
Abstract
Ureteropelvic junction obstruction (UPJO), defined as the functionally significant impairment of urinary transport from the renal pelvis to the proximal ureter, is the most common cause of hydronephrosis in newborns and young children. Left untreated, this condition may cause progressive dilation of the renal collecting system, with deterioration of renal function and loss of renal unit. UPJO has a diverse presentation, as it may be a primary congenital abnormality diagnosed prenatally, or secondarily acquired, and not apparent until late adolescence or adulthood. This chapter will focus on primary UPJO with review of the current methods of diagnosis and treatment options, as well as the authors’ approach to managing this condition.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
Ureteropelvic junction obstruction (UPJO), defined as the functionally significant impairment of urinary transport from the renal pelvis to the proximal ureter, is the most common cause of hydronephrosis in newborns and young children [1]. Left untreated, this condition may cause progressive dilation of the renal collecting system, with deterioration of renal function and loss of renal unit. UPJO has a diverse presentation, as it may be a primary congenital abnormality diagnosed prenatally, or secondarily acquired, and not apparent until late adolescence or adulthood. This chapter will focus on primary UPJO with review of the current methods of diagnosis and treatment options, as well as the authors’ approach to managing this condition.
Etiology and Epidemiology
The etiology of UPJO cannot be isolated to just one source. In children, UPJO is usually primary or congenital in nature, related to developmental abnormalities of the ureteropelvic junction or caused by extrinsic compression from anatomic variants. Less commonly it can be linked to secondary causes such as infection, vesicoureteral reflux (VUR), recurrent stone passage, or iatrogenic strictures from previous surgery.
Causes of primary intrinsic UPJO include an aperistaltic segment of the ureter from abnormalities of the ureteral musculature, congenital ureteral strictures due to excessive collagen deposition at a narrowed site, and ureteral fibroepithelial polyps [2] (Fig. 5.1). Primary extrinsic causes include high insertion of the ureter into the renal pelvis, ureteral kinking, and most frequently, vessels to the lower pole of the kidney that pass anterior to the ureteropelvic junction and intermittently cause obstruction (Fig. 5.2).

Primary intrinsic UPJO with a pathologic narrowed ureter at the ureteropelvic junction

Primary extrinsic UPJO from vessels to the lower pole of the kidney
The incidence of UPJO is approximately 1:500 with a male to female ratio of 2:1 [3]. It is more common on the left side than the right side and is reported to be bilateral in 10–40 % [3]. Associated anomalies, primarily of urologic origin, are common in those with congenital UPJO. VUR, albeit low grade, is found in 40 % of patients, renal dysplasia or multicystic dysplastic kidney disease is present in 10 %, unilateral kidney agenesis in 5 %, and VATER (Vertebral Anal Tracheal Esophageal Renal) syndrome in 20 % [1].
Presentation
The presentation of UPJO can be as varied as the etiologies of the disease. In the infant population, hydronephrosis is usually diagnosed prenatally with the use of maternal ultrasonography. These infants are typically asymptomatic at the time of delivery; however, approximately 10–30 % are found to have UPJO on postnatal evaluation [1]. In the absence of prenatal screening, infants with hydronephrosis can also present with an abdominal mass, feeding difficulties, failure to thrive, or sepsis.
In older children, presentation is typically characterized by a symptomatic episode of abdominal or flank pain and nausea and vomiting, called a Dietl’s crisis. Cyclic vomiting alone can also be a sign of intermittent UPJO; however this symptom complex is often misdiagnosed as gastrointestinal in origin. Less common presentations include urinary tract infection, hematuria, nephrolithiasis, and rarely hypertension. With the increased use of radiographic imaging, incidental diagnosis of asymptomatic UPJO is also prevalent.
Evaluation and Diagnosis
The evaluation of UPJO in the infant or child varies with presentation. The evaluation of infants with prenatally diagnosed hydronephrosis will be initiated at the time of birth. For older children, the evaluation of possible UPJO commences with their first Dietl’s crisis or clinically significant event.
Ultrasonography
For infants that have been diagnosed prenatally with hydronephrosis, a renal ultrasound should be obtained neonatally to reassess the dilatation of the renal collecting system.
Renal ultrasonography does not diagnose obstruction or predict resolution; however it can correlate with a clinically relevant obstructive process. When the anterior-posterior diameter of the renal pelvis is >15 mm, it is suggestive of the presence of obstruction, as is a trend of worsening hydronephrosis over time (Fig. 5.3). Renal size should be measured in the affected kidney and contralateral kidney over a period of time. As obstruction worsens, there tends to be an overall decrease in function and growth of the affected kidney with a compensatory hypertrophy of the contralateral healthy kidney.

Typical appearance of UPJO on ultrasound. Note dilated renal pelvis and calyces
Ultrasonography is also a useful tool in older children who present acutely. We commonly give our patients with a history of intermittent abdominal pain a prescription for a renal ultrasound, to be obtained at the time of an acute episode. This modality is a relatively simple, noninvasive test that can monitor dilation over time. It can easily be done in the office setting.
Computed Tomography
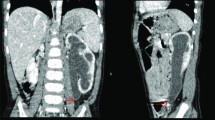
Computed tomography (CT) has not been the first-line imaging modality for the diagnosis of hydronephrosis or UPJO in children, particularly infants. This is primarily due to the radiation exposure risk of CT and the relative ease and accuracy of renal ultrasonography. However, many older children with UPJO, who present with nonspecific complaints of abdominal pain or nausea and vomiting, are evaluated with a CT scan to evaluate other possible causes of their symptoms such as appendicitis or bowel obstruction. Therefore, it is important to know the typical CT scan appearance of UPJO. Significant hydronephrosis is noted without the presence of a dilated ureter (Fig. 5.4). CT can be beneficial in defining retroperitoneal anatomy, particularly aberrant lower pole crossing vessels to the kidney. When performed with IV contrast, an overall functional assessment of the kidney can also be made; however the benefits of this modality often do not outweigh the radiation risk or cost of the study. CT as a primary imaging study should be evaluated on an individual basis after the risks and benefits have been considered.

CT appearance of UPJO obstruction. Note dilated renal pelvis and normal caliber ureter
Intravenous Pyelogram
Intravenous pyelography (IVP) has fallen out of favor in the work-up of hydronephrosis and suspected UPJO due to its high radiation exposure and the ease and accuracy of other imaging modalities such as ultrasonography. IVP can still be useful in those cases with unclear anatomy and a confusing clinical picture. The ideal timing for this study would be during an acute episode of obstruction.
Voiding Cystourethrogram
A voiding cystourethrogram (VCUG) should be performed in all children with prenatally diagnosed hydronephrosis to evaluate for the presence of VUR even if UPJO is suspected as the cause of collecting system dilatation. VUR is present in 40 % of children with UPJO, although it is usually low grade [1]. Infants with prenatal hydronephrosis should be started on prophylactic antibiotics at the time of birth, until the VCUG has confirmed the absence of VUR.
Diuretic Radionuclide Renography
Radionuclide renography is an objective study that is able to suggest the diagnosis of obstruction by analyzing quantitative data regarding differential renal function. When performed in conjunction with the administration of a diuretic, this test is able to assess the velocity of washout of the radioisotope from each kidney, hence a direct measurement of renal collecting system emptying. Initially, this test was performed with technetium-99 m diethylenetriaminepentaacetic acid (DTPA), an agent that is exclusively filtered by the glomeruli with an extraction excretion of 20 %, which provides an indirect measurement of GFR glomerular filtration rate (GFR) in nondilated kidneys [4]. This agent has largely been replaced by mercaptoacetyltriglycine (MAG3), which is excreted mostly by the proximal renal tubules and provides an indirect means of measuring estimated renal plasma flow. MAG3 radionuclide renography tends to provide more accurate functional information than DTPA radionuclide renography, particularly in dilated renal collecting systems, and has become the study of choice at most institutions.
The measurement of the excretory curve of the renogram will correlate with the efficiency of emptying of the renal pelvis. In an obstructed system, the radioisotope is not as effectively cleared from the kidney. Furosemide is usually given to promote diuresis and emptying. When the kidney does not respond to the diuretic, it is assumed that there is a loss of renal function and/or significant renal obstruction [4].
The technique and ultimately the results of the test are extremely operator dependent, and unfortunately there is no universal protocol for performing this study; therefore results can vary from center to center. The relative standard would be to perform this test in a well-hydrated child with a catheter draining the bladder, as a full bladder can lead to VUR in the susceptible ureter, or poor emptying in an otherwise unobstructed system. The administration of the diuretic can vary depending on the protocol used. It is our preference that the diuretic be administered 20–30 min after the renogram (F +20–30) or when the renal pelvis is filled with contrast, whichever is later. Following administration of the diuretic, the time to washout suggests the degree of obstruction.
The analysis of the drainage curve should take into consideration the technique and the time to diuretic administration. A general standard in analyzing the curve is to report the time it takes for the radioisotope activity to decrease by 50 % (T ½). If the T ½ is less than 10 min, the study is determined to be normal. When the T ½ is between 10 and 20 min, the study is equivocal, and if the T ½ is greater than 20 min, the kidney reportedly is obstructed (Fig. 5.5). Caution must be observed when taking these results at absolute face value, as the technique, the drainage curves, and the clinical condition of the child must be taken into consideration in the analysis. It should be noted that diuretic renography should not generally be performed in infants less than a month of age, as false-positive results may be obtained with an immature kidney.

Drainage curve of MAG3 diuretic radionuclide renography
Pressure Flow Study
A pressure flow study is an invasive test that measures the intrapelvic pressure during infusion of a fluid into the renal pelvis and the subsequent decrease in intrapelvic pressure over time. This is termed the pressure decay. The pressure decay represents the efficiency of urine transport as well as the relative compliance and volume of the collecting system [1]. A rapid pressure decay indicates a non-obstructed system, while a slow pressure decay demonstrates obstruction. Pressure flow studies are not routinely performed in the pediatric population and are usually used in equivocal clinical situations after a prior repair.
Management of Asymptomatic Patients
This category of patients is typically diagnosed prenatally or in infancy. Older management schemes included early surgical intervention within the first few months of life; however because many of these kidneys will improve spontaneously, most of these infants are managed initially with close monitoring and follow-up. There is some controversy; however the general consensus is that some patients will recover without intervention while others will progress and their renal function will deteriorate. The goal is to prevent children from having unnecessary surgery while balancing the need to intervene on the population that will deteriorate without intervention.
There are general guidelines that determine which patient is appropriate for observation. Typically patients with greater than 40 % split function of the affected kidney, stable hydronephrosis over time, stable renal function, and no urinary tract infections can be monitored closely without intervention. Renal ultrasounds should be performed every 3–4 months for the first year of life, followed by every 6 months for the next 2 years then annually. If there is a change in the renal ultrasound, diuretic radionuclide renography should be obtained. If there is greater than a 10 % decline in overall function of the affected kidney, surgical intervention should be considered.
Management of Symptomatic Patients
Patients with less than 40 % function of the affected kidney, those with progressing hydronephrosis on serial exams, or those that present clinically with colic, hematuria, stones, or infection should undergo operative intervention for the management of UPJO.
Open dismembered pyeloplasty has been the gold standard treatment of UPJO for decades, with contemporary success rates greater than 90 % [5]. However, the paradigm has begun to shift, and more minimally invasive techniques for treatment of this condition in children have been sought. Laparoscopic pyeloplasty is an accepted surgical standard for the treatment of UPJO in the adult population, and results in children have been promising. Recent outcomes of laparoscopic pyeloplasty in children are consistent with those for open pyeloplasty, with potentially less postoperative incisional discomfort, a quicker convalescence, and an excellent cosmetic outcome. In this section we will discuss the surgical options available and then describe our preferred technique.
Dismembered Pyeloplasty
Open pyeloplasty can be performed in a variety of ways; however the most commonly applied technique is the Anderson-Hynes dismembered pyeloplasty. This surgery can be performed in a flank, retroperitoneal, transperitoneal, or dorsal lumbotomy position. During this procedure the ureteropelvic junction is isolated and excised, and the proximal ureter is spatulated and reanastomosed to the renal pelvis. If crossing vessels from the lower pole of the kidney are present, the anastomosis is performed anterior to the vessels. Two key advantages to this procedure are the preservation of anomalous vessels to the kidney and the excision of the pathologic segment of the UPJ. The option of leaving the patient without a stent or nephrostomy tube is plausible with this type of repair. A small Penrose drain is often left in place for 24 h if a stent is not utilized.
Laparoscopic Pyeloplasty
With the desire to find less-invasive treatment options, there has been a recent interest in the development of minimally invasive surgical options for pediatric patients. The first pediatric series of transperitoneal laparoscopic dismembered pyeloplasty in the literature was reported in 1999, and since that time a variety of techniques and approaches have been described [5]. The technique overall is the same as the open dismembered pyeloplasty, in that the diseased segment is excised and the proximal ureter is spatulated and reapproximated to the renal pelvis. Transperitoneal, retroperitoneal, and robotic approaches have all been reported, with advocates for each procedure. In the end, the approach used should be based on the experience and comfort of the operating surgeon. Success rates for this procedure have been reported in the literature to be comparable to the open technique [5]. At our institution, we primarily perform transperitoneal laparoscopic dismembered pyeloplasty in children with UPJO, greater than 4 months of age, in need of operative repair. In our series we have not had any major complications, and in 90 patients our overall success rate is greater than 95 %.
Robotic-assisted laparoscopic pyeloplasty has been reported in the pediatric urology literature [6]. The benefit of performing the repair robotically assisted is that it allows three-dimensional visualization and 6° of wrist movement, making suturing more intuitive and lowering the learning curve. However, the use of the robot requires additional and larger ports as compared to standard laparoscopy, and the overall cost of equipment and training is much higher. In addition, the robot is not universally available.
Endoscopic Procedures
Endoscopic procedures for the correction of UPJO are commonly performed in adults, however with lower success rates than open or laparoscopic pyeloplasty. This application has not been found to be useful as a primary treatment option for children. Endopyelotomy (endoscopic incision through the narrowed area) may be performed in either an antegrade or retrograde manner and can be useful in children who have failed open or laparoscopic pyeloplasty.
Complications and Follow-Up
Complications from pyeloplasty, open or laparoscopic, are fairly uncommon. Early complications include urinary tract infection and prolonged urinary leakage from the anastomosis. This is usually treated with placement of a ureteral stent and/or Foley catheter drainage. Late complications include lack of improvement or worsening hydronephrosis, continued pain, urinary tract infections, or worsening renal function. In rare occasions, a redo pyeloplasty or ureterocalycostomy may need to be performed.
With long-term pyeloplasty success greater than 90 %, the follow-up for UPJO consists of office evaluations and imaging. In our practice, the patients have an office ultrasound performed 6 weeks and 6 months after their procedure. If there is clinical and radiographic improvement, yearly ultrasounds may or may not be recommended going forward. If the hydronephrosis worsens or the child remains symptomatic, radionuclide renography should be obtained for further evaluation.
Conclusions
UPJO is the most common cause of significant hydronephrosis in newborns and young children. With a diverse presentation, it may manifest as a congenital abnormality or secondarily acquired later in life. The evolution of the management of UPJO in the pediatric population has shifted from early intervention to observational conservative management; however, the overall goal of treatment is to preserve renal function. Surgical options for treatment have remained the gold standard with high long-term success rates. There has been a recent push toward minimally invasive techniques to further decrease the morbidity of surgical treatment options.
References
Hsu THS, Streem SB, Nakada SY. Management of upper urinary tract obstruction. In: Wein AJ, editor. Campbell-Walsh urology, vol. 4. 9th ed. Philadelphia: Saunders; 2007. p. 3359–82.
Hanna MK, Jeffs RD, Sturgess JM, Barkin M. Ureteral structure and ultrastructure: part II. Congenital ureteropelvic junction obstruction and primary obstructive megaureter. J Urol. 1976;116:725–30.
Sidhu G, Beyene J, Rosenblum ND. Outcome of isolated antenatal hydronephrosis: a systematic review and meta-analysis. Pediatr Nephrol. 2006;21:218–24.
Gonzalez R, Schimke CM. Ureteropelvic junction obstruction in infants and children. Pediatr Clin North Am. 2001;48:1505–18.
Tan BJ, Smith AD. Ureteropelvic junction repair: when, how what? Curr Opin Urol. 2004;14:55–9.
Lee RS, Borer JG. Robotic Surgery for ureteropelvic junction obstruction. Curr Opin Urol. 2006;16:291–4.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2014 Springer Science+Business Media New York
About this chapter
Cite this chapter
Sweeney, D.D., Docimo, S.G. (2014). Ureteropelvic Junction Obstruction in the Pediatric Population. In: Rabinowitz, R., Hulbert, W., Mevorach, R. (eds) Pediatric Urology for the Primary Care Physician. Current Clinical Urology. Humana Press, New York, NY. https://doi.org/10.1007/978-1-60327-243-8_5
Download citation
DOI: https://doi.org/10.1007/978-1-60327-243-8_5
Published:
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-60327-242-1
Online ISBN: 978-1-60327-243-8
eBook Packages: MedicineMedicine (R0)