
Abstract
The art of surgical endoscopy has revolutionized the diagnosis and treatment of gastrointestinal disorders. Gastroenterologists and esophageal surgeons must familiarize themselves with the proper technique of examining a patient for upper endoscopy.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others



Keywords
- Endoscopy
- Endoscope
- Endoscopic ultrasound
- Biopsy
- Endoscopic mucosal resection
- Esophageal ablation
- Mucosectomy
- Submucosal dissection
- Barrett’s
- Dysplasia
- Squamous cell lining
- Esophageal cancer
- Adenocarcinoma
- Squamous cell cancer
- High definition endoscopy
The art of surgical endoscopy has revolutionized the diagnosis and treatment of gastrointestinal disorders. Gastroenterologists and esophageal surgeons must familiarize themselves with the proper technique of examining a patient for upper gastrointestinal endoscopy.
Current endoscopic instrumentation includes a modern video high-definition endoscope, illustrated in Fig. 3.1. The video camera is connected to a control panel that can capture images, adjust lighting, and change views. At the terminal end of the insertion tube are an air or water nozzle, an objective lens, a biopsy and suction channel, and an illuminating lens. The biopsy channel allows the passage of biopsy forceps or instrumentation for cytologic testing as well as therapeutic maneuvers. The flexible end of the tube allows for atraumatic insertion, manipulation, and guidance within the esophageal lumen. A deflection control knob with a locking switch makes it possible to look up and down and right and left. Other parts of the system include an instrument port; suction, air, and water valves; suction, video, and water container connectors; and a universal cord that connects the handheld instrument to the processor.


The parts of a standard Olympus endoscope (Olympus America, Center Valley, PA)
The newer versions of endoscopes are equipped with a tiny camera at the distal end of the instrument, which transmits the digitalized image to an external television monitor for viewing. Typically, most are high definition. Carbon dioxide can be insufflated to minimize air entrapment. Developments in this technology have added special lenses to the tip of the instrument for magnification, and diagnostic ultrasound has been adapted to the instrument to facilitate the elucidation of cardiac and gastrointestinal disorders.
Esophagogastroduodenoscopy (EGD)
Indications
There are several indications for EGD examination of the upper gastrointestinal (GI) tract:
-
Investigations of symptoms such as dysphagia, odynophagia, persistent pyrosis, hematemesis, or melena
-
Retrieval of a foreign body
-
Evaluation of unremitting upper abdominal pain with a normal upper GI barium examination, or suspicious abnormalities identified on a barium upper GI series
Endoscopy Procedure
A patient being considered for any esophageal surgery should undergo endoscopic examination prior to their operation, to ensure that there have been no pathologic changes since the last endoscopy and to ensure that the tumor or abnormality is as described when the patient was initially referred. Additionally, a patient with a previous surgery should undergo surveillance endoscopy to evaluate the anastomosis for recurrence and the pylorus for patency; this endoscopy ideally should be performed by the surgeon who best understands the patient’s reconstructed anatomy.
Preparing for the Endoscopy
The patient should not be fed for 6–8 h prior to an upper endoscopy. Antireflux medication may be administered prior to the exam. In an emergency, rapid-sequence intubation may protect the airway of a patient who has recently consumed a meal.
Technique
-
The posterior pharynx is anesthetized with topical anesthetic spray or gargle, unless the procedure is being performed under general anesthesia.
-
Intravenous sedation is administered slowly until the patient is comfortable. For more complicated endoscopic procedures, we advocate the use of general anesthesia and intubation to avoid aspiration.
-
A patient who is intubated may be left in the supine position. Otherwise, with the patient in the left lateral decubitus position, the endoscope may be passed in one of two ways:
-
A mouth guard is positioned between the patient’s teeth, and the scope is advanced under direct vision (Fig. 3.2). The epiglottis and vocal cords are visualized and the instrument is passed posteriorly into the esophageal orifice. This technique allows visualization of the hypopharynx and may be particularly useful in patients with suspected lesions high in the esophagus or pharynx, or in relatively uncooperative patients.
Fig. 3.2 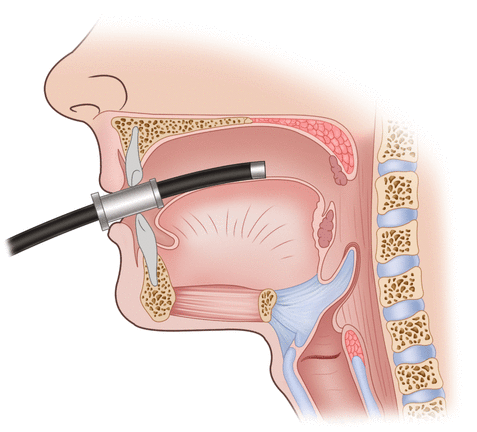
A mouthguard is typically used for insertion of the endoscope, to avoid damage to the patient’s dentition and the endoscope
-
In an alternative method, the instrument is passed by feel of the operator. The endoscopist does not attempt to observe the lumen until the scope is in the esophagus. Observation of the upper pharynx and vocal cord are performed after removal of the scope. The index and middle fingers of the endoscopist are placed over the tongue to the posterior pharynx; the scope is then placed on top of the fingers and manipulated downward to the esophageal orifice. The guiding fingers ensure that the scope glides along the wall of the pharynx and is centered.
-
-
As the patient swallows, the instrument is advanced into the esophagus. Undue force is never applied and the scope is advanced only when the lumen can be visualized, to avoid perforation of the pharynx. (Perforation of the pharynx most likely would involve the piriform sinus, and the result would be massive injection of subcutaneous air throughout the neck and mediastinum when the endoscope is insufflating the hypopharynx.)
-
The esophagus is inflated with air and inspection is begun. The normal esophagus demonstrates a long, round, tubular lumen with a pale, smooth mucosa.
-
Careful inspection of the mucosal surfaces is important to detect subtle irregularities that may herald underlying pathology. When an irregularity of the mucosa is encountered, a biopsy specimen and brushings can be obtained for cytologic examination, after ensuring (using the Doppler flow tool) that the abnormality is not a vascular structure. If there is concern about the structure and depth, then an ultrasound may be used to determine the characteristics of the lesion.
-
At the most distal end of the normal esophagus, about 40 cm from the incisors, there is a sharp transition from the pale esophageal (squamous) mucosa to the deeper orange gastric (columnar) mucosa (Fig. 3.3a, b). This junction is called the Z-line and is usually somewhat irregular. An abnormal mucosal tongue of columnar mucosa is representative of Barrett’s island, and biopsies must be performed to confirm metaplasia (Fig. 3.3c). Large extensions of gastric-type mucosa above this point may represent Barrett’s esophagus (columnar metaplasia of the esophagus). A biopsy specimen should be obtained from such an area, as dysplasia and malignancy may arise within a Barrett’s epithelium.
Fig. 3.3 

The gastroesophageal junction is easily identified where the squamous esophagus lining transitions over to the columnar gastric mucosa (a, b). When this Z-line undergoes metaplasia, biopsies must be performed to confirm Barrett’s esophagus and rule out dysplasia (c). The gastroesophageal junction is visualized on retroview of the endoscope (d, e). The pyloric sphincter (f) and its intubation into the duodenum (g) must also be visualized and documented on every routine endoscopy
-
The esophagus frequently veers slightly to the left as it traverses the diaphragm. The gastroscope should be advanced under direct vision into the stomach; it should never be advanced when a lumen cannot be identified.
-
As the gastroscope is advanced into the stomach, the endoscopist must become oriented to the gastric anatomy. The lesser curvature of the stomach occupies the 12 o’clock position and the field of observation. The mucosa in this area is usually smooth. Careful observation in the lesser curvature is warranted, as this is frequently the site of gastric ulceration or malignancy.
-
The greater curvature occupies the 6 o’clock position. This area is characterized by prominent parallel rugae folds, which do not totally flatten with insufflation of air. The 9 o’clock position represents the anterior wall of the stomach, and the posterior wall is at the 3 o’clock position.
-
As the instrument is advanced further into the body of the stomach, the gastric incisura, or angularis, becomes visible on the lesser curvature. The smooth, arching fold separates the body from the antrum of the stomach. Alteration of the smooth contour of this fold may indicate previous ulcer disease or an infiltrative process.
-
Beyond the angularis lies the antrum of the stomach. The scope should be advanced into the antrum after careful observation of all the features of the gastric corpus. Typically, there are no rugal folds in this region. The pylorus lies at the distal extent of the antrum. It is worth waiting a moment after entering the antrum to watch the peristaltic waves pass the pylorus. The peristaltic activity is useful in unfolding all areas of the antrum for observation; and watching it also ensures that there is no infiltrative process limiting motility.
-
Once positioned at the angle of the stomach, the tip of the endoscope may be turned to view the gastric cardia and fundus (Fig. 3.3d, e). This retroflexed view is useful in identifying and treating lesions of the proximal stomach and distal esophagus. It is useful to twist the insertion tube of the instrument into this position to bring the area surrounding the scope into view. Subtle lesions of the fundus and cardia are best identified in this manner, so this maneuver must be part of every endoscopic examination of the stomach.
-
When examining a patient with esophageal cancer, one must ensure that the tumor does not extend into the gastric lumen. If cardia involvement is detected, the patient may not be able to have a gastric conduit and may instead require an alternate conduit such as colon or small bowel [1, 2].
-
As the scope is advanced, the characteristics of the pylorus should be carefully observed. A normal pylorus is typically round and opens and closes in response to peristaltic activity (Fig. 3.3f). Irregularities in the shape of the pyloric aperture may suggest past or present ulcer disease. Lack of motility may indicate scarring or an infiltrative process.
-
After passing the tip of the endoscope through the pylorus, the examiner should pause briefly to observe the duodenal bulb. Not infrequently, the scope may advance beyond the bulb after passing the pylorus; it should be pulled back so that the first portion of the duodenum can be carefully examined. The bulb has no folds. Its mucosa is usually smooth and fine. Submucosal vessels are often visible. Some granularity occasionally may be present as a result of ectopic gastric mucosa. Ulcers are the most common lesions identified in this area, although other lesions such as adenomas of Brunner’s gland, heterotopic pancreas, and even malignancy occasionally may be identified. The distal extent of the duodenal bulb is marked by the first duodenal fold and the superior duodenal fold, which marks the posterior turn of the duodenal lumen into its second portion (Fig. 3.3g).






Once the surgeon has become familiar with basic endoscopic techniques, particular procedures that are performed through an endoscope may then be employed. Some of these endoscopic procedures are discussed in Chaps. 5 and 6.
Endoscopic Imaging of Barrett’s Esophagus
The importance of Barrett’s esophagus is based on the recognition that it is often a precursor of esophageal adenocarcinoma. This histologic progression from metaplasia to low-grade dysplasia to high-grade dysplasia and then to adenocarcinoma is the rationale for endoscopic screening and surveillance programs. Current surveillance protocols call for periodic endoscopic exams for mucosal abnormalities and four-quadrant random biopsies every 2 cm within the segment of Barrett’s esophagus (referred to as the Seattle protocol). The limitations of such protocols include sampling error (they sample less than 1 % of affected esophageal surface) and the effort and time required to perform each biopsy and place it into a separate cytologic cup at every level [3].
The development of endoscopic imaging modalities that identify intestinal metaplasia and facilitate differentiation of bland Barrett’s epithelium from low-grade and high-grade dysplasia and early adenocarcinoma simultaneously has been the focus of intense research. The potential merit of such imaging modalities is the possibility of complete examination of a Barrett’s esophagus segment for dysplasia without the need for biopsy or with the ability to perform focused biopsies in areas most likely to contain dysplastic epithelium. A number of endoscopic imaging methods have been developed for this purpose over the past several decades. The rest of this section focuses on the basis for each method and the technique, interpretation, and evidence for these imaging modalities.
One of the difficulties in identifying dysplastic foci and Barrett’s esophagus is the large esophageal surface area that must be examined. In general, it is difficult to apply imaging methods with high resolution, which provide greater tissue detail or histologic information, when it is necessary to scan a large segment of Barrett’s esophagus. Lower-resolution methods can be used to image a larger area of esophagus, but they are less reliable in distinguishing dysplasia from nondysplasia.
An ideal imaging technique would have several characteristics [4]:
-
High sensitivity for dysplasia
-
Moderate specificity not affected by inflammation
-
The ability to scan a wide area in real time
-
High interim server agreement
-
The ability to localize dysplastic areas for biopsy
-
Cost that is not prohibitive
Techniques that can assist an endoscopist in identifying suspicious areas within the esophagus include (but are not limited to) chromoendoscopy, narrow band imaging, autofluorescence, optical coherence tomography, endoscopic ultrasound, and confocal microscopy, as discussed below.
Chromoendoscopy
Chromoendoscopy refers to the application of contrast stains to mucosa at endoscopy, so that surface patterns are highlighted [5–7]. The use of various contrast agents such as methylene blue, acetic acid, Lugol solution, and indigo carmine has been described extensively in the literature.
-
Methylene blue is absorbed by intestinal-type epithelium. In the setting of Barrett’s esophagus, Barrett’s epithelium is stained, and nonintestinal columnar and squamous epithelium is spared. Furthermore, dysplastic Barrett’s epithelium stains less than Barrett’s epithelium without dysplasia because of the paucity of goblet cells in the setting of dysplasia. Therefore, areas of Barrett’s epithelium with dysplasia may be more evident on chromoendoscopy using methylene blue. The technique of chromoendoscopy using methylene blue involves clearance of surface mucous in the esophagus by flushing with 10 % N-acetylcysteine (Mucomyst). Subsequently, 0.5 % methylene blue is applied to the esophageal mucosa using an endoscopic spray catheter. After a 2-min standing period, excess methylene blue is cleared by flushing with sterile water.
-
Indigo carmine, unlike methylene blue, is simply a contrast agent that accentuates mucosal surface patterns. Indigo carmine is applied during endoscopy using a typical endoscopic spray catheter after the surface has been cleared of mucous with water saline or Mucomyst flush. The use of a cap fitted at the endoscopic tip has been described to stabilize high-magnification images in image areas of interest. A ridged or villous pattern with a cribriform appearance, or a circular pattern with a uniform circular or oval appearance, is typically seen in nondysplastic Barrett’s esophagus and in low-grade dysplasia. In high-grade dysplasia, on the other hand, the pattern seen is irregular and distorted.
Narrow Band Imaging
Conventional video endoscope transmits a white light from a xenon lamp, but in narrow band imaging (NBI), the light passes through a special, rotating red-green-blue filter that has been incorporated into the endoscope. The transmitted light, composed of alternating pulses of red, green, and blue light, illuminates the imaged area. Waves are absorbed or reflected by the image area and are detected by a charge-coupled device (CCD) at the endoscope tip. The light waves detected by the CCD are transmitted to the video processor unit, where superimposed red, green, and blue light images are integrated to create a final video endoscopic image that is can be seen by the human eye.
-
In NBI, an additional special filter has been incorporated into the endoscope
-
The light is preferentially absorbed by hemoglobin, so hemoglobin-containing structures such as capillaries and luminal blood are accentuated in the presence of blue light (Fig. 3.4a).
Fig. 3.4 
Narrow band imaging (NBI) endoscopic images. (a) The narrow esophageal mucosa demonstrates the fine vascular network in NBI mode. (b, c) Abnormal mucosa is seen as white patches
-
The red light, on the other hand, has a wavelength of 650 nm and penetrates tissue more deeply than blue light, with a wavelength of 475 nm.
-
Three distinct mucosal patterns in patients with Barrett’s esophagus can be identified on NBI: the ridged/villous pattern, the circular pattern, and the irregular, distorted pattern (Fig. 3.4b, c). The ridged/villous pattern is characterized by uniformly aligned ridges alternating with a villiform pattern. This pattern is seen on NBI as alternating dark and white lines. The circular pattern is characterized by a uniformly arranged, circular mucosal pattern. The irregular, distorted pattern demonstrates the ridged and villous pattern with significant irregularity and distortion, suggestive of an inflammatory or malignant change.
-
Vascular patterns on NBI are characterized as normal (thin, uniformly branching vessels) or abnormal (dilated, corkscrew vessels and nonuniform branching patterns).
-
The positive predictive value, sensitivity, and specificity of NBI for an abnormal vascular pattern and high-grade dysplasia is relatively high. False positives for abnormal vascular pattern do occur, but the rate is low.


Autofluorescence Imaging
In autofluorescence, certain molecules, termed fluorophores, absorb light energy and reach an excited state. From the excited state, fluorophores reach the ground state, and in that process, they emit light of a longer wavelength than produced in the excited state. Emitted light within the visible light spectrum accounts for the obstacle phenomenon of fluorescence.
The use of fluorescence for imaging may be based on endogenous fluorophores such as nicotinamide adenine dinucleotide (NADH) or collagen, or on the use of exogenously supplied fluorophores such as porfimer sodium or fluorescein, a fluorescent dye. Autofluorescence is the term denoting the exploitation of endogenous fluorophores and biological tissue for imaging. Variations in molecular composition and tissue microstructure lead to differences in fluorescence, thereby creating the potential for distinguishing neoplastic tissue from nonneoplastic tissue. Prototypic endoscopes that make use of this technology have been developed in recent years. The additional use of confocal microscopy including the injection of fluorescein can allow endoscopists to identify areas of dysplastic Barrett’s epithelium and target these areas for focused biopsy, but the role of this technique has been questioned [8].
Confocal Microscopy
Confocal microscopy is an optical imaging technique used to increase the optical resolution and contrast of a micrograft by using point elimination and a special pinhole to eliminate out-of-focus light and specimens that are thicker than the focal plane. It enables the reconstruction of three-dimensional structures from the obtained images. This technique has gained popularity and is now commonly used in some Barrett’s screening programs. A compilation of several scanned images can be made to provide a larger photograph of the dysplastic epithelium, which represents a map larger than that of the tip of the confocal microscope [9].
Optical Coherence Tomography
Optical coherence tomography (OCT) is a method of producing high-resolution, cross-sectional imaging of the esophagus. It is similar to ultrasound but uses light to produce the images, rather than sound waves. Real-time images of the esophagus can be obtained during endoscopy. Its particular use in the setting of esophageal pathology is in the surveillance of Barrett’s esophagus [10–12]. The planar images created can allow detection of “buried” Barrett’s epithelium that may otherwise be missed on routine EGD. This technology may be useful in the surveillance of Barrett’s after treatment such as radiofrequency ablation.
Endoscopic Ultrasound
Endoscopic Abnormalities
Any mucosal ulceration or mass noted in the esophageal or gastric lumen during endoscopy can be cultured, biopsied, or both. A number of abnormalities may be seen:
-
Typically, a dysplastic lesion will present as linear erosions, irregular mucosa, or small nodularities (Fig. 3.5a).
Fig. 3.5 
Esophageal cancer can be identified as small, abnormal nodularities (a) or a discrete mass (b)
-
If the mass is noted to involve the esophageal wall (Fig. 3.5b), then a primary tumor is most likely the diagnosis; an ultrasound of the lesion is warranted to determine its depth and associated lymphadenopathy (see Chap. 5).
-
A finding on endoscopy of a classic ringed esophagus, sometimes termed “trachealization of the esophagus” (Fig. 3.6), can be diagnostic of eosinophilic esophagitis. This diagnosis typically cannot be made from any other, noninvasive imaging. The endoscopy also can be used to obtain a definitive diagnosis by allowing the performance of an esophageal biopsy.
Fig. 3.6 
Eosinophilic esophagitis can be seen on endoscopy as ringed esophagus (trachealization). A biopsy of the mucosa would determine infiltration of the esophagus with eosinophils
-
Another uncommon clinical entity that can be visualized on endoscopy is “black esophagus,” which usually has an ischemic etiology.
-
Various fungal infections such as esophageal candidiasis can be seen as linear growths in immunocompromised patients such as those undergoing neoadjuvant chemotherapy prior to surgical resection.
-
Patients presenting with dysphagia can be worked up for a Schatzki’s ring (Fig. 3.7a), benign (Fig. 3.7b) or malignant stricture, epiphrenic or Zenker’s diverticulum, or to identify classic radiological features of achalasia such as megaesophagus or bird’s beak esophagus.
Fig. 3.7 
Other diagnoses that can be identified on endoscopy include Schatzki’s ring (a) or stricture (b)
-
Although diffuse esophageal spasm and scleroderma are connective tissue disorders and are slightly difficult to diagnose on endoscopy, characteristics such as tertiary contractions can be noted on endoscopy (Fig. 3.8).
Fig. 3.8 
Tertiary contractions noted on endoscopy in a patient with dysphagia can be suggestive of diffuse esophageal spasm (DES) or scleroderma. Esophageal manometry can be used to confirm the diagnosis








Complications of Endoscopy
Endoscopy does have pitfalls that require care.
-
Perforation may occur if the endoscope is advanced blindly into a pouch or the sidewall of the esophagus, especially in a previously radiated tumor bed (Fig. 3.9).
Fig. 3.9 
Complications of endoscopy can include iatrogenic perforation. This image demonstrates a chronic iatrogenic perforation secondary to endoscopy
-
In patients with esophageal or gastric varices, extreme caution must be used to avoid pushing the endoscopic probe too vigorously. One approach to these patients would be to decompress their portal hypertension before proceeding to elective endoscopy. The endoscopist should be familiar with a Sengstaken-Blakemore tube and be prepared to tamponade the bleeding with it if necessary.


References
Hallock GG. A paradigm shift for soft-tissue coverage of the zones of the abdominal wall using perforator flaps. Plast Reconstr Surg. 2012;130:590–9.
Kesler KA, Pillai ST, Birdas TJ, Rieger KM, Okereke IC, Ceppa D, et al. “Supercharged” isoperistaltic colon interposition for long-segment esophageal reconstruction. Ann Thorac Surg. 2013;95:1162–8; discussion 1168–9.
Kariv R, Plesec TP, Goldblum JR, Bronner M, Oldenburgh M, Rice TW, Falk GW. The Seattle protocol does not more reliably predict the detection of cancer at the time of esophagectomy than a less intensive surveillance protocol. Clin Gastroenterol Hepatol. 2009;7:653–8; quiz 606.
Urquhart P, DaCosta R, Marcon N. Endoscopic mucosal imaging of gastrointestinal neoplasia in 2013. Curr Gastroenterol Rep. 2013;15:330.
Kara MA, Ennahachi M, Fockens P, ten Kate FJ, Bergman JJ. Detection and classification of the mucosal and vascular patterns (mucosal morphology) in Barrett’s esophagus by using narrow band imaging. Gastrointest Endosc. 2006;64:155–66.
Singh R, Anagnostopoulos GK, Yao K, et al. Narrow-band imaging with magnification in Barrett’s esophagus: validation of a simplified grading system of mucosal morphology patterns against histology. Endoscopy. 2008;40:457–63.
Connor MJ, Sharma P. Chromoendoscopy and magnification endoscopy for diagnosing esophageal cancer and dysplasia. Thorac Surg Clin. 2004;14:87–94.
Boerwinkel DF, Holz JA, Kara MA, Meijer SL, Wallace MB, Wong Kee Song LM, et al. Effects of autofluorescence imaging on detection and treatment of early neoplasia in patients with Barrett’s esophagus. Clin Gastroenterol Hepatol. 2014;12:774–81.
Trovato C, Sonzogni A, Ravizza D, Fiori G, Tamayo D, De Roberto G, et al. Confocal laser endomicroscopy for in vivo diagnosis of Barrett’s oesophagus and associated neoplasia: a pilot study conducted in a single Italian centre. Dig Liver Dis. 2013;45:396–402.
Testoni PA, Mangiavillano B. Optical coherence tomography in detection of dysplasia and cancer of the gastrointestinal tract and bilio-pancreatic ductal system. World J Gastroenterol. 2008;14:6444–52.
Evans JA, Poneros JM, Bouma BE, Bressner J, Halpern EF, Shishkov M, et al. Optical coherence tomography to identify intramucosal carcinoma and high-grade dysplasia in Barrett’s esophagus. Clin Gastroenterol Hepatol. 2006;4:38–43.
Hashimo H. Subsquamous intestinal metaplasia after ablation of Barrett’s esophagus: frequency and importance. Curr Opin Gastroenterol. 2013;29:1–6.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Gaur, P., Dickinson, K.J. (2015). Esophageal Anatomy as Seen During Endoscopy and Basic Endoscopic Orientation. In: Blackmon, S.H., Kim, M.P., Dickinson, K.J. (eds) Atlas of Esophageal Disease and Intervention. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-3088-3_3
Download citation
DOI: https://doi.org/10.1007/978-1-4939-3088-3_3
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-3087-6
Online ISBN: 978-1-4939-3088-3
eBook Packages: MedicineMedicine (R0)