
Abstract
-
To review the clinical presentation of granulomatous hypophysitis (GrH) masquerading as a pituitary macroadenoma.
-
To discuss the differential diagnosis of hypophysitis.
-
To understand treatment options for GrH at initial presentation and recommendations for long-term management.
Access provided by Autonomous University of Puebla. Download chapter PDF
Similar content being viewed by others

Keywords
These keywords were added by machine and not by the authors. This process is experimental and the keywords may be updated as the learning algorithm improves.
Objectives
-
To review the clinical presentation of granulomatous hypophysitis (GrH) masquerading as a pituitary macroadenoma.
-
To discuss the differential diagnosis of hypophysitis.
-
To understand treatment options for GrH at initial presentation and recommendations for long-term management.
Case Presentation
A 73-year-old Caucasian woman presented with a year-long history of hyponatremia of “unclear” origin. She had been diagnosed with syndrome of inappropriate antidiuretic hormone secretion (SIADH) based on sodium levels of 124–128 mmol/L on different occasions. She was treated initially with fluid restrictions for >10 months with no symptomatic improvement and persistence of chronic hyponatremia. Other etiologies for hyponatremia were not entertained at that time. Following an Emergency Department (ED) presentation, she was found to be adrenally insufficient and started on prednisone at a dose of 5 mg daily. As per her medical record, hypothyroidism was “ruled out” during that admission based on a normal thyroid stimulating hormone (TSH) level. Medical history was otherwise significant for ulcerative colitis, basal cell carcinoma, familial essential tremor, and mitral valve prolapse.
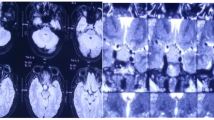
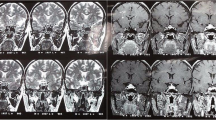
Several weeks later, the patient again presented to the ED with a severe throbbing headache. There were no aggravating or relieving factors and the headache was not associated with vomiting, fever, or any other neurologic symptoms. During evaluation by a neurologist, brain computerized tomography (CT) was performed. This revealed a sellar mass, which was better delineated in a follow-up magnetic resonance (MR) imaging, showing a 1.2 cm sellar mass abutting the optic chiasm (Fig. 4.1) and diagnosed as a pituitary adenoma. She was referred to the Oregon Health & Science University, Northwest Pituitary Center, for surgery and endocrine work-up.

T1-weighted coronal and sagittal MR images show diffusive enlargement and enhancement of the pituitary gland. The gland pyramidal in shape extending to hypophyseal stalk from the sellar base. Images also note the presence of enhanced mucosa in the bilateral sphenoid sinus and enhanced meninges around the sella. Images: preoperative (a), postoperative (b), 6 months post-high-dose GC treatment (c), 3-year follow-up off high-dose GC (d)
On review of symptoms she reported fatigue, nausea, which improved after starting steroids, brittle fingernails, edema in the legs, weakness in all extremities, memory deficits, sleep disturbances, and a history of chronic bronchitis with persistent shortness of breath.
Her family history was significant for heart disease in her mother, brother, aunt, uncles, and grandfather and tuberculosis in a great aunt.
In addition to treatment with prednisone daily at 5 mg (she was subsequently switched to hydrocortisone (HC) at a dose of 20 mg daily), medications included Azmacort, Nasonex, albuterol, a statin plus Zetia and niacin, Vivelle-Dot estrogen replacement, calcium, and multivitamins.
On physical exam she was normotensive, blood pressure was 136/69 mmHg, pulse 80, respirations 16, weight 156 lbs, and height 5ʹ8ʺ. Head, ears, eyes, nose, and throat (HEENT) exam revealed a temporal visual field (VF) deficit in the right eye and a formal VF exam indicated right temporal field restriction (Fig. 4.2). The remainder of her HEENT exam was unremarkable with extraocular movements and cranial nerves grossly intact. Pituitary function testing was performed including cortrosyn stimulation testing for adrenal insufficiency (AI); after holding HC for 24 h, AI was confirmed (Table 4.1). A diagnosis of central hypothyroidism with low free T4 and inappropriately low TSH was evident and treatment with levothyroxine was initiated. Growth hormone (GH) deficiency was suspected based on low insulin growth factor-1 (IGF-1); prolactin (PRL) was low. Based on a presumed diagnosis of nonfunctioning pituitary adenoma, the patient underwent transsphenoidal surgery (TSS) for optic chiasm decompression. In retrospect, a few MR imaging features were possibly suggestive of hypophysitis such as mild stalk thickening, sellar mass with cystic areas, and a vague ring enhancement; these are not very specific and her atypical clinical presentation in addition to VF loss warranted optic chiasmal decompression and at least a biopsy for final diagnosis. Classic features of MR imaging in hypophysitis include the presence of a “dural tail” (enhanced tissue along the dura mater), the absence of mucosal thickening in the sphenoid sinus, isointensity with gray matter on T1-weighted images, and marked homogeneous or heterogeneous enhancement by gadolinium (Table 4.2).

Visual field exam indicating right temporal field restriction
How Was the Diagnosis of Granulomatous Hypophysitis Made?
Pathology revealed necrotizing granulomas with giant cells and marked lymphoplasmacytic infiltration (Fig. 4.3). Rare acini of anterior pituitary parenchyma were also identified. Stains for microorganisms, bacilli, and fungi (Steiner, acid-fast bacilli, and Gomori methenamine silver) were negative and CD1a staining was also negative (Fig. 4.4). Reticulin staining revealed intact acinar structures, synaptophysin highlighted the native gland, and human GH was focally positive. Staining for PRL and adrenocorticotropic hormone (ACTH) was negative. There was no evidence of a tumor and no vasculitis was present in the specimen. In view of these findings, a diagnosis of granulomatous hypophysitis (GrH) with a component of lymphocytic hypophysitis (LH) was made.

Hematoxylin and eosin stained biopsy sections showing focal replacement of pituitary architecture by a lymphocytic infiltrate (400× magnification), and non-caseating epithelioid cell granulomas with multinucleated giant cells (800× magnification), and areas of fibrosis

Immunochistochemistry: synaptophysin (positive) is the most reliable and best broad spectrum marker for neuroendocrine cells and reticulin shows intact pituitary acinar structures. Sections were negative for acid-fast bacilli and CD1a
Hypophysitis is classified into primary and secondary forms and further classified by histological appearance (Fig. 4.5). Primary hypophysitis can be autoimmune, granulomatous, necrotizing, or xanthomatous. It can also be secondary to local lesions such as germinomas, craniopharyngiomas, Rathke’s Cleft cyst, and pituitary adenomas or secondary to systemic diseases. Recently, two other novel entities of hypophysitis have been described: drug-induced hypophysitis related to anti-CTLA-4 antibody therapy and hypophysitis due to IgG4-related disease. The incidence and prevalence of hypophysitis is unknown and population-based data are scarce.

Histological, demographic, MR imaging appearance, natural history, and endocrine dysfunction classification of hypophysitis
Granulomatous hypophysitis is a rare entity (approximately 40 cases have been reported) and presents commonly with an enlargement of the pituitary gland, mimicking an adenoma. M. Simmonds, in 1917, first described four cases after review of pituitaries from 2,000 autopsies. Pathogenesis is unknown and males and females are affected equally. Diagnosis is made postoperatively by histopathology. Adrenal insufficiency has rarely been reported in GrH. On imaging, the gland is seen to be diffusely enlarged with a thickened stalk seen infrequently and not easily distinguishable from a pituitary adenoma on clinical/imaging data.
Clinical presentation in most cases often includes features such as headache, with fewer cases presenting as hypopituitarism. In the case we report, the patient presented with hypopituitarism with AI and hypothyroidism that was misinterpreted as SIADH for almost a year. Although AI was clinically apparent, during this time she was most likely also hypothyroid, which may have inadvertently prevented an adrenal crisis while she was not receiving glucocorticoid (GC) replacement therapy. Visual field defects, ophthalmoplegia, nausea and/or vomiting, diabetes insipidus, hyperprolactinemia, asthenia, and fatigue are also common presentations. It is notable that in hypophysitis, PRL may be high secondary to stalk involvement or conversely low. Undetectable PRL is indicative of long-term or permanent panhypopituitarism.
Necrotizing hypophysitis, as in the case we present, is the least common variant: it is unknown if this is a separate disease entity or a variant of other types of hypophysitis. Histologically, diffuse necrosis is found surrounded by dense infiltration with lymphocytes, plasma cells, and a few eosinophils with considerable fibrosis.
Lymphocytic hypophysitis is considered the most common of all the hypophysitis and was first described in a deceased female 14 months postpartum. Autopsy showed a diffusely infiltrated anterior pituitary, Hashimoto’s thyroiditis, and atrophic adrenals. Only 18 % of cases have been reported in males with a large predominance (81 %) of cases being reported in women during late pregnancy or postpartum.
Clinically, LH, the most frequent type, and GrH are differentiated mainly by the temporal association of LH with peripartum. In LH, occasional spontaneous remission also occurs and an increased association with other autoimmune disease is described. However, LH and GrH can coexist and are possibly part of the same continuum with GrH ultimately progressing to LH.
Pituitary granulomas are rare specific lesions seen in sarcoidosis, tuberculosis, Langerhans histiocytosis (Histiocytosis-X), giant cell granulomatous hypophysitis, xanthomatous hypophysitis, and Wegener’s granulomatosis or rarely in LH. Histologically, GrH is characterized by necrotizing granulomas that are formed by collection of histiocytes, multinucleated giant cell, and variable numbers of lymphocytes and plasma cells. In the case we present, both granulomatous and lymphocytic inflammation were evidenced by well-defined epitheloid granulomas, lymphocytic infiltration, and histiocytes on histopathological examination.
Sarcoidosis is known to involve the central nervous system in about 10 % of cases. Sellar involvement can be complicated by aseptic meningitis and cranial nerve palsies. In our patient, there was no evidence of neurosarcoidosis and angiotensin-converting enzyme (ACE) level was normal.
No other evidence of autoimmune disorders was found besides ulcerative colitis: anti-neutrophil cytoplasmic antibodies, lupus, thyroid peroxidase, and thyroglobulin antibodies were all negative, erythrocyte sedimentation rate was normal, and a chest X-ray was unremarkable. Wegener granulomatosis was not compatible either with negative antibodies and there was no reported vasculitis. Thus, a diagnosis of an idiopathic or primary GrH was made.
Preoperative diagnosis of GrH is rare and requires histologic confirmation. A careful evaluation of the clinical, biochemical, and radiological characteristics is imperative for accurate diagnosis and proper management to ensure optimal outcome. Acute presentations of pituitary-based pathology can include previously unrecognized but enlarging tumors, apoplectic hemorrhage and necrosis, and LH. GrH can have an insidious clinical presentation with the risk of unrecognized AI leading to misdiagnosis and possible catastrophic outcome.
This case illustrates that hypophysitis should not be ignored in the differential diagnosis when a pituitary mass presents with double vision associated with single oculomotorius or abducens nerve neuropathy, hypopituitarism with hyperprolactinemia, hypoprolactinemia, and/or meningitis-like symptoms.
When Is Additional Treatment Postoperatively for GrH Needed?
Postoperatively, the patient reported resolution of right VF deficit and no symptoms or clinical evidence of DI or SIADH. Although DI is a frequent presentation in most cases of hypophysitis, the absence of DI does not exclude this diagnosis. Postoperative MR imaging showed optic chiasm decompression (Fig. 4.1). Formal VF was normal. She did have persistent AI and GCs were continued at replacement doses during a postoperative work-up for an etiology of GrH such as sarcoidosis and tuberculosis. However, she presented to the ED 4 weeks postoperatively with report of an acute deterioration and superior VF cuts with “graying vision” in her right eye, fatigue, and weakness. Imaging at the time indicated no change, but ophthalmologic exam indicated afferent pupillary defect and loss of color vision in the right eye but no VF deficit. She was treated with a prednisone burst of 60 mg daily tapering slowly over the following 2 months and maintained on prednisone 10 mg daily thereafter for a further 6 months. In the interim, she was also treated with Fosamax for osteoporosis prevention. After tapering to physiologic doses of GC, her VF remained normal, MR imaging remained unchanged, and her subjective visual symptoms improved.
Recurrences Are Not Uncommon
After 24 months, she again experienced VF changes with acute diplopia, sixth nerve palsy, and new inferotemporal defect in the left eye on formal ophthalmolgic VF testing. The VF deficit resolved again with a second burst of high-dose prednisone for 6 months. MR imaging showed significant improvement after treatment, which persisted for 3 years (Fig. 4.1).
Recurrence has been documented in several cases of hypophysitis requiring further treatment. GrH has been unresponsive or only partially responsive to high-dose steroids in some cases. Conversely, visual changes resolved and mass size on MR images decreased in response to steroids at each event in our patient. Therefore, we consider a trial of high-dose steroids efficacious for the treatment of GrH. It is expected that panhypopituitarism would not resolve with this approach.
Treatment
The natural history of inflammatory hypophysitis, including GrH, remains elusive and treatment is controversial. High-dose steroid therapy or anti-inflammatory and immunosuppressive (methotrexate, cyclosporine A, azathioprine) treatments have been reported with variable outcomes both as preoperative medical management and postoperative therapy.
Conservative management using clinical observation has also been advocated as the primary therapeutic option in hypophysitis variants other than GrH. Spontaneous remission has not been reported in cases of GrH. Transsphenoidal surgery is, however, both diagnostic and therapeutic and, therefore, should be performed in cases with progressive optic chiasmal compression, and when a definitive diagnosis is required for atypical presentation.
In this case, the patient required surgery to decompress the optic chiasm and surgical pathology elucidated the definitive diagnosis. Two separate prolonged courses of high-dose GC were fortunately successful in restoration of normal vision.
In conclusion, the diagnosis and treatment of hypophysitis for successful outcomes remains challenging, but is possible. Sophisticated imaging and histologic evaluation is required as well as skilled surgical excision. Symptomatic and ophthalmologic relief can be achieved with high-dose steroids, as in this patient, but is not successful in all cases. Close long-term follow-up and the timely initiation of appropriate treatment (repeat high-dose steroids, repeat surgery for optic chiasm decompression, and possibly radiation therapy) are required.
Lessons Learned
-
In the presence of hyponatremia, AI and hypothyroidism have to be ruled out before a diagnosis of SIADH is made. A normal TSH does not rule out central hypothyroidism.
-
Not all sellar masses are pituitary adenomas. Despite the accuracy of current diagnostic tools, non-adenomatous lesions of the pituitary represent a challenge for the practicing physician.
-
There are multiple forms of hypophysitis with variable anatomical and clinical presentations and precise diagnosis is challenging without biopsy, although this is not indicated in all cases. The incidence and prevalence of hypophysitis is unknown and population-based data are scarce.
-
A pituitary lesion in a woman around the time of pregnancy, a rapidly progressive pituitary lesion, pituitary function that is discordant with the size of the lesion, and the presence of AI in the absence of other pituitary deficits are suggestive of a diagnosis of LH. Granulomatous hypophysitis is rarer, but should be considered in the differential diagnosis of a pituitary adenoma.
-
New entities of hypophysitis (IgG-4 hypophysitis and drug-induced hypophysitis) have been discovered in relation to novel drug therapies and autoimmune diseases.
-
Treatment goals include mass reduction, preservation of pituitary function, and replacement of pituitary deficits. High-dose GCs were effective in this case to reduce mass size and improve visual disturbances, but may need to be repeated. Fortunately, disease relapse was also responsive to GC therapy, but sometimes a multi-modal adjuvant treatment is needed.
-
Long-term follow-up is mandatory to monitor for the development of other pituitary deficits and/or disease relapse.
Questions
-
1.
A 24-year-old female presents with new onset diabetes insipidus and was started on DDAVP. On further evaluation, she also has been found to have adrenal insufficiency. Pituitary function is otherwise normal. MRI shows significant stalk thickening. She has no significant past medical history and she delivered a healthy baby 3 months ago. Which is the most likely diagnosis in this young woman:
-
(A)
Lymphocytic hypophysitis
-
(B)
Pituitary adenoma
-
(C)
Granulomatous hypophysitis
-
(D)
Sarcoidosis
-
(A)
-
2.
Pituitary lesions’ characteristics on a dynamic MRI with gadolinium can establish with certitude a diagnosis of hypophysitis.
-
(A)
True
-
(B)
False
-
(A)
-
3.
Which is the most common anterior pituitary dysfunction associated with hypophysitis?
-
(A)
Central hypothyroidism
-
(B)
Growth hormone deficiency
-
(C)
Adrenal insufficiency
-
(D)
Diabetes insipidus
-
(A)
-
4.
Which of the following statements regarding therapy for hypophysitis is incorrect?
-
(A)
High-dose steroid therapy or anti-inflammatory and immunosuppressive (methotrexate, cyclosporine A, azathioprine) treatments have been used with variable outcomes in granulomatous hypophysitis
-
(B)
Conservative management using clinical observation has been advocated as the primary therapeutic option in lymphocytic hypophysitis
-
(C)
Spontaneous remission is very frequent in patients with granulomatous hypophysitis
-
(D)
Transsphenoidal surgery should be performed in cases with progressive optic chiasmal compression, and when a definitive diagnosis is required for atypical presentation
-
(A)
Answers to Questions
-
1.
(A)
-
2.
(B)
-
3.
(C)
-
4.
(C)
Suggested Reading
Bellastella A, Bizzarro A, Coronella C, Bellastella G, Sinisi AA, De Bellis A. Lymphocytic hypophysitis: a rare or underestimated disease? Eur J Endocrinol. 2003;149:363–76.
Carmichael JD. Update on the diagnosis and management of hypophysitis. Curr Opin Endocrinol Diabetes Obes. 2012;19:314–21.
Caturegli P, Newschaffer C, Olivi A, Pomper MG, Burger PC, Rose NR. Autoimmune hypophysitis. Endocr Rev. 2005;26:599–614.
Dillard T, Yedinak CG, Alumkal J, Fleseriu M. Anti-CTLA-4 antibody therapy associated autoimmune hypophysitis: serious immune related adverse events across a spectrum of cancer subtypes. Pituitary. 2010;13:29–38.
Freda PU, Beckers AM, Katznelson L, Molitch ME, Montori VM, Post KD, et al. Pituitary incidentaloma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:894–904.
Gutenberg A, Hans V, Puchner MJ, Kreutzer J, Bruck W, Caturegli P, et al. Primary hypophysitis: clinical-pathological correlations. Eur J Endocrinol. 2006;155:101–7.
Laws ER, Vance ML, Jane Jr JA. Hypophysitis. Pituitary. 2006;9:331–3.
Leporati P, Landek-Salgado MA, Lupi I, Chiovato L, Caturegli P. IgG4-related hypophysitis: a new addition to the hypophysitis spectrum. J Clin Endocrinol Metab. 2011;96:1971–80.
Leung GK, Lopes MB, Thorner MO, Vance ML, Laws Jr ER. Primary hypophysitis: a single-center experience in 16 cases. J Neurosurg. 2004;101:262–71.
Author information
Authors and Affiliations
Corresponding author
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Yedinak, C.G., McCartney, S., Fleseriu, M. (2015). Idiopathic Granulomatous Hypophysitis Masquerading as a Pituitary Adenoma: Are There Reliable Diagnostic Criteria?. In: Davies, T. (eds) A Case-Based Guide to Clinical Endocrinology. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-2059-4_4
Download citation
DOI: https://doi.org/10.1007/978-1-4939-2059-4_4
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-2058-7
Online ISBN: 978-1-4939-2059-4
eBook Packages: MedicineMedicine (R0)