
Abstract
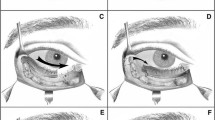
Elevation of the lateral brow is accomplished by thorough dissection of the temporal pocket inferiorly to the zygomatic arch and canthus. Fixation of the released and elevated temporal flaps is thought to be primarily accomplished by re-adherence of the flap. Fixation is performed by placement of one or two sutures to engage the temporoparietal fascia flap inferiorly and the deep temporal fascia superotemporally.
You have full access to this open access chapter, Download chapter PDF
Similar content being viewed by others


Keywords
Elevation is accomplished by thorough dissection of the temporal pocket inferiorly to the zygomatic arch and including a subperiosteal dissection at the superolateral orbital rim at least down to the canthus.
Fixation of the released and elevated temporal flaps is thought to be primarily accomplished by re-adherence of the temporoparietal fascia flap to the deep temporal fascia. To ensure that this occurs at the proper height, intraoperative fixation is performed by placement of one or two sutures (2-0 or 3-0) to engage the temporoparietal fascia flap inferiorly and the deep temporal fascia superotemporally.
-
A double skin hook can be passed into wound to engage the temporoparietal fascia flap permitting choice of best placement vector for suture. Traction with the hook will facilitate suture placement.
-
Avoid superficial passage of the suture resultant skin dimpling.
-
A rectangle of deep temporal fascia (exposing the temporalis muscle) can be excised under the temporoparietal fascia flap to enhance tissue readherence.
-
Sutures are tied with careful attention to symmetry between the two sides, using surgeons’ knots or the fisherman’s knot.
Midface extension over malar eminence is accomplished prior to fixation of the temporal flap. Continued subperiosteal dissection inferiorly along the lateral orbital rim will expose the proximal portion of the zygoma and can be continued over the malar eminence until the convex curvature makes visualization impossible. The zygomaticofacial nerve will be encountered and should be safeguarded. Release in this area will enhance the lift in the medial temporal region.
Repositioning of the lateral canthus can be accomplished through the endoscopic approach, but is difficult. Other oculoplastic techniques are better suited for this purpose.
Author information
Authors and Affiliations
Editor information
Editors and Affiliations
Rights and permissions
Copyright information
© 2015 Springer Science+Business Media New York
About this chapter
Cite this chapter
Fante, R.G. (2015). Elevation and Fixation of the Lateral Brow and Canthus. In: Hartstein, MD, FACS, M., Massry, MD, FACS, G., Holds, MD, FACS, J. (eds) Pearls and Pitfalls in Cosmetic Oculoplastic Surgery. Springer, New York, NY. https://doi.org/10.1007/978-1-4939-1544-6_94
Download citation
DOI: https://doi.org/10.1007/978-1-4939-1544-6_94
Published:
Publisher Name: Springer, New York, NY
Print ISBN: 978-1-4939-1543-9
Online ISBN: 978-1-4939-1544-6
eBook Packages: MedicineMedicine (R0)