
Abstract
As life expectancy has increased, so has the number of the elderly population that have developed end stage renal disease. Ultimately, thet may face the choice of whether to dialyze or not. This chapter will look at the challenges this elderly group faces and the benefits that home hemodialysis may offers. It is proposed that this mode of dialysis offers a viable option to the current in-center therapies for the high comorbidity population. As dialysis system become more user friendly and the benefits of home hemodialysis become more apparent, it is important to introduce information about treatment options early in the patient’s disease process. Early education and encouragement for both patient and their support system become the keys to both acceptance and success.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The Dialysis Population
Chronic renal failure requiring dialysis had been on the increase for several years until 2007 when the incidence of new end-stage renal disease (ESRD) patients per million population fell by 2.0 % (Fig. 4.1). The growth of patients ages 65–74, however, has increased which may be a reflection of the “baby boomers” developing renal failure (Fig. 4.2). Additionally, treatment of the elderly may be increasing due to longer life spans, a greater acceptance of dialysis as a modality to sustain life, and the availability of dialysis because of the proliferation of dialysis centers. For the first time in 2010, the number of patients doing in-center hemodialysis declined, and the number of patients that started home therapies, in particular, peritoneal dialysis, increased. For the majority of elderly patients with renal failure, the choice of therapy has been in-center dialysis with 96 % performing in-center hemodialysis, 3.5 % doing CAPD/CCPD, and only 0.3 % home hemodialysis [1].

Incidence of new ESRD patients (U.S. Renal Data System, USRDS 2011 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2011)

Ages of new ESRD patients (U.S. Renal Data System, USRDS 2011 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2011)
Longevity in the general population varies significantly from country to country with Japan having the longest life span averaging 82.73 years (79.25 years for men and 86.06 years for women). Compared to Japan, the United States is ranked number 40. Men in the United States reach an average age of 75.25 and women 80.51 years of age with the overall average age of 75.35 years [2]. With the average lifespan of Americans being 75.35 years, it can be assumed that the elderly starting dialysis at age 70 or older would normally have only five years of survival remaining. Although the United States has a lower life expectancy than many other countries, there are a greater number of dialysis patients in the elderly group. In some countries with socialized medicine, there has been a perception of a low acceptance rate for elderly patients for dialysis. This acceptance rate has appeared to change in the UK with the advent of peritoneal dialysis, a less costly option [3]. Dialysis rationing has been described in South Africa because of too few dialysis facilities and health care workers. In the United States in the 1960s, there was a similar rationing of dialysis before Medicare and private insurance provided coverage for long-term dialysis [4]. With Medicare and privatized insurance, the United States has not placed age restrictions on dialysis so far. If the nephrologists feel the patient is able to tolerate the therapy, dialysis is an option to prolong one’s life or act as a bridge until kidney function returns to baseline. Therefore, it is not uncommon to see 80- or 90-year-old patients being placed on dialysis, potentially prolonging life beyond their normal longevity.
The Move Away from Home Therapies
The first home hemodialysis in the United States was performed by Nose in 1961 [5]. With the development of the Scribner shunt, home hemodialysis began to flourish. By the 1970s, home hemodialysis accounted for as much as 40 % of all patients on dialysis. The prevalence of home hemodialysis began to fall, however, as the numbers of dialysis facilities increased and reimbursement through Medicare made payment of the treatment possible, whether at home or in-center.
Today there is considerable diversity worldwide among therapies chosen for dialysis. In New Zealand and Australia, home hemodialysis is performed on 16.3 % and 9.3 % of the ESRD population, respectively, as compared to 0–3.3 % in other countries (Fig. 4.3).

Renal replacement therapies in different countries (U.S. Renal Data System, USRDS 2011 Annual Data Report: Atlas of End-Stage Renal Disease in the United States, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2011)
International Trends in Home Hemodialysis
There is considerable disparity in the use of home therapies for dialysis between countries. Australia and New Zealand have always had a much higher population of home patients, but in many countries, the prevalence of home hemodialysis has fallen. Remarkably, Australia and New Zealand have maintained a high number on home hemodialysis. In a review by Disney from 1995, in Australia 68 % of the patients were receiving hemodialysis and 31 % CAPD. Of the patients dialyzing at home, the majority (62 %) used CAPD, and the remainder were on home hemodialysis. In New Zealand, 44 % of the patients are on hemodialysis with 83 % dialyzing at home. The majority (65 %) use CAPD [6]. In these countries, like others, there has been a declining home hemodialysis population, but there has been a resurgence of interest driven by a variety of factors. These include the desire for cost containment and the lower mortality risk compared to in-center treatments and peritoneal dialysis.
Mcgregor, Agar, and Blagg reviewed international trends in home hemodialysis and found little correlation to other renal replacement therapies, disease states, healthcare expenditures, or population density. They did find a strong correlation between national per capita healthcare expenditure and provision of renal replacement therapies, but no correlation with the use of home hemodialysis. Gross national income per capita also had no correlation with home hemodialysis, and there was an inverse correlation between median age and home hemodialysis [7]. In part, the resurgence of interest in home hemodialysis has been sparked by the advent of nocturnal dialysis. Performing the therapy at night gives the patient improved quality of life, more dietary and fluid freedom, need for fewer antihypertensive medications and phosphate binders, return of daytime freedom, and the capacity for full-time employment. Moreover, home hemodialysis has been found to be less expensive than in-center treatments due to the elimination of the high cost of nursing care and building costs.
Machine Options for Home Hemodialysis
There are currently two machines generally available for home hemodialysis. The Fresenius Home K is an adaption of the K in-center machine with software that helps the patient and support person doing home dialysis (Fig. 4.4).

Fresenius Home K machine
It leads the patient and helper through the process of setting up the tubing and priming the machine. Its size is smaller than the K machine and has a connection to the Internet that can allow central monitoring from a national center. The device for central monitoring is called the iCare Monitoring (Fig. 4.5).

iCare Monitoring (http://www.fmcna.com/fmcna/HomeTherapies/iCareMonitoring/icare.html)
To further protect the patient, a wireless wetness detector can be placed near the needle sites, and if wetness is detected, the device will stop the blood pump (Fig. 4.6).

Wireless wetness detector (http://www.fmcna.com/fmcna/HomeTherapies/home-therapies.html)
The Home K does require a special water system that is dependent on the quality of the patient’s local water. Deionizing tanks may be required in addition to the reverse osmosis system to create quality water. Space may be a limiting factor in using a Home K machine.
The Home K machine has been used for both daytime and nocturnal dialysis. In some centers a standard K machine or other standard hemodialysis machine may be used for home therapy. These machines would not offer a step-by-step procedure on the computer screen to lead the patient through the process and would not have the Internet connection for central monitoring.
The Home K machine requires two 20 amp separate circuits. One circuit is needed for the Home K machine itself and one circuit for the reverse osmosis system. A GFI (Ground Fault Interrupter) is mandatory to prevent any circuit overload. The water does not have to meet EPA standards, and it uses cold water. The minimal standard PSI is 40 for well water.
The NxStage machine was developed especially for home therapies but is also used for in-hospital CRRT (Fig. 4.7). The treatment has a unique process of treatment for uremia utilizing a slow dialysate flow rate that maximally concentrates urea and other uremic toxins in the filtrate. By using a very slow dialysate flow rate, a smaller amount of fluid is required. While being very efficient, the slow rate may not remove toxins as effectively because of the super saturation of the dialysate solution. Nevertheless, the device has rejuvenated interest in home hemodialysis because it is easier to learn with very intuitive steps to carry out the therapy.

NxStage machine (http://www.rubindialysis.org/homeTherapy.html)
The dialyzer and tubing are packaged as a single disposable unit making it possible to set up the machine in only 15 min. Using replacement fluid bags, the device does not require a special water system; however, the downside of using replacement bags is a higher cost per treatment as the bags are more expensive as compared to a K machine with a separate water treatment system. By using the company’s Pureflow device to create sterile dialysate solution, the overall cost can be reduced.
The water must meet EPA standards to use Pureflow. In areas of the country where the nitrate and sulfate concentrations are high, Pureflow cannot be used. The water connects directly to the faucet, garden hose, washing machine, or below the sink. All of these attachments come with the NxStage kit. The blue water source line is standard and cannot be lengthened. The drain line has a maximum of 40 ft, and the electrical connection is a grounded outlet only.
There have been other machines that have come and gone over time which have been used for home hemodialysis. One example is the AKSYS home dialysis machine that was designed specifically for home hemodialysis. The system was disinfected by heat but did experience several problems with breakdowns.
More devices are being investigated for home dialysis, so we can anticipate more options in the future. It can be expected that these devices will become more automated and patient friendly and would simplify the water system. They will likely be able to transmit data to the home dialysis department allowing the treatment to be tracked by the home dialysis nurse.
Special Considerations of the Elderly
The elderly with renal failure often face a number of formidable issues in addition to their renal failure. Because vascular disease is particularly prominent prior to starting dialysis, the elderly patient may not tolerate dialysis as well. They often have underlying heart disease with reduced cardiac function. Their peripheral vasculature has significant atherosclerosis that leads to intermittent claudication, limb ulcers, and amputation. Placement of the vascular access used for hemodialysis can lead to worsening of their circulatory compromise and/or loss of a limb. They may develop “steal syndrome” and subsequent neurological damage to their hand. They also may have an increased incidence of neurological issues such as TIAs or stroke as a result of carotid artery stenosis. They usually become very weak with dialysis treatments. The 3-day period between treatments can lead to congestive heart failure and pulmonary edema because of the inability to effectively remove all of the accumulated fluid using a three-time a week treatment regimen. In addition, cardiac status may be compromised which makes it difficult to tolerate fluid build-up between treatments. Appetite is often already suppressed and may frequently worsen with dialysis leading to protein malnutrition that in turn leads to poorer outcomes.
Training for home hemodialysis involves training a “helper” to assist the patient. Usually, this is the spouse. A suitable partner is necessary for successful home treatments, and not having a partner capable of learning the treatment may be a hindrance. Additionally, there may be medical issues with the partner that compromise his/her ability to perform the treatment, or they may have disabilities limiting their own ability to provide any care. They may have poor vision, lack of dexterity or strength, and inability to learn a new technique. The housing situation may be inadequate for the storage of equipment and supplies. Fear about performing a home treatment may prevent the patient or helper from choosing this modality. The family may be concerned that it would place too much burden on the caregiver.
Financial issues may also push the patient to do in-center dialysis. Although Medicare provides nearly universal health care coverage for most individuals at the age of 65, it doesn’t cover everything. The elderly often have fixed incomes that preclude them from affording expensive medications even when they have partial prescription coverage. Medicare does not cover an assistant at home to do the therapy. The increased electrical and water costs of the home therapy may be a strain on their fixed income. Transportation to and from the dialysis unit may be a problem, and the patient may not be able to drive himself to the dialysis facility and may have to rely on a family member or public transportation.
The elderly are also at increased risk for falling. Abdel-Pahman EM et.al described in a pilot study over a 1-year period a 26.3 % incidence of falls in their dialysis population [8]. The elderly, particularly females, were prone to falling. The greater the number of falls, the worse was the outcome. Due to an increased risk of bleeding because of the uremic state and anticoagulants that the patients receive, serious complications such as subdural hematomas can have disastrous results. Hip fractures resulting from falls will often lead to nursing home placement and subsequent death.
It has been well recognized that renal failure patients have an increased problem with depression, a sense of loss of control, general fatigue, and lack of energy. The elderly patients on dialysis are particularly prone to these symptoms. More frequent dialysis treatments may tend to improve these symptoms since the treatments can be gentler and less aggressive.
Benefits of Home Hemodialysis for the Elderly
While the problems that the elderly face are similar to younger patients with multiple comorbidities, they generally do not tolerate aggressive treatments as well. Therefore, slower treatments can be advantageous. The standard in-center dialysis treatment program today is of 3–4 h duration, 3 days a week. With home therapies, the longer and gentler treatments can be done in a cost-effective way. Short daytime or slower nighttime treatments can be done four to six times per week.
When Ipema et.al studied protein intakes between day and night hemodialysis patients, they found that the protein intake of patients improved significantly when they transitioned from daytime therapy to nighttime. With longer treatments, the patients’ phosphate levels remained stable even though their phosphorus intake was greater [9]. These factors suggest the nutritional status of the elderly dialysis patient may be enhanced with more frequent, longer and gentler treatments. Similarly, Uldall et al. described their early experience with home nocturnal dialysis patients dialyzing five to seven nights a week. They were successful in discontinuing phosphate binders and allowing a higher phosphate diet. Their patients experienced increased energy and stamina.
Sleep disturbances are common in the elderly. Improvement of sleep apnea was seen in the Canadian experience with home nocturnal dialysis. The conversion from conventional in-center dialysis to nocturnal dialysis was associated with a reduction in the frequency of apnea and hypopnea from 25+/−25 to 8+/8− episodes per hour of sleep (p = 0.03). The apnea-hypopnea index was greater on the nights when no dialysis was being performed as opposed to the nights of dialysis [10, 11]. The majority of patients also reported improved sleep.
The elderly have an increased risk of hypotension, cerebral and cardiac events, malnutrition, infection, sleep abnormalities, and psychological complications after initiation of dialysis. Home nocturnal hemodialysis is a less aggressive treatment and thus may be advantageous due to the comorbidities of the elderly. Such patients do particularly well with regard to these complications when doing home nocturnal hemodialysis.
Since fluid control can be problematic for the elderly, particularly for the extended 3-day periods, a nocturnal treatment program that offers at least quotidian therapy is an attractive option in controlling fluid balance. Improvement of left ventricular hypertrophy in home nocturnal dialysis patients has been established.
Therefore, taken altogether it becomes apparent that more frequent dialysis, slower dialysis, and extended treatments can potentially improve the outcomes and quality of life of the elderly patient on dialysis.
Benefits of Early Education
If the patient is seen early in their course by the nephrologist, the patient is more likely to choose a home therapy, less likely to start dialysis with a catheter and overall have better outcomes (Table 4.1).
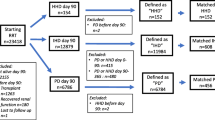
Studies at Fresenius Medical Care have shown that a proactive educational program (Treatment Options Program or TOPS) for patients with progressive renal disease will more often lead to choosing a home therapy. Education also leads to early placement of the access so it can be functional when dialysis is needed (Fig. 4.8).

Early placement of access in patients attending proactive education program vs those not participating. (Unpulished raw data)
Without the physician encouraging home hemodialysis, the patient and their family will not likely choose this form of treatment since the patient turns to the physician for advice and direction as to which therapy to choose. When patients were asked who first made them aware of home hemodialysis, only 35 % stated that their physician first made them aware of the home treatment. When asked who recommended home hemodialysis, only 11 % of the time the recommendation was made by the physician (Fig. 4.9).

Home hemodialysis recommended by physician (Chadwick Martin Bailey; NxStage Home Hemodialysis Patient Research, October 2008 p. 1–44)
Early education will lead to more patients choosing a home therapy; therefore, it is often helpful to consider the 30/20/10 rule. At a GFR of 30 ml/min, discussions regarding kidney failure and dialysis should be started with the patient and their family. All options should be presented, but home therapies can be encouraged if the patient is a good candidate. Since no one therapy fits every individual, it is realized that home hemodialysis is not the only option, but it is a more viable option than what is being encouraged today. At a GFR of 20 ml/min, a discussion for vascular access placement may be considered with the caveat that progression to ESRD is slower in the elderly. Usually grafts should not be placed early since the graft will have a limited lifespan and can be placed and used usually within 3–4 weeks.
At a GFR of 10 ml/min, dialysis will typically be started due to uremic symptoms. The 30/20/10 rule is helpful but should be used in the context of the rate of deterioration of renal function. There are patients whose renal function may deteriorate very slowly over time. If the rate of decline of renal function is slow, placement of an access could be delayed. To assess the rate of decline, using the reciprocal of the creatinine over time can help predict future value that in turn can assist in choosing the right time for access placement. The practitioner should keep in the mind that the muscle mass of the elderly is reduced making calculations of estimated GFR skewed, thus overestimating renal function. Since education is the key element to having more patients on home therapies, a team approach usually works best. The physician rarely has the time to fully educate the patient. Therefore, a patient educator will be instrumental to increasing the use of home dialysis. The educator should have pamphlets, DVDs, and time to visit with the patient and family. Group sessions can also be very helpful. When the patient finds others facing similar life-changing decisions, they realize they are not alone in having to make difficult decisions regarding treatment for renal failure. Using current home patients to provide testimonials can be very helpful. If the patient with progressive renal failure speaks to someone already on a home therapy, they often realize the benefits of home dialysis and the fear of doing a home therapy subsides. The patient often has more confidence in the advice of another patient over marketing brochures. Still marketing material can be helpful and should be available in multiple languages, if possible, so that local ethnic groups can benefit.
Encouraging Home Hemodialysis
For all patients considering dialysis, home hemodialysis should be one of the considerations. As physician, nurses, and health care providers, we have to begin considering home therapies first and in-center treatments second. Home therapies allow patients to live independently. Because funding for dialysis in the future may become more limited, looking to therapies such as home hemodialysis that reduce cost will become more attractive.
Treatments at home can be tailored to the patient. For those patients who struggle with control of their thirst and need frequent dialysis to remove fluid, dialysis in a home setting can be adjusted to manage the fluid gains. Conforming to a 3-day a week schedule does not fit everyone with ESRD. If a patient who normally complies with the diet eats excessive salt or drinks excessive fluid during a special celebration, they can simply dialyze themselves extra to manage this problem. Similarly a diabetic patient who deviates from their diabetic diet and subsequently has high blood sugars adjusts their insulin to accommodate hyperglycemia. We wouldn’t want the patient’s blood sugars to run high leading to all the consequences of hyperglycemia, but instead we would want the patient to adjust their insulin dosage to lower the blood sugar. In the situation of a renal failure patient with fluid overload, it is prudent to remove the extra fluid and reduce the after load on the heart created by fluid excess. This can be accomplished with home hemodialysis where the extra treatment can be performed by the patient when the need arises.
These types of arguments should be presented to the patient approaching dialysis. Convincing the patient and their family of the value of home hemodialysis takes time and frequent interaction. They have to hear the benefits repeatedly because the idea of starting dialysis can be overwhelming to the patient, particularly if they have never been told of the options prior to requiring dialysis. The equipment appears threatening to them, the time commitment unmanageable, and the costs insurmountable.
When we looked at our home hemodialysis program, we found that the greatest success was achieved if either the patient or the helper was employed. The next most successful population was the elderly where the patient and the helper are not employed. We had the poorest success if only the patient was solely responsible for the treatment and the partner learned only the basics to handle emergencies. It would appear that the patient needs an advocate who can offer support and help the patient day by day to perform their treatments and give them encouragement (Table 4.2).
Dialysis in Assisted Living Facilities
In the past, it was common for the elderly to be cared for at home through their declining years by their children. Today, however, the elderly often move to assisted living homes when they need help with activities of daily living. Although advantages of home hemodialysis from a clinical standpoint may be obvious, the new home situation may prevent adoption of the home treatment.
Assisted living facilities often charge their guest based on the amount of services needed. For example, if the client needs more assistance with their medications, dressing, or bathing, there may be additional charges. If home hemodialysis of the elderly were permitted in an assisted living environment, the spouse could learn the treatment, but assistance from the nursing staff at the facility could allow and encourage the elderly couple to consider home hemodialysis. While this may lead to an additional charge to the patient by the facility, it could be reasonable if the spouse would perform the majority of the therapy. It could be particularly advantageous to develop assisted living facilities that provide specialized care of the renal failure patient. The home dialysis department could work with the nursing staff of the facility to develop a comprehensive program that would assist with the diet and medications as well as with the treatment itself.
Self-Care
A middle step to home therapy that isn’t often used is self-care. Starting a self-care unit where the patient sets up their own machine, sticks their access, and runs on a schedule that allows more flexibility than in-center treatments can be a helpful option. There are currently very few self-care centers in the United States for patients but this option should be expanded to provide more options for the patient. These centers should be staffed with home dialysis nurses who will allow the patient to conduct their own treatments. Often in-center nursing staff have difficulty training elderly patients for home therapies owing to busy schedules and slow learning process. Nursing staff oriented to home therapies will usually have more successful outcomes in such settings.
Summary
The elderly are faced with many difficult problems and decisions as their kidneys fail. Typically the disease that is causing their kidney failure is not confined to the kidneys but often represents a diffuse disease process. This process frequently leads to serious cardiac problems, peripheral vascular disease, and dementia in a body simply failing from age. The elderly often have depression because of their failing health, loss of independence, and the death of loved ones. Independent living facilities and assisted living facilities have filled a gap for those whose families cannot care for their elderly parents. Currently these facilities are often not willing to take on patients performing home dialysis or assist them with their treatments. The development of specialized assisted living centers that focus on care of the elderly with renal failure may be an attractive option to in-center dialysis.
Home therapies and in particular home hemodialysis have many benefits for the elderly as has been discussed in this chapter. There are, however, many obstacles that must be dealt with to get an elderly patient on home hemodialysis. Using a team of health professionals that includes a social worker, patient educator, home dialysis nurse along with the physician can lead to more patients choosing home hemodialysis.
Key Points
-
1.
Elderly patients constitute an ever-growing segment of dialysis population, in the western world.
-
2.
In-center hemodialysis may not be the best option for a significant number of elderly hemodialysis patients.
-
3.
Home therapies are a good alternative for the elderly on dialysis.
-
4.
Home hemodialysis may offer increased flexibility and improved symptom control owing to higher frequency and/or duration of hemodialysis besides being a “gentler” form of therapy.
-
5.
Home hemodialysis machines are becoming increasingly user friendly.
-
6.
Careful patient selection and education remain the key to successful home hemodialysis option for this age group.
-
7.
Transfer from self-care units to home and home hemodialysis in assisted living facilities are under recognized options that are available to elderly patients.
References
U.S. renal data system. USRDS 2005 annual data report: atlas of end-stage renal disease in the United States (2005). National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda
List of countries by life expectancy (2010). In: Wikipedia, the free encyclopedia. Retrieved 06 Feb 2013 from http://en.wikipedia.org/w/index.php?title=List_of_countries_by_life_expectancy&oldid=536580534
Walls J (1990) Dialysis in the elderly; some U.K. experience. Adv Perit Dial 6:82
Dirks JH, Levin NW (2006) Dialysis rationing in South Africa: a global message. Kidney Int 70:982–984
Nose Y (1995) Home hemodialysis. A crazy idea in 1963. A memoir. ASAIO J 46:13–17
Disney AP (1995) Demography and survival of patients receiving treatment for chronic renal failure in Australia and New Zealand: report on dialysis and renal transplantation treatment from the Australia and New Zealand Dialysis and Transplant Registry. Am J Kidney Dis 25(1):165–175
MacGregor MS, Agar JW, Blagg CR (2006) Home haemodialysis – international trends and variation. Nephrol Dial Transplant 21:1934–1945
Abdel-Rahman EM, Yan G, Turgut F, Balogun RA (2011) Long-term morbidity and mortality related to falls in hemodialysis patients: role of age and gender – a pilot study. Nephron Clin Pract 118(3):c278–c284
Ipema KJ, van der Schans CP, Vok N, deVries JM, Westerhuis R, Duym E, Franssen CF (2012) A difference between day and night: protein intake improves after the transition from conventional to frequent nocturnal hemodialysis. J Ren Nutr 22(3):365–372
Hanly PJ, Pierratos A (2001) Improvement of sleep apnea in patients with chronic renal failure who undergo nocturnal hemodialysis. N Engl J Med 344(2):102–107
Cornelis T, Kotanko P, Goffin E, Kooman JP, van der Sande FM, Chan CT (2011) Can intensive hemodialysis prevent loss of functionality in the elderly ESRD patient? Semin Dial 24(6):645–652
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2016 Springer Science+Business Media New York
About this chapter
Cite this chapter
Ross, D.L., Schrag, W.F., Pond, P. (2016). The Pros and Cons of Home vs. In-Center Dialysis in the Elderly. In: Misra, M. (eds) Dialysis in Older Adults. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-3320-4_4
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3320-4_4
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-3318-1
Online ISBN: 978-1-4939-3320-4
eBook Packages: MedicineMedicine (R0)