
Abstract
Struma ovarii is a rare cause of hyperthyroidism. We report a case of a 52-year-old woman with the typical signs and symptoms of hyperthyroidism, in whom the diagnosis of struma ovarii was missed. We discuss the approaches leading to the correct diagnosis and we review the management of the disease.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others


Keywords
Objectives
Struma ovarii is a rare cause of hyperthyroidism. We report a case of a 52-year-old woman with the typical signs and symptoms of hyperthyroidism, in whom the diagnosis of struma ovarii was missed. We discuss the approaches leading to the correct diagnosis and we review the management of the disease.
Case Presentation
A 52-year-old secretary presented to our Center for evaluation of persistent hyperthyroidism despite having had a total thyroidectomy. Two years earlier she went to a new primary care physician and was noted to have slightly depressed TSH of 0.27 mU/l, but denied any specific symptoms of thyrotoxicosis. She was evaluated by an Endocrinologist and underwent a 24-h radioiodine uptake and scan which showed symmetric low uptake over the thyroid with 1 % uptake in 24 h (normal 10–35 %). She was initially treated with Methimazole which she did not tolerate due to gastrointestinal symptoms. She was switched to Propylthiouracil and reported similar side effects. She had a history of coronary artery disease with stent placements, and her medical regimen included beta blockers. Due to a history of sialadenitis, she did not pursue radioiodine treatment.
She underwent total thyroidectomy and final pathology showed chronic thyroiditis with focal nodular hyperplasia and focal Hurthle cell change. Postoperatively, she was placed on thyroxine 75 mcg daily. After 3 weeks, her serum TSH was <0.02 mU/l and a free T4 was 1.99 ng/dl. The dose of thyroxine was reduced to 50 mcg daily, but her serum TSH remained suppressed, and the patient reported symptoms of insomnia, nausea, diarrhea, and irritability. The thyroxine was subsequently discontinued. Four months after the total thyroidectomy, on no thyroid hormone replacement, laboratory testing showed a serum TSH of 0.02 mU/l (0.34–5.6), a Free T4 of 2.0 ng/dl (0.6–1.12), and a Total T3 of 237 ng/ml (60–181). A thyroid ultrasound showed no identifiable thyroid tissue and no lymphadenopathy.
The patient was then evaluated at our Center 5 months after surgery and reported that if she was late in taking her dose of beta blocker, she experienced palpitations, but denied any other symptoms of thyroid hormone excess. She denied any anterior neck symptoms and denied visual complaints. Her family history included a maternal aunt with Graves’ disease with eye involvement, treated with radioactive iodine. Medications included metoprolol, atorvastatin, fenofibrate, aspirin, and a multivitamin. Physical examination showed a blood pressure 141/69 mmHg, a pulse of 74 beats per minute and regular, height 67 in., weight 276 pounds, temperature 97.3 °F. Neck exam showed a midline thyroidectomy scar that was well healed with no palpable thyroid tissue and no cervical lymphadenopathy. Her laboratory evaluation showed a serum TSH of <0.02 mU/l, a Free T4 of 2.1 ng/dl (0.7–1.8), a Total T3 of 183 ng/dl, Thyroid Stimulating Immunoglobulin (TSI) 28 % (<140), Thyroglobulin 264 ng/ml (1.1–35). She was restarted on low divided dose methimazole 5 mg twice a day because of her prior gastrointestinal symptoms, and the beta blocker was continued.
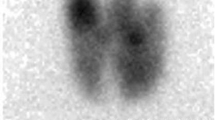
She underwent an I-123 Whole Body Scan with SPECT/CT imaging, which showed intense iodine uptake within the pelvis from an irregular lobulated mass in the region of the uterus, measuring approximately 12 × 10 × 10 cm. There was no evidence of radiotracer uptake in the region of the thyroid bed or along the expected course of an ectopic lingual or mediastinal thyroid (Fig. 7.1). She underwent a pelvic MRI, which showed heterogeneous mass measuring 11.0 × 10.6 × 8.8 cm, that was cystic and solid enhancing septations and fat, consistent with a teratoma broadly abutting the uterus and the rectum, with significant mass effect. The mass was thought to be of left ovarian origin as there was only visualization of the right ovary, and there was significant vascular supply and drainage from left ovarian vessels. There was also effacement of the fat plane between uterus and the mass, suspicious enhancing bone lesions in the left sacrum and L5, and prominent bilateral external iliac and right pelvic lymph nodes (Fig. 7.2).

Radioiodine I-123 imaging with whole body scan

MRI of pelvic mass
She was referred to the Gynecologic Oncology Clinic, and the methimazole dose was titrated until the free T4 and total T3 were within the normal range. Five months after her presentation, she underwent exploratory laparotomy, total abdominal hysterectomy, bilateral salpingo-oophorectomy, right and left pelvic node sampling. The surgical pathology showed a 13 cm struma ovarii (Figs. 7.3 and 7.4). The lesion was proliferative, with follicular crowding and nuclear atypia, which are indeterminate microscopic features, but insufficient to establish a diagnosis of carcinoma. Three lymph nodes were negative for tumor. Postoperatively, the patient was placed on thyroxine, which was titrated to a dose of 125 mcg × 7.5 tablets per week. Her laboratory tests showed an undetectable serum thyroglobulin level while on this replacement dose. Four months after surgery, she underwent Thyrogen-stimulated testing which showed a thyroglobulin of 0.9 ng/ml, and a whole body scan showed two foci of increased radiotracer localization within the thyroid bed, compatible with residual thyroid tissue. There was no evidence of uptake in the extrathyroidal neck or at distant sites, and no evidence of uptake within the pelvis outside the bladder.

Ovarian tumor containing thyroid tissue as the predominant cell type, which typically occurs as part of a teratoma

Thyroid follicle filled with colloid
Background
“Struma” is the Latin term for a “swelling in the neck,” and struma ovarii was first described in 1895 by Vol Kalden [1]. It is a rare ovarian tumor defined by the presence of thyroid tissue as a major cellular component, and most commonly occurs as part of a teratoma. In a pathologic study from two major academic centers, out of 1,390 ovarian tumors, 167 were teratomas [2]. Less than 1 % contained foci of thyroid tissue or were struma ovarii. Struma ovarii is most commonly diagnosed between the ages of 40 and 60 years [3]. Pathologically, the thyroid epithelium in the teratoma may be organized in a solid, embryonal or pseudotubular pattern, rather than forming thyroid follicles, and thyroglobulin staining may be required to identify the cells as thyroidal in origin [3].
The clinical presentation may include symptoms ranging from thyrotoxic complaints, a pelvic mass, or ascites [4]. If there is autonomous production of thyroid hormone by the struma ovarii, this would lead to TSH suppression and absence of function by the normal thyroid gland [2]. The diagnosis may be suspected in a woman with hyperthyroidism who has no goiter and minimal or absent thyroidal uptake of radioiodine. In such cases, the far more likely causes remain exogenous thyroid hormone use and various forms of thyroiditis. The diagnosis is made, as in our case, by radioiodine imaging of the pelvis. Rarely, women with struma ovarii and hyperthyroidism also have a goiter, which may be due the coexistence of Graves’ disease and struma ovarii, in which thyroid-stimulating immunoglobulins stimulate the thyroid tissue in the ovary as well as the neck, or the presence of toxic nodular goiter, in which there is also radioiodine uptake over the ovary and the neck [5].
An antithyroid drug, preferably methimazole, is given for 4–6 weeks prior to surgery, depending on the severity of the thyrotoxicosis and underlying risk factors (older age, underlying cardiovascular disease, etc.). As in this case, beta blocking drugs may also be used for symptomatic relief and for heart rate control. In cases of benign struma ovarii causing hyperthyroidism, after resection, the cervical thyroid gland that was previously suppressed may resume normal function [2].
Surgical removal is the treatment for struma ovarii, even in a patient with coexisting Graves’ disease or toxic nodular goiter, due to the risk of carcinoma. The pathologic criteria for carcinoma in struma ovarii include tumor invasion, metastases, or recurrence, or the typical cytopathologic features of papillary thyroid cancer. A pathologic study evaluated 54 patients with ovarian tumors due to struma ovarii and 13 (24 %) were found to be carcinomas, 11 with features of papillary carcinoma and 2 with features of follicular carcinoma [6]. Cancer is more likely in larger tumors and was present in 75 % of tumors >16 cm, and rarely in tumors <5 cm [6].
In cases of malignant struma ovarii, there is no standard treatment protocol. Generally, treatment includes oophorectomy and total thyroidectomy. Following surgery, a radioiodine scan is performed, after Thyrogen stimulation or thyroxine withdrawal, although there has been no consensus recommendation. If there is abnormal radioiodine uptake in the abdomen or possible metastases, high-dose radioiodine is administered [3, 7–9].
The follow-up involves monitoring for recurrence, including radioiodine whole body scan and at least 10 years of surveillance with serum thyroglobulin [3, 7–9]. An increase in serum thyroglobulin may prompt a repeat radioiodine scan [3]. Aside from recurrences of malignant struma ovarii in the abdomen, there have also been reports of recurrences at distant sites, including the bones, brain, and lung [8]. After surgical resection of the struma ovarii and total thyroidectomy, patients will require lifelong thyroxine replacement. The dose should be titrated to a goal TSH in the low normal to slightly suppressed range, although no specific cutoffs have been established [7].
The overall prognosis for benign struma is excellent. In malignant cases, surgery and I-131 treatment is often curative. The clinical behavior of thyroid-type lesions arising in struma ovarii cannot necessarily be predicted on the basis of microscopic features. Highly differentiated proliferations lacking fully developed features of carcinoma can recur. Smaller lesions qualifying for a diagnosis of carcinoma based on histologic criteria used for thyroid gland tumors can demonstrate clinically benign behavior and not recur [10]. If recurrences are detected, repeat radioiodine ablation may be indicated. In a pathologic study of 88 patients with malignant struma ovarii, the clinical factors associated with recurrence or extraovarian spread included adhesions, peritoneal fluid >1 l, ovarian tissue on membrane surfaces, papillary histology, or a struma component ≥12 cm [11]. The overall survival rate in this study was 89 % at 10 years, and 84 % at 25 years [11].
How the Diagnosis Was Made
This patient demonstrated clinical symptoms and laboratory evidence of persistent hyperthyroidism 4 months after total thyroidectomy, while she was off any known thyroxine supplementation. In this case, the elevated thyroglobulin level indicated that the hyperthyroidism was caused by an endogenous source, which was ectopic thyroid tissue. The radioiodine whole body scan revealed increased radiotracer localization in the pelvis. This was further evaluated by MRI, which characterized the pelvic mass. Surgical resection was indicated as there is a risk for malignancy, and the final pathology confirmed benign struma ovarii.
Lessons Learned
-
Struma Ovarii can present with the typical symptoms of hyperthyroidism, and a radioiodine whole body scan may help localize abnormal uptake in the body.
-
Prior to surgical treatment, hyperthyroidism from struma ovarii may be treated with antithyroid drugs and beta blockers.
-
Patients may undergo unilateral oophorectomy, or hysterectomy and bilateral salpingo-oopherectomy if there is concern about malignancy
-
If thyroid cancer is present, radioiodine treatment may be used after the thyroid has also been removed.
-
Monitoring includes serum thyroglobulin testing and radioiodine whole body scanning.
Questions
-
1.
What is the most likely reason for thyrotoxicosis in a patient without a goiter and low uptake on radioiodine imaging?
-
A.
Thyroiditis
-
B.
Thyroxine intake
-
C.
Ectopic thyroid tissue in neck
-
D.
Struma Ovarii
-
E.
A or B
-
A.
-
2.
After thyroidectomy, which laboratory test is the most useful in determining thyrotoxicosis from endogenous thyroid tissue versus exogenous thyroxine intake?
-
A.
Thyroglobulin
-
B.
TSH
-
C.
Free T4
-
D.
Thyroid-stimulating immunoglobulin (TSI)
-
A.
-
3.
Which imaging study would be most helpful in locating ectopic thyroid tissue?
-
A.
Radioiodine I-123 imaging with neck imaging
-
B.
Radioiodine I-123 imaging with whole body scan
-
C.
MRI
-
D.
Ultrasound
-
A.
Answers to Questions
-
1.
E: In cases of hyperthyroidism with low radioiodine uptake, the causes are far more likely to be thyroxine intake or various forms of thyroiditis.
-
2.
A: Thyroglobulin is made by thyroid tissue located in the neck or ectopic thyroid tissue. TSH (answer B) and Free T4 (answer C) are affected by thyroid function and thyroxine intake. Elevated TSI (answer D) may indicate Graves’ disease, but would not suggest ectopic thyroid tissue.
-
3.
B: The radioiodine imaging with whole body scan will help locate ectopic thyroid tissue in the body. Limiting the scan to the neck (answer A) may miss cases of struma ovarii in the pelvis. Further imaging with ultrasound (answer D) or MRI (answer C) may then be directed to the areas of increased radiotracer localization.
References
Yannopoulos D, Yannopoulos K, Ossowski R. Malignant struma ovarii. Pathol Annu. 1976;11:403–13.
Dunzendorfer T, deLas Morenas A, Kalir T, Levin RM. Struma ovarii and hyperthyroidism. Thyroid. 1999;9(5):499–502.
Makani S, Kim W, Gaba AR. Struma ovarii with a focus of papillary thyroid cancer: a case report and review of the literature. Gynecol Oncol. 2004;94(3):835–9.
Roth LM, Talerman A. The enigma of struma ovarii. Pathology. 2007;39(1):139–46.
Chiofalo MG, Misso C, Insabato L, Lastoria S, Pezzullo L. Hyperthyroidism due to coexistence of graves’ disease and struma ovarii. Endocr Pract. 2007;13(3):274–6.
Devaney K, Snyder R, Norris HJ, Tavassoli FA. Proliferative and histologically malignant struma ovarii: a clinicopathologic study of 54 cases. Int J Gynecol Pathol. 1993;12(4):333–43.
McGill JF, Sturgeon C, Angelos P. Metastatic struma ovarii treated with total thyroidectomy and radioiodine ablation. Endocr Pract. 2009;15(2):167–73.
Jean S, Tanyi JL, Montone K, McGrath C, Lage-Alvarez MM, Chu CS. Papillary thyroid cancer arising in struma ovarii. J Obstet Gynaecol. 2012;32(3):222–6.
DeSimone CP, Lele SM, Modesitt SC. Malignant struma ovarii: a case report and analysis of cases reported in the literature with focus on survival and I131 therapy. Gynecol Oncol. 2003;89(3):543–8.
Shaco-Levy R, Peng RY, Snyder MJ, et al. Malignant struma ovarii: a blinded study of 86 cases assessing which histologic features correlate with aggressive clinical behavior. Arch Pathol Lab Med. 2012;136(2):172–8.
Robboy SJ, Shaco-Levy R, Peng RY, et al. Malignant struma ovarii: an analysis of 88 cases, including 27 with extraovarian spread. Int J Gynecol Pathol. 2009;28(5):405–22.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Abraham, S., Cooper, D.S. (2015). Struma Ovarii. In: Davies, T. (eds) A Case-Based Guide to Clinical Endocrinology. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2059-4_7
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2059-4_7
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2058-7
Online ISBN: 978-1-4939-2059-4
eBook Packages: MedicineMedicine (R0)