associated with reduced energy expenditure during rest and physical activity, both of which could contribute to a positive energy balance and weight gain in menopausal women [23]. Women experience a gradual fall in resting metabolic rate after menopause. In a recent study, 24 h energy expenditure and sleeping energy expenditure decreased significantly with age, however, the decrease in sleeping energy expenditure was 1.5-fold greater in women who become postmenopausal compared with premenopausal controls [3]. There appear to be at least two components contribute to this change. First, it has been reported that menopausal women have slightly decreased resting metabolic rate because of the loss of fat free mass [6, 23]. Fat free mass plays a major role in RMR, and can explain 63 % variations in resting metabolic rate [40]. Furthermore, changes in fat-free mass, including a postmenopausal decline in both soft lean tissue mass and bone mass, are mainly menopause-related [4]. Second, the decreased metabolic rate in postmenopausal women may be due in part to the loss of ovarian function and luteal phase of the menstrual cycle, which can theoretically reduce energy expenditure by about 15,000–20,000 Kcal per year [6]. Cyclic variation in resting energy expenditure was found in premenopausal women. During the 14-day luteal phase following ovulation, core temperature increased, as well as 8–16 % increase in total energy expenditure measured by direct and indirect calorimetry [6, 41].
The estrogen/testosterone pathway may play an important role in the regulation of physical activity [42]. In rodents, wheel running is reduced after surgical/pharmacological gonadectomy and is increased after hormones are reinforced via capsules or injections. However, in human subject, whether the decline in hormone concentration after menopause will cause a reduction in physical activity is still unclear. Dorn et al. investigated breast cancer risk in premenopausal and postmenopausal US women with and without cancer. As a component of this analysis, the researchers asked the subjects to recall their strenuous physical activity patterns during the previous 2 years, and found a reduction in physical activity level after menopause [43]. In a recent longitudinal study, physical activity decreased 30.2 % in subjects who were initially premenopausal and then become postmenopausal during the follow-up. However, in subjects who remain menopause, it decreased even a slightly higher (38.7 %), which suggest an aging effect rather than menopause effect.
Chinese Aspects
Compared with other races and ethnic groups, Asians such as Chinese, Japanese, and Singaporeans were reported to be with lower BMI but with higher percent body fat and more abdominal fat at any given level of BMI [44–47]. Chinese women in early menopausal transition were noted with the lowest unadjusted level of serum estradiol and SHBG comparing to other ethnic groups in SWAN study. The BMI was significantly correlated with all reproductive and somatic hormones measured in the perimenopause [48]. Therefore, the effect of menopause on fat and fat distribution may be different for Chinese women.
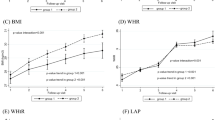
The evidence on changes of body composition during menopausal transition was extremely limited in Asian, particularly Chinese population. Teh et al. revealed an age-related increase in abdominal fat, but they did not consider the effect of menopause in their study [49]. Including menopause effect in a cross-sectional study, Sternfeld and colleagues reported a lower lean mass and possibly higher percent body fat in perimenopausal and postmenopausal Chinese women than in those in other ethnic groups [21]. Only one longitudinal study was available to date to evaluate the changes of body composition during menopausal transition in Chinese women [50]. A total of 438 middle-aged Chinese women aged 44–55 years were recruited with 30-month follow-up in Hong Kong. After controlling age, age of menarche and education level, women undergoing menopausal transition and postmenopausal women were associated with decreased lean mass, and increased percent body fat, trunk fat mass, and trunk–leg fat mass ratio comparing with women remained premenopausal (Fig. 20.1).

Baseline cross-sectional body composition measurements by age-menopausal status, adjusted for body mass index (kg m−2). Adapted from [50]
More studies with longitudinal design were encouraging to examine the effect of menopause on body composition among Chinese women. No Asian studies examined intra-abdominal fat changes during menopausal transition using CT, current gold standard to measure body composition. More research was warranted in Chinese menopausal women.
Conclusion
In conclusion, careful examination of available studies on body fat distribution and menopause suggested that menopause was associated with an acceleration in the accumulation of abdominal adipose tissue, and most likely, intra-abdominal fat. This trend toward central obesity favors increased cardiovascular, cancer, and metabolic risks, and may partially mediate the increased morbidity and mortality after menopause. Limited evidence identified the effect of menopause on fat distribution among Chinese women; however, more research was needed to confirm the findings with longitudinal design, larger sample size, and more advanced measuring technologies.
Abbreviations
- WHR:
-
Waist-to-hip ratio
- SWAN:
-
Study of women’s health across the nation
- WC:
-
Waist circumference
- DXA:
-
Dual energy X-ray absorptiometry
- BMI:
-
Body mass index
- CT:
-
Computed tomography
- MRI:
-
Magnetic resonance imaging
- MRS:
-
Magnetic resonance spectroscopy
- SHBG:
-
Sex hormone binding globulin
- HRT:
-
Hormone replacement therapy
References
Consultation, W. H. O. Obesity: preventing and managing the global epidemic. World Health Organ Tech Rep Ser. 2000;894:i-xii, 1–253.
Britton KA, Fox CS. Ectopic fat depots and cardiovascular disease. Circulation. 2011;124(24):e837–41.
Lovejoy JC, Champagne CM, de Jonge L, Xie H, Smith SR. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int J Obes (Lond). 2008;32(6):949–58.
Wang Q, Hassager C, Ravn P, Wang S, Christiansen C. Total and regional body-composition changes in early postmenopausal women: age-related or menopause-related? Am J Clin Nutr. 1994;60(6):843–8.
Wildman RP, Sowers MR. Adiposity and the menopausal transition. Obstet Gynecol Clin North Am. 2011;38(3):441–54.
Heymsfield SB, Gallagher D, Poehlman ET, Wolper C, Nonas K, Nelson D, et al. Menopausal changes in body composition and energy expenditure. Exp Gerontol. 1994;29(3–4):377–89.
Brown WJ, Williams L, Ford JH, Ball K, Dobson AJ. Identifying the energy gap: magnitude and determinants of 5-year weight gain in midage women. Obes Res. 2005;13(8):1431–41.
Wing RR, Matthews KA, Kuller LH, Meilahn EN, Plantinga PL. Weight gain at the time of menopause. Arch Intern Med. 1991;151(1):97–102.
Bjorkelund C, Lissner L, Andersson S, Lapidus L, Bengtsson C. Reproductive history in relation to relative weight and fat distribution. Int J Obes Relat Metab Disord. 1996;20(3):213–9.
Toth MJ, Tchernof A, Sites CK, Poehlman ET. Effect of menopausal status on body composition and abdominal fat distribution. Int J Obes Relat Metab Disord. 2000;24(2):226–31.
Sternfeld B, Dugan S. Physical activity and health during the menopausal transition. Obstet Gynecol Clin North Am. 2011;38(3):537–66.
Sowers M, Zheng H, Tomey K, Karvonen-Gutierrez C, Jannausch M, Li X, et al. Changes in body composition in women over six years at midlife: ovarian and chronological aging. J Clin Endocrinol Metab. 2007;92(3):895–901.
World Health Organization, International Association for the study of Obesity, International Obesity TaskForce. The Asia-Pacific perspective: Redefining obesity and its treatment. Sydney: Health Communications; 2000.
Tchernof A, Poehlman ET, Despres JP. Body fat distribution, the menopause transition, and hormone replacement therapy. Diabetes Metab. 2000;26(1):12–20.
Pasquali R, Casimirri F, Pascal G, Tortelli O, Morselli Labate A, Bertazzo D, et al. Influence of menopause on blood cholesterol levels in women: the role of body composition, fat distribution and hormonal milieu. Virgilio Menopause Health Group. J Intern Med Mar. 1997;241(3):195–203.
Zamboni M, Armellini F, Milani MP, De Marchi M, Todesco T, Robbi R, et al. Body fat distribution in pre- and post-menopausal women: metabolic and anthropometric variables and their inter-relationships. Int J Obes Relat Metab Disord. 1992;16(7):495–504.
Poehlman ET, Toth MJ, Gardner AW. Changes in energy balance and body composition at menopause: a controlled longitudinal study. Ann Intern Med. 1995;123(9):673–5.
Lee SY, Gallagher D. Assessment methods in human body composition. Curr Opin Clin Nutr Metab Care. 2008;11(5):566–72.
Ley CJ, Lees B, Stevenson JC. Sex- and menopause-associated changes in body-fat distribution. Am J Clin Nutr. 1992;55(5):950–4.
Morita Y, Iwamoto I, Mizuma N, Kuwahata T, Matsuo T, Yoshinaga M et al. Precedence of the shift of body-fat distribution over the change in body composition after menopause. J Obstet Gynaecol Res. 2006;32(5):513–6.
Sternfeld B, Bhat AK, Wang H, Sharp T, Quesenberry Jr CP. Menopause, physical activity, and body composition/fat distribution in midlife women. Med Sci Sports Exerc. 2005;37(7):1195–202.
Dawson-Hughes B, Harris S. Regional changes in body composition by time of year in healthy postmenopausal women. Am J Clin Nutr. 1992;56(2):307–13.
Geiselman PJ, Smith SR. Estrogen’s role in the regulation of appetite and body fat. In: Kohlstadt I, editor. Scientific evidence for musculoskeletal, bariatric, and sports nutrition. Boca Raton, FL: CRC/Taylor & Francis; 2006.
Gambacciani M, Ciaponi M, Cappagli B, De Simone L, Orlandi R, Genazzani AR. Prospective evaluation of body weight and body fat distribution in early postmenopausal women with and without hormonal replacement therapy. Maturitas. 2001;39(2):125–32.
Gastaldelli A, Basta G. Ectopic fat and cardiovascular disease: what is the link? Nutr Metab Cardiovasc Dis. 2010;20(7):481–90.
Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–8.
Toth MJ, Tchernof A, Sites CK, Poehlman ET. Menopause-related changes in body fat distribution. Ann N Y Acad Sci. 2000;904:502–6.
Enzi G, Gasparo M, Biondetti PR, Fiore D, Semisa M, Zurlo F. Subcutaneous and visceral fat distribution according to sex, age, and overweight, evaluated by computed tomography. Am J Clin Nutr. 1986;44(6):739–46.
Schreiner PJ, Terry JG, Evans GW, Hinson WH, Crouse 3rd JR, Heiss G. Sex-specific associations of magnetic resonance imaging-derived intra-abdominal and subcutaneous fat areas with conventional anthropometric indices. The atherosclerosis risk in communities study. Am J Epidemiol. 1996;144(4):335–45.
Rosen CJ, Bouxsein ML. Mechanisms of disease: is osteoporosis the obesity of bone? Nat Clin Pract Rheumatol. 2006;2(1):35–43.
Griffith JF, Yeung DK, Ma HT, Leung JC, Kwok TC, Leung PC. Bone marrow fat content in the elderly: a reversal of sex difference seen in younger subjects. J Magn Reson Imaging. 2012;36(1):225–30.
Haffner SM, Katz MS, Dunn JF. Increased upper body and overall adiposity is associated with decreased sex hormone binding globulin in postmenopausal women. Int J Obes. 1991;15(7):471–8.
Sumino H, Ichikawa S, Yoshida A, Murakami M, Kanda T, Mizunuma H et al. Effects of hormone replacement therapy on weight, abdominal fat distribution, and lipid levels in Japanese postmenopausal women. Int J Obes Relat Metab Disord. 2003;27(9):1044–51.
Troisi RJ, Wolf AM, Mason JE, Klingler KM, Colditz GA. Relation of body fat distribution to reproductive factors in pre- and postmenopausal women. Obes Res. 1995;3(2):143–51.
Gambacciani M, Ciaponi M, Cappagli B, Piaggesi L, De Simone L, Orlandi R, et al. Body weight, body fat distribution, and hormonal replacement therapy in early postmenopausal women. J Clin Endocrinol Metab. 1997;82(2):414–7.
Rebuffe-Scrive M, Eldh J, Hafstrom LO, Bjorntorp P. Metabolism of mammary, abdominal, and femoral adipocytes in women before and after menopause. Metabolism. 1986;35(9):792–7.
Lindberg UB, Crona N, Silfverstolpe G, Bjorntorp P, Rebuffe-Scrive M. Regional adipose tissue metabolism in postmenopausal women after treatment with exogenous sex steroids. Horm Metab Res. 1990;22(6):345–51.
Mystkowski P, Schwartz MW. Gonadal steroids and energy homeostasis in the leptin era. Nutrition. 2000;16(10):937–46.
Lovejoy JC. The influence of sex hormones on obesity across the female life span. J Womens Health. 1998;7(10):1247–56.
Johnstone AM, Murison SD, Duncan JS, Rance KA, Speakman JR. Factors influencing variation in basal metabolic rate include fat-free mass, fat mass, age, and circulating thyroxine but not sex, circulating leptin, or triiodothyronine. Am J Clin Nutr. 2005;82(5):941–8.
Webb P. 24-hour energy expenditure and the menstrual cycle. Am J Clin Nutr. 1986;44(5):614–9.
Bowen RS, Turner MJ, Lightfoot JT. Sex hormone effects on physical activity levels: why doesn’t Jane run as much as Dick? Sports Med. 2011;41(1):73–86.
Dorn J, Vena J, Brasure J, Freudenheim J, Graham S. Lifetime physical activity and breast cancer risk in pre- and postmenopausal women. Med Sci Sports Exerc. 2003;35(2):278–85.
Wang J, Thornton JC, Russell M, Burastero S, Heymsfield S, Pierson Jr RN. Asians have lower body mass index (BMI) but higher percent body fat than do whites: comparisons of anthropometric measurements. Am J Clin Nutr. 1994;60(1):23–8.
Wang J, Thornton JC, Burastero S, Shen J, Tanenbaum S, Heymsfield SB, et al. Comparisons for body mass index and body fat percent among Puerto Ricans, blacks, whites and Asians living in the New York City area. Obes Res. 1996;4(4):377–84.
Frohlich MW, Parker DS. Running gels backwards to select DNA molecules larger than a minimum size. Biotechniques. 2001;30(2):264–6.
Lear SA, Humphries KH, Kohli S, Birmingham CL. The use of BMI and waist circumference as surrogates of body fat differs by ethnicity. Obesity (Silver Spring). 2007;15(11):2817–24.
Randolph Jr JF, Sowers M, Gold EB, Mohr BA, Luborsky J, Santoro N, et al. Reproductive hormones in the early menopausal transition: relationship to ethnicity, body size, and menopausal status. J Clin Endocrinol Metab. 2003;88(4):1516–22.
Teh BH, Pan WH, Chen CJ. The reallocation of body fat toward the abdomen persists to very old age, while body mass index declines after middle age in Chinese. Int J Obes Relat Metab Disord. 1996;20(7):683–7.
Ho SC, Wu S, Chan SG, Sham A. Menopausal transition and changes of body composition: a prospective study in Chinese perimenopausal women. Int J Obes (Lond). 2010;34(8):1265–74.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2013 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ma, X., He, W., Zhu, S. (2013). Fat and Fat Distribution in Menopause: Chinese Aspects. In: Hollins Martin, C., Watson, R., Preedy, V. (eds) Nutrition and Diet in Menopause. Nutrition and Health. Humana Press, Totowa, NJ. https://doi.org/10.1007/978-1-62703-373-2_20
Download citation
DOI: https://doi.org/10.1007/978-1-62703-373-2_20
Published:
Publisher Name: Humana Press, Totowa, NJ
Print ISBN: 978-1-62703-372-5
Online ISBN: 978-1-62703-373-2
eBook Packages: MedicineMedicine (R0)