
Abstract
Pulmonary hypertension (PH) refers to a mean pulmonary arterial pressure ≥25 mmHg and may be related to elevations in left atrial pressure, pulmonary vascular resistance, cardiac output, or combinations thereof. When the mechanism of PH is related to an elevation in vascular resistance, the term pulmonary arterial hypertension is used, and may occur in the presence or absence of certain associated conditions. Identification of this subset is important as these patients are at an elevated risk of morbidity and mortality related to progressive right heart failure. Symptoms are nonspecific, and the clinician must maintain a high index of suspicion in order to minimize diagnostic delay, particularly when the history and results of ancillary testing do not suggest an alternative explanation for cardiopulmonary symptoms. Echocardiography provides valuable information that can aid the clinician in estimating the degree of PH, as well as gauge the likelihood that any observed elevations in pulmonary pressures are related to left atrial hypertension. In addition, relatively simple metrics of right ventricular size and function can be obtained. When such abnormalities exist in isolation, the clinician should have a high suspicion for pulmonary vascular disease. Right heart catheterization remains the gold standard for confirming the presence of PH, determining its hemodynamic basis, and guiding therapeutic decisions. Assessing hemodynamics with exercise may be informative in patients with predominantly exertional symptoms who display normal or equivocal values at rest.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Introduction
The evaluation of the patient with elevated pulmonary pressures requires a consistent and methodical approach aimed at identifying the correct etiology of the pulmonary hypertension (PH), assessing its physiologic impact, and choosing appropriate therapy. A recent population-based echocardiographic study from Olmsted County, Minnesota, suggests that up to 20 % of the general population exhibits an estimated right ventricular systolic pressure (RVSP) >35 mmHg (although this threshold may include individuals who do not have PH as determined by invasive testing) [1]. This fraction is likely to be significantly higher among patients referred for subspecialty evaluation [2, 3]. The identification of PH may be the result of a deliberate search in a dyspneic patient known to be at risk for PH (e.g., screening a patient with systemic sclerosis), or alternatively, may be found incidentally when diagnostic testing (i.e., an echocardiogram) is performed for another reason. The clinical classification of PH is divided into five groups, most recently updated at the 2013 Fifth World Symposium on PH held in Nice, France [4], and takes into account both hemodynamics and underlying pathophysiology (Table 8.1). The list of conditions associated with PH is long, however, and establishing a precise etiologic diagnosis is crucial to inform both prognosis and therapeutic strategy. Due to its grave implications for long-term survival if left untreated, early diagnosis of pulmonary arterial hypertension (PAH) is essential to allow institution of appropriate disease-modifying therapies. However, symptoms are often nonspecific and the presence of common comorbidities can create diagnostic confusion and delay accurate diagnosis [5], underscoring the importance of a methodical evaluation. Despite increasing awareness and scientific study of pulmonary vascular diseases over recent decades, certain tests recommended by current diagnostic algorithms [6–8] for the evaluation of PH remain underutilized [9]. Contemporary registries confirm the unfortunate reality that 70–80 % of PAH patients are in New York Heart Association (NYHA) functional classes III or IV at time of diagnosis [10–12], a statistic that has changed little over the preceding 25 years [13]. This chapter will present a practical overview of the approach to a patient with documented or suspected pulmonary hypertension.
Hemodynamic Basis of PH: An Introduction with Clinical Correlation
While a more detailed overview of pulmonary hemodynamics is presented in Chap. 10, a working knowledge of the hemodynamic basis of PH is extremely helpful in directing the clinical approach to the patient and so will be reviewed here in brief.
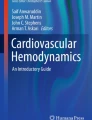
Current guidelines define PH as mean pulmonary artery pressure (mPAP) ≥25 mmHg with the patient at rest [6–8]. The definition of abnormal PAP response to exercise was considered as part of the 2013 WHO Nice deliberations, but no consensus was reached due to the lack of available data. Changes in pulmonary vascular and left ventricular compliance with aging make it difficult to determine normal and abnormal rises in PAP during exercise leading to the recommendation that exercise-induced PAP not be included in the definition of pulmonary hypertension [14]. It is crucial to note that while the pressure cutoff of 25 mmHg defines the presence or absence of disease by convention, it provides no information regarding its etiology. Application of Ohm’s law is used to describe the relationship between pressure and flow in the pulmonary circulation, but this assumes nonpulsatile, laminar flow within uniform, nondistensible vessels—all of which do not apply to the pulmonary vascular bed. With this limitation in mind, Ohm’s law dictates that mPAP is the product of pulmonary blood flow (Q p) and resistance across the pulmonary bed (pulmonary vascular resistance [PVR]), added to pulmonary venous pressure. In the absence of an anatomic shunt, Q p is approximately equal to systemic blood flow (Q s or cardiac output [CO]). Pulmonary venous pressure is difficult to measure directly in routine practice, so pulmonary capillary wedge pressure (PCWP) is used as a more readily obtained surrogate. Thus, an increase in mPAP may occur as a result of increases in Q p, PVR, or PCWP (Fig. 8.1). Each will be discussed in turn below.

Schematic representation of hemodynamic etiologies of increased pulmonary artery pressure. mPAP mean pulmonary arterial pressure, Q p pulmonary blood flow, PVR pulmonary vascular resistance, PCWP pulmonary capillary wedge pressure, LV left ventricle, PH pulmonary hypertension, PAH pulmonary arterial hypertension, AV aortic valve, MV mitral valve
Elevated Q p
Disorders associated with isolated elevations in pulmonary blood flow are relatively uncommon causes of pulmonary hypertension, since an otherwise healthy pulmonary vascular bed has the ability to recruit additional underperfused vasculature to accommodate increases in flow without a significant increase in pressure [15, 16]. In some circumstances, however, this reserve is impaired and elevations in Q p may drive, at least in part, a rise in mPAP. Usually, diagnosis of the primary condition predates the discovery of pulmonary hypertension, and there are frequently other symptoms that tend to dominate the clinical picture rather than the pulmonary hypertension per se. For these reasons, disorders associated with isolated increases in CO are not explicitly represented as a separate etiologic category in the current PH classification scheme [4].
Systemic conditions classically associated with an elevated CO include chronic anemia, pregnancy, hyperthyroidism, liver disease, and left-to-right shunts on the basis of either congenital heart disease, arteriovenous fistulae, or certain other disorders (e.g., Paget’s disease of bone, multiple myeloma). In anemia, elevated CO is a physiologic response aimed at maintaining adequate systemic oxygen delivery in the face of reduced oxygen carrying capacity. Modest levels of anemia commonly encountered in outpatient practice are not likely to cause significant elevations in CO, as a seminal hemodynamic study suggested a hemoglobin threshold of <7 g/dL is required to obligate a rise in CO in humans [17]. The increased metabolic demands of pregnancy imparted by the developing fetus also necessitate a rise in cardiac output, mediated by increases in both preload (due to plasma volume expansion) and heart rate and a reduction in systemic vascular resistance (SVR) [18]. Despite higher pulmonary blood flow, however, significant rises in PAP in healthy subjects typically do not occur presumably due to concomitant reductions in PVR [19]. Hyperthyroid states may be associated with elevated CO, wherein thyroid hormone can directly augment myocardial contractility as well as reduce SVR [20]. Interestingly, associations between abnormal thyroid function and PAH have been reported in up to half of such patients although hypothyroidism has been identified more commonly than hyperthyroidism [21, 22]. Thyroid disorders are particularly common in patients with APAH related to autoimmune disorders, potentially reflecting a common autoimmune basis in these patients. The potential pathogenic role of abnormal thyroid function in the development of PAH remains unclear; however, the association between thyroid dysfunction and pulmonary vascular disease is recognized by its inclusion in Group 5 (PH with unclear multifactorial mechanisms) of the current classification scheme [4].
Patients with end-stage renal failure who have an arteriovenous fistula for dialysis access are at risk for development of high cardiac output if the fistula flow becomes excessive. If such patients are undergoing hemodynamic catheterization, temporary occlusion of the fistula may enhance understanding of the contribution of the fistula to the high output state. Measurement of the fistula flow can be achieved by use of ultrasound or Fresenius clearance method [23]. If the fistula is resulting in excessive flow, banding of the fistula may be helpful. Arteriovenous malformations, particularly abdominal, also may result in high flow states.
Thus, while all these conditions can contribute to elevated cardiac output, they are rarely the sole cause of significant, symptomatic PH. However, they all may serve to unmask or exacerbate an underlying primary pulmonary vasculopathy (i.e., a process characterized by abnormal PVR) by superimposing an obligatorily increased Q p on an already restricted pulmonary vascular bed. In such a scenario, the normal plasticity of the pulmonary circulation is impaired which results in higher mPAP at any given level of flow.
In the context of a discussion on elevated pulmonary blood flow and PH, two conditions deserve additional comment. The first relates to elevations in Q p occurring in the context of a left-to-right anatomic shunt. Congenital defects in this category include ventricular septal defect (VSD), atrial septal defect (ASD), and patent ductus arteriosus (PDA), as well as more complex lesions such as truncus arteriosus, transposition of the great vessels, and syndromes characterized by single ventricle physiology. Anomalous pulmonary venous drainage (APVD) is another type of congenital defect associated with left-to-right shunting wherein one or more pulmonary veins return oxygenated blood to a systemic vein (most often the superior vena cava) or right atrium, and commonly co-exist with an ASD (usually sinus venosus type). In the case of VSD, ASD, or PDA, large defects typically present in infancy. However, smaller defects (in particular ASD) may go unnoticed for decades and not come to medical attention until well into adulthood [24, 25]. Initially, such anatomic defects cause PH by virtue of increased pulmonary blood flow mediated by the left-to-right shunt (elevated Q p:Q s), and PVR is normal. Over time, the increase in pulmonary blood flow can incite pathogenic changes within the pulmonary arterioles resulting in an obliterative pulmonary vasculopathy characterized by an elevated PVR. A higher pressure burden as seen in cases of VSD or PDA, combined with the detrimental effects of high flow and shear stress, may be an important factor in the more rapid development of pulmonary vascular disease in these subsets. As the process progresses, right-sided pressures increase, right ventricular insufficiency ensues, and the shunt may reverse (or become bidirectional) with resultant hypoxemia, known as Eisenmenger syndrome. Careful hemodynamic characterization with attention to the relative contributions of elevated Q p and/or PVR to elevated PAP and utilization of pulmonary vasodilator challenge to assess reversibility are crucial to determine whether correction of the defect and/or institution of pulmonary vasoactive therapy is warranted.
Cirrhosis of the liver, particularly when advanced, is also associated with a hyperdynamic state characterized by elevated systemic and pulmonary blood flow, reduced SVR [26], and potentially increased cardiac filling pressures due to excessive salt and water retention. When abnormal pulmonary pressures are identified in this population, it is more frequently related to elevated cardiac output and/or PCWP [27, 28]. However, similar to the case of an anatomic shunt, it is critical to distinguish this scenario from that where the primary hemodynamic abnormality is an elevation in PVR. This latter condition is known as portopulmonary hypertension (PoPH) and occurs in ~5 % of patients with chronic liver disease being evaluated for liver transplant [28, 29]. The presence of portal hypertension is a prerequisite for the development of PoPH, although there is no clear association between the etiology or severity of portal hypertension and the presence or severity of PoPH [30, 31]. PoPH is classified within Group 1 of the current PH classification scheme, displays pathologic changes identical to those seen in idiopathic PAH [32], and harbors a worse prognosis compared to patients with chronic liver disease without PoPH [33, 34]. Significant, untreated PoPH is associated with increased mortality in the setting of liver transplantation [33, 35, 36] and may represent a contraindication to the procedure. Patients being evaluated for liver transplantation should be screened for pulmonary hypertension by echocardiography and if found should be further evaluated by right heart catheterization [37].
Elevated PCWP
Elevation in left atrial pressure and subsequent pulmonary venous hypertension, as reflected by elevated PCWP, is the final common pathway by which various forms of left heart disease can cause PH. Systolic, restrictive, or infiltrative cardiomyopathies as well as mitral or aortic valvular disease all can lead to a rise in left atrial pressure that is transmitted back to the pulmonary arteries via the pulmonary veins. Heart failure with preserved ejection fraction (HFpEF) is increasingly recognized as a cause of chronic dyspnea, congestive heart failure, and PH. A community-based study of subjects ≥65 years of age suggests an overall prevalence of CHF of ~9 %, over half of which are associated with normal EF on echocardiography [38]. Comorbidities that frequently associate with HFpEF include older age, female sex, hypertension, atrial fibrillation, and obesity [39–41]. PH may be exceedingly common in elderly patients with HFpEF; a community-based echocardiographic study (wherein an RVSP ≥35 mmHg defined the presence of PH) has indicated an overall prevalence of PH in this population of 83 %, compared with 8 % in elderly hypertensive patients without HFpEF [42].
Occasionally, pulmonary venous hypertension may exist in the absence of left atrial hypertension in the setting of pathologic processes that primarily affect the pulmonary veins. Rarely, bulky adenopathy (such as that seen in sarcoidosis [43], tuberculosis [44], histoplasmosis, or other chronic granulomatous diseases or metastatic malignancy) or fibrosing mediastinitis [45] may lead to pulmonary vein obstruction. More recently, catheter ablation with pulmonary vein isolation, used for the treatment of atrial fibrillation, has been associated with the development of pulmonary vein stenosis and subsequent PH [46, 47].
Elevated PVR
Abnormalities in PVR may result from a broad array of pathophysiologic mechanisms, and thus, this hemodynamic abnormality encompasses a heterogeneous group of disorders spanning Groups 1, 3, 4, and 5 of the PH classification scheme. This chapter uses the term PAH (pulmonary arterial hypertension) to refer to conditions in this category wherein the primary pathophysiologic determinant is an elevated PVR.
Group 1 PAH
This group includes idiopathic (IPAH; formerly “primary pulmonary hypertension”), heritable (HPAH), and drug/toxin-mediated forms of pulmonary arterial hypertension as well as those associated with certain underlying conditions (APAH), namely congenital heart disease with left-to-right shunts, connective tissue disease (CTD), HIV infection, portal hypertension, and schistosomiasis infection. Two other rare forms of PH include pulmonary veno-occlusive disease (PVOD), characterized by obliterative lesions in the septal and preseptal pulmonary veins, and pulmonary capillary hemangiomatosis (PCH), characterized by extensive proliferation of the pulmonary capillaries into alveolar septa, bronchial walls, and the pleura; these entities are subclassified as Group 1′. PVOD may represent up to 10 % of PAH cases otherwise thought to be idiopathic [48]. It presents with symptoms similar to IPAH, but is associated with more severe derangements in oxygenation and diffusion capacity. PVOD can cause unique chest imaging findings not found in other forms of PH that should raise suspicion for this diagnosis (see section “Chest Computed Tomography (CT)”). Occult alveolar hemorrhage on bronchoalveolar lavage is also suggestive [49]. Patients with PVOD treated with pulmonary vasoactive therapy can develop life-threatening pulmonary edema due to pulmonary arteriolar vasodilation in the setting of fixed venous outflow obstruction [50].
All of the above entities are associated with similar pathologic findings within the pulmonary vascular bed, including medial hypertrophy, intimal and adventitial fibrosis, in situ thrombosis, and the advanced plexiform lesion [51]. As the disease process progresses and PVR rises, the afterload imposed on the right ventricle increases and higher pressures are required to maintain a given level of cardiac output.
Group 3 PH
Group 3 includes primarily respiratory-related disorders characterized by hypoxemia and/or hypoventilation, including all forms of obstructive and restrictive lung disease, neuromuscular or chest wall/skeletal disorders, and sleep-disordered breathing (obstructive sleep apnea and obesity hypoventilation syndrome). Patients in this group have been uniformly excluded from all of the pivotal, randomized, controlled trials of targeted PAH therapies. Although hypoxic vasoconstriction and subsequent vascular remodeling may be a final common pathway for the development of PH in many of these disparate conditions [52, 53] (discussed in greater detail in Chap. 4), other unique pathobiologic mechanisms exist that can contribute to elevations in PAP and PVR in each particular disorder. COPD, for example, is uniquely associated with hyperinflation, which can contribute to an elevated PVR due to increased alveolar pressure and compression of intra-alveolar vessels [54]. In idiopathic pulmonary fibrosis, there may be “spillover” of the inflammation in the epithelial compartment into the adjacent endothelial compartment, contributing to vascular obliteration and a rise in PVR [55, 56].
Group 4 PAH
Pulmonary arterial hypertension in this category is thought to occur from vascular obstruction due to recurrent embolic and/or in situ thrombotic events with organization and incorporation of the thrombotic material into the vessel wall. The incidence of chronic thromboembolic pulmonary hypertension (CTEPH) may be as high as 3.8 % up to 2 years after an embolic event [57]. However, because not all patients with CTEPH can recollect a discrete embolic event, the true incidence of the disease may be higher. While pulmonary arterial obstruction by organized thrombi is the sine qua non of CTEPH, patients can exhibit histopathologic changes in the small pulmonary arterioles that are indistinguishable from those seen in IPAH, and these have been observed to occur in regions of the lung spared from large-vessel obstruction [58].
Pulmonary thromboendarterectomy is a technically demanding procedure in which proximal organized thrombi are surgically removed. Individuals with more proximal, surgically accessible disease appear to derive the greatest benefit from the procedure [59], underscoring the importance of a meticulous characterization of the burden of pulmonary vascular disease and its location based on information from RHC, CT angiogram, pulmonary angiography, and, at some centers, pulmonary angioscopy [60]. Chapter 6 of this text presents a more in-depth discussion of CTEPH.
Group 5 PH
Group 5 represents a collection of disorders that have been associated with pulmonary arterial hypertension due to unique and/or ill-defined mechanisms. The current classification scheme subdivides such entities into specific categories, including hematologic (myeloproliferative disorders, splenectomy, chronic hemolytic anemias), systemic (sarcoidosis, pulmonary Langerhans cell histiocytosis, neurofibromatosis, lymphangioleiomyomatosis, neurofibromatosis, vasculitis), metabolic (glycogen storage disease, Gaucher disease, thyroid disorders), and other (tumor obstruction, fibrosing mediastinitis, chronic renal failure on dialysis).
Although some forms of Group 5 PH such as those associated with sarcoidosis and metabolic disorders closely resemble Group 1 PAH, every randomized controlled trial of PAH therapy has excluded patients with Group 5 disease.
Clinical Approach: History
A detailed history provides a wealth of information in the evaluation of a patient with known or suspected PH. Relevant elements of the history can provide information regarding the likelihood of PH being present, its potential cause or causes, and inform the clinician as to its severity and response to treatment.
The most common symptom associated with most forms of PH is dyspnea, particularly dyspnea on exertion. It is reported in virtually all patients and is often of a progressive nature. Other common symptoms include fatigue, exertional near-syncope or syncope, chest pain, edema, and palpitations [13]. The degree of dyspnea should be quantitated, and an assessment of functional class performed according to WHO criteria [61], modeled on the New York Heart Association functional class schema for patients with CHF (Table 8.2). Patients with PH may have a progressive decline in their functional capacity resulting in gradual curtailment of activities to a level where dyspnea is minimized. This can result in an apparent overestimation of functional ability by some patients, which can be elucidated with an assessment of specific activities and asking the patient how easily he or she can perform such activities now as compared with a point in the past (e.g., “How easy is it for you to climb two flights of stairs now as compared with 6 months or a year ago?” or “Are there any activities you used to do that you have stopped recently?”). Soliciting the perspective of a close contact can be helpful in corroborating or refining the patient’s assessment. Young patients, particularly those who are athletic or otherwise very fit, may report only a decrement in their ability to tolerate prolonged exercise which may be erroneously ascribed to deconditioning; this may in fact represent early pulmonary vascular disease with an impaired CO response to higher workloads.
The development of exertional chest discomfort or syncope is a potentially ominous sign of significant right ventricular (RV) ischemia and/or dysfunction and should impart an element of expediency to the diagnostic workup or modification of treatment in cases of known PAH. Anginal chest pain in PAH may arise due to increased oxygen demand from increased RV muscle mass, reduced oxygen supply due to reduced right coronary artery flow with impaired microcirculation due to right ventricular hypertrophy, and in some cases compression of the left main coronary artery by an enlarged pulmonary artery [62, 63]. In the seminal, prospective primary pulmonary hypertension registry, syncope eventually occurred in >1/3 of subjects [13] and is caused by the inability of the RV to increase CO in the face of increased demand and/or systemic vasodilation. Beyond the impairment to flow attributed to elevations in PVR, pathologic ventricular interaction results in reduced left ventricular diastolic compliance, which further limits the ability to maintain left ventricular stroke volume and adequate systemic perfusion pressure [64–67]. The abrupt onset of dyspnea in a patient with other clinical features to suggest PH should prompt consideration of acute pulmonary embolism (PE), either in isolation or superimposed on a background of chronic thromboembolic disease.
During the initial diagnostic phase, additional historical elements should be elicited to help formulate the differential diagnosis. A relatively short survey of comorbid conditions and possible associated symptoms will help the clinician quickly discern potential etiologic categories that may account for PH, and is summarized in Table 8.3. From a statistical perspective, given the relative rarity of idiopathic PAH, one should maintain a high index of suspicion of secondary pulmonary hypertension, keeping in mind that the most common cause of right heart failure is left heart failure. As such, consideration of various forms of left heart disease should be a priority in otherwise “undifferentiated” PH. Significant left ventricular systolic dysfunction or aortic or mitral valvular disease is usually readily apparent on transthoracic 2DE. An increasingly common clinical problem is that of differentiating pulmonary venous hypertension related to HFpEF (PH-HFpEF) and PAH. As discussed previously, PH appears to be a common occurrence in HFpEF [42]. Echocardiographic clues to the presence of HFpEF include Doppler features of significant diastolic filling abnormality and presence of left atrial enlargement. Conversely, some patients with PAH, particularly when more advanced, may display echocardiographic evidence of impaired left ventricular filling due to pathologic ventricular interaction [68]. In a cross-sectional study comparing PH-HFpEF and PAH, historical features more frequently associated with PH-HFpEF included older age and the presence of systemic hypertension or coronary artery disease [69]. (It should be mentioned that in this study, those with PH-HFpEF had some element of pulmonary vascular disease as the authors required an elevation in PVR or transpulmonary gradient as part of the definition of PH-HFpEF.) However, it is important to recognize that the presence of PAH is not protective against the development of these more common comorbidities and thus can co-exist. Moreover, while the classic presentation of IPAH is that of a young woman with progressive dyspnea, PAH is being diagnosed with increased frequency in the elderly; contemporary registries suggest that ≥20 % of PAH subjects are >60 years of age [10, 11].
If suspicion of left heart disease as a primary cause of PH is relatively low, then a thorough search should be undertaken to identify other associated or secondary causes of PH. Connective tissue diseases are the most common underlying conditions predisposing to the development of PAH, and as such CTD features should be sought out. In a single-center cohort of elderly patients (>65 years of age) referred for evaluation of PH, the presence of CTD was found to be a strong predictor of PAH [70]. Scleroderma (both limited and diffuse forms) and mixed connective tissue disease are the two specific CTDs most commonly associated with PAH, followed by systemic lupus erythematosus (SLE), and less frequently rheumatoid arthritis, polymyositis/dermatomyositis, and Sjögren syndrome [11, 71, 72]. Occasionally, PAH may occur in the absence or precede the development of other symptoms or exam findings to suggest scleroderma (“scleroderma sine scleroderma”) or another specific CTD. A directed history aimed at symptoms of esophageal dysfunction, Raynaud’s phenomenon and autoantibody testing may help identify a “latent” CTD [73, 74]. A history of medical problems in the postnatal period or childhood heart murmur should be obtained as a clue to potential underlying congenital heart disease. The presence of chronic cough, sputum production, or wheezing may indicate underlying obstructive or restrictive lung disease. Snoring, witnessed apneas, morning headaches, or excessive daytime sleepiness suggests the presence of sleep-disordered breathing. A prior history of deep venous thrombosis or PE may raise the suspicion for CTEPH, although 25–50 % of CTEPH patients lack prior knowledge of any thrombotic event [75–77]. Large PE, unprovoked and/or multiple embolic events, younger age, or the presence of certain medical conditions, such as splenectomy, ventriculo-atrial shunts, inflammatory bowel disease, or positive antiphospholipid antibodies, may predispose to the development of CTEPH [57, 76, 78].
A social history should be performed, documenting any pertinent travel or occupational history, anorexigen (Aminorex or fenfluramine derivatives) or recreational (stimulants, including amphetamine compounds [79]) drug exposure, and risk factors for liver cirrhosis, HIV or viral hepatitis infection. While PAH associated with HIV infection remains relatively rare, the diagnosis should be considered in any patient with HIV with dyspnea of unknown origin, irrespective of the level of immune compromise [80]. A family history is necessary to assess for heritable PAH, which in a majority of cases is caused by mutations in the gene encoding the TGF-β receptor BMPR2 and displays an autosomal dominant pattern of inheritance [81–84]. However, due to incomplete penetrance, patients with heritable PAH may not always recollect a family member known to be afflicted with the disease. Alternatively, affected family members of previous generations may have been misdiagnosed as having another cardiopulmonary condition given a relative lack of awareness of PAH in preceding decades.
Clinical Approach: Physical Examination
In concert with a focused history, the physical examination can offer critical insights into the possible causes of PH and it severity. An anatomic-based approach is presented here.
Head and Neck
Underlying conditions that can predispose to PH often have manifestations in the head and neck. Sarcoidosis may be associated with cranial nerve deficits, parotid or lacrimal gland enlargement, ocular findings (uveitis, conjunctival nodules), or hypopigmentation around the hairline. Lymphadenopathy might suggest sarcoidosis or a lymphoproliferative disorder. Scleral icterus suggests hepatobiliary dysfunction. Proptosis in conjunction with an enlarged thyroid may be indicative of Graves’ disease. An enlarged tongue, or periorbital purpura, may suggest systemic amyloidosis. Stigmata of connective tissue disease include malar rash, oral ulcers, loss of naso-labial folds, microstomia, and telangiectasias. A preponderance of telangiectasias involving mucous membranes should also raise suspicion of hereditary hemorrhagic telangiectasia (Osler-Weber-Rendu syndrome). A short, thick neck with low-riding soft palate or tonsillar crowding should raise the possibility of obstructive sleep apnea. Hypoxemic patients may display peri-oral cyanosis. Ulceration of the nasal septum may be seen in either sarcoidosis or ANCA-associated vasculitis. Aortic stenosis may result in a delayed carotid upstroke, whereas a bounding pulse may indicate aortic insufficiency or a hyperdynamic circulation, as seen in advanced cirrhosis, hyperthyroid states, or left-to-right shunting. An assessment of jugular venous pressure should be made in all patients as a surrogate for right atrial pressure; prominent v waves within the venous pulse contour indicate the presence of tricuspid regurgitation.
Cardiovascular
For obvious reasons, a careful cardiac examination is required in all patients with suspected PH. A prominent pulmonary component of the second heart sound (P2) heard best over the left sternal border in the second to fourth intercostal space is present in most patients with idiopathic PAH, but requires practice to appreciate [13]. Regurgitant murmurs related to tricuspid, and less commonly pulmonic, insufficiency may be found. An RV lift and right-sided S4 are clues to RV hypertrophy. A right-sided S3 indicates compromised RV function and correlates with reduced cardiac output [13]. Right-sided gallops are best appreciated along the left sternal border. Fixed splitting of the second heart sound is observed in the setting of an ASD; a pansystolic murmur may indicate the presence of a VSD, whereas a constant, machine-like murmur is classically associated with a PDA. Murmurs associated with either aortic or mitral valve pathology and S3 or S4 gallops heard best towards the apex suggest underlying left-sided heart disease. Systemic hypotension with a narrow pulse pressure, tachycardia, and cool extremities are ominous signs of a low cardiac output state. Patients suspected of having left-to-right shunting should undergo a search for arteriovenous communications, including iatrogenic fistulae such as those created intentionally for hemodialysis or inadvertently during femoral vascular cannulation.
Pulmonary
Patients with idiopathic, heritable, or toxin-mediated PAH typically have an unremarkable pulmonary examination. In patients with PH due to left-sided heart disease and cardiogenic edema, rales may be appreciated along with dullness to percussion signifying the presence of pleural effusions; the latter finding may also be associated with liver disease. Fine, Velcro-type rales suggest fibrotic lung disease. Wheezing or rhonchi should prompt consideration of chronic obstructive pulmonary disease. Patients with chronic thromboembolic disease may exhibit a pulmonary artery bruit, caused by turbulent blood flow through narrowed proximal pulmonary arteries. The bruit is heard best by auscultation of the interscapular area during a breath hold.
Gastrointestinal
Hepatomegaly, pulsatility of the liver, and ascites may be seen in the setting of chronic elevations in right heart pressure due to PH of any cause. Concomitant splenomegaly or the presence of caput medusae suggests underlying portal hypertension, whereas isolated splenomegaly may be indicative of a lymphoproliferative disorder. Ascites can be a presenting manifestation of constrictive pericarditis. Occasionally, patients with PAH treated with epoprostenol may develop ascites in the absence of portal hypertension [85]. Epoprostenol therapy also has been associated with progressive splenomegaly when used for the treatment of patients with portopulmonary hypertension [86, 87].
Skin, Muscles, and Joints
A thorough musculoskeletal and skin examination should be performed with particular attention to findings that may implicate an underlying connective tissue disease, such as skin thickening, sclerodactyly, rash, telangiectasias (which could also indicate liver cirrhosis), synovitis, or ulcerative lesions. Clubbing of the digits may be seen with interstitial or chronic hypoxemic lung disease, cystic fibrosis, bronchiectasis, thoracic malignancy, congenital cyanotic heart disease, pulmonary veno-occlusive disease (PVOD), and chronic inflammatory states such as inflammatory bowel disease or endocarditis. Muscle wasting may reflect generalized malnutrition or neuromuscular disease. In patients receiving vasodilator therapy for PAH (in particular prostacyclin analogues), flushing of the skin may be noted.
Diagnostic Testing
Echocardiography
In contemporary practice, 2DE remains the most common modality leading to suspicion of PH and the most common screening tool used to assess patients suspected of having PH. It can readily estimate pulmonary arterial systolic pressure (assuming certain conditions are met) and also provides supplementary anatomic and physiologic information that can help elucidate the underlying pathophysiologic mechanisms responsible for PH as well as gauge its severity vis-à-vis right heart function. 2DE is best used as a screening tool when PH is suspected due to the presence of certain symptoms or examination findings. 2DE is discussed in more detail in Chap. 9, but a brief discussion will be presented here.
When faced with an echocardiogram reporting elevations in pulmonary arterial systolic pressure (PASP), the clinician must attempt to answer several questions:
-
1.
Is the reported PASP accurate?
-
2.
If accurate, does the patient indeed have PH?
-
3.
If PH is present, what is the etiology?
-
4.
To what degree is the presence of PH impacting circulatory function?
2DE is an imperfect diagnostic test with limitations in both sensitivity and specificity. Nevertheless, an understanding of its strengths and limitations will allow the clinician to risk-stratify a patient with cardiopulmonary symptoms and help direct the remainder of the diagnostic evaluation.
Echocardiography laboratories typically calculate and report PASP using the modified Bernoulli principle, according to the following equation:
PASP will equal RV systolic pressure (RVSP) in the absence of pulmonic valve stenosis. TRvel and RAP denote Doppler-derived velocity of the tricuspid regurgitation (TR) jet and an estimate of right atrial pressure, respectively. While there is some debate as to the upper limit of normal of 2DE-derived PASP, a value of 40 mmHg is reasonable based on the available evidence, although older subjects may require a higher cutoff [1, 88]. In carefully studied populations, there is a strong correlation between 2DE- and RHC-derived values for PASP using traditional linear regression analysis when comparative measurements are obtained in close temporal proximity [89, 90]. However, suboptimal visualization or improper Doppler interrogation of the TR jet may lead to inaccurate estimates of TRvel; the error associated with this inaccuracy is then magnified exponentially. Also, some patients will have insufficient TR to measure TRvel. Estimates of RAP based on an assessment of inferior cava collapsibility are also prone to error [91]. Contemporary studies of PH referral populations using Bland-Altman analysis suggest that ~50 % of 2DE-derived PASP estimates are inaccurate; both over- and underestimation occur, though the magnitude of underestimation appears to be greater [91, 92]. Thus, 2DE estimates of PASP should be viewed as simply one piece of information as part of a broader 2DE assessment of the right heart–pulmonary circulation–left heart axis.
Because the hemodynamic definition of PH requires knowledge of the mean PAP, PASP from 2DE cannot be used to define the presence or absence of PH. Although techniques exist to derive mPAP from acceleration time within the RV outflow tract (RVOT) [93], they are not commonly reported on most echocardiograms. Alternatively, mPAP may be estimated using formulas based on PASP [94, 95]; however, such methods are not recommended to replace invasive determination of mPAP by RHC, wherein other hemodynamic variables pertinent to the evaluation of patients with suspected pulmonary vascular disease can be obtained.
If the 2DE-derived PASP is consistent with PH, perhaps the most critical issue the clinician faces is determining the likelihood that the PH is arterial (i.e., PAH) vs. venous (related to left atrial hypertension) in origin, given the ramifications for prognosis and management. In such cases, RHC is required to confirm (or refute) the suspicion and guide therapy. While RHC has a relatively low risk of complications, performing RHC on all patients with elevated PASP on 2DE is neither practical nor desirable. At present, the ideal approach to noninvasively gauge the pretest probability of pulmonary vascular disease so as to optimize use of RHC is unknown. In practice, this decision is influenced by several factors, including the patient’s risk of harboring PAH, results of other noninvasive testing (discussed below), and features on 2DE.
Beyond estimation of PASP, a thorough survey of parameters of right and left heart chamber size and function can be extremely helpful in assessing the likelihood that PAH is present. In general, the greater the extent of abnormalities related to right heart size and/or function, the higher the likelihood of PAH. When abnormalities in left heart size and/or function dominate the echocardiographic picture, there is a greater likelihood of pulmonary venous hypertension [96]. Simple indices of right heart pressure or volume overload easily seen on an apical four-chamber view include an RV:LV size ratio >1, flattening or leftward bowing of the interventricular septum, and encroachment of the RV into the apex. The presence of a mid- or late-systolic “notch” within the RVOT Doppler flow velocity envelope strongly predicts the presence of a PVR >3 Wood units [97]. A reduced tricuspid annular plane systolic excursion (TAPSE) is an easily obtainable surrogate of compromised RV longitudinal shortening and cardiac output, and has prognostic value in PAH [98–100]. When such findings are seen in the absence of significant left heart abnormalities, the clinician should increase his/her suspicion that PAH is present. In contrast, left ventricular systolic or diastolic dysfunction, left ventricular enlargement or hypertrophy, left atrial enlargement, or significant aortic or mitral valvular disease suggests a substrate for increased left atrial pressure and thus pulmonary venous hypertension. A 2DE-based prediction rule incorporating left atrial size, Doppler-based parameters from the RVOT (acceleration time, presence of notching), and lateral mitral E:e′ (a surrogate for left atrial filling pressure) was recently shown to have an area under the receiver operator characteristic (ROC) curve of 0.92 for the identification of PAH [101]. A pericardial effusion, while not specific for PAH, has been consistently associated with a poor prognosis in this group [102–105]. Lastly, 2DE (with or without agitated saline contrast) may disclose evidence of an intracardiac shunt, which could be the cause of PH (e.g., ASD, VSD, PDA), or, in the case of a PFO, may explain significant shunt-type hypoxemia in a patient with idiopathic or other types of PAH and elevated right heart pressures. If suspicion of an intracardiac shunt is high but transthoracic 2DE is nondiagnostic, transesophageal echocardiography [106] or cardiac magnetic resonance [107] should be performed. A comparison of various 2DE parameters which can help the clinician distinguish pulmonary arterial vs. venous hypertension is provided in Table 8.4.
The issue of diastolic dysfunction in the context of PH deserves additional comment. The clinician should recognize that diastolic dysfunction may worsen with exercise due to further impairment in filling time secondary to increased heart rate, and as such may be underappreciated as a cause of exertional dyspnea based on 2DE parameters obtained at rest. In such situations, assessment of diastolic function with exercise 2DE may be informative [108]. While diastolic dysfunction appears to be very common, particularly in the elderly or those with other comorbidities as discussed previously, patients with PAH due to pulmonary vascular disease may also exhibit impaired left ventricular relaxation as a consequence of pathologic right → left ventricular interaction [66, 109]. A recent study of idiopathic/heritable PAH patients found an 88 % prevalence of Grade 1 diastolic dysfunction (impaired relaxation) [68]. Thus, the simple presence of mild diastolic dysfunction or impaired relaxation in the setting of an elevated PASP should not be considered synonymous with pulmonary venous hypertension. Rather, the clinician should attempt to integrate this finding with the overall clinical picture and echocardiographic assessment of left and right heart function to arrive at an assessment of the likely etiology of PH.
Using 2DE as a screening tool in populations considered at high risk for PAH has been recommended by various professional societies, although this is largely based on expert opinion [6–8]. Regular screening with 2DE seems reasonable for patients with a family history of PAH or with known BMPR2 mutations given that ~20 % of carriers will ultimately develop PAH [110, 111]. In dyspneic patients with scleroderma but without significant lung disease, ~8 % will have PAH by RHC [112]. Screening of patients with the scleroderma spectrum of diseases is recommended. The DETECT study provides useful guidance in this regard [113]. Screening methods in this setting can include a combination of PFTs with diffusion capacity for carbon monoxide (DLco), serum levels of brain natriuretic peptide (BNP) or its N-terminal pro-hormone (NT-proBNP), and echocardiography. As mentioned previously, given the elevated morbidity associated with uncontrolled portopulmonary hypertension in the setting of liver transplantation, 2DE should be performed in all patients being considered for this procedure [37].
Chest X-ray (CXR)
Given its relative low cost and ease, the CXR can provide useful information in the evaluation of patients with suspected PH; however, its suboptimal sensitivity precludes its use as a primary screening modality [114]. General CXR findings of PH include enlarged main pulmonary arteries and right-sided cardiac chamber enlargement; however, such changes may not be apparent in less advanced PH. In the NIH primary PH registry, 90 % of subjects displayed prominence of the main pulmonary artery [13]. An obliterated retrosternal air space as visualized on the lateral projection specifically suggests RV hypertrophy. When PAH is present and related to increased PVR, rapid tapering (or “pruning”) of the pulmonary arteries may be seen. In contrast, when PH is related to increases in left atrial pressure or high pulmonary flow from an anatomic shunt, increased vascular markings and Kerley B lines may be observed; a similar pattern is associated with PVOD where the resistance to blood flow through the small pulmonary veins can result in areas of increased pulmonary capillary pressure. Focal areas of oligemia or an abrupt cutoff of a pulmonary artery should raise suspicion for CTEPH [115], particularly when pleural abnormalities are present which may represent sequelae of prior infarcts [116, 117]. Calcification of the pulmonary arteries has been described in congenital heart disease with reversed shunts (Eisenmenger syndrome) [118], and occasionally large pulmonary artery aneurysms may develop in cases of long-standing PAH. CXR may be particularly useful in assessing for associated conditions that may cause PH, such as hyperinflation (COPD), increased reticulation/cystic changes/honeycombing (interstitial lung disease/pulmonary fibrosis), or reduced lung volumes that may be associated with hypoventilation (obesity hypoventilation syndrome, neuromuscular, or skeletal conditions).
Electrocardiogram (ECG)
Like CXR, the ECG is a readily obtainable ancillary tool that may corroborate a suspicion for PH, but is of limited sensitivity, particularly in the detection of early disease [114]. While a majority of patients with significant PAH will display findings of right axis deviation, RV hypertrophy or RV strain, up to 13 % of patients will have a normal ECG [13, 119]. Recently, a QRS duration of ≥120 ms was found to be an independent predictor of mortality in a small cohort of IPAH subjects [120]. When evaluating a patient with known PH who is clinically deteriorating, the ECG can confirm suspicion of a tachy- or bradyarrhythmia as a contributing factor.
Pulmonary Function Tests (PFTs) and Arterial Blood Gas (ABG) Analysis
PFTs are commonly obtained in the evaluation of the dyspneic patient. In the context of suspected PH, they are extremely important in determining whether airway or parenchymal lung processes are present which may account for PH (i.e., Group 3 PH). A mild restrictive defect may be seen in IPAH [13, 121] and may be related to bronchial and vascular smooth muscle hypertrophy [122] or respiratory muscle weakness [123, 124]. Interestingly, IPAH has also been associated with peripheral airway obstruction [125, 126]. Thus, mild perturbations in pulmonary function indices should not immediately implicate the presence of intrinsic lung disease, but should trigger consideration of such potential etiologies; in such cases, chest CT can be very useful in refining the clinical assessment. The attribution of PH to intrinsic parenchymal or airway disease engenders uncertainty when spirometric or lung volume parameters fall within moderate grades of dysfunction, as studies have not typically proven a strong correlation between the severity of lung disease and the presence or severity of PH, although PH is typically associated with more advanced lung disease [43, 127–133]. Recently, PH has been identified as a significant complication of the combined pulmonary fibrosis and emphysema syndrome [134, 135]. These patients may display relatively preserved (“pseudonormalized”) spirometry and lung volumes due to the counterbalancing effects of coexistent restriction and obstruction, but typically have significant reductions in DLco and abnormal CT imaging.
It appears that an assessment of DLco may be a more specific marker of pulmonary vascular disease, particularly when reduced “out of proportion” to reductions in lung volumes. A reduced DLco is common in IPAH (found in 75 % of patients [121]), and in the scleroderma population may signal the occult presence or future development of PH [136]. In a cohort of scleroderma patients suspected of having PH based on certain clinical characteristics, a percent-predicted FVC/DLco ratio of >2 displayed a negative and positive predictive value of ~70 % for the diagnosis of PAH [137]. Utilizing a lower cutoff (>1.6) [138] may improve the sensitivity of this parameter for the detection of PAH, though comparative data are lacking. In practice, the finding of an isolated reduction in DLco in the absence of significant anemia should heighten one’s suspicion for the presence of pulmonary vascular disease.
ABG analysis should be performed to confirm a suspected hypoventilatory disorder, and may also quantify severity of hypoxemia. If shunt physiology is suspected, the ABG should be performed after inspiring 100 % oxygen for 20–30 min via a tight-fitting mask which can permit estimation of the right-to-left shunt fraction (Q s/Q t) [139].
Ventilation-Perfusion (V/Q) Scintigraphy
The V/Q study remains an integral component of the workup of patients with suspected PH, mainly to exclude the presence of chronic thromboembolic disease. In CTEPH, perfusion images will demonstrate at least one (or multiple) segmental or larger mismatched defects [140, 141]. V/Q has demonstrated superior sensitivity over CT angiography for the diagnosis of CTEPH. In one study where digital subtraction pulmonary angiography was used as the reference standard, V/Q scan displayed 97.4 % sensitivity and 98.5 % negative predictive value for the diagnosis of CTEPH (where a positive test was defined as an intermediate or high probability result), whereas CT angiography only displayed 51.3 % sensitivity and 79.7 % negative predictive value [142]. Thus, a normal V/Q scan essentially rules out chronic thromboembolism. A positive scan, however, cannot be used to make definitive statements regarding the anatomic extent of clot burden as the V/Q tends to underestimate the amount of disease observed at pulmonary angiogram or endarterectomy [143]. Patients with IPAH may also display an abnormal pattern on V/Q, described as a diffuse patchy abnormality or “mottled” appearance [13]. While it has been suggested that a high-probability scan due to PVOD may mimic CTEPH [144], a larger series has recently failed to confirm this association [145]. Rarely, tumor microemboli can lead to a clinical presentation very similar to CTEPH with mismatched defects seen on V/Q scanning [146, 147]. If right-to-left shunt is suspected, the clinician can request additional perfusion images be obtained over the brain and kidneys; detection of tracer in these regions implicates the presence of an anatomic shunt [148], but does not disclose the specific location (intracardiac, intrapulmonary, etc.).
Chest Computed Tomography (CT)
When performed for other reasons, findings on CT that may suggest the presence of pulmonary hypertension include an enlarged pulmonary artery (>29 mm in diameter [149] or pulmonary artery:aorta diameter ratio >1 [150]) and/or enlarged right-sided cardiac chambers with or without septal shift [151, 152], pericardial effusion [153], or reflux of contrast into the IVC and hepatic veins in the setting of elevated right atrial pressure [154]. In patients with chronic dyspnea and clinical concern for PH, nonenhanced CT scanning of the chest should be considered to exclude parenchymal lung disease, particularly when suggested by examination or PFT findings. This may be particularly important in patients with collagen vascular diseases who may be at risk for various types of interstitial disease (e.g., nonspecific, usual, or lymphocytic interstitial pneumonia or organizing pneumonia). PVOD is associated with several specific findings on chest CT that may aid in identifying the diagnosis and are related to the consequences of postcapillary venular obstruction to pulmonary blood flow, such as bilateral pleural effusions, mediastinal lymphadenopathy, and prominence of the interlobular septae and/or centrilobular opacities [155, 156]. This pattern may also be seen with pulmonary venous hypertension arising from left heart disease.
Contrast-enhanced CT angiography (CTA) can provide useful information regarding the anatomy of the pulmonary vasculature. Results from the Prospective Investigation of Pulmonary Embolism Diagnosis (PIOPED) II study indicate that CTA has an overall sensitivity of 83 % for the diagnosis of acute PE; its NPV is 96 % when clinical pretest probability is low, but falls to only 60 % when clinical suspicion is high [157]. CTA may prove useful for mapping proximal clot burden in CTEPH, but displays limited sensitivity for the detection of peripheral small vessel involvement as discussed previously [142]. Endoluminal CTA findings of CTEPH include eccentric or concentric luminal irregularities, abrupt cutoffs, webs, and pouches [158]. Additional findings that may implicate CTEPH include bronchial artery dilation [159, 160] and mosaic attenuation of the lung parenchyma [158, 161], because of either hypoperfusion of obstructed segments or regional air trapping secondary to vascular-mediated alterations in small airway tone. CTA can also identify other nonthrombotic lesions of the pulmonary vascular bed. Takayasu’s arteritis is a large-vessel vasculitis which may affect the pulmonary circulation in a significant number of cases and may be misdiagnosed as CTEPH [162]. The presence of concomitant aortic disease should raise the suspicion for Takayasu’s, although isolated pulmonary arteritis has been reported [163]. Other CTA findings that may differentiate this entity from CTEPH include circumferential pulmonary arterial wall thickening and delayed mural enhancement [164, 165]. Pulmonary artery aneurysms may be seen in Behçet’s disease [165, 166].
Overnight Oximetry and Polysomnography (PSG)
Overnight pulse oximetry in the home is a relatively simple test to search for nocturnal hypoxemia. Nocturnal oxygen desaturation may occur in the IPAH population in the absence of sleep-disordered breathing [167]. Correction with supplemental oxygen is intuitive but it is not known whether such a strategy improves outcomes. Standard polysomnography is the gold standard for the diagnosis of obstructive sleep apnea.
Exercise Testing
The 6-min walk test (6MWT) is a submaximal test of exercise capacity that has been employed extensively in the evaluation and management of patients with PH. It is inexpensive, reproducible, and easy to perform by most patients, even those with more advanced disease. In the PAH population, results from the 6MWT have been shown to correlate with functional class, hemodynamics (CO and total pulmonary resistance), as well as peak oxygen consumption as determined by cardiopulmonary exercise testing [168]. Contemporary, prospective cohort studies indicate that the 6MWT has independent prognostic value in PAH in addition to parameters related to right heart function [102, 169]. Although a matter of some debate, it appears that it is the absolute value of 6MWT that is prognostically most relevant rather than the magnitude of change over time, as studies have failed to show a consistent association between improvements in walk distance on-therapy and outcomes [170–172]. Values below 300–380 m at baseline or after a period of time on-treatment have been associated with a worse prognosis in various studies [168, 173–175].
Cardiopulmonary exercise testing (CPET) is a maximal exercise study which is more labor-intensive, but provides the most comprehensive, integrative assessment of cardiac, pulmonary, and peripheral muscle function at progressively higher workloads. Abnormalities on CPET associated with pulmonary vascular disease include a reduced peak oxygen uptake, increased ventilatory inefficiency (as reflected by an elevated ratio of minute ventilation to CO2 production [V E/V CO2] and reduced end-tidal CO2), and reduced oxygen pulse [176]; however, these are not specific to pulmonary vascular disease and can be seen in obstructive and restrictive disorders as well as left heart failure. This combination of derangements is more likely to represent PAH when other ancillary tests (chest imaging, PFTs, 2DE, etc.) do not suggest an alternate diagnosis. One study of IPAH subjects found peak oxygen uptake to be an independent predictor of mortality [177], prompting some to advocate a treat-to-target (goal-oriented) strategy incorporating this parameter to help guide therapeutic decisions [178]. However, this approach has not been externally validated and therefore the use of CPET for this purpose remains center-dependent. Marked elevation of V E/V CO2 in the absence of major ventilatory abnormality on PFTs can be a sign of right-to-left shunting or thromboembolic PH. CPET is discussed in more detail in Chap. 11.
Serologic Tests
Serologic tests can provide useful information in establishing potential etiologies of PH as well as help guide therapy. From a diagnostic perspective, serologies play a central role in confirming chronic viral hepatitis or HIV infection. The presence of certain autoantibodies may suggest the presence of an underlying connective tissue disease when considered in the context of appropriate clinical features. In the original NIH primary PH registry, 29 % of subjects had a positive antinuclear antibody (ANA) [13]. In scleroderma, anticentromere antibodies are usually associated with limited disease, and anti-Scl-70 antibodies with diffuse disease. The presence of antibodies against U3-RNP (fibrillarin) is associated specifically with PAH [179, 180].
In cases of CTEPH, the only consistent hypercoagulable abnormality identified has been the presence of antiphospholipid antibodies, found in up to 20 % of cases [181, 182]. Most patients, however, do not have any identifiable abnormality in coagulation, and therefore the lack of any laboratory-identified hypercoagulable state cannot be used to exclude the possibility of CTEPH.
BNP and NT-proBNP are proteins released from myocardial tissue in the setting of pressure or volume overload. Serum levels of BNP peptides may be elevated in patients with PAH and RV dysfunction, and lower levels have been associated with better outcomes [102, 175, 183, 184]. It is important to note that BNP is not specific to the RV and can be elevated in left-sided congestive heart failure and in renal dysfunction. In cases where PH is suspected to be related to HFpEF, BNP may be particularly unreliable, as a recent study demonstrated that 29 % of symptomatic outpatients with HFpEF and hemodynamically confirmed elevations in PCWP had a normal BNP level [41]. Studies in left-sided heart failure suggest that elevations in BNP or NT-proBNP may be attenuated by obesity, possibly related to either underproduction or increased peripheral clearance by adipose tissue [185–187]. A recent analysis of a PAH cohort has shown that, despite higher right-sided filling pressures, obese PAH patients have lower BNP levels than those who are not obese [188].
Other laboratory tests frequently obtained include complete blood count and general chemistries including indices of renal and hepatic function. Anemia should raise suspicion of a possible hemolytic disorder in the appropriate clinical context. Among patients with nonhemolytic PAH, iron deficiency and/or frank anemia occurs in ~25–60 % and has been shown to be a negative prognostic factor [189–191]. Anemia can also be seen as a side effect of treatment with endothelin receptor antagonists (ERAs). Thrombocytopenia should raise consideration of cirrhosis, HIV infection, or autoimmune disease. Prostacyclin therapy can also induce thrombocytopenia which in some cases may be related to splenomegaly [86]. Right-sided heart failure can lead to congestive hepatopathy; this pattern usually is characterized by a predominant rise in unconjugated bilirubin with minimal elevation in alkaline phosphatase and transaminases [192], though more dramatic rises in these latter parameters can be seen with severe RV failure and low cardiac output. Alternatively, a predominant liver injury pattern with elevated transaminases has been associated with ERA therapy [193, 194] which is dose-dependent and reversible upon discontinuation. Hyponatremia occurs in the setting of right heart failure and has been associated with worse prognosis [195].
Right Heart Catheterization (RHC)
For reasons discussed previously, RHC remains the gold standard for the diagnosis and characterization of elevated pulmonary artery pressures and is discussed in detail in Chap. 10. RHC serves to confirm the presence of PH, elucidate its hemodynamic origin, and, in cases of precapillary PAH, assess the extent of pulmonary vasoreactivity in response to a short-acting pulmonary vasodilator. Distinguishing between pre- and postcapillary causes of PH is critical, and thus requires an accurate assessment of left-sided filling pressures. Pressure measurements should always be made at end expiration. Failure to do so, or using the digital average reported by the pressure recorder, may result in an underestimation of PCWP and thus misclassification of left heart disease as pulmonary arterial hypertension, particularly in patients with concomitant hypoxic lung disease or morbid obesity [196]. When there is a high suspicion for pulmonary venous hypertension but measured PCWP is normal or borderline, a direct measurement of left ventricular end-diastolic pressure (LVEDP) may help avoid misclassification [197]. RHC by itself is very safe with an extremely low risk of mortality (≤0.2 %) [198, 199].
Assessment of PA Pressures with Exercise
Given that many patients only complain of symptoms with a certain amount of activity, assessing the hemodynamic response to exercise makes intuitive sense to better characterize changes in pressures, flow, and resistance in an attempt to define the predominant pathophysiology. While previous definitions of PH included an exercise criterion (mPAP >30 mmHg at peak exercise), current consensus statements have eliminated a definition of exercise-induced PH [6, 7]. This decision was largely based on growing uncertainty as to what constitutes a normal physiologic response of the pulmonary vascular bed to exercise. A recent literature synthesis on the topic concluded that ~20 % of healthy subjects aged <50 years will exceed an mPAP of 30 mmHg when exercised in the supine position, with an upper limit of normal (defined as 2 standard deviations above the mean) of 37 mmHg at maximal exercise. Older healthy subjects (≥50 years) may in fact have greater rises in pulmonary pressures; in this subgroup, the mean mPAP during “slight” exercise was 29.4 ± 8.4 mmHg, yielding an upper limit of normal of 46 mmHg. Older subjects display higher PCWP with exercise than do younger subjects (16.8 ± 6.5 vs. 10.9 ± 3.9 mmHg) [200].
With these concerns is mind, data exist to suggest that exercise-induced PH may be clinically relevant. Grunig et al. have demonstrated greater rises in PASP with exercise in both asymptomatic carriers of the BMPR2 mutation [201] and relatives of patients with idiopathic and heritable PAH [202]. Tolle and colleagues described CPET characteristics of patients with exercise-induced PAH (defined as a maximum mPAP ≥30 mmHg with PCWP <20 mmHg). This group displayed decrements in aerobic capacity and hemodynamic perturbations that were intermediate between normals and those with resting PAH [203]. Steen et al. performed exercise 2DE on patients with scleroderma who, based on certain clinical characteristics, were deemed to be at higher risk for PH. Exercised-induced PH by 2DE was defined as an increase in the PASP of ≥20 mmHg from baseline. They found that 44 % of patients displayed a positive exercise 2DE, which was confirmed to be PAH by RHC in 81 % of patients; in 12.5 % of cases the positive 2DE was due to pulmonary venous hypertension from diastolic dysfunction [204]. Mild elevations in PA pressure with moderate exercise have been associated with reduced exercise capacity in scleroderma [205]. In a large registry of CTD-associated PAH in the United Kingdom, 16 % of patients in the absence of significant lung disease had exercise-induced PAH as defined by invasive hemodynamic criteria of a mean PAP over 30 mmHg during exercise. Of these, 19 % displayed progression to resting PAH and four out of five reported deaths in this subgroup were attributed to PAH [206]. At present, however, it is unknown whether specific interventions aimed at reducing peak PA pressures in these populations will have a benefit on longer-term outcomes. Recently, a small, uncontrolled pilot study of ambrisentan in scleroderma-spectrum patients with exercise-induced PAH suggested a beneficial effect on hemodynamics and 6-min walk distance [207].
Assessing invasive hemodynamics may be particularly helpful in patients without clear risk factors for PAH and where occult HFpEF is suspected. In a study of 55 patients with exertional dyspnea with normal LVEF, BNP level, and resting hemodynamics, 58 % of subjects displayed abnormal increases in left-heart filling pressures (defined as PCWP ≥25 mmHg) with exercise [208]. In the series of patients undergoing CPET and exercise RHC for the evaluation of unexplained dyspnea reported by Tolle et al., 27 % of subjects were identified as having left ventricular diastolic dysfunction [203].
Concluding Remarks
Pulmonary hypertension can occur in many contexts. Echocardiographic diagnosis of PH has become increasingly common due to increased use of 2DE for the assessment of various cardiac and pulmonary complaints. Differentiation of pulmonary arterial from pulmonary venous hypertension is crucial to identify patients with an elevated risk of morbidity and mortality and allow institution of appropriate therapies. Ultimately, the diagnosis of PAH must be made at right heart catheterization. A thorough history, physical examination, laboratory investigation, and use of ancillary tests will aid the clinician in formulating a pretest probability of pulmonary vascular disease.
Table 8.5 summarizes various clinical features that should trigger suspicion for the presence of pulmonary arterial hypertension. In general, the greater number of such features, the higher the likelihood of PAH. In such patients, RHC should be pursued, and measurement of exercise hemodynamics should be considered if resting values are not informative.
Abbreviations
- 2DE:
-
2-Dimensional echocardiography
- 6MWT:
-
6-min Walk test
- ABG:
-
Arterial blood gas
- AcT:
-
Acceleration time
- ANA:
-
Antinuclear antibody
- ANCA:
-
Antineutrophil cytoplasmic antibody
- APAH:
-
Associated pulmonary arterial hypertension
- APVD:
-
Anomalous pulmonary venous drainage
- ASD:
-
Atrial septal defect
- AV:
-
Aortic valve
- BMPR2:
-
Bone morphogenetic protein receptor type 2
- BNP:
-
Brain natriuretic peptide
- CO:
-
Cardiac output
- CPET:
-
Cardiopulmonary exercise test
- CT:
-
Computed tomography
- CTA:
-
Computed tomographic angiography
- CTD:
-
Connective tissue disease
- CTEPH:
-
Chronic thromboembolic pulmonary hypertension
- CXR:
-
Chest X-ray
- DLco:
-
Diffusing capacity of the lung for carbon monoxide
- ECG:
-
Electrocardiogram
- FVC:
-
Forced vital capacity
- FVE:
-
Flow velocity envelope
- HFpEF:
-
Heart failure with preserved ejection fraction
- HIV:
-
Human immunodeficiency virus
- HPAH:
-
Heritable pulmonary arterial hypertension
- IPAH:
-
Idiopathic pulmonary arterial hypertension
- IVC:
-
Inferior vena cava
- JVD:
-
Jugular venous distention
- LA:
-
Left atrium
- LV:
-
Left ventricle
- LVEF:
-
Left ventricular ejection fraction
- LVH:
-
Left ventricular hypertrophy
- mPAP:
-
Mean pulmonary artery pressure
- MV:
-
Mitral valve
- NIH:
-
National Institutes of Health
- NYHA:
-
New York Heart Association
- PAH:
-
Pulmonary arterial hypertension
- PASP:
-
Pulmonary artery systolic pressure
- PCWP:
-
Pulmonary capillary wedge pressure
- PDA:
-
Patent ductus arteriosus
- PE:
-
Pulmonary embolism
- PFT:
-
Pulmonary function test
- PH:
-
Pulmonary hypertension
- PIOPED:
-
Prospective Investigation of Pulmonary Embolism Diagnosis
- PoPH:
-
Portopulmonary hypertension
- PSG:
-
Polysomnogram
- PVOD:
-
Pulmonary veno-occlusive disease
- PVR:
-
Pulmonary vascular resistance
- Q p :
-
Pulmonary blood flow
- Q s :
-
Systemic blood flow
- RA:
-
Right atrium
- RAP:
-
Right atrial pressure
- RHC:
-
Right heart catheterization
- RNP:
-
Ribonucleoprotein
- ROC:
-
Receiver operating characteristic
- RV:
-
Right ventricle
- RVOT:
-
Right ventricular outflow tract
- RVSP:
-
Right ventricular systolic pressure
- SLE:
-
Systemic lupus erythematosus
- SVR:
-
Systemic vascular resistance
- TAPSE:
-
Tricuspid annular plane systolic excursion
- TGG-β:
-
Transforming growth factor beta
- TR:
-
Tricuspid regurgitation
- TRvel :
-
Velocity of the tricuspid regurgitation jet
- V/Q:
-
Ventilation/perfusion
- VSD:
-
Ventricular septal defect
- WHO:
-
World Health Organization
References
Lam CS, Borlaug BA, Kane GC, et al. Age-associated increases in pulmonary artery systolic pressure in the general population. Circulation. 2009;119:2663–70.
Leung CC, Moondra V, Catherwood E, et al. Prevalence and risk factors of pulmonary hypertension in patients with elevated pulmonary venous pressure and preserved ejection fraction. Am J Cardiol. 2010;106:284–6.
Bursi F, McNallan SM, Redfield MM, et al. Pulmonary pressures and death in heart failure: a community study. J Am Coll Cardiol. 2012;59:222–31.
Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2013;62:D34–41.
Brown LM, Chen H, Halpern S, et al. Delay in recognition of pulmonary arterial hypertension: factors identified from the REVEAL Registry. Chest. 2011;140:19–26.
McLaughlin VV, Archer SL, Badesch DB, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American College of Cardiology Foundation Task Force on Expert Consensus Documents and the American Heart Association developed in collaboration with the American College of Chest Physicians; American Thoracic Society, Inc.; and the Pulmonary Hypertension Association. J Am Coll Cardiol. 2009;53:1573–619.
Galie N, Hoeper MM, Humbert M, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Respir J. 2009;34:1219–63.
McGoon M, Gutterman D, Steen V, et al. Screening, early detection, and diagnosis of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126:14S–34.
McLaughlin VV, Langer A, Tan M, et al. Contemporary trends in the diagnosis and management of pulmonary arterial hypertension: an initiative to close the care gap. Chest. 2013;143:324–32.
Thenappan T, Shah SJ, Rich S, et al. A USA-based registry for pulmonary arterial hypertension: 1982–2006. Eur Respir J. 2007;30:1103–10.
Humbert M, Sitbon O, Chaouat A, et al. Pulmonary arterial hypertension in France: results from a national registry. Am J Respir Crit Care Med. 2006;173:1023–30.
Badesch DB, Raskob GE, Elliott CG, et al. Pulmonary arterial hypertension: baseline characteristics from the REVEAL Registry. Chest. 2010;137:376–87.
Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hypertension: a national prospective study. Ann Intern Med. 1987;107:216–23.
Hoeper MM, Bogaard HJ, Condliffe R, et al. Definitions and diagnosis of pulmonary hypertension. J Am Coll Cardiol. 2013;62:D42–50.
Brofman BL, Charms BL, Kohn PM, et al. Unilateral pulmonary artery occlusion in man; control studies. J Thorac Surg. 1957;34:206–27.
Harris P, Segel N, Bishop JM. The relation between pressure and flow in the pulmonary circulation in normal subjects and in patients with chronic bronchitis and mitral stenosis. Cardiovasc Res. 1968;2:73–83.
Brannon ES, Merrill AJ, Warren JV, et al. The cardiac output in patients with chronic anemia as measured by the technique of right atrial catheterization. J Clin Invest. 1945;24:332–6.
Robson SC, Hunter S, Boys RJ, et al. Serial study of factors influencing changes in cardiac output during human pregnancy. Am J Physiol. 1989;256:H1060–5.
Robson SC, Hunter S, Boys RJ, et al. Serial changes in pulmonary haemodynamics during human pregnancy: a non-invasive study using Doppler echocardiography. Clin Sci (Lond). 1991;80:113–7.
Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl J Med. 2001;344:501–9.
Chu JW, Kao PN, Faul JL, et al. High prevalence of autoimmune thyroid disease in pulmonary arterial hypertension. Chest. 2002;122:1668–73.
Li JH, Safford RE, Aduen JF, et al. Pulmonary hypertension and thyroid disease. Chest. 2007;132:793–7.
Badr B, Bories P, Marais R, et al. Transonic, thermodilution, or ionic dialysance to manage vascular access: which method is best? Hemodial Int. 2014;18:127–35.
Horvath KA, Burke RP, Collins Jr JJ, et al. Surgical treatment of adult atrial septal defect: early and long-term results. J Am Coll Cardiol. 1992;20:1156–9.
Engelfriet P, Meijboom F, Boersma E, et al. Repaired and open atrial septal defects type II in adulthood: an epidemiological study of a large European cohort. Int J Cardiol. 2008;126:379–85.
Kowalski HJ, Abelmann WH. The cardiac output at rest in Laennec’s cirrhosis. J Clin Invest. 1953;32:1025–33.
Castro M, Krowka MJ, Schroeder DR, et al. Frequency and clinical implications of increased pulmonary artery pressures in liver transplantation. Mayo Clin Proc. 1996;71:543–51.
Krowka MJ, Swanson KL, Frantz RP, et al. Portopulmonary hypertension: results from a 10-year screening algorithm. Hepatology. 2006;44:1502–10.
Fritz JS, Fallon MB, Kawut SM. Pulmonary vascular complications of liver disease. Am J Respir Crit Care Med. 2013;187:133–43.
Colle IO, Moreau R, Godinho E, et al. Diagnosis of portopulmonary hypertension in candidates for liver transplantation: a prospective study. Hepatology. 2003;37:401–9.
Hadengue A, Benhayoun MK, Lebrec D, et al. Pulmonary hypertension complicating portal hypertension: prevalence and relation to splanchnic hemodynamics. Gastroenterology. 1991;100:520–8.
Edwards BS, Weir EK, Edwards WD, et al. Coexistent pulmonary and portal hypertension: morphologic and clinical features. J Am Coll Cardiol. 1987;10:1233–8.
Swanson KL, Wiesner RH, Nyberg SL, et al. Survival in portopulmonary hypertension: Mayo Clinic experience categorized by treatment subgroups. Am J Transplant. 2008;8:2445–53.
Kawut SM, Taichman DB, Ahya VN, et al. Hemodynamics and survival of patients with portopulmonary hypertension. Liver Transpl. 2005;11:1107–11.
Krowka MJ, Mandell MS, Ramsay MA, et al. Hepatopulmonary syndrome and portopulmonary hypertension: a report of the multicenter liver transplant database. Liver Transpl. 2004;10:174–82.
Krowka MJ, Plevak DJ, Findlay JY, et al. Pulmonary hemodynamics and perioperative cardiopulmonary-related mortality in patients with portopulmonary hypertension undergoing liver transplantation. Liver Transpl. 2000;6:443–50.
Murray KF, Carithers Jr RL. AASLD practice guidelines: evaluation of the patient for liver transplantation. Hepatology. 2005;41:1407–32.
Kitzman DW, Gardin JM, Gottdiener JS, et al. Importance of heart failure with preserved systolic function in patients > or = 65 years of age. Am J Cardiol. 2001;87:413–9.
Klapholz M, Maurer M, Lowe AM, et al. Hospitalization for heart failure in the presence of a normal left ventricular ejection fraction: results of the New York Heart Failure Registry. J Am Coll Cardiol. 2004;43:1432–8.
Lee DS, Gona P, Vasan RS, et al. Relation of disease pathogenesis and risk factors to heart failure with preserved or reduced ejection fraction: insights from the Framingham Heart Study of the National Heart, Lung, and Blood Institute. Circulation. 2009;119:3070–7.
Anjan VY, Loftus TM, Burke MA, et al. Prevalence, clinical phenotype, and outcomes associated with normal B-type natriuretic peptide levels in heart failure with preserved ejection fraction. Am J Cardiol. 2012;110:870–6.
Lam CS, Roger VL, Rodeheffer RJ, et al. Pulmonary hypertension in heart failure with preserved ejection fraction: a community-based study. J Am Coll Cardiol. 2009;53:1119–26.
Nunes H, Humbert M, Capron F, et al. Pulmonary hypertension associated with sarcoidosis: mechanisms, haemodynamics and prognosis. Thorax. 2006;61:68–74.
Palevsky HI, Cone L, Alavi A. A case of false-positive high probability ventilation-perfusion lung scan due to tuberculous mediastinal adenopathy with a discussion of other causes of false-positive high probability ventilation-perfusion lung scans. J Nucl Med. 1991;32:512–7.
Berry DF, Buccigrossi D, Peabody J, et al. Pulmonary vascular occlusion and fibrosing mediastinitis. Chest. 1986;89:296–301.
Robbins IM, Colvin EV, Doyle TP, et al. Pulmonary vein stenosis after catheter ablation of atrial fibrillation. Circulation. 1998;98:1769–75.
Saad EB, Marrouche NF, Saad CP, et al. Pulmonary vein stenosis after catheter ablation of atrial fibrillation: emergence of a new clinical syndrome. Ann Intern Med. 2003;138:634–8.
Mandel J, Mark EJ, Hales CA. Pulmonary veno-occlusive disease. Am J Respir Crit Care Med. 2000;162:1964–73.
Montani D, Price LC, Dorfmuller P, et al. Pulmonary veno-occlusive disease. Eur Respir J. 2009;33:189–200.
Palmer SM, Robinson LJ, Wang A, et al. Massive pulmonary edema and death after prostacyclin infusion in a patient with pulmonary veno-occlusive disease. Chest. 1998;113:237–40.
Pietra GG, Capron F, Stewart S, et al. Pathologic assessment of vasculopathies in pulmonary hypertension. J Am Coll Cardiol. 2004;43:25S–32.
Fishman AP. Hypoxia on the pulmonary circulation: how and where it acts. Circ Res. 1976;38:221–31.
Stenmark KR, Fagan KA, Frid MG. Hypoxia-induced pulmonary vascular remodeling: cellular and molecular mechanisms. Circ Res. 2006;99:675–91.
Harris P, Segel N, Green I, et al. The influence of the airways resistance and alveolar pressure on the pulmonary vascular resistance in chronic bronchitis. Cardiovasc Res. 1968;2:84–92.
Heath D, Gillund TD, Kay JM, et al. Pulmonary vascular disease in honeycomb lung. J Pathol Bacteriol. 1968;95:423–30.
Ebina M, Shimizukawa M, Shibata N, et al. Heterogeneous increase in CD34-positive alveolar capillaries in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2004;169:1203–8.
Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350:2257–64.
Moser KM, Bloor CM. Pulmonary vascular lesions occurring in patients with chronic major vessel thromboembolic pulmonary hypertension. Chest. 1993;103:685–92.
Thistlethwaite PA, Kaneko K, Madani MM, et al. Technique and outcomes of pulmonary endarterectomy surgery. Ann Thorac Cardiovasc Surg. 2008;14:274–82.
Shure D, Gregoratos G, Moser KM. Fiberoptic angioscopy: role in the diagnosis of chronic pulmonary arterial obstruction. Ann Intern Med. 1985;103:844–50.
Rubin LJ. Diagnosis and management of pulmonary arterial hypertension: ACCP evidence-based clinical practice guidelines. Chest. 2004;126:7S–10.
van Wolferen SA, Marcus JT, Westerhof N, et al. Right coronary artery flow impairment in patients with pulmonary hypertension. Eur Heart J. 2008;29:120–7.
Kawut SM, Silvestry FE, Ferrari VA, et al. Extrinsic compression of the left main coronary artery by the pulmonary artery in patients with long-standing pulmonary hypertension. Am J Cardiol. 1999;83:984–6. A910.
Louie EK, Rich S, Brundage BH. Doppler echocardiographic assessment of impaired left ventricular filling in patients with right ventricular pressure overload due to primary pulmonary hypertension. J Am Coll Cardiol. 1986;8:1298–306.
Kasner M, Westermann D, Steendijk P, et al. Left ventricular dysfunction induced by nonsevere idiopathic pulmonary arterial hypertension: a pressure-volume relationship study. Am J Respir Crit Care Med. 2012;186:181–9.
Stojnic BB, Brecker SJ, Xiao HB, et al. Left ventricular filling characteristics in pulmonary hypertension: a new mode of ventricular interaction. Br Heart J. 1992;68:16–20.
Gan CT, Lankhaar JW, Marcus JT, et al. Impaired left ventricular filling due to right-to-left ventricular interaction in patients with pulmonary arterial hypertension. Am J Physiol Heart Circ Physiol. 2006;290:H1528–33.
Tonelli AR, Plana JC, Heresi GA, et al. Prevalence and prognostic value of left ventricular diastolic dysfunction in idiopathic and heritable pulmonary arterial hypertension. Chest. 2012;141:1457–65.
Thenappan T, Shah SJ, Gomberg-Maitland M, et al. Clinical characteristics of pulmonary hypertension in patients with heart failure and preserved ejection fraction. Circ Heart Fail. 2011;4:257–65.
Pugh ME, Sivarajan L, Wang L, et al. Causes of pulmonary hypertension in the elderly. Chest. 2014;146:159–66.
Chung L, Liu J, Parsons L, et al. Characterization of connective tissue disease-associated pulmonary arterial hypertension from REVEAL: identifying systemic sclerosis as a unique phenotype. Chest. 2010;138:1383–94.
Launay D, Hachulla E, Hatron PY, et al. Pulmonary arterial hypertension, a rare complication of primary Sjogren syndrome: report of 9 new cases and review of the literature. Medicine (Baltimore). 2007;86:299–315.
Poormoghim H, Lucas M, Fertig N, et al. Systemic sclerosis sine scleroderma: demographic, clinical, and serologic features and survival in forty-eight patients. Arthritis Rheum. 2000;43:444–51.
Toya SP, Tzelepis GE. The many faces of scleroderma sine scleroderma: a literature review focusing on cardiopulmonary complications. Rheumatol Int. 2009;29:861–8.
Simonneau G, Azarian R, Brenot F, et al. Surgical management of unresolved pulmonary embolism: a personal series of 72 patients. Chest. 1995;107:52S–5.
Bonderman D, Wilkens H, Wakounig S, et al. Risk factors for chronic thromboembolic pulmonary hypertension. Eur Respir J. 2009;33:325–31.
Pepke-Zaba J, Delcroix M, Lang I, et al. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation. 2011;124:1973–81.
Bonderman D, Skoro-Sajer N, Jakowitsch J, et al. Predictors of outcome in chronic thromboembolic pulmonary hypertension. Circulation. 2007;115:2153–8.
Chin KM, Channick RN, Rubin LJ. Is methamphetamine use associated with idiopathic pulmonary arterial hypertension? Chest. 2006;130:1657–63.
Mehta NJ, Khan IA, Mehta RN, et al. HIV-related pulmonary hypertension: analytic review of 131 cases. Chest. 2000;118:1133–41.
Deng Z, Morse JH, Slager SL, et al. Familial primary pulmonary hypertension (gene PPH1) is caused by mutations in the bone morphogenetic protein receptor-II gene. Am J Hum Genet. 2000;67:737–44.
Lane KB, Machado RD, Pauciulo MW, et al. Heterozygous germline mutations in BMPR2, encoding a TGF-beta receptor, cause familial primary pulmonary hypertension. Nat Genet. 2000;26:81–4.
Cogan JD, Pauciulo MW, Batchman AP, et al. High frequency of BMPR2 exonic deletions/duplications in familial pulmonary arterial hypertension. Am J Respir Crit Care Med. 2006;174:590–8.
Aldred MA, Vijayakrishnan J, James V, et al. BMPR2 gene rearrangements account for a significant proportion of mutations in familial and idiopathic pulmonary arterial hypertension. Hum Mutat. 2006;27:212–3.
Jones DK, Higenbottam TW, Wallwork J. Treatment of primary pulmonary hypertension intravenous epoprostenol (prostacyclin). Br Heart J. 1987;57:270–8.
Findlay JY, Plevak DJ, Krowka MJ, et al. Progressive splenomegaly after epoprostenol therapy in portopulmonary hypertension. Liver Transpl Surg. 1999;5:362–5.
Touma W, Nayak RP, Hussain Z, et al. Epoprostenol-induced hypersplenism in portopulmonary hypertension. Am J Med Sci. 2012;344:345–9.
McQuillan BM, Picard MH, Leavitt M, et al. Clinical correlates and reference intervals for pulmonary artery systolic pressure among echocardiographically normal subjects. Circulation. 2001;104:2797–802.
Currie PJ, Seward JB, Chan KL, et al. Continuous wave Doppler determination of right ventricular pressure: a simultaneous Doppler-catheterization study in 127 patients. J Am Coll Cardiol. 1985;6:750–6.
Chan KL, Currie PJ, Seward JB, et al. Comparison of three Doppler ultrasound methods in the prediction of pulmonary artery pressure. J Am Coll Cardiol. 1987;9:549–54.
Fisher MR, Forfia PR, Chamera E, et al. Accuracy of Doppler echocardiography in the hemodynamic assessment of pulmonary hypertension. Am J Respir Crit Care Med. 2009;179:615–21.
Rich JD, Shah SJ, Swamy RS, et al. Inaccuracy of Doppler echocardiographic estimates of pulmonary artery pressures in patients with pulmonary hypertension: implications for clinical practice. Chest. 2011;139:988–93.
Kitabatake A, Inoue M, Asao M, et al. Noninvasive evaluation of pulmonary hypertension by a pulsed Doppler technique. Circulation. 1983;68:302–9.
Chemla D, Castelain V, Provencher S, et al. Evaluation of various empirical formulas for estimating mean pulmonary artery pressure by using systolic pulmonary artery pressure in adults. Chest. 2009;135:760–8.
Chemla D, Castelain V, Humbert M, et al. New formula for predicting mean pulmonary artery pressure using systolic pulmonary artery pressure. Chest. 2004;126:1313–7.
Roberts JD, Forfia PR. Diagnosis and assessment of pulmonary vascular disease by Doppler echocardiography. Pulm Circ. 2011;1:160–81.
Arkles JS, Opotowsky AR, Ojeda J, et al. Shape of the right ventricular Doppler envelope predicts hemodynamics and right heart function in pulmonary hypertension. Am J Respir Crit Care Med. 2011;183:268–76.
Forfia PR, Fisher MR, Mathai SC, et al. Tricuspid annular displacement predicts survival in pulmonary hypertension. Am J Respir Crit Care Med. 2006;174:1034–41.
Rajagopalan N, Saxena N, Simon MA, et al. Correlation of tricuspid annular velocities with invasive hemodynamics in pulmonary hypertension. Congest Heart Fail. 2007;13:200–4.
Ghio S, Klersy C, Magrini G, et al. Prognostic relevance of the echocardiographic assessment of right ventricular function in patients with idiopathic pulmonary arterial hypertension. Int J Cardiol. 2010;140:272–8.
Opotowsky AR, Ojeda J, Rogers F, et al. A simple echocardiographic prediction rule for hemodynamics in pulmonary hypertension. Circ Cardiovasc Imaging. 2012;5:765–75.
Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 2010;122:164–72.
Raymond RJ, Hinderliter AL, Willis PW, et al. Echocardiographic predictors of adverse outcomes in primary pulmonary hypertension. J Am Coll Cardiol. 2002;39:1214–9.
Hinderliter AL, Willis PW, Long W, et al. Frequency and prognostic significance of pericardial effusion in primary pulmonary hypertension. Am J Cardiol. 1999;84:481–4. A410.
Eysmann SB, Palevsky HI, Reichek N, et al. Two-dimensional and Doppler-echocardiographic and cardiac catheterization correlates of survival in primary pulmonary hypertension. Circulation. 1989;80:353–60.
Gorcsan III J, Edwards TD, Ziady GM, et al. Transesophageal echocardiography to evaluate patients with severe pulmonary hypertension for lung transplantation. Ann Thorac Surg. 1995;59:717–22.
Diethelm L, Dery R, Lipton MJ, et al. Atrial-level shunts: sensitivity and specificity of MR in diagnosis. Radiology. 1987;162:181–6.
Burgess MI, Jenkins C, Sharman JE, et al. Diastolic stress echocardiography: hemodynamic validation and clinical significance of estimation of ventricular filling pressure with exercise. J Am Coll Cardiol. 2006;47:1891–900.
Marcus JT, Vonk Noordegraaf A, Roeleveld RJ, et al. Impaired left ventricular filling due to right ventricular pressure overload in primary pulmonary hypertension: noninvasive monitoring using MRI. Chest. 2001;119:1761–5.
Loyd JE, Primm RK, Newman JH. Familial primary pulmonary hypertension: clinical patterns. Am Rev Respir Dis. 1984;129:194–7.
Loyd JE, Butler MG, Foroud TM, et al. Genetic anticipation and abnormal gender ratio at birth in familial primary pulmonary hypertension. Am J Respir Crit Care Med. 1995;152:93–7.
Hachulla E, Gressin V, Guillevin L, et al. Early detection of pulmonary arterial hypertension in systemic sclerosis: a French nationwide prospective multicenter study. Arthritis Rheum. 2005;52:3792–800.
Coghlan JG, Denton CP, Grunig E, et al. Evidence-based detection of pulmonary arterial hypertension in systemic sclerosis: the DETECT study. Ann Rheum Dis. 2014;73:1340–9.
Algeo S, Morrison D, Ovitt T, et al. Noninvasive detection of pulmonary hypertension. Clin Cardiol. 1984;7:148–56.
Chitwood Jr WR, Sabiston Jr DC, Wechsler AS. Surgical treatment of chronic unresolved pulmonary embolism. Clin Chest Med. 1984;5:507–36.
Woodruff III WW, Hoeck BE, Chitwood Jr WR, et al. Radiographic findings in pulmonary hypertension from unresolved embolism. AJR Am J Roentgenol. 1985;144:681–6.
Satoh T, Kyotani S, Okano Y, et al. Descriptive patterns of severe chronic pulmonary hypertension by chest radiography. Respir Med. 2005;99:329–36.
Timpanelli AE, Steinberg I. Calcification of the pulmonary artery in patent ductus arteriosus with reversal of blood flow: report of four cases. Am J Med. 1961;30:405–17.
Ahearn GS, Tapson VF, Rebeiz A, et al. Electrocardiography to define clinical status in primary pulmonary hypertension and pulmonary arterial hypertension secondary to collagen vascular disease. Chest. 2002;122:524–7.
Sun PY, Jiang X, Gomberg-Maitland M, et al. Prolonged QRS duration: a new predictor of adverse outcome in idiopathic pulmonary arterial hypertension. Chest. 2012;141:374–80.
Sun XG, Hansen JE, Oudiz RJ, et al. Pulmonary function in primary pulmonary hypertension. J Am Coll Cardiol. 2003;41:1028–35.
Schindler MB, Bohn DJ, Bryan AC, et al. Increased respiratory system resistance and bronchial smooth muscle hypertrophy in children with acute postoperative pulmonary hypertension. Am J Respir Crit Care Med. 1995;152:1347–52.
Meyer FJ, Lossnitzer D, Kristen AV, et al. Respiratory muscle dysfunction in idiopathic pulmonary arterial hypertension. Eur Respir J. 2005;25:125–30.
de Man FS, van Hees HW, Handoko ML, et al. Diaphragm muscle fiber weakness in pulmonary hypertension. Am J Respir Crit Care Med. 2011;183:1411–8.
Fernandez-Bonetti P, Lupi-Herrera E, Martinez-Guerra ML, et al. Peripheral airways obstruction in idiopathic pulmonary artery hypertension (primary). Chest. 1983;83:732–8.
Meyer FJ, Ewert R, Hoeper MM, et al. Peripheral airway obstruction in primary pulmonary hypertension. Thorax. 2002;57:473–6.
Chaouat A, Bugnet AS, Kadaoui N, et al. Severe pulmonary hypertension and chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;172:189–94.
Thabut G, Dauriat G, Stern JB, et al. Pulmonary hemodynamics in advanced COPD candidates for lung volume reduction surgery or lung transplantation. Chest. 2005;127:1531–6.
Scharf SM, Iqbal M, Keller C, et al. Hemodynamic characterization of patients with severe emphysema. Am J Respir Crit Care Med. 2002;166:314–22.
Lettieri CJ, Nathan SD, Barnett SD, et al. Prevalence and outcomes of pulmonary arterial hypertension in advanced idiopathic pulmonary fibrosis. Chest. 2006;129:746–52.
Hurdman J, Condliffe R, Elliot CA, et al. Pulmonary hypertension in COPD: results from the ASPIRE registry. Eur Respir J. 2013;41:1292–301.
Patel NM, Lederer DJ, Borczuk AC, et al. Pulmonary hypertension in idiopathic pulmonary fibrosis. Chest. 2007;132:998–1006.
Lederer DJ, Arcasoy SM, Wilt JS, et al. Six-minute-walk distance predicts waiting list survival in idiopathic pulmonary fibrosis. Am J Respir Crit Care Med. 2006;174:659–64.
Mejia M, Carrillo G, Rojas-Serrano J, et al. Idiopathic pulmonary fibrosis and emphysema: decreased survival associated with severe pulmonary arterial hypertension. Chest. 2009;136:10–5.
Cottin V, Le Pavec J, Prevot G, et al. Pulmonary hypertension in patients with combined pulmonary fibrosis and emphysema syndrome. Eur Respir J. 2010;35:105–11.
Steen V, Medsger Jr TA. Predictors of isolated pulmonary hypertension in patients with systemic sclerosis and limited cutaneous involvement. Arthritis Rheum. 2003;48:516–22.
Hsu VM, Moreyra AE, Wilson AC, et al. Assessment of pulmonary arterial hypertension in patients with systemic sclerosis: comparison of noninvasive tests with results of right-heart catheterization. J Rheumatol. 2008;35:458–65.
Fischer A, Bull TM, Steen VD. Practical approach to screening for scleroderma-associated pulmonary arterial hypertension. Arthritis Care Res (Hoboken). 2012;64:303–10.
Chiang ST. A nomogram for venous shunt (Qs/Qt) calculation. Thorax. 1968;23:563–5.
Powe JE, Palevsky HI, McCarthy KE, et al. Pulmonary arterial hypertension: value of perfusion scintigraphy. Radiology. 1987;164:727–30.
Fedullo P, Kerr KM, Kim NH, et al. Chronic thromboembolic pulmonary hypertension. Am J Respir Crit Care Med. 2011;183:1605–13.
Tunariu N, Gibbs SJ, Win Z, et al. Ventilation-perfusion scintigraphy is more sensitive than multidetector CTPA in detecting chronic thromboembolic pulmonary disease as a treatable cause of pulmonary hypertension. J Nucl Med. 2007;48:680–4.
Ryan KL, Fedullo PF, Davis GB, et al. Perfusion scan findings understate the severity of angiographic and hemodynamic compromise in chronic thromboembolic pulmonary hypertension. Chest. 1988;93:1180–5.
Bailey CL, Channick RN, Auger WR, et al. “High probability” perfusion lung scans in pulmonary venoocclusive disease. Am J Respir Crit Care Med. 2000;162:1974–8.
Seferian A, Helal B, Jais X, et al. Ventilation/perfusion lung scan in pulmonary veno-occlusive disease. Eur Respir J. 2012;40:75–83.
Sostman HD, Brown M, Toole A, et al. Perfusion scan in pulmonary vascular/lymphangitic carcinomatosis: the segmental contour pattern. AJR Am J Roentgenol. 1981;137:1072–4.
Roberts KE, Hamele-Bena D, Saqi A, et al. Pulmonary tumor embolism: a review of the literature. Am J Med. 2003;115:228–32.
Genovesi MG, Tierney DF, Taplin GV, et al. An intravenous radionuclide method to evaluate hypoxemia caused by abnormal alveolar vessels: limitation of conventional techniques. Am Rev Respir Dis. 1976;114:59–65.
Kuriyama K, Gamsu G, Stern RG, et al. CT-determined pulmonary artery diameters in predicting pulmonary hypertension. Invest Radiol. 1984;19:16–22.
Ng CS, Wells AU, Padley SP. A CT sign of chronic pulmonary arterial hypertension: the ratio of main pulmonary artery to aortic diameter. J Thorac Imaging. 1999;14:270–8.
Oliver TB, Reid JH, Murchison JT. Interventricular septal shift due to massive pulmonary embolism shown by CT pulmonary angiography: an old sign revisited. Thorax. 1998;53:1092–4.
Reid JH, Murchison JT. Acute right ventricular dilatation: a new helical CT sign of massive pulmonary embolism. Clin Radiol. 1998;53:694–8.
Baque-Juston MC, Wells AU, Hansell DM. Pericardial thickening or effusion in patients with pulmonary artery hypertension: a CT study. AJR Am J Roentgenol. 1999;172:361–4.
Yeh BM, Kurzman P, Foster E, et al. Clinical relevance of retrograde inferior vena cava or hepatic vein opacification during contrast-enhanced CT. AJR Am J Roentgenol. 2004;183:1227–32.
Swensen SJ, Tashjian JH, Myers JL, et al. Pulmonary venoocclusive disease: CT findings in eight patients. AJR Am J Roentgenol. 1996;167:937–40.
Resten A, Maitre S, Humbert M, et al. Pulmonary hypertension: CT of the chest in pulmonary venoocclusive disease. AJR Am J Roentgenol. 2004;183:65–70.
Stein PD, Fowler SE, Goodman LR, et al. Multidetector computed tomography for acute pulmonary embolism. N Engl J Med. 2006;354:2317–27.
Schwickert HC, Schweden F, Schild HH, et al. Pulmonary arteries and lung parenchyma in chronic pulmonary embolism: preoperative and postoperative CT findings. Radiology. 1994;191:351–7.
Kauczor HU, Schwickert HC, Mayer E, et al. Spiral CT of bronchial arteries in chronic thromboembolism. J Comput Assist Tomogr. 1994;18:855–61.
Hasegawa I, Boiselle PM, Hatabu H. Bronchial artery dilatation on MDCT scans of patients with acute pulmonary embolism: comparison with chronic or recurrent pulmonary embolism. AJR Am J Roentgenol. 2004;182:67–72.
Sherrick AD, Swensen SJ, Hartman TE. Mosaic pattern of lung attenuation on CT scans: frequency among patients with pulmonary artery hypertension of different causes. AJR Am J Roentgenol. 1997;169:79–82.
Kerr KM, Auger WR, Fedullo PF, et al. Large vessel pulmonary arteritis mimicking chronic thromboembolic disease. Am J Respir Crit Care Med. 1995;152:367–73.
Lie JT. Isolated pulmonary Takayasu arteritis: clinicopathologic characteristics. Mod Pathol. 1996;9:469–74.
Park JH, Chung JW, Im JG, et al. Takayasu arteritis: evaluation of mural changes in the aorta and pulmonary artery with CT angiography. Radiology. 1995;196:89–93.
Marten K, Schnyder P, Schirg E, et al. Pattern-based differential diagnosis in pulmonary vasculitis using volumetric CT. AJR Am J Roentgenol. 2005;184:720–33.
Hamuryudan V, Yurdakul S, Moral F, et al. Pulmonary arterial aneurysms in Behcet’s syndrome: a report of 24 cases. Br J Rheumatol. 1994;33:48–51.
Rafanan AL, Golish JA, Dinner DS, et al. Nocturnal hypoxemia is common in primary pulmonary hypertension. Chest. 2001;120:894–9.
Miyamoto S, Nagaya N, Satoh T, et al. Clinical correlates and prognostic significance of six-minute walk test in patients with primary pulmonary hypertension: comparison with cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2000;161:487–92.
Humbert M, Sitbon O, Chaouat A, et al. Survival in patients with idiopathic, familial, and anorexigen-associated pulmonary arterial hypertension in the modern management era. Circulation. 2010;122:156–63.
Savarese G, Paolillo S, Costanzo P, et al. Do changes of 6-minute walk distance predict clinical events in patients with pulmonary arterial hypertension?: a meta-analysis of 22 randomized trials. J Am Coll Cardiol. 2012;60:1192–201.
Gabler NB, French B, Strom BL, et al. Validation of 6-minute walk distance as a surrogate end point in pulmonary arterial hypertension trials. Circulation. 2012;126:349–56.
Rich S. The 6-minute walk test as a primary endpoint in clinical trials for pulmonary hypertension. J Am Coll Cardiol. 2012;60:1202–3.
Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. 1996;334:296–301.
Sitbon O, Humbert M, Nunes H, et al. Long-term intravenous epoprostenol infusion in primary pulmonary hypertension: prognostic factors and survival. J Am Coll Cardiol. 2002;40:780–8.
Fritz JS, Blair C, Oudiz RJ, et al. Baseline and follow-up 6-min walk distance and brain natriuretic peptide predict 2-year mortality in pulmonary arterial hypertension. Chest. 2013;143:315–23.
Arena R, Lavie CJ, Milani RV, et al. Cardiopulmonary exercise testing in patients with pulmonary arterial hypertension: an evidence-based review. J Heart Lung Transplant. 2010;29:159–73.
Wensel R, Opitz CF, Anker SD, et al. Assessment of survival in patients with primary pulmonary hypertension: importance of cardiopulmonary exercise testing. Circulation. 2002;106:319–24.
Hoeper MM, Markevych I, Spiekerkoetter E, et al. Goal-oriented treatment and combination therapy for pulmonary arterial hypertension. Eur Respir J. 2005;26:858–63.
Sacks DG, Okano Y, Steen VD, et al. Isolated pulmonary hypertension in systemic sclerosis with diffuse cutaneous involvement: association with serum anti-U3RNP antibody. J Rheumatol. 1996;23:639–42.
Okano Y, Steen VD, Medsger Jr TA. Autoantibody to U3 nucleolar ribonucleoprotein (fibrillarin) in patients with systemic sclerosis. Arthritis Rheum. 1992;35:95–100.
Auger WR, Permpikul P, Moser KM. Lupus anticoagulant, heparin use, and thrombocytopenia in patients with chronic thromboembolic pulmonary hypertension: a preliminary report. Am J Med. 1995;99:392–6.
Wolf M, Boyer-Neumann C, Parent F, et al. Thrombotic risk factors in pulmonary hypertension. Eur Respir J. 2000;15:395–9.
Nagaya N, Nishikimi T, Uematsu M, et al. Plasma brain natriuretic peptide as a prognostic indicator in patients with primary pulmonary hypertension. Circulation. 2000;102:865–70.
Fijalkowska A, Kurzyna M, Torbicki A, et al. Serum N-terminal brain natriuretic peptide as a prognostic parameter in patients with pulmonary hypertension. Chest. 2006;129:1313–21.
Mehra MR, Uber PA, Park MH, et al. Obesity and suppressed B-type natriuretic peptide levels in heart failure. J Am Coll Cardiol. 2004;43:1590–5.
Wang TJ, Larson MG, Levy D, et al. Impact of obesity on plasma natriuretic peptide levels. Circulation. 2004;109:594–600.
Bayes-Genis A, Lloyd-Jones DM, van Kimmenade RR, et al. Effect of body mass index on diagnostic and prognostic usefulness of amino-terminal pro-brain natriuretic peptide in patients with acute dyspnea. Arch Intern Med. 2007;167:400–7.
Batal O, Faulx M, Krasuski RA, et al. Effect of obesity on B-type natriuretic peptide levels in patients with pulmonary arterial hypertension. Am J Cardiol. 2012;110:909–14.
Ruiter G, Lankhorst S, Boonstra A, et al. Iron deficiency is common in idiopathic pulmonary arterial hypertension. Eur Respir J. 2011;37:1386–91.
Rhodes CJ, Howard LS, Busbridge M, et al. Iron deficiency and raised hepcidin in idiopathic pulmonary arterial hypertension: clinical prevalence, outcomes, and mechanistic insights. J Am Coll Cardiol. 2011;58:300–9.
Krasuski RA, Hart SA, Smith B, et al. Association of anemia and long-term survival in patients with pulmonary hypertension. Int J Cardiol. 2011;150:291–5.
Dunn GD, Hayes P, Breen KJ, et al. The liver in congestive heart failure: a review. Am J Med Sci. 1973;265:174–89.
Rubin LJ, Badesch DB, Barst RJ, et al. Bosentan therapy for pulmonary arterial hypertension. N Engl J Med. 2002;346:896–903.
Galie N, Olschewski H, Oudiz RJ, et al. Ambrisentan for the treatment of pulmonary arterial hypertension: results of the ambrisentan in pulmonary arterial hypertension, randomized, double-blind, placebo-controlled, multicenter, efficacy (ARIES) study 1 and 2. Circulation. 2008;117:3010–9.
Forfia PR, Mathai SC, Fisher MR, et al. Hyponatremia predicts right heart failure and poor survival in pulmonary arterial hypertension. Am J Respir Crit Care Med. 2008;177:1364–9.
Ryan JJ, Rich JD, Thiruvoipati T, et al. Current practice for determining pulmonary capillary wedge pressure predisposes to serious errors in the classification of patients with pulmonary hypertension. Am Heart J. 2012;163:589–94.
Halpern SD, Taichman DB. Misclassification of pulmonary hypertension due to reliance on pulmonary capillary wedge pressure rather than left ventricular end-diastolic pressure. Chest. 2009;136:37–43.
Mills SR, Jackson DC, Older RA, et al. The incidence, etiologies, and avoidance of complications of pulmonary angiography in a large series. Radiology. 1980;136:295–9.
Nicod P, Peterson K, Levine M, et al. Pulmonary angiography in severe chronic pulmonary hypertension. Ann Intern Med. 1987;107:565–8.
Kovacs G, Berghold A, Scheidl S, et al. Pulmonary arterial pressure during rest and exercise in healthy subjects: a systematic review. Eur Respir J. 2009;34:888–94.
Grunig E, Janssen B, Mereles D, et al. Abnormal pulmonary artery pressure response in asymptomatic carriers of primary pulmonary hypertension gene. Circulation. 2000;102:1145–50.
Grunig E, Weissmann S, Ehlken N, et al. Stress Doppler echocardiography in relatives of patients with idiopathic and familial pulmonary arterial hypertension: results of a multicenter European analysis of pulmonary artery pressure response to exercise and hypoxia. Circulation. 2009;119:1747–57.
Tolle JJ, Waxman AB, Van Horn TL, et al. Exercise-induced pulmonary arterial hypertension. Circulation. 2008;118:2183–9.
Steen V, Chou M, Shanmugam V, et al. Exercise-induced pulmonary arterial hypertension in patients with systemic sclerosis. Chest. 2008;134:146–51.
Kovacs G, Maier R, Aberer E, et al. Borderline pulmonary arterial pressure is associated with decreased exercise capacity in scleroderma. Am J Respir Crit Care Med. 2009;180:881–6.
Condliffe R, Kiely DG, Peacock AJ, et al. Connective tissue disease-associated pulmonary arterial hypertension in the modern treatment era. Am J Respir Crit Care Med. 2009;179:151–7.
Saggar R, Khanna D, Shapiro S, et al. Effect of ambrisentan treatment on exercise-induced pulmonary hypertension in systemic sclerosis: a prospective single-center, open-label pilot study. Arthritis Rheum. 2012;64:4072–7.
Borlaug BA, Nishimura RA, Sorajja P, et al. Exercise hemodynamics enhance diagnosis of early heart failure with preserved ejection fraction. Circ Heart Fail. 2010;3:588–95.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Fritz, J.S., Palevsky, H.I. (2015). Approach to the Patient with Elevated Pulmonary Arterial Pressure. In: Klinger, J., Frantz, R. (eds) Diagnosis and Management of Pulmonary Hypertension. Respiratory Medicine, vol 12. Humana Press, New York, NY. https://doi.org/10.1007/978-1-4939-2636-7_8
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2636-7_8
Publisher Name: Humana Press, New York, NY
Print ISBN: 978-1-4939-2635-0
Online ISBN: 978-1-4939-2636-7
eBook Packages: MedicineMedicine (R0)